zimbabwe quality assurance and quality improvement
TRANSCRIPT

Quality Assurance and QualityImprovement Strategy
2016-2020
Ministry of Health and Child Care
ZIMBABWE

Quality Assurance and QualityImprovement Strategy
2016-2020
Ministry of Health and Child Care
ZiMbabwe
Printed bySupporting the National Health Strategyto improve access to quality healthcare in Zimbabwe
HealthDevelopment FundM
INIS
TRYOF HEALTH & CHIL
DC
AR
E
PR
IMARY HEALTH
CAR
E
AH
EALTH Y NATION
ZIM BAB WE
FOREWORD
e mission of the Ministry of Health and Child Care in line with the Primary Health CareApproach is “to provide, administer, coordinate, promote and advocate for the provisionof equitable, appropriate, accessible, affordable and acceptable quality health services andcare to Zimbabweans while maximizing the use of available resources.” It is thereforeimportant the country has a policy on Quality Assurance and Quality Improvement(QA/QI) with the ultimate aim of providing the highest quality of healthcare services tothe people of Zimbabwe. I sincerely believe that this is achievable and we have the potentialto deliver.
e development of the QA/QI Strategy was a consultative process involving multiplestakeholders in the Health Sector. is was led by the Ministry of Health and Child Careincluding, public, mission, private and public health programs and projects in the countrywith technical assistance from partners. ematic working groups with wide stakeholderrepresentation were instrumental in the development of this strategy. e two main focusareas of the strategy are the horizontal dimension of the strategy dealing with QI of cross-cutting issues related to health service organisation, and the vertical dimension of thestrategy dealing with QI for disease specific issues.
We are aware of the challenges in delivery of reliable and responsive high quality healthcareand improving people’s lives. is strategy provides a basis for all to focus our combinedefforts on what is required to address current and future challenges to ensure high qualityhealthcare for ourselves and generations to come.
Brigadier G. Dr. B.GwinjiSecretary Minister of Health and Child Care
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe i
ACKNOWLEDGEMENTS
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabweii
e Quality Assurance (QA) and Quality Improvement (QI) Department within theMinistry of Health and Child Care (MOHCC) would like to acknowledge the contributionof various individuals and organisations to the formulation of the QI Strategic plan forHealth in Zimbabwe. eir contributions were through providing information duringinterviews, relevant documents and participating in thematic group discussions. e listof contributing persons and organisations is listed in appendix section. Special thanks goesto Secretary for Health and Child Care Brigadier General Dr G. Gwinji and Dr D. G.Dhlakama Principal Director Policy Planning Monitoring and Evaluation for their excellentsupport throughout the strategy development process.
e QA and QI department acknowledges the Maternal and Child Health IntegratedProgram (MCHIP) for financial and technical support in hiring of the consultants andconvening of stakeholder meetings. e QA and QI department also acknowledges thetechnical contributions of Prof R Kambarami, Dr H Chiguvare from MCHIP, and Dr JKeatinge from USAID.
Likewise, the QA and QI department would like to also acknowledge the financial andtechnical contributions of the World Bank via support for a consultant and ongoingcontributions to the QA/QI policy and strategy documents.
e consultancy services for desk review, coordination, writing and final production of thedocument were provided by Dr N Masuka, Dr K Hill and Dr G Shambira. e QAdepartment led by Dr Z Chiware provided secretarial support and coordination ofstakeholders who participated in the formulation of this strategy. e final editing andproof reading was done by Drs Endris Mohammed, B. B. Khabo and J. Z. Chiware.
EXECUTIVE SUMMARY
e health sector in Zimbabwe is in recovery mode aer a decade of significant challengesspanning from inadequate financing and shortages of qualified staff, poor infrastructureand obsolete equipment. As the health sector recovers, it is important that QualityAssurance (QA) and Quality Improvement (QI) be embedded and become a culture ofdoing business in the Health Sector.
e development of the QA/QI strategy was led by the MOHCC through a consultativeprocess involving selected stakeholders including Provincial and District Health Executiveteams, public and private health workers, Non-Government Organisations and technicalpartners involved in the health sector. e process started in late 2012, with support froma team of two consultants who were hired with specific terms of reference. A series ofmeetings, key informant interviews and stakeholder workshops were conducted fromsituation analysis to draing of a policy framework culminating in the strategic plan. Fourmain thematic working groups were formed on: Standards of Healthcare; Patient/ClientSafety; Patient/Client Satisfaction; and Health Worker Attitudes and Performance.
Among major strengths noted were the existence of institutions for setting standards suchas Standards Association of Zimbabwe (SAZ) and regulatory bodies such as the HealthProfessions Authority. Political commitment to QA/QI was demonstrated by theestablishment of a Quality Assurance and Improvement Directorate in the MOHCC.Within the health sector there are a number of treatment guidelines and protocols whichif adhered to, will help in the standardization of care and improved outcomes.Opportunities that may enhance QA/QI include existence of patient and service charters,recent lessons from the Performance Based Financing pilot in 18 districts of Zimbabwe,as well as health centre committees for more meaningful participation of communities inhealth care. e Standardized Maternal Care project by MCHIP in Manicaland alsodemonstrated the feasibility of implementing QI initiatives with existing resources. reatsto successful implementation of QA/QI relate mainly to underfunding and donordependency on health financing.
e target audience for this QA/QI framework includes all health providers, planners,programme managers, implementers, teaching/academic institutions, partners in theprivate and public sectors, non-governmental organisations in the health sector, patients,families and communities. e aim of this strategy is to guide the process of ensuringquality as well as continual quality improvement in both public and private sectors in thehealth sector. e vision and mission are articulated in the main body of the document.
e strategy takes a systems approach to improving and sustaining high-quality healthservices in Zimbabwe, highlighting cross-cutting priority intervention areas related to theWorld Health Organisation’s health system building blocks and priority quality domains(e.g. safety, clinical effectiveness) and priority interventions in vertical disease control
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe iii
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabweiv
programs targeting major causes of morbidity and mortality. e simultaneous focus onstrengthening essential cross-cutting health system functions and continuous improvementof vertical disease programs will help to build a strong health system capable of continuousimprovement for achieving optimum health for all Zimbabwean citizens.
Mechanisms for implementation of the strategic plan include the creation of a nationaladvisory committee and technical working groups, creation and support of regional anddistrict QI focal points, regular monitoring of priority quality measures within the healthinformation system tailored to specific stakeholders, as well as provisions for monitoringof the strategy implementation.
Executive Summary
TABLE OF CONTENTS
Foreword ............................................................................................................................................iAcknowledgements ...............................................................................................................................iiExecutive Summary .............................................................................................................................iiiTable of Contents ...................................................................................................................................vAcronyms .........................................................................................................................................viiDefinitions of Terms ............................................................................................................................ix
1. baCKGROUND............................................................................................................11.1 Strategy Development Process ......................................................................................21.2 Situation Analysis ............................................................................................................2
Zimbabwe Health Status.................................................................................................2Child Health.....................................................................................................................3Gaps in the quality of care for newborns, infants and under 5 years to be addressed by this strategy .....................................................................................5Maternal Health...............................................................................................................6Gaps in quality of maternal care to be addressed by this strategy ............................7HIV and AIDS .................................................................................................................7Gaps in HIV and AIDS quality of care to be addressed by this strategy .................9Malaria............................................................................................................................10Non Communicable Diseases (NCDs).......................................................................10
1.3 Strengths, Weaknesses, Opportunities and reats (SWOT) Analysis..................11Strengths: ........................................................................................................................11Weaknesses:....................................................................................................................11Opportunities: ...............................................................................................................12reats: ...........................................................................................................................12Experience and Progress so far in QI initiatives in Zimbabwe ...............................13Anti-Retroviral erapy (ART) Quality Improvement............................................13Quality Improvement in PMTCT ...............................................................................14Improving the quality of Maternal and Newborn Care in Zimbabwe ...................15
2. THe NaTiONaL QUaLiTY iMPROVeMeNT STRaTeGiC FRaMewORK ........17Rationale for a Strategy on Quality Improvement in Health Care .........................17
2.1 Aim and Guiding Principles of the Strategy..............................................................18Guiding Principles ........................................................................................................18
2.2 Strategic Objectives, Priorities and Interventions.....................................................19Conceptual Framework for National QI Strategy.....................................................19
2.3 Quality Improvement Principles and Methodologies ..............................................36
3. iMPLeMeNTaTiON OF THe Q1 STRaTeGY.........................................................37National Level ................................................................................................................39Government ...................................................................................................................41Private for Profit Sector (Private providers from different sectors including private hospitals, surgeries, laboratories, pharmacies) ...........................41
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe v
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwevi
Community Representatives, Civil Society, Non-governmental Organisations.................................................................................................................42
3.1 Perfomance Measurement in Quality.........................................................................42Quality Assessment Indicators ....................................................................................43Sources of Data ..............................................................................................................44
3.2 Monitoring and Evaluation..........................................................................................45Data Analysis and Reporting.......................................................................................46
aNNeXeS ...........................................................................................................................49Annex A: Quality Improvemnt Methodologies...............................................................49
Model For Improvement – Plan-Do-Study-Act Model ................................50Clinical Practice Improvement (CPI)..............................................................52Root Cause Analysis ..........................................................................................53Quality Improvement Collaborative................................................................53
Annex B: List of Participants in Strategy Plan Formulation..........................................56
TabLe OF FiGUReS
Figure 1: Life Expectancy at birth in Zimbabwe and sub-Saharan Africa 1992-2012 .............................................................................................................3
Figure 2: ZDHS Infant Mortality and Under 5 Mortality in Zimbabwe between 1999-2014:.........................................................................................................3
Figure 3: Fresh Still Births per 1000 live births by province and central institutions 2012...............................................................................................................4
Figure 4: Early Neonatal deaths per 1000 live births by province and institution Zimbabwe, 2012............................................................................................4
Figure 5: ZDHS Maternal Mortality Ratio Trends, Zimbabwe 1999-2014...............................6Figure 6: Institutional maternal deaths by province and institution,
Zimbabwe, 2012...............................................................................................................6Figure 7: ZDHS Trends in HIV Prevalence, Zimbabwe 2005-2011 ..........................................8Figure 8: Quality Improvement relationships ............................................................................38Figure 9: Support and Supervision for QI...................................................................................46Figure 10: Model for Improvement................................................................................................51
TabLeS
Table 1: Number of neonatal, infant and under 5 deaths by specific disease and rural provinces in Zimbabwe, 2012 .......................................................................5
Table 2: Delivery in health facility and skilled attendance at birth by province in Zimbabwe, ZDHS 2010/11 ........................................................................7
Table 3: HIV Prevalence by province, ZDHS 2010-11 ..............................................................8Table 4: Dimension 1 - Strategic and Intermediate Objectives, Key Activities,
Indicators and projected costs .....................................................................................20Table 5: Dimension 2 - Priority health areas and associated high impact
interventions, QI approaches, quality of care indicators and projected costs................................................................................................................28
Table of Contents
ACRONYMS
AMTSL Active Management of ird Stage of Labour
ART Anti-Retroviral erapy
BMI Body Mass Index
CCZ Consumer Council of Zimbabwe
CME Continuing Medical Education
CPD Continuing Professional Development
CQI Continuous Quality Improvement
CVD Cardiovascular Disease
DHE District Health Executive
EDLIZ Essential Medicine List of Zimbabwe
EMR Electronic Medical Record
ENND Early Neonatal Death
EPMS Electronic Patient Monitoring System
FSB Fresh Still Birth
HPA Health Professions Authority
HMIS Health Management Information System
ICU Intensive Care Unit
IMR Infant Mortality Rate
ISO International Standards Organization
IYCF Infant and Young Child Feeding
MCAZ Medicines Control Authority of Zimbabwe
MDPCZ Medical and Dental Professions Council of Zimbabwe
MIMS Multiple Indicator Monitoring Survey
MNCH Maternal Newborn and Child Health
MMR Maternal Mortality Ratio
MOHCC Ministry of Health and Child Care
MOU Memorandum of Understanding
NCD Non-Communicable Diseases
NDTPAC National Medicines and erapeutics Policy Advisory Council
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe vii
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabweviii
NIHFA National Integrated Health Facility Assessment
NQIC National Quality Improvement Committee
ORT Oral Rehydration erapy
PDSA Plan-Do¬-Study-Act
PHC Primary Health Care
PHE Provincial Health Executive
PMTCT Prevention of Mother to Child Transmission
PPH Post-Partum Haemorrhage
QA Quality Assurance
QAD Quality Assurance Department
QI Quality Improvement
QMS Quality Management System
RBM Results Based Management
RBF Results Based Financing
ROM Rupture of Membranes
RUTF Ready to Use erapeutic Feeds
SAZ Standards Association of Zimbabwe
SOP Standard Operating Procedures
STI Sexually Transmitted Infection
SWOT Strength Weaknesses Opportunities and reats
TB Tuberculosis
U5MR Under 5 Mortality Rate
VMAHS Vital Medicines Availability and Health Services Survey
WHO World Health Organisation
ZANSP Zimbabwe AIDS National Strategic Plan
ZDHS Zimbabwe Demographic and Health Survey
ZINARA Zimbabwe National Road Authority
ZNHS Zimbabwe National Health Strategy
ZINQAP Zimbabwe Quality Assurance Programme (ZINQAP)
Acronyms
DEFINITION OF TERMS
best Practice: A way or method of accomplishing a function or process that is consideredto be superior to all other known methods. In health care, it is oen used torefer to tools, materials, and models of care, organisational arrangements, andother practices that have been shown in multiple settings to facilitatecompliance with evidence-based standards of care.
Collaborative: A systematic approach to health care quality improvement in whichorganisations and providers test and measure practice innovations, then sharetheir experiences in an effort to accelerate learning and widespreadimplementation of best practices.”Everyone teaches, everyone learns”
Continuous Quality improvement: An approach to health care based on evaluation ofa product or the outcome(s) of a process, and an understanding the needs andexpectations of the consumers of these products or processes.
Quality assurance: A system to support performance according to standards. It impliesa systematic way of establishing and maintaining quality improvementactivities as an integral and sustainable part of systems or organisations. isincludes all activities that contribute to the design, assessment, monitoring ofstandards agreed upon by all stakeholders and improving quality of servicedelivery, client satisfaction and effective utilization.
Quality improvement: An interdisciplinary process designed to raise the standards ofthe delivery of preventive, diagnostic, therapeutic and rehabilitative measuresin order to restore and improve health outcomes of individuals and populationsfocusing on systems, clients, processes, team work and use of data.
Quality Management: e application of management practice to systematically maintainand improve organisation-wide performance.
indicator: A measurable variable (or characteristic) that can be used to determine thedegree of adherence to a standard or the level of quality achieved.
Quality: ere are many definitions, but for our purposes, quality is defined as theextent to which health care, services, systems, and programmes conform tonational or international standards/ requirements/ specifications. Accordingto the Institute of Medicine (IOM), health care is of high quality if it is safe,effective, patient-centred, timely, efficient; and equitable.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe ix
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwex
Quality improvement initiatives: Cycles of interventions that are linked to assessmentand that have the goal of improving the process, outcome, and efficient ofcomplex systems or simply put: interventions for assessing, measuring, definingand resolving health care delivery issues with an aim to improving the safety,timeliness, equity, access, and appropriateness of health care services.
Patient Centred Care: Providing care that is respectful and responsive to individualpreferences, needs and values and ensures that patient values guide all clinicaldecisions
Patient Safety: e prevention of errors and adverse events to patients associated withhealth care.
Standard of Care: Preformed and agreed upon statements issued for the purpose ofinfluencing decisions and health interventions.
Plan-Do-Study-act (PDSa) Cycle: A process to describe quality improvement cycleusing four steps: Plan, Do, Study, Act. It is sometimes referred to as the Shewartor as the Deming cycle.
Definition of Terms
BACKGROUND
Overview of the Zimbabwe Health System
At Independence in 1980, Zimbabwe adopted the Primary Health Care (PHC) Approachin line with the Alma Ata Declaration of 1978. e implementation of the PHC approachresulted in decentralization of health service provision from central level (cities and towns)to administrative wards at district level in the rural communities. Four tiers for healthservice delivery were established as follows:
l Quaternary Level: Central Teaching Hospitals with specialist medical services in thecapital city Harare, the second largest city Bulawayo and in Chitungwiza.
l Tertiary Level: Provincial Hospitals with ambulatory and inpatient specialist servicesin the eight rural provinces of Zimbabwe.
l Secondary Level: District Hospitals with emergency, ambulatory and inpatientservices in the sixty-two districts of Zimbabwe.
l Primary Level: Rural Health Centers with primary care services in the 220 wards ofZimbabwe.
is decentralization was associated with a significant improvement of most healthindicators in the 1980s and early 1990’s. It is in the context of a decentralized health systemthat quality of care will be viewed in this strategy. In addition there is a private for profitsector whose operations will also be guided by this strategy.
e Zimbabwe health system has been undergoing a revitalization process since the launchof the Zimbabwe Health Sector Investment case in 2009, aer a near collapse on thebackground of socio-economic challenges which reached a peak in 2008. is process isembedded in the Zimbabwe National Health Strategy (ZNHS 2009-2015) in which thevision of the Ministry of Health and Child Care (MoHCC) is “to have the highest possiblelevel of health and quality of life for the citizens of Zimbabwe”.
e mission of the MoHCC as stated in the ZNHS 2009-15 is "to provide, administer,coordinate, promote and advocate for the provision of equitable, appropriate, accessible,affordable and acceptable quality health services and care to Zimbabweans whilemaximizing the use of available resources, in line with the primary health care approach.e provision of these services is guided by the Results Based Management system (RBM),which was adopted by the Zimbabwean government in 2005 as a performance monitoringand evaluation system.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 1
1

Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe2
1.1 STRATEGY DEVELOPMENT PROCESS
e development of the QI Strategy was a consultative process involving stakeholders inthe Health Sector. is was led by Task Force on quality improvement chaired by theMinistry of Health and Child Care directorate of Quality Assurance and Improvement.e Task Force comprised technical experts from MCHIP, USAID, the World Bank andtwo local consultants. e Task Force facilitated a desk review of policy and strategicdocuments in the MOHCC, and the two consultants carried out key informant interviewsand undertook a situational analysis of the quality of care within the public health facilities and institutions. Consultations with stakeholders from public, mission, private, civil society,technical partners and public health programs and NGO projects in the country wereundertaken.
Dimensions of Quality of Care
Major dimensions of quality of health care guiding the formulation of this strategy arenoted below. All except coordination of care are adopted from the Institute of Medicine(IOM) dimensions of quality:
effectiveness: delivering health care that is adherent to an evidence base and results inimproved health outcomes for individuals and communities, based on need.
efficiency: delivering health care in a manner which maximizes resource use and avoidswaste.
accessibility: health care that is timely, geographically reasonable, and provided in a settingwhere skills and resources are appropriate to medical need.
acceptable/patient-centred: health care, which takes into account the preferences andaspirations of individual service users and the cultures of their communities.
equity: health care, which does not vary in quality because of personal characteristics suchas gender, race, ethnicity, geographical location, or socioeconomic status.
Safety: delivering health care which minimises risks and harm to service users.
Coordination and continuity of care: Access to care provided by families andcommunities, by outpatient and outreach services, and by clinical services throughout thelifecycle, including adolescence, pregnancy, childbirth, the postnatal period, and childhood.Saving lives depends on high coverage and quality of integrated service-delivery packagesthroughout the continuum, with functional linkages between levels of care in the healthsystem and between service-delivery packages, so that the care provided at each time andplace, contributes to the effectiveness of all the linked packages.
1.2 SITUATION ANALYSIS
Zimbabwe Health Status
e life expectancy at birth for Zimbabwe decreased from 61 years in 1992 to 41 years in2002, which was lower than the average life expectancy at birth in sub-Saharan Africa.
Background1
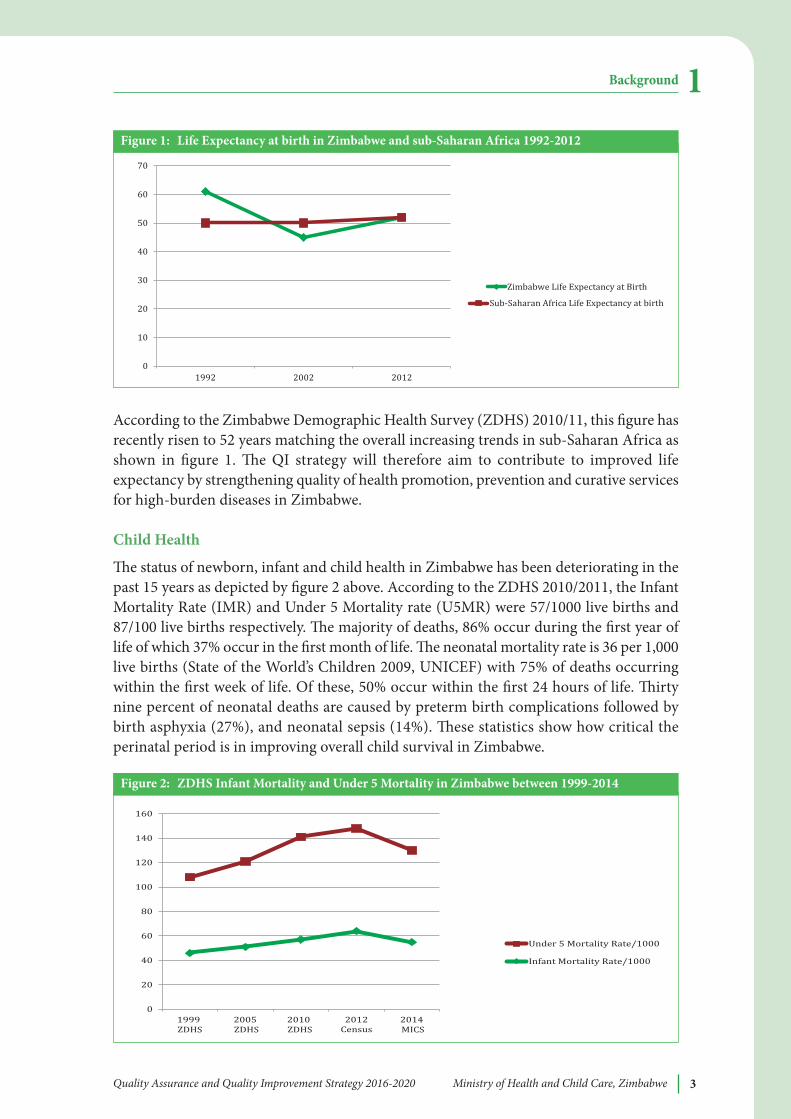
According to the Zimbabwe Demographic Health Survey (ZDHS) 2010/11, this figure hasrecently risen to 52 years matching the overall increasing trends in sub-Saharan Africa asshown in figure 1. e QI strategy will therefore aim to contribute to improved lifeexpectancy by strengthening quality of health promotion, prevention and curative servicesfor high-burden diseases in Zimbabwe.
Child Health
e status of newborn, infant and child health in Zimbabwe has been deteriorating in thepast 15 years as depicted by figure 2 above. According to the ZDHS 2010/2011, the InfantMortality Rate (IMR) and Under 5 Mortality rate (U5MR) were 57/1000 live births and87/100 live births respectively. e majority of deaths, 86% occur during the first year oflife of which 37% occur in the first month of life. e neonatal mortality rate is 36 per 1,000live births (State of the World’s Children 2009, UNICEF) with 75% of deaths occurringwithin the first week of life. Of these, 50% occur within the first 24 hours of life. irtynine percent of neonatal deaths are caused by preterm birth complications followed bybirth asphyxia (27%), and neonatal sepsis (14%). ese statistics show how critical theperinatal period is in improving overall child survival in Zimbabwe.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 3
Background 1
010203040506070
1992 2002 2012
Figure 1: Life expectancy at birth in Zimbabwe and sub-Saharan africa 1992-2012
020406080
100120140160
1999 ZDHS 2005 ZDHS 2010 ZDHS 2012Census 2014 MICS
Under 5 Mortality Rate/1000Infant Mortality Rate/1000
Figure 2: ZDHS infant Mortality and Under 5 Mortality in Zimbabwe between 1999-2014
Zimbabwe Life Expectancy at BirthSub-Saharan Africa Life Expectancy at birth
0

Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe4
e Fresh Still Birth (FSB) rate is a strong indicator of the quality of intra-partum care.Figure 3 shows that the country still has unacceptably high rates ranging from 40/1000 inMutare Provincial hospital to 7/1000 at Harare Central hospital and Mashonaland Eastprovince. e QI strategy must therefore give direction on ways to improve the quality ofcare to reduce the FSB rate.
Figure 4 below shows the Early Neonatal Deaths (ENND) per 1000 live births by institutionand province in 2012. ese ranged from a highest of 88/1000 in Harare Central hospitalto 11/1000 in Mashonaland Central, Matebeleland South and St Lukes hospital. e QIstrategy will prioritize strategies for reducing ENND in high-mortality institutions andprovinces by strengthening quality of Essential Newborn Care and early detection andevidence-based care for major causes of early neonatal mortality (asphyxia, sepsis andprematurity).
Background1
0
5
10
15
20
25
30
35
40
45
FSB Rate/1000 live births
Figure 3: Fresh Still births per 1000 live births by province and central institutions 2012
0
10
20
30
40
50
60
70
80
90
100
ENND/1000 live births
F
Figure 4: early Neonatal deaths per 1000 live births by province and institution Zimbabwe, 2012
Note: Data is from the national T5 series HMIS
Note: Data is from the national T5 series HMIS
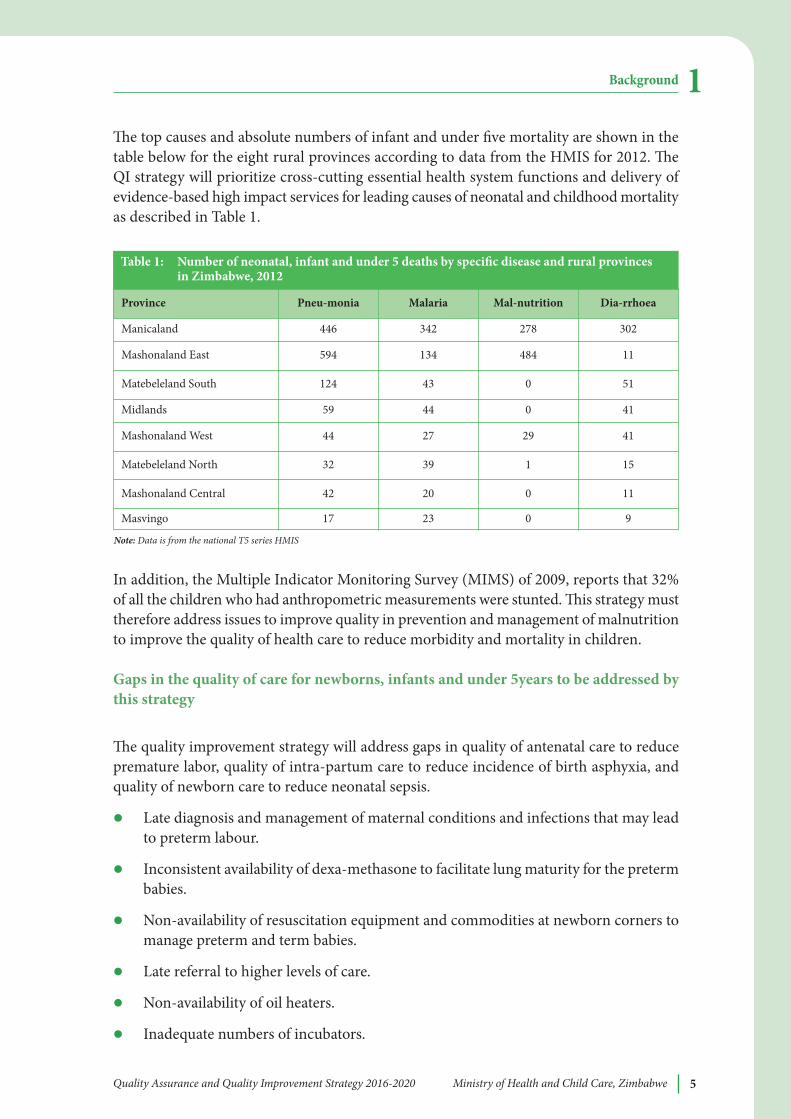
e top causes and absolute numbers of infant and under five mortality are shown in thetable below for the eight rural provinces according to data from the HMIS for 2012. eQI strategy will prioritize cross-cutting essential health system functions and delivery ofevidence-based high impact services for leading causes of neonatal and childhood mortalityas described in Table 1.
In addition, the Multiple Indicator Monitoring Survey (MIMS) of 2009, reports that 32%of all the children who had anthropometric measurements were stunted. is strategy musttherefore address issues to improve quality in prevention and management of malnutritionto improve the quality of health care to reduce morbidity and mortality in children.
