18 3416 gentili.qxp annali 102
TRANSCRIPT
452 Ann. Ital. Chir., 92, 4, 2021
Comparison of indocyanine green fluorescencelymphangiography and magnetic resonancelymphangiography to investigate lymphedema of the extremities
Ann. Ital. Chir., 2021 92, 4: 452-459pii: S0003469X21034163
Pervenuto in Redazione Luglio 2020. Accettato per la pubblicazioneSettembre 2020Correspondence to: Francesco Gentili, Section of Radiology, Unit ofSurgical Sciences, Department of Medicine and Surgery, University ofParma, 43126 Parma, Italy (e-mail: [email protected])
Francesco Gentili*, Francesco Giuseppe Mazzei*, Ilaria Monteleone**, Guido Gabriele***,Andrea Nigri****, Federico Zerini***, Michael Gasser Aboud***, Maria Antonietta Mazzei**, Paolo Gennaro***
*Unit of Diagnostic Imaging, Azienda Ospedaliera Universitaria Senese, Siena, Italy**Department of Medicine, Surgery and Neuro Sciences, Unit of Diagnostic Imaging, Azienda Ospedaliera Universitaria Senese,University of Siena, Siena, Italy. ***Department of Medical Biotechnology, Unit of Maxillofacial Surgery, Azienda Ospedaliera Universitaria Senese, University of Siena,Siena, Italy****Faculty of Statistics, “Sapienza” University of Rome, Rome, Italy
Comparison of indocyanine green fluorescence lymphangiography and magnetic resonance lymphan-giography to investigate lymphedema of the extremities
PURPOSE: The aim of this study is to compare two dynamic imaging modalities employed to study peripheral lymphaticsystem, Magnetic Resonance Lymphangiography (MRL) and Indocyanine Green Lymphangiography (ICGL), evaluatingtheir role for planning lymphaticovenular anastomosis (LVA) or other surgical-nonsurgical treatments in patients withlymphedema of the extremities.MATERIALS AND METHODS: We conducted a retrospective study of 32 patients (26 women) with a mean age of 38years (range 18-73) enrolled from January 2014 to December 2018; 20 out of 32 were affected by lower limb lym-phedema with 6 cases of primary lymphedema; all of them had stage II disease. All the patient underwent ICGL andMRL within a month of one another, by injecting different contrast medium into interdigital web spaces. In each patientwe rated the number of lymphatic vessels visualized, considering the wrist for the upper limb and the ankle for the low-er limb. Student’s t-test was applied.RESULTS: All patients completed both the diagnostic examinations without any significant complications. A statisticallysignificant difference (p < 0.05) was found between the number of lymphatic vessels identified on the wrist/ankle (34on ICGL vs 70 on MRL and 82 on ICGL vs 26 on MRL, considering affected and healthy limbs respectively). Inparticular, dermal backflow in advanced lymphedema seems to hinder lymphatic vessels detection on ICGL. Conversely,on healthy limbs, MRL hardly identifies lymphatics, because of their fast lymphatic flow and almost virtual lumen. CONCLUSIONS: Both MRL and ICGL are dynamic diagnostic modalities that permit an effective evaluation of lymphaticvessels anatomical and functional status in extremities lymphedema these diagnostic procedures may be considered com-plementary because they show different aspects of lymphatic system.
KEY WORDS: Indocyanine green, MR lymphangiography
Introduction
According to the International society of lymphology(ISL), lymphedema is an external and/or internal man-ifestation of lymphatic system insufficiency and derangedlymph transport.It is defined as an illness by the International Classifi-cation of Diseases from the World Health Organization 1.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
According to etiology, lymphedema can be classifiedeither as primary or secondary. Primary lymphedema iscaused by a congenital malformation (mutations ofFOXC2, FLT-4, SOX18, etc.), such as aplasia orhypoplasia of lymphatic channels, whereas secondary dis-ease is caused by stenosis or obstruction of lymphaticvessels associated with cancer therapy (node dissections,radiotherapy, etc.) or infections (Wuscheria Bancroftii)2. In Western Countries most of secondary lymphede-ma of upper limbs derives from surgery for breast can-cer. The incidence ranges between 20% and 25% inwomen who underwent mastectomy or quadrantectomyand axillary lymph node dissection, and reaches about35% when adjuvant radiotherapy is performed 3,4.Clinical manifestations are represented by a swelling, pro-duced by accumulation of excess water, filtered/diffusedplasma proteins, extravascular blood cells and parenchy-mal/stromal cell products in the extracellular space. Thisprocess culminates in proliferation of parenchymal andstromal elements with excessive deposition of extracellu-lar matrix substances and adipose tissue. The ISLdescribes four clinical stages, from stage 0 (subclinical)to stage III (no pitting, fibrotic tissue). Lymphedema most often becomes a chronic, generallyincurable condition, that requires lifelong care and atten-tion along with psychosocial support 2,5.If untreated, the disease can impair the quality of lifeof patients and lead to severe complications such asrepeated cellulitis of the affected limb which often requireadmission to hospital.An accurate diagnosis of lymphedema is essential forappropriate therapy 6.In most patients, the diagnosis of lymphedema can bereadily determined from the clinical history and physi-cal examination, but if symptoms are unclear or in casewe need a better definition, ultrasound techniques arethe first one to be used and lymphoscintigraphy (LS)has largely replaced conventional oil contrast lymphog-raphy for visualizing the lymphatic network 1. Other diagnostic and investigational tools are magneticresonance imaging (MRI) – including MR lymphogra-phy (MRL) and MR angiography techniques, computedtomography (CT), CT lymphograms, 3-D oil contrastlymphography, CT-SPECT, indirect (water soluble) lym-phography (IL) and ICG lymphography (ICGL) 7-13.Identifying and treating lymphedema at an early stageoffers greater success rate. Recently, in patients undergoing cancer treatment,prospective surveillance models (PSM) have been devel-oped to address early detection of lymphedema leadingto earlier and more efficacious treatment 1. In fact, dura-tion of lymphedema more than stage of disease seemsto determine a poor prognosis 14.Nowadays, no gold standard treatment has been defined,and therapy of peripheral lymphedema is divided intoconservative (physical therapy and adjuvants, drug ther-apy, psychosocial rehabilitation) and operative methods
Ann. Ital. Chir., 92, 4, 2021 453
Comparison of indocyanine green fluorescence lymphangiography and magnetic resonance lymphangiography, ect.
