1. back & vertebral column (76).pptx
TRANSCRIPT

Back and Vertebral Column
Objectives: Understand the vertebral column Describe the primary and secondary curvatures Understand the different types of abnormal
curvatures Back pain causes Fractures and dislocation of the vertebrae Intervertebral discs Spondylolysis and spondylolisthesis Understand the meninges and their extent Gray and white mater of the spinal cord Spinal nerve and its functional components Epidural anesthesia Lumbar puncture

The back includes the: Skin and subcutaneous tissue.
Muscles: a superficial layer, and deeper layers Vertebral column: the vertebrae, intervertebral (IV) discs, and
associated ligaments.
Ribs (in the thoracic region): particularly their posterior portions, medial to the angles of the ribs.
Spinal cord and meninges (membranes that cover the spinal cord).
Various segmental nerves and vessels.
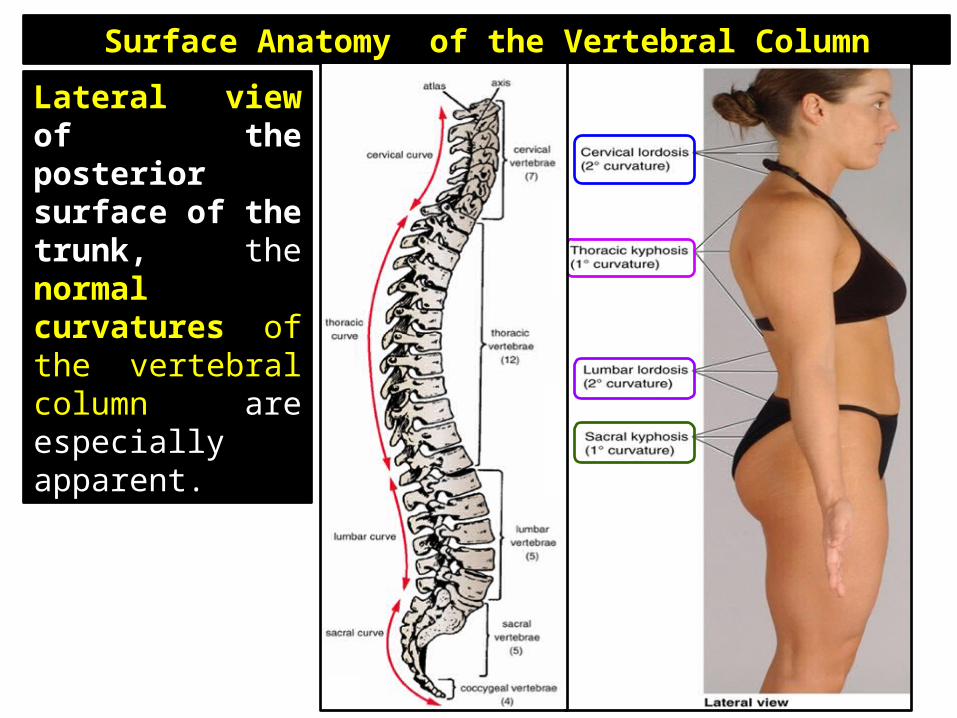
Surface Anatomy of the Vertebral Column
Lateral view of the posterior surface of the trunk, the normal curvatures of the vertebral column are especially apparent.

Vertebral column: vertebrae and IV discs collectively make up the vertebral column. Extends from the cranium (skull)
to the apex of the coccyx.
Adult vertebral column: 72 - 75 cm long.
Function: Protects the spinal cord and spinal
nerves. Supports the weight of the body Rigid and flexible axis for the body Plays an important role in posture
and locomotion

VertebraeConsists of 33 vertebrae arranged in five regions: 7 cervical 12 thoracic 5 lumbar 5 sacral 4 coccygeal
5 sacral vertebrae are fused in adults to form the sacrum
4 coccygeal vertebrae fuse to form the coccyx.

Vertebrae Lumbosacral angle
occurs at the junction of, and is formed by, the long axes of the lumbar region of the vertebral column and the sacrum.
Vertebrae reach maximum size immediately superior to the sacrum, which transfers the weight to the pelvic girdle at the sacroiliac joints.

Vertebrae
The cervical, thoracic, lumbar, and first sacral vertebrae also articulate at synovial zygapophysial joints, which facilitate and control the vertebral column's flexibility.

Structure and Function of the Vertebrae
A typical vertebra consists of • vertebral body • vertebral arch • seven processes
Vertebral body:Size of the vertebral bodies increases as the column descends, most markedly from T4 inferiorly, as each bears progressively greater body weight.

Structure and Function of the Vertebrae Vertebral body consists of vascular,
trabecular (spongy, cancellous) bone enclosed by a thin external layer of compact bone.
Trabeculae are occupied by red marrow, hematopoietic (blood-forming) tissues of the mature individual.
One or more large foramina in the posterior surface of the body accommodate basivertebral veins that drain the marrow .

Structure and Function of the VertebraeSuperior and inferior surfaces of the vertebral body are covered with discs of hyaline cartilage.