Gaps in the quality of care for newborns, infants and under 5years to be addressed bythis strategy
e quality improvement strategy will address gaps in quality of antenatal care to reducepremature labor, quality of intra-partum care to reduce incidence of birth asphyxia, andquality of newborn care to reduce neonatal sepsis.
l Late diagnosis and management of maternal conditions and infections that may leadto preterm labour.
l Inconsistent availability of dexa-methasone to facilitate lung maturity for the pretermbabies.
l Non-availability of resuscitation equipment and commodities at newborn corners tomanage preterm and term babies.
l Late referral to higher levels of care.
l Non-availability of oil heaters.
l Inadequate numbers of incubators.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 5
Background 1
Table 1: Number of neonatal, infant and under 5 deaths by specific disease and rural provinces in Zimbabwe, 2012
Note: Data is from the national T5 series HMIS
Province Pneu-monia Malaria Mal-nutrition Dia-rrhoea
Manicaland 446 342 278 302
Mashonaland East 594 134 484 11
Matebeleland South 124 43 0 51
Midlands 59 44 0 41
Mashonaland West 44 27 29 41
Matebeleland North 32 39 1 15
Mashonaland Central 42 20 0 11
Masvingo 17 23 0 9
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe6
l Inconsistent availability of cleaning materials for infection control.
l Poor or no monitoring and evaluation of infection control procedures e.g. by doingswabs for microscopy culture and sensitivity.
l Inconsistent use of the partograph leading to failure by health workers to react in atimely and appropriate manner when emergencies or complications occur.
l Late diagnosis of neonatal sepsis.
l Inconsistent availability of antibiotics for treatment of neonatal sepsis.
l Inadequate staff trained in IMNCI guidelines
l Poor adherence to IMNCI guidelines on management of illnesses (pneumonia,diarrhoea and malaria)
l Late infant diagnosis of HIV and commencement of pediatric ART
l Late diagnosis and management of severe malnutrition
Maternal Health
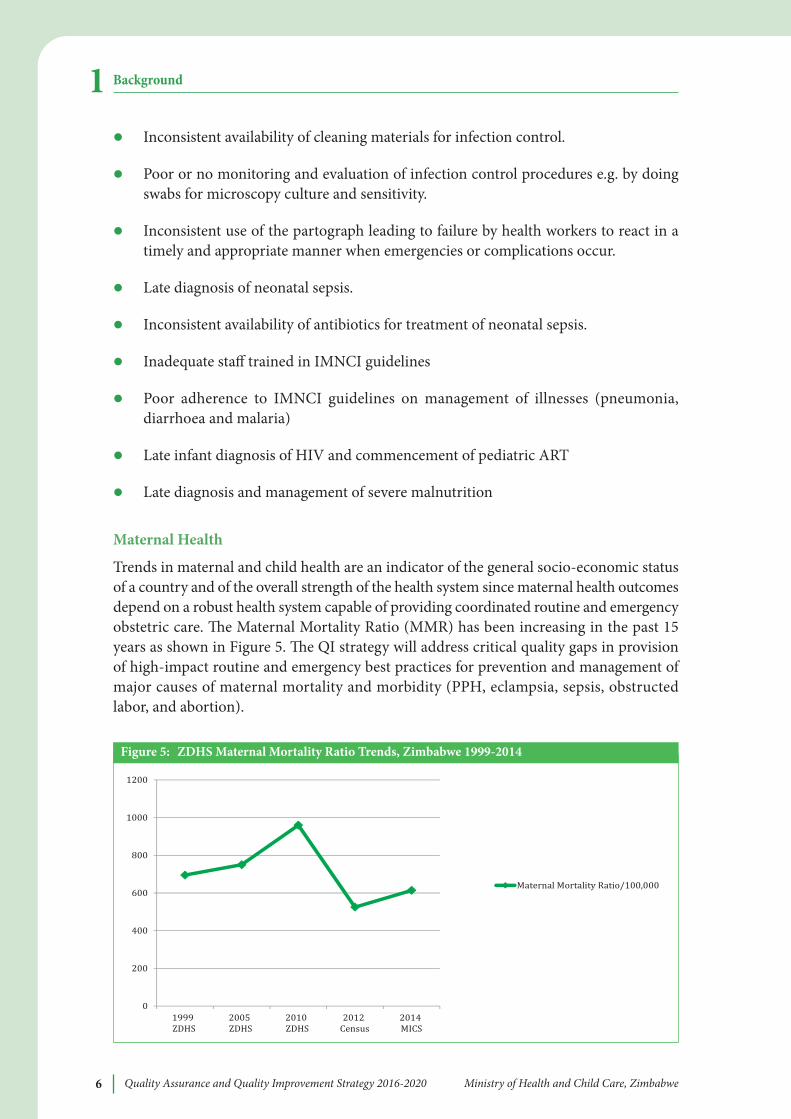
Trends in maternal and child health are an indicator of the general socio-economic statusof a country and of the overall strength of the health system since maternal health outcomesdepend on a robust health system capable of providing coordinated routine and emergencyobstetric care. e Maternal Mortality Ratio (MMR) has been increasing in the past 15years as shown in Figure 5. e QI strategy will address critical quality gaps in provisionof high-impact routine and emergency best practices for prevention and management ofmajor causes of maternal mortality and morbidity (PPH, eclampsia, sepsis, obstructedlabor, and abortion).
Background1
0200400600800
10001200
1999 ZDHS 2005 ZDHS 2010 ZDHS 2012 Census 2014 MICS
Maternal Mortality Ratio/100,000
Figure 5: ZDHS Maternal Mortality Ratio Trends, Zimbabwe 1999-2014
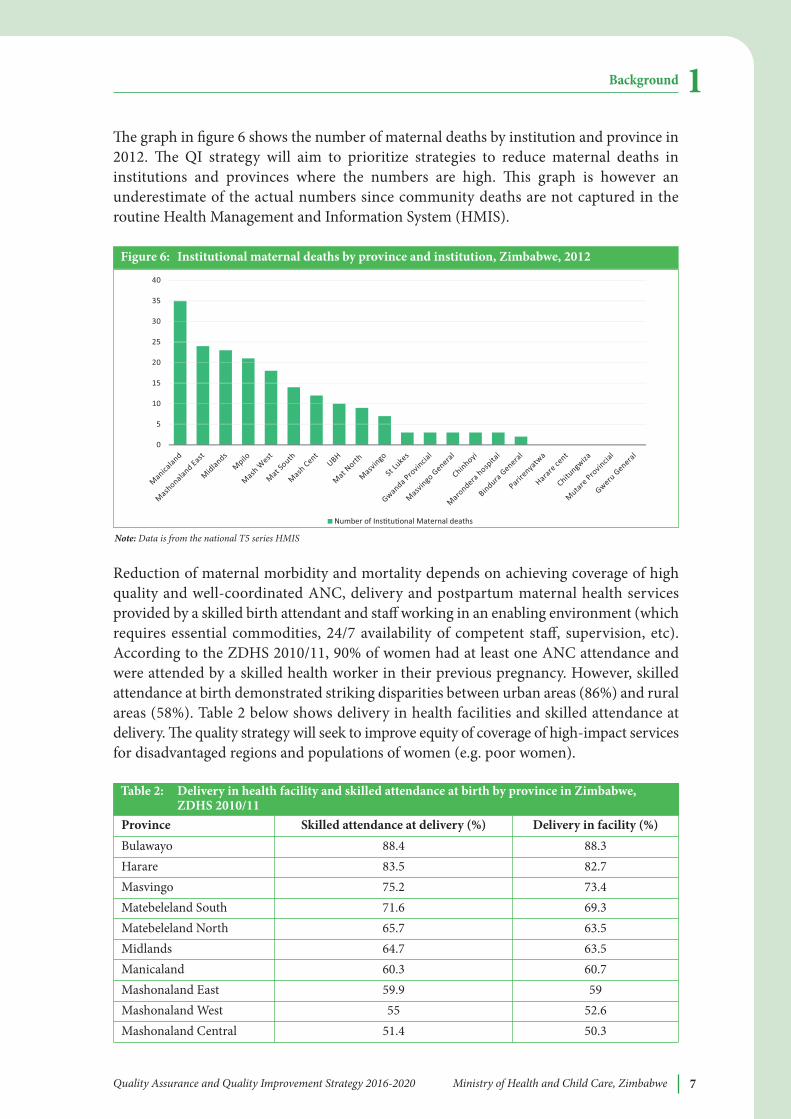
e graph in figure 6 shows the number of maternal deaths by institution and province in2012. e QI strategy will aim to prioritize strategies to reduce maternal deaths ininstitutions and provinces where the numbers are high. is graph is however anunderestimate of the actual numbers since community deaths are not captured in theroutine Health Management and Information System (HMIS).
Reduction of maternal morbidity and mortality depends on achieving coverage of highquality and well-coordinated ANC, delivery and postpartum maternal health servicesprovided by a skilled birth attendant and staff working in an enabling environment (whichrequires essential commodities, 24/7 availability of competent staff, supervision, etc).According to the ZDHS 2010/11, 90% of women had at least one ANC attendance andwere attended by a skilled health worker in their previous pregnancy. However, skilledattendance at birth demonstrated striking disparities between urban areas (86%) and ruralareas (58%). Table 2 below shows delivery in health facilities and skilled attendance atdelivery. e quality strategy will seek to improve equity of coverage of high-impact servicesfor disadvantaged regions and populations of women (e.g. poor women).
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 7
Background 1
0
5
10
15
20
25
30
35
40
Number of Ins tu onal Maternal deaths
Figure 6: institutional maternal deaths by province and institution, Zimbabwe, 2012
Note: Data is from the national T5 series HMIS
Province Skilled attendance at delivery (%) Delivery in facility (%)Bulawayo 88.4 88.3Harare 83.5 82.7Masvingo 75.2 73.4Matebeleland South 71.6 69.3Matebeleland North 65.7 63.5Midlands 64.7 63.5Manicaland 60.3 60.7Mashonaland East 59.9 59Mashonaland West 55 52.6Mashonaland Central 51.4 50.3
Table 2: Delivery in health facility and skilled attendance at birth by province in Zimbabwe, ZDHS 2010/11
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe8
Gaps in quality of maternal care to be addressed by this strategy
Some of the gaps in quality of maternal care are as follows:
l Poor history taking leading to missing of critical information to identify at riskpregnancies.
l Unavailability of BP machines and urinalysis kits.
l High patient midwife ratio in some institutions.
l Low skilled attendance at birth especially in rural institutions.
l Inconsistent utilization of the partograph leading to poor monitoring of labourresulting in delayed reactions.
l Non-availability of quality checklists in labour ward.
l Inconsistent availability of theatre drugs and commodities including oxygen.
l Late referral of critical cases.
l Lack of on-the-job supervision and mentorship.
l Inconsistent availability of blood and blood products.
l Inappropriate management of pregnancy induced hypertension, pre-eclampsia andeclampsia.
l Inconsistent availability of antibiotics for management of HIV related co morbidity.
HiV and aiDS
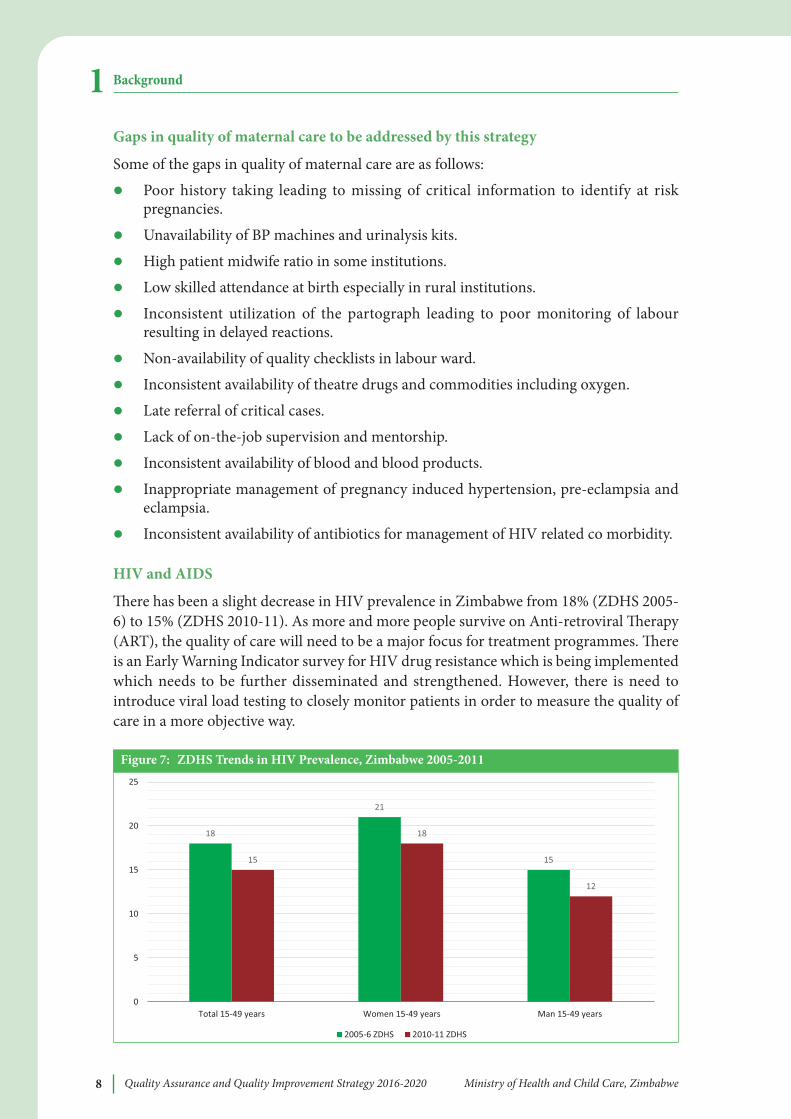
ere has been a slight decrease in HIV prevalence in Zimbabwe from 18% (ZDHS 2005-6) to 15% (ZDHS 2010-11). As more and more people survive on Anti-retroviral erapy(ART), the quality of care will need to be a major focus for treatment programmes. ereis an Early Warning Indicator survey for HIV drug resistance which is being implementedwhich needs to be further disseminated and strengthened. However, there is need tointroduce viral load testing to closely monitor patients in order to measure the quality ofcare in a more objective way.
Background1
18
21
1515
18
12
0
5
10
15
20
25
Total 15-49 years Women 15-49 years Man 15-49 years
2005-6 ZDHS 2010-11 ZDHS
Figure 7: ZDHS Trends in HiV Prevalence, Zimbabwe 2005-2011
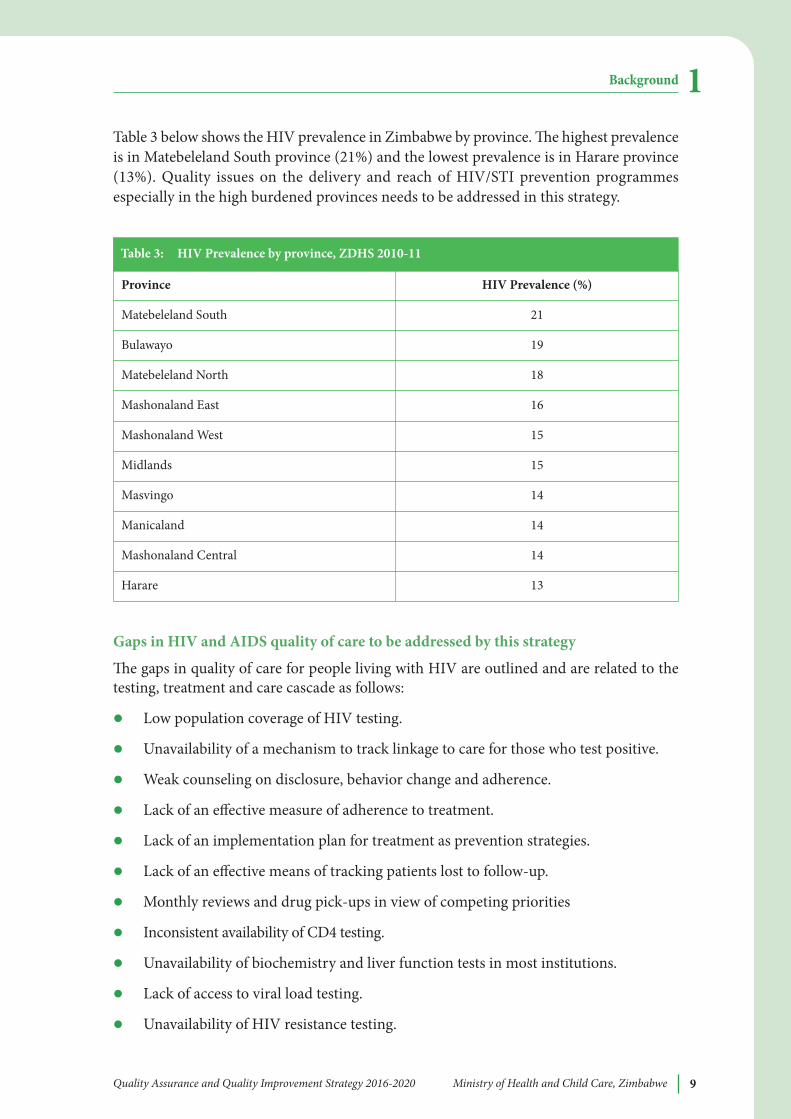
Table 3 below shows the HIV prevalence in Zimbabwe by province. e highest prevalenceis in Matebeleland South province (21%) and the lowest prevalence is in Harare province(13%). Quality issues on the delivery and reach of HIV/STI prevention programmesespecially in the high burdened provinces needs to be addressed in this strategy.
Gaps in HiV and aiDS quality of care to be addressed by this strategy
e gaps in quality of care for people living with HIV are outlined and are related to thetesting, treatment and care cascade as follows:
l Low population coverage of HIV testing.
l Unavailability of a mechanism to track linkage to care for those who test positive.
l Weak counseling on disclosure, behavior change and adherence.
l Lack of an effective measure of adherence to treatment.
l Lack of an implementation plan for treatment as prevention strategies.
l Lack of an effective means of tracking patients lost to follow-up.
l Monthly reviews and drug pick-ups in view of competing priorities
l Inconsistent availability of CD4 testing.
l Unavailability of biochemistry and liver function tests in most institutions.
l Lack of access to viral load testing.
l Unavailability of HIV resistance testing.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 9
Background 1
Province HiV Prevalence (%)
Matebeleland South 21
Bulawayo 19
Matebeleland North 18
Mashonaland East 16
Mashonaland West 15
Midlands 15
Masvingo 14
Manicaland 14
Mashonaland Central 14
Harare 13
Table 3: HiV Prevalence by province, ZDHS 2010-11
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe10
MalariaMalaria incidence has been on the decline in Zimbabwe in the past ten years and with oneprovince, Matebeleland South province entering the pre-elimination stage of malariacontrol. According to the ZDHS 2010-11, 41% of households had at least one mosquitonet and 29% had at least one insecticide treated mosquito net (ITN). Seventeen per cent ofhouseholds reported that they had received indoor residual spraying in the past 12 months.On the night before the survey, 14% of children under the age of 5 years slept under amosquito net.
Malaria case management audits have demonstrated above average adherence to malariadiagnosis and first line therapy. However, inadequate monitoring of in-patients with severemalaria has been associated with high case fatality rate. (Malaria Case Management Audit,2010).
Gaps in malaria quality of care to be addressed by this strategye gaps in quality of care in malaria care are related to prevention, suspicion, diagnosisand case management of malaria as outlined below;
l Low coverage of indoor residual spraying, inadequate insecticide treated nets, and lownumbers of children under 5 sleeping under treated nets.
l High suspicion of malaria at the expense of other differential diagnosis.
l Late diagnosis of malaria.
l Inappropriate case management of malaria.
l Poor management of complicated malaria.
l Late referral of complicated malaria cases.
Non Communicable Diseases (NCDs)Hypertension and its associated complications (stroke, heart and kidney failure) is themajor NCD affecting the Zimbabwean population and is now contributing more to theburden of disease in Zimbabwe. e WHO Stepwise approach to Surveillance (STEPs)survey conducted in Zimbabwe in 2005 showed a high prevalence of hypertension: 23.2%among adult males and 29% among adult females.1 increasingly, younger persons underthe age of 40 years are presenting with hypertension which is oen poorly controlled. isis against a background of low awareness of hypertension in the population and poor bloodpressure control among those on treatment, high prevalence of risk factors such as obesityamong females (32% prevalence), and alcohol and tobacco consumption among males.Evidence suggests that tertiary hospitals in Harare are now overwhelmed with increasingnumbers of individuals presenting with complications of uncontrolled NCDs such asstroke, heart and renal failure with increasing bed occupancy levels. ere has been asignificant increase in the incidence of cancers such as cervical, breast and prostate cancerin an environment where diagnostic and treatment facilities are limited.
Gaps in quality of care for Non-Communicable diseases to be addressed by this strategye gaps in quality of care of patients with non-communicable diseases remain extensivesince these conditions have been largely ignored over the past 10 years because of the focus
Background1

on MOHCC’s priorities which are mostly communicable disease control programs. Someof the gaps are:
l Non-availability of screening facilities and equipment for NCDs.
l Lack of diagnostic facilities for NCDs.
l Late presentation of patients with NCDs leading to avoidable deaths.
l Poor clinical management and monitoring of NCDs.
l Unavailability of drugs and commodities for the management of NCDs.
l Lack of effective follow-up mechanisms for patients with NCDs.
1.3 STRENGTHS, WEAKNESSES, OPPORTUNITIES ANDTHREATS (SWOT) ANALYSIS
ere are crosscutting health system weaknesses impairing optimal health systemfunctioning and delivery of high quality services in Zimbabwe. An overall SWOT analysisfor the provision of quality healthcare is summarised below:
Strengths:
l Existence of institutions responsible for setting standards of care such as the StandardsAssociation of Zimbabwe and regulatory bodies such as the Health ProfessionsAuthority among others.
l Commitment and leadership from the MOHCC to ensure QA&QI processes areadopted as evidenced by the formation of the Quality Assurance Department in theMOHCC.
l Existence of some clinical treatment, infection control, and clinical audit guidelines.
l Well established proficiency testing system for laboratories.
weaknesses:
l Underfunding of health services.
l Variable provider competence to deliver best practices.
l Low staffing levels against a background of high workload.
l Lack of well-defined quality management systems in health training institutions.
l Inconsistent and poor staff support and supervision, assessment of competences andevaluation of performance aer training.
l Non-systematic undertaking of clinical audits.
l Inadequate capacity of the QA department within the MOHCC to oversee QA&QIactivities.
l Lack of inclusion of quality of care (content) measures, including regular analysis ofsuch measures as part of routine facility health services and national and local HealthManagement and Information Systems.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 11
Background 1

Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe12
l Lack of improvement capacity and experience among mid-level managers and front-line health service delivery staff to support continuous improvement to overcomeimportant quality of care gaps.
l Lack of pre- and in-service competency based training on quality of care.
l Lack of data on major quality of care gaps and service delivery and health systemobstacles related to priority health conditions.
l Lack of good monitoring and feedback mechanism to allow two-way flow ofinformation.
l A health system fragmented along vertical programmes.
l Availability of essential commodities and stock management.
Opportunities:
l Political commitment at national level to the importance of quality for achievingpriority national health outcomes.
l Existence of Quality Assurance Department within the MOHCC.
l Commitment of partners and professional associations to QA&QI initiatives.
l Examples/models of good functional hospital quality management systems in placeto adopt.
l Several QA&QI initiatives in the country to learn from e.g. HIV/TB QA&QIinitiatives, Maternal, Newborn and Child Health QA&QI initiatives, Results BasedFinancing experiences.
l Existence of QA&QI policies and guidelines for some national programmes.
l New constitutional provisions prioritizing health as a human right.
l Institutional memory on QA&QI activities during the “good old days”.
l Existence of a patient’s charter.
l Existence of health centre committees.
l Availability of intrinsically motivated community health workers.
reats:
l Underfunding and inefficiencies in the utilisation of health care resources.
l Dependence on donors for funding of QA&QI activities.
l Expectations for remuneration from staff whenever QA&QI is mentioned.
l Lack of empowerment (education and knowledge of the patient’s charter).
l Resistance to change among providers and managers.
l Lack of data on the quality of care of the leading conditions of morbidity and mortalityin Zimbabwe.
Background1
Experience and Progress so far in QI initiatives in Zimbabwe
e MOHCC formed a Directorate of Quality Assurance at national level under thePrincipal Director of Policy Planning Monitoring and Evaluation, which is a sign of highlevel commitment to fulfil the mission of delivering quality health services. e Directorateof Quality Assurance with assistance from technical partners and stakeholders led theformulation of a QA&QI policy, which is now at final dra level and awaits approval andlaunching. is strategy recognises and seeks to build on QI initiatives already undertakenand in progress in different programmes, levels of care and areas of Zimbabwe. Severalquality improvement initiatives undertaken in Zimbabwe are briefly described below,highlighting key elements that have informed this strategy.
anti-Retroviral erapy (aRT) Quality improvemente MOHCC has piloted a quality improvement initiative in 83 of the 700 ART sites. eprogramme has 5 key elements:
l Performance measurement - using mostly process indicators along the ART cascadee.g. % of patients retained in care 6 and 12 months from enrollment (ART eligible andART-ineligible).
l Quality improvement - problem identification using management tools such asprocess mapping, 5 Whys fishbone analysis and prioritization of interventions usinga decision making matrix.
l Coaching and mentoring including peer learning and exchange visits.
l Consumer involvement - clients involved during training and development of QIimplementation plans. However no indicators have been developed to monitor thisinvolvement.
l Quality management system - organisational assessment to build the necessaryinfrastructure that supports QI.
Of the 83 sites that have been trained and participated in the initial phase of theperformance measurement process, 35 of them have started using the information gatheredto undertake quality improvement activities through ART QI subcommittees, which reportto the overall QI committee at the respective institution aer getting the training on basicprinciples of quality improvement. e ART quality improvement initiative is closely linkedto the recently introduced Electronic Patient Management system (EPMS) in 84 main ARTsites countrywide. is system allows the ART programme to easily capture qualityindicators used for performance measurement at both local and central levels.
e ART model of QI including the EPMS, provides a base on which this strategy can buildon. Other programmes and clinical disciplines can adapt this strategic framework to suittheir needs for QI.
electronic Patient Management System – Since the inception of HIV/TB programme, allpatient related data has been collected using a manual paper based system. e manualsystem has been unable to function properly owing to increased number of patientsrequiring HIV/TB services and this affected accurate monitoring, tracking and reporting
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 13
Background 1
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe14
of patients accessing HIV/TB services. e quality of data was suffering because of the highworkload but also because of the challenge of tracking the ‘drop-out’ rate of patients fromthe system (e.g. moving to another clinic, death, not coming to an appointment etc.). Inaddition, health workers are spending significant amounts of time entering data intoregistries or generating monthly monitoring tallies. To address this gap and to ensure thatHIV/TB data is collected in a timely manner and is of good quality, the MOHCC resolvedto establish an electronic system to collect and manage patient level HIV/TB data.
e roll out of the EPMS is on course although there are some challenges. ese include:
l Inadequate funding to conduct supportive visits to sites.
l Internet Service Provider (ISP) Network not covering all health facilities
l Frequent power cuts.
l Few teams responsible for installations, maintenance and trainings.
l Inadequate IT skills among most health care workers.
Quality improvement in PMTCTIn 2012, the MOHCC with support from EGPAF piloted a QI initiative for PMTCT atfacility level that started with the sensitization of District Medical Officers, District NursingOfficers and PMTCT District Focal Persons. Concepts, processes, planning anddocumentation tools were developed focusing on 4 specific areas:
l CD4 count testing for pregnant women.
l ART initiation for eligible pregnant women.
l Early Infant diagnosis.
l Early infant ART initiation.
Aer the introduction of Option B+ for PMTCT in 2014, the indicators on CD4 count,Early infant ART initiation and ART initiation for eligible pregnant women were revisedaccordingly and a new additional indicators was added. e revised and the newlyindicators are:
l ART initiation in ANC for all HIV positive pregnant women
l Pediatric ART initiation for <2 years HIV positive children
l Retention in care of HIV positive women and children < 2 years aer being initiatedon ART
Almost all districts were involved. However, only 125 sites were consistently reporting onall or any of the indicators of the specific areas mentioned above. Some experiencesencountered in implementing QI include:
l Local initiatives have demonstrated improvements on some indicators e.g. related tobetter communication between facilities and communities.
l Improvement were also seen on some of the indicators on which the sites are workingon e.g.the percentage of HIV positive pregnant women who were initiated on ARTthe same day has increased from 70 to 96%.
Background1
l e QI implementing sites were provided coaching visits through QI coaches and peerlearning meetings were also conducted.
l Lack of agreed measurable and verifiable standards hindered the objective assessmentof progress made.
l Overlap in training across the concepts of Quality Assurance, Quality Managementand Quality improvement might have led to challenges to participants grasping theconcept of QI.
l Protocol issues oen necessitated the need for repeat sensitization of stakeholdersleading to increased costs and delays in implementation.
l Low capacity of providers at service delivery point in appreciating and using local datafor decision making. is is happening in the context of perceived low morale amonghealth workers.
l Inadequate resources for coaching, support and supervision and a general lack ofaccountability at various levels of the MOHCC.
l e community lacks a culture of interrogating the quality of service rendered inrelation to their rights. Feedback on QI activities or surveys has generally not beenrelayed back to clients.
improving the quality of Maternal and Newborn Care in Zimbabwe
e MOHCC with support from Maternal and Child Health Integrated Programme(MCHIP) piloted a QI initiative in 2 districts in Manicaland Province from 2010 to 2013.is programme used the Standards Based Management and Recognition (SBM-R) qualityimprovement approach which has been successfully implemented in several othercountries. e SBM-R consists of:
l Setting performance standards based on national norms, policies, and guidelineswhich are consistent with international best practices and evidence based.
l Implementing standards through a systematic and structured approach.
l Measuring progress continuously to guide performance improvement activities.Recognizing achievement of the target performance improvement standards
Following an inclusive consultative process, standards for Maternal, Newborn and ChildHealth (MNCH) were identified and packaged into 5 clinical areas (process) and 5 areasof support systems (context) and written on a standard template. e implementation ofthe QI approach was modular in nature and followed the following steps:
1. Measuring the performance gaps using Standards set (expected level of quality) tomeasure the actual performance.
2. Analyzing the cause(s)/root cause analysis for the performance gaps, selecting priorityinterventions, implementing interventions (training, procurements, supervision,refurbishments, and others).
