2011 outcomes - cleveland clinic · welcome to cleveland clinic’s 2011 outcomes books. they...
TRANSCRIPT

Respiratory Institute
2011Outcomes


To promote quality improvement, Cleveland Clinic has created a series of
Outcomes books similar to this one for many of its institutes. Designed for a
physician audience, the Outcomes books contain a summary of our surgical and
medical trends and approaches, data on patient volumes and outcomes, and a
review of new technologies and innovations.
Although we are unable to report all outcomes for all treatments provided at
Cleveland Clinic — omission of outcomes for a particular treatment does not
necessarily mean we do not offer that treatment — our goal is to increase
outcomes reporting each year. When outcomes for a specific treatment are
unavailable, we often report process measures associated with improved
outcomes. When process measures are unavailable, we may report volume
measures; a volume/outcome relationship has been demonstrated for many
treatments, particularly those involving surgical techniques.
In addition to our internal efforts to measure clinical quality, Cleveland Clinic
supports transparent public reporting of healthcare quality data and participates
in the following public reporting initiatives:
• JointCommissionPerformanceMeasurementInitiative(qualitycheck.org)
• CentersforMedicare&MedicaidServices(CMS)HospitalCompare
(hospitalcompare.hhs.gov)
• OhioDepartmentofHealth(ohiohospitalcompare.ohio.gov)
• ClevelandClinicQualityPerformanceReport(clevelandclinic.org/QPR)
Our commitment to providing accurate, timely information about patient care also
will help patients and referring physicians make informed healthcare decisions.
Wehopeyoufindthesedatavaluable,andweinviteyourfeedback.Pleasesend
comments and suggestions to us at [email protected]. To view
allourOutcomesbooks,pleasevisitClevelandClinic’sQualityandPatientSafety
website at clevelandclinic.org/outcomes.

Dear Colleague:
Welcome to Cleveland Clinic’s 2011 Outcomes books. They include data on clinical outcomes, patient volumes, innovations and publications. Cleveland Clinic pioneered the collection and annual publication of outcomes data. This initiative has become part of the national discussion on lowering costs and improving the quality of healthcare.
Cleveland Clinic uses data to manage outcomes across the full continuum of care. Clinical services are delivered through patient-centered institutes, each based around a single disease or organ system. Institutes combine medical and surgical services, along with research and education, under unified leadership. Each institute defines quality benchmarks for its specialty services and reports longitudinal progress.
Cleveland Clinic Outcomes books are available in print and online. Additional data is available throughouronlineQualityPerformanceReport(clevelandclinic.org/QPR).Thesiteoffersdatainadvance of national and state public reporting sites in key areas, including heart attack, heart failure, stroke and infection prevention.
We hope you will find this information useful.
Sincerely, DelosM.Cosgrove,MD CEOandPresident

Prefer an e-version?
Visit clevelandclinic.org/OutcomesOnline, and
we’ll remove you from the hard copy mailing list
and email you when next year’s books are online.
what’s insideChairman’s Letter 04
Institute Overview 05
Quality and Outcomes Measures
CriticalCareMedicine 08
TheRespiratorySpecialCareUnit(ReSCU) 11
Bronchology 12
Asthma 14
LungandHeart/LungTransplantation 16
Pneumonia 18
PatientExperience 20
Innovations 24
SelectedPublications 40
StaffListing 48
Contact Information 50
Institute Locations 52
ImprovingQuality,SafetyandthePatientExperience 54
About Cleveland Clinic 59
Resources 61
Outcomes 20114
Chairman LetterChairman’s Letter
4 Outcomes 2011
TheRespiratoryInstituteispleasedtopresenttheeighthedition of our Outcomes book. This booklet provides a condensed overview of our clinical activities and programs, including reports of clinical volumes and patient outcomes. We believe it is important and useful to share this information with our referring physicians, training program alumni, potential patients and other individuals interested in respiratory diseases.
At Cleveland Clinic, patients with respiratory diseases benefit from the expertise of a multidisciplinary team consisting of clinicians who specialize in pulmonary and critical care medicine, allergy and clinical immunology, and thoracic surgery, all working in close collaboration with thoracic radiologists and pulmonary pathologists.
In 2011, we experienced continued growth in our clinical programs, research funding and application of innovative technologies. We are proud of these accomplishments and thankful for all those who helped us achieve this level of success. We are firmly committed to providing ever-increasing levels of clinical excellence in the future.
HerbertP.Wiedemann,MD,MBAChairman,RespiratoryInstitute