(microsurgical procedures, vascularized lymph node trans-plantation (VLTN), liposuction, surgical resection, tissueengineering/lymphatic revascularization) 15,16.Satisfactory studies comparing different methods oftreatment do not exist. However, conservative treatmentshould be used as the first step whereas surgery shouldbe used if conservative treatment has been unsuccess-ful 17.Imaging investigation is necessary to identify function-al vessels or nodes to manipulate and to plan thesurgery.LS is the gold standard method by which we can assessthe lymphatics but it has the disadvantage of low spa-tial, temporal and quality resolutions so the images arefuzzy, and the technique gives no information on theconditions of the subdermal lymphatics 18.ICGL introduced in the 2007 by Unno et al. 19 hasbeen increasingly used because allowed the surgeon tovisualize the status of subdermal lymphatics in real time20.In addition to peripheral ICGL also MRL is becom-ing more widespread in use around the world, becausethese two different imaging modalities provide bothanatomical and functional information of lymphaticvessels 21. The first one, ICGL exploits the fluorescenceimages obtained through a hand-held, near-infraredcamera after intradermal injection of indocyanine green;the second one, MRL, involves the injection ofGadolinium in the web spaces of the fingers or toesto image the lymphatics along with subtraction venog-raphy in order to determine which vessels are lymphaticand which are venous.22.Deciphering whether a structure is a lymphatic or avein can be very difficult 8. However, with the innovation of using Feraheme (fer-umoxytol) to block out the venous signal, this willbecome easier and more reliable. MRL also gives a lotof supplemental information about the limb: theamount of fat deposition, the appearance of the mus-cle compartments as well as giving accurate volumetricinformation on the limb 23. Another big advantage isthe possibility to create a venous map. In literature there are an EBM-based diagnostic algo-rithm and a lot of different comparatives studies (con-trast and non-contrast MRL comparison with LS, com-parison of LS and ICGL, etc.) but there is not a clearclinical way to choose which one of these different diag-nostic or surgical techniques should be used. The pre-ferred approach depends by the treatment team train-ing and availability of various treatments, for example,imaging techniques for the presurgical planning.The purpose of this work is to analyze and comparethe capability of ICGL and MRL to visualize lymphaticvessels in patients suffering from lymphedema and toevaluate how much more information can give MRLrespect to ICGL for planning lymphaticovenular anas-tomoses (LVA) or other surgical-nonsurgical treatments.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
F. Gentili, et al.
454 Ann. Ital. Chir., 92, 4, 2021
Material and Methods
PATIENTS
We conducted a retrospective study of 41 patients affect-ed by lymphedema of the upper or lower limbs whohave performed MRL and ICGL in our hospital fromJanuary 2014 to December 2018.Applying inclusion end exclusion criteria (patients under-went ICGL and MRL after a maximum of 1 month;MRL and ICGL both on healthy and sick limbs; uni-lateral lymphedema; lymphedema secondary to tumor;patient undergoing surgical treatment) we have includ-ed in the study 32 patients (26 women) with a meanage of 38 years (range 18-73); 20 out of 32 were affect-ed by lower limb lymphedema with 6 cases of primarylymphedema; the others were secondary to cancer treat-ment. All the patients had stage II disease, in whichlimb elevation alone rarely reduces swelling. All proce-dures performed in this study involving human partici-pants were undertaken in accordance with the ethicalstandards of the institutional and/or national researchcommittee and the 1964 Helsinki declaration and its lat-er amendments or comparable ethical standards.
ICGL EXAMINATION
Patient’s position - The examination was performed withthe patient supine for the study of both the upper andlower limbs. Contrast agent administration, equipment,image analysis - About 15 minutes before the injectionof indocyanine green (ICG) we have applied an anestheticcream (Emla, 2,5% prilocaine + 2,5% lidocaine) in thesecond and in the fourth interdigital spaces bilaterally. Thelimbs were examined one by one. About 0.2-0,.3 ml ofICG (Diagnogreen 0.5%; Daiichi Pharmatical, Tokyo,Japan) was subcutaneously injected in the second and inthe fourth interdigital spaces at the dorsum of the footor hand with a 27-gauge needle. Immediately after theinjection, fluorescence images of subcutaneous lymphaticvessels were obtained using an infrared camera system(PDE; Hamamatsu Photonics K.K. Hamamatsu, Japan),which activates ICG with emitted light (wavelength: 760nm) and filters out light with a wavelength below 820nm. The light source for emission of ICG consisted of760-nm LEDs, and the detector was a charge-coupleddevice (CCD) camera. The fluorescence images were real-time observed, recording a video, through a monitor ofa laptop by 2 operators, one of whom, at the same time,marked on the skin the course of lymphatic vessels (Fig.1). The exam lasts about 10-15 minutes.
MRL EXAMINATION
Patient’s position - Position of the patient changed
depending on the site of investigation. For the lowerlimb, patient was placed in the supine position, feet firstwith the arms bent over the head. For the upper limb,patient was placed in the prone position, head first witharms extended laterally over the head and palms down. Contrast agent administration - A standard dose (0.1ml/kg body weight) of gadobenate dimeglumine (Gd-BOPTA, Multihance, 0.5 M injectable solution, BraccoImaging, Milan, Italy) was divided into 8 portions andinjected in all interdigital web spaces with a 24 G nee-dle by 2 radiologists consecutively and simultaneously (1for each extremity).MR equipment and sequences - MR exams were per-formed with a 1.5T MR unit (Signa Twin Speed HDxt;General Electric Healthcare). A phased-array peripheralvascular coil was used for the study of the lower extrem-ities and an 8-channel body array coil for the upperextremities. The imaging protocol consisted of the followingsequences according to previous studies 9,10: (1) a sur-vey and a calibration performed for all stations; (2) a3D steady-state free precession (SSFP) balanced electro-cardiography (ECG)-triggered sequence (FIESTA, GE)with spectral fat saturation, before the injection of thecontrast medium; (3) a pre-contrast and post-contrastcoronal 3D spoiled gradient-recalled echo T1-weightedsequence with SPECtral inversion at lipid. The examslast about 1-1.15 hours.Image analysis - Assessment of the results of MRL andICGL was performed separately.Two surgeons (with 10 years of experience in ICGL)analyzed together the 24 recorded lymphography’svideos, counting and reporting the number of vessels atthe ankle or wrist of both healthy and diseased limbs.Moreover, the presence of dispersion of the contrastmedium in soft tissue due to proximal obstruction oflymph drainage, known as dermal backflow (DBF) andthe type of pattern (splash, stardust, etc.) was evaluated.At the same time, two radiologists (with 3 years of MRLexperience) reviewed in consensus the source images ofeach sequence on a 3D workstation to obtain real-time360° 3D post-processed images. Multiplanar reformations (MPR), thin-section maximumintensity projection (MIP) reconstructions (section thick-ness 10–15 mm) and the 3D pointer were used to iden-tify and localise lymphatic vessels for LVA treatment.The post-processed images, with the essential spatial anddepth information, were then recorded in the picturearchiving and communication system (PACS), so thatthey can be easily accessible to the surgeon before per-forming LVA.