3. Evaluating progress through continuous self and peer assessments, and scheduledexternal assessments.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 15
Background 1
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe16
In the baseline assessment conducted in 2010-11, less than 40% of the MNH standardswere fully met at any facility. e performance was particularly poor in the clinical areas.Following implementation of SBM-R, there was a demonstrated statistically significantincrease in performance scores for MNCH Services from 2010 to 2013 with the scoreincreasing from approximately 20% to 80%. A notable reduction in early neonatal mortalitywas clearly documented during the intervention period.
ese initiatives although mostly donor funded have a common purpose of improvingquality of care. While they differ in terms of approach to implementation, the conceptsand principles are largely similar. Linking performance to minimal institutional incentivessuch as in Results Based Financing (RBF) has also shown some association withimprovement in quality of care from the community perspective for example patientsatisfaction with staff attitudes as noted in the Mid-Term Review of the RBF program.(RBFmid-term Review Report, June 2013).
is initiative is now being implemented in all districts in Manicaland province.
Results based Financing (RbF) program as pay for quality improvement initiative
RBF programme funded by World Bank has been implemented by CORDAID- Zimbabwein 18 districts since 2011. e health facilities have been receiving subsidies with a focuson MNCH indicators. e subsidies are provided according to the results obtained fromquantity verification, quality supervision checklists for hospitals and health centres andclient tracer satisfaction survey results. e quality supervision checklist has both structuraland clinical indicators and is administrated by DHEs and PHEs. e PHEs and DHEs wereprovided adequate training on the use of the quality supervision checklist.
e client tracer satisfaction surveys are conducted by CBOs on the clients identified duringthe quantify verification exercises from registers using the systematic random samplingtechnique. CBO were trained on how to effectively conduct client satisfaction surveys andwrite a report on the findings. e findings from quality supervision, quantity supervisionand client satisfaction surveys have been discussed at provincial, district, and HCcommittee level. Some provinces and districts have designed and implemented a postassessment support mechanism to address the identified gaps. In order to maintain thequality of the verification mechanism, external verification has been conducted byUniversity of Zimbabwe Community Health Department quarterly on selected healthfacilities.
Preliminary evaluation results have shown improvement on few quality process indicatorse.g. an increase of 13 and 12 % were seen on in facility delivery rate and post natal coverage,respectively and most women received full package of ANC services. Taking in to accountthe preliminary findings and the findings from the quality supervision checklists, MoHCCdecided to scale up the RBF approach to 42 additional districts in 2014 using HTF. isapproach has paved the way for the institutionalization of the pay for quality model ofimprovement.
Background1
e National QualityImprovement StrategicFramework
Rationale for a Strategy on Quality Improvement in Health Care
e Quality Improvement strategy is expected to help ensure the rational application ofdifferent quality approaches and streamline efforts through the introduction of priorities,targets and milestones. Since this strategy is introduced on the background of a multitudeof factors hindering the provision of quality services, a phased approach is suggested thattakes into account the resource constrained environment in which it will be implemented.e earlier phases of implementation will focus on the most immediate health challengesthat help build necessary foundations for quality, measurement, accountability and changeare in place to enable further success.
National Qi Strategy
e QI Strategy has ten strategic priorities to:
1. Strengthen leadership structures and mechanisms that will develop, advocate for,implement and sustain QA/QI processes in the health sector.
2. Increase patients’ participation and empowerment by promoting client awareness oftheir rights when interfacing with the health system.
3. Address and prioritise issues of access, effectiveness, efficiency and equity of healthcare.
4. Improve patient/client safety, reducing errors in health care and improving health carewaste management to reduce possible harm to staff, patients and communities.
5. Develop long-term mechanisms that attract and retain staff in the health system.
6. Strengthen supportive supervision as well as routine self-assessment of performance.
7. Develop accountability frameworks that hold providers and staff responsible for thequality of services provided.
8. Ensure efficiency in service provision through reorganisation and inte-gration ofdifferent programmes.
9. Strengthen the health information management system to adequately monitor andevaluate quality in health care and facilitate operations research on QA&QI in healthand dissemination of levels of provider achievement in quality of care.
10. Mobilise and leverage financial and non-financial resources (expertise andtechnology) from other sectors towards the resuscitation of health services thatincorporates a culture of QI.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 17
2
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe18
2.1 AIM AND GUIDING PRINCIPLES OF THE STRATEGY
Aim: To provide quality preventive, curative and rehabilitative health services which areaccessible, acceptable, effective, safe and equitable, as efficiently as possible and within thecontext of continuous improvements. e ultimate aim is to deliver the highest qualityhealthcare services to the people of Zimbabwe.
Guiding Principles1. Patient-centred care recognising and reflecting the uniqueness of the individual, their
experience of their health, illness and healthcare, and enabling them to share indecision-making about their care, to manage their own health and illness, throughsupport and access to advice and information for them, their families and carers.
2. Delivering services through empowered staff enabling people working in the healthsector to use their skills, further improving staff experience, staff engagement, andbuilding capacity, providing support and incorporating a culture of continuous QualityImprovement into routine practice.
3. Health Systems approach guided by the six building blocks for health systemsstrengthening.
4. a culture of continuous Quality improvement that recognises the centrality ofmeeting client expectations and values and delivering safe, effective health care. isculture will permeate health care organisations which will be reorganised to deliverbased on client needs and evidence-based care.
5. Reward for performance that encourages and rewards proactively, collaborativeefforts that emphasise prevention and improves positive health outcomes.
6. Standardising processes of care and ensuring adherence to these will lead to betterutilisation of resources and better patient outcomes.
7. Creating a shared learning culture that uses lessons learned to modify systems toprevent negative occurrences and enhance patient safety and which actively spreadsthese lessons in support of continuous shared learning. Sharing of data collected onquality indicators and activities in a transparent manner will promote shared learningto accelerate the uptake of best practices from QI efforts.
8. innovative ways of problem solving will require an agreed methodology for problemroot cause analysis.
9. basing approaches on evidence-based strategies/practices which whenimplemented will lead to more favourable patient outcomes.
10. Collective effort and team work where QI committees are composed of the rightbalance of stakeholders is crucial to the success of improvement efforts.
11. Results-driven processes with regular real-time measurement and analysis ofprioritised results will be critical for a strong QI approach.
ese guiding principles for quality improvement cut across all the six building blocks ofhealth systems strengthening approach which are summarised below.a. Leadership and Governance: Quality improvement increases oversight, stewardship
and accountability in governance of the health system as well as more meaningfulparticipation of citizens in healthcare.
e National Quality Improvement Strategic Framework2
b. Service delivery: QI fosters the delivery of proven high impact interventions in astandardised way leading to the closure of the gap between minimum expectedstandards and actual practice.
c. Human Resources: QI enhances the responsiveness, performance, satisfaction andretention of staff ensuring adequate numbers of appropriately skilled staff can operatein an efficient manner.
d. information: QI will increase the capacity of health institutions to collect analyse andutilise reliable and timely health information on quality of care.
e. Financing: QI helps optimize the efficient use of resources for greater impact and mayact as a stimulus for resource mobilisation.
f. Medical supplies, vaccines and technology: QI promotes a scientifically sound andcost-effective use of these commodities. e.g. adherence to guidelines on rational useof medicines.
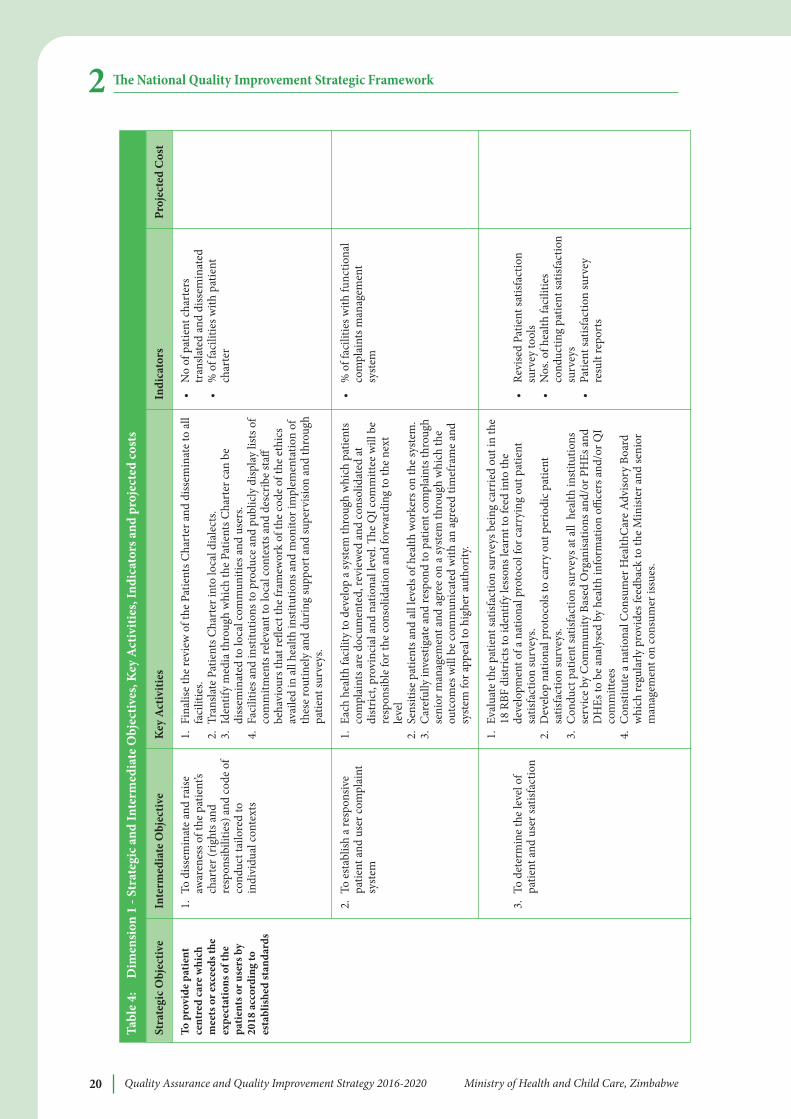
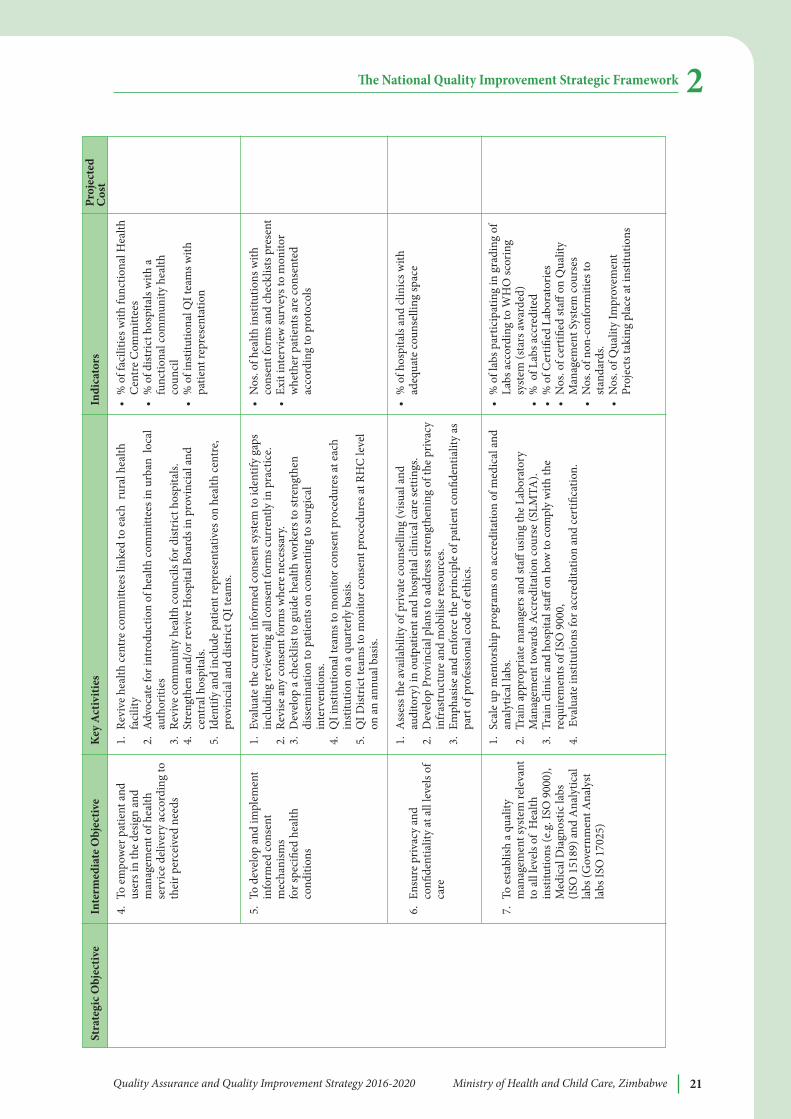
2.2 STRATEGIC OBJECTIVES, PRIORITIES ANDINTERVENTIONS
Conceptual Framework for National Qi Strategy
e strategy introduces a two-dimensional framework to support continuous improvementand sustaining of high quality care at all levels of the Zimbabwe health system and acrossall priority technical areas (e.g. MNCH, HIV/AIDS, TB, Malaria, NCDs).
e horizontal dimension defines a set of specific strategic objectives along the dimensionsof quality of care(based on national QI/QA policy strategic priorities and priority qualitydimensions) designed to achieve broad-ranging improvements in essential health systemfunctions and health services in the coming five to eight years in support of the nationalQI/QA Policy. Each strategic objective includes intermediate sub-objectives and specificactivities to achieve the intermediate objectives and overall strategic objective. Strategicobjectives and related interventions are designed to improve the capacity of the healthsystem to provide high quality services.
Strategic objectives along dimensions of care are:
l Improving patient safety.
l Providing client centred services.
l Strengthening data recording, reporting system and use of this data for decisionmaking.
l Improving clinical practices (effectiveness of care).
l Building pre-service and in-service capacity to continuously improve.
l A professional and motivated health workforce with an enforceable code of ethics.
l Improved and efficient, cost effective supply of equipment, medicines, consumablesand health related commodities.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 19
e National Quality Improvement Strategic Framework 2
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe20
e National Quality Improvement Strategic Framework2Ta
ble
4:
Dim
ensi
on 1
- St
rate
gic a
nd in
term
edia
te O
bjec
tives
, Key
act
iviti
es, i
ndic
ator
s and
pro
ject
ed co
sts
To p
rovi
de p
atie
ntce
ntre
d ca
re w
hich
mee
ts o
r exc
eeds
the
expe
ctat
ions
of t
hepa
tient
s or u
sers
by
2018
acc
ordi
ng to
esta
blis
hed
stan
dard
s
1.To
diss
emin
ate
and
raise
awar
enes
s of t
he p
atie
nt’s
char
ter (
right
s and
resp
onsib
ilitie
s) a
nd co
de o
fco
nduc
t tai
lore
d to
indi
vidu
al c
onte
xts
2.To
est
ablis
h a
resp
onsiv
epa
tient
and
use
r com
plai
ntsy
stem
3.To
det
erm
ine
the
leve
l of
patie
nt a
nd u
ser s
atisf
actio
n
•N
o of
pat
ient
char
ters
tran
slate
d an
d di
ssem
inat
ed•
% o
f fac
ilitie
s with
pat
ient
char
ter
•%
of f
acili
ties w
ith fu
nctio
nal
com
plai
nts m
anag
emen
tsy
stem
•Re
vise
d Pa
tient
satis
fact
ion
surv
ey to
ols
•N
os. o
f hea
lth fa
cilit
ies
cond
uctin
g pa
tient
satis
fact
ion
surv
eys
•Pa
tient
satis
fact
ion
surv
eyre
sult
repo
rts
1.Fi
nalis
e th
e re
view
of t
he P
atie
nts C
hart
er a
nd d
issem
inat
e to
all
faci
litie
s.2.
Tran
slate
Pat
ient
s Cha
rter
into
loca
l dia
lect
s.3.
Iden
tify
med
ia th
roug
h w
hich
the
Patie
nts C
hart
er c
an b
edi
ssem
inat
ed to
loca
l com
mun
ities
and
use
rs.
4.Fa
cilit
ies a
nd in
stitu
tions
to p
rodu
ce a
nd p
ublic
ly d
ispla
y lis
ts o
fco
mm
itmen
ts re
leva
nt to
loca
l con
text
s and
des
crib
e st
affbe
havi
ours
that
refle
ct th
e fr
amew
ork
of th
e co
de o
f the
eth
ics
avai
led
in a
ll he
alth
inst
itutio
ns a
nd m
onito
r im
plem
enta
tion
ofth
ese
rout
inel
y an
d du
ring
supp
ort a
nd su
perv
ision
and
thro
ugh
patie
nt su
rvey
s.
1.Ea
ch h
ealth
faci
lity
to d
evel
op a
syst
em th
roug
h w
hich
pat
ient
sco
mpl
aint
s are
doc
umen
ted,
revi
ewed
and
cons
olid
ated
atdi
stric
t, pr
ovin
cial
and
nat
iona
l lev
el.
e Q
I com
mitt
ee w
ill b
ere
spon
sible
for t
he co
nsol
idat
ion
and
forw
ardi
ng to
the
next
leve
l2.
Sens
itise
pat
ient
s and
all
leve
ls of
hea
lth w
orke
rs o
n th
e sy
stem
.3.
Car
eful
ly in
vest
igat
e an
d re
spon
d to
pat
ient
com
plai
nts t
hrou
ghse
nior
man
agem
ent a
nd a
gree
on
a sy
stem
thro
ugh
whi
ch th
eou
tcom
es w
ill b
e co
mm
unic
ated
with
an
agre
ed ti
mef
ram
e an
dsy
stem
for a
ppea
l to
high
er au
thor
ity.
1.Ev
alua
te th
e pa
tient
satis
fact
ion
surv
eys b
eing
car
ried
out i
n th
e18
RBF
dist
ricts
to id
entif
y le
sson
s lea
rnt t
o fe
ed in
to th
ede
velo
pmen
t of a
nat
iona
l pro
toco
l for
car
ryin
g ou
t pat
ient
satis
fact
ion
surv
eys.
2.D
evel
op n
atio
nal p
roto
cols
to c
arry
out
per
iodi
c pat
ient
satis
fact
ion
surv
eys.
3.C
ondu
ct p
atie
nt sa
tisfa
ctio
n su
rvey
s at a
ll h
ealth
inst
itutio
nsse
rvic
e by
Com
mun
ity B
ased
Org
anisa
tions
and
/or P
HEs
and
DH
Es to
be
anal
ysed
by
heal
th in
form
atio
n offi
cers
and
/or Q
Ico
mm
ittee
s4.
Con
stitu
te a
nat
iona
l Con
sum
er H
ealth
Car
e A
dviso
ry B
oard
whi
ch re
gula
rly p
rovi
des f
eedb
ack
to th
e M
inist
er a
nd se
nior
man
agem
ent o
n co
nsum
er is
sues
.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
d C
ost
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 21
e National Quality Improvement Strategic Framework 24.
To e
mpo
wer
pat
ient
and
user
s in
the
desig
n an
dm
anag
emen
t of h
ealth
serv
ice
deliv
ery
acco
rdin
g to
thei
r per
ceiv
ed n
eeds
5.To
dev
elop
and
impl
emen
tin
form
ed co
nsen
tm
echa
nism
s fo
r spe
cifie
d he
alth
cond
ition
s
6.En
sure
priv
acy
and
confi
dent
ialit
y at
all
leve
ls of
care
7.To
est
ablis
h a
qual
itym
anag
emen
t sys
tem
rele
vant
to a
ll le
vels
of H
ealth
inst
itutio
ns (e
.g. I
SO 9
000)
,M
edic
al D
iagn
ostic
labs
(ISO
151
89) a
nd A
naly
tical
labs
(Gov
ernm
ent A
naly
stla
bs IS
O 1
7025
)
•%
of f
acili
ties w
ith fu
nctio
nal H
ealth
Cen
tre
Com
mitt
ees
•%
of d
istric
t hos
pita
ls w
ith a
func
tiona
l com
mun
ity h
ealth
coun
cil
•%
of i
nstit
utio
nal Q
I tea
ms w
ithpa
tient
repr
esen
tatio
n
•N
os. o
f hea
lth in
stitu
tions
with
cons
ent f
orm
s and
chec
klist
s pre
sent
•
Exit
inte
rvie
w su
rvey
s to
mon
itor
whe
ther
pat
ient
s are
con
sent
edac
cord
ing
to p
roto
cols
•%
of h
ospi
tals
and
clin
ics w
ithad
equa
te c
ouns
ellin
g sp
ace
•%
of l
abs p
artic
ipat
ing
in g
radi
ng o
fLa
bs a
ccor
ding
to W
HO
scor
ing
syst
em (s
tars
awar
ded)
•%
of L
abs a
ccre
dite
d•
% o
f Cer
tified
Lab
orat
orie
s•
Nos
. of c
ertifi
ed st
aff o
n Q
ualit
yM
anag
emen
t Sys
tem
cou
rses
•N
os. o
f non
-con
form
ities
tost
anda
rds.
•N
os. o
f Qua
lity
Impr
ovem
ent
Proj
ects
taki
ng p
lace
at in
stitu
tions
1.Re
vive
hea
lth ce
ntre
com
mitt
ees l
inke
d to
eac
h ru
ral h
ealth
faci
lity
2.A
dvoc
ate
for i
ntro
duct
ion
of h
ealth
com
mitt
ees i
n ur
ban
loca
lau
thor
ities
3.Re
vive
com
mun
ity h
ealth
coun
cils
for d
istric
t hos
pita
ls.4.
Stre
ngth
en a
nd/o
r rev
ive
Hos
pita
l Boa
rds i
n pr
ovin
cial
and
cent
ral h
ospi
tals.
5.
Iden
tify
and
incl
ude
patie
nt re
pres
enta
tives
on
heal
th ce
ntre
,pr
ovin
cial
and
dist
rict Q
I tea
ms.
1.Ev
alua
te th
e cu
rren
t inf
orm
ed co
nsen
t sys
tem
to id
entif
y ga
psin
clud
ing
revi
ewin
g al
l con
sent
form
s cur
rent
ly in
pra
ctic
e.2.
Revi
se a
ny co
nsen
t for
ms w
here
nec
essa
ry.
3.D
evel
op a
chec
klist
to g
uide
hea
lth w
orke
rs to
stre
ngth
endi
ssem
inat
ion
to p
atie
nts o
n co
nsen
ting
to su
rgic
alin
terv
entio
ns.
4.Q
I ins
titut
iona
l tea
ms t
o m
onito
r con
sent
pro
cedu
res a
t eac
hin
stitu
tion
on a
qua
rter
ly b
asis.
5.Q
I Dist
rict t
eam
s to
mon
itor c
onse
nt p
roce
dure
s at R
HC
leve
lon
an
annu
al b
asis.
1.A
sses
s the
avai
labi
lity
of p
rivat
e co
unse
lling
(visu
al a
ndau
dito
ry) i
n ou
tpat
ient
and
hos
pita
l clin
ical
car
e se
tting
s.2.
Dev
elop
Pro
vinc
ial p
lans
to a
ddre
ss st
reng
then
ing
of th
e pr
ivac
yin
fras
truc
ture
and
mob
ilise
reso
urce
s.3.
Emph
asise
and
enf
orce
the
prin
cipl
e of
pat
ient
confi
dent
ialit
y as
part
of p
rofe
ssio
nal c
ode
of e
thic
s.
1.Sc
ale
up m
ento
rshi
p pr
ogra
ms o
n ac
cred
itatio
n of
med
ical
and
anal
ytic
al la
bs.
2.Tr
ain
appr
opria
te m
anag
ers a
nd st
aff u
sing
the
Labo
rato
ryM
anag
emen
t tow
ards
Acc
redi
tatio
n co
urse
(SLM
TA).
3.Tr
ain
clin
ic a
nd h
ospi
tal s
taff
on h
ow to
com
ply
with
the
requ
irem
ents
of I
SO 9
000,
4.
Eval
uate
inst
itutio
ns fo
r acc
redi
tatio
n an
d ce
rtifi
catio
n.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost
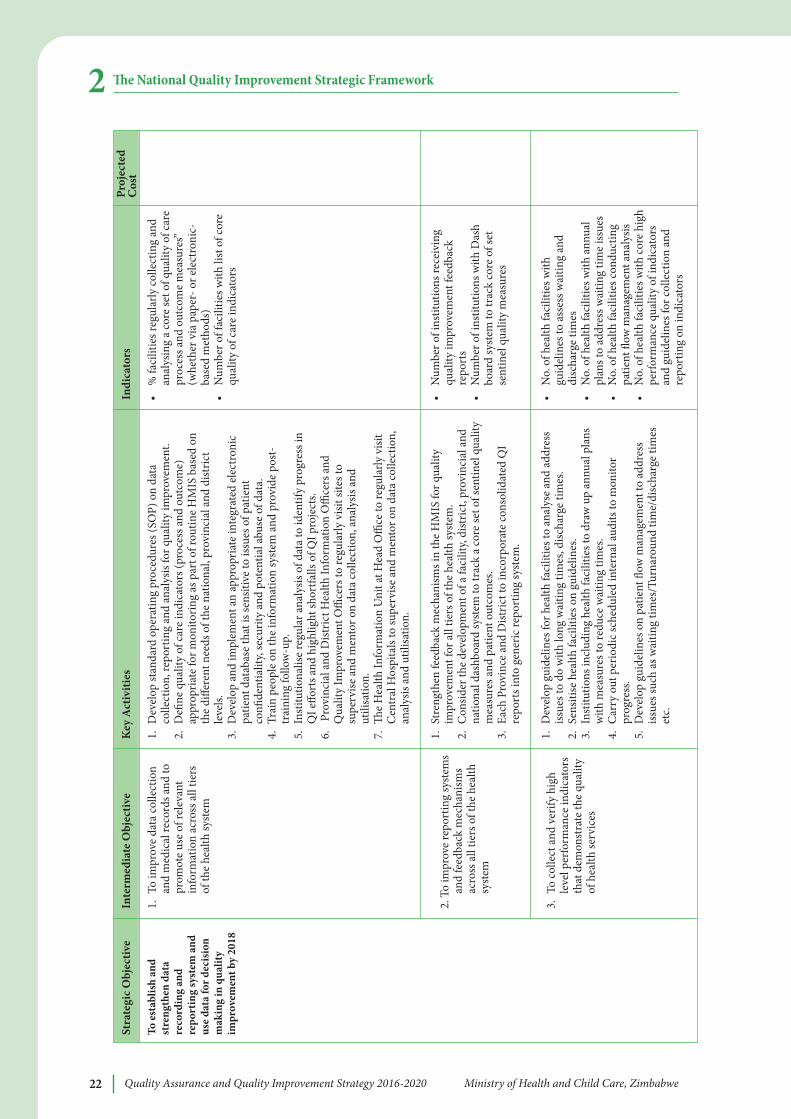
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe22
e National Quality Improvement Strategic Framework2
To e
stab
lish
and
stre
ngth
en d
ata
reco
rdin
g an
dre
port
ing
syst
em a
ndus
e da
ta fo
r dec
isio
nm
akin
g in
qua
lity
impr
ovem
ent b
y 20
18
1.To
impr
ove
data
col
lect
ion
and
med
ical
reco
rds a
nd to
prom
ote
use
of re
leva
ntin
form
atio
n ac
ross
all
tiers
of th
e he
alth
syst
em
2. T
o im
prov
e re
port
ing
syst
ems
and
feed
back
mec
hani
sms
acro
ss a
ll tie
rs o
f the
hea
lthsy
stem
3.To
colle
ct a
nd v
erify
hig
hle
vel p
erfo
rman
ce in
dica
tors
that
dem
onst
rate
the
qual
ity
of h
ealth
serv
ices
•%
faci
litie
s reg
ular
ly c
olle
ctin
g an
dan
alys
ing
a co
re se
t of q
ualit
y of
car
epr
oces
s and
out
com
e m
easu
res”
(whe
ther
via
pap
er- o
r ele
ctro
nic-
base
d m
etho
ds)
•N
umbe
r of f
acili
ties w
ith li
st o
f cor
equ
ality
of c
are
indi
cato
rs
•N
umbe
r of i
nstit
utio
ns re
ceiv
ing
qual
ity im
prov
emen
t fee
dbac
kre
port
s•
Num
ber o
f ins
titut
ions
with
Das
hbo
ard
syst
em to
trac
k co
re o
f set
sent
inel
qua
lity
mea
sure
s
•N
o. o
f hea
lth fa
cilit
ies w
ithgu
idel
ines
to a
sses
s wai
ting
and
disc
harg
e tim
es•
No.
of h
ealth
faci
litie
s with
ann
ual
plan
s to
addr
ess w
aitin
g tim
e iss
ues
•N
o. o
f hea
lth fa
cilit
ies c
ondu
ctin
gpa
tient
flow
man
agem
ent a
naly
sis•
No.
of h
ealth
faci
litie
s with
cor
e hi
ghpe
rfor
man
ce q
ualit
y of
indi
cato
rsan
d gu
idel
ines
for c
olle
ctio
n an
dre
port
ing
on in
dica
tors
1.D
evel
op st
anda
rd o
pera
ting
proc
edur
es (S
OP)
on
data
colle
ctio
n, re
port
ing
and
anal
ysis
for q
ualit
y im
prov
emen
t.2.
