2010 field staff immunization clinic program...
TRANSCRIPT

Revised. 09/08/2010 Field Staff Immunization Clinic Program Guide 1
2010 Field Staff Immunization Clinic Program Guide
© Summit Health, Inc.
25300 Telegraph Road, Suite 250 Southfield, MI 48033
Phone (248) 7998303 • Fax (248) 7990876

Rev. 9/8/2010
Thank you for partnering with Summit Health as we work to bring immunizations to communities and employer groups throughout the country. We are excited about the opportunities that exist for us to work together while providing these valuable services to our clients.
Summit Health has improved upon existing immunization and health and wellness programs by developing and adding new service modules to the menu of options. For the last ten years, Summit Health has been attracting the most talented and professional wellness facilitators in the industry. The collective knowledge and industry experience of management, support staff, and clinical personnel will allow us to continue to flourish! Thank you for being a critical part of our team.
Moving forward, we have every expectation of strengthening our business relationships while delivering exceptional service. The “behind-the-scenes operations” of the company continue to be enhanced which will allow us to more effectively manage clinic operations and increase quality of service. The ongoing development of a world class software system will ultimately enable Summit Health to be more responsive to agencies, nurses, and field staff. Additionally, our systems will allow us to better facilitate the needs of our clients.
The individual and team efforts of everyone involved with bringing these services to market are to be applauded. The Centers for Disease Control now recognizes community vaccination providers as vital partners in the campaign to deliver influenza and pneumonia vaccination services to those in need.
This manual is your guide to facilitating vaccination clinics coordinated by Summit Health. Please read the manual, take notes and ask questions! The commitment and professionalism that you display in the field has a direct impact on our business relationships. We appreciate your support and value your skills. We look forward to a successful vaccination season and welcome your feedback!
Healthfully yours,
Summit Health

Rev. 9/8/2010
TABLE OF CONTENTS
WORKING WITH SUMMIT HEALTH ................................................................................................... 1
MANUAL TERMS & DEFINITIONS ................................................................................................................ 1 QUALIFICATIONS...................................................................................................................................... 2 TRAINING MATERIALS ........................................................................................................................ 3 CLINIC SUPPLIES AND DISTRIBUTION ............................................................................................. 4 SUPPLY CATEGORIZATION ............................................................................................................... 4 CLINIC DRY GOODS DISTRIBUTION .................................................................................................. 5 PAPERWORK DISTRIBUTION ............................................................................................................ 6 QUICK GUIDE SHIP TO PROCESS ..................................................................................................... 7 CLIENT SPECIFIC REQUIREMENTS .................................................................................................. 7 IMMUNIZATION FORMS DESCRIPTION ......................................................................................................... 8
Consent Forms ............................................................................................................................. 8 ► HIPAA Notice of Privacy Practices ................................................................................... 9 ► Blank Doctor’s Orders / Medical Directives ..................................................................... 9 ► VIS forms ............................................................................................................................. 9
ADMINISTRATIVE ITEMS .......................................................................................................................... 10
CHAPTER 2: CLINIC ADMINISTRATION ......................................................................................... 11
CLINIC PREPARATIONS .......................................................................................................................... 11 Clinic Supplies Checklist .............................................................................................................. 11
STORING AND TRANSPORTING VACCINES ................................................................................................ 12 INVENTORY OF SUPPLIES ....................................................................................................................... 13 RECEIPT OF SH VACCINES, EPINEPHRINE & SUPPLIES ............................................................................. 13 RETURNING UNUSED VACCINE ............................................................................................................... 13 CUSTOMER SERVICE ............................................................................................................................. 13 CLINIC POLICIES.................................................................................................................................... 14
Blood Policy ................................................................................................................................. 14 Filling Syringes ............................................................................................................................. 14 Vaccine Lot Numbers ................................................................................................................... 14
CHAPTER 3: CLINIC PREPARATION & OPERATION ..................................................................... 15
CLINIC SET-UP ..................................................................................................................................... 15 1. Lead Nurse Duties .................................................................................................................... 15 2. Arrival Protocol ......................................................................................................................... 15 3. Clinic Set-up ............................................................................................................................. 16 Workflow Tips ............................................................................................................................... 16 4. Starting the Clinic ..................................................................................................................... 16
CLINIC SHUT-DOWN .............................................................................................................................. 17 POST-CLINIC FOLLOW UP ...................................................................................................................... 18
CHAPTER 4: VACCINE ADMINISTRATION ..................................................................................... 19
PARTICIPANT ELIGIBILITY RULES ............................................................................................................. 19 SAFETY PROCEDURES ........................................................................................................................... 21
Standard Precautions ................................................................................................................... 21 PARTICIPANT SAFETY ............................................................................................................................ 21
5 Rights of Medication Administration .......................................................................................... 21 VACCINE SELECTION BASED ON AGE OF PARTICIPANT ............................................................................. 21

Rev. 9/8/2010
BIOHAZARD WASTE DISPOSAL ................................................................................................................ 21 SAFETY NEEDLE / SYRINGE USAGE ......................................................................................................... 22 VACCINATION POLICIES .......................................................................................................................... 24
Intramuscular Injection – Vaccine Clinical Procedure ................................................................... 24 Subcutaneous Injection - Epinephrine Only - Clinical Procedure ................................................. 25
INFLUENZA VACCINATION PROCEDURES .................................................................................................. 26 Influenza dosage and Type based on Age ................................................................................... 26
PNEUMONIA VACCINATION PROCEDURES ................................................................................................ 27 Pneumonia dosage ...................................................................................................................... 27
CHAPTER 5: ADVERSE REACTION PROTOCOL ........................................................................... 28
ADVERSE REACTIONS ............................................................................................................................ 28 EMERGENCY TREATMENT PROCEDURE ................................................................................................... 28 ANAPHYLACTIC REACTION (ANAPHYLAXIS) .............................................................................................. 29
Definition ...................................................................................................................................... 29 Causes ......................................................................................................................................... 29 Assessment .................................................................................................................................. 29
EPINEPHRINE ADMINISTRATION............................................................................................................... 30 Systemic Anaphylaxis .................................................................................................................. 30
FAINTING - INCIDENT PROTOCOL ............................................................................................................. 30
APPENDIX - FORMS ......................................................................................................................... 33
TWO-PART CONSENT FORM ................................................................................................................... 33 SCANTRON BUBBLE CONSENT - FRONT SIDE 1............................................................................ 34 SCANTRON BUBBLE CONSENT - FRONT SIDE 2............................................................................ 35 SCANTRON BUBBLE CONSENT - BACK SIDE 1 .............................................................................. 36 SCANTRON BUBBLE CONSENT - BACK SIDE 2 .............................................................................. 37 CLINIC RECORD FORM .................................................................................................................... 38 HIPAA NOTICE OF PRIVACY PRACTICES ....................................................................................... 39 CONFIDENTIAL ENVELOPE ............................................................................................................. 40 INDUSTRY BEST PRACTICES ON-SITE CAREGIVERS ................................................................................. 41 2010-2011MEDICAL DIRECTIVES - INFLUENZA ........................................................................................ 42 2010-2011MEDICAL DIRECTIVES - PNEUMONIA ....................................................................................... 43 ANAPHYLACTIC SHOCK POLICY & PROCEDURE ........................................................................................ 44

Revised. 09/08/2010 Field Staff Immunization Clinic Program Guide 1
WORKING WITH SUMMIT HEALTH Manual Terms & Definitions
SH – Summit Health
Client – Client is the Corporate or Retail Site hosting the clinic, not to be confused with
Participant or Patient.
Site coordinator – The representative from the Corporate or Retail Site that is hosting the clinic.
Independent Subcontractor – The nurse contracted directly with SH independent of an
agency.
Lead Nurse – The lead nurse at the clinic who is responsible for supplies and contact with
the client site coordinator at each clinic.
AP (Agency Partner) - The Local Staffing Agency facilitating the clinic on behalf of SH.
Agency Contact - The contact at the Local Staffing Agency responsible for medical staffing assignments.
Participant – The patient receiving Immunization services at the client site.
WOC – The Work Order Confirmation has two purposes; 1) To acknowledge and confirm the assignment of a clinic to a Lead Nurse/Independent Subcontractor/AP; 2) To provide the assigned Lead Nurse/Independent Subcontractor/AP with clinic details such as: company name, client contact, service to be delivered, quantity, paperwork requirements and other data pertinent to the success of the immunization clinic.
Portal – Web based tool provides all SH medical staff visibility to assigned clinics, available clinics within territory, access to training materials, forms, time cards and more.
Flu Kit – Term used to define supplies shipped from SH containing clinic dry goods that are packaged per the individual clinic WOC. Dry goods are shipped to the Lead Nurse or Agency Partner only and NEVER to the client site.
Dry Goods – Are the ancillary medical items contained in the Flu Kit. Dry goods are required for the administration of immunizations. The ancillary medical dry goods are the following: syringes, gauze, gloves, bandages, hand sanitizer, tablecloths, garbage bags, sharps container and epinephrine.
Paperwork – Documents required to conduct clinics and for the legal administration of vaccines. Paperwork is defined as: Consent Forms, Privacy form, VIS, Clinic Record, Incident Report, Confidential Envelope, Pens/Pencils and an overnight return bag for consent forms. These items will either be included in the Flu Kit with the dry goods shipped to the Lead Nurse or Agency Partner or mailed to the Client. If you receive a Flu Kit without paperwork included, check your WOC to verify the ship to contact. If this information is not included on your WOC contact the SH Staffing Coordinator asap!

Rev. 9/8/2010 2
Qualifications
RN & LPN Job Description The professional Registered Nurse/Licensed Practical Nurse provides skilled care to the Participant to whom a vaccination is being administered. Protocol has been established by SH and is in compliance with the nursing policies, procedures, and regulations as established by the State Licensing Board of Nursing.
RN & LPN Qualifications Education – has graduated from an approved school of nursing.
Licensure – is currently licensed and is in excellent standing with the applicable State Board of Nursing.
(Nurses hired for purposes of administering immunization services will have been properly screened and interviewed per the SH Subcontractor Agreement)
Experience – has a minimum of one year of experience (not including clinical training) providing injections.
Training – has attended (or will attend) an orientation/training session (live, web, or conference call)
Specific Job Description/Expectations All duties and responsibilities shall be in accordance with Federal, State, and Local laws. Employees are also expected to:
Adhere to all policies, procedures, and guidelines in this Immunization Clinic Guide. Adhere to the Medical Professionals Industry Best Practices (see Forms section for full document). Provide quality, professional nursing care and maintain a safe environment for each Participant and self. Remember that customer service is a high priority. Be organized. Follow all guidelines in the manual, with special attention to the Immunization Process. Use aseptic technique at all times. Wear Gloves as outlined on the vaccination procedure pages of this
manual. Be current with all information on vaccines. Be able to educate the Participant regarding the requested vaccines. Supervise, teach, and assist the clerk (when applicable) as necessary. Be honest and trustworthy while handling all money and checks.
Clerk Job Description The clerk is instrumental at events whereby, collecting money (where required) and keeping order during large clinics. Make sure that you bring a cash box (for example, a shoe box) with you to all clinics where cash/checks will be collected. A large clinic envelope is provided for each clinic.
Qualifications The clerk must have:
Valid driver’s license Social Security card – documentation of the legal right to work in the US Auto insurance
(Staff contracted for purposes of clerking will have been properly screened and interviewed per the SH Subcontractor Agreement.)In addition, the clerk must also:
Be honest and have integrity. Be able to accurately count money. Write legibly. Possess good people skills.