STATISTICAL ANALYSIS
Student’s t test for paired samples was applied to com-pare the number of lymphatic vessels visualised by IGL
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
Ann. Ital. Chir., 92, 4, 2021 455
Comparison of indocyanine green fluorescence lymphangiography and magnetic resonance lymphangiography, ect.
and MRL both on affected and healthy limbs, under thefollowing hypothesis:
H1 : μ ≠ μ0
H0 : μ = μ0
A p value of less than 0.05 was considered to indicatea significant difference.
Results
All patients completed both the diagnostic examinations(ICGL and MRL) without any significant complications.In particular, no complications were observed during orafter the intradermal injection of ICG and Gd-BOPTA. A concomitant venous contamination was detected ineach MRL exam; however, pre-contrast SSFP balancedECG-triggered sequences however, pre-contrast SSFPbalanced ECG-triggered sequences simplified distinctionbetween veins and lymphatic vessels on post-contrastsequences. A statistically significant difference (p<0.05) was foundbetween the number of lymphatic vessels identified onthe calf/wrist, both in the affected and healthy limbs (34on ICGL vs 70 on MRL and 82 on ICGL vs 26 onMRL, considering affected and healthy limbs respective-ly). On MR examination, lymphedema showed high-sig-nal intensity in 3D-SSFP balanced images with an epi-fascial distribution in 28 out of 32 patients (87.5%) andan epifascial/subfascial distribution in the remaining 4patients (12.5%).
On MRL lymphatic vessels in affected limbs were dis-tinctly recognised by their tortuous and beaded appear-ance in 24 patients (75%), whereas they were funda-mentally rectilinear in the remaining 8 (25%), 6 of themwith primary lymphedema; the adjacent veins were
Table I - Comparison of MRL and IGL findings.
MRL IGL p-value
N° of lymphatic vessels in affected limbs 70 34 < 0.05N° of lymphatic vessels in healthy limbs 26 82 < 0.05N° of cases with dermal backflow 14 14 > 0.05
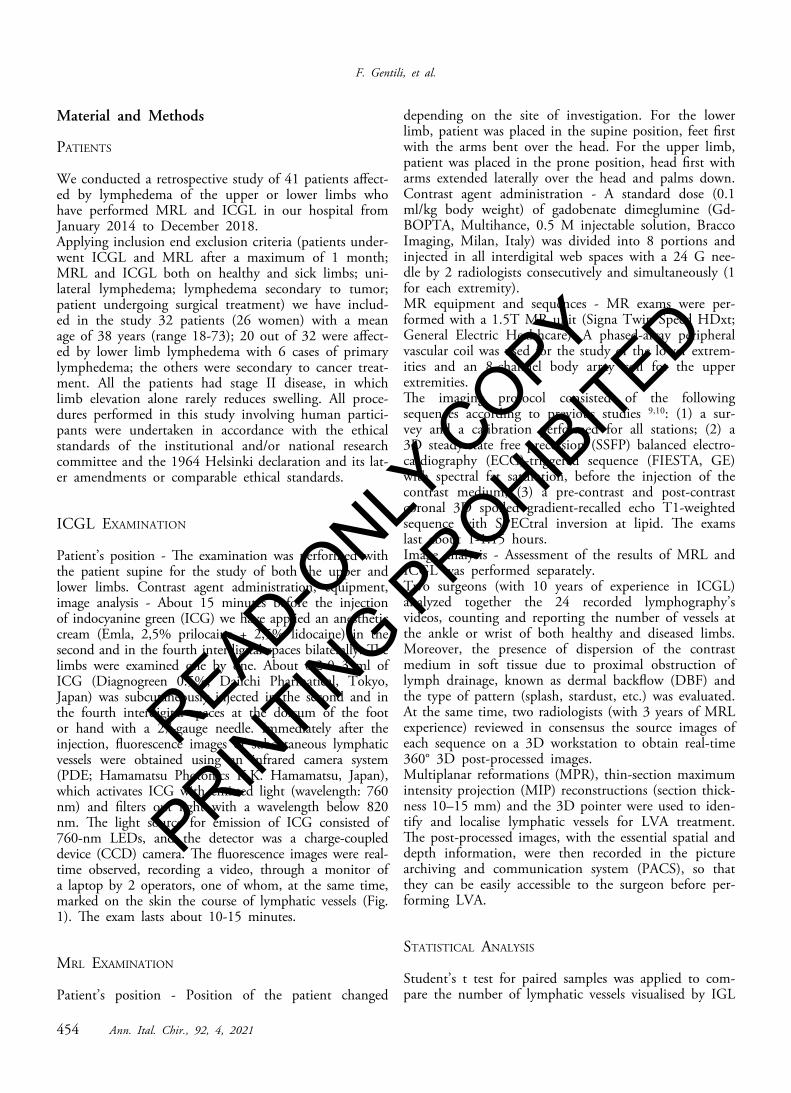
Fig. 1: The course of lymphatic vessels marked with a pen on ICGL.