Defi
ne q
ualit
y of
car
e in
dica
tors
(pro
cess
and
out
com
e)ap
prop
riate
for m
onito
ring
as p
art o
f rou
tine
HM
IS b
ased
on
the
diffe
rent
nee
ds o
f the
nat
iona
l, pr
ovin
cial
and
dist
rict
leve
ls.
3.D
evel
op a
nd im
plem
ent a
n ap
prop
riate
inte
grat
ed el
ectr
onic
patie
nt d
atab
ase
that
is se
nsiti
ve to
issu
es o
f pat
ient
confi
dent
ialit
y, se
curit
y an
d po
tent
ial a
buse
of d
ata.
4.Tr
ain
peop
le o
n th
e in
form
atio
n sy
stem
and
pro
vide
pos
t-tr
aini
ng fo
llow
-up.
5.In
stitu
tiona
lise
regu
lar a
naly
sis o
f dat
a to
iden
tify
prog
ress
inQ
I effo
rts a
nd h
ighl
ight
shor
tfalls
of Q
I pro
ject
s.6.
Prov
inci
al a
nd D
istric
t Hea
lth In
form
atio
n O
ffice
rs a
ndQ
ualit
y Im
prov
emen
t Offi
cers
to re
gula
rly v
isit s
ites t
osu
perv
ise a
nd m
ento
r on
data
colle
ctio
n, a
naly
sis a
ndut
ilisa
tion.
7.
e H
ealth
Info
rmat
ion
Uni
t at H
ead
Offi
ce to
regu
larly
visi
tC
entr
al H
ospi
tals
to su
perv
ise a
nd m
ento
r on
data
colle
ctio
n,an
alys
is an
d ut
ilisa
tion.
1.St
reng
then
feed
back
mec
hani
sms i
n th
e H
MIS
for q
ualit
yim
prov
emen
t for
all
tiers
of t
he h
ealth
syst
em.
2.C
onsid
er th
e de
velo
pmen
t of a
faci
lity,
dist
rict,
prov
inci
al a
ndna
tiona
l das
hboa
rd sy
stem
to tr
ack
a co
re se
t of s
entin
el q
ualit
ym
easu
res a
nd p
atie
nt o
utco
mes
.3.
Each
Pro
vinc
e an
d D
istric
t to
inco
rpor
ate
cons
olid
ated
QI
repo
rts i
nto
gene
ric re
port
ing
syst
em.
1.D
evel
op g
uide
lines
for h
ealth
faci
litie
s to
anal
yse
and
addr
ess
issue
s to
do w
ith lo
ng w
aitin
g tim
es, d
ischa
rge
times
.2.
Sens
itise
hea
lth fa
cilit
ies o
n gu
idel
ines
.3.
Inst
itutio
ns in
clud
ing
heal
th fa
cilit
ies t
o dr
aw u
p an
nual
pla
nsw
ith m
easu
res t
o re
duce
wai
ting
times
.4.
Car
ry o
ut p
erio
dic s
ched
uled
inte
rnal
audi
ts to
mon
itor
prog
ress
.5.
Dev
elop
gui
delin
es o
n pa
tient
flow
man
agem
ent t
o ad
dres
siss
ues s
uch
as w
aitin
g tim
es/T
urna
roun
d tim
e/di
scha
rge
times
etc.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost
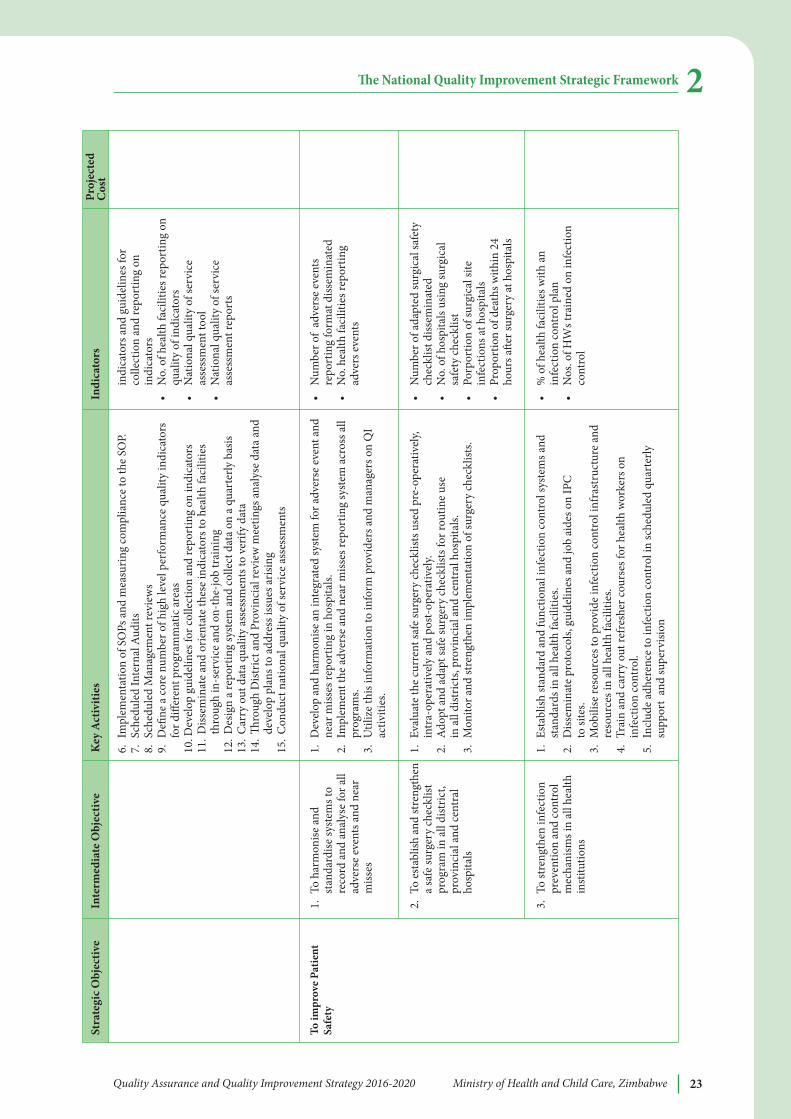
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 23
e National Quality Improvement Strategic Framework 2
To im
prov
e Pa
tient
Safe
ty1.
To h
arm
onise
and
stan
dard
ise sy
stem
s to
reco
rd a
nd a
naly
se fo
r all
adve
rse
even
ts a
nd n
ear
miss
es
2. T
o es
tabl
ish a
nd st
reng
then
a sa
fe su
rger
y ch
eckl
istpr
ogra
m in
all
dist
rict,
prov
inci
al a
nd ce
ntra
lho
spita
ls
3.To
stre
ngth
en in
fect
ion
prev
entio
n an
d co
ntro
lm
echa
nism
s in
all h
ealth
inst
itutio
ns
indi
cato
rs a
nd g
uide
lines
for
colle
ctio
n an
d re
port
ing
onin
dica
tors
•N
o. o
f hea
lth fa
cilit
ies r
epor
ting
onqu
ality
of i
ndic
ator
s•
Nat
iona
l qua
lity
of se
rvic
eas
sess
men
t too
l•
Nat
iona
l qua
lity
of se
rvic
eas
sess
men
t rep
orts
•N
umbe
r of
adve
rse
even
tsre
port
ing
form
at d
issem
inat
ed•
No.
hea
lth fa
cilit
ies r
epor
ting
adve
rs e
vent
s
•N
umbe
r of a
dapt
ed su
rgic
al sa
fety
chec
klist
diss
emin
ated
•N
o. o
f hos
pita
ls us
ing
surg
ical
safe
ty ch
eckl
ist•
Porp
ortio
n of
surg
ical
site
infe
ctio
ns at
hos
pita
ls•
Prop
ortio
n of
dea
ths w
ithin
24
hour
s ae
r sur
gery
at h
ospi
tals
•%
of h
ealth
faci
litie
s with
an
infe
ctio
n co
ntro
l pla
n•
Nos
. of H
Ws t
rain
ed o
n in
fect
ion
cont
rol
6.Im
plem
enta
tion
of S
OPs
and
mea
surin
g co
mpl
ianc
e to
the
SOP.
7.Sc
hedu
led
Inte
rnal
Aud
its8.
Sche
dule
d M
anag
emen
t rev
iew
s9.
Defi
ne a
cor
e nu
mbe
r of h
igh
leve
l per
form
ance
qua
lity
indi
cato
rsfo
r diff
eren
t pro
gram
mat
ic a
reas
10. D
evel
op g
uide
lines
for c
olle
ctio
n an
d re
port
ing
on in
dica
tors
11.D
issem
inat
e an
d or
ient
ate
thes
e in
dica
tors
to h
ealth
faci
litie
sth
roug
h in
-ser
vice
and
on-
the-
job
trai
ning
12.D
esig
n a
repo
rtin
g sy
stem
and
colle
ct d
ata
on a
qua
rter
ly b
asis
13.C
arry
out
dat
a qu
ality
ass
essm
ents
to v
erify
dat
a14
.ro
ugh
Dist
rict a
nd P
rovi
ncia
l rev
iew
mee
tings
ana
lyse
dat
a an
dde
velo
p pl
ans t
o ad
dres
s iss
ues a
risin
g15
.Con
duct
nat
iona
l qua
lity
of se
rvic
e as
sess
men
ts
1.D
evel
op a
nd h
arm
onise
an
inte
grat
ed sy
stem
for a
dver
se e
vent
and
near
miss
es re
port
ing
in h
ospi
tals.
2.Im
plem
ent t
he a
dver
se a
nd n
ear m
isses
repo
rtin
g sy
stem
acr
oss a
llpr
ogra
ms.
3.U
tiliz
e th
is in
form
atio
n to
info
rm p
rovi
ders
and
man
ager
s on
QI
activ
ities
.
1.Ev
alua
te th
e cu
rren
t saf
e su
rger
y ch
eckl
ists u
sed
pre-
oper
ativ
ely,
intr
a-op
erat
ivel
y an
d po
st-o
pera
tivel
y.2.
Ado
pt a
nd a
dapt
safe
surg
ery
chec
klist
s for
rout
ine
use
in a
ll di
stric
ts, p
rovi
ncia
l and
cent
ral h
ospi
tals.
3.M
onito
r and
stre
ngth
en im
plem
enta
tion
of su
rger
y ch
eckl
ists.
1.Es
tabl
ish st
anda
rd a
nd fu
nctio
nal i
nfec
tion
cont
rol s
yste
ms a
ndst
anda
rds i
n al
l hea
lth fa
cilit
ies.
2.D
issem
inat
e pr
otoc
ols,
guid
elin
es a
nd jo
b ai
des o
n IP
C
to si
tes.
3.M
obili
se re
sour
ces t
o pr
ovid
e in
fect
ion
cont
rol i
nfra
stru
ctur
e an
dre
sour
ces i
n al
l hea
lth fa
cilit
ies.
4.Tr
ain
and
carr
y ou
t ref
resh
er co
urse
s for
hea
lth w
orke
rs o
nin
fect
ion
cont
rol.
5.In
clud
e ad
here
nce
to in
fect
ion
cont
rol i
n sc
hedu
led
quar
terly
supp
ort
and
supe
rvisi
on
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost
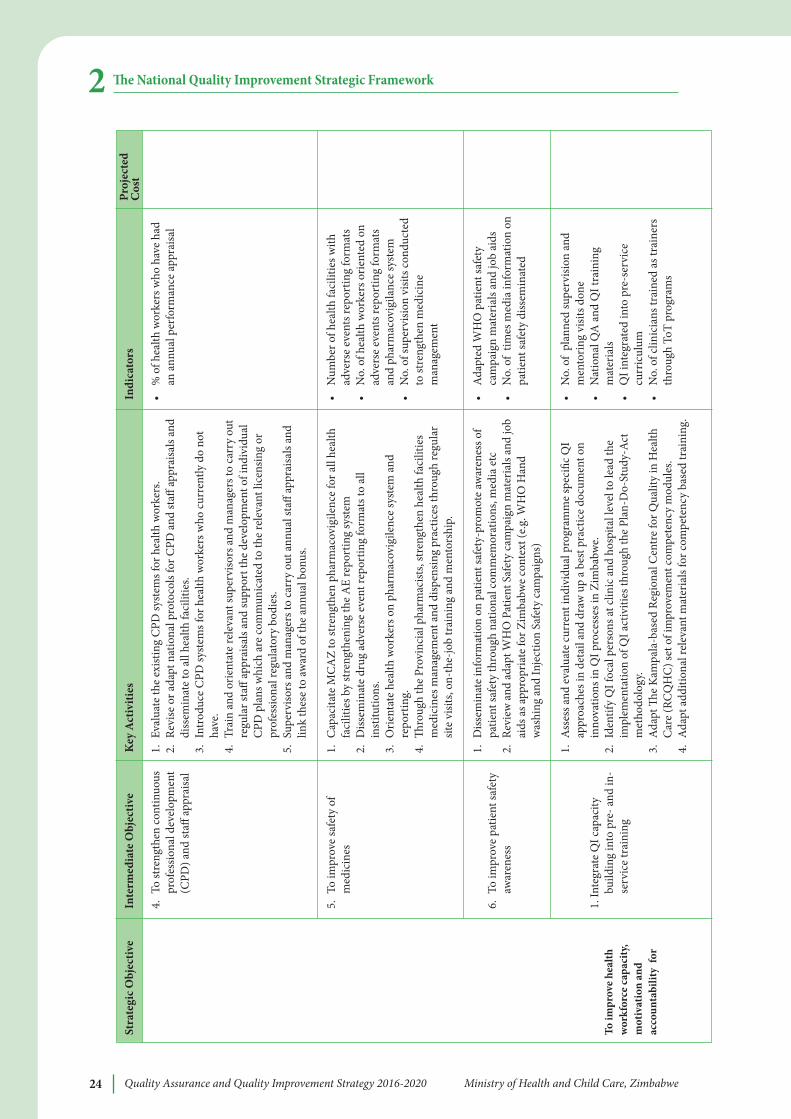
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe24
e National Quality Improvement Strategic Framework2
To im
prov
e he
alth
wor
kfor
ce c
apac
ity,
mot
ivat
ion
and
acco
unta
bilit
y fo
r
4.To
stre
ngth
en co
ntin
uous
prof
essio
nal d
evel
opm
ent
(CPD
) and
staff
appr
aisa
l
5.To
impr
ove
safe
ty o
fm
edic
ines
6.To
impr
ove
patie
nt sa
fety
awar
enes
s
1. In
tegr
ate
QI c
apac
itybu
ildin
g in
to p
re- a
nd in
-se
rvic
e tr
aini
ng
•%
of h
ealth
wor
kers
who
hav
e ha
dan
ann
ual p
erfo
rman
ce ap
prai
sal
•N
umbe
r of h
ealth
faci
litie
s with
adve
rse
even
ts re
port
ing
form
ats
•N
o. o
f hea
lth w
orke
rs o
rient
ed o
nad
vers
e ev
ents
repo
rtin
g fo
rmat
san
d ph
arm
acov
igila
nce
syst
em•
No.
of s
uper
visio
n vi
sits c
ondu
cted
to st
reng
then
med
icin
em
anag
emen
t
•A
dapt
ed W
HO
pat
ient
safe
tyca
mpa
ign
mat
eria
ls an
d jo
b ai
ds•
No.
of
times
med
ia in
form
atio
n on
patie
nt sa
fety
diss
emin
ated
•N
o. o
f pl
anne
d su
perv
ision
and
men
torin
g vi
sits d
one
•N
atio
nal Q
A a
nd Q
I tra
inin
gm
ater
ials
•Q
I int
egra
ted
into
pre
-ser
vice
curr
icul
um•
No.
of c
linic
ians
trai
ned
as tr
aine
rsth
roug
h To
T pr
ogra
ms
1.Ev
alua
te th
e ex
istin
g C
PD sy
stem
s for
hea
lth w
orke
rs.
2.Re
vise
or a
dapt
nat
iona
l pro
toco
ls fo
r CPD
and
staff
appr
aisa
ls an
ddi
ssem
inat
e to
all
heal
th fa
cilit
ies.
3.In
trod
uce
CPD
syst
ems f
or h
ealth
wor
kers
who
cur
rent
ly d
o no
tha
ve.
4.Tr
ain
and
orie
ntat
e re
leva
nt su
perv
isors
and
man
ager
s to
carr
y ou
tre
gula
r sta
ff ap
prai
sals
and
supp
ort t
he d
evel
opm
ent o
f ind
ivid
ual
CPD
pla
ns w
hich
are
com
mun
icat
ed to
the
rele
vant
lice
nsin
g or
prof
essio
nal r
egul
ator
y bo
dies
.5.
Supe
rviso
rs a
nd m
anag
ers t
o ca
rry
out a
nnua
l sta
ff ap
prai
sals
and
link
thes
e to
awar
d of
the
annu
al b
onus
.
1.C
apac
itate
MC
AZ
to st
reng
then
pha
rmac
ovig
ilenc
e fo
r all
heal
thfa
cilit
ies b
y st
reng
then
ing
the
AE
repo
rtin
g sy
stem
2.D
issem
inat
e dr
ug a
dver
se e
vent
repo
rtin
g fo
rmat
s to
all
inst
itutio
ns.
3.O
rient
ate
heal
th w
orke
rs o
n ph
arm
acov
igile
nce
syst
em a
ndre
port
ing.
4.
roug
h th
e Pr
ovin
cial
pha
rmac
ists,
stre
ngth
en h
ealth
faci
litie
sm
edic
ines
man
agem
ent a
nd d
ispen
sing
prac
tices
thro
ugh
regu
lar
site
visit
s, on
-the
-job
trai
ning
and
men
tors
hip.
1.D
issem
inat
e in
form
atio
n on
pat
ient
safe
ty-p
rom
ote
awar
enes
s of
patie
nt sa
fety
thro
ugh
natio
nal c
omm
emor
atio
ns, m
edia
etc
2.Re
view
and
ada
pt W
HO
Pat
ient
Saf
ety
cam
paig
n m
ater
ials
and
job
aids
as a
ppro
pria
te fo
r Zim
babw
e co
ntex
t (e.g
. WH
O H
and
was
hing
and
Inje
ctio
n Sa
fety
cam
paig
ns)
1.A
sses
s and
eva
luat
e cu
rren
t ind
ivid
ual p
rogr
amm
e sp
ecifi
c QI
appr
oach
es in
det
ail a
nd d
raw
up
a be
st p
ract
ice
docu
men
t on
inno
vatio
ns in
QI p
roce
sses
in Z
imba
bwe.
2.Id
entif
y Q
I foc
al p
erso
ns at
clin
ic a
nd h
ospi
tal l
evel
to le
ad th
eim
plem
enta
tion
of Q
I act
iviti
es th
roug
h th
e Pl
an-D
o-St
udy-
Act
met
hodo
logy
.3.
Ada
pt
e K
ampa
la-b
ased
Reg
iona
l Cen
tre
for Q
ualit
y in
Hea
lthC
are
(RC
QH
C) s
et o
f im
prov
emen
t com
pete
ncy
mod
ules
.4.
Ada
pt a
dditi
onal
rele
vant
mat
eria
ls fo
r com
pete
ncy
base
d tr
aini
ng.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost
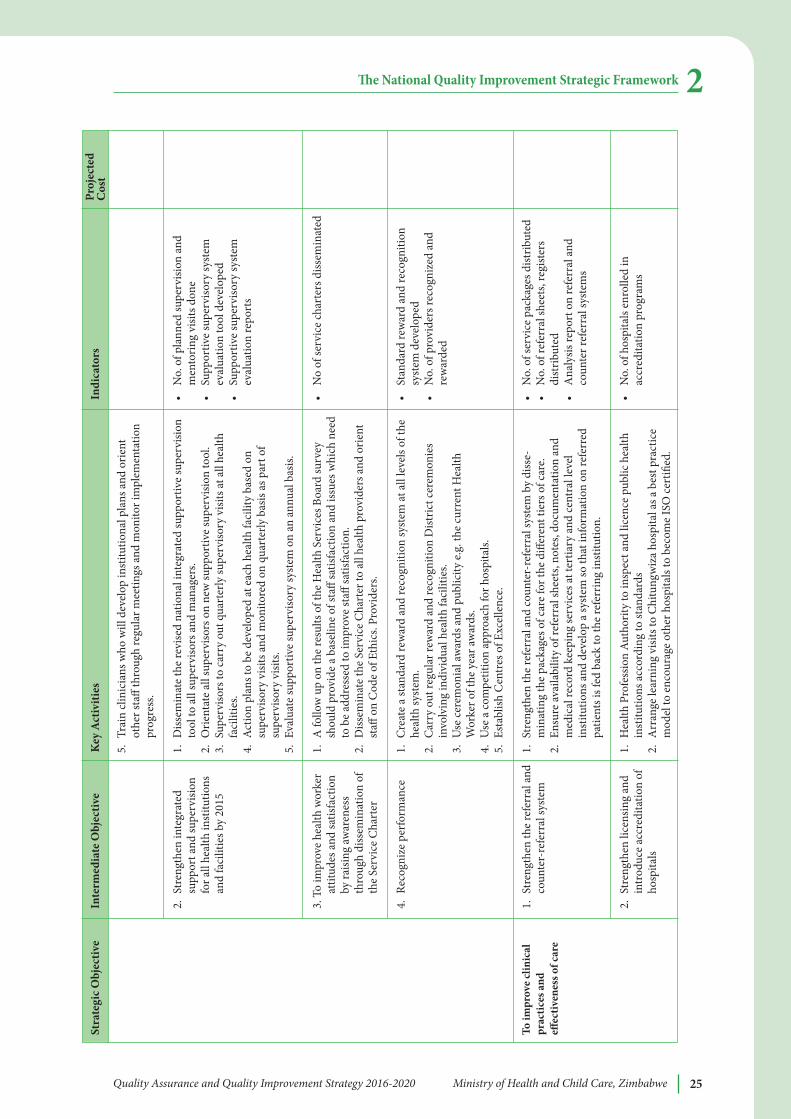
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 25
e National Quality Improvement Strategic Framework 2
To im
prov
e cl
inic
alpr
actic
es a
ndeff
ectiv
enes
s of c
are
2.St
reng
then
inte
grat
edsu
ppor
t and
supe
rvisi
onfo
r all
heal
th in
stitu
tions
and
faci
litie
s by
2015
3. T
o im
prov
e he
alth
wor
ker
attit
udes
and
satis
fact
ion
by ra
ising
awar
enes
sth
roug
h di
ssem
inat
ion
ofth
e Se
rvic
e C
hart
er
4.Re
cogn
ize
perf
orm
ance
1.St
reng
then
the
refe
rral
and
coun
ter-
refe
rral
syst
em
2.St
reng
then
lice
nsin
g an
din
trod
uce
accr
edita
tion
ofho
spita
ls
•N
o. o
f pla
nned
supe
rvisi
on a
ndm
ento
ring
visit
s don
e•
Supp
ortiv
e su
perv
isory
syst
emev
alua
tion
tool
dev
elop
ed•
Supp
ortiv
e su
perv
isory
syst
emev
alua
tion
repo
rts
•N
o of
serv
ice
char
ters
diss
emin
ated
•St
anda
rd re
war
d an
d re
cogn
ition
syst
em d
evel
oped
•N
o. o
f pro
vide
rs re
cogn
ized
and
rew
arde
d
•N
o. o
f ser
vice
pac
kage
s dist
ribut
ed•
No.
of r
efer
ral s
heet
s, re
gist
ers
dist
ribut
ed•
Ana
lysis
repo
rt o
n re
ferr
al a
ndco
unte
r ref
erra
l sys
tem
s
•N
o. o
f hos
pita
ls en
rolle
d in
accr
edita
tion
prog
ram
s
5.Tr
ain
clin
icia
ns w
ho w
ill d
evel
op in
stitu
tiona
l pla
ns a
nd o
rient
othe
r sta
ff th
roug
h re
gula
r mee
tings
and
mon
itor i
mpl
emen
tatio
npr
ogre
ss.
1.D
issem
inat
e th
e re
vise
d na
tiona
l int
egra
ted
supp
ortiv
e su
perv
ision
tool
to a
ll su
perv
isors
and
man
ager
s.2.
Orie
ntat
e al
l sup
ervi
sors
on
new
supp
ortiv
e su
perv
ision
tool
.3.
Supe
rviso
rs to
car
ry o
ut q
uart
erly
supe
rviso
ry v
isits
at a
ll he
alth
faci
litie
s.4.
Act
ion
plan
s to
be d
evel
oped
at e
ach
heal
th fa
cilit
y ba
sed
onsu
perv
isory
visi
ts a
nd m
onito
red
on q
uart
erly
bas
is as
par
t of
supe
rviso
ry v
isits
.5.
Eval
uate
supp
ortiv
e su
perv
isory
syst
em o
n an
ann
ual b
asis.
1.A
follo
w u
p on
the
resu
lts o
f the
Hea
lth S
ervi
ces B
oard
surv
eysh
ould
pro
vide
a b
asel
ine
of st
aff sa
tisfa
ctio
n an
d iss
ues w
hich
nee
dto
be
addr
esse
d to
impr
ove
staff
satis
fact
ion.
2.
Diss
emin
ate
the
Serv
ice
Cha
rter
to a
ll he
alth
pro
vide
rs a
nd o
rient
staff
on
Cod
e of
Eth
ics.
Prov
ider
s.
1.C
reat
e a
stan
dard
rew
ard
and
reco
gniti
on sy
stem
at a
ll le
vels
of th
ehe
alth
syst
em.
2.C
arry
out
regu
lar r
ewar
d an
d re
cogn
ition
Dist
rict c
erem
onie
sin
volv
ing
indi
vidu
al h
ealth
faci
litie
s. 3.
Use
cere
mon
ial a
war
ds a
nd p
ublic
ity e.
g. th
e cu
rren
t Hea
lthW
orke
r of t
he y
ear a
war
ds.
4.U
se a
com
petit
ion
appr
oach
for h
ospi
tals.
5.Es
tabl
ish C
entr
es o
f Exc
elle
nce.
1.St
reng
then
the
refe
rral
and
coun
ter-
refe
rral
syst
em b
y di
sse-
min
atin
g th
e pa
ckag
es o
f car
e fo
r the
diff
eren
t tie
rs o
f car
e.2.
Ensu
re av
aila
bilit
y of
refe
rral
shee
ts, n
otes
, doc
umen
tatio
n an
dm
edic
al re
cord
kee
ping
serv
ices
at te
rtia
ry a
nd ce
ntra
l lev
elin
stitu
tions
and
dev
elop
a sy
stem
so th
at in
form
atio
n on
refe
rred
patie
nts i
s fed
bac
k to
the
refe
rrin
g in
stitu
tion.
