2005 also® syllabus update g: malpresentations ... chapter g... · 2005 also® syllabus update g:...
TRANSCRIPT

2005 ALSO® Syllabus Update
G: Malpresentations, Malpositions, and Multiple Gestations
Evidence Review completed: October 18, 2005 By Allan Wilke, MD and Harry (Chip) Taylor, MD, MPH
Update published: December 6, 2005
SORT A Recommendation • Planned cesarean birth reduces perinatal mortality, neonatal mortality, and serious
neonatal morbidity compared to planned vaginal breech delivery. SORT B Recommendation • Planned cesarean birth does not reduce the risk of death or neurodevelopmental
delay in children at 2 year follow-up compared to planned vaginal breech delivery.
A Cochrane Review1 of 3 RCTs with a total of 2396 breech deliveries found that planned cesarean birth (PCB) led to a reduction in perinatal/neonatal morbidity and mortality when compared to planned vaginal birth (PVB). PCB was associated with a corresponding increase in short-term maternal morbidity. (See table below). The Term Breech Trial2 was the largest of the 3 RCTs and drove the conclusions of the Review. It was the only RCT with long term follow-up; 920 infants and 917 mothers were evaluated 2 years after breech birth. The infant outcomes (death or neurodevelopmental delay) were similar in PCB and PVB groups.3 Maternal outcomes in the two groups (including perineal pain, back pain, sexual problems, painful intercourse, incontinence, and others) were also similar.3# Events/Patients (%)
Outcomes
PCB PVB
Relative Risk (95% Confidence
Interval)
NNT/ NNH**
Perinatal/neonatal death or severe neonatal morbidity*
17/1039 (1.64%)
52/1039 (5.00%)
0.33 (0.19-0.56) 30
Perinatal/neonatal death 3/1166 (0.26%)
14/1222 (1.15%)
0.29 (0.10-0.86) 112
Maternal morbidity (short-term) 107/1169 (9.15%)
106/1227 (8.64%)
1.29 (1.03-1.61) 196
Death or neurodevelopmental delay at age 2 years*
14/457 (3.06%)
13/463 (2.81%)
1.09 (0.52-2.30) ***
* Combined outcome ** NNT is the number needed to treat; NNH is the number needed to harm. *** Since the 95% Confidence Interval includes 1.00, the result is not statistically significant and the NNH is not calculated. Fatal anomalies were excluded from the perinatal/neonatal death rates. The American College of Obstetrics and Gynecology (ACOG) issued an Opinion4 noting that reduction in risk from cesarean versus planned vaginal breech delivery is greatest in industrialized nations with low perinatal mortality rates. ACOG concludes that planned vaginal delivery of a singleton term breech may no longer be appropriate.

2005 ALSO® Syllabus Update
G: Malpresentations, Malpositions, and Multiple Gestations
ALSO® acknowledges the important implications of this new evidence and the recommendations of the ACOG Committee. ALSO® does not advocate routine vaginal delivery for breech presentation. However, the decision how best to deliver a breech presentation is complicated and may be based on consideration of many factors, including the patient’s informed consent. Because unanticipated breech vaginal deliveries do occur, obstetrical caregivers need to have the knowledge and skills to safely handle this situation. It is for this reason that ALSO® teaches a standard method to prepare ALSO® providers to manage a vaginal breech delivery.
1 Hofmeyr GJ, Hannah ME. Planned caesarean section for term breech delivery. The Cochrane Database of Systematic Reviews 2005, Issue 4. [Evidence level 1, systematic review of RCTs] 2 Hannah ME, Hannah WJ, Hewson SA, et al. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet. 2000;356(9239):1375-1383. [Evidence level 1, RCT] 3 Hannah ME, Whyte H, Hannah WJ, et al. Maternal outcomes at two years after planned cesarean section versus planned vaginal birth for breech presentation at term: the International Randomized Term Breech Trial. Am J Obstet Gynecol. 2004;191:917-927. [Evidence level 2, prospective cohort study] 4 ACOG committee opinion: number 265, December 2001. Mode of term single breech delivery. Obstet Gynecol. 2001;98:1189-1190. [Evidence level 3, consensus guideline]

G: Malpresentations, Malpositions, and Multiple Gestation1
Objectives(slide 2) At the end of this lecture / discussion and workstation, participants will be
able to:
1. Define six types of malpresentations and methods for diagnosis.
2. List complications associated with each malpresentation.
3. Discuss the criteria for allowing vaginal delivery, and the management ofvaginal delivery, when appropriate.
4. Discuss multiple gestation, with special attention to labor and delivery.
5. Perform safe, effective delivery of various malpositions andmalpresentations using the maternal-fetal mannequin.
Definitions(slide 3) Definitions are important to a discussion of malpresentations. Lie refers to the
relationship of the long axis of the fetus to that of the mother, specified aslongitudinal, transverse, or oblique (also referred to as unstable). Presentationrefers to the portion of the fetus that is foremost or “presenting” in the birthcanal. The fetus may present by its vertex, breech, face, brow, or shoulder.Position refers to a reference point on the presenting part, and how it relates tothe maternal pelvis. For example, the reference point on the vertex is the occiput.When the fetal occiput is directed toward the mother’s symphysis, or anteriorly,the fetus is in occiput anterior (OA) position. When the occiput is directed towardthe maternal spine, the fetus is occiput posterior (OP). Intermediate positionsaround the compass are left and right occiput anterior (LOA and ROA), left andright occiput transverse (LOT and ROT), and left and right occiput posterior (LOPand ROP).
Methods of Diagnosis(slide 4) There are three principal methods of determining fetal lie, presentation, and
position. The first is Leopold’s maneuvers or abdominal palpation. The secondmethod is vaginal exam. The third method is imaging. Ultrasound is the preferredimaging method. Labor floor ultrasound examination is widely utilized in hospitals
G: Malpresentations, Malpositions, andMultiple Gestation
(slide 1)
Steven H. Eisinger, M.D.

2G: Malpresentations, Malpositions, and Multiple Gestation
of all sizes, and every birth provider should have acquaintance with ultrasoundskills in this setting to determine fetal lie, presentation, and position. Occasionallyx-ray is necessary, particularly when fine detail is needed, such as the position ofthe limbs in a breech.
Incidence of Malpresentations at Term1,2
Malpresentation Incidence Percent
Occiput posterior 1 in 10 to 20 5 to 10
Breech 1 in 25 to 33 3 to 4
Transverse lie or shoulder presentation 1 in 322 to 420 0.3 to 0.23
Face 1 in 500 to 1200 0.2 to 0.08
Compound presentation 1 in 700 to 2235 0.14 to 0.047
Brow 1 in 4470 0.02
The Fetal Head and the Maternal Pelvis(slide 5) Most fetal malpresentations (posterior, breech, face, brow) are clinically
significant because the fetal head is not round, but rather ovoid or egg-shaped.The smallest of the fetal diameters is the suboccipitobregmatic; the largest is theoccipitomental. The difference between them is three centimeters, or about 24percent. When the head is in full flexion, the suboccipitobregmatic or smallestdiameter presents to the pelvis. When the head is in full extension (or deflexion)the occipitomental or largest diameter presents. Delivery is much more likely tooccur, and will be easier, if a smaller diameter presents. Therefore, the attitude ofthe fetal head (flexion versus extension) as it presents to the pelvis is ofparamount importance. A degree of fetal extension of the head occurs with OPpresentations, face and brow presentations, and some breeches.
(slide 6) Asynclitism also plays a major role in the mechanics of labor. Asynclitism islateral flexion of the head, such that the sagittal suture is not in the middle of thebirth canal. Some degree of asynclitism is normal, and the fetal head may evenshift back and forth from anterior to posterior asynclitism as the headaccommodates more deeply into the pelvis. Extreme degrees of asynclitism mayprevent labor from progressing. Asynclitism becomes a major factor in adequateforceps application.

The maternal pelvis also plays an important role in the cause of various(slide 7) malpresentations and prognosis for delivery. There are four pure types of pelves.
Most women have a gynecoid or intermediate type:
• Gynecoid (round)
• Anthropoid (oval, with the long axis in the AP plane)
• Platypelloid (oval, with the long axis in the transverse plane)
• Android (triangular or heart-shaped, with the apex of the triangle anteriorly)
While a full discussion of pelvic types and pelvimetry is of limited clinicalusefulness, it can be generalized that a narrow pelvis such as the anthropoid cancause persistent occiput posterior; the platypelloid pelvis can cause a transversearrest; the android pelvis is prejudicial to delivery with all malpresentations; andan inadequate or small pelvis can be associated with most of themalpresentations, mainly based on the inability of the head to descend, engage,or rotate.
Occiput Posterior PositionIn the Occiput Posterior (OP) position, the fetus lies with its occiput towards themother’s spine and its face towards the mother’s symphysis and abdomen. Inother words, the fetus is face up when the mother is supine or in lithotomyposition. Usually the fetus in occiput posterior position will rotate spontaneouslyto occiput anterior (OA) and deliver spontaneously. Spontaneous rotation fails tooccur in five to ten percent of cases, and the fetus remains in persistent occiputposterior position. The exact cause of persistent OP is unknown, but transversenarrowing of the pelvis plays a role. All occiput posterior fetuses are somewhatdeflexed because the vertex drops back to fill the hollow of the sacrum. Thecombination of deflexion and posterior presentation causes less favorablediameters of the fetal head to present to the pelvis than when the fetus is in theocciput anterior position.
(slide 8) The diagnosis of OP is based on observation of the patient and examination.Ultrasound imaging can be helpful but is sometimes confusing. Easy palpation ofthe anterior fontanel on vaginal exam is a diagnostic aid in determining OPposition. This is true because the anterior fontanel is most easily felt when thehead is somewhat deflexed. If the anterior fontanel is palpated, then one mustidentify the sagittal suture. This can be accomplished by following each suturewith the examining finger until the posterior fontanel is encountered. Occasionallyan ear can be palpated, revealing the fetal position. The exam can be confusingdue to molding, overriding of sutures, edema, and asynclitism. Dilation is oftenasymmetric and a persistent anterior lip is common. Back pain, or “back labor,” isa clinical hallmark of OP position.
G: Malpresentations, Malpositions, and Multiple Gestation3