Rev. 9/8/2010 3
Dress neatly, have excellent hygiene. Wear ID badge at all times during clinic. Take directions from Lead Nurse. Be on time. Adhere to the Immunization Clinic Guide.
TRAINING MATERIALS
Training Orientation must be provided for all clinic staff. The Agency Partner must ensure that each nurse has had experience or training in administering vaccines and is familiar with the specific vaccine(s) and protocols for this program. The Independent Nurse has been pre-screened by SH, has had experience or training in administering vaccines and is familiar with the specific vaccine(s) and protocols for this program.
The Summit Health Flu Video and the 2010 Field Staff Vaccination Clinic Program Guides are required for review.
► Please note the following directions to view the video or access the manual.
1) Via the Internet, go to:
http://www.streamingvideoslive.com/VideosWebPage.htm
2) When the page opens, at the top middle (Flu), begin viewing all of the modules. If you are unable to open or connect to the link above copy the link and place in your browser. At the top middle (Flu), begin viewing the Flu modules.
► You can also view our training web site and download flu documents by going to your portal and
under the “Summit Health Training Materials” tab on the bottom left hand side. The training video is on the top of the page in the middle.
► A total of 3 Live Webinar presentations were conducted September 1st- 3rd for Nursing staff and
Agency Partners. A recording of the presentation will be made available for audio and visual review on or before September 10th. Viewing instructions will be made available soon.

Rev. 9/8/2010 4
CLINIC SUPPLIES AND DISTRIBUTION
SUPPLY CATEGORIZATION
Clinic supplies at Summit Health are categorized into the following 3 main groups:
1) Vaccine 2) Dry Goods and 3) Paperwork
Summit Health ships all vaccine and ancillary medical supplies, referred to as dry goods, to the clinics assigned lead nurse or agency partner and NEVER to the client.
Vaccine Distribution Source
Vaccines are shipped from one of either two sources to the assigned clinic staff. One originating source of vaccines supplies will be Summit Health’s corporate office, located in Southfield, Michigan. The second originating shipping source of vaccine is Henry Schein, one of the nation’s largest distributors of the product.
Ship To Address/Contact
Vaccine product shipped from distributor Henry Schein is addressed to the name of Summit Health’s state Medical Director with c/o Summit Health. Although the ship to address will be that of the lead nurse or agency partner, but not the ship to contact, be careful to avoid refusing acceptance of supplies intended for your scheduled clinic.
Vaccine product shipped from Summit Health’s corporate office located in Southfield, Michigan is shipped and addressed to the lead nurse or agency partner only.
Packaging & Shipping Method
Vaccines shipments are sent to lead staff and/or agency partners only Monday – Thursday via overnight mail through carriers UPS or Fed Express. Vaccines are packaged in Styrofoam coolers along with frozen ice packs, to maintain the appropriate cold chain guidelines and the overall integrity of the product.
The vaccine shipment contains no other supplies. Other clinic supplies such as dry goods and paperwork are shipped independently of the vaccine.
It is the responsibility of Summit Heath to ensure on-time deliveries and the proper vaccine quantities are shipped to our lead nurse and agency partners. Transportation and delivery of vaccine supplies and dry goods to the clinic site, however, is the responsibility of the lead nurse or agency partner. Don’t leave home without your supplies!
Storage &Transporting Vaccine
All vaccine should be removed from the shipping container and refrigerated immediately upon receipt. The ice packs included should be placed in the freezer for use in transporting the vaccine to the client site using the Summit Health cooler.
New this year for transporting vaccine to Summit Health clinics are branded soft sided thermal cooler bags with handles added for easy transport. The traditional white Styrofoam coolers will be distributed as well with freezer packs.
Vaccine Shipping Schedule Vaccine will be shipped on a weekly basis. Vaccine will be shipped the week prior for clinics the following week. The shipments should arrive by Thursday the week before your clinic(s).

Rev. 9/8/2010 5
Vaccine for clinics scheduled September 22 - 25th, should arrive to clinic assigned Lead Nurses or Agency Partners between September 14th and 16th. Vaccine for clinics scheduled September 26th -October 2nd, should arrive to clinic assigned Lead Nurses or Agency Partners between September 21st and 23rd.
CLINIC DRY GOODS DISTRIBUTION
Now that you have an understanding of how Summit Health ships and delivers vaccine to our medical staff, let’s take a look next at how the dry goods are shipped. Dry goods are the medical supplies needed to support the administration of vaccine to clinic participants. Dry goods, just like vaccines, are shipped to the lead nurse or agency partner and NEVER the client.
Dry goods are as follows:
► epinephrine kit syringes sharps container gloves gauze
► bandages hand sanitizer waste basket liners tablecloth
This year we are very proud to introduce “per clinic” packaging for all dry good supplies. Also, new for 2010 is the package containing the dry good supplies referred to as the Flu kit. See kit picture on page….. The new flu kit will allow our staff an easy and less cumbersome way to transport dry good supplies to and from clinic sites.
Dry Goods Distribution Source
Dry goods are shipped from the corporate office of Summit Health located in Southfield, Michigan. Dry good supplies for 2010 are being shipped from no other source outside of Summit Heath. All dry goods will be shipped via ground mail.
Ship To Address/Contact
All Dry good supplies are shipped addressed to the Lead Nurse or Agency Partner. Again these supplies are never shipped to the Summit Health client or clinic site.
Packaging & Shipping Method
Dry good quantities will be packaged to the order i.e. clinic order as outlined on the Lead Nurse or Agency Partners WOC.
The individual dry good supplies as defined earlier will be packaged in a new easy to carry box referred to as the Flu kit for 2010. Although the Flu kit will be packaged with dry goods per clinic, shipping of the kits will be mailed several at a time. Each Flu kit has a clearly defined label with the clinic ID and other clinic details on the outside of the box.
Transporting Dry goods
The new Flu kit box will be provided for transporting dry goods. See kit picture on page….

Rev. 9/8/2010 6
..
PAPERWORK DISTRIBUTION
Finally, the third category of supplies to review is the Paperwork. The required clinic paperwork is mandatory in order to administer vaccines to participants. Without paperwork such as the consent form, a nurse is unable to legally administer a vaccination to anyone
without having their signed consent.
The most important fact to remember about Summit Health’s shipping and handling process for paper work is this;
Of the 3 different categories of supplies, paperwork is the only of the 3 that is shipped to either the client or the assigned Lead Nurse or Agency Partner. Also, the paperwork supplies are the only supplies that can be returned by the client when applicable.
Paperwork is defined as follows:
► Consent forms HIPAA Privacy document VIS Statement
► Clinic Record form Incident report sharpeners
► Confidential envelope Return Package Pencils/Pens
Paperwork Distribution Source
Paperwork is all shipped from the corporate office of Summit Health located in Southfield, Michigan. These supplies are never shipped from another source other than Summit Heath. Paperwork shipped either to the client or Lead Nurse or Agency Partner is shipped via ground mail.
Paperwork Ship To Address/Contact
Paperwork will be shipped from Summit Health to either the client site contact or the assigned Lead Nurse or Agency Partner but never to both. The ship to source or destination point for clinic paperwork will be stated on the Lead Nurse or Agency Partners WOC from Summit Health.
Packaging & Shipping Method
Paperwork that is shipped to the Lead Nurse or Agency Partner will be packaged in quantities equal to the amount reflected on the WOC. Paperwork, when shipped to the Lead Nurse or Agency Party, will be included in the Flu Kit along with the dry goods reviewed on the prior page of this manual.
When the client site contact is shipped the clinic paperwork it is packaged in an Admin kit. Upon the arrival of the nursing staff on the day of the scheduled clinic, the client site contact has been instructed to provide the nursing staff with the clinic paperwork.
Transporting Paperwork
Paperwork shipped to Lead Nurse or Agency Partner is shipped and included within the new Flu Kit. Paperwork shipped to the client is shipped and packaged in a package referred to as the Admin kit.

Rev. 9/8/2010 7
QUICK GUIDE SHIP TO PROCESS
QUICK GUIDE RETURN PROCESS
Client
Type
Paperwork Returned by
Dry GoodsReturned by
Vaccine Returned by
Home Depot Lead Nurse/Agency Lead Nurse/Agency Lead Nurse/Agency
Lowes Lead Nurse/Agency Lead Nurse/Agency Lead Nurse/Agency
All Other
Corporations
Client Site
Coordinator Lead Nurse/Agency Lead Nurse/Agency
Pharmacies Client Site
Coordinator Lead Nurse/Agency Lead Nurse/Agency
CLIENT SPECIFIC REQUIREMENTS
Summit Health provides Wellness and Immunization services to a variety of clients. Some of the clients you as our staff will work with are Managed care companies such as insurance groups and their clients, fortune 500 & 1000 clients and small business clients as well. Our clients are primarily defined as managed care companies also known as third –party clients, stand alone Corporations or direct clients and Pharmacy clients. Let’s take a further look at the basic clinic requirements of our clients which will give you insight into some of the services you will help to deliver. We will also point out clients requiring any non-standard services or procedures as well.
Client Type Paperwork Shipped to
Dry GoodsShipped to
Vaccine Shipped to
Home Depot Lead Nurse Lead Nurse/Agency Lead Nurse/Agency
Lowes Lead Nurse Lead Nurse/Agency Lead Nurse/Agency
All other
Corporations
SH Client Site
Coordinator
Lead Nurse/Agency Lead Nurse/Agency
Pharmacies SH Client Site
Coordinator
Lead Nurse/Agency Lead Nurse/Agency

Rev. 9/8/2010 8
CLIENT REQUIREMENTS
Managed Care Corporate Pharmacy
Type of consent form required Scantron Scantron,
2 -Part 2-Part 2-Part 2-Part
Participant Payment method Insurance, Bill company
Insurance, Bill company
Insurance, cash, checks
checks, Bill com
checks, Bill com
Participants eligible under 18yrs No No No No no
Pregnant or nursing mothers eligible
No No No Yes No
Thimerisol vaccine available No No No Yes No
Clinic open to the public No No Yes No No
Clinic paperwork shipped to client Yes Yes Yes No No
Participant sign in sheet required by client
Not likely Not likely Yes Yes No
Online appointment system used 1% 1% No No No
Other special requirements No No No Survey
No
Immunization Forms Description
Consent Forms - Summit Health uses a combination Consent Form which covers both influenza and pneumonia vaccinations. Please be sure that you mark the correct box for the applicable injection. The participant signing the Consent form gives legal documentation to their responses to the Screening Questions. In addition, the lot # of the vaccine given, and other relevant participant information is gathered.
The consent form is used by SH to generate billing for vaccination services provided. Upon receipt of the completed participant consent forms, depending on the payment method, SH will either submit an insurance claim on behalf of the participant or invoice the participant’s employer. Summit Health is paid based solely on completed and accurate consent forms. Please ensure the consent forms are completed in their entirety with neat and legible writing.
Completed Consent Forms – will be either (1) given to the Client site coordinator at the end of the clinic and mailed back to Summit Health by the client site coordinator OR (2) at clinics for Home Depot, Lowes and others defined on your WOC, must be sent back to the Agency Partner Office or taken with the Independent Lead Nurse and then shipped back to SH’s corporate office. Specific directions will be included on the Work Order Confirmation for the event.
There are three styles of Consent Forms, based on the Clinic type:

