1 the physical examination of heart 1 st affiliated hospital liaoning medical college he xin
TRANSCRIPT
1
The Physical Examination
of Heart
1st Affiliated Hospital Liaoning Medical College
He Xin
2
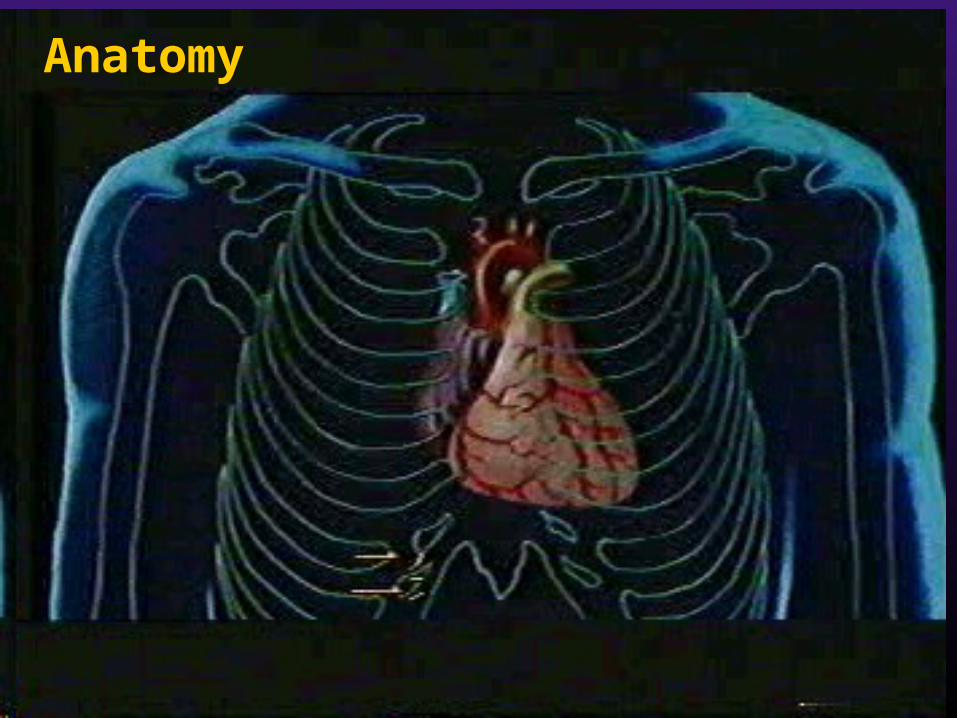
Anatomy
3
一、 Inspection with tangential lighting
1 、 Thoracic deformity
2 、 Apical impulse
3 、 Abnormal pulsations of precardium
4
1 、 Thoracic deformity---protrusion of precordium
--Right ventricular hypertrophy (L3-5)
congenital heart disease( tetralogy of Fallot)
valvular heart disease( MS,PS)
--pericardial effusion (large , childhood)
--The second right intercostal space (2nd ICS-RS)
aneurysm of aortic arch
dilatation of ascending aorta
---flat chest
---pigeon chest/ funnel chest
5
2 Apical impulse---Normal --Position : in the left fifth intercostal space about
0.5-1.0cm medial from the midclavicular line --Range: no larger than 2.0-2.5cm in diameter
6
( 1 ) Location Posture Diaphragm Mediastinum Enlargement of the heart Dextrocardia( 右位心 ): 5-ICS—RS
---Abnormal
7
Posture: ---Recumbent( 仰 ) position—upper ---left lateral( 侧 ) position—to the left 2-3cm ---right lateral position—to the right 1.0-2.5cm
8
Diaphragm: ---“transverse position” upper,outward obesity ,child, pregnacy ascites; tumor of abdominal cavity ---“vertical position” inferior,inner thin, high, emphysema
9