The diagnosis of OP can be very difficult. Most obstetric care providers have hadthe experience of making the diagnosis at the last minute when the fetal headseems to fill the posterior pelvis as it delivers, or even later as the fetal facebecomes visible under the symphysis. In the “old days” even skilled operatorsoccasionally rotated babies “the wrong way,” from OA to OP, to the delight oftheir residents!
(slide 9) The conduct of labor and delivery with a persistent OP is not markedly differentfrom that of the fetus in the occiput anterior position.1 (Category C) The progressof labor can be followed by cervical dilation and the descent of the vertex throughthe birth canal. Labor with OP position is prolonged on the average for one hour inparous women, and two hours in nulliparous women. Perinatal mortality does notdiffer significantly from OA, and there is no significant difference in Apgar scores.However, perineal lacerations and extensions of episiotomies may be increasedbecause the vertex sweeps through the posterior pelvis, larger diameters arepresented to the pelvic outlet, and the occiput places maximal pressure on theperineum as it delivers. There are five possibilities for vaginal delivery whenpersistent occiput posterior occurs:
1. Spontaneous Delivery – Spontaneous delivery occurs 45 percent of the timein one study utilizing expectant management.3 Because the fetal headcannot stem upward until the face has cleared the symphysis, the fetalvertex must pass through the posterior pelvis, where it places strain on theperineum. These babies look like they “want” to deliver through the rectum.However, frequently the delivery is easy.
(slide 10) 2. Manual Rotation – Midwives and labor and delivery nurses have longheld that fetuses in OP position can be turned by placing the laboringwoman in various positions such as on her side, squatting or ambulating, onhands and knees, or with her back arched (to make the fetusuncomfortable, so it turns itself!). Failing these maneuvers, manual rotationbecomes an attractive alternative during a long second stage of laborbecause it can be attempted during any vaginal exam. If successful,delivery may be greatly expedited; if unsuccessful, no harm has been done.
The key to manual rotation is to enhance the natural and normal forces ofrotation. Rotation normally occurs when the flexed fetal head strikes themuscles of the pelvic floor, known as the levator sling. The operator mustfirst therefore flex the fetal head. This is accomplished by placing a hand inthe posterior pelvis behind the occiput. The operator’s hand essentiallyreplicates and enhances the levator sling effect, acting like a wedge to flexthe head. Then rotatory force is applied to the head, using for purchase anyfontanel or suture that may be felt with the examining fingers. Someoperators grasp the head with the thumb as well. The rotation should beattempted at the same time as a contraction, and with the mother pushingas well, to force the head down on the levator sling (and the hand), which is
G: Malpresentations, Malpositions, and Multiple Gestation4

the natural mechanism for flexion and rotation. An experienced assistantmay massage the fetal shoulder in the direction of the rotation withsuprapubic or abdominal pressure. Manual rotation may be attempted withthe patient in lithotomy position, or lateral Sims’ position, or on hands andknees. In the hands and knees position the abdominal assist is impractical.
A commonly encountered question relates to which hand should be used torotate the fetus. If the fetus were straight OP, the operator would naturallyuse his/her dominant hand. But, if the fetus were already rotatedsomewhat, either in the ROP or LOP position, then rotation should go “theshortest distance”. Therefore, an ROP should be rotated clockwise, and aLOP should be rotated counterclockwise. The hand should be used whichpronates during the rotation (like closing a book): left hand for ROP andright hand for LOP.4 (Category C)
Manual rotation is part of the “gentle art” of obstetrics. It is a neglectedskill, but one which requires no technology or instrumentation. Risk isminimal. With practice, confidence and skill improve. Successful manualrotation may shorten the second stage of labor and avoid instrumentation,or even a cesarean delivery.
(slide 11) 3. Vacuum Delivery – Vacuum delivery is an attractive option inpersistent OP presentation. The vacuum cup may safely be applied evenwhen the operator is not completely confident of the exact position of thehead, due to molding, edema, and overriding of sutures. The vacuum maysuccessfully draw the head out in the OP position. Alternatively, in flexingthe head and drawing it down against the levator sling, the vacuum maypromote rotation. Delivery will then occur in the OA position. The vacuumallows the fetal head to find its own best plane for delivery. Many operatorshave been startled to see the head rotate 180 degrees as they tract,sometimes in the very moment before delivery.
The vacuum cup should be placed as far posteriorly on the head aspossible to promote flexion. (See Chapter H. Assisted Vaginal Delivery) Nodirect rotary force should be applied to the cup, as this may cause “cookiecutter” type injury to the scalp, and also may cause the cup to disengage.The mechanism of delivery for an OP is the same with a vacuum as withforceps or a spontaneous delivery: the fetal vertex takes a more posteriorcourse through the pelvis. As with any vacuum delivery, the shaft of theextractor must be kept at right angles to the plane of the cup, ordetachment will occur.
G: Malpresentations, Malpositions, and Multiple Gestation5

(slide 12) 4. Forceps Delivery – The usual indications for forceps delivery apply.Forceps fit the occiput posterior vertex equally as well as the occiputanterior vertex. The mere presence of an OP presentation is not in itself asufficient indication for forceps use.
The mechanism of delivery is the same as for a spontaneous OP delivery.The head is actually born by flexion, not extension. The fetal face must passbeneath the symphysis before the head can flex upward, so traction on theforceps must be in a more posterior direction for longer than with OAdeliveries. Pressure on the perineum can be intense with resulting third andfourth degree lacerations.
Occasionally, with an occiput posterior and a prolonged second stage,severe molding and edema will occur. Then the fetal vertex will present inthe midpelvis or even on the perineum, but careful exam will reveal that thefetal head is very elongated and the biparietal diameter is not evenengaged. Under such circumstances attempts at operative delivery are notlikely to be successful, and may even be hazardous. Cesarean delivery isindicated, at which time the lack of engagement may be confirmed by theease with which the fetus is lifted out of the pelvis.
5. Forceps Rotation – Only skilled operators trained in the Scanzoni orKielland techniques should consider forceps rotation. In most Americanhospitals, these techniques are seldom practiced now. Cesarean deliveryshould always be the backup method of delivery for any OP presentationthat cannot be safely delivered vaginally.
Breech PresentationBreech presentation is defined as the fetal breech or buttocks presenting in the
(slide 13) birth canal, with the head aftercoming in the uterine fundus. Breechpresentations may be classified as follows:
• Frank breech: hips flexed and legs extended over the anterior surface ofthe body, occurring in 45 to 50 percent of breeches.
• Complete breech: (also called Full): hips and legs flexed (tailor sitting orsquatting), occurring in 10 to 15 percent of breeches.
• Footling breech: one or both hips and knees extended with one or both feetpresenting, occurring in 35 to 45 percent of breeches.
(slide 14) Breech presentation has many predisposing factors. Prematurity is commonlyassociated with breech, and as the fetus approaches term the incidence ofbreech drops to three to four percent.
G: Malpresentations, Malpositions, and Multiple Gestation6

7G: Malpresentations, Malpositions, and Multiple Gestation
Fetal Presentation at Various Gestational AgesModified from Scheer and Nubar5
Gestation (weeks) Percent breech
21 to 24 33 percent
25 to 28 28 percent
29 to 32 14 percent
33 to 36 9 percent
37 to 40 7 percent
Other predisposing factors include high parity and relaxation of the uterine andabdominal wall; uterine anomalies; pelvic tumors; polyhydramnios; oligohydramnios;various fetal anomalies including hydrocephalus, anencephaly, and Down Syndrome;macrosomia; multiple pregnancy; placenta previa; absolute cephalopelvicdisproportion; and previous breech. Because of these associated factors, a formalultrasound with a fetal anatomical survey is indicated when the diagnosis of breechis made in the mid-third trimester or later. Often, no cause is found.
DiagnosisThe diagnosis of breech can often be made by abdominal palpation and vaginalexam. On Leopold’s maneuvers, the firm, ballotable, rounded head is felt in thefundus.
On vaginal exam, either small parts or the breech itself may be detected. If smallparts are palpated, it is essential to distinguish between a hand and a foot.
The breech itself is smooth and rounded, and may feel remarkably like a vertex.Most childbirth providers have had the experience of “missing a breech” onvaginal exam. The key is to seek fontanels and sutures with the examining finger,which always signify a vertex. In breech presentation, the anus and ischialtuberosities form a straight line, whereas the mouth and malar prominences forma triangle. Additionally, the skin of the fetal buttock is smooth. An alert examinercan distinguish it from the hairy feel of the scalp. This subtle sign may raise anexaminer’s index of suspicion to perform a more definitive exam. If the examiner’sfinger encounters an orifice, then the finger can be gently inserted into the orifice.If it is the mouth, (signifying a face presentation) the fetus will suck on the finger.If it is the anus (signifying a breech), the finger will be coated with meconiumwhen withdrawn.