Rev. 9/8/2010 9
► Two- Part Carbon Consent Form - are primarily used at retail and pharmacy store-based clinics (e.g. Spartan Stores and independent pharmacies), Home Depot and Lowes where insurance claims are not typically required as a payment method for service.
The Two-Part consent form has a second carbon copy which should be separated and provided
to the participant as their receipt. The vaccine information statement published by the CDC is printed on the back of the carbon for the participant. Black or Blue ink pens are to be used for their completion.
If copies of the Two-Part consent form are not included in your Flu Kit, check your WOC to verify if the consents were shipped to the client site contact.
► Scantron Bubble Consent Forms – have been created to include the VIS and Privacy
Statement all within one Form. Please note a #2 Pencil must be used, write legibly inside each box, and complete the bubbles below each box. After you record the medical information in the “for medical use only” section of the form, tear and separate the VIS /Privacy page at the perforation and give to the participant.
The Scantron bubble page of the form is kept at your station until Clinic Shutdown. When you arrive at the clinic site the site contact will provide you with the clinic forms including the consents. After the medical staff has completed Clinic Shutdown, the medical staff will retrieve the white envelope from the admin kit provided by the client and place the completed participant consents within the envelope. The medical staff will seal the envelope and provide the package to the Client site coordinator.
► Client Specific Scantron Consent Forms – have been customized for the Clients usage, however differ in their design. Please note a #2 Pencil must be used, write legibly inside each box, and complete the bubbles below each box. These forms will be sent directly to the Client site coordinator who will provide you with the forms on the day of the clinic. After the AP or Independent Nurse has completed Clinic Shutdown, the staff will retrieve the envelope from the admin kit provided by the client placing the completed consents within the envelope. The medical staff will seal the envelope and provide the package to the Client site coordinator.
► HIPAA Notice of Privacy Practices – This form must be available to clinic participants. SH is committed to protecting the privacy of the participants’ health information and SH has implemented policies and safeguards to protect their privacy. SH is also required by state and federal laws to protect the confidentiality of the participants’ health information and to provide them with this Notice. This form is not printed on the Two- Part Carbon consent form as is the case with the Scantron Bubble.
► Blank Doctor’s Orders / Medical Directives - are located in the back of the manual. These must be reviewed by each nurse prior to and the day of the Clinic. A signed copy of your state’s order is held in the SH Corporate Office and available upon request.
► VIS forms – must be provided to the participant for review prior to immunization. Both the Scantron Bubble consent and Two-Part consent are printed with the CDC’s vaccine information statement on the consent. The VIS should be given to the participant after they have been completely serviced as it provides them proof of their vaccination services received.
► Clinic Record Form- The clinic record form is to be completed by the nursing staff at the conclusion of each flu clinic. The purpose of this document is to provide a record of the number

Rev. 9/8/2010 10
of vaccines provided and an accounting of funds received (if applicable). This document is a 1 page form but with 3 carbon copies. After completing this form the lead nurse or agency partner will provide 1 of the 3 copies to the client site contact. The second copy will be placed in the envelope with the completed consents with the final copy retained by the lead nurse or agency partner.
► Incident Report – This form must be completed by the lead nurse or independent subcontractor when an on-site medical incident occurs at a clinic. See the emergency protocol procedures on pages …….for instruction on completing this form.
SEE ALL FORMS IN THE APPENDIX SECTION
Administrative Items
It is the responsibility of all staff, administrative and medical, to read the full manual, and follow all
of the required procedures and protocols.
The Lead Nurse must contact the Client site coordinator 72 hours in advance to confirm directions. Always introduce yourself as with Summit Health.
Work order request – This document serves as the official request for staff. Service Requests are submitted via email and made available on the portal to independent nursing staff, clerks and or agency partners to fulfill a specific job/clinic.
Work order confirmation - This document is the acknowledgement that Summit Health has assigned a specific clinic to the independent staff, lead nurse or agency partner.. The WOC should also be printed and provided to all medical staff who has been assigned clinics. This document will provide staff with the clinic address, company name, client site contact details, product to be provided and amount required, clinic date/time participant payment method, paperwork ship to and returns guidelines etc. Don’t leave home without it!

Revised. 09/08/2010 Field Staff Immunization Clinic Program Guide 11
Chapter 2: Clinic Administration
Clinic Preparations
Clinic Supplies Checklist Proper preparation of materials and supplies will greatly enhance the outcome of any vaccination clinic. The key is to make sure that you are adequately stocked.
Most offices will be receiving separate Flu Kits which have enough supplies to provide 50 injections. Always attend each scheduled clinic with enough supplies. Whether or not you are the Lead Nurse, please be sure you bring all of your supplies with you to each clinic. Review the estimates on your Work Order Confirmation for each clinic on your schedule to gain a better idea about supply needs.
All prepackaged Flu Kits should contain the following items:
Safety Syringe with Needle Device Band aids Alcohol Preps Gauze Gloves Sharps container Hand sanitizer Garbage bag
► Reminder: Make sure you do not select a kit that has already been used and does not contain all the supplies for 50injections.
Additionally, you will pick up from your office the following: Required for ALL events:
Work Order Confirmation - one for each clinic that you are staffing as lead nurse. If multiple nurses are working the same clinic, each nurse should have a copy of this document.
Vaccine (arrange to have all the same lot # for all injections at any one particular clinic, if possible) o Influenza o Pneumonia (only present if it appears on your WOC )
Cooler with gel ice packs Emergency EPI Kit – No Epinephrine No clinic. Don’t forget it! B/P Cuff and Stethoscope (nurse to supply) Sharps Container
Required for Home Depot, Lowes, and Spartan events:
Clinic Record Forms – one for each clinic that you are staffing as lead nurse Consent Forms – If not included in your Flu Kit check your WOC to determine if they were shipped to the
client VIS forms - provide to the participant for review prior to the immunization being completed. Large Yellow
Envelope (for clinic paperwork) and Small Envelope (for checks/ money orders) where required SH Incident Report All clinic personnel must arrive adequately prepared with sufficient supplies. Even if you are not the lead
nurse, please bring any supplies you may have to all clinics (we may need them). Refer to the Work Order Confirmation/ for arrival time and clinic start time. The arrival time is always 1 hour prior to the start time of the clinic.
Nurses MUST arrive as requested per the Work Order Confirmation, on time and prepared. Arrive as scheduled and check in with your contact. Always introduce yourself as being with Summit Health.

Rev. 9/8/2010 12
Storing and Transporting Vaccines
DO NOT FORGET THE MEDICAL SUPPLIES.
The efficacy and potency of a vaccine is directly related to the conditions in which it is stored and
transported. Follow the guidelines for storing and transporting vaccines:
Vaccines must be stored in a clean refrigerator that maintains a constant temperature between 35° – 46°F (standard refrigerator temperatures). They must be stored separately from food and other drugs; place in separate refrigerator, shelf or drawer. Do not store on the door of the refrigerator due to temperature range from opening / closing.
Do not use vaccine that has been frozen. Vaccines are destroyed by freezing.
Verify you select the correct Vaccine for the event. The Inflenza Vaccine used is Age dependent:
The GSK influenza vaccine (FluLuval) for participates age 18 and above, will be the most commonly used.
The Novartis influenza vaccine (Fluvirin) can be used for all participants between the ages of 9 and 18, will predominately be used at retail stores. However, Summit Health does not vaccinate participants under the age of 18.
Thimerisol Free vaccine will be shipped to nurses assigned to work Home Depot clinics to be administered to pregnant and/or nursing mothers only at Home Depot.
Vaccines may be transported to the clinic in an insulated container (such as a cooler) with cold packs. o To prevent freezing, ensure that the vials of vaccine are not in direct contact with the cold packs. o Vials are to be protected from the cold packs with a protective buffer layer, to prevent direct contact. Use
bubble wrap or crushed newspaper, approximately 1” buffer should be used. o Ensure that enough cooler packs are present to maintain a constant temperature between 35° – 46°F
(temperature strips not required). o During hot weather, transport the container in a cool place like the air conditioned interior of a car. Do not
leave vaccines unattended or in the trunk of a parked car. o During cold weather, do not leave the container in an unheated area because the vaccines may freeze.
Limit the access to stored vaccine and epinephrine to authorized personnel only. Clearly define who in your organization is authorized to have access to the drugs.
You must take the Epinephrine kit provided in the Flu Kits to all clinic sites. You cannot conduct a clinic without an EPI Kit

Rev. 9/8/2010 13
Inventory of Supplies
The Agency Contact or Independent Lead Nurse must check the supplies for the clinic using the Work Order Confirmation . SH will update the Agency Contact/ Independent Lead Nurse in the event that the clinic forecast changes.
Please be proactive regarding supplies. The estimated number of shots for each clinic is noted on your Work Order Request. Monitor your inventory and communicate any low levels to your SH staffing coordinator immediately. This will enable SH to allocate and ship adequate
supplies for upcoming clinics. Please do not wait until the last minute to call for more supplies. Please understand that vaccine supply is limited and product must be allocated on a controlled basis, provide at least 5 days notice.
Receipt of SH Vaccines, Epinephrine & Supplies
Appropriate supervision of vaccines and other drugs begins with clear identification of the vaccine at the time of delivery. Please follow these instructions when the vaccine shipment arrives at your Agency Office / Independent Nurse:
1. Before accepting delivery of the shipment, count the number of boxes being delivered. Verify that the number of received boxes matches the shipping documents. Only sign for what has actually been delivered, note any discrepancies, and advise SH shipping immediately at 248-416-1542.
2. Open the boxes immediately. Remove and refrigerate vaccine. Save the Styrofoam shipping container and
ice packs for transportation of the vaccine as well as Return Shipments.
3. Assign a person to take responsibility to inspect the contents of the boxes. They must: a. Verify that the contents match the Work Order Confirmation. b. Verify that all the flu vials are intact with 2011 or beyond expiration date. c. Verify that the pneumonia vials are intact and have an appropriate expiration date.
4. Epinephrine is to be stored at controlled room temperature 59 – 86 degrees (15 – 30 degrees C), do not expose to extreme temperatures. Epinephrine is also to be protected from light.
Returning Unused Vaccine
At the end of the program, all vaccine (flu and pneumonia) needs to be returned to SH. The shipment of vaccine needs to follow standard storage procedures for flu and pneumonia vaccine (see Storage and Shipping Vaccine). Use the insulated container and cold packs initially received with shipment, pack following Storing and Transporting Vaccines guidelines. Pre-addressed Summit Health Corporate Courier account (UPS) labels are included in the Flu Kit. Return Labels can also be printed from the Summit Health website or portal. Record the shipping details on the provided form.
Vaccine must be shipped via Overnight Shipping. Vaccine is to be shipped for return to SH on Monday through Thursday only, so that it will be received at Summit Health prior to end of workday on Friday, for immediate refrigeration upon arrival.
Customer Service
Good customer service is a major component of a successful clinic. Use the following tips for interacting with clinic Participants:
Address the Participant by Mrs. /Ms. / Mr. and last name. Pay dedicated, courteous attention to the Participant at all times during the interaction. Make and maintain eye contact with the Participant when asking questions, when listening to responses, and after
administering the vaccination. Be aware that all the Participants waiting for their injections are watching how you perform.