5
Institute Overview
RespiratoryInstitute
AtClevelandClinic’sRespiratoryInstitute,patientswithpulmonarydisordersbenefitfromtheexpertiseofamultidisciplinaryteamofspecialists.Specifically,expertsinfourdepartments—Pulmonary,AllergyandCriticalCareMedicine;ThoracicandCardiovascularSurgery;ThoracicImaging;andPulmonaryPathology—collaboratetocare for these patients.
We provide comprehensive care for all patients with respiratory disorders. Our national experts treat patients with the following conditions:
• Acuterespiratorydistresssyndrome(ARDS)
• Allergies(allergicrhinitis,food,drug,latex,etc.)
• Asthma
• Beryllium-inducedlungdisease
• Chronicobstructivepulmonarydisease(COPD), including alpha-1 antitrypsin deficiency
• Idiopathicpulmonaryfibrosis
• Interstitiallungdisease
• Lungcancer
• Lymphangioleiomyomatosis(LAM)
• Pulmonaryalveolarproteinosis(PAP)
• Pulmonaryvasculardiseases(idiopathicpulmonary hypertension,pulmonaryembolicdisease,etc.)
• Sarcoidosis
2011 % Increase 2008 – 2011
TotalVisits 107,670 38%
InterstitialLungDiseaseVisits 1,951 -10%
PulmonaryArterialHypertensionVisits 1,898 30%
SarcoidosisVisits 1,942 45%
LungCancerVisits 1,215 55%
COPDVisits 6,741 56%
TotalHospitalAdmissions 1,868 65%
ResearchFunding $7.8million 70%
ResearchGrants/Contracts 105 40%

Outcomes 20116
Institute Overview
In collaboration with our thoracic surgery colleagues, we evaluate patients for:
• Invasivediagnosticprocedures(lungbiopsy,mediastinoscopy,etc.) • Pulmonaryresections(lungcancer,etc.) • Lung-volumereductionsurgery(LVRS)foremphysema • Pulmonarythromboendarterectomy(forchronicpulmonaryhypertensionsecondarytothromboemboli) • Lungtransplantation
TheRespiratoryInstitute’ssixformalsectionsprovideadvancedsub-specializedcareinthefieldsofallergyandclinicalimmunology, bronchology, critical care medicine, lung transplantation, respiratory therapy and sleep medicine. Diagnosing and managingthefullspectrumofrespiratoryandallergicdisorders,theRespiratoryInstituteprovidesmorethan107,000patientvisits annually.
Alsowithinourinstitutearethefollowingcenters:CenterforMajorAirwayDiseases(inconjunctionwiththoracicsurgery),Asthma Center and Alpha-1 Antitrypsin Deficiency Center of Excellence.
Ourinstitutebringscareintothecommunity,providingoutpatientservicesattheBeachwoodFamilyHealthandSurgeryCenter(Pulmonary),BrunswickFamilyHealthCenter(Pulmonary),ChagrinFallsFamilyHealthCenter(Pulmonary&Allergy),IndependenceFamilyHealthCenter(Pulmonary&Allergy),MedinaMedicalOfficeBuilding(Allergy),MentorOffice(Pulmonary),RichardE.JacobsHealthCenterinAvon(Pulmonary&Allergy),StrongsvilleFamilyHealthandSurgeryCenter(Pulmonary&Allergy),TwinsburgFamilyHealthandSurgeryCenter(Pulmonary&Allergy),WilloughbyHillsFamilyHealthCenter(Pulmonary&Allergy)andWoosterFamilyHealthCenter(Pulmonary&Allergy).RespiratoryInstitutestaffalsoprovidecomprehensive(ICU,inpatient,outpatient)pulmonarycareatHillcrest,EuclidandSouthPointehospitals.
This past year, our institute has seen continued growth in our clinical programs and research activities, which are primarily conductedatClevelandClinic’smaincampusfacilities(clinics,hospitalandresearchlaboratories).Thecollaborationbetweenourclinicians and researchers helps to shorten the gap between the laboratory discoveries of today and the patient care of tomorrow.
Outpatient Visits to Cleveland Clinic Respiratory Institute
2007 – 2011
120
100
80
0
60
40
20
Outpatient Visits (in thousands)
2011107,670
200771,553
200878,062
200988,970
201095,755N =
AllergyPulmonary and Critical Care