Prenatal Management of Breech(slide 15) There are four elements to the prenatal management of breech. First, a cause
must be sought for the breech presentation. Most of the causes of breechpresentation that can be identified are detectable by ultrasound. Secondly, thepatient may attempt certain exercises to turn the breech. Thirdly, external cephalicversion may be contemplated and attempted. Fourthly, failing successful version, adecision must be reached regarding the most favorable mode of delivery.
Postural Management of Breech Presentation (slide 16) Various exercises and positions have been tried in an attempt to turn a breech.
No difference in outcome has been noted in a review of trials in which womenwere randomized to either a postural management group or a control group.6, 7
(Category C)
The exercises themselves are simple. One version of the exercises is for thewoman to assume a knee-chest position for 15 minutes three times a day, for fivedays after the diagnosis of the breech. Another version is for the woman toassume a deep Trendelenburg position by elevating her hips nine to twelve incheswhile lying supine, for ten minutes once or twice a day. Pelvic rocking while ineither of these positions is often recommended.
While efficacy cannot be proven, these exercises do no harm, and they doprovide a focus of activity for an anxious gravida (and maternity care provider!).There are no contraindications to doing these exercises.
External Cephalic Version (ECV) External cephalic version, or turning a breech fetus to vertex by manipulationthrough the mother’s abdominal wall and uterus, has become an acceptedcomponent of the prenatal management of breech presentation. WilliamsObstetrics (20th Edition), the Cochrane Data Base, and ACOG Practice Bulletin(Feb. 2000 #13) all support ECV for breech presentations. 8,9,10 This procedure islow tech and low cost, can lower cesarean delivery rates, saving these womenfrom potential operative morbidity. The risk of an adverse event occurring as aresult of ECV is small, and the cesarean delivery rate is significantly lower amongwomen who have undergone successful version. Women near term with breechpresentations should be offered a version attempt. 9,10 (Category A)
The success rate of ECV, averaged from many studies, is 58 percent. In acomprehensive program of ECV, cesarean delivery for breech can be reduced by
(slide 17) half. Factors associated with success of ECV are: parity, frank breechpresentation, normal or increased amniotic fluid, and a relaxed uterus. Negativelyassociated with success are: nulliparity, obesity, oligohydramnios, anteriorplacenta, and low station of the breech. The operator’s skill and the patient’stolerance of the procedure also play a large role in success. Gestational age is
G: Malpresentations, Malpositions, and Multiple Gestation8

also a factor in the success rate. Prior to 37 weeks, the initial success is good,but reversion is common. Furthermore, if expedited delivery becomesnecessary, the fetus is premature. ECV after 37 weeks has a significantly lowersuccess rate. This gestational age appears to be optimal for ECV, as thesuccess rate is still good, the reversion rate back to breech is low, and, shouldimmediate delivery be necessary, the fetus is sufficiently mature.9,10 (CategoryA) ECV in early labor is difficult, although some success has been reported.
(slide 18) Several contraindications to ECV exist: multiple pregnancy (although ECV is agood potential management strategy for a breech second twin), non-reassuringfetal heart rate tracing, utero-placental insufficiency, uterine anomalies,placenta previa or unexplained bleeding, and maternal medical conditions suchas cardiac disease or pregnancy-induced hypertension. One small, randomizedstudy examined ECV in patients with previous cesarean delivery; success wasgood and uterine rupture did not occur.11
Various strategies have been employed to increase the success of ECV. Routinetocolysis appears to reduce the failure rate of external cephalic version at term.Although promising, there is not enough evidence to evaluate the use of fetalacoustic stimulation in midline fetal spine positions.12 There is not enoughevidence to evaluate the use of epidural analgesia or transabdominalamnioinfusion for external cephalic version at term.12
(slide 19) Complications of ECV are infrequent. Fetal bradycardia and decelerations arecommon, noted in 40 percent of cases, but usually resolve spontaneously orwith cessation of the procedure. Sporadic reports have been noted ofabruption, fetal hemorrhage, maternal hemorrhage, knotted or entangled cord,fetal mortality, and maternal mortality due to amniotic fluid embolism. A 1993report noted no fetal deaths since 1980.13 When performing ECV, facilities andpersonnel must be available for performing an immediate cesarean delivery.13
(Category C)
G: Malpresentations, Malpositions, and Multiple Gestation9

Procedure for External Cephalic Version (This is a sample protocol similar to many published protocols. Other variations exist.)
Preparation:• Patient may be accompanied by support person• Patient NPO (nothing by mouth)• Patient gowned, bladder empty• Confirm breech by ultrasound and rule out fetal anomalies• Perform NST (nonstress test) or BPP (biophysical profile)• Obtain consent• Cesarean delivery personnel and facilities available• Intravenous access• Tocolysis (recommended for primagravidas; optional for multiparas): 0.25 mg of terbutaline
(subcutaneous) 15 minutes before starting the procedure, or any approved tocolytic regimen• Position: supine, slight left lateral tilt, Trendelenburg, knees slightly bent • Abdomen coated with ultrasound gel
Procedure (for two operators)(slide 20) • Operator #1 elevates breech from pelvis by driving a hand suprapubically beneath the breech.
• Operator #1 pushes the breech into the iliac fossa.(slide 21) • Operator #2 flexes the head (for a forward roll), and rotates the fetus into an oblique lie.
• Two thirds of the force or pressure should be applied to the breech, and one third of the force shouldbe applied to the head. Avoid excessive force. Use a massaging motion when possible rather thandirect steady pressure.
• Both operators should rotate the fetus slowly around. Just enough force or pressure should be usedthat moves the fetus. Progress will occur in stages, or “cogwheel” fashion. The fetus will rotateslightly, then resist, then rotate more. Allow the mother and fetus brief rest periods when resistance isfelt, while attempting to maintain the progress already achieved.
(slide 22) • Monitoring may be by ultrasound or doppler, and should be performed every 30 seconds, duringrest periods.
(slide 23) • When the fetus is just past the transverse, it may rotate the rest of the way without effort,as it accommodates to the shape of the uterus
• The vertex may be guided gently over and into the pelvic inlet with suprapubic manipulation and fundalpressure.
(slide 24) • Ultrasound to confirm success. • After successful version, monitor for 20 to 30 minutes or until a reactive pattern occurs.• If the ECV is very easy, or if it is a second ECV after a fetus has reverted to breech, then a binder may
be placed on the abdomen to hold the fetus in place, and induction initiated.• In Rh negative patients, administer D-immune globulin (Rhogam ®); may obtain Kleihauer-Betke test.• If the forward roll fails, then try a backward flip, especially if the vertex and breech lie on the same
side of the maternal midline.• This procedure can be strenuous for the operators. A third operator can relieve the other two at
intervals.• If no success by 15 to 20 minutes, then discontinue the procedure.• If the patient feels sharp pain, stop the procedure.• If bradycardia occurs, stop the procedure. If it persists, then revert the fetus to its original breech
position. If the bradycardia still persists, then prepare for cesarean delivery.
G: Malpresentations, Malpositions, and Multiple Gestation10

Choosing Route of Delivery for BreechThe optimal route of delivery for breech infants has been the subject of muchcontroversy. Currently, in the United States, most breeches (well over 90 percentin some institutions and nearly all primagravidas) are delivered by cesareandelivery. However, rigorous support for this practice has been lacking in theliterature. Numerous studies have shown the safety of vaginal delivery forselected breeches. Additionally, cesarean delivery does not prevent all infantmorbidity, which, in some cases, arises from the same problems that caused thebreech presentation in the first place.14 A Cochrane review suggests thatadequate evidence does not exist to evaluate the use of a policy of plannedcesarean section for breech presentation.15 However, a multi-center,international, randomized controlled trial compared elective cesarean delivery tovaginal delivery for selected breech presentations: greater than 37 weeks, frankor complete breech, and less than 4000 grams estimated fetal weight.17,18 Thistrial was terminated early, in April 2000, after preliminary data analysis showedsignificant reduction in perinatal mortality and morbidity, and no increase inserious maternal complications, in the elective cesarean group.17
Two considerations, not strictly medical, enter into the decision regardingcesarean versus vaginal delivery. First, the skills to perform a safe vaginal breechdelivery are not being taught in many residencies, and practitioners who retainthese skills are aging. Second, the medical-legal ramifications of vaginal deliveryare prohibitive in the minds of many.
(slide 25) Certain contraindications exist for elective vaginal delivery of breech infants:• Unfavorable pelvis: if the pelvis is known to be small, or if it is android or
platypelloid, vaginal delivery should not be attempted. X-ray or CTpelvimetry have not been shown to improve outcomes for breech births.
• Macrosomia (defined variously, from 3800 grams upward).
• Severe prematurity (defined variously).
• Intrauterine growth restriction or evidence of placental insufficiency.
• Footling breech.
• Hyperextension of the fetal head: delivery can be difficult, and labor canresult in neurological injuries with a hyperextended head. An X-ray of theabdomen may be necessary to determine the attitude of the fetal head.
• Fetal anomalies such as hydrocephalus.
• Nuchal arm: again an x-ray is required to diagnose this condition.
• Absence of labor, as in premature rupture of membranes, or non-progressive labor: induction and augmentation of labor are controversial inthe literature, but often avoided in favor of cesarean delivery.
• Lack of a physician with the experience and skill necessary for vaginaldelivery.
G: Malpresentations, Malpositions, and Multiple Gestation11