Rev. 9/8/2010 14
You can demonstrate your knowledge by answering questions confidently and directly to the Participant. Use Standard Precautions and Safety (good infection control practices). Tables must be clean and uncluttered. If a Participant is unhappy with the procedural process or your inability to administer the vaccine (for any
reason), remain calm, keep your voice low and offer to assist them in resolving the issue. If resolution is impossible, please involve the Client site coordinator for assistance.
Do not argue with a Participant or allow yourself to be provoked into doing anything that is against nursing practice or your best judgment.
Eating, drinking and cell phone usage are prohibited at all screening work areas. Eating is permitted only in the client’s designated areas. Water is acceptable if stored in a discreet manner.
Please refer to your Medical Professionals Best Practices form for a complete list of policies and procedures.
Clinic Policies
Blood Policy
Gloves must be worn on both hands. Do not reuse gloves. A new pair is used for each Participant. If you have blood on them, dispose of
them in the biohazard container. If you have a bloody cotton ball, dispose of it in the required biohazard container. Do not use your gloved finger to stop the injection site from bleeding. Use gauze to control the bleeding and then
place a bandage over the site. No needles / biohazard items are allowed in the client trash can.
Filling Syringes
The flu vaccine is contained in 5.0 to 5.50 mL vials. Because one standard Adult dose equals 0.5 mL, there should be enough vaccine per vial for 11 to 12 doses using the syringes provided. A nurse may fill a syringe using multiple vials as long as they are from the same lot number.
Vaccine Lot Numbers
When a vaccine is produced, it is marked by a lot number. Lot numbers may vary by shipment. It is important to document, on the Consent Form which lot number the vaccine comes from in the event it is recalled or should a reaction occur. The lot number must be recorded by the nurse on the Consent Form at the time the vaccination is administered.

Rev. 9/8/2010 15
Chapter 3: Clinic Preparation & Operation
Clinic Set-Up
1. Lead Nurse Duties
The Client site coordinator contact information is located on the Work Order Confirmation which you will receive for each clinic.
Call your Client site coordinator 72 hours prior to the clinic date to:
a. Always reference Summit Health in your introduction call to the Client site coordinator. We also suggest you make a note of the date / time and who you spoke with on your Work Order Confirmation.
b. Get directions and parking instructions from the client site coordinator if you are not familiar with their location.
c. Verify the clinic time and date. d. If the WOC states the clinic paperwork was shipped to the client site contact remind the client to bring
the paperwork including the consent forms they received from Summit Health to the clinic at the arrival time.
e. Familiarize yourself with the requirements of each clinic. Do not guess on the requirements of a clinic. Do not proactively ask the client to verify the number of their expected participants or vaccines they will require. However, if the Client site coordinator asks you to verify the amount of vaccines you will be bringing, you may provide them with the information as stated on your Work Order Confirmation. If the client requests you to provide anything different other than what the work order confirmation requires, advise them to contact their SH program manager immediately.
f. Confirm that the clinic site will have an area available for your clinic set up, along with a table, chairs, and a trash container.
g. Make sure that you have a Large Envelope with clinic paperwork for each clinic that you staff if noted on your Work Order Confirmation. If the WOC states the paperwork was shipped to you the staff, be sure it is included in your Flu Kit and take it with you.
2. Arrival Protocol
Arrive at the time stated on the Work Order Confirmation. It is your responsibility to arrive 60 minutes prior to scheduled start time.
IMPORTANT:
a. If a situation arises and you are not able to cover your clinic, call your Agency Office immediately. Do not wait. Then, call SH immediately. The SH Independent Nurse must contact Summit Health immediately. If you are not able to reach SH, notify your Client site coordinator to let them know your status.
b. It is not acceptable to arrive at the clinic site late. If you arrive at the clinic start time—you are
LATE! If you are delayed for some reason beyond your control, please call the Client site coordinator and let them know and then call the SH Staffing coordinator. Communicate!
c. When you arrive, find your Client Site Contact and introduce yourself as representing Summit Health,
and then set up the clinic. Make sure that table/ chairs/wastebaskets have been provided by the Client Site Contact. If you arrive and the Client Site Contact has not provided space or table/ chairs/wastebaskets, contact the SH staffing coordinator immediately.
d. Ask the Client site coordinator to provide you with the Consent forms and the Administrative Kit mailed
to them by Summit Health if stated on your WOC. The Administrative Kits include the following: consent forms, VIS forms, SH Privacy Forms, clinic record, incident report, pens/pencils, sharpeners, confidential return envelope, UPS/return package (for participant consents).

Rev. 9/8/2010 16
3. Clinic Set-up Clinic staff is to set up the immunization clinic in the location designated by the client. All clients have
been requested to provide tables, chairs, and trash cans to be setup prior to the arrival of the nurse. If the table/ chairs/wastebaskets are not set up, ask the Client site coordinator for assistance. The clinic layout will vary based on location.
A sample clinic layout is as shown:
Table
Customer Line
Nurse Patient
Table
Customer Line
Nurse Patient
Place a tablecloth on the table and the trash can under the table. Then, post any appropriate signage on the table.
Workflow Tips
Arrange clinic materials on the table in a manner that will enable you to vaccinate Participants quickly and efficiently. The clinic area is to be kept organized, neat, and professional in appearance. Take the time to organize all of your materials, vaccines, supplies, paperwork, and all promotional literature so that your clinic will run efficiently. Sometimes space is very limited, but you must remain organized.
Do not pre-draw any vaccine. Never open more than one vial of product per nurse station to assist in eliminating waste. At end of clinic, date and sign the label on any open vial containing unused serum.
Have plenty of blank Consent Forms and Pens / Pencils, dependent on the Consent Form to be used.
For Scantron Consent forms, No. 2 Pencils are to be used. Do not use Ink Pens. Make solid marks, completely fill in the appropriate bubbles where required.
Review your Work Order Confirmation for the clinic protocols as they relate to each clinic (i.e., Medicare, insurance, payment methods, etc.)
4. Starting the Clinic
Once the clinic staff is set up, the Lead Nurse should start the clinic even if the start time is prior to the advertised or scheduled start time. Inform the client that you are opening the clinic and remember:
1. Record the clinic starting time on the Clinic Record Form. 2. Communicate with Participants and form a line for those who are waiting.
Ask all waiting Participants to read the VIS form and then read and sign the Consent Form. While they are standing in line, reiterate to Participants the risks and contraindications for the requested
vaccination. Typically, if reactions occur, it is because of poor screening prior to injection, or because the injection is
not given in the proper location (refer to Vaccination Policies). Be very repetitive with instructions and information. The Participants have selective hearing; keep
verbalizing instructions and information throughout the clinic. Don’t be shy. If you have a line, keep talking and keep the Participants organized.
3. The nurse must begin clinics by using partial vials first. 4. Review the Work Order Confirmation and the Consent Form to familiarize yourself with the fields that are
applicable for your particular event.

Rev. 9/8/2010 17
The payment methods to be checked by clinic staff are as follows: Cash, Check, Medicare, CIGNA, Invoice Company and Other.
o For Medicare or authorized insurances SH accepts, please be sure to ask the participant to show you their insurance card and verify the number(s) on their card with the number(s) they wrote down on their consent form. If the number is not legible, please re-write the number on the top of the form. Make sure each Participant signs the Consent Form. The Consent Form is used to either invoice the participant’s employer or submit for billing an
insurance claim to the authorized insurance carrier. Make certain that the form has been properly and legibly completed.
Clinic Shut-Down
1. Close down the clinic at the published end time as indicated on the WOC. If customer line exists and supplies will support additional vaccinations, call SH for an Authorization Code (simple and quick process) to continue the event until the line is exhausted. It is imperative that you call for an Authorization Code as this will eliminate payment issues when payroll and invoicing are processed. SH will authorize the extension of the clinic (notify the SH corporate office immediately to obtain an authorization number). It is imperative that clinics operating beyond the scheduled times be authorized to continue to provide services. Record the authorization code provided by the SH staffing coordinator on the space provided on the Clinic Record form.
► If time/supplies do not permit the extension of the clinic, notify the customers before the end of the
clinic that time/supplies do not allow us to provide the service and notify them about any clinics scheduled for future dates.
► Thank the Client site coordinator for hosting a clinic.
2. Repack all used vaccine and medical supplies (pack out what you bring in). Mark open vaccine vials with the date and sign the vial. Transport accordingly.
3. Close sharps containers(s) for transportation and disposal at the home office. It is each office’s responsibility to
arrange for the sharps/medical waste disposal. Do not return filled sharps containers to SH.
4. Take down the signs and clean up the area where the clinic was conducted.
5. Remove all used tablecloths from tables and discard in wastebaskets provided by client.
6. When all non-biohazard waste has been disposed of, tie all trash bags in wastebaskets provided by Client site coordinator.
7. Complete the Clinic Record Form. The designated nurse or lead will complete this form. To complete the
Clinic Record form, the designated/lead nurse must refer to the Work Order Confirmation to obtain most of the data needed.
8. Organize all paperwork. Place all consent forms, separated by type of payment, into the large confidential envelope provided. Place the following forms in the Large Confidential Envelope:
► Completed Participant Consent Forms ► Clinic Record form – White Copy ► Vaccine Adverse Event Reporting Forms (VAERS, if applicable) ► SH Incident Report Forms (if applicable) ► If applicable place checks/money orders in package

Rev. 9/8/2010 18
9. a) If the WOC states the client is responsible for shipping the completed paperwork back to Summit Health, seal the confidential envelope and provide it along with the pink copy of the clinic record to the client site contact.
b) If the WOC reflects the medical staff as responsible for returning the completed paperwork, seal the confidential envelope and provide only the pink copy of the clinic record to the client site contact.
10. Remove all remaining/unused documents off site.
11. Retain the yellow copy of the Clinic Record form for yourself for 90 days.
12. If you are required to return the completed clinic paperwork at this time locate the pre-paid, self addressed return package provided in you Flu Kit. Place the confidential envelope in the pre paid return package and seal. Record the UPS tracking number from the return package onto your copy of the clinic record and again retain for 90 days. Drop the UPS package with the completed clinic documents in the appropriate carriers shipping bin.
Return Sharps containers to your Local Staffing Office for proper handling. Independent Nurse will follow SH guidelines for return of sharps containers.
Post-Clinic Follow Up
After each clinic, the Agency Contact or Independent Lead Nurse should:
1. Reconcile the number of vaccine vials returned from the clinic with the number of vaccinations provided. 2. At Events where the Nurse Collects Payments, reconcile the cash, checks or money orders with the number of
vaccinations provided. No cash should be mailed; any cash received should be converted into a money order. * Summit Health makes every effort to dissuade the collection of money at events; however there will be a few occasions where participants will be allowed to make direct payments to you for their vaccinations.
3. Dispose of bio-hazardous waste generated by the clinic following all required guidelines.
4. Using the white copy of the clinic record form, record the number of shots administered after each clinic in the Portal. When mailing the completed participant consent forms and the clinic receivables, record the UPS tracking number on the return package, provided in your Flu kit, onto the clinic record form. Include 1 copy of the clinic record form in the confidential envelope and retain 1 copy for yourself for 90 days. Mail package to Summit Health immediately.
5. For Corporate or pharmacy clinic (excluding Spartan) retrieve the clinic record and the confidential envelope from the administrative kit provided to you by the client site coordinator. Complete the clinic record form. Place all consents in the envelope, place 1 copy of the clinic record form in the envelope with the consents. Seal the envelope. Provide the client site coordinator with a copy of the clinic record form and keep the 3rd copy of the clinic record form for yourself for 90 days.
6. Remove all remaining supplies such as: all unused paperwork, tablecloths, garbage bags, vaccine, needles, EPI kits, pens, pencils etc from the client site and take with you.
SH has provided pre-addressed Summit Health Corporate Courier account (UPS) bags to mail back the Large Clinic Envelopes. In situations where the office has a large number of flu clinics, the office will need to return the paperwork every two to three days. Please keep a copy of the shipping label or retain the UPS tracking number from the shipping label in the event SH needs to track the shipment.
Summit Health, Inc.
25300 Telegraph Road, Suite 250
Southfield, MI 48034 248 799-1542