1.H
ealth
Pro
fess
ion
Auth
ority
to in
spec
t and
lice
nce
publ
ic h
ealth
inst
itutio
ns a
ccor
ding
to st
anda
rds
2.A
rran
ge le
arni
ng v
isits
to C
hitu
ngw
iza
hosp
ital a
s a b
est p
ract
ice
mod
el to
enc
oura
ge o
ther
hos
pita
ls to
bec
ome
ISO
cert
ified
.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost
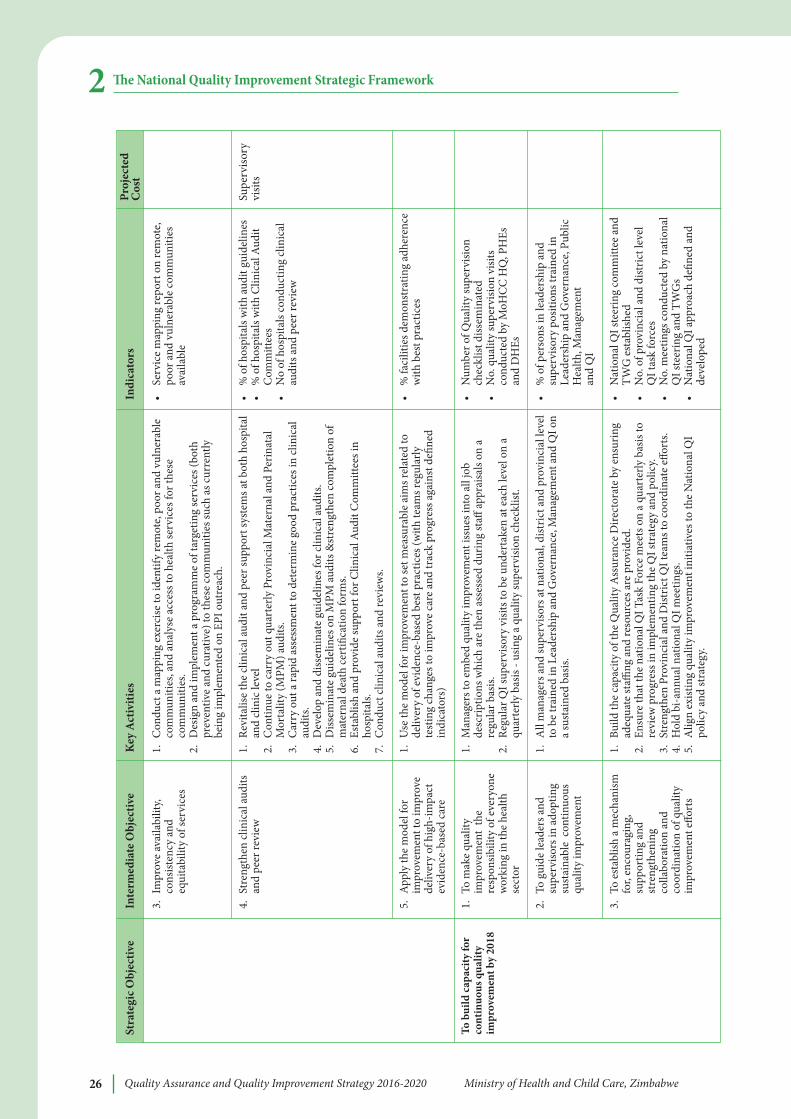
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe26
e National Quality Improvement Strategic Framework2
To b
uild
cap
acity
for
cont
inuo
us q
ualit
yim
prov
emen
t by
2018
3.Im
prov
e av
aila
bilit
y,co
nsist
ency
and
equi
tabi
lity
of se
rvic
es
4.St
reng
then
clin
ical
audi
tsan
d pe
er re
view
5.A
pply
the
mod
el fo
rim
prov
emen
t to
impr
ove
deliv
ery
of h
igh-
impa
ctev
iden
ce-b
ased
car
e
1.To
mak
e qu
ality
impr
ovem
ent
the
resp
onsib
ility
of e
very
one
wor
king
in th
e he
alth
sect
or
2.To
gui
de le
ader
s and
supe
rviso
rs in
ado
ptin
gsu
stai
nabl
e c
ontin
uous
qual
ity im
prov
emen
t
3.To
est
ablis
h a
mec
hani
smfo
r, en
cour
agin
g,su
ppor
ting
and
stre
ngth
enin
gco
llabo
ratio
n an
dco
ordi
natio
n of
qua
lity
impr
ovem
ent e
ffort
s
•Se
rvic
e m
appi
ng re
port
on
rem
ote,
poor
and
vul
nera
ble
com
mun
ities
avai
labl
e
•%
of h
ospi
tals
with
audi
t gui
delin
es•
% o
f hos
pita
ls w
ith C
linic
al A
udit
Com
mitt
ees
•N
o of
hos
pita
ls co
nduc
ting
clin
ical
audi
ts a
nd p
eer r
evie
w
•%
faci
litie
s dem
onst
ratin
g ad
here
nce
with
bes
t pra
ctic
es
•N
umbe
r of Q
ualit
y su
perv
ision
chec
klist
diss
emin
ated
•N
o. q
ualit
y su
perv
ision
visi
tsco
nduc
ted
by M
oHC
C H
Q, P
HEs
and
DH
Es
•%
of p
erso
ns in
lead
ersh
ip a
ndsu
perv
isory
pos
ition
s tra
ined
inLe
ader
ship
and
Gov
erna
nce,
Publ
icH
ealth
, Man
agem
ent
and
QI
•N
atio
nal Q
I ste
erin
g co
mm
ittee
and
TWG
est
ablis
hed
•N
o. o
f pro
vinc
ial a
nd d
istric
t lev
elQ
I tas
k fo
rces
•N
o. m
eetin
gs c
ondu
cted
by
natio
nal
QI s
teer
ing
and
TWG
s•
Nat
iona
l QI a
ppro
ach
defin
ed a
ndde
velo
ped
Supe
rviso
ryvi
sits
1.C
ondu
ct a
map
ping
exe
rcise
to id
entif
y re
mot
e, po
or a
nd v
ulne
rabl
eco
mm
uniti
es, a
nd a
naly
se a
cces
s to
heal
th se
rvic
es fo
r the
seco
mm
uniti
es.
2.D
esig
n an
d im
plem
ent a
pro
gram
me
of ta
rget
ing
serv
ices
(bot
hpr
even
tive
and
cura
tive)
to th
ese
com
mun
ities
such
as c
urre
ntly
bein
g im
plem
ente
d on
EPI
out
reac
h.
1.Re
vita
lise
the
clin
ical
audi
t and
pee
r sup
port
syst
ems a
t bot
h ho
spita
lan
d cl
inic
leve
l2.
Con
tinue
to c
arry
out
qua
rter
ly P
rovi
ncia
l Mat
erna
l and
Per
inat
alM
orta
lity
(MPM
) aud
its.
3.C
arry
out
a ra
pid
asse
ssm
ent t
o de
term
ine
good
pra
ctic
es in
clin
ical
audi
ts.
4.D
evel
op a
nd d
issem
inat
e gu
idel
ines
for c
linic
al au
dits
.5.
Diss
emin
ate
guid
elin
es o
n M
PM au
dits
&st
reng
then
com
plet
ion
ofm
ater
nal d
eath
cert
ifica
tion
form
s.6.
Esta
blish
and
pro
vide
supp
ort f
or C
linic
al A
udit
Com
mitt
ees i
nho
spita
ls.7.
Con
duct
clin
ical
audi
ts a
nd re
view
s.
1.U
se th
e m
odel
for i
mpr
ovem
ent t
o se
t mea
sura
ble
aim
s rel
ated
tode
liver
y of
evi
denc
e-ba
sed
best
pra
ctic
es (w
ith te
ams r
egul
arly
test
ing
chan
ges t
o im
prov
e ca
re a
nd tr
ack
prog
ress
aga
inst
defi
ned
indi
cato
rs)
1.M
anag
ers t
o em
bed
qual
ity im
prov
emen
t iss
ues i
nto
all j
obde
scrip
tions
whi
ch a
re th
en a
sses
sed
durin
g st
aff ap
prai
sals
on a
regu
lar b
asis.
2.Re
gula
r QI s
uper
viso
ry v
isits
to b
e un
dert
aken
at e
ach
leve
l on
aqu
arte
rly b
asis
- usin
g a
qual
ity su
perv
ision
chec
klist
.
1.A
ll m
anag
ers a
nd su
perv
isors
at n
atio
nal,
dist
rict a
nd p
rovi
ncia
l lev
elto
be
trai
ned
in L
eade
rshi
p an
d G
over
nanc
e, M
anag
emen
t and
QI o
na
sust
aine
d ba
sis.
1.Bu
ild th
e ca
paci
ty o
f the
Qua
lity
Ass
uran
ce D
irect
orat
e by
ens
urin
gad
equa
te st
affing
and
reso
urce
s are
pro
vide
d.2.
Ensu
re th
at th
e na
tiona
l QI T
ask
Forc
e m
eets
on
a qu
arte
rly b
asis
tore
view
pro
gres
s in
impl
emen
ting
the
QI s
trat
egy
and
polic
y.3.
Stre
ngth
en P
rovi
ncia
l and
Dist
rict Q
I tea
ms t
o co
ordi
nate
effo
rts.
4.H
old
bi-a
nnua
l nat
iona
l QI m
eetin
gs.
5.A
lign
exist
ing
qual
ity im
prov
emen
t ini
tiativ
es to
the
Nat
iona
l QI
polic
y an
d st
rate
gy.
Stra
tegi
c Obj
ectiv
ein
term
edia
te O
bjec
tive
Key
act
iviti
esin
dica
tors
Proj
ecte
dC
ost

Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 27
e National Quality Improvement Strategic Framework 2Vertical dimension of the national Qi strategic framework
Table 5 lays out the specific elements of the vertical dimension of the national QI strategicframework with regard to MOHCC priority health conditions. In each MOHCC priorityhealth care area, leading causes of mortality and morbidity and the associated high-impactinterventions able to reduce such mortality are summarised along with proposedimprovement activities and quality measures to assess progress toward meeting definedtargets. e following are the key priority areas as outlined in the National Strategic Plan:
l Maternal, Newborn and Child Care
l Nutrition
l Priority Communicable Diseases including HIV and AIDS, TB, Malaria, STI,Neglected Tropical Diseases
l Non-Communicable Diseases, Chronic Diseases and Mental Health
l Environmental Health
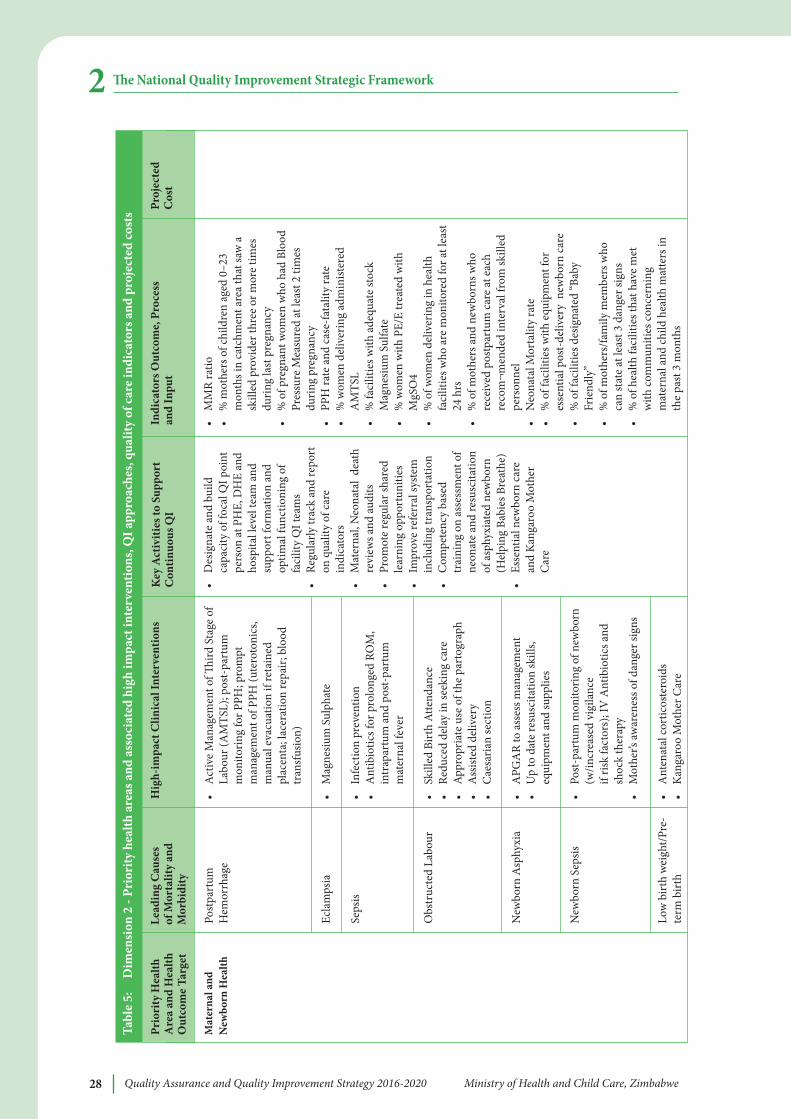
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe28
e National Quality Improvement Strategic Framework2Ta
ble
5:
Dim
ensi
on 2
- Pr
iori
ty h
ealth
are
as a
nd a
ssoc
iate
d hi
gh im
pact
inte
rven
tions
, Qi a
ppro
ache
s, qu
ality
of c
are
indi
cato
rs a
nd p
roje
cted
cost
s
Mat
erna
l and
New
born
Hea
lth
Post
part
umH
emor
rhag
e
Ecla
mps
ia
Seps
is
Obs
truc
ted
Labo
ur
New
born
Asp
hyxi
a
New
born
Sep
sis
Low
birt
h w
eigh
t/Pre
-te
rm b
irth
•D
esig
nate
and
bui
ldca
paci
ty o
f foc
al Q
I poi
ntpe
rson
at P
HE,
DH
E an
dho
spita
l lev
el te
am a
ndsu
ppor
t for
mat
ion
and
optim
al fu
nctio
ning
of
faci
lity
QI t
eam
s•
Regu
larly
trac
k an
d re
port
on q
ualit
y of
car
ein
dica
tors
•M
ater
nal,
Neo
nata
l de
ath
revi
ews a
nd au
dits
•Pr
omot
e re
gula
r sha
red
lear
ning
opp
ortu
nitie
s•
Impr
ove
refe
rral
syst
emin
clud
ing
tran
spor
tatio
n•
Com
pete
ncy
base
dtr
aini
ng o
n as
sess
men
t of
neon
ate
and
resu
scita
tion
of a
sphy
xiat
ed n
ewbo
rn(H
elpi
ng B
abie
s Bre
athe
)•
Esse
ntia
l new
born
car
ean
d K
anga
roo
Mot
her
Car
e
•M
MR
ratio
•%
mot
hers
of c
hild
ren
aged
0–2
3m
onth
s in
catc
hmen
t are
a th
at sa
w a
skill
ed p
rovi
der t
hree
or m
ore
times
durin
g la
st p
regn
ancy
•%
of p
regn
ant w
omen
who
had
Blo
odPr
essu
re M
easu
red
at le
ast 2
tim
esdu
ring
preg
nanc
y•
PPH
rate
and
cas
e-fa
talit
y ra
te•
% w
omen
del
iver
ing
adm
inist
ered
AM
TSL
•%
faci
litie
s with
ade
quat
e st
ock
Mag
nesiu
m S
ulfa
te•
% w
omen
with
PE/
E tr
eate
d w
ithM
gSO
4•
% o
f wom
en d
eliv
erin
g in
hea
lthfa
cilit
ies w
ho a
re m
onito
red
for a
t lea
st24
hrs
•%
of m
othe
rs a
nd n
ewbo
rns w
hore
ceiv
ed p
ostp
artu
m c
are
at e
ach
reco
m¬m
ende
d in
terv
al fr
om sk
illed
pers
onne
l•
Neo
nata
l Mor
talit
y ra
te•
% o
f fac
ilitie
s with
equ
ipm
ent f
ores
sent
ial p
ost-
deliv
ery
new
born
car
e•
% o
f fac
ilitie
s des
igna
ted
“Bab
yFr
iend
ly”
•%
of m
othe
rs/fa
mily
mem
bers
who
can
stat
e at
leas
t 3 d
ange
r sig
ns•
% o
f hea
lth fa
cilit
ies t
hat h
ave
met
with
com
mun
ities
con
cern
ing
mat
erna
l and
child
hea
lth m
atte
rs in
the
past
3 m
onth
s
•A
ctiv
e M
anag
emen
t of
ird S
tage
of
Labo
ur (A
MTS
L); p
ost-
part
umm
onito
ring
for P
PH; p
rom
ptm
anag
emen
t of P
PH (u
tero
toni
cs,
man
ual e
vacu
atio
n if
reta
ined
plac
enta
; lac
erat
ion
repa
ir; b
lood
tran
sfus
ion)
•M
agne
sium
Sul
phat
e
•In
fect
ion
prev
entio
n•
Ant
ibio
tics f
or p
rolo
nged
RO
M,
intr
apar
tum
and
pos
t-pa
rtum
mat
erna
l fev
er
•Sk
illed
Birt
h At
tend
ance
•Re
duce
d de
lay
in se
ekin
g ca
re•
Appr
opria
te u
se o
f the
par
togr
aph
•A
ssist
ed d
eliv
ery
•C
aesa
rian
sect
ion
•A
PGA
R to
ass
ess m
anag
emen
t •
Up
to d
ate
resu
scita
tion
skill
s,eq
uipm
ent a
nd su
pplie
s
•Po
st-p
artu
m m
onito
ring
of n
ewbo
rn(w
/incr
ease
d vi
gila
nce
if ris
k fa
ctor
s); I
V A
ntib
iotic
s and
shoc
k th
erap
y•
Mot
her’s
awar
enes
s of d
ange
r sig
ns
•A
nten
atal
cor
ticos
tero
ids
•K
anga
roo
Mot
her C
are
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
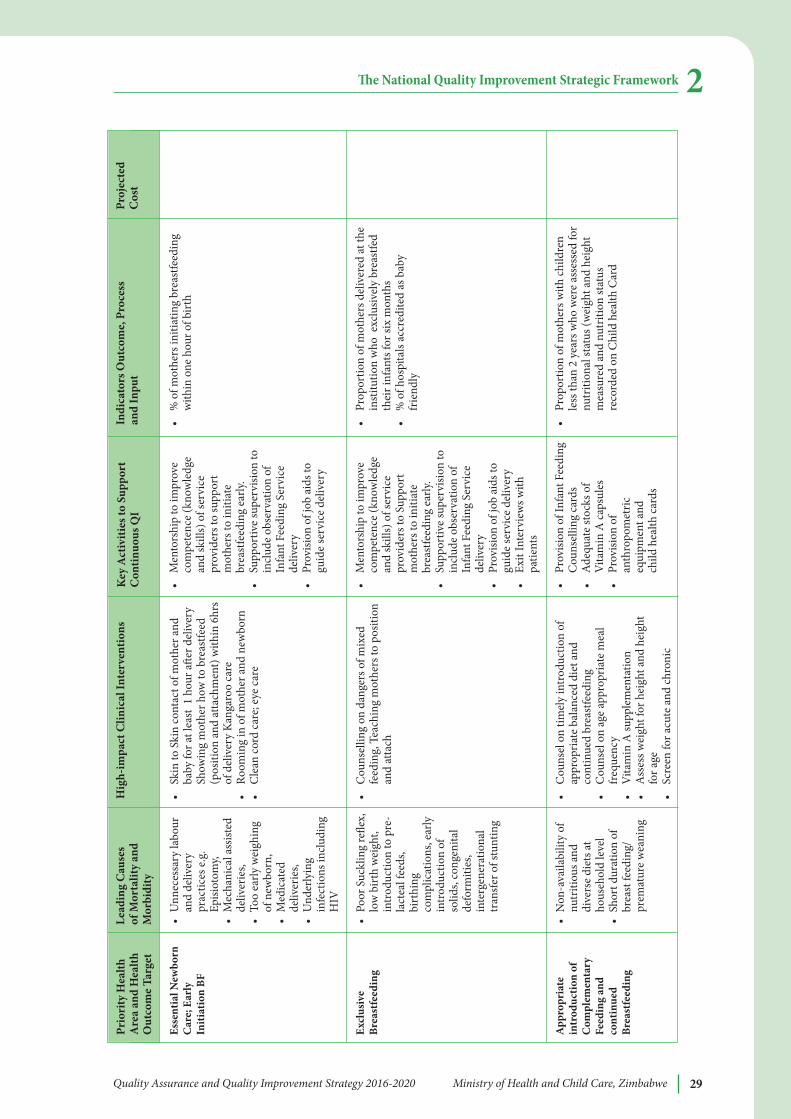
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 29
e National Quality Improvement Strategic Framework 2
esse
ntia
l New
born
Car
e; e
arly
initi
atio
n bF
excl
usiv
ebr
east
feed
ing
app
ropr
iate
intr
oduc
tion
ofC
ompl
emen
tary
Feed
ing
and
cont
inue
dbr
east
feed
ing
•U
nnec
essa
ry la
bour
and
deliv
ery
prac
tices
e.g.
Episi
otom
y, •
Mec
hani
cal a
ssist
edde
liver
ies,
•To
o ea
rly w
eigh
ing
of n
ewbo
rn,
•M
edic
ated
deliv
erie
s, •
Und
erly
ing
infe
ctio
ns in
clud
ing
HIV
•Po
or S
uckl
ing
refle
x,lo
w b
irth
wei
ght,
intr
oduc
tion
to p
re-
lact
eal f
eeds
,bi
rthi
ngco
mpl
icat
ions
, ear
lyin
trod
uctio
n of
solid
s, co
ngen
ital
defo
rmiti
es,
inte
rgen
erat
iona
ltr
ansf
er o
f stu
ntin
g
•N
on-a
vaila
bilit
y of
nutr
itiou
s and
dive
rse
diet
s at
hous
ehol
d le
vel
•Sh
ort d
urat
ion
ofbr
east
feed
ing/
prem
atur
e w
eani
ng
•M
ento
rshi
p to
impr
ove
com
pete
nce
(kno
wle
dge
and
skill
s) o
f ser
vice
prov
ider
s to
supp
ort
mot
hers
to in
itiat
ebr
east
feed
ing
early
.•
Supp
ortiv
e su
perv
ision
toin
clud
e ob
serv
atio
n of
Infa
nt F
eedi
ng S
ervi
cede
liver
y •
Prov
ision
of j
ob a
ids t
ogu
ide
serv
ice
deliv
ery
•M
ento
rshi
p to
impr
ove
com
pete
nce
(kno
wle
dge
and
skill
s) o
f ser
vice
prov
ider
s to
Supp
ort
mot
hers
to in
itiat
ebr
east
feed
ing
early
.•
Supp
ortiv
e su
perv
ision
toin
clud
e ob
serv
atio
n of
Infa
nt F
eedi
ng S
ervi
cede
liver
y
•Pr
ovisi
on o
f job
aid
s to
guid
e se
rvic
e de
liver
y•
Exit
Inte
rvie
ws w
ithpa
tient
s
•Pr
ovisi
on o
f Inf
ant F
eedi
ngC
ouns
ellin
g ca
rds
•A
dequ
ate
stoc
ks o
fV
itam
in A
cap
sule
s •
Prov
ision
of
anth
ropo
met
riceq
uipm
ent a
nd
child
hea
lth c
ards
•%
of m
othe
rs in
itiat
ing
brea
stfe
edin
gw
ithin
one
hou
r of b
irth
•Pr
opor
tion
of m
othe
rs d
eliv
ered
at th
ein
stitu
tion
who
exc
lusiv
ely
brea
stfe
dth
eir i
nfan
ts fo
r six
mon
ths
•%
of h
ospi
tals
accr
edite
d as
bab
yfr
iend
ly
•Pr
opor
tion
of m
othe
rs w
ith ch
ildre
nle
ss th
an 2
yea
rs w
ho w
ere
asse
ssed
for
nutr
ition
al st
atus
(wei
ght a
nd h
eigh
tm
easu
red
and
nutr
ition
stat
usre
cord
ed o
n C
hild
hea
lth C
ard
•Sk
in to
Ski
n co
ntac
t of m
othe
r and
baby
for a
t lea
st 1
hou
r ae
r del
iver
ySh
owin
g m
othe
r how
to b
reas
tfeed
(pos
ition
and
atta
chm
ent)
with
in 6
hrs
of d
eliv
ery
Kan
garo
o ca
re
•Ro
omin
g in
of m
othe
r and
new
born
•C
lean
cord
car
e; e
ye c
are
•C
ouns
ellin
g on
dan
gers
of m
ixed
feed
ing,
Tea
chin
g m
othe
rs to
pos
ition
and
atta
ch
•C
ouns
el o
n tim
ely
intr
oduc
tion
ofap
prop
riate
bal
ance
d di
et a
ndco
ntin
ued
brea
stfe
edin
g
•C
ouns
el o
n ag
e ap
prop
riate
mea
lfr
eque
ncy
•V
itam
in A
supp
lem
enta
tion
•
Ass
ess w
eigh
t for
hei
ght a
nd h
eigh
tfo
r age
•
Scre
en fo
r acu
te a
nd ch
roni
c
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
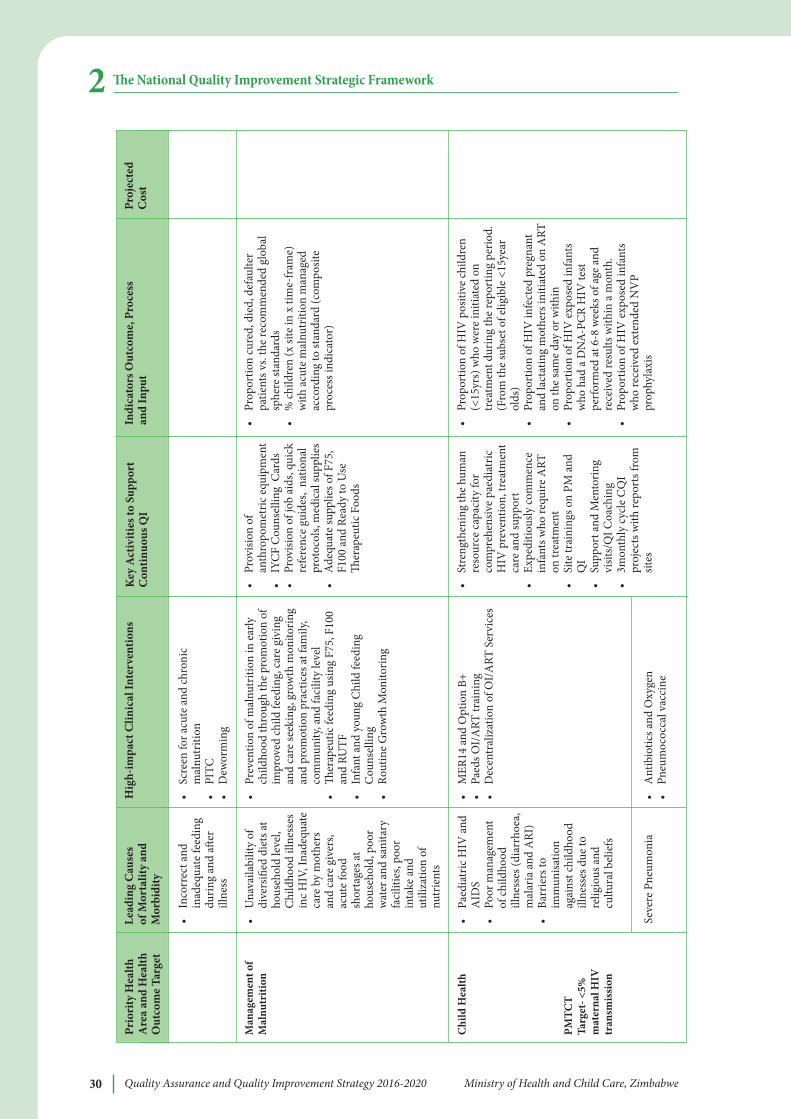
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe30
e National Quality Improvement Strategic Framework2
Man
agem
ent o
fM
alnu
triti
on
Chi
ld H
ealth
PMTC
TTa
rget
- <5%
mat
erna
l HiV
tran
smis
sion
•In
corr
ect a
ndin
adeq
uate
feed
ing
durin
g an
d a
erill
ness
•U
nava
ilabi
lity
ofdi
vers
ified
die
ts at
hous
ehol
d le
vel,
Chi
ldho
od il
lnes
ses
inc
HIV
, Ina
dequ
ate
care
by
mot
hers
and
care
giv
ers,
acut
e fo
odsh
orta
ges a
tho
useh
old,
poo
rw
ater
and
sani
tary
faci
litie
s, po
orin
take
and
utili
zatio
n of
nutr
ient
s
•Pa
edia
tric
HIV
and
AID
S•
Poor
man
agem
ent
of ch
ildho
odill
ness
es (d
iarr
hoea
,m
alar
ia a
nd A
RI)
•Ba
rrie
rs to
imm
unisa
tion
agai
nst c
hild
hood
illne
sses
due
tore
ligio
us a
ndcu
ltura
l bel
iefs
Seve
re P
neum
onia
•Pr
ovisi
on o
fan
thro
pom
etric
equ
ipm
ent
•
IYC
F C
ouns
ellin
g C
ards
•Pr
ovisi
on o
f job
aid
s, qu
ick
refe
renc
e gu
ides
, na
tiona
lpr
otoc
ols,
med
ical
supp
lies
•A
dequ
ate
supp
lies o
f F75
,F1
00 a
nd R
eady
to U
se
erap
eutic
Foo
ds
•St
reng
then
ing
the
hum
anre
sour
ce c
apac
ity fo
rco
mpr
ehen
sive
paed
iatr
icH
IV p
reve
ntio
n, tr
eatm
ent
care
and
supp
ort
•Ex
pedi
tious
ly co
mm
ence
infa
nts w
ho re
quire
ART
on tr
eatm
ent
•Si
te tr
aini
ngs o
n PM
and
QI
•Su
ppor
t and
Men
torin
gvi
sits/
QI C
oach
ing
•3m
onth
ly c
ycle
CQ
Ipr
ojec
ts w
ith re
port
s fro
msit
es
•Pr
opor
tion
cure
d, d
ied,
def
aulte
rpa
tient
s vs.
the
reco
mm
ende
d gl
obal
sphe
re st
anda
rds
•%
child
ren
(x si
te in
x ti
me-
fram
e)w
ith a
cute
mal
nutr
ition
man
aged
acco
rdin
g to
stan
dard
(com
posit
epr
oces
s ind
icat
or)
•Pr
opor
tion
of H
IV p
ositi
ve ch
ildre
n(<
15yr
s) w
ho w
ere
initi
ated
on
trea
tmen
t dur
ing
the
repo
rtin
g pe
riod.
(Fro
m th
e su
bset
of e
ligib
le <
15ye
arol
ds)
•Pr
opor
tion
of H
IV in
fect
ed p
regn
ant
and
lact
atin
g m
othe
rs in
itiat
ed o
n A
RTon
the
sam
e da
y or
with
in
•Pr
opor
tion
of H
IV e
xpos
ed in
fant
sw
ho h
ad a
DN
A-PC
R H
IV te
stpe
rfor
med
at 6
-8 w
eeks
of a
ge a
ndre
ceiv
ed re
sults
with
in a
mon
th.