Various scoring systems have been developed to predict outcome of vaginalbreech delivery. The best known of these systems is the Zatuchni-AndrosPrognostic Scoring Index. It awards points for parity, gestational age less than 37weeks, estimated fetal weight less than seven pounds, previous breech delivery,dilation at presentation, and station at presentation.16 This system has severalfaults, among them rewarding prematurity, and also rewarding the gravida whostays home to labor, thus presenting at a greater dilation and lower station.However, no better-validated system of predicting breech outcome has beendeveloped.
In summary, the decision as to the best mode of delivery of a breech iscomplicated. Many factors must be taken into account, including the bestconclusions from the medical literature, community and national standards, thespecifics of each individual case, the patient’s wishes, and the skill of the operator.
Labor and DeliveryPresented here is a standard method of delivering a breech per vagina.Variations of this method exist. ALSO® offers this technique as not necessarilythe only one, nor even the best, but one which is widely accepted by Americanpractitioners and which can be learned and practiced on the mannequin. ALSO®
acknowledges that vaginal breech deliveries do occur, sometimes emergentlyunder circumstances in which cesarean delivery or consultation are not possible.Therefore, every obstetric provider should have a working knowledge of how todeliver a breech.
(slide 26) There are fundamental differences in delivery between cephalic and breechpresentations. With cephalic or vertex presentation, the largest part of the fetus,the head, delivers first. Molding of the cranium can occur over several hours.With a breech delivery, first the breech, then the shoulders, then the headdelivers, each larger and less compressible than the previous part. Molding of thehead has no opportunity to occur because the fetal head is in the pelvis only for afew minutes, and because it enters the pelvis with the base of the skull leading,which, unlike the vertex, cannot mold. The great challenge of the vaginal breechdelivery is that the last part of the fetus to deliver is also the largest part, and itmight not fit through the pelvis.
G: Malpresentations, Malpositions, and Multiple Gestation12

Labor with a breech is not very different from labor with a vertex, and may beallowed to continue spontaneously as long as progressive dilation and descentoccur, and there is no fetal or maternal compromise.
A frank breech will distend the perineum and dilate the introitus in a mannersimilar to a vertex. Episiotomy is often recommended. While episiotomy will notcreate more room in the bony pelvis, it will enable the operator to perform variousmanipulations more easily, including emergency procedures such as Piperforceps application. Episiotomy is very difficult to perform once the whole body isout.
(slide 27) The frank breech usually delivers with the axis of the hips in the AP plane, and thefetal sacrum will either be to the left or the right. Usually, the anterior hip descendsto the introitus and passes below the symphysis in a manner analogous to theanterior shoulder. Then with lateral flexion of the fetal body, the posterior hipdelivers over the perineum. The operator may support the perineum with a Ritgen-type maneuver, or the breech may be allowed to deliver spontaneously. Externalrotation follows delivery of the breech, allowing the infant’s back to turn anteriorly.
Delivery should proceed spontaneously until the fetal umbilicus appears at theintroitus. The mother should be making strong, but controlled, pushing efforts atthis point in the delivery. Traction by the operator prior to delivery of the umbilicusmay promote extension of the fetal head or nuchal placement of the arms. Do notpull on the fetus until the umbilicus is delivered, and, even then, traction is notnecessary if the delivery continues to progress.
When the umbilicus delivers, a loop of several inches of cord should be gentlypulled down. This prevents tension on the cord as the body delivers, and alsoallows easy monitoring of the fetal pulse by palpation.
(slide 28) The legs of a frank breech may be delivered by inserting a finger behind the kneeto flex the knee and abduct the thigh. Active efforts to deliver the legs are notmandatory, as the legs will deliver spontaneously and the feet will “spring” freeeventually. Delivery of the legs in this manner can be accomplished, before thebreech has delivered, by a skilled practitioner who is attempting a total breechextraction.
(slide 29) After the umbilicus is born, gentle downward traction may be used to deliver theinfant’s torso. The fetus may be grasped by the operator’s fingers on the fetalpelvis, with thumbs on the sacroiliac regions. This avoids placing the hands toohigh on the fetus and injuring abdominal organs such as the spleen or liver.Traction should be in a 45-degree downward axis, toward the floor. It is helpful forthe operator to assume a position below the fetus, as for example on one knee infront of a delivery room table.
The fetal trunk may deliver quickly and without operator effort, or considerableeffort may be required to deliver the trunk. Rotation of the fetal back from oneanterior oblique to the other anterior oblique may be helpful in extracting the
G: Malpresentations, Malpositions, and Multiple Gestation13

trunk, and it also encourages the fetal arms to gather in a flexed position acrossthe chest. This rotatory maneuver carries an eponym in Great Britain, where it iscalled the Lovsett maneuver. Of critical importance is keeping the back up duringthe delivery, which allows the fetal head to enter the pelvis occiput anterior. If thefetus rotates abdomen up, the fetal head will present very unfavorable diametersto the maternal pelvis, severely jeopardizing safe delivery.
(slide 30) Delivery of the arms is accomplished by rotating the fetal body into the oblique.The tip of the fetal scapula will come into view, usually quite easy to identifybecause it is “winged.” The anterior arm may then be swept down across thefetal chest and out of the introitus. If possible, the humerus should be splintedwith two fingers rather than simply hooking the antecubital fossa with a finger.Rotation of the fetus into the opposite oblique allows delivery of the opposite armin a similar fashion.
Delivery of the head follows, and is potentially the most difficult and hazardouspart of the breech delivery. The head must be born by flexion through the pelvis.When the breech head is flexed and occiput anterior, and then passes throughthe birth canal by further flexion, the same favorable diameters are presented tothe pelvis as in the case of a vertex occiput anterior delivery.
(slide 31) A modification of the Mauriceau Smellie Veit (MSV) maneuver is recommended todeliver the head by flexion. Everything about the MSV maneuver is designed topromote flexion. One of the operator’s hands should be placed above the fetuswith one finger inserted into the vagina and placed on the occiput, and one fingeron each of the fetal shoulders. The other hand is placed beneath the fetus. Theclassical MSV maneuver describes placing a finger in the mouth, but this is notrecommended because traction on the jaw can cause dislocation. As analternative, two fingers may be placed on the maxillae. A very competentassistant should follow the head abdominally, and be prepared to applysuprapubic pressure to flex the head through the pelvis. The fetus may bewrapped in a sling that is also held by an assistant, or may be draped on theoperator’s lower arm.
Delivery of the head then commences. The head is flexed through the pelvis byfour separate mechanisms: the occipital finger applies flexing pressure on theocciput; the assistant applies suprapubic pressure on the occiput as well; thefingers on the maxillae apply pressure on the lower face, which tends to promoteflexion. The fetal body is raised upward by the sling in a large arc. While strong,controlled expulsive efforts by the mother are most helpful, some traction is alsorequired for the delivery. This is accomplished by downward pressure of thefingers on the shoulders. The assistant holding the fetus by a sling may also holdthe feet, and pull gently as the body describes its arc. The fetal body should stayin a neutral position with regard to the head, avoiding hyperextension. Ultimately,the body becomes upside down and vertical, and at this point an assistant musthold the feet to prevent the fetus from falling on the floor.
G: Malpresentations, Malpositions, and Multiple Gestation14

As the mouth and nose appear over the perineum they may be suctioned. Thecranial vault then delivers by further flexion. The operator may use a Ritgentechnique on the perineum. As the head finally emerges, the infant’s body actuallyflips over past vertical onto the mother’s abdomen.
Extraction of a breech at cesarean delivery requires maneuvers similar to thoseused in vaginal birth. Thus cesarean delivery of a breech gives an opportunity forthe surgeons to practice. The goal of cesarean delivery with a breech is to afforda gentle delivery. If the uterine or abdominal incisions prove to be too small foreasy delivery, they can be enlarged. This is not an option during vaginal birth.
Piper ForcepsPiper forceps are specifically designed to deliver the aftercoming head of abreech. They are very long, and have an axis traction curve built in. It isimpossible to determine if a Piper application is “good” or “bad” on the fetal skull.Therefore, they are always applied the same way: straight to the maternal pelvisas if the position were OA. The blades are springy and grasp the fetal head in anon-specific basket catch that has proved safe and effective.
Forceps are indicated when the MSV maneuver fails. Although strict guidelinesare lacking, one should consider Piper forceps if two or three minutes havepassed without progress while attempting the MSV maneuver. Pipers may also beapplied prophylactically if a fetus is believed to be fragile, such as a prematurefetus. It is prudent to have the Pipers readily available for any vaginal breechdelivery, but in an emergency, any forceps will do.
To apply Pipers, the fetus (including the arms) is wrapped in a sling and gentlyheld up and to the operator’s left. The left blade is always applied first. It is held inthe operator’s left hand and is applied to the left side of the mother’s pelvis (but tothe right side of the fetus). Unlike other forceps applications, the operator holdsthe handle in a horizontal position and below the fetus. The right hand is placed inthe vagina alongside the fetal head to protect the vaginal sidewalls. Then theforceps blade is insinuated between the right hand and the fetal head, followingthe cephalic curve of the blade around the head. Once inserted, the handle maybe allowed to dangle or may be supported by an assistant.
The right blade is then inserted in a similar fashion, by grasping the handle withthe right hand and sliding the blade into the vagina alongside the head, whileprotecting the sidewall with the left hand. The forceps should then be locked.When the right blade is applied over the left blade the lock will articulatenormally. The handles are usually separated slightly away from the lock, andshould not be squeezed together. Since the operator cannot determine how theblade is applied to the fetal skull and face, no effort is made to do so.
With the application completed, delivery of the head may commence. Theoperator applies a small amount of traction to the forceps. Since the shanks of
G: Malpresentations, Malpositions, and Multiple Gestation15