Rev. 9/8/2010 19
Chapter 4: Vaccine Administration
Participant Eligibility Rules
Immunization Process
1. Review - the Nurse must review, in detail, the Medical Directive (refer to physician’s orders located in Sample Forms section).
► Select the vaccine based on participant’s age. ► Identify the name of the vaccine to be administered, the correct dose, and the route.
► Identify the appropriate response for any anaphylaxis reaction.
► Compare the Medical Directive for Storage and Administration of Vaccine to the vaccine(s) and
anaphylaxis drugs and supplies that have been provided to ensure the correct products have been supplied to the clinic.
2. Consent Form - Each Participant must complete a Consent Form. If a participant does not complete and sign
the consent form, do not administer the immunization.
3. Answer questions – answer any questions the Participant may have before proceeding with the immunization(s).
4. Vaccine Information Statement (VIS) is a separate Form, with a CDC Mandate that the participant must review prior to receiving the immunization. In addition, the VIS edition and date the participant reviewed will be added to new consent forms.
5. Determine eligibility – decide if the Participant is a candidate to receive the immunization(s) requested (the
nurse has the discretion to refer any Participant to his physician). Then: Verify that the Participant is at least 18 years of age (refer to specific client protocols for age restrictions)
Immunizations will not be administered to minors under 9 years old. Minors (Participant under 18 years old) must have signed parental consent prior to the administration of the vaccine. Typically, Summit Health does not vaccinate anyone under the age of 18. Some exceptions will apply. Please refer to your Work Order Confirmation.
Except at Home Depot clinics, Summit Health does NOT vaccinate pregnant women nor nursing mothers. Do NOT administer to women who may be pregnant or breast-feeding (even with a doctor’s note), refer them to their physician. Review the screening question portion of the Consent Form with the Participant. If the Participant
answered “Yes” to any of the screening questions, refer them to their physician to receive the vaccination.
If anyone has experienced any of the conditions listed with the Helpful Reminders, do not provide them with a vaccination. Politely explain to them that there is a possibility of a reaction. Request they consult their physician. If you have any concerns about the potential reaction from vaccinating someone, do not vaccinate.
If a Participant has ever experienced a reaction to an influenza vaccination, deny vaccination and
request that they consult their physician.
6. Pneumonia shots - will be administered at select sites and retail-based locations (refer to your specific Work Order Confirmation for details.) Pneumonia shots are effective for a five year period. If a Medicare Part B Participant requests a pneumonia shot, verify that they have not received a shot within the last 5 years.

Rev. 9/8/2010 20
7. Verify Consent – confirm that all portions of the Consent Form have been filled out correctly, are legible and
signed. 8. Payment method – To determine the method of payment for the clinic participants refer to the Work Order
Confirmation. At the bottom of each participant consent form, you are required to select the appropriate payment method(s) for each person receiving vaccination. The payment options are as follow: Cash, Check, Medicare, CIGNA, Invoice Company and Other. In most of the Employer locations, money will not be collected from the Participant. If the employer is paying, mark the box for “Other” and write INVOICE Company.
If a spouse or other non-employee is present and has to pay for the immunization at a corporate function,
only checks will be accepted. Please refer to your WOC for the Method of Payment for each clinic. Cash payment collection – Cash, money orders or checks are the only accepted form of cash payment.
Checks or Money Orders must be made out to Summit Health. All cash received must be transferred into a Money Order at the end of the clinic.
Collect payment or Medicare Part B information (see Immunization Clinic Documentation section).
There will not be any Medicare Part B for the Employer Groups
Medicare Part B Payment - verify the Participant’s Medicare Part B eligibility. All of the information on the Consent Form must be completed accurately in order to bill Medicare Part B. SH will not be able to bill Medicare Part B without complete beneficiary information (see Medicare Information section). Please make sure the Participant signs the Medicare Part B section. The Medicare Information Sheet should be placed on the table as a reference for both the Participant and nurse.
9. Administer the vaccination(s) – administer vaccines according to the Medical Directive for Purchase, Storage
and Administration of Vaccine and this manual. Remember to use partial vials first.
During the administration and preparation, nurses must wear gloves and change both gloves after each Participant and sanitize hands.
The GSK influenza vaccine (FluLuval) for participates age 18 and above.
The Novartis influenza vaccine (Fluvirin) can be used for all participants between the ages of 9 and 18. However, Summit Health typically does not vaccinate anyone under the age of 18. Some exceptions may apply and will be comminucated on the Work Order Confirmation.
10. Post-vaccination - any Participants needing or requesting a bandage should have one applied
11. Complete Consent Form – after administration of the injection, record the Vaccine Lot Number, Dose, and Route/Site used for vaccination on the Consent Form. Sign and date the bottom of the Consent Form, document the time the vaccination was administered. For Scantron Consent forms, separate the VIS/Notice of Privacy practices form and give it to the participant. For Multi Page Consent forms, give the Participant Copy (Yellow Copy) to the Participant. 12. Instruct the Participant to wait – tell the Participant to wait for 10-15 minutes in the clinic area to ensure there
is no reaction. Allergic reactions are usually immediate, though in very rare instances there can be a delayed reaction.
Vaccine shortage - If the nurse runs out of vaccine, clinic staff should try to contact the Local Staffing Office for more vaccine, and contact Summit Health. If this is not possible, the clinic should be closed, the client informed, and the stop time recorded on the Clinic Record Form. Call SH to report.

Rev. 9/8/2010 21
Safety Procedures
Standard Precautions
Each nurse is expected to be compliant in the use of CDC Universal Precautions and Exposure Control during the Clinic. Non-latex disposable gloves are provided and must be worn when administering an injection.
If clinics are providing more than one type of vaccine, separate the different vaccines to avoid confusion and misidentification of vaccines. For example, if the clinic is providing Flu and Pneumococcal vaccines for Participants, the nurse should identify and segregate flu vials from pneumonia vials and verify the requested vaccination with each Consent Form.
DO NOT DISPOSE OF PARTIALLY-USED VIALS OF VACCINE. They are to be refrigerated for use in the next vaccination clinic. Label partially-used vials with the date the vials were accessed, and sign the vial. Return to the Local Staffing Office as indicated.
Participant Safety
Ensure Participant safety by making the Right decisions.
5 Rights of Medication Administration
1. Right DRUG: Have you verified the identity of the vaccine that you are about to administer? Have you read the label of the vaccine and verified it against the written protocol and physician’s order for this particular clinic?
2. Right DOSE: Have you verified and drawn up the correct dose according to the written protocol and
physician’s order?
3. Right ROUTE: Have you read the vaccine protocols and do you know the right route of administration?
4. Right TIME: Have you taken the time to double-check the label? Have you taken the time to review the immunization clinic procedures?
5. Right PARTICIPANT: Have you obtained a signed Consent Form that identifies both the Participant and the
vaccine? Do your Participants meet the requirements of the Consent Form (i.e. age, allergies, etc.)?
Vaccine Selection Based On Age of Participant
IMPORTANT ! The Inflenza Vaccine used is Age dependent:
The GSK influenza vaccine (FluLuval) for participates age 18 and above.
The Novartis influenza vaccine (Fluvirin) can be used for all participants between the ages of 9 and older.
Biohazard Waste Disposal
Clinic supplies include a sharps container. All needles, syringes, and used vaccine bottles
and blood contaminants are placed in the sharps container. Safety needles / syringes are used for both your and your patient’s safety. At the end of the clinic the sharps container is sealed and transported off the client site. NEVER LEAVE a sharps container with used syringes at a
clinic site. Do not send used sharps containers back to SH.
All remaining waste products (needle caps, used alcohol preps, gauze, band aids, adhesive tape, paper towels, and used gloves) are disposed of in the lined waste receptacle provided by the client.

Rev. 9/8/2010 22
Safety Needle / Syringe Usage
For the 2010-2011 Vaccination season, the BD Integra 1ml Syringe with Retracting needle or the InviroSnap Safety Syringe have been selected to be used as the vaccine delivery device. * If substitution is required due to availability, a similar Safety Device will be supplied.
The Nurse is to follow Manufacturer guidelines for the appropriate usage of this safety device. With the usage of the Retracting needle device, the needle is retracted into the barrel of the syringe after activation, and will no longer be visible. Please note the insert below. The Nurse must familiarize her/himself to the appropriate and proper use of this safety device.
* If supplies vary during the Flu Season, please familiarize yourself with proper usage of the safety needle / syringe unit received.
How to Use the InviroSNAP! Retractable Safety Syringe
Rev. 9/8/2010 23
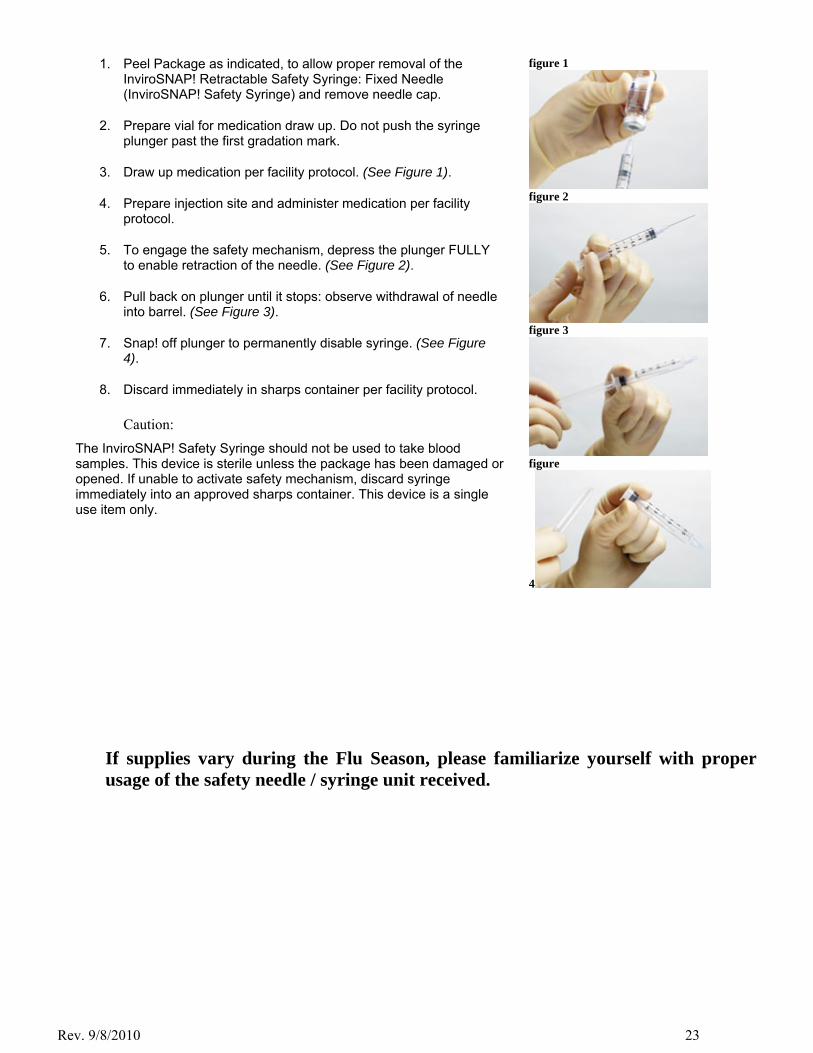
1. Peel Package as indicated, to allow proper removal of the InviroSNAP! Retractable Safety Syringe: Fixed Needle (InviroSNAP! Safety Syringe) and remove needle cap.
2. Prepare vial for medication draw up. Do not push the syringe plunger past the first gradation mark.
3. Draw up medication per facility protocol. (See Figure 1).
4. Prepare injection site and administer medication per facility protocol.
5. To engage the safety mechanism, depress the plunger FULLY to enable retraction of the needle. (See Figure 2).
6. Pull back on plunger until it stops: observe withdrawal of needle into barrel. (See Figure 3).
7. Snap! off plunger to permanently disable syringe. (See Figure 4).
8. Discard immediately in sharps container per facility protocol.
Caution:
The InviroSNAP! Safety Syringe should not be used to take blood samples. This device is sterile unless the package has been damaged or opened. If unable to activate safety mechanism, discard syringe immediately into an approved sharps container. This device is a single use item only.
figure 1
figure 2
figure 3
figure
4
If supplies vary during the Flu Season, please familiarize yourself with proper usage of the safety needle / syringe unit received.