mediastinum: • one side pleural effusion or pneumothorax ---to the healthy side • one side atelectasis or pleural adhesion ---to the affected side
10
Enlargement of the heart • right ventricular dilatation – displaced
to the left or slightly upper • left ventricular dilatation— displaced to
the left inferior • LV &RV dilatation –left inferior (both
side dilatation)
11
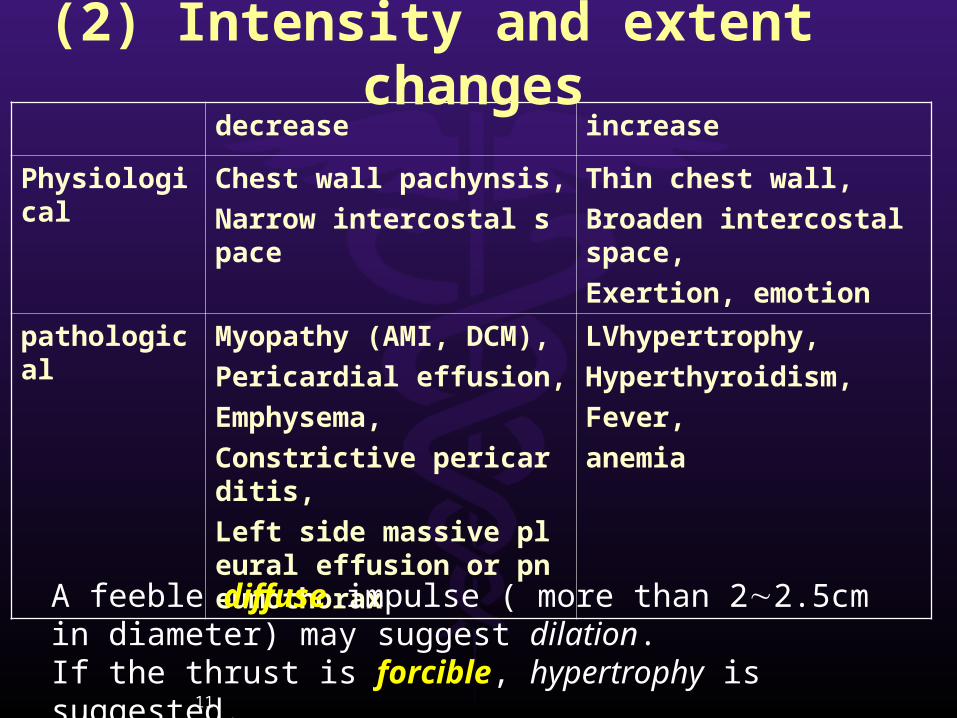
decrease increase
Physiological Chest wall pachynsis,
Narrow intercostal space
Thin chest wall,
Broaden intercostal space,
Exertion, emotion
pathological Myopathy (AMI, DCM),
Pericardial effusion,
Emphysema,
Constrictive pericarditis,
Left side massive pleural effusion or pneumothorax
LVhypertrophy,
Hyperthyroidism,
Fever,
anemia
(2) Intensity and extent changes
A feeble diffuse impulse ( more than 22.5cm in diameter) may suggest dilation. If the thrust is forcible, hypertrophy is suggested.
12
(3)Inward impulse( 负性心尖搏动 ): apex excavation in the systole
--adhesive pericarditis --prominent RV hypertrophy
13
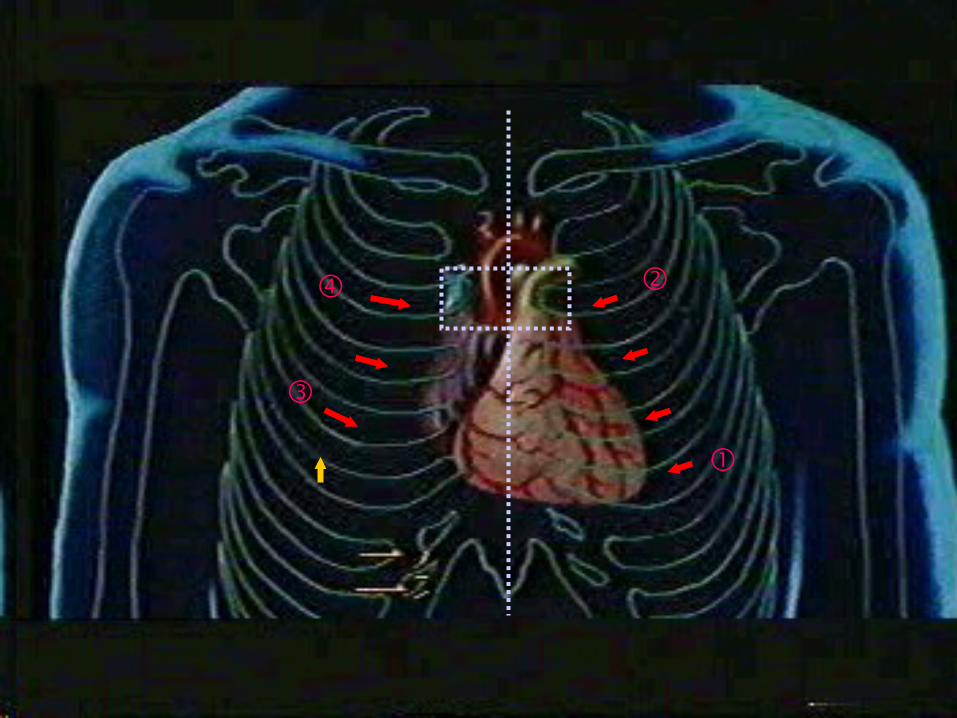
(1)left third-forth intercostal space lateral to the sternum (3,4ICS-LS)
---RV hypertrophy(2)xiphoid process
---RV hypertrophy ---Abdominal aorta (aneurysm) (The pulsation of the abdominal aorta may often be felt in the epig
astric area. Also, the impulse from right ventricle can be felt by the fingertips placed under the xiphoid process while inspiration.)