the forceps have a large axis traction curve built in, no special maneuvers such asthe Pajot maneuver are required to ensure that traction is in the correct vector. Theprimary motion of the forceps is to raise the handles in a large arc, starting abouthorizontal and ending at or past vertical. This arc will flex the head through thepelvis with exactly the same geometry as the MSV maneuver, but with greatlyincreased leverage due to the length of the forceps. None of the flexing maneuversof the MSV maneuver are required when the Pipers are used. The fetus may beheld in the sling or laid on the shanks of the forceps during the delivery.
The principal difficulty in applying Pipers is a result of the condition that indicatestheir use: that is, failure of the MSV maneuver implies a tight fit of head to pelvis.There may be insufficient room to place a hand alongside the head. In thissituation the blade must be applied “blind” with risk of injury to mother and fetus.Once the Pipers are on, delivery can be accomplished in almost every case.
Complications of Breech DeliveryA nuchal arm may occur, that is, one or both arms may be extended upwardbehind the neck, which may impede delivery of the head. In this event there arethree delivery options. If the fetus is small or the pelvis large, the head andextended arm may be delivered together. Alternatively, the operator may attemptto flex the arm and sweep it down over the face and chest. As a maneuver of lastresort the operator may rotate the fetus 360 degrees in the direction that willsweep the arm out of its nuchal position (clockwise for a left nuchal arm,counterclockwise for a right nuchal arm).
Entrapment of the aftercoming head by the cervix is another serious complicationof breech delivery. This situation occurs primarily in premature and footlingbreeches in which the body has slipped through an incompletely dilated cervix.The head, being the largest part, becomes entrapped by the cervix. The problemis most severe in a nulliparous woman, whose cervix has never been fully dilated.
(slide 32) Resolution without excessive traction may require cutting the cervix, a procedureknown as Dührssen’s incisions. Ring forceps are placed in pairs, parallel to eachother at 2:00, 10:00 and if possible 6:00, extending three to four centimeters intothe cervix. A radial incision is made between the ring forceps of each pair.Anesthesia and exposure are major technical problems, and hemorrhage is amajor potential complication. This procedure is recommended only in the mostextreme life-threatening circumstances.
Hydrocephalus may present as a breech delivery with an entrapped head. Theappearance of a meningomyelocele or spina bifida may herald the hydrocephalus,occurring in about a third of such cases. Although prenatal diagnosis will call forhighly individualized management and probable cesarean delivery, theunexpected diagnosis at the time of a breech delivery presents a significant
G: Malpresentations, Malpositions, and Multiple Gestation16

dilemma. Decompression of the fetal ventricles or cephalocentesis may beprejudicial to the fetus, but the only way for the delivery to be completed. Thisprocedure may be accomplished with a long needle either transvaginally ortransabdominally.
Transverse Lie or Shoulder PresentationIn transverse lie the long axis of the fetus is approximately perpendicular or atright angles to that of the mother. In the back down transverse lie or shoulderpresentation, the shoulder is over the pelvic inlet, the head is lying in one of theiliac fossae, and the breech in the other. Transverse lie can also occur in theback up orientation, most commonly in the second twin. Occasionally an unstableor oblique lie will be noted, in which the fetus changes from a breech or vertex toa transverse lie or assumes an intermediate lie.
Transverse lie occurs in about 0.3 percent of singleton births. The commoncauses of transverse lie are: unusual relaxation of the abdominal wall, pretermfetus, placenta previa, abnormal uterus (e.g. subseptate), contracted pelvis, tumoroccluding the birth canal, and polyhydramnios.
DiagnosisThe diagnosis of transverse lie is usually easily made by palpation. No presentingpart will be felt suprapubically, and the head will be felt in the iliac fossa. Onvaginal exam the pelvis will be empty. Imaging can confirm the diagnosis.
Mechanism of Labor and Management of DeliverySpontaneous birth of a full term fetus is impossible. Therefore, cesarean deliveryis mandatory in most cases. If transverse lie is encountered before the onset oflabor and rupture of membranes, an attempt at external cephalic version isreasonable assuming there are no contraindications to vaginal delivery, such asplacenta previa.
If a fetus presents with a back-up transverse lie and a fully dilated cervix, such asmight be the case with a second twin, then either external cephalic version orinternal podalic version may be contemplated. This is described in the section onmultiple gestation.
(slide 33) When labor ensues with a back down transverse lie, the shoulder is forced intothe pelvis, and an arm may prolapse. With continued labor a retraction ringdevelops. Ultimately, in a neglected labor, the uterus ruptures and the mother andfetus risk death. This scenario is rarely seen in modern obstetrics but may beencountered in parts of the world where access to care is a problem.
G: Malpresentations, Malpositions, and Multiple Gestation17

Cesarean delivery for a back down transverse lie may require a low verticalincision in order for the operator to successfully deliver one of the fetal polesthrough the uterine incision.
Face PresentationIn a face presentation, the head is hyperextended so the occiput is in contactwith the fetal back, and the face is the presenting part. The fetal skull diameterthat presents to the pelvis is the submentobregmatic, which is favorable fordelivery in most cases. The reference point on the fetus is the chin (mentum).Face presentation occurs in 0.1 to 0.2 percent of singleton deliveries.
The causes of face presentation are numerous and often obscure. When the fetusis very large or the pelvis is contracted, there is a predisposition to extension ofthe fetal head. The pendulous abdomen of a grand multipara also promotesextension of the fetal head. In exceptional instances, enlargement of the neckbecause of goiter or cystic hygroma, or numerous coils of cord around the neckmay cause extension. Anencephalic fetuses often present by the face because ofabsent development of the cranium.
DiagnosisThe clinical diagnosis of a face presentation relies principally on the vaginalexam. The mouth, nose, and the malar prominences may be palpated. A facepresentation may be confused with a breech presentation, particularly sincebreech is 20 times more common. The mouth may be mistaken for the anus, andthe malar prominences mistaken for the ischial tuberosities. The anus and ischialtuberosities of a breech form a straight line, whereas the mouth and malarprominences of a face form a triangle. The exam may be very confusing due toedema of the facial structures, even for the most experienced practitioner.Imaging will confirm the diagnosis and rule out anencephaly.
Mechanism of Labor(slide 34) The key for successful delivery of a face is for the chin to end up under the
symphysis, or be in mentum anterior position. Then, with further descent of thefetus, the cranial vault can sweep through the posterior pelvis and the head canbe born by flexion.
Although this mechanism does not present the most favorable diameter of thefetal head to the pelvis, if the fetus is not too large and the pelvis is adequate,spontaneous delivery can occur. If the chin rotates or remains posteriorly
(slide 35) (mentum posterior) then there is no mechanism that allows the fetus to utilize thespace in the posterior pelvis in the hollow of the sacrum, and delivery cannot occur.
G: Malpresentations, Malpositions, and Multiple Gestation18

Management of DeliverySpontaneous vaginal delivery may occur sometimes with surprising ease. Thefetus must rotate to a mentum anterior position. A persistent mentum posteriormandates a cesarean delivery. Attempts to manually convert a face to a vertexare outmoded and dangerous, as are attempts to rotate a mentum posterior to amentum anterior. Forceps however, can be safely and successfully applied to amentum anterior that is on the perineum. The vacuum extractor is absolutelycontraindicated. Likewise, scalp electrode internal monitoring is contraindicated,to avoid injuring the face. Oxytocin augmentation should be used only withextreme caution, and is usually considered contraindicated. A large episiotomymay be recommended to accommodate the vertex coming through the posteriorpelvis. Parents should be prepared for the dramatically bruised and edematousface of the infant, but recovery is prompt.
Brow PresentationIn a brow presentation the portion of the fetal head between the orbital ridge andthe anterior fontanel presents at the pelvic inlet. The fetal head is in an attitudebetween full flexion and full extension (or face). The presenting diameter of thefetal skull is the occipitomental, which is very unfavorable for delivery. Delivery ofa persistent brow usually cannot take place unless the fetus is very small or thepelvis is very large.
Brow presentation is found in 0.02 percent of singleton deliveries. The causes ofthis rare presentation are similar to those for face presentation. A browpresentation is usually unstable and will convert either to a face or a vertexpresentation.
DiagnosisDiagnosis is by vaginal exam. The frontal sutures, anterior fontanel, orbital ridges,eyes, and root of the nose may be felt. Frequently the exam is confusing becauseof edema and unfamiliarity of the presenting features.
Mechanism and Management of Labor A persistent brow cannot deliver vaginally under normal conditions. If it convertsto vertex or face, then delivery may occur according to their respectivemechanisms. In the absence of conversion and progress in labor, cesareandelivery is required.
G: Malpresentations, Malpositions, and Multiple Gestation19