Rev. 9/8/2010 24
Vaccination Policies
Intramuscular Injection – Vaccine Clinical Procedure
Intramuscular injections may only be given by persons licensed to do so, such as LPN’s, RN’s, PA’s (refer to State Board of Nursing Guidelines). If two vaccines are to be given to the same client at the same time, one vaccine will be administered in the right deltoid and one vaccine will be administered in the left deltoid. If the Participant does not have both deltoids available, the vaccine may be administered in an alternate muscular site. The site must be documented.
Immunization Clinical Procedure
1. Verify consent (ask questions, verify, signature, etc.). 2. Change both gloves after each injection and sanitize hands 3. Gather materials – syringe containing intramuscular needle, 5/8” or 1”, 23 or 25 gauge, syringe. 4. Swab top of serum vial, and invert. 5. Inject needle and withdraw appropriate amount (0.5ml or ½ cc for flu or pneumonia). 6. Withdraw needle from vial and purge any air, being careful not to waste serum. 7. Loose clothing is advised. Have the Participant expose the area in which the injection is to be given. Do not
allow restrictive clothing to be bunched above the injection site (this causes unnecessary bleeding, soreness, and misplacement of the injection).
a. Draw an imaginary horizontal line at the level of the shoulder bone (acromion process) and at the level of the lower edge of the armpit (axilla).
b. Injection site is within the center of the imaginary lines. c. The upper arm muscle is much smaller than other muscles often used for injections. d. The needle is inserted until the tip of the needle is in the middle of the thickest part of the muscle.
This will be a shorter distance for thin people and a longer distance for heavy people. e. Do NOT give two injections in the same deltoid muscle.
8. Clean injection site in a circular motion with alcohol prep, begin at the point of injection and move outward for a distance of about 1 to 2.5 inches. Allow the site to dry before administering the injection.
9. Pinch a two-inch fold of skin with the other hand. With one quick motion, inject the needle into the skin using an injection angle of 90°.
10. While holding the syringe steady, release the two-inch fold of skin. 11. Before injecting, pull back on the plunger to make sure there is no blood in the syringe.
Blood in the syringe indicates that the needle was placed in a vessel. If this occurs, remove the needle, discard the syringe, and prepare a new syringe and injection site for injection.
12. Slowly and evenly inject the serum until the syringe is empty. 13. Pull the needle out quickly while holding firm pressure at the injection site with a cotton
ball. 14. Dab injection site with cotton and put a bandage on the injection site. 15. If bleeding occurs, apply pressure until it stops. 16. Dispose of used syringes after activation of safety device into the sharps container. Do not recap needles. 17. Document date, site of injection, lot number, expiration date, and manufacturer on the consent form. 18. Advise the Participant to stay in the general area 10-15 minutes for observation.

Rev. 9/8/2010 25
Subcutaneous Injection - Epinephrine Only - Clinical Procedure
1. Verify consent (ask questions, verify, signature, etc.). 2. Change both gloves after each injection and sanitize hands. 3. Gather materials – syringe containing subcutaneous needle: 25 gauge by 5/8” or 1”. (Insulin syringes are used
exclusively for subcutaneous injections). 4. Epinephrine is provided in 1cc Ampoules, swab the vial and break off top, place the top in the sharps container.
The needles supplied with the EPI Kit are created to filter the serum when aspirated. 5. Inject needle and withdraw appropriate amount. 6. Withdraw needle from vial and purge any air, being careful not to waste serum. 7. Change out the filtered needle. 8. Have the client expose the area in which the injection is to be given. Do not allow restrictive clothing to be
bunched above the injection site (this causes unnecessary bleeding, soreness, and misplacement of the injection). o Usual sites for subcutaneous injection in a clinic situation are the right and left upper, outer arm
regions, just below the deltoid muscle. o If two injections are required, give in the same area of fatty tissue a minimum of 1 inch apart.
9. Clean injection site in a circular motion with alcohol prep, begin at the point of injection and move outward for a distance of about 1 to 2.5 inches. Allow the site to dry before administering the injection.
10. Uncap the needle and hold the syringe in the hand you will use to inject the needle into the skin. 11. Pinch a two-inch fold of skin with the other hand. With one quick motion, inject the needle into the skin using
an injection angle of 45° to 90°. 12. Hold the barrel of the syringe steady and release the two-inch fold of skin. 13. Gently retract the plunger slightly to assess for any blood in the syringe. If no blood is present, push in the
plunger to inject the vaccine. If blood is present, remove the needle, discard the syringe using appropriate disposal technique and prepare a new syringe and a new site for injection.
14. Slowly and evenly inject the serum until the syringe is empty. 15. While holding a cotton ball at the injection site, pull the needle from the skin. Gently wipe the site with the
alcohol swab. Do not massage the area. 16. Dab injection site with cotton and put a bandage on the injection site. 17. If bleeding occurs, apply pressure until it stops. 18. Follow procedures for safety needle closure, dispose of the used needle and syringe in the sharps container. 19. Document date, site of injection, lot number, expiration date, and manufacturer on the Consent Form.
Reminder:
If a Participant requests more than one immunization, indicate to them that there is a higher probability of a localized reaction.
If two injections are requested, place one in the left arm and one in the right arm.
Do not give two injections in the same arm on the same day.
Restrictive clothing may cause bruising/swelling at injection site (ask them to remove shirt if it is too
restrictive). Instruct the Participate to use the muscle vigorously for the next 48 hours.

Rev. 9/8/2010 26
Influenza Vaccination Procedures
Do NOT administer influenza vaccine if Participant:
Has an elevated temperature of 101°F or higher or is currently on an antibiotic. Has had an adverse reaction to a previous dose of the Flu or other Vaccine. Is pregnant or breast-feeding, refer them to their physician (Except for Home Depot) Under the age of 9 years old. Is allergic to eggs, chicken, chicken feathers, or thimerisol (preservative found in contact lens solution). Has an active neurological disorder (for example, MS, Guillain – Barre Syndrome). Cannot understand the consent form due to language differences.
Influenza dosage and Type based on Age
Give 0.5 ml (1/2cc) intramuscularly in the deltoid muscle. Use a 23 or 25 gauge by 5/8 to 1 inch, or longer, needle
► The Inflenza Vaccine used is Age dependent:
The GSK influenza vaccine (FluLuval) for participates age 18 and above, will be the most commonly used.
The Novartis influenza vaccine (Fluvirin) can be used for all participants between the ages of 9 and over, will predominately be used at retail stores. Summit Health typically does not vaccinate anyone under the age of 18. Some exceptions will apply. Please refer to your Work Confirmation Order.
Symptoms
Inform Participants about symptoms which may occur:
Sore/hot arm around injection site, possible fever, chills, or headache lasting 24 to 48 hours. Possible risk of anaphylactic reaction.
Ask
Participant to stay in the area for 10-15 minutes in the rare event that an anaphylactic reaction should occur (especially first timers).
If a person has received a flu shot in the recent past without a reaction, chances are that they will not incur a problem and are probably not allergic. However, it is suggested that they remain nearby for observation.
Remember
This vaccine is manufactured from dead virus; it will not cause the patient to get the flu. It takes two weeks to fully protect the client. If a Participant gets the flu during that two week span, they will not
be fully protected. Every Participant must complete a Consent Form with the lot number and manufacturer name recorded on the Consent Form.

Rev. 9/8/2010 27
Pneumonia Vaccination Procedures
Do NOT administer pneumonia vaccine if Participant:
Has a history of neurological symptoms or ever had Guillain – Barre Syndrome. Has had an adverse reaction to a previous dose of the Flu or other Vaccine. Is pregnant or breast-feeding, refer them to their physician. Is under the age of 18 without a physician’s order. Has a febrile respiratory illness or active infection. Has received a prior Pneumococcal vaccination within the past 5 years. Cannot understand the consent form due to language difficulties.
Pneumonia dosage
Give 0.5 ml (1/2cc) intramuscularly in the deltoid muscle. Use a 23 or 25 gauge by 5/8 or 1 inch needle.
Symptoms
Inform Participants about symptoms which may occur:
Sore/swollen area or rash at the injection site. Possible low-grade fever subsiding within 24 to 48 hours. Possible risk of anaphylactic reaction.
Ask
Participants to stay in the area for 10-15 minutes in the rare event that an anaphylactic reaction should occur (especially first timers).
Remember
This vaccine is not made from the actual bacteria, but from a non-infectious extract. This vaccine immunizes against 23 of the most prevalent strains of pneumonia.
Do not ever give pneumonia and tetanus at the same time. A two week separation is suggested. Every Participant must sign a Consent Form with the lot number and manufacturer name recorded on the
Consent Form.
Re-Vaccination
1. Medicare pays for pneumonia every 5 years. If Participant cannot remember, refer them to their doctor. 2. If a Participant has received a prior Pneumococcal vaccination, re-vaccination is recommended if the adult was
younger than age 65 and received the vaccination 5 or more years ago.

Rev. 9/8/2010 28
Chapter 5: Adverse Reaction Protocol
Adverse Reactions
In the event of an allergic or anaphylactic reaction or medical emergency occurring while the nurse is on-site at the clinic, it is the nurse’s responsibility to act appropriately and within the scope of nursing practice to treat the medical emergency until emergency medical personnel arrives.
All clinic Participants are screened for any allergies/medical conditions that contraindicate administration of the vaccine, and must sign a consent form prior to vaccine administration. It is the nurse’s responsibility to review the signed Consent Form for Participant specific responses (to avoid reaction occurrence) prior to administering the vaccine.
Nursing staff must make a judgment call regarding the potential for a reaction. After reviewing the consent, if a possibility of an allergic or anaphylactic reaction exists, the nurse MUST NOT administer the vaccine. Instead, the nurse will follow this procedure:
1. The nurse informs the Participant of the reason for the refusal to administer the vaccine and refers them to his/her personal physician. 2. The nurse then documents on the Consent Form why the vaccine was not given and marks a diagonal line
across the Consent Form indicating that no vaccine was provided. 3. If the Participant is unhappy with the nurse’s refusal to administer the vaccine, he should be given the SH
office phone number for further follow up.
Upon receiving the vaccine, the Participant is verbally informed to stay for 15 minutes in the clinic vicinity for observation of an adverse reaction. It is the nurse’s responsibility to advise the participant to stay for observation.
In the event of a health emergency, call 911, initiate emergency response, and notify your office as soon as possible. All anaphylactic reactions are sent to the ER, regardless of severity.
Emergency Treatment Procedure
In the event of a medical emergency:
1. Lead Nurse evaluates the Participant to determine the cause of the medical emergency (allergic reaction, anaphylactic reaction, medical emergency unrelated to vaccine administration, such as heart attack, diabetic reaction, etc.) and/or records vital signs on the back of the consent form, and then administers Epinephrine, if necessary (per anaphylaxis policy).
2. Document all side effects from the injection properly (time, symptoms) on the back of the Consent Form. 3. Take B/P and pulse 5 minutes apart, up to 4 times to rule out anaphylaxis. 4. Maintain Participant airway as necessary. 5. Initiate CPR as necessary. 6. Place unconscious Participant in shock position. 7. Monitor vital signs until ambulance arrives. 8. Assess Participant’s status for need of further interventions until emergency medical personnel arrive. 9. Do not ever allow a Participant to leave the clinic if he is not feeling well. 10. Inquire about other health issues, food intake, etc.