RespiratoryInstitute 7
*Includes14heart/lung&4liver/lung
Bronchoscopies
Lung Transplants*
2007 – 2011
2007 – 2011
200
150
0
100
50
Procedures
N =2011108
200772
200857
2009157
2010122
3,500
2,500
0
2,000
3,000
1,000
1,500
500
Procedures
20102,771N =
20113,109
20072,391
20082,365
20092,572

Outcomes 20118
TheRespiratoryInstitutemanagesandstaffstheMedicalIntensiveCareUnit(MICU)atClevelandClinic.Theunithasseenasteadyincreaseinpatientvolumeoverthepastsixyears,withtheunitnowconsistingof53dedicatedbeds.Directinter-hospitaltransfersaccountfor37%oftotalMICUadmissions.
The unit is staffed by board-certified intensivists, who have been providing in-house coverage 24 hours per day since July2008.
Patientoutcomescontinuetobeexcellent,asexhibitedbymortalityratesbelowtherisk-adjustedpredictedvalues,improvinginfectionratesandlowreadmissionrateswithin48hoursofdischarge.
Score
N = 708 692 727 709
75
65Q1 Q2 Q3 Q4
70
*TheAcutePhysiologyandChronicHealthEvaluationsystem (APACHEIV)isusedtorisk-adjustour population of critical care patients.
Mean APACHE IV* Score
2011
ClevelandClinicAPACHEIVmeanscoreof71iswellabovethebenchmarkof54fromalargeadult populationthatreflectsthecurrentpracticeofcriticalcareintheUnitedStates.
References
LillyC,ZuckermanI,BadawiO,RikerR.BenchmarkDataFromMoreThan240,000AdultsThatReflecttheCurrentPracticeofCriticalCareintheUnitedStatesCHEST.2011Nov;140(5):1232-1242.
8
Critical Care Medicine
RespiratoryInstitute 99RespiratoryInstitute
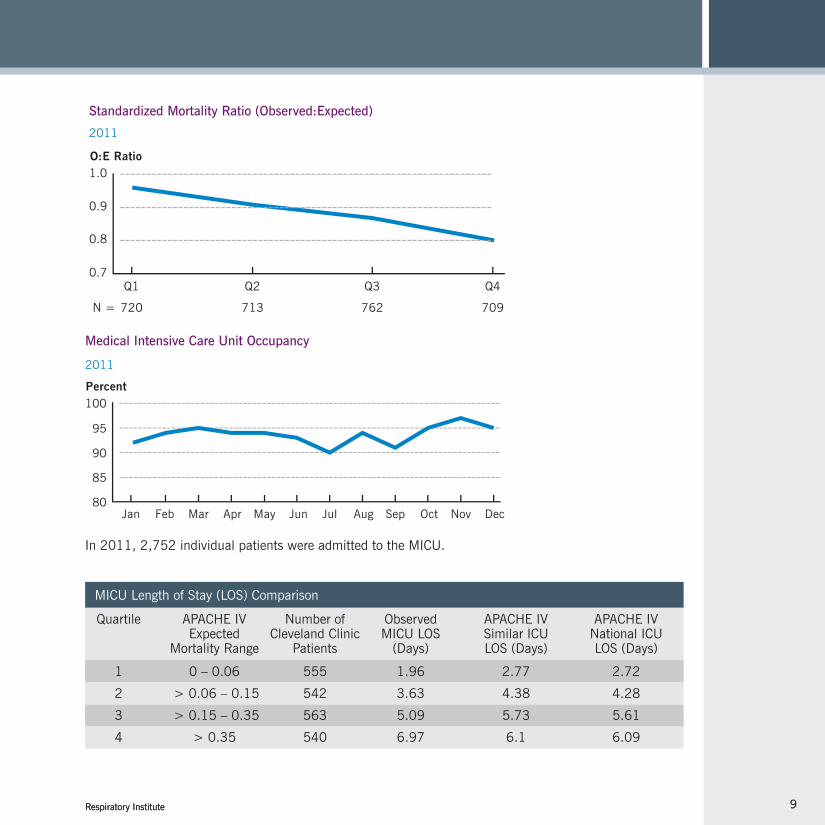
In2011,2,752individualpatientswereadmittedtotheMICU.
Medical Intensive Care Unit Occupancy
2011
Percent100
80Jan Mar May Jul Sep NovFeb Apr Jun Aug Oct Dec
85
90
95
MICULengthofStay(LOS)Comparison
Quartile APACHEIV Numberof Observed APACHEIV APACHEIV Expected ClevelandClinic MICULOS SimilarICU NationalICU MortalityRange Patients (Days) LOS(Days) LOS(Days)
1 0–0.06 555 1.96 2.77 2.72
2 >0.06–0.15 542 3.63 4.38 4.28
3 >0.15–0.35 563 5.09 5.73 5.61
4 >0.35 540 6.97 6.1 6.09
Standardized Mortality Ratio (Observed:Expected)
2011
O:E Ratio1.0
0.7Q1 Q2 Q3 Q4
0.8
0.9
N = 720 713 762 709