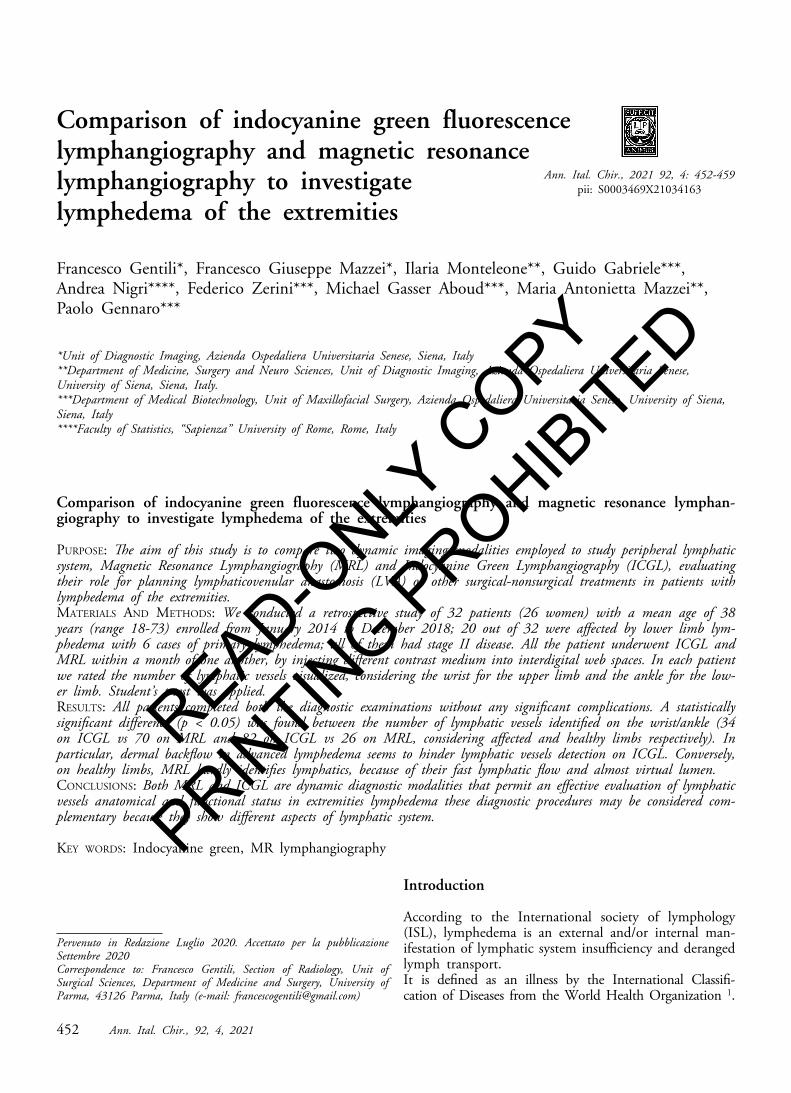
Fig. 2: (A, B). Rectilinear lymphatic vessels in the right lower limbdepicted by both ICGL (A) and MRL (B).
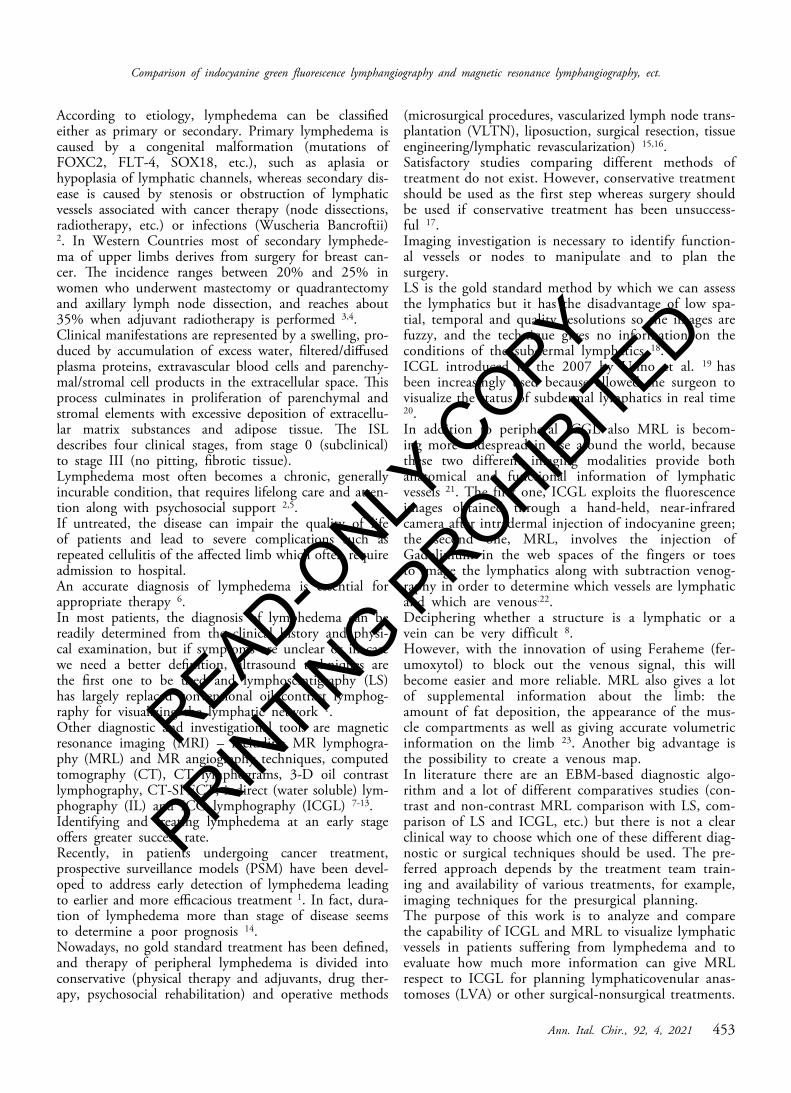
Fig. 3: (A, B). A tortuous pathological lymphatic vessel (arrows) withan area of dermal backflow (arrowheads) in 53-year-old man withsecondary lymphedema of the lower limb. ICGL (A) and MRL (B)show the same findings.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