3 、 Abnomal pulsations of percardium
14
(3)basal part of the heart ---2 ICS-LS: dilatation of the pulmonary arter
y or pulmonary hypertensin, occasionally healthy young man
---2 ICS-RS: aneurysm of aortic arch or dilatation of ascending aorta
3 、 Abnomal pulsations of percardium
15
二、 Palpation
1 Apical impulse and pulsation of precardium
2 Thrill
3 Pericardial friction rub
16
1 、 Apical impulse and pulsation of precardium
---Exact position of apex
---The beginning of systole of ventricle
first sound
---Heaving apex impulse: reliable of LV
hypertrophy
17
2 、 Thrill---Mechanism : the flow of blood→narrowed
orifice→vortices→vibration→chest wall
---One of characteristic signs of organic heart
disease : CHD or valvular stenosis, occasionally
insurficiency
---thrill - high frequency
murmurs - low frequency
---Key point: position, phase of cardiac cycle,
clinical significance
18
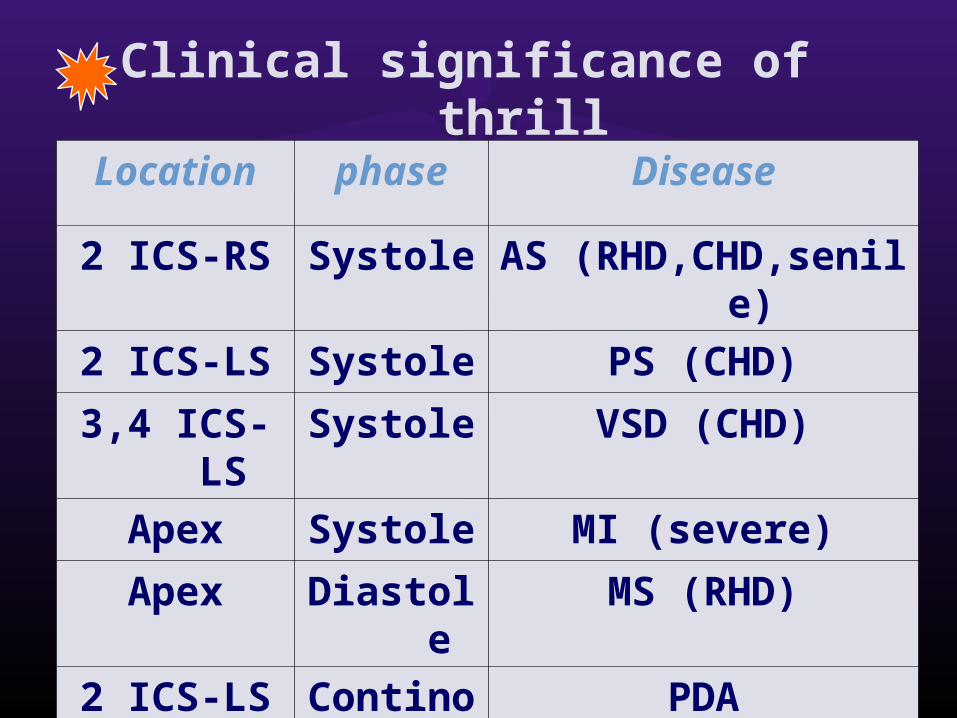
Clinical significance of thrill
Location phase Disease
2 ICS-RS Systole AS (RHD,CHD,senile)
2 ICS-LS Systole PS (CHD)
3,4 ICS-LS Systole VSD (CHD)
Apex Systole MI (severe)
Apex Diastole MS (RHD)
2 ICS-LS Continous PDA
19
3 、 Pericardil friction rub---Precardium -4th ICS-LS
---both phases of the cardiac cycle
---systolic period, sitting erect and leaning
forward, the end of expiration
---mechanism: rub of the visceral and
parietal layers of pleura
---seen: acute pericarditis

20
三、 Percussion ---Aim: to determine the size and shape of the heart ---Absolute dullness: contain no gas
Relative dullness : real size
21
1 、 maneuver of percussion ---patient in erect position
–the pleximeter is vertical with the intercostal space
---patient in the recumbent position
–the pleximeter is parallel with the intercostal space
22
2 、 order :---left—right ; upwards ; inward
---left margin : from 2-3 cm lateral to
the apex beat up to the 2nd ICS
---right margin : one intercostal space
higher than the border of liver dullness
up to the 2nd ICS
---size: vertical distance from margin to
the anterior midline
23
Percussion of cardiac dullness border starts tothe left on the chest, from 23cm apart from theapical impulse towards cardiac dullness (relativecardiac dullness). Percussion is performed fromleft towards cardiac dullness in the 4th, 3rd and2nd intercostal spaces. Next, to the right of thechest, percussion is done in the midclavicularline down to a dull point (the upper margin ofliver). Then, percuss from right towards cardiacdullness in the 4th (above the liver dullness), 3rd,and 2nd intercostal spaces.
