1 interesting cases orthopedic grand rounds interesting cases nov8/2002 abdul aziz al-ahaideb
Post on 21-Dec-2015
216 views
TRANSCRIPT

1
Orthopedic Grand Rounds interesting casesinteresting cases
Nov8/2002Abdulaziz Al-Ahaideb

2
History
11 year- old girl complains of left hip painStarted end of June 2002.
?
3
History
Pain is mainly at the medial side of the left hip. Has not improved and she started to limp.
Pain is increased by motion and relieved by rest
There is a history of a fall at school after which the mother thought the pain started.
No history of fever or chills
4
History
No history of rashes She complains of no other joint
symptomatology. She could not participate in sports secondary
to pain and also developed a limp with apparent leg length discrepancy
Her past medical history is negative. Not on meds NKDA
5
History
She was seen by GP and x-rays were done and told there was no fracture.
Pain got worse. Referred to a pediatric orthopedic surgeon.
6
Physical Examination

7
Physical Examination
She was a febrile on presentation to the UAH and was looking well

8
Left hip : Pain on range of motion
limitation of abduction and flexion
9
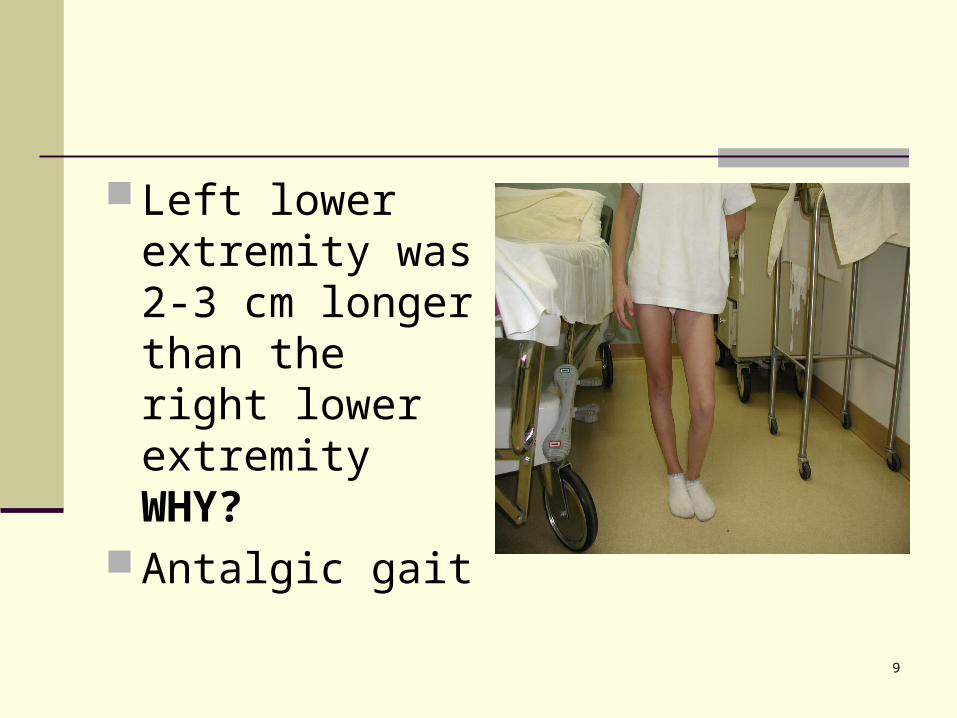
Left lower extremity was 2-3 cm longer than the right lower extremity WHY?
Antalgic gait