F. Gentili, et al.
456 Ann. Ital. Chir., 92, 4, 2021
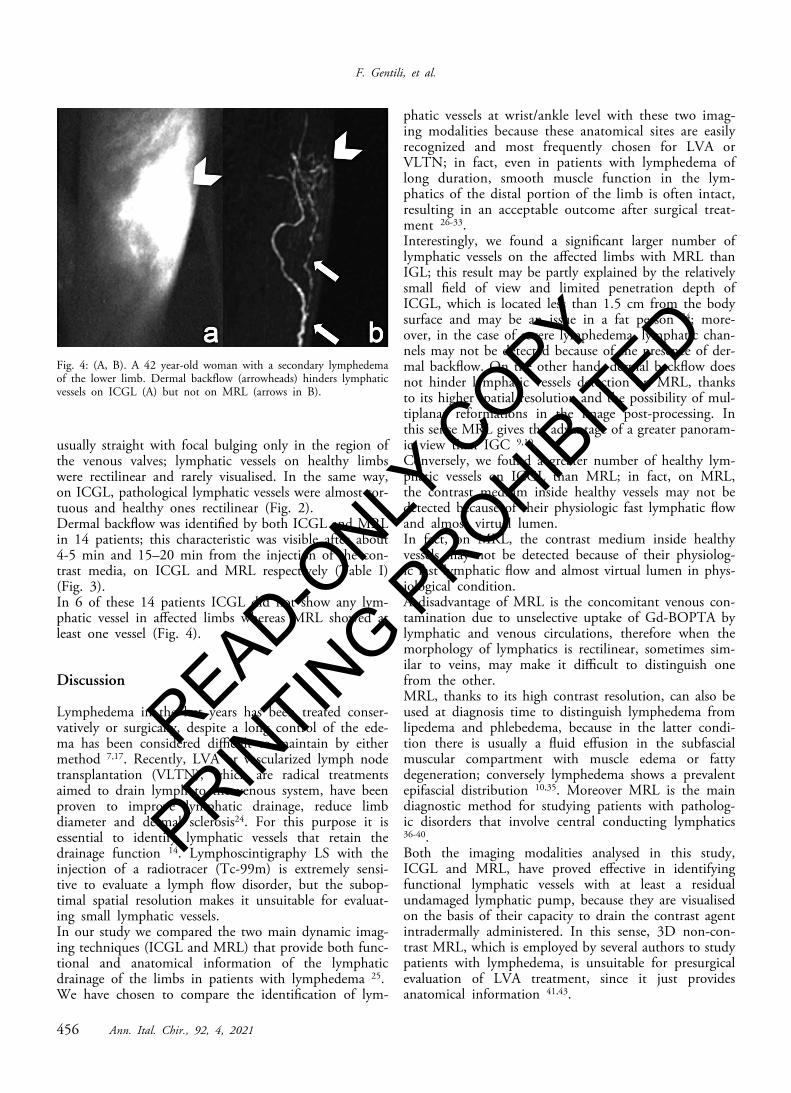
usually straight with focal bulging only in the region ofthe venous valves; lymphatic vessels on healthy limbswere rectilinear and rarely visualised. In the same way,on ICGL, pathological lymphatic vessels were almost tor-tuous and healthy ones rectilinear (Fig. 2). Dermal backflow was identified by both ICGL and MRLin 14 patients; this characteristic was visible after about4-5 min and 15–20 min from the injection of the con-trast media, on ICGL and MRL respectively (Table I)(Fig. 3). In 6 of these 14 patients ICGL did not show any lym-phatic vessel in affected limbs whereas MRL showed atleast one vessel (Fig. 4).
Discussion
Lymphedema in the last years has been treated conser-vatively or surgically, despite a long control of the ede-ma has been considered difficult to maintain by eithermethod 7,17. Recently, LVA or vascularized lymph nodetransplantation (VLTN), which are radical treatmentsaimed to drain lymph to the venous system, have beenproven to improve lymphatic drainage, reduce limbdiameter and dermal sclerosis24. For this purpose it isessential to identify lymphatic vessels that retain thedrainage function 14. Lymphoscintigraphy LS with theinjection of a radiotracer (Tc-99m) is extremely sensi-tive to evaluate a lymph flow disorder, but the subop-timal spatial resolution makes it unsuitable for evaluat-ing small lymphatic vessels. In our study we compared the two main dynamic imag-ing techniques (ICGL and MRL) that provide both func-tional and anatomical information of the lymphaticdrainage of the limbs in patients with lymphedema 25.We have chosen to compare the identification of lym-
phatic vessels at wrist/ankle level with these two imag-ing modalities because these anatomical sites are easilyrecognized and most frequently chosen for LVA orVLTN; in fact, even in patients with lymphedema oflong duration, smooth muscle function in the lym-phatics of the distal portion of the limb is often intact,resulting in an acceptable outcome after surgical treat-ment 26-33.Interestingly, we found a significant larger number oflymphatic vessels on the affected limbs with MRL thanIGL; this result may be partly explained by the relativelysmall field of view and limited penetration depth ofICGL, which is located less than 1.5 cm from the bodysurface and may be an issue in a fat person 34; more-over, in the case of severe lymphedema, lymphatic chan-nels may not be detected because of the presence of der-mal backflow. On the other hand, dermal backflow doesnot hinder lymphatic vessels detection on MRL, thanksto its higher spatial resolution and the possibility of mul-tiplanar reformations in the image post-processing. Inthis sense MRL gives the advantage of a greater panoram-ic view than IGC 9,10.Conversely, we found a greater number of healthy lym-phatic vessels on ICGL than MRL; in fact, on MRL,the contrast medium inside healthy vessels may not bedetected because of their physiologic fast lymphatic flowand almost virtual lumen. In fact, on MRL, the contrast medium inside healthyvessels may not be detected because of their physiolog-ic fast lymphatic flow and almost virtual lumen in phys-iological condition.A disadvantage of MRL is the concomitant venous con-tamination due to unselective uptake of Gd-BOPTA bylymphatic and venous circulations, therefore when themorphology of lymphatics is rectilinear, sometimes sim-ilar to veins, may make it difficult to distinguish onefrom the other.MRL, thanks to its high contrast resolution, can also beused at diagnosis time to distinguish lymphedema fromlipedema and phlebedema, because in the latter condi-tion there is usually a fluid effusion in the subfascialmuscular compartment with muscle edema or fattydegeneration; conversely lymphedema shows a prevalentepifascial distribution 10,35. Moreover MRL is the maindiagnostic method for studying patients with patholog-ic disorders that involve central conducting lymphatics36-40.Both the imaging modalities analysed in this study,ICGL and MRL, have proved effective in identifyingfunctional lymphatic vessels with at least a residualundamaged lymphatic pump, because they are visualisedon the basis of their capacity to drain the contrast agentintradermally administered. In this sense, 3D non-con-trast MRL, which is employed by several authors to studypatients with lymphedema, is unsuitable for presurgicalevaluation of LVA treatment, since it just providesanatomical information 41,43.