24
一. Measure the vertical distances from each point of cardiac dullness to the mid-sternal line with a stiff ruler
二. When the left border of cardiac dullness falls outside the midclavicular line, it usually indicates that the left ventricle is enlarged
三. If the left border of cardiac dullness goes out of left midclavicular line (the left cardiac border towards left in the 5th intercostal space), it suggests that the right ventricle enlarged
四. The cardiac dullness enlarged towards two sides: (1)both left and right ventricles enlarged, (2) a large volume of fluid in the cavity of pericardium. In this case, the cardiac borders will be changed following the change of the patient's position
25
①
③
②④

26
Right(cm) ICS Left(cm)
SVC,SA 2~3
Ⅱ 2~3 PA
RA 2~3 III 3.5~4.5 LA
RA 3~4 Ⅳ 5~6 LV
Ⅴ 7~9 LV
3 、 Normal heart borders (area of relative dullness)
27
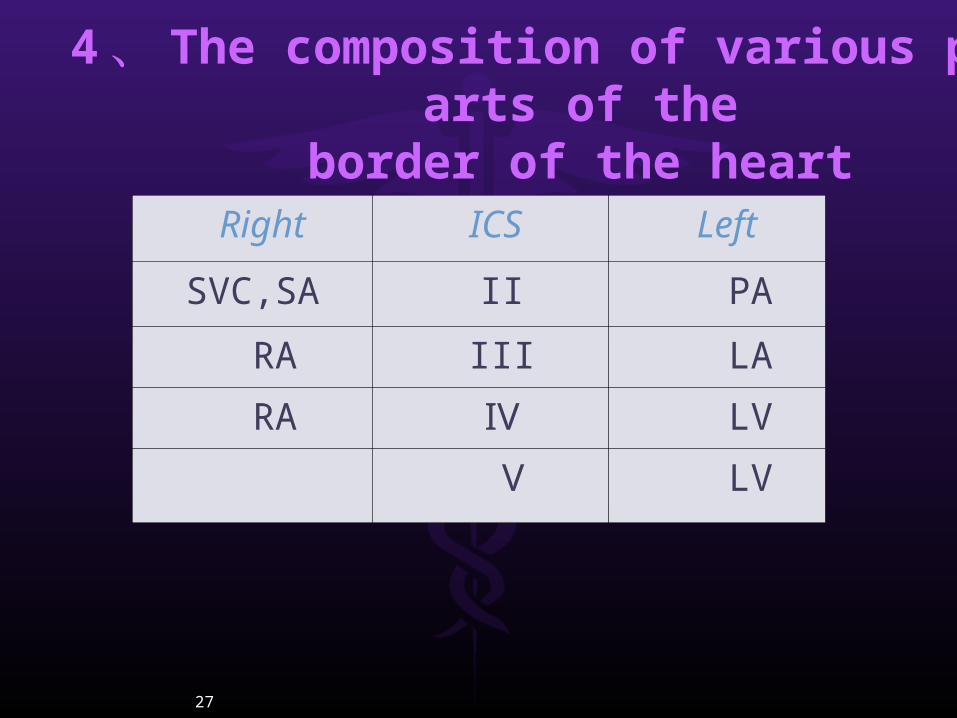
Right ICS Left
SVC,SA II PA
RA III LA
RA Ⅳ LV
Ⅴ LV
4 、 The composition of various parts of theborder of the heart
28
---The upper border –the lower border of the anterior end of the third rib↑---The basal part —the second intercostal space upward left: aortic node and PA---Concave part –between the aorta and the left ventricle
29
( 1 ) body’s position: 1) recumbent position : widening of base
of the heart 2) erect position:“triangular shape”
5 、 Changes in the area of cardiac dullness and its significance
30
( 2 ) Cardiac factors :
1)LV enlargement: “boot shape” Seen:aortic valvular disease ,
hypertension heart disease2)RV enlargement :
slightly↑--absolute dullness↑ Prominent↑--relative dullness↑ to the left side prominently Seen:PHD, MS
31
3)Two ventricle ↑:
“generally enlarged heart”
seen:DCM , Kashan cardiomyopathy
4)LA and/or pulmonary artery:
“pear shape”
LA:concave part disappear
LA+PA:2,3 ICS-LS outwards
Seen: MS--- “mitrial type”
32
5)pericardial effusion:
enlargement of both sides of the border