•Pr
opor
tion
of H
IV e
xpos
ed in
fant
sw
ho re
ceiv
ed e
xten
ded
NV
Ppr
ophy
laxi
s
•Sc
reen
for a
cute
and
chro
nic
mal
nutr
ition
•PI
TC
•D
ewor
min
g
•Pr
even
tion
of m
alnu
triti
on in
ear
lych
ildho
od th
roug
h th
e pr
omot
ion
ofim
prov
ed ch
ild fe
edin
g, c
are
givi
ngan
d ca
re se
ekin
g, g
row
th m
onito
ring
and
prom
otio
n pr
actic
es at
fam
ily,
com
mun
ity, a
nd fa
cilit
y le
vel
•
erap
eutic
feed
ing
usin
g F7
5, F
100
and
RUTF
•In
fant
and
you
ng C
hild
feed
ing
Cou
nsel
ling
•Ro
utin
e G
row
th M
onito
ring
•M
ER14
and
Opt
ion
B+•
Paed
s OI/
ART
trai
ning
•D
ecen
tral
izat
ion
of O
I/A
RT S
ervi
ces
•A
ntib
iotic
s and
Oxy
gen
•Pn
eum
ococ
cal v
acci
ne
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
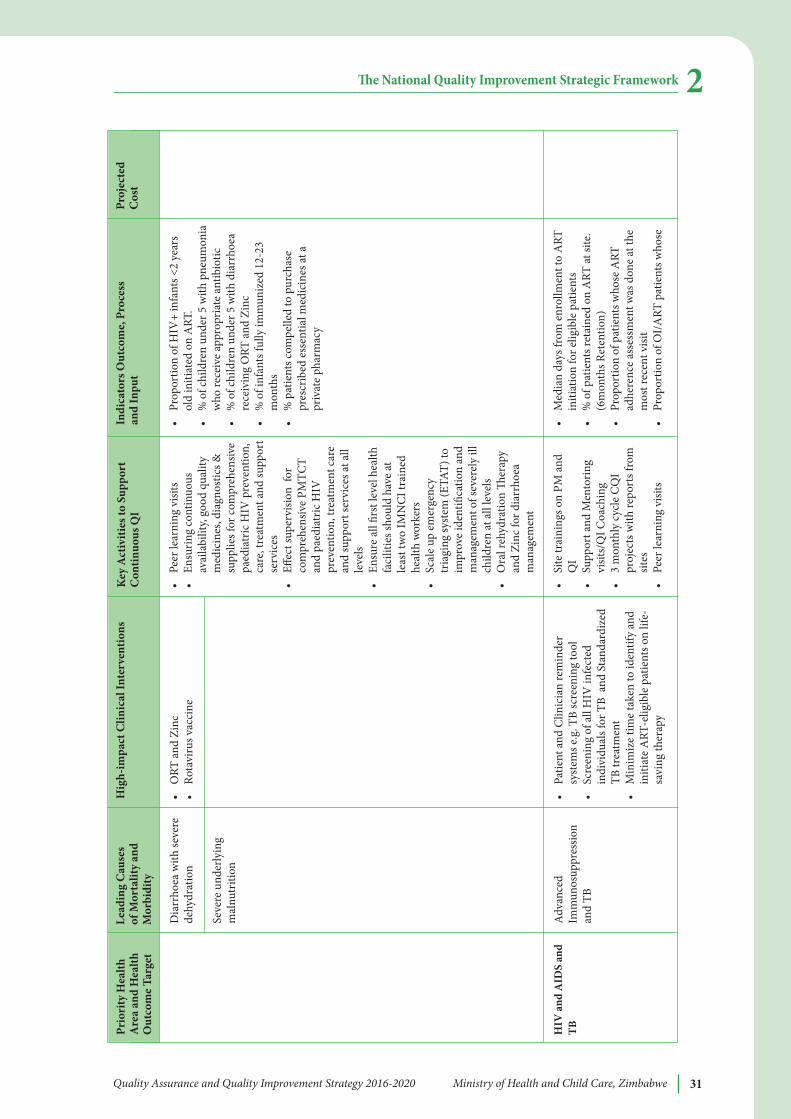
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 31
e National Quality Improvement Strategic Framework 2
HiV
and
aiD
S an
dTb
Dia
rrho
ea w
ith se
vere
dehy
drat
ion
Seve
re u
nder
lyin
gm
alnu
triti
on
Adv
ance
dIm
mun
osup
pres
sion
and
TB
•Pe
er le
arni
ng v
isits
•En
surin
g co
ntin
uous
avai
labi
lity,
good
qua
lity
med
icin
es, d
iagn
ostic
s &su
pplie
s for
com
preh
ensiv
epa
edia
tric
HIV
pre
vent
ion,
care
, tre
atm
ent a
nd su
ppor
tse
rvic
es•
Effec
t sup
ervi
sion
for
com
preh
ensiv
e PM
TCT
and
paed
iatr
ic H
IVpr
even
tion,
trea
tmen
t car
ean
d su
ppor
t ser
vice
s at a
llle
vels
•En
sure
all
first
leve
l hea
lthfa
cilit
ies s
houl
d ha
ve at
leas
t tw
o IM
NC
I tra
ined
heal
th w
orke
rs•
Scal
e up
em
erge
ncy
tria
ging
syst
em (E
TAT)
toim
prov
e id
entifi
catio
n an
dm
anag
emen
t of s
ever
ely
illch
ildre
n at
all
leve
ls•
Ora
l reh
ydra
tion
er
apy
and
Zinc
for d
iarr
hoea
man
agem
ent
•Si
te tr
aini
ngs o
n PM
and
QI
•Su
ppor
t and
Men
torin
gvi
sits/
QI C
oach
ing
•3
mon
thly
cyc
le C
QI
proj
ects
with
repo
rts f
rom
sites
•Pe
er le
arni
ng v
isits
•Pr
opor
tion
of H
IV+
infa
nts <
2 ye
ars
old
initi
ated
on
ART
.•
% o
f chi
ldre
n un
der 5
with
pne
umon
iaw
ho re
ceiv
e ap
prop
riate
ant
ibio
tic
•%
of c
hild
ren
unde
r 5 w
ith d
iarr
hoea
rece
ivin
g O
RT a
nd Z
inc
•%
of i
nfan
ts fu
lly im
mun
ized
12-
23m
onth
s•
% p
atie
nts c
ompe
lled
to p
urch
ase
pres
crib
ed e
ssen
tial m
edic
ines
at a
priv
ate
phar
mac
y
•M
edia
n da
ys fr
om e
nrol
lmen
t to
ART
initi
atio
n fo
r elig
ible
pat
ient
s•
% o
f pat
ient
s ret
aine
d on
ART
at si
te.
(6m
onth
s Ret
entio
n)•
Prop
ortio
n of
pat
ient
s who
se A
RTad
here
nce
asse
ssm
ent w
as d
one
at th
em
ost r
ecen
t visi
t•
Prop
ortio
n of
OI/
ART
pat
ient
s who
se
•O
RT a
nd Z
inc
•Ro
tavi
rus v
acci
ne
•Pa
tient
and
Clin
icia
n re
min
der
syst
ems e
.g. T
B sc
reen
ing
tool
•Sc
reen
ing
of a
ll H
IV in
fect
edin
divi
dual
s for
TB
and
Sta
ndar
dize
dTB
trea
tmen
t•
Min
imiz
e tim
e ta
ken
to id
entif
y an
din
itiat
e A
RT-e
ligib
le p
atie
nts o
n lif
e-sa
ving
ther
apy
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
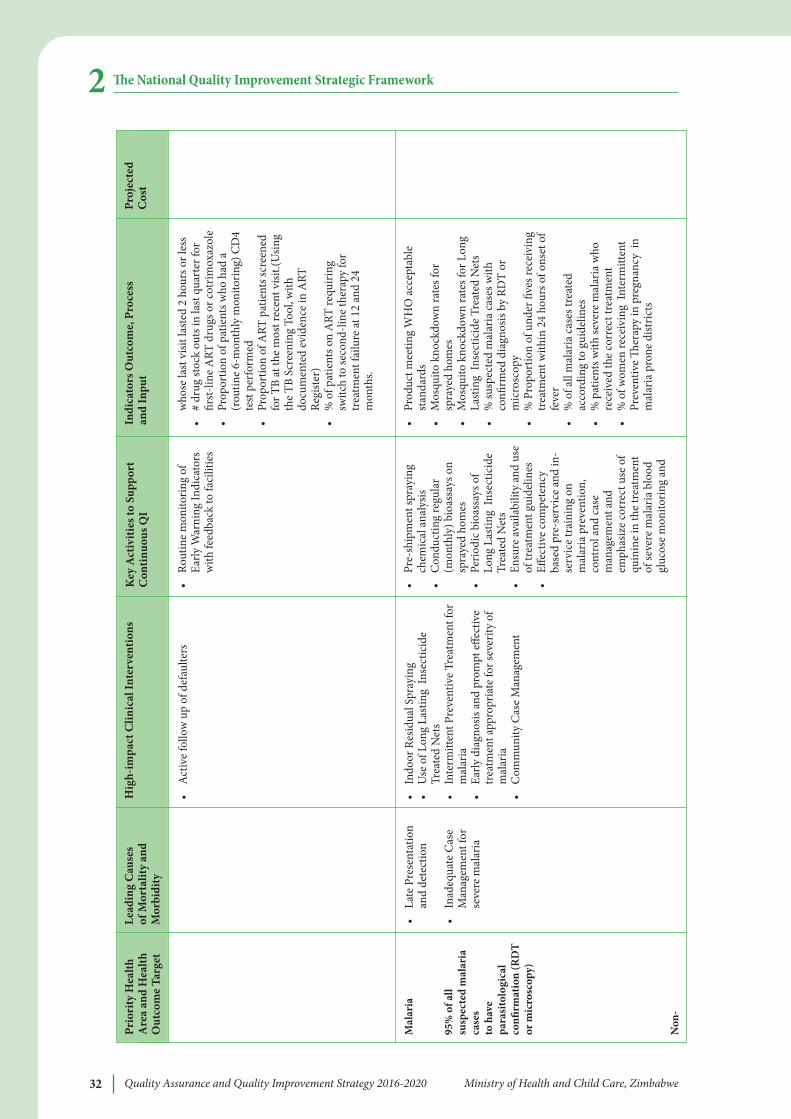
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe32
e National Quality Improvement Strategic Framework2
Mal
aria
95%
of a
llsu
spec
ted
mal
aria
case
s to
hav
epa
rasi
tolo
gica
lco
nfirm
atio
n (R
DT
or m
icro
scop
y)
Non
-
•La
te P
rese
ntat
ion
and
dete
ctio
n
•In
adeq
uate
Cas
eM
anag
emen
t for
seve
re m
alar
ia
•Ro
utin
e m
onito
ring
ofEa
rly W
arni
ng In
dica
tors
with
feed
back
to fa
cilit
ies
•Pr
e-sh
ipm
ent s
pray
ing
chem
ical
ana
lysis
•C
ondu
ctin
g re
gula
r(m
onth
ly) b
ioas
says
on
spra
yed
hom
es•
Perio
dic b
ioas
says
of
Long
Las
ting
Inse
ctic
ide
Trea
ted
Net
s•
Ensu
re av
aila
bilit
y an
d us
eof
trea
tmen
t gui
delin
es•
Effec
tive
com
pete
ncy
base
d pr
e-se
rvic
e an
d in
-se
rvic
e tr
aini
ng o
nm
alar
ia p
reve
ntio
n,co
ntro
l and
cas
em
anag
emen
t and
emph
asiz
e co
rrec
t use
of
quin
ine
in th
e tr
eatm
ent
of se
vere
mal
aria
blo
odgl
ucos
e m
onito
ring
and
who
se la
st v
isit l
aste
d 2
hour
s or l
ess
•#
drug
stoc
k ou
ts in
last
qua
rter
for
first
-line
ART
dru
gs o
r cot
rimox
azol
e•
Prop
ortio
n of
pat
ient
s who
had
a(r
outin
e 6-
mon
thly
mon
itorin
g) C
D4
test
per
form
ed•
Prop
ortio
n of
ART
pat
ient
s scr
eene
dfo
r TB
at th
e m
ost r
ecen
t visi
t.(U
sing
the
TB S
cree
ning
Too
l, w
ithdo
cum
ente
d ev
iden
ce in
ART
Regi
ster
)•
% o
f pat
ient
s on
ART
requ
iring
switc
h to
seco
nd-li
ne th
erap
y fo
rtr
eatm
ent f
ailu
re at
12
and
24m
onth
s.
•Pr
oduc
t mee
ting
WH
O a
ccep
tabl
est
anda
rds
•M
osqu
ito k
nock
dow
n ra
tes f
orsp
raye
d ho
mes
•M
osqu
ito k
nock
dow
n ra
tes f
or L
ong
Last
ing
Inse
ctic
ide
Trea
ted
Net
s•
% su
spec
ted
mal
aria
cas
es w
ithco
nfirm
ed d
iagn
osis
by R
DT
orm
icro
scop
y •
% P
ropo
rtio
n of
und
er fi
ves r
ecei
ving
trea
tmen
t with
in 2
4 ho
urs o
f ons
et o
ffe
ver
•%
of a
ll m
alar
ia c
ases
trea
ted
acco
rdin
g to
gui
delin
es•
% p
atie
nts w
ith se
vere
mal
aria
who
rece
ived
the
corr
ect t
reat
men
t•
% o
f wom
en re
ceiv
ing
Inte
rmitt
ent
Prev
entiv
e
erap
y in
pre
gnan
cy i
nm
alar
ia p
rone
dist
ricts
•A
ctiv
e fo
llow
up
of d
efau
lters
•In
door
Res
idua
l Spr
ayin
g•
Use
of L
ong
Last
ing
Inse
ctic
ide
Trea
ted
Net
s•
Inte
rmitt
ent P
reve
ntiv
e Tr
eatm
ent f
orm
alar
ia•
Early
dia
gnos
is an
d pr
ompt
effe
ctiv
etr
eatm
ent a
ppro
pria
te fo
r sev
erity
of
mal
aria
•C
omm
unity
Cas
e M
anag
emen
t
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
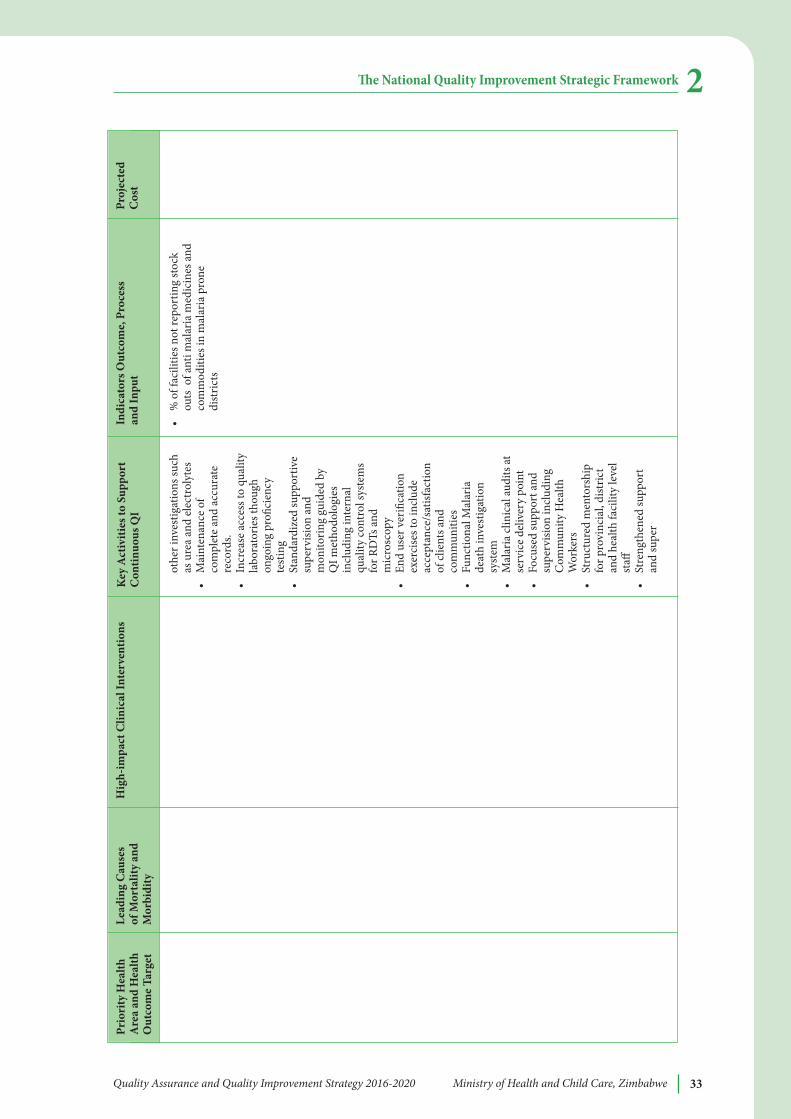
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 33
e National Quality Improvement Strategic Framework 2
othe
r inv
estig
atio
ns su
chas
ure
a an
d el
ectr
olyt
es
•M
aint
enan
ce o
fco
mpl
ete
and
accu
rate
reco
rds.
•In
crea
se a
cces
s to
qual
ityla
bora
torie
s tho
ugh
ongo
ing
profi
cien
cyte
stin
g•
Stan
dard
ized
supp
ortiv
esu
perv
ision
and
mon
itorin
g gu
ided
by
QI m
etho
dolo
gies
incl
udin
g in
tern
alqu
ality
cont
rol s
yste
ms
for R
DTs
and
mic
rosc
opy
•En
d us
er v
erifi
catio
nex
erci
ses t
o in
clud
eac
cept
ance
/sat
isfac
tion
of cl
ient
s and
com
mun
ities
•Fu
nctio
nal M
alar
iade
ath
inve
stig
atio
nsy
stem
•M
alar
ia cl
inic
al au
dits
atse
rvic
e de
liver
y po
int
•Fo
cuse
d su
ppor
t and
supe
rvisi
on in
clud
ing
Com
mun
ity H
ealth
Wor
kers
•St
ruct
ured
men
tors
hip
for p
rovi
ncia
l, di
stric
tan
d he
alth
faci
lity
leve
lst
aff•
Stre
ngth
ened
supp
ort
and
supe
r
•%
of f
acili
ties n
ot re
port
ing
stoc
kou
ts o
f ant
i mal
aria
med
icin
es a
ndco
mm
oditi
es in
mal
aria
pro
nedi
stric
ts
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
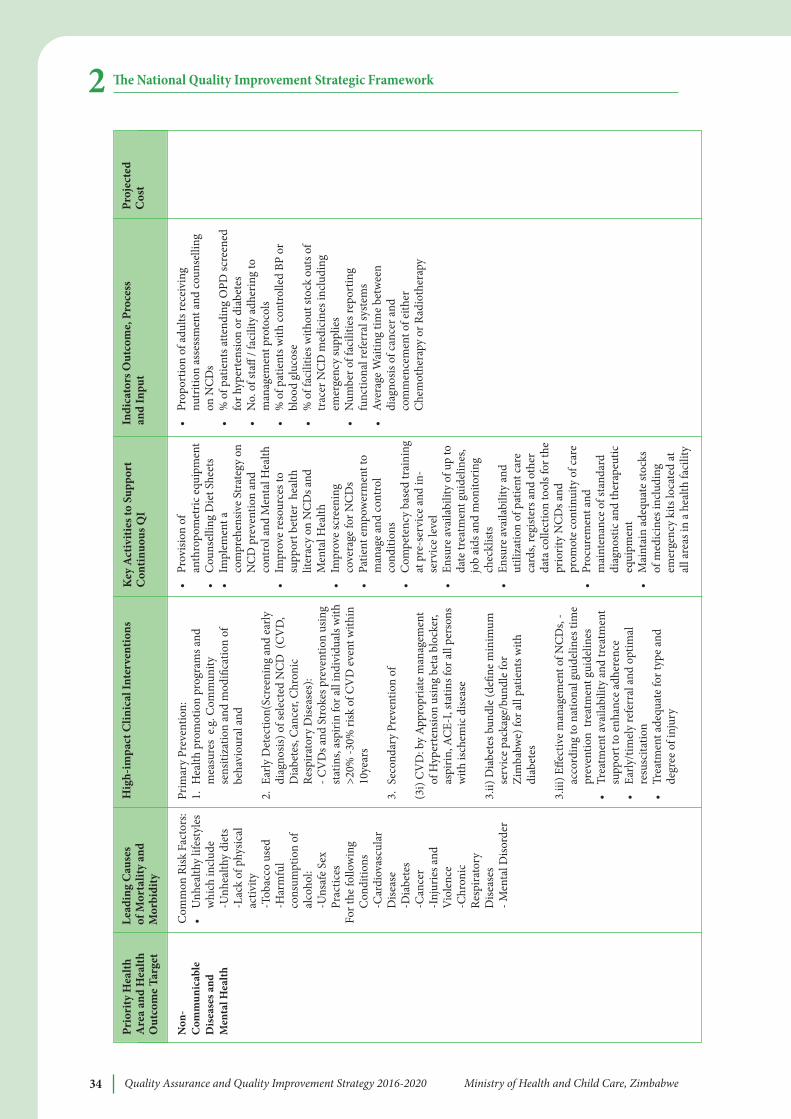
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe34
e National Quality Improvement Strategic Framework2
Non
-C
omm
unic
able
Dis
ease
s and
Men
tal H
ealth
Com
mon
Risk
Fac
tors
:•
Unh
ealth
y lif
esty
les
whi
ch in
clud
e-U
nhea
lthy
diet
s-L
ack
of p
hysic
alac
tivity
-Tob
acco
use
d-H
arm
ful
cons
umpt
ion
ofal
coho
l:
-Uns
afe
Sex
Prac
tices
For t
he fo
llow
ing
Con
ditio
ns-C
ardi
ovas
cula
rD
iseas
e-D
iabe
tes
-Can
cer
-Inj
urie
s and
Vio
lenc
e-C
hron
icRe
spira
tory
Dise
ases
- Men
tal D
isord
er
•Pr
ovisi
on o
fan
thro
pom
etric
equ
ipm
ent
•
Cou
nsel
ling
Die
t She
ets
•Im
plem
ent a
com
preh
ensiv
e St
rate
gy o
nN
CD
pre
vent
ion
and
cont
rol a
nd M
enta
l Hea
lth•
Impr
ove
reso
urce
s to
supp
ort b
ette
r he
alth
liter
acy
on N
CD
s and
Men
tal H
ealth
•Im
prov
e sc
reen
ing
cove
rage
for N
CD
s•
Patie
nt e
mpo
wer
men
t to
man
age
and
cont
rol
cond
ition
s•
Com
pete
ncy
base
d tr
aini
ngat
pre
-ser
vice
and
in-
serv
ice
leve
l•
Ensu
re av
aila
bilit
y of
up
toda
te tr
eatm
ent g
uide
lines
,jo
b ai
ds a
nd m
onito
ring
chec
klist
s•
Ensu
re av
aila
bilit
y an
dut
iliza
tion
of p
atie
nt c
are
card
s, re
gist
ers a
nd o
ther
data
colle
ctio
n to
ols f
or th
epr
iorit
y N
CD
s and
prom
ote
cont
inui
ty o
f car
e•
Proc
urem
ent a
ndm
aint
enan
ce o
f sta
ndar
ddi
agno
stic
and
ther
apeu
ticeq
uipm
ent
•M
aint
ain
adeq
uate
stoc
ksof
med
icin
es in
clud
ing
emer
genc
y ki
ts lo
cate
d at
all a
reas
in a
hea
lth fa
cilit
y
•Pr
opor
tion
of a
dults
rece
ivin
gnu
triti
on a
sses
smen
t and
cou
nsel
ling
on N
CD
s•
% o
f pat
ient
s atte
ndin
g O
PD sc
reen
edfo
r hyp
erte
nsio
n or
dia
bete
s•
No.
of s
taff
/ fac
ility
adh
erin
g to
man
agem
ent p
roto
cols
•%
of p
atie
nts w
ith c
ontr
olle
d BP
or
bloo
d gl
ucos
e•
% o
f fac
ilitie
s with
out s
tock
out
s of
trac
er N
CD
med
icin
es in
clud
ing
emer
genc
y su
pplie
s•
Num
ber o
f fac
ilitie
s rep
ortin
gfu
nctio
nal r
efer
ral s
yste
ms
•Av
erag
e W
aitin
g tim
e be
twee
ndi
agno
sis o
f can
cer a
ndco
mm
ence
men
t of e
ither
Che
mot
hera
py o
r Rad
ioth
erap
y
Prim
ary
Prev
entio
n:1.
Hea
lth p
rom
otio
n pr
ogra
ms a
ndm
easu
res
e.g. C
omm
unity
sens
itiza
tion
and
mod
ifica
tion
ofbe
havi
oura
l and
2.Ea
rly D
etec
tion(
Scre
enin
g an
d ea
rlydi
agno
sis) o
f sel
ecte
d N
CD
(C
VD
,D
iabe
tes,
Can
cer,
Chr
onic
Resp
irato
ry D
iseas
es):
- CV
Ds a
nd S
trok
es p
reve
ntio
n us
ing
stat
ins,
aspi
rin fo
r all
indi
vidu
als w
ith>2
0% -3
0% ri
sk o
f CV
D e
vent
with
in10
year
s
3.Se
cond
ary
Prev
entio
n of
(3i)
CV
D: b
y A
ppro
pria
te m
anag
emen
tof
Hyp
erte
nsio
n us
ing
beta
blo
cker
,as
pirin
, AC
E-I,
stat
ins f
or a
ll pe
rson
sw
ith is
chem
ic d
iseas
e
3.ii)
Dia
bete
s bun
dle
(defi
ne m
inim
umse
rvic
e pa
ckag
e/bu
ndle
for
Zim
babw
e) fo
r all
patie
nts w
ithdi
abet
es
3.iii
) Effe
ctiv
e m
anag
emen
t of N
CD
s, -
acco
rdin
g to
nat
iona
l gui
delin
es ti
me
prev
entio
n tr
eatm
ent g
uide
lines
•Tr
eatm
ent a
vaila
bilit
y an
d tr
eatm
ent
supp
ort t
o en
hanc
e ad
here
nce
•Ea
rly/ti
mel
y re
ferr
al a
nd o
ptim
alre
susc
itatio
n•
Trea
tmen
t ade
quat
e fo
r typ
e an
dde
gree
of i
njur
y
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
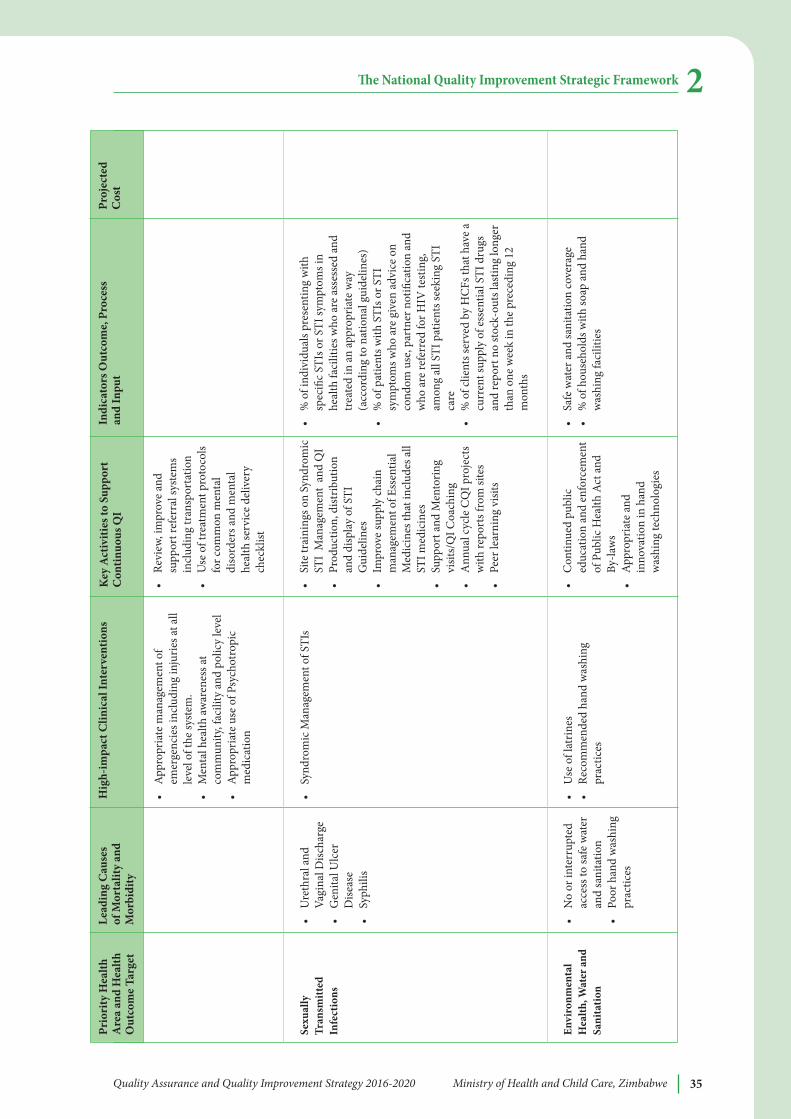
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 35
e National Quality Improvement Strategic Framework 2
Sexu
ally
Tran
smitt
edin
fect
ions
envi
ronm
enta
lH
ealth
, wat
er a
ndSa
nita
tion
•U
reth
ral a
ndVa
gina
l Disc
harg
e •
Gen
ital U
lcer
Dise
ase
•Sy
phili
s
•N
o or
inte
rrup
ted
acce
ss to
safe
wat
eran
d sa
nita
tion
•Po
or h
and
was
hing
prac
tices
•Re
view
, im
prov
e an
dsu
ppor
t ref
erra
l sys
tem
sin
clud
ing
tran
spor
tatio
n•
Use
of t
reat
men
t pro
toco
lsfo
r com
mon
men
tal
diso
rder
s and
men
tal
heal
th se
rvic
e de
liver
ych
eckl
ist
•Si
te tr
aini
ngs o
n Sy
ndro
mic
STI
Man
agem
ent
and
QI
•Pr
oduc
tion,
dist
ribut
ion
and
disp
lay
of S
TIG
uide
lines
•Im
prov
e su
pply
chai
nm
anag
emen
t of E
ssen
tial
Med
icin
es th
at in
clud
es a
llST
I med
icin
es•
Supp
ort a
nd M
ento
ring
visit
s/Q
I Coa
chin
g•
Ann
ual c
ycle
CQ
I pro
ject
sw
ith re
port
s fro
m si
tes
•Pe
er le
arni
ng v
isits
•C
ontin
ued
publ
iced
ucat
ion
and
enfo
rcem
ent
of P
ublic
Hea
lth A
ct a
ndBy
-law
s•
Appr
opria
te a
ndin
nova
tion
in h
and
was
hing
tech
nolo
gies
•%
of i
ndiv
idua
ls pr
esen
ting
with
spec
ific
STIs
or S
TI sy
mpt
oms i
nhe
alth
faci
litie
s who
are
ass
esse
d an
dtr
eate
d in
an
appr
opria
te w
ay(a
ccor
ding
to n
atio
nal g
uide
lines
)•
% o
f pat
ient
s with
STI
s or S
TIsy
mpt
oms w
ho a
re g
iven
adv
ice
onco
ndom
use
, par
tner
not
ifica
tion
and
who
are
refe
rred
for H
IV te
stin
g,am
ong
all S
TI p
atie
nts s
eeki
ng S
TIca
re•
% o
f clie
nts s
erve
d by
HC
Fs th
at h
ave
acu
rren
t sup
ply
of e
ssen
tial S
TI d
rugs
and
repo
rt n
o st
ock-
outs
last
ing
long
erth
an o
ne w
eek
in th
e pr
eced
ing
12m
onth
s
•Sa
fe w
ater
and
sani
tatio
n co
vera
ge•
% o
f hou
seho
lds w
ith so
ap a
nd h
and
was
hing
faci
litie
s
•A
ppro
pria
te m
anag
emen
t of
emer
genc
ies i
nclu
ding
inju
ries a
t all
leve
l of t
he sy
stem
.•
Men
tal h
ealth
awar
enes
s at
com
mun
ity, f
acili
ty a
nd p
olic
y le
vel
•Ap
prop
riate
use
of P
sych
otro
pic
med
icat
ion
•Sy
ndro
mic
Man
agem
ent o
f STI
s
•U
se o
f lat
rines
•Re
com
men
ded
hand
was
hing
prac
tices
Prio
rity
Hea
ltha
rea
and
Hea
lthO
utco
me
Targ
et
Lead
ing
Cau
ses
of M
orta
lity
and
Mor
bidi
ty
Key
act
iviti
es to
Sup
port
Con
tinuo
us Q
iin
dica
tors
Out
com
e, P
roce
ss
and
inpu
tPr
ojec
ted
Cos
tH
igh-
impa
ct C
linic
al in
terv
entio
ns
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe36
e National Quality Improvement Strategic Framework2It is important to note that the horizontal dimension strategic objectives provide a base forthe provision of quality healthcare services in the MOHCC priority areas listed above. Since“quality is everybody’s business”, the MOHCC QA division and all relevant technicaldivisions within the MOHCC, collaboratively worked together to define specificintermediate objectives, activities and indicators for defined QI strategic objectives. ishelped avoid duplication and ensured that current MOHCC strategies across all divisionsare optimally leveraged in support of the national QI strategy.
