yellow flags and exercise treatment: predictor or result of poor outcome?
DESCRIPTION
Yellow Flags and Exercise Treatment: Predictor or Result of Poor Outcome?. Ron Donelson, MD, MS SelfCare First, LLC. Red Flags. Yellow Flags. Others. Black Flags Family and system factors (insurance claim conflicts, overly solicitous family or health care provider). Red flags - PowerPoint PPT PresentationTRANSCRIPT

Yellow Flags and Exercise Treatment:Predictor or Result of Poor Outcome?
Ron Donelson, MD, MSSelfCare First, LLC
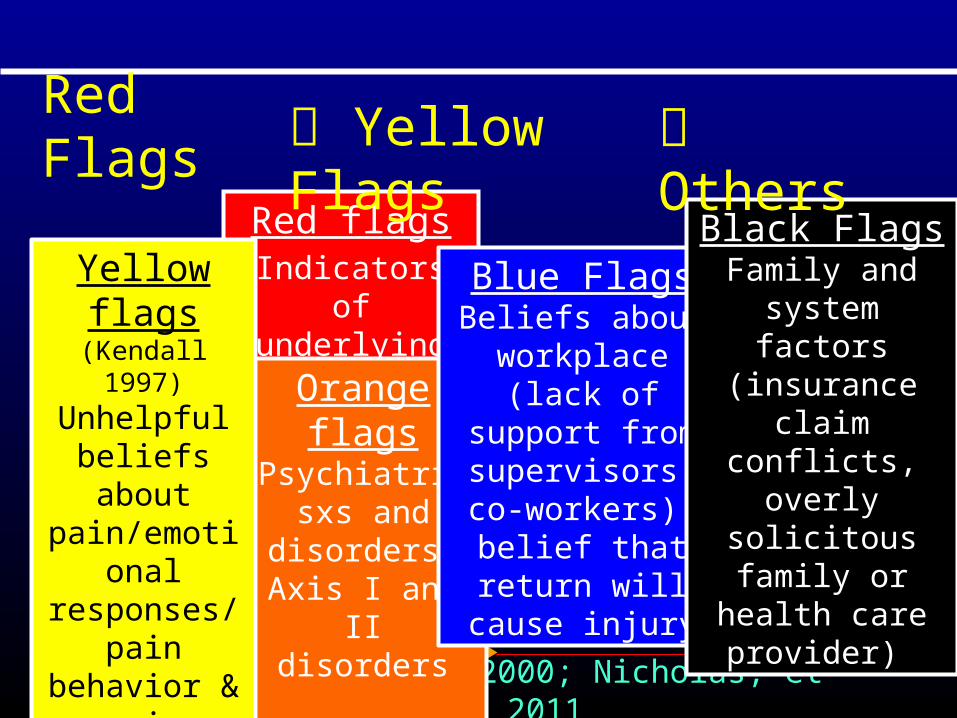
Red Flags
Red flagsIndicators of underlying insidious
pathology: spine fracture, tumor,
infx
Main & Burton, 2000; Nicholas, et al, 2011
Orange flagsPsychiatric sxs and disorders: Axis I and II
disorders
Blue FlagsBeliefs about
workplace (lack of support from
supervisors, co-workers); belief that
return will cause injury
Black FlagsFamily and system factors (insurance claim conflicts, overly solicitous family or health care provider)
Others
Yellow flags (Kendall 1997)
Unhelpful beliefs about
pain/emotional responses/pain
behavior & coping
Yellow Flags

Yellow Flags
Psychological and social factors that increase the likelihood of long-term disability and work loss in persons
with low back pain.
But not always.
Yellow flags: “Obstacles to Recovery”
More questions than answers..
Some YFs are indeed obstacles to recovery that need attention.
But some aren’t. They’re false-positives.
Q#1: How do we know which are which?