10
What is the differential diagnosis ?
Perthes disease
Septic arthritis
SCFE
Fracture
Juvenile rheumatoid arthritis

11
Investigations
X-rays: AP

12
Investigations
Lateral view

13
Investigations
Blood work:
CBC & diff : WNL
ESR 16 CRP 1.8

14
WHAT TO DO ?
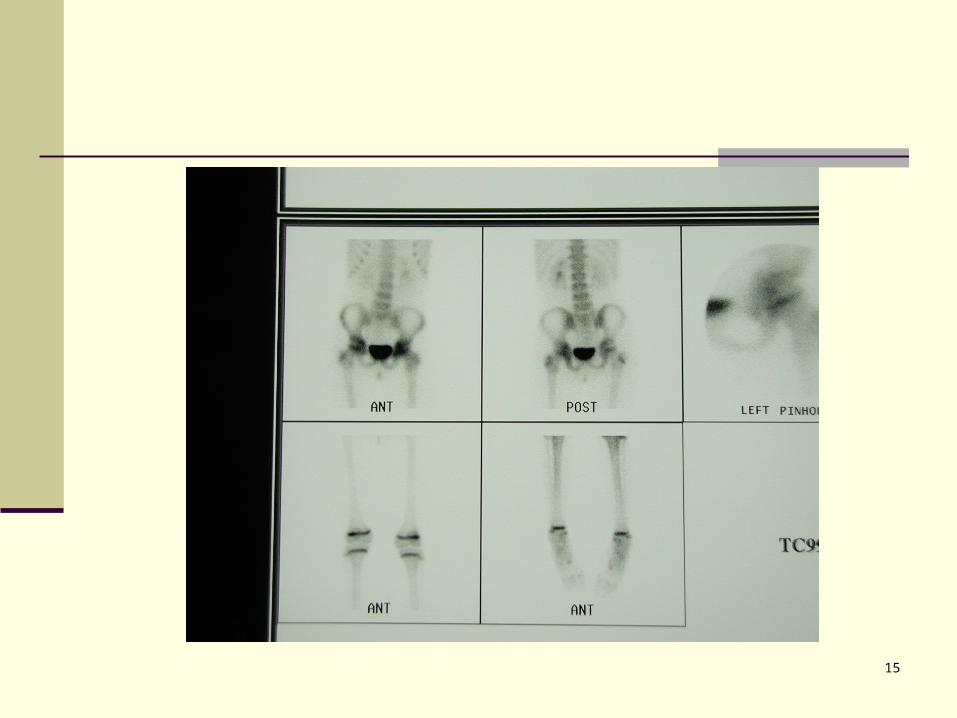
15

16
Bone scan: increased uptake in the Lt hip

17
Now what ?Now what ?

18
MRI
19
What is the most likely diagnosis ?

20
Management done:
Physiotherapy for ROM esp. abduction PWB with crutches Rheumatology consult NSAIDs F/U 2 wks

21
The rheumatologist agrees with our diagnosis
The mother thinks her daughter didn’t improve with physiotherapy

22
IDIOPATHIC CHONDROLYSIS
23
INTRODUCTION
Chondrolysis represents a process characterized by progressive destruction of articular cartilage resulting in secondary joint space narrowing and stiffness.
Types: May follow infection, trauma, prolonged immobilization and severe burns about the lower extremities. Also, it may be a complication of slipped capital femoral epiphysis.
Another type is idiopathic, characterized by an acute form of rapidly progressive chondrolysis occurring most frequently during adolescence with isolated involvement of the hip joint, but without a demonstrable cause.
24
Historical Review
Jones in 1971 described chondrolysis not associated with SCFE or infection in 9 adolescent black African girls.
Since that time, reports of idiopathic chondrolysis have been recorded in different races.
The female to male ratio is 6:1 and 52% of these patients are Caucasian

25
ETIOLOGY
Etiology is unknown. Proposed theories include:
nutritional abnormalities mechanical injury, ischemia, abnormal intracapsular pressure, and an inherent abnormal chondrocyte
metabolism within the articular cartilage.

26
The most accepted theory is that proposed by Golding in 1973 (JBJS-Br), which postulated articular cartilage resorption to be secondary to an autoimmune response in genetically susceptible individuals.
27
INCIDENCE
This remains unreported in the literature, although 42 have been reported up to 1989. (Incidence of chondrolysis in SCFE is 8.2%).