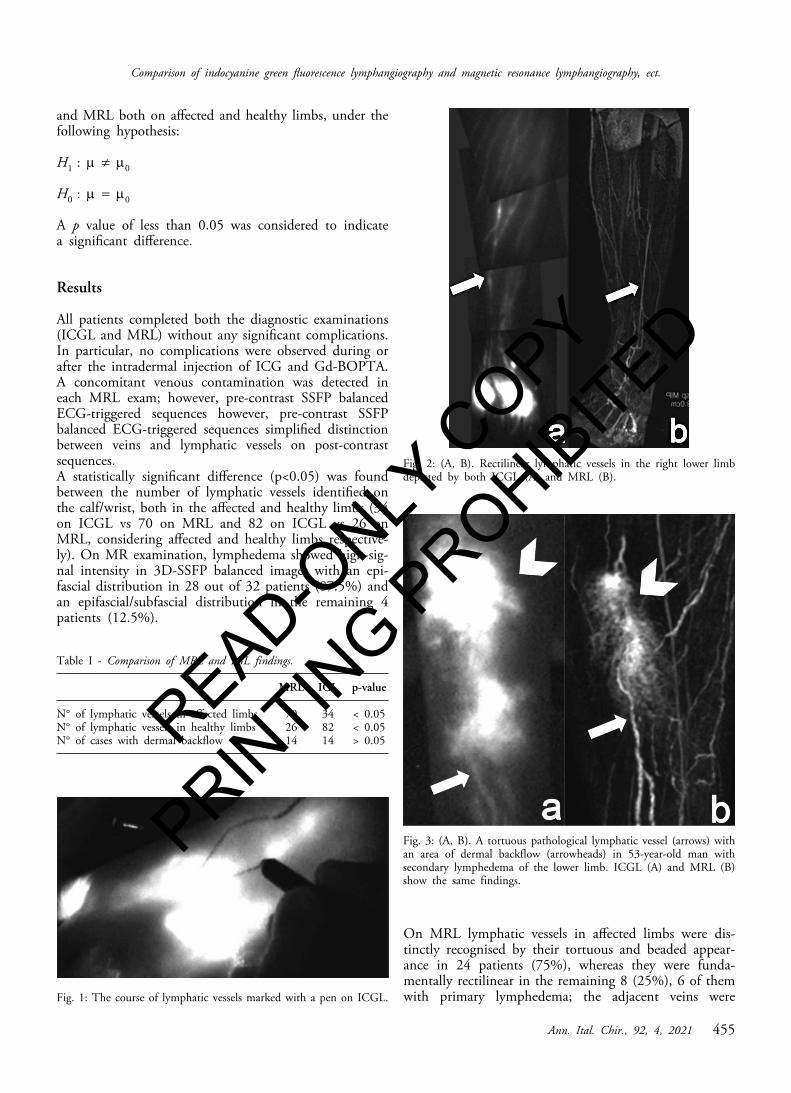
Fig. 4: (A, B). A 42 year-old woman with a secondary lymphedemaof the lower limb. Dermal backflow (arrowheads) hinders lymphaticvessels on ICGL (A) but not on MRL (arrows in B).
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
This is the first single-center study that compares ICGLwith MRL for studying peripheral lymphedema; boththe imaging modalities are effective for this purpose, eachone with some advantages and disadvantages.Some limitations of our study should be noted. First, itis a retrospective study, although all the examinationsare reevaluated in a prospective setting; second the smallcase series; third the surgeon and the radiologist ana-lyzed the images individually and finally both the imag-ing modalities are operator-dependent.
Conclusions
Both MRL and ICGL are dynamic diagnostic modali-ties that permit an effective evaluation of lymphatic ves-sels anatomical and functional status in extremities lym-phedema. In our experience they may be considered complemen-tary, because they showed different aspects of lymphat-ic system. They are important not only for the diagno-sis but especially for choosing the right surgical treat-ment, allowing to preserve functional vessels and toensure that the lymphatic chosen is only transected oncealong its course.ICGL is simple to use intraoperatively for the surgeon,minimally invasive, rapid and highly sensitive.It has the disadvantage that it cannot detect lymphaticchannels deeper than 1,5-2 cm under the skin, which isa problem in patients with a thick subcutaneous tissueor in case of dermal back-flow; however we have alsoseen its superiority in showing lymphatic vessels in thehealthy limbs, facilitating surgical planning on the affect-ed ones.MRL gives the best panoramic view, providing an imageof the entire extremity and showing both the superficialand deep lymphatic vessels, the edema, the venous pat-tern and the fat hypertrophy or fibrosis; however it hard-ly depicts lymphatics in healthy limbs, it requires expertradiologists, it has a higher cost, it is more invasive forthe patients and evaluating and choosing MRL coordi-nates is not a trivial process.
Riassunto
Questo lavoro confronta le due principali metodiche diimaging attualmente utilizzate per studiare il sistema lin-fatico periferico nei pazienti affetti da linfedema, la RM(Magnetic Resonance Lymphangiography, MRL) e lostudio a fluorescenza con verde di indocianina(Indocyanine Green Lymphangiography, ICGL), perpianificare il trattamento chirurgico di anastomosi lin-fatico-venosa o eventuali altri trattamenti. Sono stati inclusi 32 pazienti, dei quali 26 donne, conuna età media di 38 anni (range 18-73), arruolati da
Ann. Ital. Chir., 92, 4, 2021 457
Comparison of indocyanine green fluorescence lymphangiography and magnetic resonance lymphangiography, ect.