Rev. 9/8/2010 29
Anaphylactic Reaction (Anaphylaxis)
Definition
Anaphylaxis is an exaggerated hypersensitivity reaction to a previously-encountered antigen. A severe reaction may precipitate vascular collapse, leading to systemic shock and sometimes, death.
Causes
Anaphylaxis results from exposure to sensitizing drugs or other substances. It may result from drugs such as penicillin (the most common cause), other antibiotics, serums, vaccines, allergen extracts, enzymes, hormones, anesthetics, salicylate, and polysaccharide.
Assessment
An anaphylactic reaction is an emergency and usually produces sudden distress within seconds or minutes after exposure to the allergen. A delayed or persistent reaction may occur up to 24 hours later. The severity of symptoms depends on the original sensitizing dose of antigen, the amount and distribution of antibodies, and the route of entry and dose of antigen.
Initial signs and symptoms may include:
Feeling of impending doom or fright Difficulty breathing, wheezing Sweating Sneezing Pruritus (itching) and/or urticaria (rash) Angioedema (swelling of blood vessels)
Cardiovascular signs may include:
Hypotension, (blood pressure dropping, increased pulse rate) Dysrhythmia (irregular heart beat) which may precipitate circulatory collapse
Respiratory signs may include:
Nasal mucosa edema Profuse watery rhinorrhea Sudden sneezing attacks Wheezing Hoarseness, Stridor and Dyspnea, early signs of acute respiratory failure
G.I. and G.U. signs may include:
Severe stomach cramps Urinary urgency and incontinence Diarrhea
For any symptoms or reactions, recommend that the participant contacts their primary care provider for further follow-up and medical evaluation, even if symptoms resolve completely; as symptoms can reoccur as much as 24 hours later.

Rev. 9/8/2010 30
Epinephrine Administration
Systemic Anaphylaxis
TYPE SYMPTOMS ACTIONS Local Mild Pain
Redness
Itching or swelling at injection site
Apply Ice to site and Observe for 30 minutes
Mild Systemic Anaphylaxis
Itching
Redness
Hives
Swelling around the mouth and lips
Administer epinephrine
Dial 911
May repeat up to a maximum of three (3) times
See the Proper Dosage Table below for proper doses
Severe Anaphylaxis Feeling of impending doom
Difficulty breathing
Wheezing
Sweating
Sneezing attacks
Itching, rash, hives
Blood pressure drop
Increased pulse rate
Severe abdominal cramping
Diarrhea
Respiratory and/or cardiac arrest
Administer epinephrine
Dial 911
May repeat dose every 10‐20 minutes to a maximum of three (3) doses
Keep patient lying down unless he/she has breathing difficulty
Monitor BP, pulse, and respirations every five (5) minutes & record results on back of Consent Form
Maintain airway
Perform CPR if necessary
Proper Epinephrine Dosage Table
Age Weight
5 years 0.20 mL (0.20 mg) 51 to 60 lbs: Epinephrine (1:1000). 0.25 SQ
6-9 years 0.30 mL (0.30 mg) 61 to 70 lbs.: Epinephrine (1:1000) 0.3cc SQ
10-13 years 0.40 mL (0.40 mg) 71 to 80 lbs.: Epinephrine (1:1000) 0.35cc SQ
14+ 0.50 mL (0.50 mg) 81to 100 lbs.: Epinephrine (1:1000) 0.40cc SQ
100 lbs or more : Epinephrine (1:1000) 0.5cc SQ
► IF Epinephrine is administered, Dial 911. ► Anyone receiving Epinephrine must be sent to the Emergency Room.
Fainting - Incident Protocol
Record the Patient’s vital signs every five (5) minutes, medications given, time given, dosage, participant's response, and name of nurse administering medications. During the emergency assign someone to write down this information for you.
Complete and send an Incident Report to SH. Fax (248)799-0876
Rev. 9/8/2010 31
At Immunization and Health & Wellness events, the most common concern is Fainting or Syncope. Some individuals may state they have a “problem” with blood draws, however treat all individuals as if fainting may occur. For events where the individuals have been Fasting, there is an increased possibility of fainting or dizziness occurring.
Start by explaining what the procedure is and that it will be over quickly. Have the individual in a relaxed sitting position, leaning back in the chair and both feet flat on the floor, which promotes blood circulation and breathing. If the participant notes that they “have had problems with this before” or “became faint”, elevate their feet on another chair prior to starting the procedure to assist in preventing symptoms.
It is not uncommon that some people actually hold their breath unknowingly during a procedure. It is helpful then to talk with them throughout the procedure so that they are answering your questions (breathing), and distracted from what is occurring. Be aware of the participant at all times, note any change in tenseness, coloring, breathing or sweating and immediately respond.
FAINTING:
Fainting occurs when the blood supply to the brain is momentarily inadequate, causing the individual to lose consciousness and is usually brief. Fainting can have no medical significance, or the cause can be a serious disorder. Therefore, treat loss of consciousness as a medical emergency until the signs and symptoms are relieved and the cause is known. In all incidences, the Site Contact or their designated person must be notified of the occurrence immediately.
Fainting - Early signs:
Pallor (paleness, loosing color noted in the skin or lips)
Perspiring / sweating or stating they are Cold / chilling
Yawning
Ringing in ears or Visual Disturbances
Nausea
Action:
Have participant seated and elevate their feet, non-rolling chairs should be used
Have them loosen the clothing around the neck, also their waist if constrictive
Remind them to relax and breathe slowly, in through the nose and out through the mouth.
Apply cold compresses to the back of the neck and forehead if available
Offer participant orange (or similar) juice, if available
Monitor the participants BP and Pulse every 5 minutes until symptoms clear.
Have the participant remain seated until symptoms are gone, typically 5 – 15 minutes
After symptoms subside, have them sit with their feet on the floor for 1 – 2 minutes before standing. Verify all symptoms are gone before they begin walking / leave the area
Fainting / Loss of Consciousness - Late Signs:
Loss of consciousness, not responding to stimuli
Slow pulse
Some rhythmic jerking movements of extremities
Action: Follow the guidelines for First Aid “ABC’s, which focus on the lifesaving assessment of the Airway, Breathing and Circulation, and appropriate intervention.
Lie person flat to Help restore blood flow - If the person is breathing, restore blood flow to the brain by raising the person's legs above the level of the head. Position the person on his or her back. Elevate the legs above heart level — about 12 inches (30 centimeters), if possible.

Rev. 9/8/2010 32
Loosen clothing - Loosen belts, collars or other constrictive clothing.
Check the person's airway - Clear any obstructions, watch for vomiting. If vomiting occurs, turn the patient on their side to prevent choking.
The person should revive quickly. If the person doesn't regain consciousness within 1 – 2 minutes, dial 911 or call for emergency medical assistance. Immediately have Site Contact notified if they are not in the area. Follow the site guidelines if they have Emergency Protocol in place.
Monitor Vital Signs every 5 minutes. Monitor the BP and Pulse for improvement, writing down for medical personnel reference.
Check for signs of circulation (breathing, coughing or movement). If the person is not breathing, begin CPR. Call 911 or your local emergency number. Continue CPR until help arrives or the person responds and begins to breathe. Follow the site guidelines if they have Emergency Protocol in place.
If seizure activity is present, your first goal is to prevent injury. Provide a safe area, do not attempt to hold them down or restrain them. Call 911 or your local emergency number. Continue monitoring patient until help arrives or the person responds. Follow the site guidelines if they have Emergency Protocol in place.
After the individual regains consciousness:
Keep person lying down, as symptoms subside. When all symptoms are gone, typically 5 – 15 minutes, allow person to first set up slowly before attempting to stand.
Do not offer any liquids while severe symptoms are present to prevent choking or vomiting.
If needed, apply first aid to injuries
Fill out Incident Report
Inform Client site coordinator of incident immediately
Incident Report Protocol
The Incident Report will be used to report all out of process incidents at all screening and vaccine events. The report should be filled out at end of day or as soon as reasonably possible and turned in to the manager or director to whom the person completing the report has reporting responsibility. The Summit Health Staffing Department should be notified ASAP, see contact information on your Service Order Confirmation and fax copy of the Summit Health Incident Report sent to (248) 416-1208. Summit Health will complete the VAERS form if required using the SH Incident Report you will fax
in after the clinic. VAERS is an acronym for Vaccine Adverse Event Reporting System. The form should be completed for Severe Adverse Reactions. Do not complete the form for mild or localized reactions.
1. If a clinic Participant has an adverse reaction, the nurse will report as soon as possible to the SH Staffing department and complete the SH Incident Report, which includes: Participant’s name Specific adverse reaction the Participant experienced Nurse’s actions Participant’s current medical status and whereabouts
2. Do not offer reimbursement for medical expenses or doctors’ visits resulting from an adverse reaction to an immunization. Requests for reimbursement will be directed to SH and the Risk Management department.
3. FAX the completed SH Incident Report immediately to SH, Risk Management department, must be received within 24 hours. The Risk Department will complete the recommended VAERS report. Please fax to SH at (248) 799-1208.
In the event that an anaphylactic reaction or any other incident occurs at the time of clinic or thru clinic follow-up, it is necessary to report such occurrences to SH via the SH Incident Report form. Please complete the form and send to SH via fax at (248) 799-1208.