Vertebral arch: posterior to the vertebral body and consists of two (right and left) pedicles and laminae .
Pedicles: short, stout cylindrical processes that project posteriorly from the vertebral body to meet two broad, flat plates of bone, called laminae, which unite in the midline.
Vertebral foramen: vertebral arch and the posterior surface of the vertebral body form the walls of the vertebral foramen.

Vertebral canal: succession of vertebral foramina in the articulated vertebral column forms the vertebral canal (spinal canal).Contains: Spinal cord Roots of the spinal Membranes (meninges), Fat Blood vessels

Vertebral notches: indentations observed in lateral views of the vertebrae
Intervertebral foramina:
Bounded by the superior and inferior vertebral notches of adjacent vertebrae and the IV discs connecting.
Spinal nerves emerge from the vertebral column with their accompanying vessels.

Spinal nerve roots and intervertebral foramen:
C1: passes superior to the posterior arch of C1 vertebra
C8: passes through the IV foramen between C7 & T1 vertebrae
T1 : passes through the IV foramen between T1 & T2
L5 :passes through the IV foramen between L5 & S1
Any spinal nerve which exits through IV foramen, passes through the superior bony half of the foramen, not affected by a herniated disc at that level. But the nerve which passes immediately below the IV foramen, directly across the area of herniation and is affected.
Incase of IV disc prolapse, compresses the nerve root numbered one below the level of the herniated disc.
L5 nerve root is compressed by an L4-L5 Inter Vertebral disc herniation.

Seven processes : One median spinous process
projects posteriorly from the vertebral arch at the junction of the laminae.
Two transverse processes project posterolaterally from the junctions of the pedicles and laminae.
Four articular processes: two superior and two inferior also arise from the junctions of the pedicles and laminae, each bearing an articular facet.

Laminectomy The surgical excision of one or more spinous
processes and the adjacent supporting vertebral laminae in a particular region of the vertebral column is called a laminectomy.
The term is also commonly used to denote removal of most of the vertebral arch by transecting the pedicles .
Laminectomies are performed surgically (or anatomically in the dissection laboratory) to gain access to the vertebral canal, providing posterior exposure of the spinal cord (if performed above the L2 level) and/or the roots of specific spinal nerves.
Surgical laminectomy is often performed to
relieve pressure on the spinal cord or nerve roots caused by a tumor, herniated IV disc, or bony hypertrophy (excess growth).

Cervical Vertebrae: form the skeleton of the neck. Smaller in size IV discs thinner Horizontal orientation
of the articular facets
Elevated superolateral margin is the uncus of the body (uncinate process).
Spinous processes of the C3 - C6 vertebrae are short and usually bifid.

Atypical cervical vertebrae: Vertebra C1, also called the atlas Has neither a body nor a spinous
process. Transverse processes of the atlas
arise from the lateral masses Kidney-shaped, concave superior
articular surfaces of the lateral masses receive two large cranial protuberances called the occipital condyles.
Anterior and posterior arches, each of which bears a tubercle .
Posterior arch, which corresponds to the lamina of a typical vertebra, has a wide groove for the vertebral artery on its superior surface. The C1 nerve also runs in this groove.

Vertebra C2, Axis: C1, rotates on C2, as when a person
turns the head. � Two large, flat bearing surfaces, the
superior articular facets, on which the atlas rotates .
Odontoid process (Dens): lies anterior to the spinal cord and serves as the pivot about which the rotation occurs.
Dens: held in position against the posterior aspect of the anterior arch of the atlas by the transverse ligament of the atlas.
Transverse ligament prevents posterior (horizontal) displacement of the dens and anterior displacement of the atlas.

Cervical Vertebrae Oval transverse foramen in the
transverse process (L. foramen transversarium).
Vertebral arteries and their accompanying veins pass through the transverse foramina, except those in C7, which transmit only small accessory veins.
Transverse processes of cervical vertebrae end laterally in two projections: an anterior tubercle and a posterior tubercle.
Tubercles provide attachment for a laterally placed group of cervical muscles (levator scapulae and scalenes).
Grooves on the transverse processes between tubercles (the floor of the groove being formed by a costotransverse bar) accommodate the anterior rami of the cervical spinal nerves.

Carotid tubercles:C6 vertebra: called carotid tubercles because the common carotid arteries may be compressed here, in the groove between the tubercle and body to control bleeding from these vessels.

C7 vertebra characterized by a long spinous process; because of this prominent process, is called the vertebral prominens.
Run your finger along the midline of the posterior aspect of your neck until you feel the prominent C7 spinous process.