Compound Presentation(slide 36) In a compound presentation an extremity, usually a hand, prolapses alongside the
main presenting part, usually the head. Compound presentation occurs in 0.04 to0.14 percent of deliveries. Often no cause is found. It is more common withpremature infants and when the fetal presenting part does not completelyocclude the pelvic inlet.
DiagnosisThe diagnosis is usually readily made on vaginal exam. It is critically important todistinguish between a hand and a foot prolapsed alongside the head.
Management of DeliveryAs long as labor is progressing normally, no intervention is necessary. Mostcommonly the prolapsed limb will deliver spontaneously along with the head, orsometimes the fetus will retract its limb spontaneously. If the prolapsed armappears to be impeding descent, it should be gently elevated upward and thehead manipulated simultaneously downward.1 (Category C) Occasionallycesarean delivery will be necessary. The parents should be warned to expectbruising and edema of the prolapsed extremity.
Prolapse of the Umbilical Cord(slide 37) Prolapse of the umbilical cord is a true obstetrical emergency. The cord may
become compressed or occluded between the presenting part of the fetus andthe pelvic brim or sidewall resulting in asphyxia and death. The incidence of cordprolapse is 0.4 percent in vertex presentations, 0.5 percent in frank breeches, fourto six percent in complete breeches, and 15 to 18 percent in footling breeches.
(slide 38) Cord prolapse is most common when the fetus does not occlude the pelvic inletwell, as is the case with a footling breech. Other factors that may contribute tocord prolapse are prematurity, polyhydramnios, high presenting part, and a longcord. Occasionally the cause is iatrogenic, as for example when the membranesare ruptured with the presenting part high out of the pelvis. A gush of fluid maythen wash the cord down into the vagina. On the other hand, the cord may havealready been coiled beneath the fetal presenting part (occult cord prolapse) suchthat rupture of the membranes merely revealed the prolapse, but did not cause it.
(slide 39) Rapid identification and response may truly save the life of the fetus. Themanagement steps are:
1. Diagnose the cord prolapse by visual inspection or palpation on immediatevaginal exam. The cord may be found extruded from the vagina, coiled in thevagina, or wrapped across the presenting part. The only hint may be a severevariable deceleration or bradycardia following rupture of the membranes.
G: Malpresentations, Malpositions, and Multiple Gestation20

2. Quickly assess the fetal status by monitoring or ultrasound.
3. Assess the dilation and status of labor. If the fetus can be delivered morequickly and safely per vagina than by cesarean delivery, then proceedimmediately using forceps, vacuum or total breech extraction asappropriate.
4. If immediate vaginal delivery is not feasible then prepare for cesareandelivery. Elevate the presenting part out of the pelvis in an effort to protectthe cord from occlusion. This may be performed by placing a hand in thevagina and forcefully (but carefully) elevating the presenting part upward.Alternatively, some success has been achieved by filling the bladder rapidlywith 500 to 700 cc of saline. Tocolysis (e.g. terbutaline 0.25 mgsubcutaneously) is helpful if the patient is in labor. Deep Trendelenburgposition also is useful to add gravity to other efforts to elevate the fetus offthe cord. The efficacy of these maneuvers can be measured by monitoringthe fetus or palpating the cord.
5. Do not attempt the futile tactic of attempting to replace the cord in theuterus.
6. Perform an emergent cesarean delivery while continuing all efforts to holdthe presenting part off the cord.
7. If delay is encountered, wrap the cord in warm wet packs.
(slide 40) Prevention of cord prolapse is difficult but may be accomplished on occasion byidentifying risk factors or by identifying a cord presentation by ultrasound.Artificial rupture of the membranes should not be done when the station is high. Ifartificial rupture of membranes is essential to manage a difficult obstetricsituation, and the head is unengaged and high, the membranes can be needledunder double set-up conditions. The same procedure can be used to rupture themembranes in cases of polyhydramnios.
Patients in the latter stages of pregnancy who are at high risk for cord prolapse(e. g. footling breech, polyhydramnios) can be identified. They can be instructedto examine themselves for cord prolapse if their membranes rupture out ofhospital. If a prolapse is identified, they should assume a deep knee-chestposition and maintain the position even during transport to the hospital.
G: Malpresentations, Malpositions, and Multiple Gestation21

Multiple Gestation(slide 41) Multiple gestation occurs in approximately 1.5 percent of births in the United
States. Perinatal morbidity and mortality are increased two to five fold, largelydue to prematurity. Congenital anomalies, IUGR, and intrapartum complicationsalso contribute. Dizygosity (fraternal twinning) occurs in about two thirds of twingestations, and is increased with age, parity, and certain familial and racialcircumstances. Monozygosity (identical twinning) occurs in one third of twingestations and is unrelated to any predisposing factors. Morbidity and mortalityare higher in monozygotic twins.
Maternal complications are common in multiple gestation. These includepregnancy induced hypertension, anemia, hyperemesis, abruption, placentaprevia, postpartum hemorrhage, and increased operative delivery.
DiagnosisThe routine use of ultrasound has greatly diminished the difficulties of diagnosing
(slide 42) multiple gestation. Historical and physical findings suggestive of multiplegestation and indicating an ultrasound exam are: uterus larger than dates,hyperemesis gravidarum, early PIH, elevated maternal serum alpha feto-protein(MSAFP), suggestive palpatory or auscultory findings, polyhydramnios, ovulationinduction, and family history.
Prenatal Management(slide 43) Several issues distinguish multiple gestations from singleton pregnancies:
1. Prematurity is the greatest threat to multiple gestation infants, andprevention of prematurity is of the highest priority. Unfortunately, nopreventive measures, including bed rest and tocolytics, have been clearlyeffective in preventing premature labor. The best approach appears to beattentive general support.
2. Compared to singletons, congenital anomalies and developmental defectsare doubled in all twin pregnancies, and higher yet in monozygotic twinpregnancies. Ultrasound, and in some cases amniocentesis, should beconsidered. Monoamniotic twinning, which may be diagnosed byultrasound, presents a very high risk situation due to cord entanglement.
3. Compared to singletons, pregnancy induced hypertension is doubled in twingestations. Active surveillance and management are recommended. Irondeficiency is common, and iron supplementation is generally indicated. Thepossibility of intrauterine growth restriction (IUGR) and discordant growthrequires surveillance. IUGR has been reported from 12 to 47 percent anddiscordancy from four to 23 percent, depending on the standard used (15 to25 percent difference in weight using the larger twin as reference).
G: Malpresentations, Malpositions, and Multiple Gestation22

23G: Malpresentations, Malpositions, and Multiple Gestation
Ultrasound exams every four weeks are recommended for early diagnosis.Intervention in the presence of significant discordancy is a complicatedissue, and beyond the scope of this chapter.
4. Fetal death occurs in 0.5 to 6.8 percent of twin pregnancies. Conservativemanagement of the surviving twin is indicated, at least until lung maturity isproven. The patient should be monitored for development of coagulopathy.
5. The incidence of placenta previa is increased in multiple gestations,possibly because of the larger surface area of the two placentas.
Certain complications of pregnancy do not seem to be increased in multiplegestations. These include diabetes, pyelonephritis, and third trimester bleeding.
Intrapartum management No obstetric situation presents a greater range of challenges than multiplegestation. Only the most skilled and confident obstetric providers should plan toattend twin deliveries without backup.
Intrapartum complications include malpresentations, locking of twins, cordprolapse, abruption, non-reassuring fetal heart rate tracing, dysfunctional labor,and postpartum hemorrhage. Several of these complications can arise from themanner in which the twins present. Either fetus may be vertex, breech or in atransverse lie. Theoretically there are nine combinations of presentation of twins
(slide 44) A and B, but for practical purposes there are three.
Presentation of Twins
Twin A Twin B Occurrence (percent)
Vertex Vertex 43 percent
Vertex Non-vertex 38 percent
Non-vertex NA 19 percent
Vertex-vertex presentations are the most common and least complicated. Withappropriate monitoring and the capability to respond to an emergency, labor maybe allowed to progress to vaginal delivery of both infants. Oxytocin induction oraugmentation, epidural anesthesia, and other interventions are all acceptablewith caution. The interval between deliveries is not critical as long as the secondfetus is doing well, but oxytocin augmentation is often used when delay isencountered between deliveries.
When twin A is vertex, but twin B is non-vertex, controversy exists as to the bestmode of delivery. Although many practitioners advocate cesarean delivery, it isnot always necessary in this situation. Vaginal delivery of twin B in the nonvertexpresentation is a reasonable option for a neonate with an estimated weight

greater than 1,500 gm as long as criteria for vaginal delivery of a singleton breechare met.19 Cesarean delivery of a second twin not presenting cephalically has yetto be demonstrated to improve neonatal outcome.20 (Category A) A policy ofroutine cesarean delivery should not be adopted without further controlled trials.
(slide 45) When vaginal delivery is attempted, the crisis point occurs after the delivery oftwin A, at which time the physician must determine the presentation of twin B(which may be different from its presentation before twin A was born). Acombination of external exam, internal exam, and ultrasound may be used.Assuming twin B is breech or in a transverse lie, a decision must then be madewhether to 1) attempt an external version to vertex; 2) deliver twin B as a breech;or 3) perform a cesarean delivery. The exact obstetric circumstances, theexperience of the operator, condition of the fetus, state of mind of the mother, andthe available resources are all factors in the decision.
External cephalic version is frequently successful, easy, and safe, as the uterus isoften very relaxed after delivery of twin A, and there is plenty of room for twin Bto turn. Once the vertex has been placed over and guided into the inlet manually,the membranes can be ruptured or oxytocin augmentation given (or both) and avertex delivery should ensue.
A breech delivery is also a possibility for twin B. This may be inadvisable for verysmall fetuses, but macrosomia with difficult delivery is rarely a problem in thesecond twin. Breech delivery is a reasonable choice in the followingcircumstances:
1. When external version is unsuccessful or not attempted
2. When labor is strong and the second fetus presents with the breech deepin the pelvis, in which case external version is not likely to succeed andprompt delivery is anticipated
3. When emergencies such as cord prolapse or a non-reassuring FHR tracingoccur, and a skilled operator is available to perform a breech extraction.
Occasionally twin B presents as a transverse lie with the back up and the feetdangling towards the cervix. In this situation, a procedure known as internalpodalic version may be appropriate. The operator grasps both feet firmly throughthe membranes and pulls the feet into the vagina. An assistant helps rotate thefetus into proper position abdominally. With the operator exerting steady downwardtraction on the feet to maintain the breech as the presenting part, the membranesare then ruptured. The delivery then proceeds as a breech. This is probably themost difficult and dangerous procedure permissible in modern obstetrics.
G: Malpresentations, Malpositions, and Multiple Gestation24