6)dilatation of the aorta /ascending aortic
aneurysm:
widening if the dull area of first and
second intercostal space (with systolic
pulsation)
33
( 3 ) Extacardial factors :1)large pleural effusions and pneumothorax → to the healthy side2)atelectasis /pleural pachynsis →to the affected3)a large amount of ascites or big abdominal tumor:
diaphragm elevated→transverse position →left side enlargement
34
四、 Auscultation
1 、 Cardiac valve areas for precordial
auscultation
2 、 Order
3 、 Contents
35
1 、 cardiac valve areas forprecordial auscultation
1)ausclutatory mitral area: apical area
2)auscultatory pulmonary area:2 ICS-LS
3)ausclutatory aortic area: 2 ICS-RS
4)second ausclutatory aortic area: 3rd ICS
LS—Erb area
5)tricuspid area :4,5 ICS-LS
36
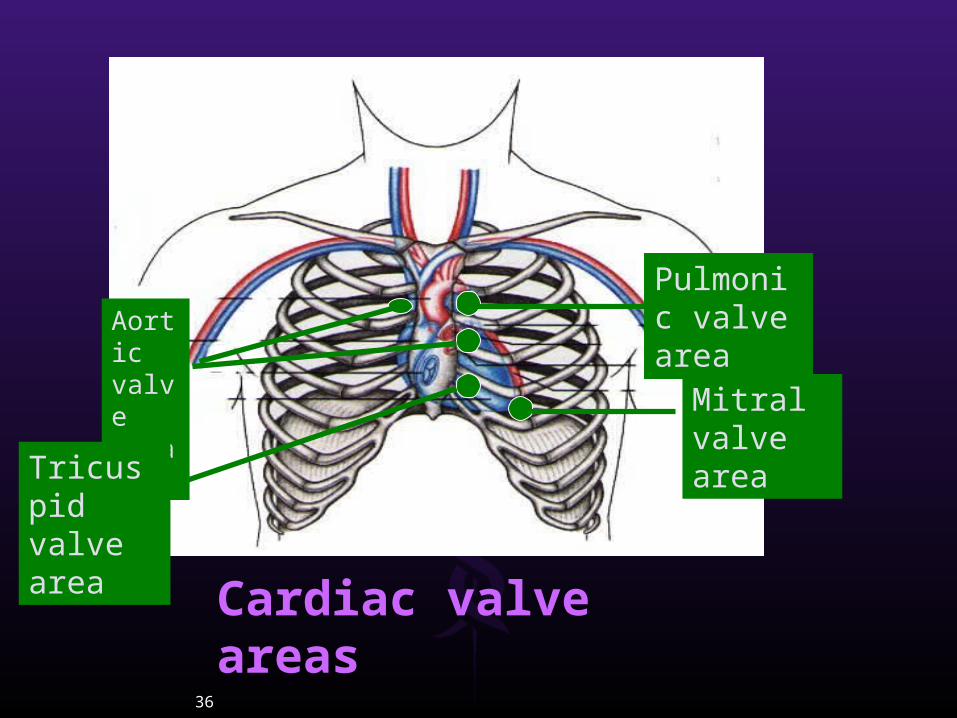
Aortic valve areas
Tricuspid valve area
Pulmonic valve area
Mitral valve area
Cardiac valve areas
37
2 、 Order: Apical area Pulmonary valve area
Aortic valve area 2 nd aortic valve area Tricuspid valve area
MV---PV---AV1---AV2---TV
38
3 、 Contents :
1) rate
2)rhythm
3)heart sound
4)extra heart sound
5)murmurs
6)pericardial friction sound
39
(1)heart rate
Normal heart rate is 60-100/min (adult)
above 100/min (below 3 years old)
Tarchycardia : above 100/min (adult)
above 150/min (infant)
Bradycardia: below 60/min
40
(2)cardiac rhythm:
sinus arrythmia—affected by breath
premature beat—frequently: > 6 bpm
occasionally: < 6 bpm
atrial fibrillation: —absolute irregular rhythm S1 intensity inequality Pulse deficit
41
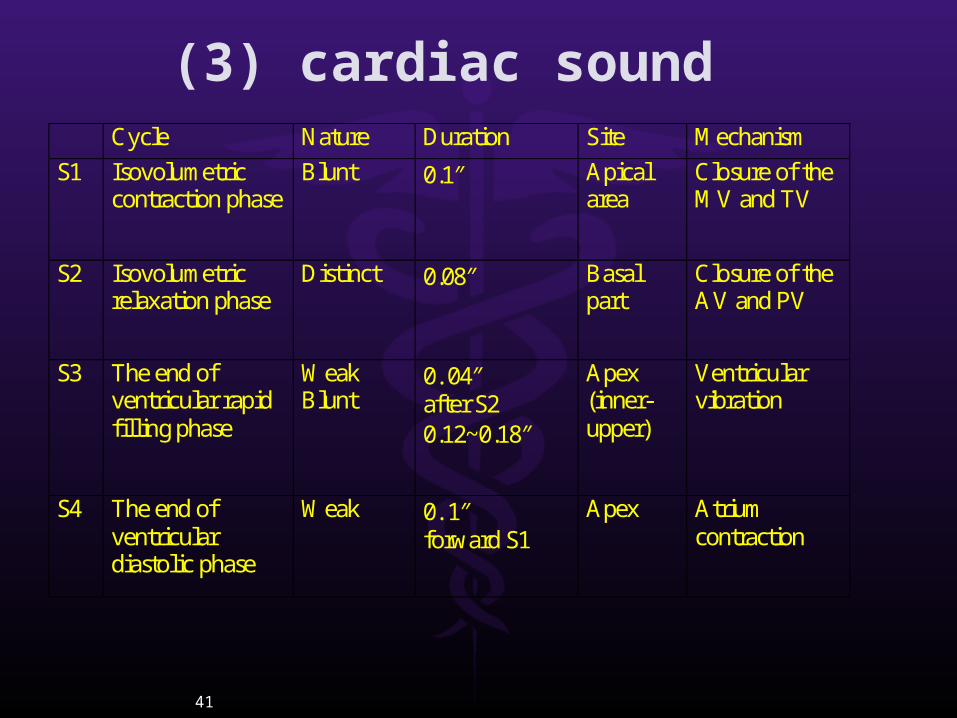
(3) cardiac sound Cycle Nature Duration Site Mechanism
S1 Isovolumetric contraction phase
Blunt 0.1″ Apical area
Closure of the MV and TV
S2 Isovolumetric relaxation phase
Distinct 0.08″ Basal part
Closure of the AV and PV
S3 The end of ventricular rapid filling phase
Weak Blunt
0. 04″ after S2 0.12~0.18″
Apex (inner-upper)