Dislocation of the Cervical Vertebrae Can be dislocated in neck injuries with less force
than is required to fracture them.
Because of the large vertebral canal in the cervical region, slight dislocation can occur here without damaging the spinal cord.
Severe dislocations, or dislocations combined with fractures (fracture & dislocations) injure the spinal cord.
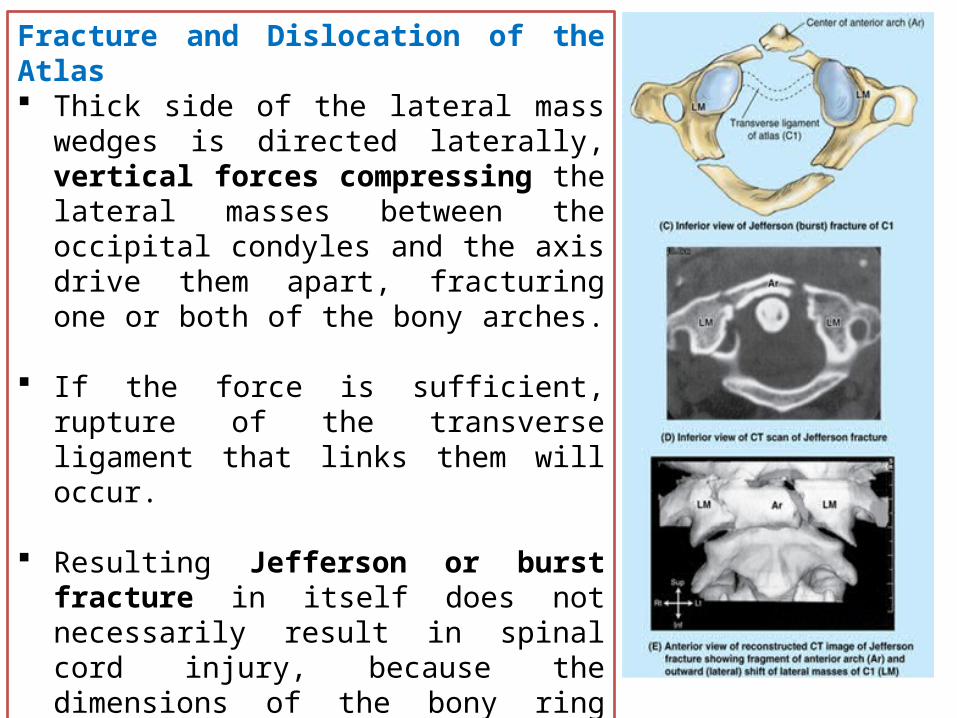
Fracture and Dislocation of the Atlas Thick side of the lateral mass wedges is
directed laterally, vertical forces compressing the lateral masses between the occipital condyles and the axis drive them apart, fracturing one or both of the bony arches.
If the force is sufficient, rupture of the transverse ligament that links them will occur.
Resulting Jefferson or burst fracture in itself does not necessarily result in spinal cord injury, because the dimensions of the bony ring actually increase.
Spinal cord injury is more likely, however, if the transverse ligament has also been ruptured indicated radiographically by widely spread lateral masses.

Fracture and Dislocation of the Axis Usually the fracture occurs in the bony column
formed by the superior and inferior articular processes of the axis.
A fracture in this location, called a traumatic spondylolysis of C2, usually occurs as a result of hyperextension of the head on the neck
Hyperextension of the head was used to execute criminals by hanging, thus this fracture is called a hangman's fracture.
With or without such subluxation (incomplete dislocation) of the axis, injury of the spinal cord and/or of the brainstem is likely, sometimes resulting in quadriplegia (paralysis of all four limbs) or death.
Fractures of the dens are also common axis injuries (40 - 50%), which may result from a horizontal blow to the head.

Thoracic Vertebrae Middle four thoracic vertebrae (T5 - T8) demonstrate all the features
typical of thoracic vertebrae.
The articular processes of thoracic vertebrae extend vertically with paired articular facets
Attachment of the rib cage combined with the vertical orientation of articular facets and overlapping spinous processes limits flexion and extension as well as lateral flexion.

T1: atypical of thoracic vertebrae: Has a long, almost
horizontal spinous process
Has a complete costal facet on the superior edge of the body for the 1st rib
Demifacet on the inferior edge that contributes to the articular surface for the 2nd rib.

T9 - T12 vertebrae have some features of lumbar vertebrae.The tubercles similar to the accessory and mammillary processes of lumbar vertebrae.
Most of the transition in characteristics from thoracic to lumbar region occurs over the length of a single vertebra: vertebra T12.
Consequently, vertebra T12 is subject to transitional stresses that cause it to be the most commonly fractured vertebra.

Thoracic VertebraePart CharacteristicsBody Heart shaped
one or two costal facets for articulation with head of ribVertebral foramen Circular and smaller than those of cervical and lumbar vertebrae
Transverse processes
Long and strong and extend posterolaterally Length diminishes from T1 to T12 (T1 - T10 have facets for articulation
with tubercle of rib)Articular processes Superior facets directed posteriorly and slightly laterally
Inferior facets directed anteriorly and slightly medially Plane of facets lies on arc centered about vertebral body
Spinous processes Long and slope posteroinferiorly Tips extend to level of vertebral body below

Lumbar Vertebrae

Lumbar Vertebrae
Part CharacteristicsBody •Massive
•Kidney shaped when viewed superiorlyVertebral foramen •Triangular
•Larger than in thoracic vertebrae and smaller than in cervical vertebraeTransverse processes
•Long and slender•Accessory process on posterior surface of base of each process
Articular processes •Superior facets directed posteromedially (or medially)•Inferior facets directed anterolaterally (or laterally)•Mammillary process on posterior surface of each superior articular process
Spinous processes •Short ,Thick, broad, and hatchet shaped