gennaio 2014 a dicembre 2018; 20 di 32 avevano un lin-fedema agli arti inferiori e 6 casi di linfedema erano pri-mari; tutti i pazienti avevano una malattia al II stadio.Entrambi gli esami sono stati eseguiti a tutti i pazienti intempi differenti (intervallo di tempo massimo 1 mese),iniettando il mezzo di contrasto a livello intradermico(Diagnogreen 0.5%; Daiichi Pharmatical, Tokyo, Japanper ICGL e Gd-BOPTA, Multihance, 0.5 M injectablesolution, Bracco Imaging, Milan, Italy per MRL), neglispazi interdigitali delle mani o dei piedi con un ago da24 G. Per ogni paziente sono stati conteggiati, in entrambele metodiche, i vasi linfatici visualizzati a livello del pol-so per gli arti superiori e a livello della caviglia per gliarti inferiori, sia negli arti sani che nei malati. Tutti i pazienti hanno completato gli esami senza signi-ficative complicazioni. In ogni esame RM il contrastoera in parte drenato anche dal sistema venoso mentre ilverde di indocianina era selettivo per il sistema linfati-co. Una differenza statisticamente significativa tra le duemetodiche è stata trovata tra il numero di vasi linfaticia livello della caviglia/polso sia negli arti malati che neisani (34 con ICGL vs 70 con MRL e 82 con ICGL vs26 con MRL), considerando arti malati e sani rispetti-vamente. In entrambe le metodiche i vasi linfatici negli arti lin-fedematosi apparivano per lo più tortuosi, mentre i sanipresentavano una morfologia lineare ed erano difficil-mente visualizzati in RM a causa del rapido flusso lin-fatico e del loro lume, pressochè virtuale. Lo stravasointradermico del mezzo di contrasto (dermal backflow)è stato identificato in 14 pazienti, in 6 dei quali lo stu-dio a fluorescenza non ha potuto identificare nessun vasolinfatico, mentre in RM almeno un vaso linfatico è sta-to visualizzato.Da questi risultati emerge che entrambe le metodicheindagate forniscono informazioni anatomiche e funzion-ali sul sistema linfatico periferico degli arti, permetten-do di scegliere e localizzare accuratamente in fase pre-chirurgica quei vasi con una pompa linfatica residua. Lostudio a fluorescenza con verde di indocianina è rapido,ben tollerabile dal paziente e può essere impiegato anchein sala operatoria. La RM fornisce una visione panoram-ica dell’arto, la visulizzazione dei vasi linfatici non è osta-colata dalla presenza stravaso intradermico del mezzo dicontrasto grazie alla superiore risoluzione spaziale, e per-mette di valutare allo stesso tempo il drenaggio venoso;d’altra parte è un esame costoso e meno tollerabile dalpaziente per i lunghi tempi d’acquisizione.
References
1. Executive Committee: The diagnosis and treatment of peripherallymphedema: 2016 consensus document of the international society oflymphology. Lymphology, 2016; 49(4):170-84.
2. Olszewski W: On the pathomechanism of development of postsur-gical lymphoedema. Lymphology, 1973; 6: 35-51.
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED
F. Gentili, et al.
458 Ann. Ital. Chir., 92, 4, 2021
3. Campisi C, Boccardo F, Zilli A, et al.: Linfedema secondario altrattamento del cancro mammario: Possibilità di prevenzione diagnos-tica e terapeutica. Lymphedema secondary to breast cancer treatment:Possibility of diagnostic and therapeutic prevention. Ann Ital Chir,2002; 73(5):493-98.
4. Campisi C: Chirurgia del cancro della mammella, linfedema sec-ondario e qualità di vita: Una sfida per il chirurgo generale. Surgeryof breast cancer, secondary lymphedema and quality of life: A chal-lenge for the general surgeon. Ann Ital Chir, 2002; 73(5):471.
5. Witte CL, Witte MH: Lymphaticovenular anastomosis to preventcellulitis associated with lymphoedema. Br J Surg, 2014; 101:1391-396.
7. Witte CL, Witte MH, Unger EC: Advances in imaging of lymphflow disorders. RadioGraphics, 2000; 20:1697-719.
8. Gennaro P, Chisci G, Mazzei F, Gabriele G: Magnetic resonancelymphangiography: How to prove it? J Magn Reson Imaging, 2016;44(2):509-10.
9. Mazzei MA, Gentili F, Mazzei FG, Gennaro P, Guerrieri D,Nigri A: High-resolution MR lymphangiography for planning lym-phaticovenous anastomosis treatment: A single-centre experience. RadiolMed, 2017; 122:918-27.
10. Mazzei FG, Gentili F, Guerrini S, Cioffi Squitieri N, GuerrieriD, Gennaro P, et al.: MR lymphangiography: A practical guide toperform it and a brief review of the literature from a technical pointof view. Biomed Res Int, 2017; 2598358.
11. Gennaro P, Borghini A, Chisci G, Mazzei FG, Weber E,Tedone Clemente E, et al.: Could MRI visualize the invisible? AnItalian single center study comparing magnetic resonance lymphography(MRL), super microsurgery and histology in the identification of lym-phatic vessels. Eur Rev Med Pharmacol Sci, 2017; 21:687-94.
12. Aung T, Taeger C, Geis S, Schiltz D, Brix E, Wenzel C etal.: WITHDRAWN: The use ofintegrated indocyanine green fluores-cence microscope camera for intraoperative lymphography of supermi-crosurgery. Clin Hemorheol Microcirc, 2018.
13. Ktaft JC, Treuting PM, Ho RJY: Indocyanine green nanoparti-cles undergo selective lymphatic uptake, distribution and retention andenable detailed mapping of lymph vessels, nodes and abnormalities. JDrug Target, 2018; 26:494-504.
14. Boccardo F, Campisi C: Disabilità e linfedema. Disability andlymphedema. Ann Ital Vhir. 2002; 73(5):484-88.
15. Koshima I, Marushima M, Yamamoto T, Mihara M, Iida:Recent advancement on surgical treatments for lymphedema. Ann VascDis, 2012; 5(4) 409-15.
16. Nagase T, Gonda K, Inoue K, Higashino T, Fukuda N, GoraiK et al.: Treatment of lymphedema with lymphaticovenular anasto-moses. Int J Clin Oncol, 2005; 10:304-10.
17. Leduc O, Leduc A: Rehabilitation protocol in upper limb lym-phedema. Ann Ital Chir, 2002; 73(5):479-84.
18. Mihara M, Hara H, Narushima M, Todokoro T, Iida T, OhtsuH, et al.: Indocyanine green lymphography is superior to lym-phoscintigraphy in imaging diagnosis of secondary lymphedema of thelower limbs. J Vasc Surg Venous Lymphat Disord, 2013;1(2):194-201.
19. Unno N, Inuzuka K, Suzuki M, Yamamoto N, Sagara D,Nishiyama M, et al.: Preliminary experience with a novel fluorescence
lymphography using indocyanine green in patients with secondary lym-phedema. J Vasc Surg, 2007; 45(5):1016-21.
20. Akita S, Mitsukawa N, Kazama T, Kuriyama M, Kubota Y,Omori N, et al.: Comparison of lymphoscintigraphy and indocyaninegreen lymphography for the diagnosis of extremity lymphoedema. J PlastReconstr Aesthet Surg, 2013; 66(6):792-98.