Cesarean delivery may be required for a non-vertex twin B. Situations mandatingCesarean delivery include a non-reassuring fetal heart tracing, cord prolapse,abruption, or rupture of the membranes trapping the fetus in a transverse lie. Acontributing problem occurs when the cervix “closes down” after twin A is born.These situations can arise suddenly, so resources for immediate cesareandelivery should be available.
When twin A is non-vertex, cesarean delivery is generally required for safety.External cephalic version of a breech twin A is not technically feasible. Whentwin A is breech and twin B is vertex or transverse, locking or collision of thetwins is a disastrous event.
Cesarean delivery in multiple gestation presents anesthetic and surgicalchallenges due to the enlarged uterus, the exaggerated physiologic response topregnancy, and the potential for exotic presentations of the fetuses. Thenecessity for a vertical incision in both skin and uterus is a special considerationwhen the twins are in unusual or entwined positions. Conjoining of twins is a rareproblem beyond the scope of this chapter, but should always be considered ifultrasound shows twins “face to face” or “back to back.”
Undiagnosed twins are rare in areas where ultrasound is frequently used.However, in the pre-ultrasound era, as many as 50 percent of twins wereunsuspected until after delivery of twin A. Therefore, when no ultrasound hasbeen performed, birth attendants should always be alert for this possibility.
After delivery, postpartum hemorrhage is relatively common due to theoverdistension of the uterus. Providers should be fully prepared with intravenousaccess, proper oxytocics, and readily available blood products.
Neonatal resuscitation is often required due to prematurity or the many potentialcomplications of multiple gestation. Not uncommonly, two infants need attentionsimultaneously. Adequate personnel and equipment must be available.
(slide 46) Summary There are six types of malpresentations. Some are common (occiput posteriorpresentation, breech) and some are rare (transverse lie, brow, face, compoundpresentation). Diagnosis is made by a combination of physical examination andimaging. A high index of suspicion is helpful in making the diagnosis. Each type ofmalpresentation has its complications. Providers should be alert not only forcomplications resulting from labor and delivery, but also for problems that may beetiologic for the malpresentation in the first place.
Vaginal delivery may be considered for four of the six malpresentations: occiputposterior presentation, breech, face, and compound presentation. With occiputposterior presentation, the provider has several management choices for delivery.With breech, complex criteria determine if vaginal delivery can occur safely.
G: Malpresentations, Malpositions, and Multiple Gestation25

External cephalic version can prevent breech presentation at term. A high degreeof technical skill and judgment is required to deliver patients withmalpresentations safely. Multiple gestation presents a wide variety of specialchallenges to the provider.
Summary of Recommendations
Category AWomen with breech presentation who meet standard criteria near term should beoffered an attempted external cephalic version.9,10,12
Caesarean section for delivery of a second twin not presenting cephalically as yethas not identified improvement in neonatal outcome.20
Category BThirty seven weeks appears to be the optimal gestational age for ECV.9,10
Cesarean delivery does not prevent all infant morbidity in breech presentation.14,15
Category CThe conduct of labor and delivery with a persistent OP is not markedly differentfrom that of the fetus in the occiput anterior position.1
In an OP rotation, the hand should be used which pronates during the rotation(like closing a book): left hand for ROP and right hand for LOP.4
Various exercises and positions have been tried in an attempt to turn a breechand no difference in outcome has been noted in either a postural managementgroup or a control group.6,7
When performing ECV, facilities and personnel must be available for performingan immediate cesarean delivery.13
There is insufficient evidence to recommend routine tocolysis for ECV formultiparous patients.12
In a compound presentation, if the prolapsed arm appears to be impeding descentit should be gently elevated upward and the head manipulated simultaneouslydownward.1
G: Malpresentations, Malpositions, and Multiple Gestation26

References
1. Cunningham, MacDonald, Gant, et al (eds). Williams Obstetrics, 20th Edition, 1997; Appleton & Lange,Stamford, CT, Chapter 18: Dystocia – Abnormal presentation, position, and development of the fetus. pp448-449. (Level III)
2. Cruickshank DP. Malpresentations and Umbilical Cord Complications. In: Danforth's Obstetrics andGynecology, Sixth edition, Scott JR, DiSaia PJ, Hammond CB, and Spellacy WN (eds); J.B LippincottCompany, 1990. (Level III)
3. Pearl ML, Roberts JM, Laros RK, and Hurd WW. Vaginal delivery from the persistent occiput posteriorposition. Journal of Reproductive Medicine 1993;38(12):955-960. (Level II-2)
4. Cunningham, MacDonald, Gant, et al (eds). Williams Obstetrics, 20th Edition, 1997; Appleton & Lange,Stamford, CT, Chapter 18: Dystocia – Abnormal presentation, position, and development of the fetus. pp482-483. (Level III)
5. Scheer K, Nubar J: Variation of fetal presentation with gestational age. Am J Obstet Gynecol1976;125:269. (Level III)
6. Hofmeyr GJ, Kulier R. Cephalic version by postural management for breech presentation (CochraneReview). In: The Cochrane Library Issue 3, 1999. Oxford: Update Software. (Level I)
7. Smith C, Crowther C, Wilkinson C, Pridmore B, and Robinson J. Knee-chest postural management forbreech at term: A randomized controlled trial. Birth 1999;26(2):71-75. (Level I)
8. Cunningham, MacDonald, Gant, et al (eds). Williams Obstetrics, 20th Edition, 1997; Appleton & Lange,Stamford, CT, Chapter 18, pp 442-443. (Level III)
9. Hofmeyr GJ, Kulier R. External cephalic version for breech presentation at term (Cochrane Review). In:The Cochrane Library, Issue 3, 1999. Oxford: Update Software. (Level I)
10. External Cephalic Version. ACOG Practice Bulletin, Feb. 2000; No.13:1-6. (Level III)
11. Flamm BL, Fried MW, Lonky NM and Saurenman Giles W. External cephalic version after previouscesarean delivery. Am J Obstet Gynecol 1991;165(2):370-372. (Level II-2)
12. Hofmeyr GJ. External cephalic version facilitation for breech presentation at term. The Cochrane Library,Issue 1, 2000. Oxford: Update Software. (Level I)
13. Zhang J, Watson AB, and Fortney JA. Efficacy of external cephalic version: A review. Obstetrics &Gynecology 1993;82(2):306-312. (Level III)
14. Danielian PJ, Wang J, and Hall MH. Long term outcome by method of delivery of fetuses in breechpresentation at term: Population based follow up. Br Med J 1996;312:1451-1453. (Level II-2)
15. Hofmeyr GJ, Hannah ME. Planned Caesarean section for term breech delivery (Cochrane Review). In:The Cochrane Library, Issue 1, 2000. Oxford: Update Software. (Level I)
16. Zatuchni GI, and Andros GJ. Prognostic Index for vaginal delivery in breech presentation at term. Am JObstet.Gynecol 1965;93:237. (Level III)
17. Hannah, M and others for the Term Breech Trial Collaborative Group. What is the best way to deliver abreech baby? Lancet 2000;356:1375-83. (Level I)
18. The Society of Obstetricians and Gynaecologists of Canada. SOGC Interim Position on Management ofTerm Breech. September 27, 2000. (Level III)
19. Special Problems of Multiple Gestation. ACOG Educational Bulletin No. 253, November 1998. page 807.(Level III)
20. Crowther CA: Caesarean delivery for the second twin (Cochrane Review). In: The Cochrane Library, Issue1, 2000. Oxford: Update Software. (Level I)
G: Malpresentations, Malpositions, and Multiple Gestation27
1
MalpresentationsMalpresentationsMalpresentations
Supplementary Provider Course Slides
Supplementary Provider Course Slides
1
Planned Cesarean Delivery for Breech PresentationPlanned Cesarean Delivery for Breech Presentation
• Term Breech Trial (2000)Planned cesarean birth reduces perinatal/neonatal mortality and serious neonatal morbidity compared to vaginal breech delivery
• ACOG Position: “Planned vaginal delivery of a singleton term breech may no longer be appropriate”
2
Planned Cesarean Delivery for Breech PresentationPlanned Cesarean Delivery for Breech Presentation
• Term Breech Trial 2-year follow-up (2004)
Re-evaluated the combined endpoint of death or neurodevelopmental delay at 2 yearsFound no difference between planned cesarean and vaginal breech groups
• ALSO continues to teach vaginal breech delivery because unanticipated breech deliveries do occur
3

1
1
Malpresentations, Malpositions and
Multiple Gestation
Malpresentations, Malpositions and
Multiple Gestation
2
ObjectivesObjectives
• Define six types of malpresentations
• List complications associated with various malpresentations
• Discuss criteria for selection and management of vaginal delivery with malpresentation
• Discuss delivery management of multiple gestation (optional)
• Perform delivery of malpresentations using maternal-fetal mannequin
3
DefinitionsDefinitions
• LieRelationship of long axis of fetus to motherLongitudinal, transverse, oblique
• PresentationPortion of fetus foremost in birth canalVertex, breech, face, brow, shoulder
• PositionReference point on presenting partExamples: LOA / ROA / LOP
4
Methods of DiagnosisMethods of Diagnosis
• Leopold’s (abdominal palpation)
• Vaginal exam
• Imaging – ultrasound, flat plate of abdomen
5
Fetal Head DiametersFetal Head Diameters
Posterior Fontanel
Occiptomentaldiameter: 12.5cm
Subocciptobregmaticdiameter: 9.5cm
Anterior Fontanel
CoronalSuture
6
AsynclitismAsynclitism
• Lateral flexion of fetal head
• Sagittal suture not in midline
• Normal in small degrees
• Extreme degrees lead to dystocia
• Major factor in forceps application