L5
Largest of all vertebrae
Distinguished by its massive body and transverse processes.
Body is markedly deeper anteriorly
Responsible for the lumbosacral angle between the long axis of the lumbar region of the vertebral column and that of the sacrum .
Body weight transmits from L5 vertebra to the base of the sacrum, formed by the superior surface of S1 vertebra.
Vertebra L5

Identify the structures

Sacrum Large, triangular, wedged-shaped sacrum Composed of five fused sacral vertebrae
in adults. Provides strength and stability to the
pelvis Transmits the weight of the body to the
pelvic girdle. Base: Formed by the superior surface of the S1
vertebra. Superior articular processes articulate
with the inferior articular processes of the L5 vertebra.
The anterior projecting edge of the body of the S1 vertebra is the sacral promontory, an important obstetrical landmark.
Apex :tapering inferior end, has an oval facet for articulation with the coccyx.

Sacral Canal: Continuation of the vertebral
canal in the sacrum.
Contains: spinal nerve roots arising inferior to the L1 vertebra, known as the cauda equina (L. horse tail).
Sacral foramina: Four pairs of sacral foramina
present on the pelvic and posterior surfaces of the sacrum for the exit of the posterior and anterior rami of the spinal nerves.

Pelvic surface of the sacrum:
Smooth and concave.
Four transverse lines on this surface of sacra from adults indicate where fusion of the sacral vertebrae occurred.
Fusion of the sacral vertebrae starts after age 20
Lateral surface: Superior part looks like an
auricle is called the auricular surface.

Dorsal surface of the sacrum: Rough, convex, and marked by five
prominent longitudinal ridges.
Median crest: represents the fused rudimentary spinous processes of the superior three or four sacral vertebra; S5 has no spinous process.
Intermediate crest: represent the fused articular processes
Lateral crest: tips of the transverse processes of the fused sacral vertebrae.

Sacral hiatus: Results from the absence of the laminae and spinous process of S5 and sometimes S4.
Sacral cornua: representing the inferior articular processes of S5 vertebra, project inferiorly on each side of the sacral hiatus
Sacral hiatus and the sacral cornua together is inverted U-shaped and clinically important surface land mark for caudal (epidural) anesthesia

Caudal Epidural Anesthesia A local anesthetic agent is injected
into the fat of the sacral canal that surrounds the proximal portions of the sacral nerves.
Can be accomplished by the sacral hiatus. Because the sacral hiatus is located between the sacral cornua and inferior to the S4 spinous process
Anesthetic solution spreads superiorly and extradurally, where it acts on the S2 and Co spinal nerves of the cauda equina.

Transsacral epidural anesthesia
Anesthetic agents injected through the posterior sacral foramina into the sacral canal around the spinal nerve roots.

Abnormal Fusion of Vertebrae Sacralization : approximately
5% of people, L5 is partly or completely incorporated into the sacrum
Lumbarization : S1 is more or less separated from the sacrum and is partly or completely fused with L5 vertebra

Coccyx Small triangular bone
Formed by fusion of the four rudimentary coccygeal vertebrae
Pelvic surface: concave and relatively smooth
Posterior surface: rudimentary articular processes.
Co1:largest and broadest of all the coccygeal vertebrae.
Transverse processes: connected to the sacrum
Articular processes form coccygeal cornua, articulate with the sacral cornua.

Injury of the Coccyx
An abrupt fall onto the lower back may cause a painful subperiosteal bruising or fracture of the coccyx, or a fracture dislocation of the sacrococcygeal joint.
Displacement is common, and surgical removal of the fractured bone may be required to relieve pain.
In difficult childbirth occasionally injures the mother's coccyx.
A troublesome syndrome, coccygodynia, often follows coccygeal trauma; pain relief is commonly difficult.

Cervical Ribs A relatively common anomaly is a cervical rib. In 1-2% of
people, the developmental costal element of C7, becomes abnormally enlarged.
Bilaterally about 60% of the time.
The supernumerary (extra) rib may place pressure on structures that emerge from the superior thoracic aperture: notably the subclavian artery or inferior trunk of the brachial plexus and may cause thoracic outlet syndrome

Effect of Aging on Vertebrae Osteophytes (bony spurs) commonly develop around the
margins of the vertebral body
Osteophytes develop along the attachments of the joint capsules and accessory ligaments, especially those of the superior articular process.
Some patients with these manifestations present with pain, others demonstrate the same age-related changes but have no pain.

Anomalies of the Vertebrae: Spina bifida occulta:
Present in up to 24% of the population
Epiphysis of a transverse process fails to fuse.
Laminae (neural arches) of L5 and/or S1 fail to develop normally and fuse posterior to the vertebral canal.
Concealed by the overlying skin
Location is often indicated by a tuft of hair.
X-ray image of spina bifida occulta in S-1
Myelomeningocele Most common and most severe form of Spina Bifida Unfused portion of the spinal column allows the spinal
cord to protrude through an opening. The meningeal membranes that cover the spinal cord
form a sac enclosing the spinal elements. Myelomeningocele

In severe types of spina bifida: Spina bifida cystica
One or more vertebral arches may fail to develop completely.
Associated with herniation of the meninges (meningocele, a spina bifida associated with a meningeal cyst) and/or the spinal cord (meningomyelocele).
Neurological symptoms are usually present in severe cases of meningomyelocele (e.g., paralysis of the limbs and disturbances in bladder and bowel control).
Severe forms of spina bifida result from neural tube defects, such as the defective closure of the neural tube during the 4th week of embryonic development.