21. Pons G, Clavero JA, Alomar X, Rodríguez-Bauza E, Tom LK,Masia J: Preoperative planning of lymphaticovenous anastomosis: Theuse of magnetic resonance lymphangiography as a complement to indo-cyanine green lymphography. J Plast Reconstr Aesthet Surg, 2019;72(6):884-91.
22. Liu N, Zhang Y: Magnetic resonance lymphangiography for thestudy of lymphatic system in lymphedema. J Reconstr Microsurg, 2016;32(1):66-71.
23. Bae JS, Yoo RE, Choi SH, Park SO, Chang H, Suh M, et al.:Evaluation of lymphedema in upper extremities by MR lymphangiog-raphy: Comparison with lymphoscintigraphy. Magn Reson Imaging,2018; 49:63-70.
24. Koshima I, Nanba Y, Tsutsui T, Takahashi Y, Itoh S: Long-term follow-up after lymphaticovenular anastomosis for lymphedema inthe leg. J Reconstr Microsurg, 2003; 19(4):209-15.
25. Liu NF, Lu Q, Jiang ZH, Wang CG, Zhou JG: Anatomic andfunctional evaluation of the lymphatics and lymph nodes in diagnosisof lymphatic circulation disorders with contrast magnetic resonance lym-phangiography. J Vasc Surg, 2009; 49(4):980-87.
26. Mihara M, Hara H, Kawakami Y, Zhou HP, Tange S, KikuchiK, et al.: Site specific evaluation of lymphatic vessel sclerosis in lowerlimb lymphedema patients. Lymphat Res Bio, 2018; 16(4):360-67.
27. Gennaro P, Gabriele G, Aboh IV, Cascino F, Zerini F, AboudMG: Ultramicrosurgery: A new approach to treat primary male gen-ital lymphedema. JPRAS Open, 2019; 20:72-80.
28. Ierardi AM, Piacentino F, Pesapane F, Carnevale A, Curti M,Fontana F, et al.: Basic embolization techniques: Tips and tricks. ActaBiomed, 2020; 91(8-S):71-80.
29 Gennaro P, Gabriele G, Salini C, Chisci G, Cascino F, Xu JFet al.: Our supramicrosurgical experience of lymphaticovenular anasto-mosis in lymphoedema patients to prevent cellulitis. Eur Rev MedPharmacol Sci, 2017; 21(4):674-79.
30 Mihara M, Hara H, Furniss D, Narushima M, Iida T, KikuchiK et al.: Lymphaticovenular anastomosis to prevent cellulitis associat-ed with lymphoedema. Br J Surg, 2014; 101(11):1391-96.
31 Gennaro P, Gabriele G, Mihara M, Kikuchi K, Salini C, AbohI et al.: Supramicrosurgical lymphatico-venular anastomosis (LVA) intreating lymphoedema: 36-months preliminary report. Eur Rev MedPharmacol Sci, 2016; 20(22):4642-653.
32 Mihara M, Hara H, Kikuchi K, Yamamoto T, Iida T,Narushima M, et al.: Scarless lymphatic venous anastomosis for latentand early-stage lymphoedema using indocyanine green lymphographyand non-invasive instruments for visualising subcutaneous vein. J PlastReconstr Aesthet Surg, 2012; 65(11):1551-558.
33 Barone V, Borghini A, Tedone Clemente E, Aglianò M, GabrieleG, Gennaro P, et al.: New Insights into the Pathophysiology of Primaryand Secondary Lymphedema: Histopathological Studies on HumanLymphatic Collecting Vessels. Lymphat Res Biol, 2020.
34 Unno N, Nishiyama M, Suzuki M, Yamamoto N, Inuzuka K,
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED

Ann. Ital. Chir., 92, 4, 2021 459
Comparison of indocyanine green fluorescence lymphangiography and magnetic resonance lymphangiography, ect.
Sagara D, et al.: Quantitative lymph imaging for assessment of lymphfunction using indocyanine green fluorescence lymphography. Eur J VascEndovasc Surg, 2008; 36:230-36.
35 Gentili F, Guerrini S, Mazzei FG, Volterrani L, Mazzei MA:MRL as one-shot examination for patients suffering from lymphedema.Radiol Med, 2020; 125(8):798-99.
36 Kim EY, Hwang HS, Lee HY, Cho JH, Kim HK, Lee KS, etal.: Anatomic and functional evaluation of central lymphatics withnoninvasive magnetic resonance lymphangiography. Medicine(Baltimore), 2016; 95(12):e3109.
37 Krishnamurthy R, Hernandez A, Kavuk S, Annam A, PimpalwarS: Imaging the central conducting lymphatics: Initial experience withdynamic MR lymphangiography. Radiology, 2015; 274(3):871-78.
38 Mignarri A, Gentili F, Masia F, Genua A, Cenciarelli S, BrunoriP et al.: Imaging of the thymus in myotonic dystrophy type 1. NeurolSci, 2018; 39(2):347-51.
39 Bennett D, Fossi A, Refini RM, Gentili F, Luzzi L, VoltoliniL et al.: Posttransplant solid organ malignancies in lung transplantrecipients: A single-center experience and review of the literature.Tumori. 2016; 102(6):574-81.
40. Gentili F, Pelini V, Lucii G, Luzzi L, Mazzei FG, Fausto A,et al.: Update in diagnostic imaging of the thymus and anterior medi-astinal masses. Gland Surg, 2019; 8(Suppl 3):S188-S207.
41. Liu N, Wang C, Sun M: Noncontrast three-dimensional mag-netic resonance imaging vs lymphoscintigraphy in the evaluation oflymph circulation disorders: A comparative study. J Vasc Surg, 2005;41(1):69-75.
42. Mazzei MA, Squitieri NC, Sani E, et al.: Differences in perfu-sion CT parameter values with commercial software upgrades: A pre-liminary report about algorithm consistency and stability. Acta Radiol,2013; 54(7):805-11.
43. Guerrini S, Gentili F, Mazzei FG, Gennaro P, Volterrani L,Mazzei MA: Magnetic resonance lymphangiography: With or withoutcontrast? Diagn Interv Radiol 9 October 2020 10.5152/ dir.2020.19482 [Epub Ahead of Print]
READ-ONLY
COPY
PRINTIN
G PROHIB
ITED