28
CLINICAL PRESENTATION
Adolescent girl average of 12.5 years. Right hip slightly higher than left hip Insidious onset of pain in anterior or medial
side of affected hip associated with joint stiffness and limp.
Patient is afebrile Restriction of motion in all planes with
associated muscle spasm Contracture about the joint; most commonly,
fixed flexion, abduction and external rotation

29
BLOOD WORK
CBC, UA, RF, ANA, HCA-B27, Blood culture, and TB (PPD) are WNL.
ESR can be slightly elevated and rarely over 30.
30
RADIOGRAPHS
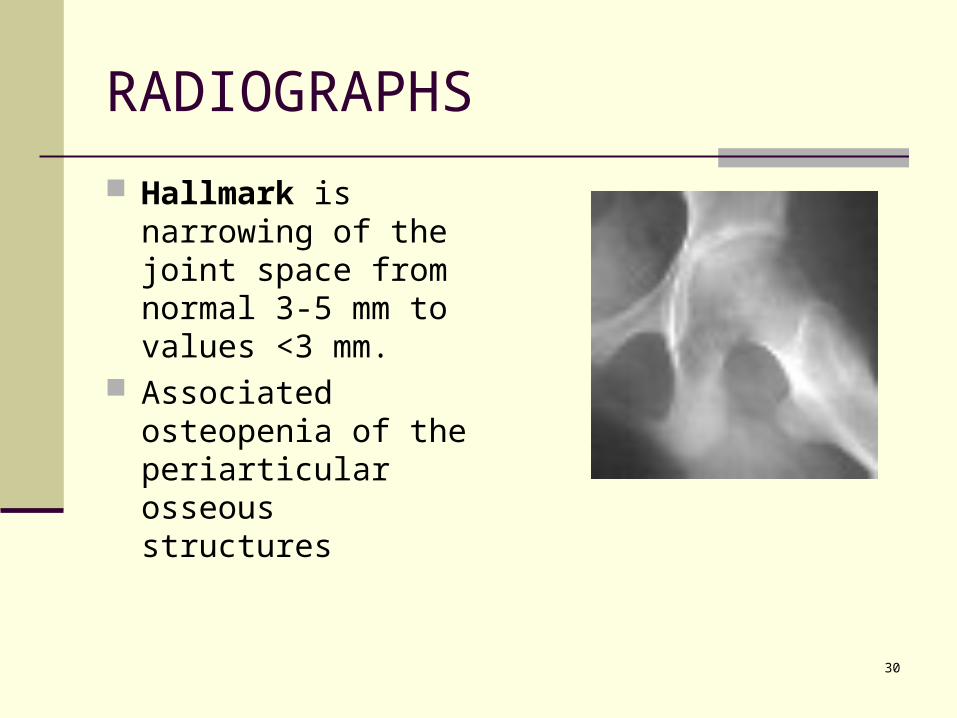
Hallmark is narrowing of the joint space from normal 3-5 mm to values <3 mm.
Associated osteopenia of the periarticular osseous structures

31
RADIOGRAPHS
Irregular blurring of subchondral sclerotic lines With time, can develop mild coxa magna and femoral
neck widening and frequently a premature closure of the proximal femoral physis and trochanteric apophysis.
Mild protrusion and a lateral buttressing osteophyte at the acetabulum
Limited area of periosteal new bone formation along inferior femoral neck

32
The complex of symptoms and radiographic findings is so characteristic that idiopathic chondrolysis should not be a diagnosis if exclusion.