Contents of the Vertebral Canal
Spinal cord Spinal nerve roots Spinal meninges Vascular structures

Spinal Cord Cylindrical structure.
Flattened anteriorly and posteriorly.
Begins as a continuation of the medulla oblongata.
In adults, 42-45 cm long .
Extends from the foramen magnum in the occipital bone to the level of the L1 or L2 vertebra.

Spinal cord:Enlarged in two regions: Cervical enlargement
extends from the C4 through T1 segments of the spinal cord.
Lumbosacral (lumbar) enlargement extends from T11 through S1 segments of the spinal cord.

Spinal Nerve RootsVentral: Motor
Dorsal: SensoryBoth the root meet together and form Trunk of the spinal nerve

In embryos, the spinal cord occupies the full length of the vertebral canal
During the fetal period, the vertebral column grows faster than the spinal cord; as a result, the cord ascends relative to the vertebral canal.
At birth, the tip of the medullary cone is at the L4-L5 level.
Postnatal life, the spinal cord is shorter than the vertebral column
Progressive obliquity of the spinal nerve roots.

The lumbar and sacral nerve roots are the longest, extending far beyond the termination of the adult cord at approximately the L2 level to reach the remaining lumbar, sacral, and coccygeal IV foramina.
This loose bundle of spinal nerve roots arising from the lumbosacral enlargement and the medullary cone of the spinal cord resembles a horse's tail, hence its name the cauda equina (L. horse tail).

Filum Terminale (terminal filum): Proximal end (the pial part or
internal terminal filum) consists of vestiges of neural tissue, connective tissue, and neuroglial tissue covered by pia mater.
Terminal filum perforates the inferior end of the dural sac, gaining a layer of dura and continuing through the sacral hiatus as the dural part or external terminal filum (also known as the coccygeal ligament) to attach to the dorsum of the coccyx.