In order for this strategy to be implemented there is a need to create and maintain anenabling environment through:l Leadership and commitment at policy levell Advocacy and communicationl Training and Capacity buildingl Ensuring sustainabilityl Monitoring and Evaluation mechanisms
2.3 Quality Improvement Principles and Methodologies
Several principles underpin much of the improvement work implemented in high- andlow-resource settings.
Core principles of quality improvement include: l Effective teamwork (at all relevant system levels) that engages managers; providers,
staff, patients and relevant stakeholders to achieve a common quality improvementaim;
l An understanding of how systems and processes of care function within a healthsystem and the critical bottlenecks that impede reliable health care processes;
l Use of data (tailored to each system level) to continuously measure and track progresstoward an explicit improvement aim;
l An understanding and focus on patient needs; andl Taking into account the issue of sustainabilityl Regular shared learning.
ere are many QI methods in the literature that have been used in a number of settingswith varying degrees of success. e following 5 methodologies may be used inimplementing QI. ey have been selected owing to their success in other settings andtheir relative simplicity to understand and implement.1. 5S Method2. Model for Improvement – the Plan-Do-Study-Act (PDSA) model3. Clinical practice improvement (CPI) method4. Root cause analysis.5. Quality Improvement Collaborative
Annexe A provides a brief explanation of how these methodologies may be applied by QIteams for example.
Implementation of the QI Strategy
Phased ApproachIt will not be possible to implement all QI strategies and approaches at once. Hence aphased approach that recognizes the current operating environment and available resourcesis proposed. e phased approach also recognizes the importance of demonstrating quickwins in order to obtain buy in from the relevant stakeholders. Accreditation and pay forperformance, which is a value based payment system to encourage efficiency and improvedquality will occur at later phases the QI movement gains momentum.
Phase 1
l Establish QI teams at provincial, district and centrallevel
l Review and development of standards and guidelines of care where applicable.
l Strengthen licensing procedures and adherence to minimum standards by healthfacilities.
l Strengthen quality control of medicines, laboratories and radiology facilities.
l Strengthen and capacitate hospitals to adhere to infection control guidelines.
l Introduction of quality improvement work in at least one technical area in a subset ofdistricts in every province. An emphasis will be on Quality improvement training,activities and establishment of facility based quality improvement focal groups,overseeing continuous real-time monitoring of agreed quality of care measures(process measures and outcome measures). Each technical area will outline a 3-5year plan in which intermediate objectives from the Table 5 (vertical interventions)are sequentially introduced to guide focused improvement work in a selected ofdistricts.
l Introduction of QI skills and methods in pre-service training (with participation ofstudents in ongoing improvement projects to the extent possible).
l Strengthen monitoring of compliance to standards and guidelines e.g. medical audit.
l Establishment of improvement collaborative.
Phase 2
l Institutionalize formal recognition of performance and accreditation of hospitals
l Introduction of pay for performance at central and provincial hospital level
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 37
3
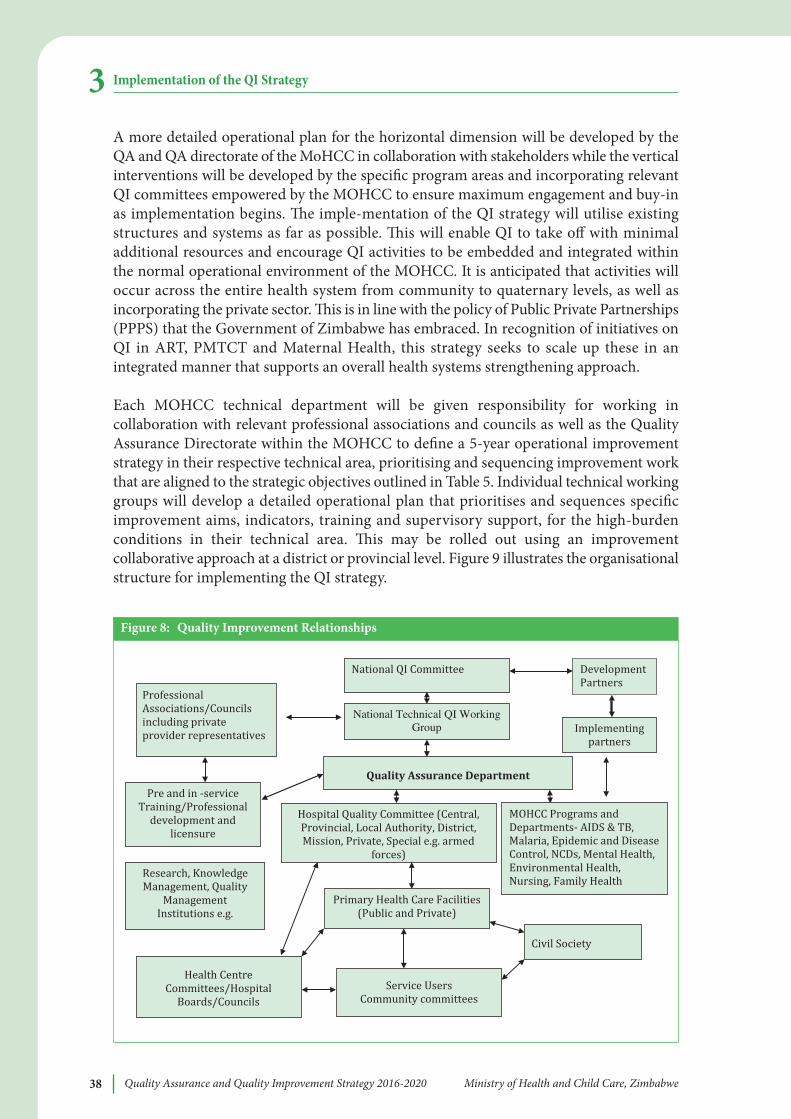
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe38
A more detailed operational plan for the horizontal dimension will be developed by theQA and QA directorate of the MoHCC in collaboration with stakeholders while the verticalinterventions will be developed by the specific program areas and incorporating relevantQI committees empowered by the MOHCC to ensure maximum engagement and buy-inas implementation begins. e imple-mentation of the QI strategy will utilise existingstructures and systems as far as possible. is will enable QI to take off with minimaladditional resources and encourage QI activities to be embedded and integrated withinthe normal operational environment of the MOHCC. It is anticipated that activities willoccur across the entire health system from community to quaternary levels, as well asincorporating the private sector. is is in line with the policy of Public Private Partnerships(PPPS) that the Government of Zimbabwe has embraced. In recognition of initiatives onQI in ART, PMTCT and Maternal Health, this strategy seeks to scale up these in anintegrated manner that supports an overall health systems strengthening approach.
Each MOHCC technical department will be given responsibility for working incollaboration with relevant professional associations and councils as well as the QualityAssurance Directorate within the MOHCC to define a 5-year operational improvementstrategy in their respective technical area, prioritising and sequencing improvement workthat are aligned to the strategic objectives outlined in Table 5. Individual technical workinggroups will develop a detailed operational plan that prioritises and sequences specificimprovement aims, indicators, training and supervisory support, for the high-burdenconditions in their technical area. is may be rolled out using an improvementcollaborative approach at a district or provincial level. Figure 9 illustrates the organisationalstructure for implementing the QI strategy.
Implementation of the QI Strategy3
Service Users Community committees
National QI Committee
Quality Assurance Department
Development Partners Professional Associations/Councils including private provider representatives Hospital Quality Committee (Central, Provincial, Local Authority, District, Mission, Private, Special e.g. armed forces)
Implementing partners
Civil Society Health Centre Committees/Hospital Boards/Councils
Primary Health Care Facilities (Public and Private)
Pre and in -service Training/Professional development and licensure Research, Knowledge Management, Quality Management Institutions e.g.
MOHCC Programs and Departments- AIDS & TB, Malaria, Epidemic and Disease Control, NCDs, Mental Health, Environmental Health, Nursing, Family Health
National Technical QI Working Group
Figure 8: Quality improvement Relationships
National Level
It is of paramount importance that a National Steering Committee with representationfrom senior management within the MOHCW as well as relevant stakeholders, overseeand guide the institutionalization of QA/QI processes to support health care servicedelivery in the country. Ideally this advisory group will be chaired by the Minister of Healthand Child Welfare or an appointed representative and will include key representatives fromother ministries such as higher education and finance, UN agencies, bilateral partners,health insurance representatives, professional associations, regulatory bodies, civil society,private sector and non-governmental organizations. e National QI Committee drivesquality improvement and ensures that QI becomes a nationwide continuous system wideapproach.
e National QI steering Committee has five main areas of responsibility:
1. Strategic Planning: prioritizing goals so that most critical areas are addressed first.
2. Overseeing Qi implementation: ensuring that all quality improvement activities aredone effectively in line with key quality priorities.
3. Providing guidance: overseeing activities to ensure that activities are on track andbeing responsive to staff, clients and partners during the improvement process.Support and encouragement to the provincial level is necessary to maintain themomentum built.
4. Resource mobilization: for building capacity for quality. e national QI committeewill be responsible for building sustainable infrastructure that fosters a culture ofquality service delivery.
5. enforcing accountability: tracking and reporting on implementation progress usinga set of agreed indicators and re-setting implementation course when necessary.
e QI committee will meet quarterly.
a National Qi Technical working Group will be established to provide technical supportto the QI committee on the five areas of responsibility outlined above. e group will meetquarterly.
Once the National Technical QI Working Group has been established, sub-groups will beformed to focus on specific goals or priorities. ese workgroups will include especiallypeople with expertise in the area of focus.
It is envisioned that there will be 7 working groups, each of which will define a detailedimplementation plan and annual targets with respect to their technical area:
1. MNCH:
2. HIV and AIDS, TB and other communicable diseases Neglected Diseases
3. NCDs and Mental health
4. Water and environment
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 39
Implementation of the QI Strategy 3
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe40
5. Information Systems
6. Commodities and supply chain, including laboratory and pharmacy
7. Client-centered care (with strong client/community representation)
Quality assurance Department
e Quality Assurance department is mandated to ensure that the quality of servicesprovided is within acceptable standards for the entire sector, both public and private healthservices. is is to be achieved through facilitating the establishment of internal qualityassurance and improvement capacity at all levels. ere is therefore need to provide human,material and financial capacity for this critical department to fulfil this mandate.
More specifically the Quality Assurance department is tasked to:
1. Provide overall operational oversight and coordination for QI.
2. Consolidate Quality Management Plans and oversee implementation.
3. Support QI teams developing and disseminating standards and guidelines on QI.
4. Establish data collection systems for performance measurement of QI
5. Provide support to the provincial level for QI through training and provision oftechnical assistance.
6. Coordinate the planning and resource mobilisation efforts for QI.
7. Work with training institutions and other MOHCC departments to develop andimplement the national QI training curriculum and materials.
8. Document quality improvement best practices and identify platforms forinformation sharing among healthcare facilities and with other interestedstakeholders.
9. Act as secretariat for the National QI Committee and lead the QI TWG.
10. To recognise the best performing Province
Other levels
Quality Improvement Committees shall be established at each hospital level. e provincialQI committee will provide overall monitoring and supporting of quality in the respectivedistricts. e Provincial QI teams would be responsible for consolidating all the initiativesfrom both hospitals and the district QI committees for then sharing to the national. edistrict QI committee will monitor and support quality at health facility level. Similarstructures will be used to monitor quality in the provision of healthcare from urbanfacilities. Central hospitals will receive oversight of QI from QAD with support from theQITWG. e roles of the QI committees’ will include:
1. Guiding implementation of QI Activities
2. Development of local QI implementation plans and budgets, integrating QI plansinto broader work plans to the extent possible (e.g. district health plan; facilityhealth plan)
Implementation of the QI Strategy3
3. Active role in capacity building and learning activities
4. Supervision, mentoring and coaching
5. Monitoring and evaluation of performance of subordinate QI teams
6. Identify best practices to be rewarded and recognized
e Provincial and District Quality focal persons will be secretariat for the QI Committees.e focal persons will be part of a management team where their central position is clearwithin the organizational structure. ey will be involved in the strategic planning processfor QI. e quality manager serves as the subject matter expert in quality. In order for theQI focal person to be proactive the QAD will put in place a programme to capacitate themwith the necessary change management, knowledge management and communicationskills. e QI focal person will also be incorporated in the planning and implementationof QI activities in specific technical areas. e QI focal person with support from the QI Committee will be responsible for checking to ensure that the quality of services meetclient expectations.
Roles and Responsibilities of Stakeholders
Government
e MOHCC will provide overall leadership and oversee planning, implementation,monitoring and evaluation of standards on QA/QI in the health sector. Other functionswill include:
l Formulate enabling legislation for QA and QI initiatives in the health sector.
l Provide technical guidelines and protocols in support for QA and QI processes.
l Provision of high quality services and maintenance of infrastructure and equipmentat all levels of care.
l Create a conductive environment for continuous learning through training andeffective mentoring.
l Identify and disseminate indicators and data collection tools on QA and QI.
l Promote operations research that informs policy implementation of QA and QIprocesses.
Private for Profit Sector (Private providers from different sectors including privatehospitals, surgeries, laboratories, pharmacies)
l Complement government efforts in the provision of accessible, affordable and qualityhealth care in line with agreed national standards and guidelines.
l Mobilize and allocate resources to QA/QI approaches in the provision of healthservices in the workplace.
l Participate in national monitoring and evaluation on QA/QI processes.
l Promote networking among private companies and developing mechanisms of peerreview on QA/QI approaches.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 41
Implementation of the QI Strategy 3

Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe42
l Involve communities in QA/QI processes in the context of social responsibilityprogrammes.
l Assist government leverage on technical expertise such as setting of qualitymanagement systems.
Development partners
l Provide technical and financial support for sustainable QA/QI initiatives.
l Advocate for increased global and national commitment to QA/QI processes in thehealth sector.
l Support operations research on QA/QI approaches.
Community Representatives, Civil Society, Non-governmental Organisations
l Advocate for the rights of the population with respect to equitable access to qualityhealth care services.
l Act as watchdogs to improve accountability to providing quality health services in thecountry.
l Forge partnerships that promote a culture that demands quality for services providedin communities.
l Implement community based strategies that promote healthy behaviours as well astimely health seeking behavior.
l Articulate community needs and influencing quality policy and the way healthservices are provided to them.
l Complement government efforts in the provision of quality health care.
Professional associations
l Self-regulation of individual and institutional standards of practice.
l Contribute to clinical guidelines development.
l Provision of professional recognition of good performance.
3.1 PERFOMANCE MEASUREMENT IN QUALITY
Measurement is a core principle underpinning all improvement and an important tool fordriving large-scale improvements in quality of care. An important role of the technicalworking groups will be to review current indicators tracked in the national HMIS systemand as part of existing QI initiatives, make recommendations about specific quality of careand outcome indicators that should be tracked by RHCs, hospitals and as part of the routineHealth Management and Information Systems to permit regular tracking and analysis ofpriority quality of care indicators and facilitate results-based action at all levels of the health
Implementation of the QI Strategy3
system. Scientifically valid and clinically relevant performance measures have the potentialto significantly improve the quality and efficiency of patient care across Zimbabwe. egoal in assessing performance is to create a system that promotes the best clinical standardsand ensures the highest quality of patient care through transparency, accountability, andcredibility. Unfortunately, the nation is in its infancy of formulating a coordinated strategyfor collecting and combining performance data, and thus, lacks an effective method forpinpointing gaps in quality and efficiency across the country. is section of the strategicplan outlines ways of bridging this gap.
Creating systems that collect and use data to improve performance is essential todemonstratingvalue and providing consistent, evidence-based care. Incorporatingmeasurement into daily practice highlights strengths and weaknesses, identifiesopportunities to improve delivery of care, and provides insight into whether changesactually lead to improvement. It is recognised that different stakeholders in a system mayneed information tailored to the specific functions for which they are responsible.Performance measures will be categorized into three basic types: structure e.g. midwife tonumber of women of child bearing age ratio, process e.g. correct use of partograph, andoutcomes e.g. still birth rate.
Quality assessment indicators
e following list of specific areas under the domains mentioned above shall guide thedevelopment of quality indicators with guidance from the Quality Assurance Department.
Structural indicators
l Accessibility to health care- geographical coverage and location, distance and time tothe health facility, continuity of services, financial etc;
l Availability of trained and competent health workers
l Availability of diagnostic equipment, medicines and supplies
l Work environment organisation
l Logistics management
l Data management, use and dissemination
Process indicators
l Availability and use of up to date standards, treatment guidelines and protocols
l Organisational management for implementing QI
l Safety to service providers and users
l Infection prevention and control practices
l Testing and documentation of changes
l Client involvement
l Staff engagement, responsiveness and attitude to work
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 43
Implementation of the QI Strategy 3
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe44
Outcome indicators
l Health outcomes (e.g. mortality, incidence of complications)
l Equitable health care to reduce outcome variations across the population divide
l Waiting time and crowding at service points
l Adverse events reporting
l Responsiveness in the institution health care system
l Community participation
l Level of initial and continuous utilization of services
l Extent to which health care is delivered in a manner which maximizes resourcesand avoids waste
l Indicators for standardization
l Indicators for sustainability
l Client and community satisfaction
Sources of Data
Both routine and periodic data collected from facilities and communities will be used tomonitor quality of service provided. e nature and detail of the data will depend on agreedperformance measures and indicators that will facilitate monitoring, evaluation, researchinto QI and evidence based decision making for specific interventions.
l Health Facility Data - data will be collected routinely using the existing data collectiontools and transmission mechanisms using an integrated approach as far as possible.
l It is recognised that in some (many) facilities, established records and registers donot capture necessary information to permit reliable calculation of quality of caremeasures. In such cases, there may be a need for modest adaptation of records andregisters to permit capture of essential data. Indeed, improving quality of facility dataand the capacity of facility staff and MOHCC staff to collect aggregate and analysequality of care data in real time will be a central objective of the national qualityimprovement strategy.
l administrative data will provide information on health infrastructure, supervision,management meetings, logistics management, human resource profiles, financialresource flows and expenditures at the different levels of the health sector.
l Vital Statistics will provide critical information on births, deaths and cause of death.
l Population based Surveys such as the Zimbabwe Demographic and Health Surveywill incorporate questions that seek to measure quality of care.
l Periodic assessments of quality of facility health care services – in general, there islimited available information about the quality of care of specific services inZimbabwe. In order to deepen understanding of critical quality of care gaps to helpprioritize improvement aims and design of improvement work and to develop a multi-
Implementation of the QI Strategy3
year operational strategy, individual technical working groups may recommend a one-time assessment of quality of care in a representative number of facilities if resourcespermit. For neglected diseases and NCDs, in particular, there is scarce high qualitydata related to quality of health care and prevalence and epidemiology of specificconditions (e.g. for heart failure). Better baseline data may be necessary to informdevelopment of the most rationale operational improvement plan for certain technicalareas.
3.2 MONITORING AND EVALUATION
e M&E framework will be streamlined to ensure that maximum value is obtained fromthe investment on data collection and compilation.
Progress towards the quality objectives will be assessed nationally by reference to QualityOutcome Measures. ese measures will be based on a combination of patient and staffreported experiences and outcomes as well as measures of patient safety and clinicaleffectiveness. Indicators may be selected in line with agreed areas for specific acceleratedimprovement for each year. A few indicators of quality should be incorporated into thebasic health information system. Examples of indicators that may be easy to report onroutinely include case fatality rates for major conditions such as pneumonia, head injuryand general hospital mortality rates, accuracy and timeliness of reporting. Otherconsiderations include comments on quality of care appearing in the press andparliamentary debates.
Priority QI initiatives will undergo evaluation to follow up on whether the intendedoutcomes are achieved. e type of evaluation to be planned for and conducted shouldreflect the nature and scope of the public investment. Evaluations will be conducted atbaseline, mid-term and at final phase. Impact evaluations will be prioritized to assess cost-effectiveness and determine whether or not the investment should be scaled up.
e QA department will work closely with respective programmes and institutions in theplanning and conduct of evaluations with a focus on using external or peer evaluators inorder to minimize the bias normally associated with self-evaluation. It is very importantthat the results of the evaluations are shared at widely as possible for example shared at theannual “MODO”, Provincial and District Health Team meetings. e MOHCC websitealso provides a wider platform for the dissemination of evaluation findings. At the highestlevel, inclusion of QI should be high on the agenda of the weekly Permanent Secretarymeetings.
Systematic Monitoring and Correction of Quality
Supervision and the checklists used to conduct systematic monitoring must include simpleelements of quality assessment based mostly on direct observation. Supervision should becarried out in a constructive, supportive and not demoralizing manner, recognizing thesensitivities and feelings of those supervised. A standardized quality supervision tool willbe developed by the Quality assurance department for all levels of care to assess the qualityof services and support them in improving the quality of service provided.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 45
Implementation of the QI Strategy 3
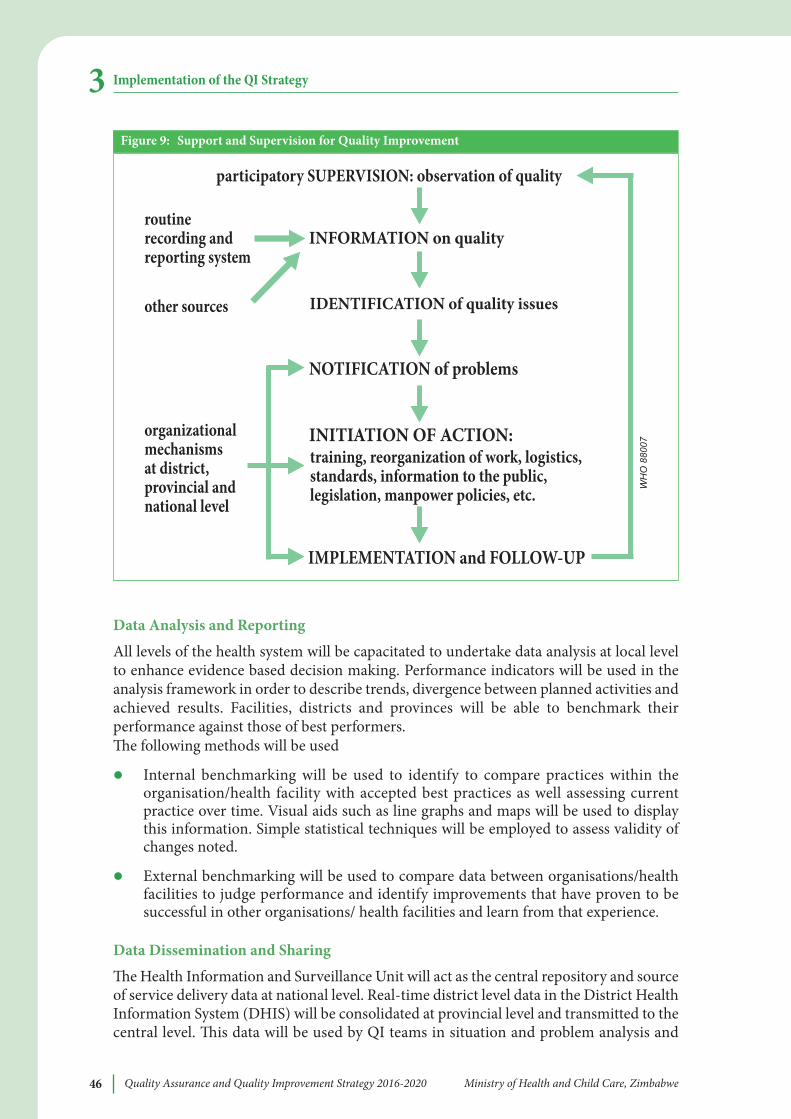
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe46
Data analysis and Reporting
All levels of the health system will be capacitated to undertake data analysis at local levelto enhance evidence based decision making. Performance indicators will be used in theanalysis framework in order to describe trends, divergence between planned activities andachieved results. Facilities, districts and provinces will be able to benchmark theirperformance against those of best performers.e following methods will be used
l Internal benchmarking will be used to identify to compare practices within theorganisation/health facility with accepted best practices as well assessing currentpractice over time. Visual aids such as line graphs and maps will be used to displaythis information. Simple statistical techniques will be employed to assess validity ofchanges noted.
l External benchmarking will be used to compare data between organisations/healthfacilities to judge performance and identify improvements that have proven to besuccessful in other organisations/ health facilities and learn from that experience.
Data Dissemination and Sharing
e Health Information and Surveillance Unit will act as the central repository and sourceof service delivery data at national level. Real-time district level data in the District HealthInformation System (DHIS) will be consolidated at provincial level and transmitted to thecentral level. is data will be used by QI teams in situation and problem analysis and
Implementation of the QI Strategy3
participatory SUPERVISION: observation of quality
INFORMATION on quality
IDENTIFICATION of quality issues
NOTIFICATION of problems
INITIATION OF ACTION:
IMPLEMENTATION and FOLLOW-UP
routinerecording andreporting system
other sources
organizationalmechanismsat district,provincial andnational level
training, reorganization of work, logistics,standards, information to the public,legislation, manpower policies, etc. W
HO
880
07
Figure 9: Support and Supervision for Quality improvement
planning QI activities. Other data from patient surveys for example will be collated byprovince and shared on the MOHCC website.
Data will need to be interpreted in the context of the internal and external operatingenvironment. Service delivery data shall be packaged and displayed at the various healthfacilities using the HMIS format to be provided for standardization purposes. e timingof information dissemination should fit in the planning cycles and needs of the users.Information will be available through platforms such as the Health Matters Magazine, theMOHCC website, press releases and through electronic and print media.
Client Satisfaction Surveys
Service providers, regulatory bodies such as the Health Professions Authority andprofessional associations will on a regular basis conduct client surveys to determine thequality of services from the service user’s perspective. Standardised tools will be developedby the Quality Assurance department for the different levels of care.
accreditation, Recognition and Reward
e following strategic approaches to regulation and accreditation of facilities will be used:
l Align regulatory focus with health sector priorities.
l Build on self-regulatory mechanisms for compliance.
l Reduce the costs of regulation via rational sampling, focused accreditation, and tieredinspection.
l Assess/accredit management and internal QA processes and structures.
l Minimize internal costs of response to inspection.