33
OTHER INVESTIGATIONS
Arthrography - help document cartilage resorption and joint space narrowing
Bone scan shows increased uptake on both sides of joint
CT Pelvis - document subchondral bone changes, cartilage resorption, and narrowing of joint space
MRI - may be of benefit, but there is no large volume of experience using MRI found in the literature
These modalities are mainly used to rule out other diagnoses.
34
PATHOLOGY
Capsule is routinely thickened Irregular thinning, fibrillation and
fragmentation of the cartilage Microscopic review of biopsy of synovium
demonstrates nonspecific chronic inflammation

35
DIFFERENTIAL DIAGNOSIS
Infectious arthritis including TB: Will see increased CBC, ESR, Temp, and positive PPD.
JRA: There is an extended period of time with symptoms prior to chondrolysis. Rarely see restrictions in range of motion as that seen with Idiopathic Chondrolysis.
Seronegative spondyloarthropathy: You will see additional joint involvement and the HLAB-27 will be positive.
PVNS: Has a more chronic and prolonged course. Usual findings include cystic erosions in subchondral bone and a bloody aspirate.
36
Natural History
Not well known It appears to have two stages:
Acute: lasts 6-16 months. Inflammatory response within the affected hip leading to a painful hip with a decrease of ROM and loss of articular cartilage
37
Chronic: may last for 3-5 yrs. 3 possible outcomes
1. deterioration to a painful and malpositioned ankylosis
2. the hip becomes painlessly ankylosed with some limitation of motion
3. the hip may have a resolution of pain with partial or complete return of motion and improved joint space width shown on radiographs

38
MANAGEMENT
therapeutic doses of NSAIDS Aggressive physiotherapy for ROM Periodic traction and bedrest Prolonged non-weight bearing or partial
weight bearing
39
Several small series reported improvement following partial capsulectomy and soft tissue release followed by traction and aggressive rehabilitation.
However, more recent long follow up showed no significant difference in pain, ROM, or radiographic appearance, when comparing surgically treated hips to non-surgically treated hips.

40

41
The second case

42
3 year-old child had a month-long history of pain in his left thigh, and x-rays showed a benign-appearing lytic lesion. A bone scan showed that this was an isolated lesion and had very minimal uptake.
The patient was taken to OR on June 11/ 98 for excisional biopsy and insertion of Osteoset pellets

43
Intra-operatively a window was made and fluid-filled cavity was encountered.
There was only minimal lining and a portion of this was sent for culture and pathologic examination.
He was placed in a hip spica for four weeks

44

45
Pathology confirmed the diagnosis as Unicameral bone cyst
The patient was lost to follow up and came recently after having pain in his left hip

46

47
What should be done ?

48
What are the risks ?

49
The patient was taken to the OR on May 15/02
Currettage was done through a window made in the lateral cortex
5 ml of bone marrow was aspirated from the iliac crest and mixed with Osteosets and packed into the defect
50
Prophylactic internal fixation of left intertrochanteric region was done utilizing 130 degree four hole blade plate
The blade plate was carefully introduced up the femur and gently advanced until it was in the epiphysis.
Position was confirmed with fluoroscopy