WARNING: Diagnosing low back pain means sorting through many false-positives
or misleading findings
Unreliable exam findings: asymmetries, tenderness Referred tenderness: SIJ, myofascial trigger points, pyriformis, trochanteric bursitis Imaging: HNPs and DDD in symptomatics
Q#2: Which findings are relevant? False-positives?
Q#3: Why are YFs sorelevant with LBP?
Why aren’t they also prominent with abdominal, chest, shoulder, hip or knee pain?
Or even spinal fractures, HNPs and sciatica?
Would making a patho-mechanical diagnosis (DP?) early make a difference?
Would making a diagnosisearly make a difference?
Q#4: Are YFs only relevant whenthe underlying diagnosis is uncertain?

Q#5: Do YFs cause pain to persist or does
persisting pain cause YFs to develop?
OR BOTH?

Do they ever co-exist?If so, which prevails?
Dir. pref. and centralization are found in most LBP patients and predict an excellent prognosis for recovery.
Consider:
In contrast, YFs are considered to be possible obstacles to recovery.

Centralization and Fear-Avoidance Beliefs
Centralizers have lower involvement of psychological factors.
The presence of yellow flags (elevated fear-avoidance beliefs) was associated with non-centralization.
Christiansen D, et al. Pain responses in rpted end-range spinal mvts and psycho’l factors in sick-listed pts with LBP: is there an association? J Rehabil Med. 2009.