Role of Research in Quality Improvement
e Ministry of Health and Child Care (QAD) in partnership with Academic Institutionsand other relevant partners will dra a research agenda that tackles problems in deliveringquality of care. Formation of a task force to coordinate and support research is suggested.Potential institutional homes for such a task force include College of Health Sciences,National Institute of Health Research, Medicines Control Authority of Zimbabwe,Standards Association of Zimbabwe and others. is research will use proven scientificmethods leading to new or revised interventions as well informing policy relating to accessand delivery of health care. One deliberate strategy would be to steer more healthprofessionals in training institutions towards research focused at quality improvement atboth programmatic and service delivery point. e task force mentioned earlier will alsotake the lead in the formulating core sets of standardized performance measures whichwill guide researchers in evaluating quality in healthcare.
In some areas e.g. NCDs that have historically received fewer resources or attention, atargeted quality of care assessment must be prioritized. is assessment could be very usefulto help inform prioritization and sequencing of improvement aims based on leading qualityof gaps identified along the continuum of care.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 47
Implementation of the QI Strategy 3
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe48
Applied health services research should be expanded and should emphasize thedevelopment of knowledge, tools, and strategies that can support quality enhancement atdifferent levels of the health sector. To ensure better understanding and use of researchfindings a number of platforms will be used to present these. ese include district andprovincial team meetings, various research symposia such as the Annual Research Dayhosted by the College of Health Sciences, National Malaria Conference, Student Seminars,National AIDS conference as well the MOHCC website.
Communication and Knowledge Management
Communication is a key component of the Quality Improvement Strategy, not just in termsof raising awareness about goals and objectives, but as a major driver to motivate andinspire everyone across Zimbabwe to take appropriate action to make their contributionto achieving the shared vision for high quality healthcare services. e key aims ofcommunication are:
l To raise awareness both internally and externally of the Government of Zimbabwe’svision for the MOHCC to ensure the delivery of high quality healthcare services atboth public and private institutions.
l Inspire staff and the public to appreciate and understand the role they play indelivering the Quality Improvement Strategy’s vision.
l Highlight national and local programmes and services which are helping deliverquality healthcare
e following approaches will be used to achieve these communication aims:
l Position and frame the Quality Improvement Strategy’s purpose and vision in throughpress releases and the electronic media. is will provide more meaning andunderstanding to the general public of Zimbabwe.
l Use all available approaches (events, publications, campaigns and media) to engagewith all stakeholders throughout Zimbabwe at a national and local level informingthem of the vision for quality improvement and their role in the achievement of thisgoal.
l Motivate, inspire, equip and support the people working in the health and relatedsectors with information about what they can do to help the MOHCC and its partnersbecome a world leader in delivering quality healthcare.
Promoting regular shared learning for rapid uptake and dissemination of emerging bestpractices will be a high priority for the QI improvement strategy. e provincial quarterlyreview meetings are an ideal platform to implement this. e Principal Director, Policy,Planning, Monitoring and Evaluation though the Quality Assurance Department (QAD)will arrange platforms that allow and promote regular shared learning acrossprovinces/districts working on similar technical areas. e MOHCC – QAD incollaboration with research institutions, programme managers will oversee theimplementation of national level research activities, communication and knowledgemanagement. Provincial and City Medical Directors will be responsible for follow-up ofinstitutional and district based activities.
Implementation of the QI Strategy3
ANNEXESANNEX A:QUALITY IMPROVEMENT METHODOLOGIES
5-S Method5S is a management tool which originated in the Japanese manufacturing sector. It is usedas a basic, fundamental, systematic approach for productivity, quality, and safetyimprovement in all types of organisations. Although 5S originated in the manufacturingenvironment, it translates well to other work situations including hospitals, general offices,telecommunication companies, etc. e 5S are abbreviations of the Japanese words Seiri,Seiton, Seiso, Seiketsu, and Shitsuke. In English, the 5S are translated as Sort, Set, Shine,Standardise, and Sustain.
5-S seeks to create a neat, clean and orderly work environment that allows for the provisionof effective, efficient, acceptable and safe health care. It is the initial step andfoundation/gateway towards establishing Continuous quality Improvement (CQI or Kaizenin Japanese)-Total Quality Management (TQM) programs.
1. SORT (S1)Focuses on eliminating unnecessary items from the workplace. is is achievedthrough categorization of the different items in the working place into three categoriesi.e. necessary, not necessary and may be necessary. is exercise will also help toaddress the ‘’just in case’’ attitude.
2. SeT (S2)Organizing everything needed in proper order for easy operation matching the workflow. It should be done based on finding efficient and effective storage of necessaryitem and can be applied using “Can see, Can take out, and can return” philosophy.is will save time and energy spent to look for required items..
3. SHiNe (S3)Cleaning up one’s workplace daily so that there is no dust on floors, machines orequipment, etc. to maintain a high standard of cleanness. It creates ownership andbuild pride in the workers.
4. STaNDaRDiSe (S4)Maintaining an environment where S1 to S3 are implemented in the same mannerthroughout the organization. It gives opportunities to employees to take active partin the development of these standards. It can be achieved by developing and usingstandard operating procedures, work instructions, checklists and symbols among others.
5. SUSTaiN (S5) Maintaining S1-S4 through discipline, commitment and empowerment. It focuses ondefining a new mind set and a standard in workplace. It can be facilitated throughregular progress reporting; refresher training; periodic evaluation of the 5S program;appreciation; recognition; awarding and putting a reminder system using 5S cornerand newsletter.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 49
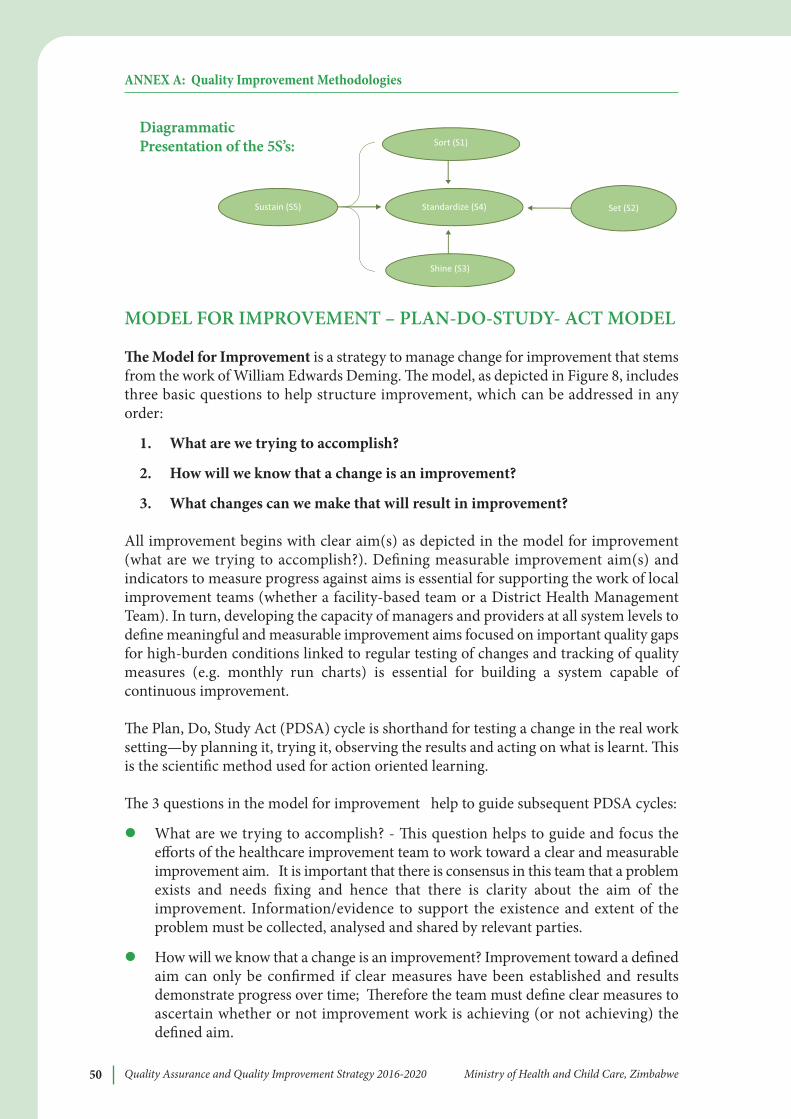
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe50
MODEL FOR IMPROVEMENT – PLAN-DO-STUDY- ACT MODEL
e Model for improvement is a strategy to manage change for improvement that stemsfrom the work of William Edwards Deming. e model, as depicted in Figure 8, includesthree basic questions to help structure improvement, which can be addressed in anyorder:
1. what are we trying to accomplish?
2. How will we know that a change is an improvement?
3. what changes can we make that will result in improvement?
All improvement begins with clear aim(s) as depicted in the model for improvement(what are we trying to accomplish?). Defining measurable improvement aim(s) andindicators to measure progress against aims is essential for supporting the work of localimprovement teams (whether a facility-based team or a District Health ManagementTeam). In turn, developing the capacity of managers and providers at all system levels todefine meaningful and measurable improvement aims focused on important quality gapsfor high-burden conditions linked to regular testing of changes and tracking of qualitymeasures (e.g. monthly run charts) is essential for building a system capable ofcontinuous improvement.
e Plan, Do, Study Act (PDSA) cycle is shorthand for testing a change in the real worksetting—by planning it, trying it, observing the results and acting on what is learnt. isis the scientific method used for action oriented learning.
e 3 questions in the model for improvement help to guide subsequent PDSA cycles:
l What are we trying to accomplish? - is question helps to guide and focus theefforts of the healthcare improvement team to work toward a clear and measurableimprovement aim. It is important that there is consensus in this team that a problemexists and needs fixing and hence that there is clarity about the aim of theimprovement. Information/evidence to support the existence and extent of theproblem must be collected, analysed and shared by relevant parties.
l How will we know that a change is an improvement? Improvement toward a definedaim can only be confirmed if clear measures have been established and resultsdemonstrate progress over time; erefore the team must define clear measures toascertain whether or not improvement work is achieving (or not achieving) thedefined aim.
ANNEX A: Quality Improvement Methodologies
Sort (S1)
Standardize (S4) Set (S2)
Shine (S3)
Sustain (S5)
DiagrammaticPresentation of the 5S’s:
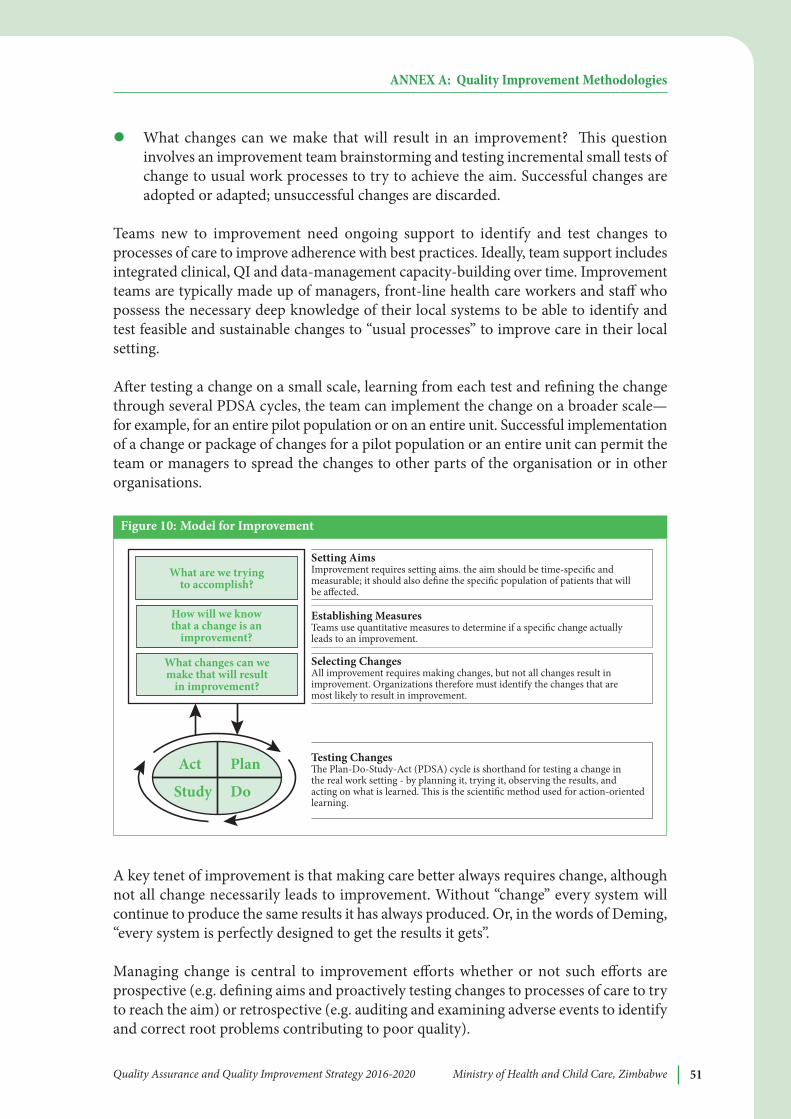
l What changes can we make that will result in an improvement? is questioninvolves an improvement team brainstorming and testing incremental small tests ofchange to usual work processes to try to achieve the aim. Successful changes areadopted or adapted; unsuccessful changes are discarded.
Teams new to improvement need ongoing support to identify and test changes toprocesses of care to improve adherence with best practices. Ideally, team support includesintegrated clinical, QI and data-management capacity-building over time. Improvementteams are typically made up of managers, front-line health care workers and staff whopossess the necessary deep knowledge of their local systems to be able to identify andtest feasible and sustainable changes to “usual processes” to improve care in their localsetting.
Aer testing a change on a small scale, learning from each test and refining the changethrough several PDSA cycles, the team can implement the change on a broader scale—for example, for an entire pilot population or on an entire unit. Successful implementationof a change or package of changes for a pilot population or an entire unit can permit theteam or managers to spread the changes to other parts of the organisation or in otherorganisations.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 51
ANNEX A: Quality Improvement Methodologies
Figure 10: Model for Improvement
Act Plan
Study Do
What are we trying to accomplish?
How will we know that a change is an
improvement?
What changes can we make that will result
in improvement?
Establishing MeasuresTeams use quantitative measures to determine if a speci�c change actually leads to an improvement.
Setting AimsImprovement requires setting aims. the aim should be time-speci�c and measurable; it should also de�ne the speci�c population of patients that will be a!ected.
Selecting ChangesAll improvement requires making changes, but not all changes result in improvement. Organizations therefore must identify the changes that are most likely to result in improvement.
Testing Changes"e Plan-Do-Study-Act (PDSA) cycle is shorthand for testing a change in the real work setting - by planning it, trying it, observing the results, and acting on what is learned. "is is the scienti�c method used for action-oriented learning.
Figure 10: Model for improvement
A key tenet of improvement is that making care better always requires change, althoughnot all change necessarily leads to improvement. Without “change” every system willcontinue to produce the same results it has always produced. Or, in the words of Deming,“every system is perfectly designed to get the results it gets”.
Managing change is central to improvement efforts whether or not such efforts areprospective (e.g. defining aims and proactively testing changes to processes of care to tryto reach the aim) or retrospective (e.g. auditing and examining adverse events to identifyand correct root problems contributing to poor quality).
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe52
While context has a strong influence on which changes may be most feasible and effectivefor overcoming gaps in a specific setting, categories of quality and system gaps andeffective changes (solutions) are oen common across settings. Diverse settings can learnfrom each other to overcome common quality and system gaps. Increasingly, manyimprovement approaches (e.g. Improvement Collaborative) mobilize teams to worktogether across health system levels and geographic sites to identify, test and sharesuccessful changes for overcoming important quality and system gaps, e.g., weeklysimulated resuscitation practice using structured peer to peer observation to maintainprovider competence. Promoting regular shared learning among teams helps to accelerateand scale up improvement efforts.
CLINICAL PRACTICE IMPROVEMENT (CPI)
CPI methodology has been widely used by health-care professionals to improve thequality and safety of health care. It does this through a detailed scrutiny of the processesand outcomes in clinical care. e success of a CPI approach depends on the teamcovering each of the following five phases.
Project phase: e team needs to ask themselves what it is they wish to fix or achieve.ey do this by developing a mission statement or objective that describes what it is theywish to do in a few sentences. is is the time to select the team members who should beselected on the basis of their knowledge about the problem. It is important that patientsshould always be considered as appropriate members of the team at this initial stage.
Diagnostic phase: e team needs to ask if the problem they have identified is worthsolving. e team should establish the full extent of the problem by gathering as muchinformation about the problem as possible. A brainstorming exercise by the team willgenerate possible changes that could lead to an improvement. A decision about how tomeasure the improvement needs to be resolved during this phase. During this phase theteam collects and analyses quantitative and qualitative data of the process beinginvestigated to establish causes of and potential solutions.
intervention Phase: Each of the solutions have to be tested through a trial and errorprocess by using the PDSA cycles to test changes, observe them and keep the bits thatwork.
impact and implementation Phase: is is the time to measure and record the resultsof the trials of the interventions. Did they make any difference? All changes are requiredto be measured for impact so that the change can be said to truly have made a differencerather than a coincidence or a one-off effect. e goal is to introduce a change that hassustained improvement.
Sustaining and improvement phase: e final phase requires the team to develop andagree upon a monitoring process and plans for continuous improvement. Improvementsmade now will become failures in the future if there are no plans to sustain theimprovements.
ANNEX A: Quality Improvement Methodologies
is will involve:
l Standardization of existing processes and systems for undertaking work activities
l Documentation of relevant policies procedures protocols and guidelines
l Measurement and review to enable the change to become routine
l Training and education of staff
ROOT CAUSE ANALYSIS
A root cause analysis is a defined process that seeks to explore all of the possible factorsassociated with an incident by asking what happened, why it occurred and what can bedone to prevent it from happening again. is applies especially to severe adverse eventssuch as avoidable deaths.
Root cause analysis will be used to determine the underlying causes of adverse events,incidents or situations. A root cause analysis may be used for example aer an incidenthas occurred to uncover the primary possible causes. As such, it focuses on the particularincident and the circumstances surrounding it. ere are many lessons to be gained fromthis retrospective process that may prevent similar incidents in the future if this isconducted in a systematic way. Techniques such as problem trees, driver diagrams andthe 5 Whys technique will be applied in conducting root cause analysis.
Health-care workers will receive instruction in this method as part of QI training at bothpre and in-service levels.
For effective root cause analysis the following components are critical:
l Multidisciplinary team which includes community representatives particularlythose that may bring out a patient perspective
l Composed of people who can add value because of their knowledge, position inthe organisation or unique perspective they bring
l Committed persons trained in root cause analysis
QUALITY IMPROVEMENT COLLABORATIVE
e improvement collaborative is a structured improvement approach that organizes alarge number of teams or sites to work together for a 12 to 24 month period to achievesignificant improvements in a specific area of care. e collaborative approach combinestraditional QI methods of team work, process analysis, and introduction of standards,measurement of quality indicators, training, job aides, and coaching. e collaborativeorganises regular sharing of results among teams through learning sessions in whichteams learn from each other about which changes have been successful and which werenot. is results in a dynamic improvement strategy in which many teams working onrelated problem areas can learn from each other in a way that facilitates rapid
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 53
ANNEX A: Quality Improvement Methodologies
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe54
dissemination of successful practices. In its emphasis on spread and scale-up ofimprovements, the improvement collaborative model offers a powerful new tool for QI.
e following elements are key to successful collaboratives:
l Clear improvement objectives
l Organisational structure
l Change package and clear dissemination plan
l Qualified and functional quality improvement teams
l Monitoring systems for quality of processes and results
l Regular coaching support to quality improvement teams
l Opportunities to share experiences and results obtained from changes made
improvement Collaborative Phase
e improvement collaborative will typically will go through the following phases:
Preparation: A situation analysis of current quality standards with a focus on identifyingroot causes of the discrepancy between expected standards and what is obtaining is thefirst task of the collaborative. Involvement of key stakeholders is critical during this phase.e organisational structure of the collaborative is established as well as the capacity andresource needs. Aer selection of initial sites a spread and communication strategy andcollaborative implementation plan is laid out. is process will take 6 to 8 months.
implementation: A collaborative will focus on one technical area (e.g. malaria, ART, TB,newborn care etc.). Interventions may also focus on issues of health systemsstrengthening (safety, health worker responsiveness and performance). e model forimprovement will incorporate 4 key elements:
l Specific and measurable aims
l Measurements of improvement that are tracked over time
l Key changes that will result in the desired improvement
l Series of parallel testing plan-do-study-act (PDSA) cycles. PDSA cycles shouldbe short but significant, testing a big change idea in a short timeframe so that ateam can identify ways to improve or change the idea.
ese stages involve the organisation of content and methods of learning sessions andaction periods as well as determine when to synthesise best practices and dissemination.
Learning sessions will typically be a national or provincial / regional workshop for teamsto share experiences and learn from one another, learn QI as well as clinical content.Attendees will comprise team representatives from each facility, provincial, district andnational stakeholders and trainers.
ANNEX A: Quality Improvement Methodologies
Documentation of improvement changes or best practices will assist in motivating teamsto sustain gains. e implementation stage will last 18-24 months. Aer completion anddemonstration of significant improvements the team may then focus on another technicalarea.
a spread strategy is a crucial feature of a collaborative. A spread strategy defines howone plans to gets to escalate or disseminate improvements made as a result of a testedand proven change package. In this phase the more experienced initial teams providesupport and mentorship to new teams.
e success of collaborative will hinge on qualified, functional and committed qualityimprovement teams. rough teamwork they will strive to understand their clients,analyse management processes, monitor results, and plan, implement and study changesor innovations to improve performance. ese teams are expected to come together atdefined intervals as a network with other teams to share results, innovations, and issues,and to learn from one another.
Monitoring is a vital feature of any collaborative. Quality improvement teams shall usea common agreed set of process and outcome indicators to measure quality. Whereverpossible, data should come from existing sources and not from a separate data collectionsystem. Occasionally, existing health information collection systems may be slightlymodified to capture essential information e.g. waiting time.
It is essential, that the quality improvement teams receive regular support throughcoaching. A coach will be an experienced person in quality improvement who will inturn help build the capacity of the local team in the collaborative process towards beingself-sufficient in QI.
Collaboratives have as their overall goal to provide an improved set of norms, models ofcare and/or best practices in an organisation for carrying out norms that can be rapidlyspread to other sites. Collaboratives provide a mechanism for resolving the operationalbarriers or obstacles around implementing any set of norms. us, a key feature of acollaborative is to arrive at a tested and refined “change package” and/or a set of bestpractices related to its implementation.
National, Provincial and District Quality improvement workshops
e National, Provincial and District Health Executives will facilitate inter-facilitylearning sessions where QI teams will share their experiences on the methods they usedto improve quality, results and lessons learnt. ese workshops will include cases studies,interactive illustrated presentations, discussion of common themes, and walk throughposter gallery through various team presentations. It is recommended that health careproviders in implementing facilities attend these workshops and that a verifiable methodof feedback to their facilities is put in place. A suggested frequency of a least bi-annualmeeting is suggested. It is important that leadership demonstrates commitment to qualityso as to motivate healthcare providers. Recognition and awards for performance shouldbe made at such platforms to help build a culture of quality improvement.
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe 55
ANNEX A: Quality Improvement Methodologies
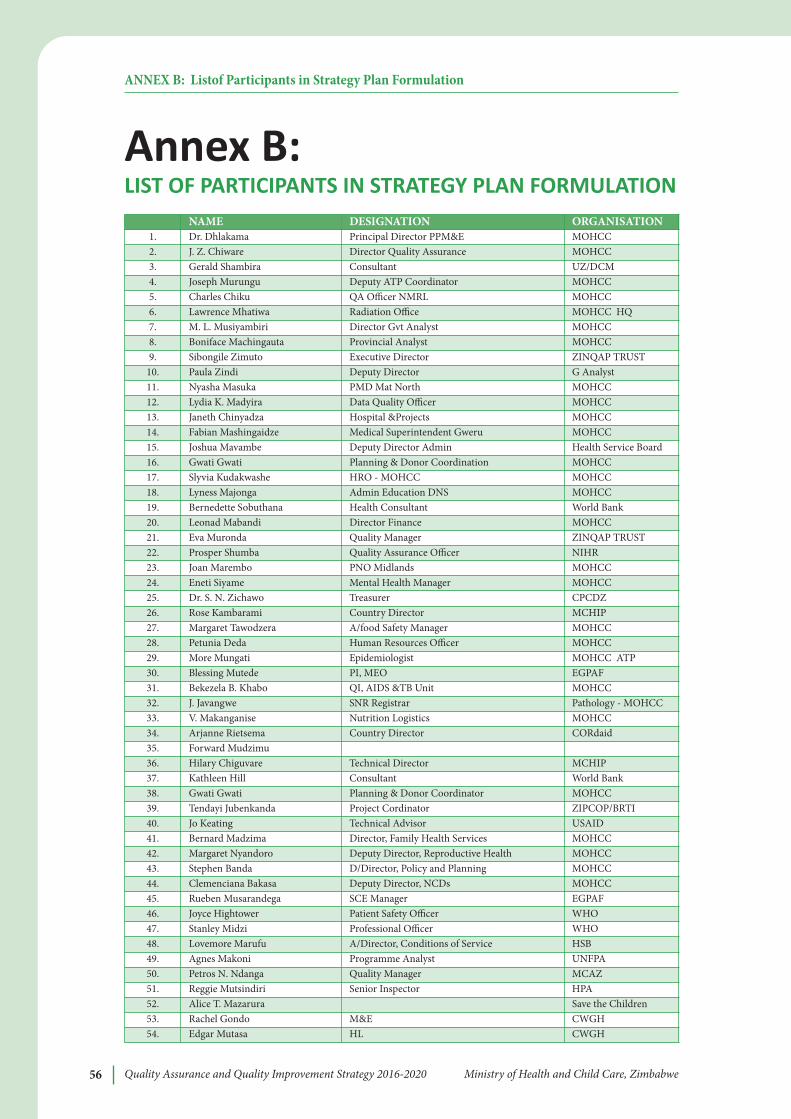
Quality Assurance and Quality Improvement Strategy 2016-2020 Ministry of Health and Child Care, Zimbabwe56
Annex B: LIST OF PARTICIPANTS IN STRATEGY PLAN FORMULATION
ANNEX B: Listof Participants in Strategy Plan Formulation
NaMe DeSiGNaTiON ORGaNiSaTiON 1. Dr. Dhlakama Principal Director PPM&E MOHCC2. J. Z. Chiware Director Quality Assurance MOHCC3. Gerald Shambira Consultant UZ/DCM4. Joseph Murungu Deputy ATP Coordinator MOHCC5. Charles Chiku QA Officer NMRL MOHCC6. Lawrence Mhatiwa Radiation Office MOHCC HQ7. M. L. Musiyambiri Director Gvt Analyst MOHCC8. Boniface Machingauta Provincial Analyst MOHCC9. Sibongile Zimuto Executive Director ZINQAP TRUST
10. Paula Zindi Deputy Director G Analyst11. Nyasha Masuka PMD Mat North MOHCC12. Lydia K. Madyira Data Quality Officer MOHCC13. Janeth Chinyadza Hospital &Projects MOHCC14. Fabian Mashingaidze Medical Superintendent Gweru MOHCC15. Joshua Mavambe Deputy Director Admin Health Service Board16. Gwati Gwati Planning & Donor Coordination MOHCC17. Slyvia Kudakwashe HRO - MOHCC MOHCC18. Lyness Majonga Admin Education DNS MOHCC19. Bernedette Sobuthana Health Consultant World Bank20. Leonad Mabandi Director Finance MOHCC21. Eva Muronda Quality Manager ZINQAP TRUST22. Prosper Shumba Quality Assurance Officer NIHR23. Joan Marembo PNO Midlands MOHCC24. Eneti Siyame Mental Health Manager MOHCC25. Dr. S. N. Zichawo Treasurer CPCDZ26. Rose Kambarami Country Director MCHIP27. Margaret Tawodzera A/food Safety Manager MOHCC28. Petunia Deda Human Resources Officer MOHCC29. More Mungati Epidemiologist MOHCC ATP30. Blessing Mutede PI, MEO EGPAF31. Bekezela B. Khabo QI, AIDS &TB Unit MOHCC32. J. Javangwe SNR Registrar Pathology - MOHCC33. V. Makanganise Nutrition Logistics MOHCC34. Arjanne Rietsema Country Director CORdaid35. Forward Mudzimu36. Hilary Chiguvare Technical Director MCHIP37. Kathleen Hill Consultant World Bank38. Gwati Gwati Planning & Donor Coordinator MOHCC39. Tendayi Jubenkanda Project Cordinator ZIPCOP/BRTI40. Jo Keating Technical Advisor USAID41. Bernard Madzima Director, Family Health Services MOHCC42. Margaret Nyandoro Deputy Director, Reproductive Health MOHCC43. Stephen Banda D/Director, Policy and Planning MOHCC44. Clemenciana Bakasa Deputy Director, NCDs MOHCC45. Rueben Musarandega SCE Manager EGPAF46. Joyce Hightower Patient Safety Officer WHO47. Stanley Midzi Professional Officer WHO48. Lovemore Marufu A/Director, Conditions of Service HSB49. Agnes Makoni Programme Analyst UNFPA50. Petros N. Ndanga Quality Manager MCAZ 51. Reggie Mutsindiri Senior Inspector HPA52. Alice T. Mazarura Save the Children53. Rachel Gondo M&E CWGH 54. Edgar Mutasa HL CWGH