51
Intra-op fluoro
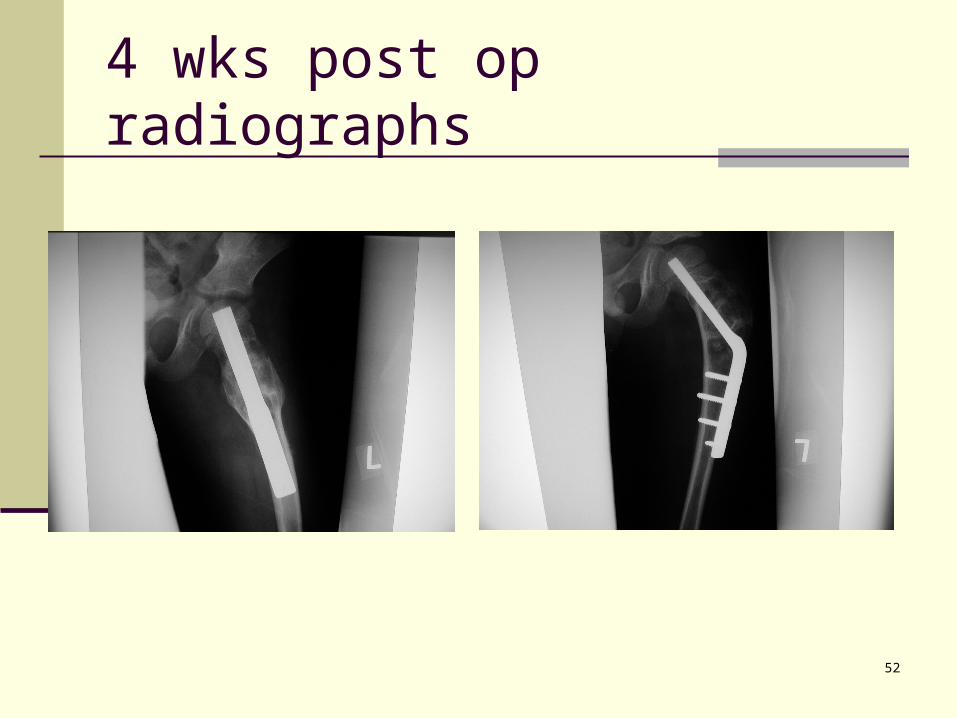
52
4 wks post op radiographs

53
Unicameral bone cyst ( UBC)
a membrane lined cavity containing a clear yellow fluid, occurs most often in children 4-10 years of age
they enlarge during skeletal growth and become inactive, or latent, after skeletal maturity

54
They are generally seen in the metaphyseal areas of long bones in skeletally immature persons.
The etiology of these lesions, which represent about 3% of biopsied bone tumors, is unknown

55
The commonest sites are the proximal humerus (50 %) and proximal femur (40 %)
The fluid within the cyst has been analyzed and shown to contain high levels of oxygen-radicals and prostaglandins which cause bone resorption and may play a role on the formation and growth of the cysts

56
Pathophysiology
The most recent research supports the theory that a vascular occlusion phenomenon occurs within the cyst. The pressures within a cyst are elevated above venous pressures.

57
Clinical presentation
The lesions are painless and rarely symptomatic. The diagnosis is often made incidentally when a radiograph is made for other purposes. A common presentation is with pathologic fracture which has been estimated to occur in 30 to 40 percent of the recognized lesions.
58
DDx
ABC
Fibrous dysplasia
Enchondroma
Osteosarcoma
Infection
59
Treatment
Is only indicated if the cyst is symptomatic or there is a pathological fracture
Surgical treatment remains controversial. Interpretation of the reported clinical series
presents a dilemma because it is virtually impossible to ascertain whether the cysts in these studies were active, latent, or involutional when they were treated.

60
Treatment
The consensus is that the surgeon should wait and allow the cyst to heal before proceeding with treatment.
By waiting, internal fixation can usually be avoided.
The exception is when the fracture is in a high-stress weight-bearing area, such as the femur

61
Surgical modalities
Steroid injections 80-200 mg of methylprednisolone are injected
into the cavity using two needles technique, Done every 6-8 wks JBJS 1997 Hashimi et al , 32 patients with
UBC received multiple intralesional steroid injections: earliest time to healing was 3 months
62
autologous bone marrow injection JBJS 96 F Lokiec et al 10 children with simple bone cysts in the
proximal humerus, proximal femur or tibia Treated by the injection of autogenous bone
marrow aspirated from the iliac crest All the patients became pain free after a mean
of two weeks and resumed full activities within six weeks. All ten cysts consolidated radiologically and showed remodeling within four months. Review at 12 to 48 months showed satisfactory healing without complications

63
Open curettage and packing with a bone graft or substitute:
In published series, the recurrence rate may be as high as 45 %
The choice of autologous bone graft or substitute is dependent on the orthopedic surgeon’s preference
DBM can be injected percutaneously into the cysts

64
Injecting normal saline into the cyst Drill holes into the cyst In small cysts in the intertrochanteric hip,
cannulated screws can be used to drain the cyst.
In the proximal femur prophylactic internal fixation is advocated
65
Thank You