Spinal Meninges and Cerebrospinal Fluid:• Dura mater• Arachnoid mater• Pia mater
These membranes surround, support, and protect the spinal cord and spinal nerve roots.
Contain the cerebrospinal fluid (CSF) in which these structures are suspended.
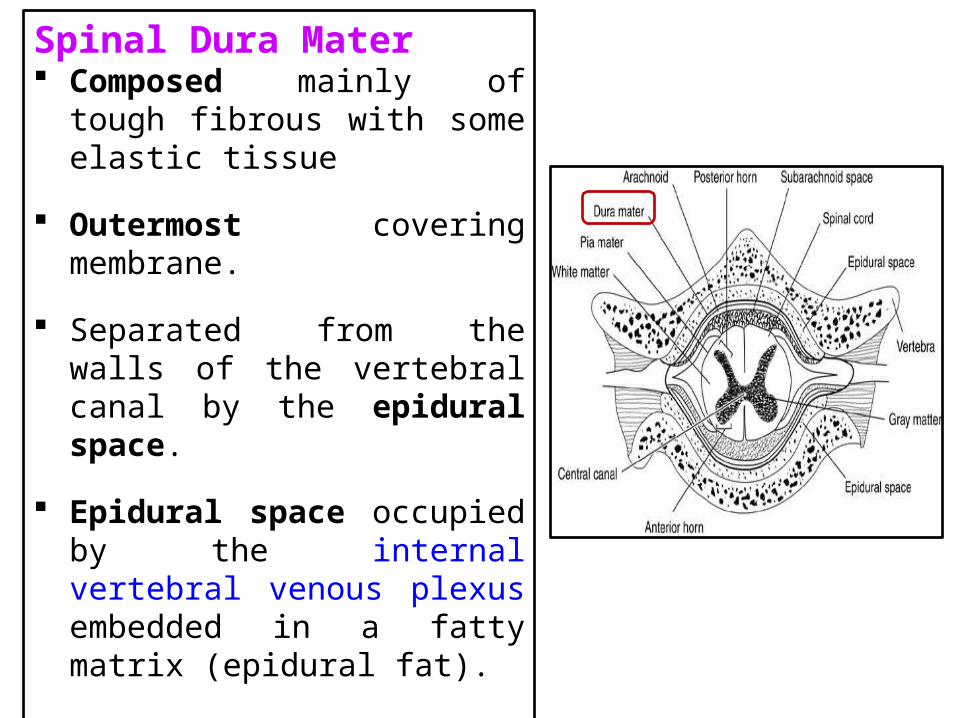
Spinal Dura Mater Composed mainly of tough fibrous
with some elastic tissue
Outermost covering membrane.
Separated from the walls of the vertebral canal by the epidural space.
Epidural space occupied by the internal vertebral venous plexus embedded in a fatty matrix (epidural fat).
Epidural space extends from the foramen magnum to the sacral hiatus .
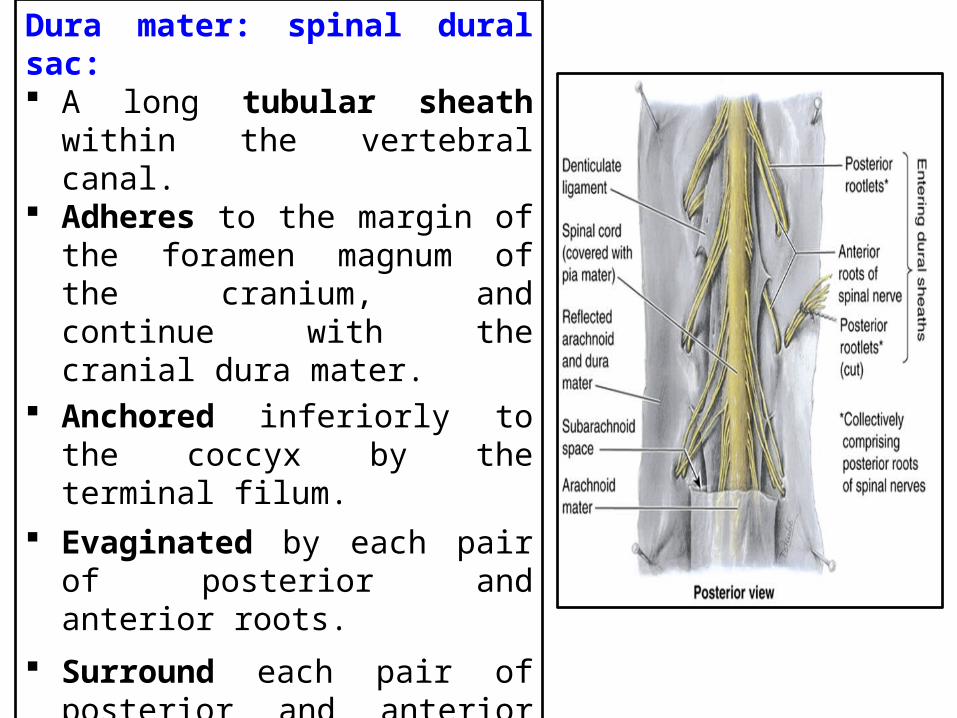
Dura mater: spinal dural sac: A long tubular sheath within the
vertebral canal. Adheres to the margin of the
foramen magnum of the cranium, and continue with the cranial dura mater.
Anchored inferiorly to the coccyx by the terminal filum.
Evaginated by each pair of posterior and anterior roots.
Surround each pair of posterior and anterior nerve roots as dural root sheaths, or sleeves.
Dural sheaths blend with the epineurium and adheres to the periosteum lining the IV foramina.

Spinal Arachnoid Mater: Delicate, avascular membrane. Composed of fibrous and
elastic tissue. Lines the spinal dural sac and
its dural root sheaths.
Encloses the CSF-filled subarachnoid space
In a lumbar spinal puncture, the needle traverses the dura and arachnoid mater simultaneously.
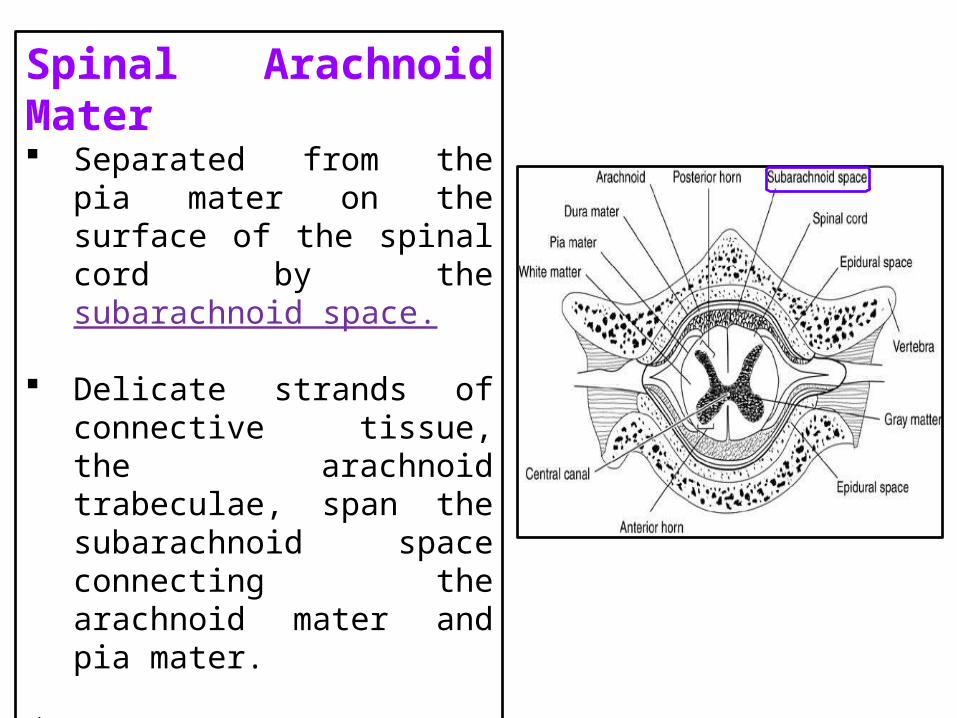
Spinal Arachnoid Mater Separated from the pia mater
on the surface of the spinal cord by the subarachnoid space.
Delicate strands of connective tissue, the arachnoid trabeculae, span the subarachnoid space connecting the arachnoid mater and pia mater.
Bleeding into this layer creates a pathological space at the dura arachnoid junction in which a subdural hematoma is formed.