Ventricular vibration
S4 The end of ventricular diastolic phase
Weak 0. 1″ forward S1
Apex Atrium contraction
42
(4)Abnormal cardiac sound 1)Intensity:
cardiac sound is influenced by a number of factor
---position of the atrioventricular valve
---Ventricular contractility and output
---Valvular integrity and activity
43
S1 Accentuation: ---MS
---HR↑contractility↑
fever,anemia,hyperthyroidism
---complete AVB →cannon sound
44
S1 attenuation : ---MI ---P-R interval enlong ---AI ---myocarditis,myopathy,MI,HFS1 inequality: ---AF ---III°-AVB
45
S2---A2+P2
S2 ↑ ---pressure and flow of blood ↑ A2 : hypertensin, arterisclerosis P2 : PHD,CoHD(L--R),LVF
S2 ↓ ---pressure↓ flow ↓
Seen:hypotension,AS/AL,PS/PI
46
2)Quality
mono rhythm
pendular rhythm---embryocardia
47
3)Splitting of heart sound
S1 splitting:
seen—RBBB, right heart failure Ebetein malformation ,MS LA myxoma
48
S2 splitting:
physiological splitting :end of inspiration
general splitting : most commonly seen: CRBBB, PS, MS,MI ,VSD
fixed splitting :ASD
paradoxical splitting(reversed splitting) : pathologicalseen: CLBBB ,AS, hypertension
49
(5)extra cardiac sound 1)Diastolic period
①gallop rhythm:
--protodiastolic gallop: S1+S2+S3 the third
sound gallop (sign of organic heart disease) seen : HF ( AMI, severe myocarditis , myopathy )
-- late diastolic gallop: atrial gallop S1+S2+S4 seen : HBP ,HCM ,AS ,CHD
-- summation gallop: quadruple rhythm
seen:HF,cardiomyopathy
50
②opening snap :MS
③pericardial knock: constrictive
pericarditis
④tumor plop: LA myxoma
51
2)Systolic period
①early systolic ejection sound(click) ---pulmonary :pulmonary hypertension;
pulmonary artery dilatation , PS, ASD,
VSD
---Aortic: hypertension, aneurysm ,
AS, AI ,aorta constriction
②mid and late systolic click: S1----mid < 0.08″ late > 0.08″
seen: mitral prolapse
52
3)iatrogenic
① prosthetic valvular sound
② pacemaker
53
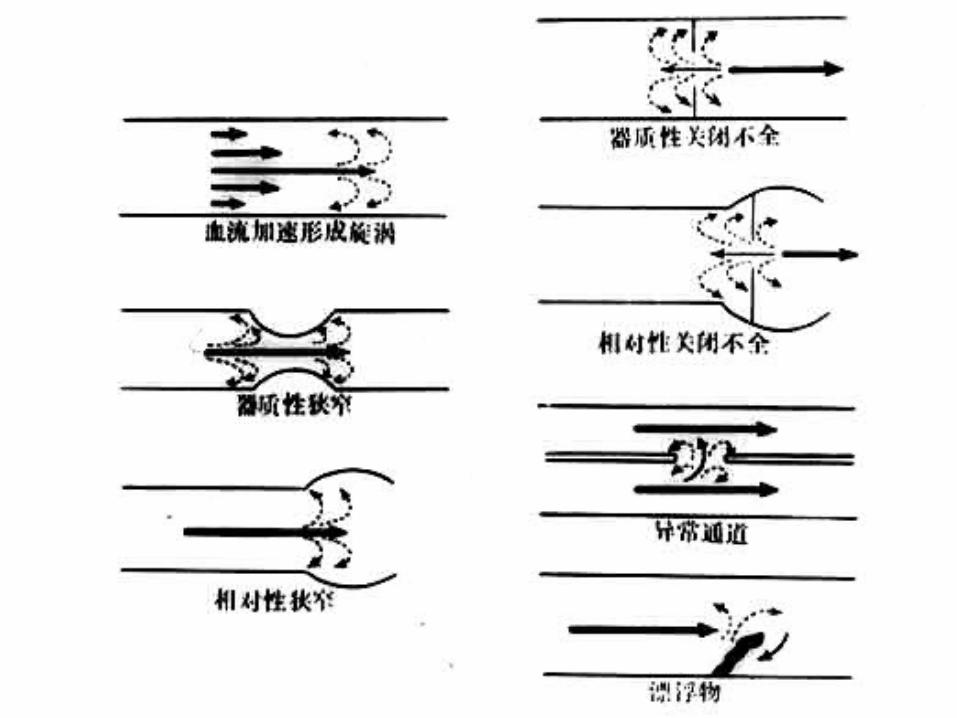