Centralization and Fear-Avoidance
Fear-avoidance was equally present in centralizers and non-centralizers.
Even with high fear, centralization still predicted a good outcome in the majority. So in centralizers, addressing fear-avoidance beliefs is unnecessary.
If centralization is not present, but high levels of fear are, formal cognitive behavioral techniques should be used to address these beliefs.
Werneke M, Hart D, George S. Clinical outcomes for patients classified by fear-avoidance beliefs and centralization phenomenon. Arch Phys Med Rehab. 2009
Yellow flags were common: non-organic physical signs, overt pain behaviors, depressive symptoms, somatization, fear-avoidance beliefs, and perceived disability.
When treated with directional exercises, the outcomes at one year were so positive, the yellow flags were
non-predictors of outcome.
Werneke M, Hart DL. Centralization phenomenon as a prognostic factor for chronic low back pain and disability. Spine 2001
In 223 acute back and neck pain centralizers with a DP:
In 71 patients with a dir. pref.:
Both Beck Depression Inventory and Interference With Work and Leisure Activity significantly improved after just two weeks of matching directional exercises only.
It is futile to conduct prognostic studies without including baseline centralization/DP
determination.
Long A, Donelson R, Fung T. Does it matter which exercise? A randomized controlled trial of exercise for low back pain. Spine 2004
All studies of LBP outcome predictors need to include baseline determination of
the presence or absence of both:
Yellow FlagsDirectional Preference
On the other hand…..with directional preference so common and
so strongly predictive of good outcomes with appropriate directional treatment….
How important is baselineYellow Flag determination?
Yellow flags may only have relevance if MDT evaluation and treatment fail….
Along with imaging, injections, and surgeries.
As high quality MDT becomes thefront-line of care for painful cervical
and lumbar disorders….
yellow flags, imaging, medications, injections, and surgeries need only be considerations for a
small percentage of patients.
17
a non-specific symptom that once was attributed to non-physical issues:
immorality, lack of faith, etc.
But innovative diagnostic technologies:microscope microbes infection, and
sensitivities to antibiotics.
FEVER
> 60% of health care budget 14%.
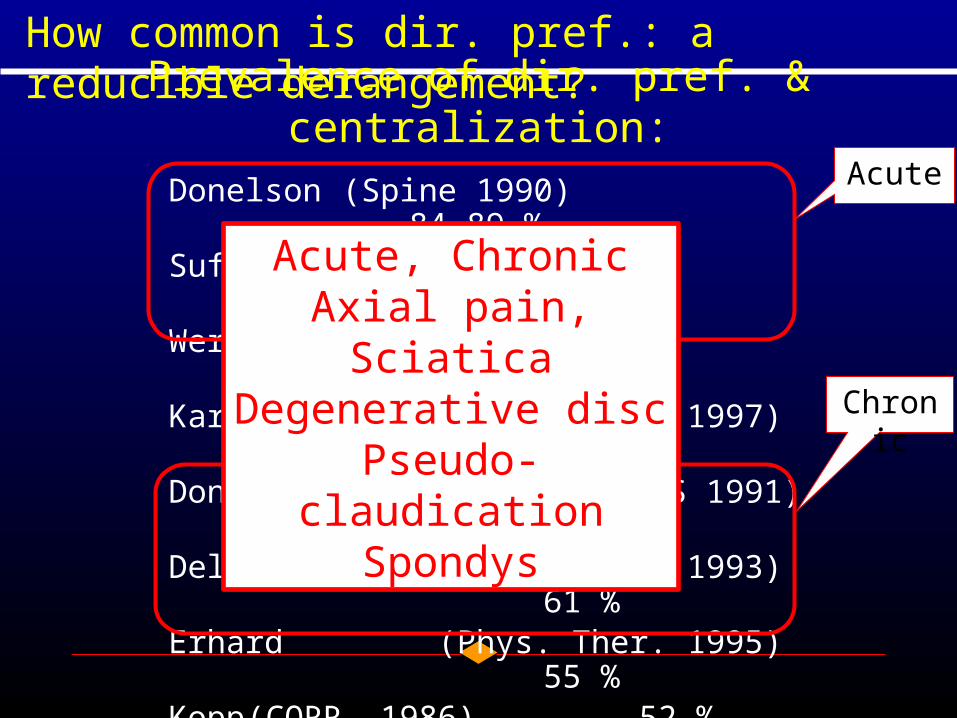
Prevalence of dir. pref. & centralization:
Donelson(Spine 1990) 84-89 %Sufka (JOSPT, 1998) 60-83 %Werneke (Spine, 1999) 77 %Karas (Phys. Ther. 1997) 73
%Donelson(Spine 1991, ISSLS 1991) 58 %Delitto (Phys. Ther. 1993) 61
%Erhard (Phys. Ther. 1995) 55
%Kopp (CORR, 1986) 52 %Long (Spine, 1995) 43
%Donelson (Spine ,1997) 49
%Laslett (Spine Jrnl, 2005) 32 %
Acute
Chronic
How common is dir. pref.: a reducible derangement?
Acute, ChronicAxial pain, SciaticaDegenerative disc
Pseudo-claudicationSpondys
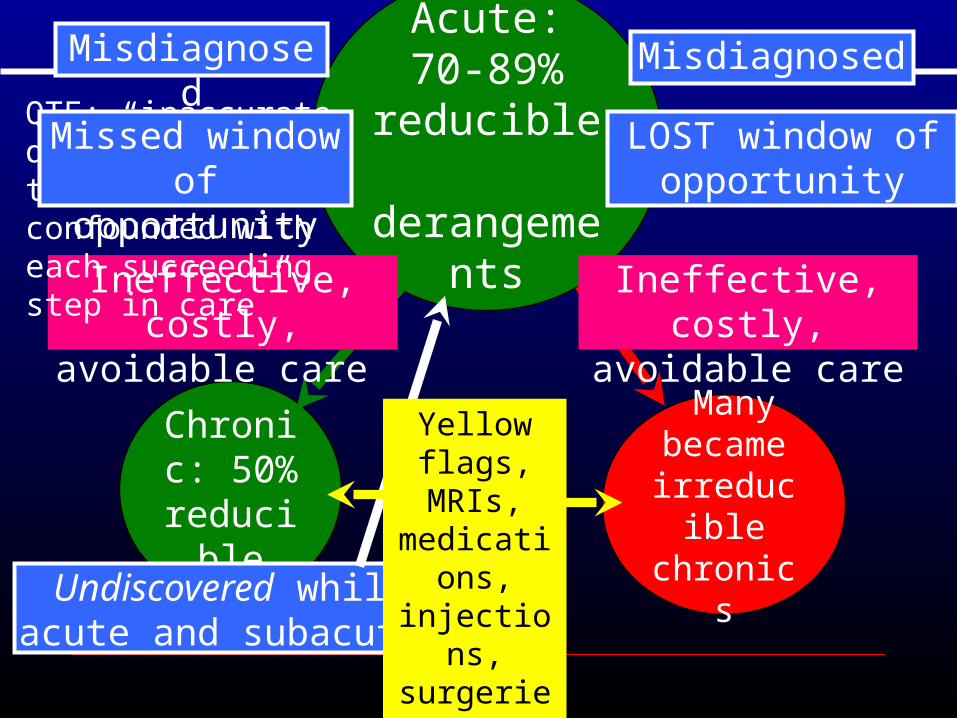
Chronic: 50%
reducible
Acute: 70-89%
reducible derangements
Many became
irreducible chronics
Misdiagnosed
Ineffective, costly, avoidable care
LOST window of opportunity
Undiscovered whileacute and subacute.
Ineffective, costly, avoidable care
Misdiagnosed
QTF: “inaccurate dxs which are then further confounded with each succeeding step in care”
Missed window of opportunity
Yellow Flags
Yellow flags, MRIs, medications, injections, surgeries