Spinal Pia Mater Innermost covering membrane
Consists of flattened cells .
Covers the roots of the spinal nerves and the spinal blood vessels.
Forms Ligamentum denticulum:
sawtooth denticulate ligaments (L. denticulus, small tooth), which run longitudinally along each side of the spinal cord.
Continues as the terminal filum.

Spaces Associated with the Spinal MeningesSpace Location Contents
Extradural (epidural) • Space between periosteum lining bony wall of vertebral canal and dura mater
• Fat (loose connective tissue)
• Internal vertebral venous plexuses
• Ensheathed roots of spinal nerves
Subarachnoid (leptomeningeal)
• Space between arachnoid mater and pia mater
• CSF• Arteries & Veins: Radicular Segmental Medullary Spinal • Arachnoid trabeculae

Subarachnoid Space Located between the arachnoid mater and the pia mater. Filled with CSF Enlargement of the subarachnoid space in the dural sac, caudal to
the medullary cone and containing CSF and the cauda equina, is the spinal or lumbar cistern.
Lumbar cistern extends from the L2 vertebra to the second segment of the sacrum.

Lumbar Spinal Puncture (spinal tap): Extraction or sampling of CSF from
the lumbar cistern,
Examination of CSF can also determine if blood is present.
Performed with the patient leaning forward or lying on the side with the back flexed.
Flexion of the vertebral column facilitates insertion of the needle by spreading the vertebral laminae and spinous processes apart, stretching the ligamenta flava.

Lumbar Spinal Puncture
A lumbar puncture needle, fitted with a stylet, is inserted in the midline between the spinous processes of the L3 and L4 (or L4 and L5) vertebrae.
At these levels, there is no danger of damaging the spinal cord.
Needle punctures the dura mater and arachnoid mater and enters the lumbar cistern.
When the stylet is removed, CSF escapes at the rate of approximately one drop per second.
If subarachnoid pressure is high, CSF flows out or escapes as a jet.
Lumbar puncture is not performed in the presence of increased intracranial pressure

Epidural BlocksAn anesthetic agent can be injected into the extradural (epidural) space by Lumbar Spinal Puncture, (lumbar epidural block), or through the sacral hiatus (caudal epidural block).
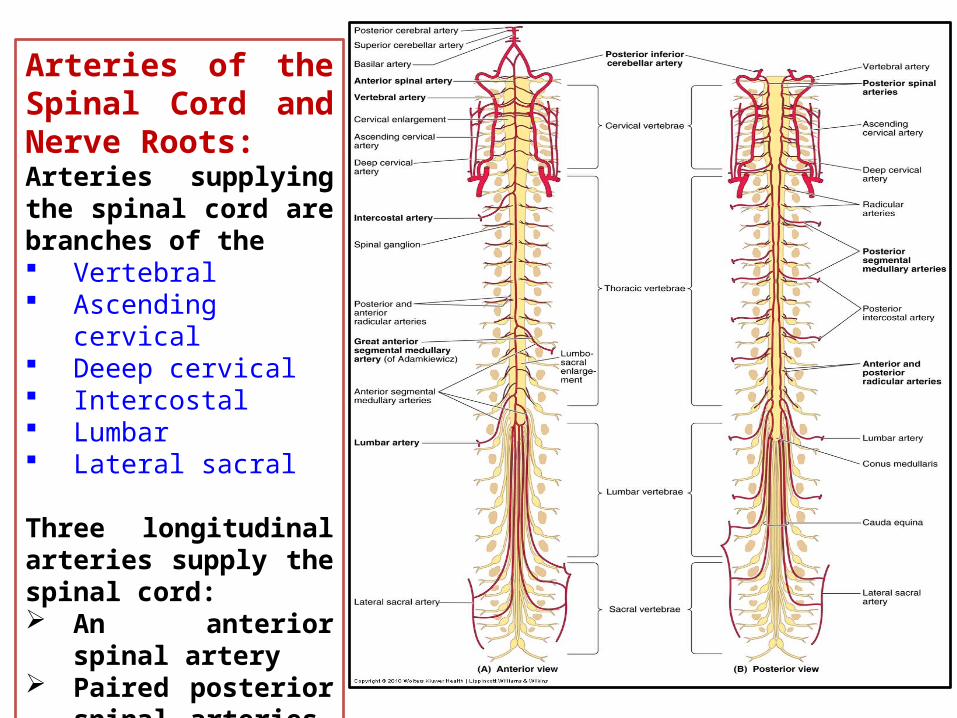
Arteries of the Spinal Cord and Nerve Roots:Arteries supplying the spinal cord are branches of the Vertebral Ascending cervical Deeep cervical Intercostal Lumbar Lateral sacral
Three longitudinal arteries supply the spinal cord: An anterior spinal
artery Paired posterior spinal
arteries.