1 ) Mechanism ---acceleration of blood flow --- Blood viscosity --- Valve: narrowed or incompetent; organic or relative ---abnormal passage ---foreign body ---dilatation of vessles(aneurysm)
( 6 ) Cardiac murmurs

54
55
56
2 ) characterization of murmur and
ausclutatory key points
①Location and Transmission
②Timing
③Quality
④Intensity
⑤Effect of position, respiration and exercise
on intensity of murmurs

57
①Location and Transmission ---location: where it is audible most significantly
L3,4 –VSD L2,3—PDA ---transmission: which direction it come from MI ---left axilla AS---neck
58
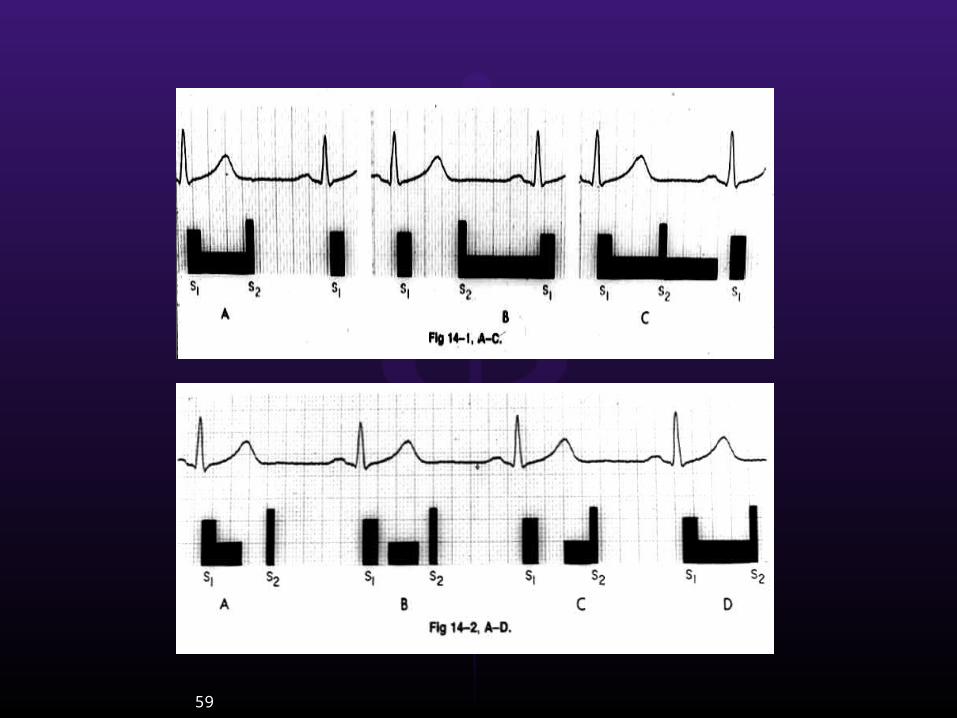
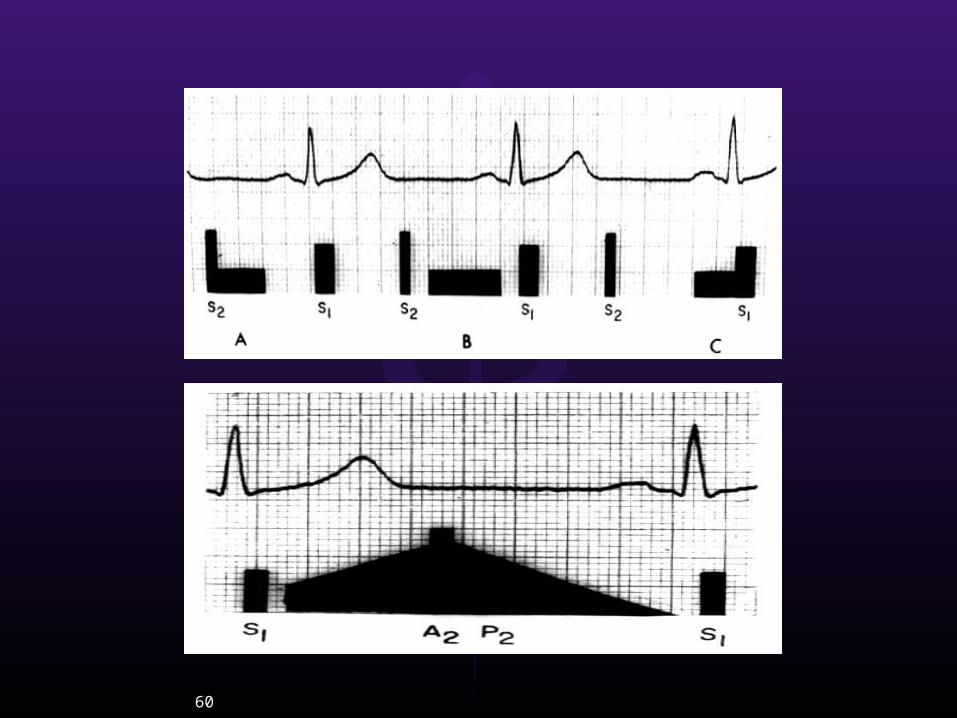
②Timing---Murmurs are timed according to the phase of cardiac cycle during which they occur.---SM, DM , CM.---Early, middle, late
59
60
61
③Quality ---Depend on: frequency and intensity of so
und wave ---Related to: pathology and hemodynamic changes of the heart---Soft , harsh, musical.---SM: blowing, harsh, musical (seagull)---DM: blowing, sigh-like, rumbling. ---CM: machine-like, hum

62
④IntensitySix-point scale of for grading the intensity ofheart murmur
Grade Ⅰ: basely audible Grade Ⅱ: usually readily heardGrade Ⅲ: loudGrade Ⅳ: quite loudGrade Ⅴ: even most pronounced Grade Ⅵ: can be heard with thestethoscope removed from the chest wall
63
⑤Effect of position, respiration and exercise on intensity of murmurs ---body position:
MS--left lateral positionAI--sitting erected and forward MI,TI,PVS--lie on one’ back Lie → stand: HCM
---breath: expiration--LV murmurs inspiration --RV murmurs valsalva--HCM ---exercise: HR↑murmurs ↑
64
3 ) The clinical value of heart murmur
① systolic murmurs
② Diastolic murmurs ③continuous murmurs
65
① systolic murmursMitral valve area : functional:exercise,fev
er,anemia,pregnancy,hyperthyroidism
Soft, blowing SM, Grade II/VI well localized wethout transmission. S1 normal.