Outcomes 201110
Cleveland Clinic MICU Central Line-Associated Bloodstream Infections (CLABSI)
2008–2011
Cleveland Clinic MICU Nosocomial Ventilator-Associated Pneumonia (VAP)
2008–2011
MICU Infection Rates
Cleveland Clinic MICU Nosocomial C. difficile
2008–2011
Rate (per 1,000 Line Days)10
8
6
4
0Q1 Q2 Q3 Q4
2
2008 2009 2010 2011Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
4.0
0
1.0
2.0
Rate (per 1,000 Vent Days)
3.0
2008 2009 2010 2011Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2.0
0
0.5
1.0
Rate (per 1,000 Patient Days)
1.5
2008 2009 2010 2011Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Critical Care Medicine

RespiratoryInstitute
TheRespiratorySpecialCareUnit(ReSCU)wascreatedforpatientswhodependonmechanical ventilation to breathe but who are otherwise healthy enough to leave the intensive care unit. TheprimarygoalsoftheReSCUareto:
• Helppatientsbreathewithoutaventilator
• Teachpatientsself-care
• Teachfamilymembershowtocareforthepatientandmanagetheventilatorathome
• Preparepatientandfamilyforpatient’sdischargetoanotherfacility
When appropriate, patients on partial or complete ventilator support are discharged to long-term acute care facilities before complete weaning is acheived.
ReSCUStatistics2011 Numberofdischarges 81
TotalReSCUdays 2,427
Numberofpatientscompletelyweanedfromventilation 43
Number of deaths 1 Averagelengthofstay(days) 30.09
Status at ReSCU Discharge 2008–2011
BasedondatafromJanuary1toDecember31,2011.
80
100
40
60
02008 2009 2010
54N= 55 57201181
20
Patients
Complete VentilatorSupport
Completely Weaned
Partial VentilatorSupport
Expired in ReSCU
The Respiratory Special Care Unit (ReSCU)
11

Outcomes 2011
ClevelandClinic’sRespiratoryInstituteprovidesthefullrangeofadvanceddiagnosticand interventional bronchoscopy techniques. We have some of the world’s most extensive experience with:
•Electromagneticnavigation •Lungtransplant-relatedairwaydisease •Airwaystenting •Managementofairwaycomplicationsduetohistoplasmosis •Benignairwaydiseases •Metallicstentremoval
Weperformed2,935bronchoscopiesduring2011,a54percentincreaseinsixyears. Importantly, our complication rates remain low.
Post-bronchoscopycomplicationrateisfarlowerthanexpectedpublishedaverages.
Post-Bronchoscopy Complication Rate (N = 2,935)
2011
Transbronchial lung biopsy 1,279Transbronchialneedleaspiration 687Endobronchialultrasound 629Electrocautery/laser ablation 240Electromagnetic navigation 104Balloontrachealbronchoplasty 261Bronchial/tracheal stenting 110Bronchial thermoplasty 9Pleuralcatheterplacement 18
SelectedProcedureVolumes2011
12
0.5
0.6
0.3
0.4
0Pneumothorax Reversal of Sedation
RequiredICU
Admission
17N = 6 15
Clinically SignificantBleeding
6
0.2
0.1
Percent
Bronchology