Rev. 9/8/2010 33
Appendix - Forms
Two-Part Consent Form

Rev. 9/8/2010 34
SCANTRON BUBBLE CONSENT - FRONT SIDE 1
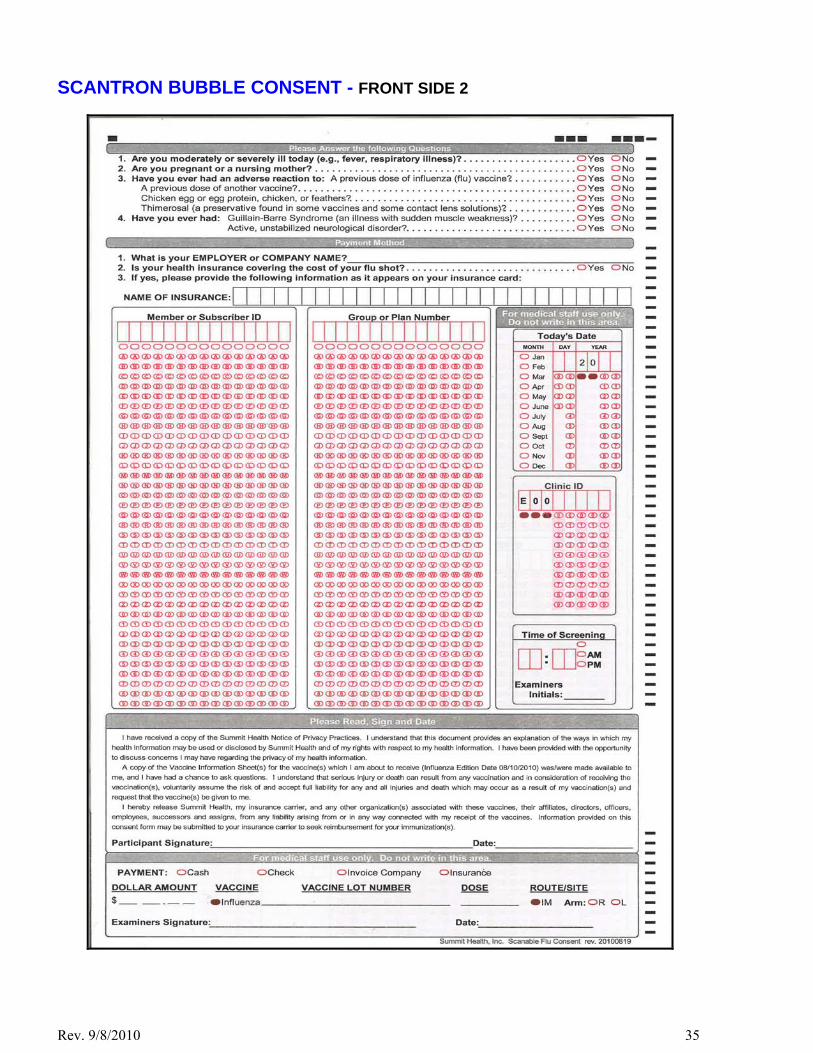
Rev. 9/8/2010 35
SCANTRON BUBBLE CONSENT - FRONT SIDE 2

Rev. 9/8/2010 36
SCANTRON BUBBLE CONSENT - BACK SIDE 1

Rev. 9/8/2010 37
SCANTRON BUBBLE CONSENT - BACK SIDE 2

Rev. 9/8/2010 38
CLINIC RECORD FORM

Rev. 9/8/2010 39
HIPAA NOTICE OF PRIVACY PRACTICES
FRONT- SIDE BACK - SIDE

Rev. 9/8/2010 40
CONFIDENTIAL ENVELOPE
FOR COMPLETED PARTICIPANT CONSENT FORMS
NOTE: SEAL THIS ENVELOPE IMMEDIATELY AFTER ENCLOSING THE COMPLETED PARTICIPANT CONSENTS FORMS AND THE WHITE COPY OF THE COMPLETED CLINIC RECORD FORM

Rev. 9/8/2010 41
Industry Best Practices On-Site Caregivers
Many individuals, who receive medical related services in an office setting, rather than in a hospital or doctor’s office, often are anxious about receiving such services. To alleviate such anxiety and put participants at ease, caregivers should adhere to generally recognized “industry best practices.” Such practices are outlined below.
Arrival and Setup: A well run, on-site medical services program is critical to alleviating participant anxiety. To ensure such a program, caregivers should:
Confirm site contact information, directions, building and room location, and parking options, to ensure timely arrival at site location.
Arrive on-site at least 60 minutes before services are scheduled to begin and be ready to perform services 15 minutes before the scheduled start time.
Determine in advance the necessity for an earlier arrival time, taking into consideration site variables, including among others, (1) complexity of set up, (2) security procedures, and (3 available parking.
Notify the site contact representative if not able to arrive 60 minutes prior to event start time. Notice should be provided prior to the 60-minute advance arrival time.
Wear a name badge at all times while on premises. Demeanor, Conduct and Appearance: A caregiver’s professional dress, good hygiene, and overall appearance increases participant confidence and promotes the spirit and intent of the client’s health and wellness program. To project the proper image, caregivers should:
Engage the participant in light conversation to ease any anxiety, refrain from discussing caregiver’s medical conditions or health, and limit questions about a participant’s health to only those that directly pertain to the services being provided.
Refrain from smoking during a clinic, and due to the lingering odor of cigarette smoke, refrain from smoking prior to arrival.
Keep all food and drinks (other than bottled water) out of presence of participants. Avoid chewing gum in the presence of participants. Use cosmetics and perfume in moderation and not apply in the presence of participants. Avoid using cell phones, PDA’s and other similar devices during clinics, place such devises on silent mode during clinic
and use said devices for personal use only during break times. Dress professionally, consistent with a medical office setting (e.g. white lab coat or examiner coat over business casual
shirt or blouse with black or dark slacks and dark shoes). Running shoes, sneakers, and shoes with open toes or heels convey an unprofessional office image and should not be worn.
Portray a conservative look by limiting earrings in size to no larger than a US quarter and located in the earlobe, and removing other body piercings and covering tattoos while on-site.
Practice good hygiene, including making sure that hands and fingernails are clean, fingernails are trimmed (no longer than ¼ inch beyond the fingertip), and avoiding discernable body odor and strong perfumes and colognes.
Safety: Maintaining participant and caregiver safety is of paramount importance. To help avoid accidents and injuries, caregivers should:
Wear appropriate footwear (rubber soled lace or loafer style shoes, covering the entire foot). Secure hair back and off the shoulders to prevent contact with contaminated materials or surfaces or moving machinery
such as a centrifuge. Men with beards should observe the similar precautions. I hereby acknowledge receipt of Industry Best Practices – On-Site Caregivers Name: ________________________ Date: ___________
Signature: _______________________________________
AA01\223358.3 ID\MJMU

Rev. 9/8/2010 42
2010-2011Medical Directives - Influenza
The Summit Health on-site influenza vaccination program was developed in 1999 for companies wishing to immunize their employees against the influenza virus. Public clinics have been conducted since 1999. The 2010-2011influenza vaccine was developed on the current recommendation of the Center for Disease Control. The following guidelines are to be followed when administering influenza vaccine:
1. Everyone must sign a current consent form with the lot number and manufacturer name recorded on the consent form.
2. Injections of 0.5 ml of influenza vaccine are recommended to be given intramuscularly in the deltoid of the arm the person uses least; utilizing a 22–25g, 1–1½" needle, or as supplied in pre-filled syringes from the manufacturer.
3. Before injecting, the skin over the site to be injected should be cleansed with a suitable germicide. After needle insertion, aspirate to help avoid inadvertent injection into a blood vessel.
4. If a person is on blood anticoagulant treatment, such as Coumadin or Heparin, apply pressure to the injections site for 3 - 5 minutes following injection.
5. Contraindications for the vaccine are for individuals who: a. have a history of hypersensitivity (allergy) to egg proteins (eggs or egg products) chicken, chicken
feathers or dander, or Thimerosal b. an anaphylactic reaction to a previous dose of any vaccine. c. have ever had Guillain-Barre Syndrome or have an active neurological disorder d. currently breast-feeding or pregnant (to receive from their personal physician), vaccine contains
Thimerosal e. currently have a moderate or severe acute illness f. are under the age of 9 g. are presently receiving immunosuppressive therapy as this may reduce the immune response (to
receive from their personal physician) 6. The patient should wait at least 15 minutes after the injection for observation of possible adverse reaction.
This Medical Directive is Ordered and Approved by:
____________________________________________________________________ Print Physician’s Name DEA # / State License #
____________________________________________________________________ Physician’s Signature Date
Sample – State Specific are on File at SH Corporate office.

Rev. 9/8/2010 43
2010-2011Medical Directives - Pneumonia
The Summit Health on-site pneumonia vaccination program has been developed as a value added service to the influenza vaccination program designed to provide low cost and/or no cost vaccination services to the general public. The 2010-2011 Pneumococcal vaccine immunizes against 23 of the most prevalent strains of pneumonia.
The following guidelines are to be followed when administering pneumococcal vaccine:
1. Everyone must sign a current consent form with the lot number and manufacturer name recorded on the consent form.
2. Injections of 0.5 ml of vaccine are recommended to be given either intramuscularly (22–25g, 1–1½” needle) in the deltoid muscle or subcutaneously (23–25g, 5/8" needle) in the posterolateral fat of the upper arm.
3. Before injecting, the skin over the site to be injected should be cleansed with a suitable germicide. After needle insertion, aspirate to help avoid inadvertent injection into a blood vessel.
4. If a person is on blood anticoagulant treatment, such as Coumadin or Heparin, apply pressure to the injections site for 3 - 5 minutes following injection.
5. Contraindications for the vaccine are for individuals who: a. have a history of hypersensitivity to any component of the vaccine including phenol which is used as
a preservative b. an anaphylactic reaction to a previous dose of any vaccine. c. currently breast-feeding or pregnant (to receive from their personal physician) d. currently have a febrile respiratory illness or have an active infection e. are under the age of 18 f. have received a prior Pneumococcal vaccination and are currently under the age of 65 g. have had episodes of Pneumococcal pneumonia or other Pneumococcal infection
6. The patient should wait at least 15 minutes after the injection for observation of possible adverse reaction. This Medical Directive is Ordered and Approved by:
____________________________________________________________________ Print Physician’s Name DEA # / State License #
____________________________________________________________________ Physician’s Signature Date
Sample – State Specific are on File at SH Corporate office.

Rev. 9/8/2010 44
Anaphylactic Shock Policy & Procedure
POLICY
To prevent anaphylaxis, all patients should be questioned regarding drug sensitivity prior to receiving any medication. Anaphylactic shock should be anticipated with those persons having a history of allergy (deny vaccination if you have concern about anaphylaxis). The responsible medical staff (DO, MD, PA, NP, RN or LPN / LVN dependent on state guidelines) based on the following procedure shall administer immediate treatment. The patient shall then be immediately referred to a physician.
PROCEDURE
1. Definition - a generalized life-threatening allergic reaction. 2. Etiology - drugs, insect bites or other sensitizing agents. 3. Findings - 1) Subjective - itching, sensation of warmth, apprehension, shortness of breath. 2) Objective - edema, pupil dilation, cyanosis, wheezing, weak or rapid pulse, respiratory distress,
decreased blood pressure (shock), and respiratory and/or cardiac arrest. 4. Treatment Plan - Administer treatment first – have another person call 911 or, if no one is available,
call 911 after treatment is given. All anaphylactic reactions are sent to the ER, regardless of severity!!
(a) Epinephrine for- (i) Mild anaphylaxis (urticaria, rhinitis, conjunctivitis, mild bronchospasm)
0.3 - 0.5 ml 1:1000 subcutaneous (ii) Moderate anaphylaxis (generalized urticaria, angioedema, hypotension, early laryngeal edema,
BP < 80 mm HG) 0.3 - 0.5 1:1000 subcutaneous (b) Keep patient in supine position unless he or she is having breathing difficulty. If breathing is difficult,
patient’s head may be elevated, provided blood pressure is adequate to prevent loss of consciousness. If blood pressure is low, elevate legs.
(c) Perform cardiopulmonary resuscitation (CPR), if necessary, and maintain airway. (d) Monitor blood pressure and pulse every 5 minutes. (e) To be seen by physician immediately
5. Follow-up - counseling as necessary to prevent recurrence and send a report to VAERS (Vaccine Adverse
Event Reporting System). Policy and Procedure Approved by:
____________________________________________________________________ Print Physician’s Name DEA # / State License #
____________________________________________________________________ Physician’s Signature Date
Sample – State Specific are on File at SH Corporate office.