66
① systolic murmursMitral valve area : relative:HBP,CHD,DCM,anemia
Dilatation of LV and mitral valve relative insufficiency
---blowing SM
---Grade II-III/VI with or without transmission
---S1 usually normal.
67
① systolic murmursMitral valve area : organic : MI(RHD),mitral prolapse
Pansystolic murmur, blowing or harsh, Grade III/VI or more, transmited toward axilla or left back, S1 masked, the SM can be intensified by lying on left lateral position.
68
① systolic murmursAortic valve areas :Organic : aortic stenosis
---harsh ejection SM
---Grade III-IV/VI, often accompanied by a thrill
---crescendo-decrescendo type (diamond shaped)
---transmitted toward neck and apex
---A2 diminished or absent
69
① systolic murmursAortic valve areas :Functional : due to relative aorticstenosis
( dilatation of aorta , severe
hypertension atherosclerosis of aorta)
---Soft
---A2 accentuated
70
① systolic murmursPulmonary valve areas :Physiology : (children)
---Soft blowing SM
---Grade II/VI
---shorter

71
① systolic murmursPulmonary valve areas :relative : MS 、 ASD Dilatation of pulmonary artery ( pulmonary hypertension or large outflow from RV) ---Soft blowing SM ---Grade II/VI,well location ---Shorter ---P2 accentuated
72
① systolic murmursPulmonary valve areas :organic : pulmonary stenosis
---harsh ejection SM,
---Grade III-IV/VI, often accompanied
by a thrill
---crescendo-decrescendo type
(diamond shaped)
---P2 diminished or absent.
73
① systolic murmursTricuspid valve areas :relative : RV enlarged ---Soft blowing SM ---Grade III/VIorganic : rare
other location: 3-4nd I.c.s left to sternum (VSD,ventricular septal defect) ---Loud, harsh SM, ejection ---accompanied by a thrill

74
② Diastolic murmursmitral valve area
Organic : rheumatic mitral stenosis
---S1 loud and snappy OS audible
---well localized to the apex
---rumbling in quality in middle-late
of diastole crescendo characte
---In many instances, it is
accompanied by a thrill.
75
② Diastolic murmurs
mitral valve arearelative MS : Austin Flint murmur: In severe aorti
c insufficiency, reduced overload of left ventricular in diastolic there may be heard a rumbling DM over the apex which can be distinguished from the organic MS by following points
--- not accompanied by a loud snappy S1 , or a thrill
---(There are unequivocal fingings compatible with AR,i.e.blowing DM of AR over aortic valve areas , lift ventricular enlargement, peripheral vascular signs
76
② Diastolic murmurs
Aortic valve areas. aortic insurfficiency
---decrescendo, sighing DM
---best heard in sitting position, leaning
forward,holding breath in expiration
---transmitted downward along both sides of
sternum
---A2 diminished
---In cases of severe degree of AR, there may be
present: DM (Austin Flint) over apex and peripheral
vascular signs
77
② Diastolic murmurs
pulmonary valve areas Relative : Graham Steel murmur:dilate of
pulmonary artery relative pulmonary
insufficiency
---decrescendo
---Blowing,soft
---P2 accentuated
---Seen in mitral stenosis
78
③continuous murmurs
PDA (patent ducuts arteriosus)
---Continuous murmur PDA, characteristic murmur of PDA is a comtinuous , machinary murmur
---at 2 nd i.c.s. Left to sternum
---with an accentuated P2
---A systolic thrill may be present
79
---both phases , unaffected by
respiration
---seen: pericarditis
RHD ,AMI ,renal failure
( 7 ) pericardial friction sound
80
THANK YOU !