Arteries of the Spinal Cord and Nerve Roots Anterior spinal artery:
formed by the union of branches of the vertebral arteries, runs inferiorly in the anterior median fissure.
Sulcal arteries arise from the anterior spinal artery and enter the spinal cord through this fissure.

Arteries of the Spinal Cord and Nerve Roots Circulation to the spinal cord
depends on segmental medullary and radicular arteries.
Anterior and posterior segmental medullary arteries are derived from spinal branches of the
• Ascending cervical• Deep cervical • Vertebral • Posterior intercostal • Lumbar arteries

Great anterior segmental medullary artery (of Adamkiewicz):
Present on the is on the left side in about 65% of people,
Reinforces the circulation to two thirds of the spinal cord, including the lumbosacral enlargement.
Larger than the other segmental medullary arteries
Arises from an inferior intercostal or upper lumbar artery.
Enters the vertebral canal through the IV foramen at the lower thoracic or upper lumbar level.

Veins of the Spinal Cord Veins draining the
spinal cord have a distribution similar to that of the spinal arteries.
Three anterior and three posterior spinal veins.
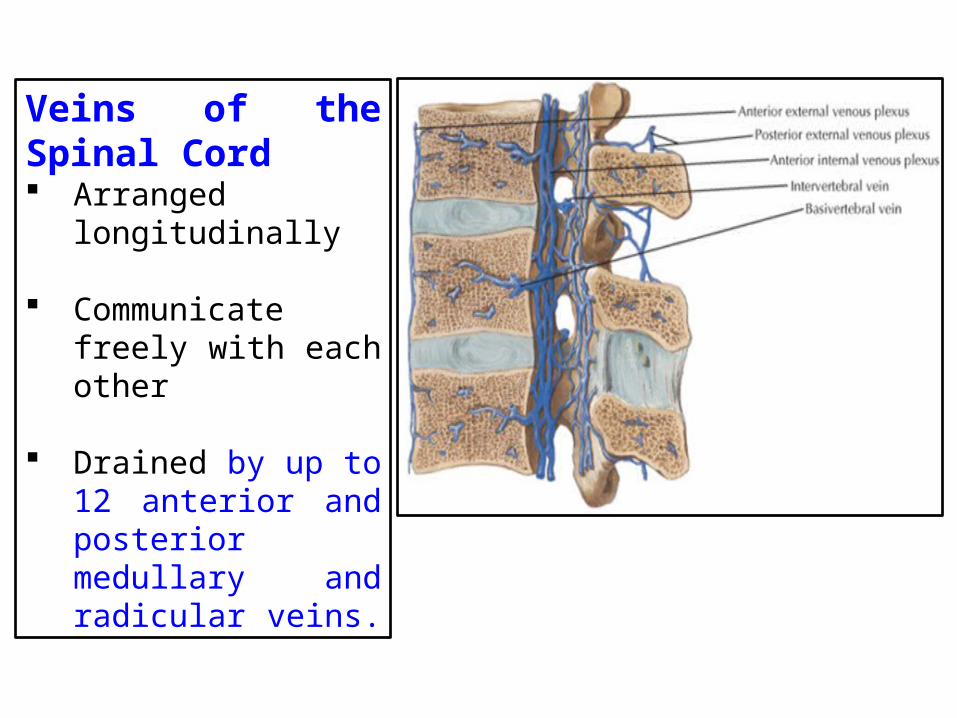
Veins of the Spinal Cord Arranged longitudinally
Communicate freely with each other
Drained by up to 12 anterior and posterior medullary and radicular veins.

Veins of the Spinal Cord Join the internal vertebral
(epidural) venous plexus in the epidural space.
Internal vertebral venous plexus communicate with dural sinuses and vertebral veins in the cranium.
Internal vertebral plexus communicates with the external vertebral venous plexus on the external surface of the vertebrae.

Ischemia of the Spinal Cord: Fractures, dislocations, and fracture dislocations
may interfere with the blood supply to the spinal cord from the spinal and medullary arteries.
Ischemia of the spinal cord affects its function and can lead to muscle weakness and paralysis.

Ischemia of the Spinal CordRuptured aneurysms of the aorta or occlusion of the great anterior segmental medullary artery(of Adamkiewicz): Results lose all sensation
Voluntary movement inferior to the level of impaired blood supply to the spinal cord (paraplegia).
Degeneration of neurons in the part of the spinal cord supplied by the anterior spinal artery.

Ischemia of the Spinal Cord
When systemic blood pressure drops severely for 3-6 min, blood flow from the segmental medullary arteries to the anterior spinal artery supplying the midthoracic region of the spinal cord may be reduced or stopped.
Patient may also lose sensation and voluntary movement in the areas supplied by the affected level of the spinal cord.

Thank you