After TESIs, MDT exam repeated
Total Relief N-C No Surg N-C+Surgery Centralizers0
5
10
15
20
25
30
35
Series 1
69 non-centralizers
van Helvoirt H, et. al. Transforaminal epidural steroid injections followed by Mechanical Diagnosis and Therapy to prevent surgery for lumbar disc herniation. Pain Medicine. 2014.
16% 16%
22%
46%
Cen
tral
izer
s
38% Non-Centralizers
underwent TESIs.
Yellow Flags?
Recurrences: Benign or Worsening? Survey of 589 respondents with LBP:
• 73% had prior episodes; 54% had 10 or more and 19% had more than 50 episodes.
• 61% had recent episodes worse than prior ones; 21% were worse in all 5 surveyed domains.
Conclusion: Recurrences often worsen over time.
Donelson R, McIntosh G, Hamilton H. Is it time to rethink the typical courseof low back pain? Physical Medicine & Rehabilitation Journal. 2012.
Recurrences often progressively worsen and last longer….
Until recovery finally stops……and pain becomes constant and chronic?
Are worsening recurrences acommon a pathway to chronicity?
Ques: If dir. pref. is found in 70-90% ofacute LBP, predicts excellent
outcomes and prevents recurrences using directional exercises, what is the biggest
obstacle to recovery?Answer: Depriving patients of
a good MDT assessment.
A far more significant obstaclethan the presence of yellow flags?

Chronic: 50%
reducible
Acute: 70-89%
reducible derangements
Chronic: 30%(?)
now irreducible
All preventable!
Accurate mechanical
diagnosis when acute or subacute
So are YFs the biggest obstacle to recovery from LBP and neck pain?
Not if their influence disappears in the presence of a dir. pref.
If 70-89% of acute LBP have a dir. pref., then YFs are only
relevant in the other 11-30%.
To minimize the effects of Yellow Flags, LBP clinical guidelines recommend
reassurance of likely recover…..based on the positive natural history.
What could possibly be more reassuring than showing a patient that their pain is reversible and
that they can eliminate it themselves?
Is that why Yellow Flags disappearas obstacles to recovery with Dir. Pref.?

Red Flags Yellow Flags
Red flagsIndicators of underlying insidious
pathology: spine fracture, tumor,
infx
Main & Burton, 2000; Nicholas, et al, 2011
Yellow flags (Kendall 1997)
Unhelpful beliefs about
pain /emotional responses / pain
behavior & coping
Orange flagsPsychiatric sxs and disorders: Axis I and II
disorders
Blue FlagsBeliefs about
workplace (lack of support from
supervisors, co-workers; belief that
return will cause injury
Black FlagsFamily and system factors (insurance claim conflicts), overly solicitous family or health care provider
Green FlagDirectional preference /
centralization