2
7
Pelvic TypesPelvic TypesGynecoid Anthropoid Platypelloid Android
Round inletnormal spines
Oval inlet (AP) prominent
spines
Triangular inlet prominent spines narrow forepelvis
Oval inlet (transverse)flat spines 8
Occiput PosteriorOcciput Posterior
• “Back labor”
• Asymmetric dilation, persistent anterior lip
• Ease of palpation of anterior fontanel on vaginal exam
• Palpation of ear
9
Mechanisms of OP DeliveryMechanisms of OP Delivery
10
Manual Rotation of OP
Manual Rotation of OP
Flex fetal head by placing a hand in the
hollow of sacrum, behind the occiput
11
Vacuum Delivery of OPVacuum Delivery of OP
Note how vectors of force promote flexion with a posterior application
12
Forceps Delivery of OPForceps Delivery of OP

3
13
Breech PresentationBreech Presentation
Frank Complete Footling14
Risk Factors for BreechRisk Factors for Breech
• Prematurity
• High parity
• Uterine anomalies
• Pelvic tumors
• Polyhydramnios, oligohydramnios
• Fetal anomalies
• Absolute CPD
• Previous breech
15
Prenatal ManagementPrenatal Management
• Seek a cause for the breech
• Attempt maternal position exercises to turn breech
• Attempt external cephalic version
• Determine most favorable mode of delivery
16
Breech ExercisesBreech Exercises
Deep Trendelenburg
Knee Chest Position
17
External Cephalic VersionFactors Associated with SuccessExternal Cephalic VersionFactors Associated with Success
• Parity
• Frank breech
• Normal or increased amniotic fluid
• Relaxed uterus
• Gestational age <37 weeks
• Tocolysis
• Acoustic stimulation18
Contraindications to ECVContraindications to ECV
• Multiple pregnancy
• Utero-placental insufficiency
• Non-reassuring FHR tracing
• Uterine anomalies
• Placenta previa
• Unexplained bleeding
• Maternal medical conditions

4
19
Complications of ECVComplications of ECV
• Fetal bradycardia, decelerations
• Abruption
• Fetal hemorrhage
• Maternal hemorrhage
• Knotted or entangled cord
• Fetal mortality
• Amniotic fluid embolus, maternal death20
Elevate breech with suprapubic
hand
21
Push breech into
iliac fossa
Assistant flexes head
22
Now fetus in transverse lie
Ultrasound is used to monitor progress and heart rate
23
Fetus is past transverse
Little effort required to
guide head into a vertex
presentation
24
Ultrasound confirmation
of fetal presentation

5
25
Vaginal Breech ContraindicationsVaginal Breech Contraindications
• Unfavorable pelvis
• Macrosomia
• Severe prematurity
• IUGR, placental insufficiency
• Footling breech
• Hyperextension of fetal head
• Fetal anomalies
• Nuchal arm
• PROM or non-progressive labor
• Lack of birth attendant skills26
Breech DeliveryBreech Delivery
Most favorable diameter for breech is same as that of cephalic
Breech Cephalic
Symphysis Symphysis
SacrumSacrum
27
Vaginal Breech Delivery:Delivery of the Fetal Pelvis
• Hand gently supporting the emerging breech
• Keep the sacrum anterior
28Delivery of the Legs - Optional Maneuver
29
Gentle Traction on Fetal Pelvis
30
Delivery of the Anterior Arm in a Vaginal Breech Extraction
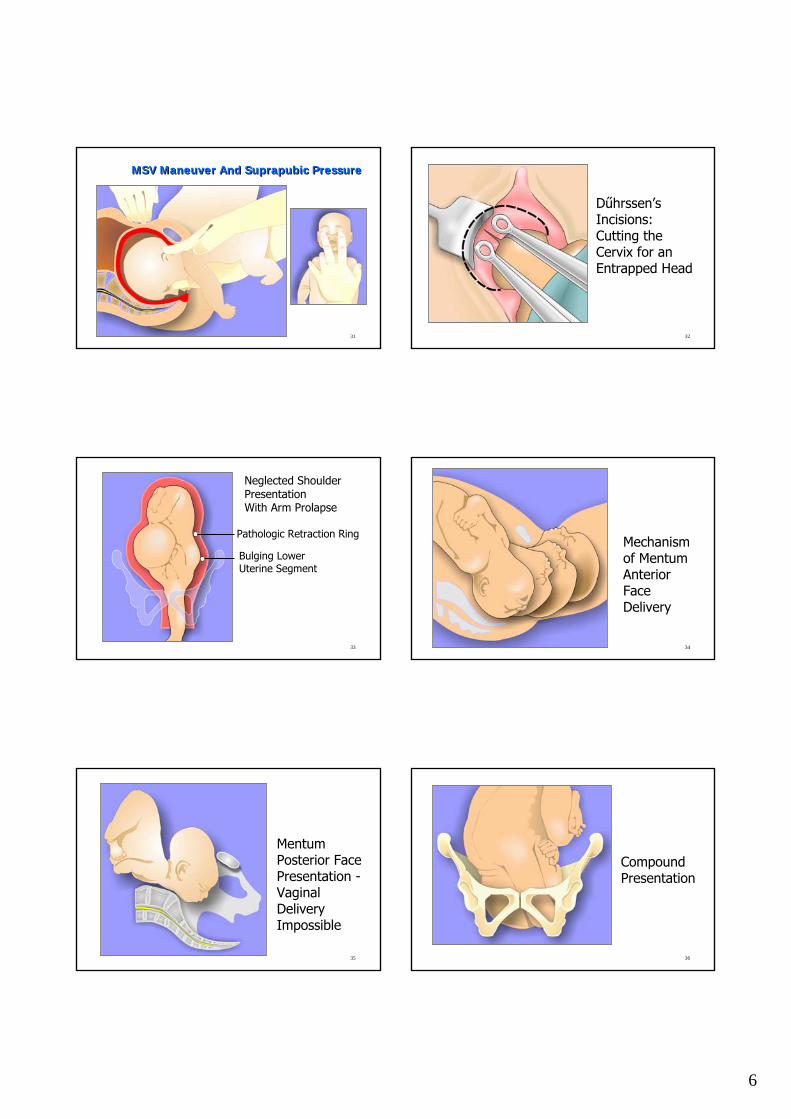
6
31
MSV Maneuver And Suprapubic PressureMSV Maneuver And Suprapubic Pressure
32
Dűhrssen’sIncisions: Cutting the Cervix for an Entrapped Head
33
Pathologic Retraction Ring
Bulging Lower Uterine Segment
Neglected Shoulder Presentation With Arm Prolapse
34
Mechanism of MentumAnterior Face Delivery
35
MentumPosterior Face Presentation -Vaginal Delivery Impossible
36
Compound Presentation

7
37
Umbilical Cord Prolapse Umbilical Cord Prolapse
• Risk FactorsMalpresentation, prematurity, polyhydramnios, high presenting part, long cord
• Epidemiology
IncidencePresentation
0.5%Frank breech
15%-18%Footling breech
4.0-6.0%Complete breech
0.4%Vertex
38
Prolapsed Umbilical Cord in Footling Breech
39
Rapid Response to ProlapseRapid Response to Prolapse
• Recognize non-reassuring tracing
• Visually inspect / palpate cord to diagnose
• Assess fetal status (FHTs, ultrasound)
• Assess labor progress (dilation, station)
• Do not attempt to replace cord
• Hold presenting part off cord Foley catheter
Position change (Trendelenburg, Knee-chest)
• Tocolysis 40
Prevention of ProlapsePrevention of Prolapse
• Identify risk factorsMalpresentation, high presentation
Patient education re: membrane rupture at home
• No AROM when station highMay “needle” membranes under double set-up
41
Multiple GestationMultiple Gestation
• Occurs in 1.5% of U.S. births
• 2-5 X higher perinatal mortality
• Maternal complications commonHTN, anemia, hyperemesis, abruption, previa, PPH, operative delivery
• Dizygosity (fraternal) = 2/3Increases with age, parity, familial factors
• Monozygosity (identical) =1/342
Diagnosis of Multiple GestationDiagnosis of Multiple Gestation
• Ovulation induction
• Family history
• Hyperemesis
• Uterine size > dates
• Early PIH
• Elevated MSAFP
• Auscultation of >1 fetal heart beat
• Polyhydramnios

8
43
Associated ComplicationsAssociated Complications
• Prematurity
• Congenital anomalies
• Pregnancy-induced hypertension
• Placenta previa
• Fetal death: 0.5%-6.8%
44
Presentation of TwinsPresentation of Twins
Vertex-Vertex43%
Vertex-NonVertex38%
NonVertex(twin A) 19%
45
Delivering Twin BDelivering Twin B
• Attempt internal podalic version
• Breech delivery is reasonable choice when:External version unsuccessful or not attempted
Strong labor and Baby B deep in pelvis
Cord prolapse or nonreassuring FHR tracing
46
SummarySummary
• Six types of malpresentations
• Diagnosis by physical exam and imaging
• Be alert to etiologic associations
• Be alert to potential complications
• Vaginal delivery may be considered for OP, breech, face and compound presentation