13RespiratoryInstitute
TheRespiratoryInstituteisamemberoftheACCPQualityImprovementRegistry,Evaluation,andEducation(AQuIRE)BronchoscopyModuleforInterventional/TherapeuticRegistry.Thisisaweb-based,IRB-approveddatacollectiontool,which Cleveland Clinic has been using to collect data from all therapeutic bronchoscopy cases. The goals are to understand resource utilization, look for evidence of performance/complications, seek opportunities for research and publication, and foster quality improvement. It is possible that, in the future, the registry may be used for assessing professional competencies and assessing fellows/trainees. Because the registry is still a work in progress, additional centers and individuals are being added to it.
AQuIREBronchoscopyRegistryIndicatorAnalysis
January–October2011
Successrateofinterventional procedures in patients with malignant disease Complication rate of interventional procedures with malignant disease
Successrateof interventional procedures in patients with nonmalignant disease
Complication rate of interventional procedures in patients with nonmalignant disease
30-daymortalityofinterventional patients with malignant disease
30-daymortalityofinterventional patients with nonmalignant disease
96.4% N=80
1.4% N=80
94.3% N=283
0.8% N=283
9.8% N=80
2.5% N=283
RespiratoryInstitute OverallRegistry
For more information, see chestnet.org/accp/quality-improvement/aquire.
96.6% N=321
3.7% N=321
97.3% N=587
3.4% N=587
12.1% N=321
3.4% N=587

Outcomes 201114
Asthmacontrolcanbeassessedbyusingvalidatedinstruments,includingtheAsthmaControlTest(ACT).TheACTincludesfivequestionsthatassessdaytimesymptoms,nighttimesymptoms,relianceonPRN“rescue” medication, the impact of asthma on everyday functioning and patient self-assessment of control, with each of these five responses scored on a 1 to 5 scale.
Amajorobjectiveofasthmamanagementistoachievewell-controlled(ACT=20-25)asthma.Ifasthmaisnotwellcontrolled(ACT=16-19)orispoorlycontrolled(ACT≤15),evidenceindicatessuchpatientsare at elevated risk for exacerbation of asthma over time.
ClevelandClinichasusedtheACTinAllergy/Immunologyformorethan6yearsonaroutinebasistoinfluence treatment decisions. All asthma patients complete the ACT when seen at initial and follow-up visits.ShownbelowareACTscorescategorizedbylevelofcontrolforpatientsseenin2011.
Asthma Control Test (ACT) Score Categories (N = 431)
2011
ACT Scores at Visits in 2011
Poorly Controlled(< 15)
Not Well Controlled(16-19)
Well Controlled(20-25)
0
40
20
60
80
100
Percent
Follow-upInitial
Patient Visits
33%
25%
42%
20%
19%
61%
Asthma Center

RespiratoryInstitute
As ACT scores < 20 have been associated with higher rates of health service utilization, and well controlled asthma(ACT≥20)isassociatedwithimprovedqualityoflife,ourdataprovideindirectevidencedemonstratingthat care in Allergy/Immunology at the Cleveland Clinic leads to reduced overall costs of asthma care and provides value.
References
LangDM.Newguidelinesemphasizecontrol,regularmonitoring.Cleve Clin J Med.2008;75:641-653. WilliamsSA,etal.Theassociationbetweenasthmacontrolandhealthcareutilization,workproductivityloss and health-related quality of life. J Occ Env Med.2009;51:780-785.
15

Outcomes 2011
In2011,theLungTransplantProgramperformed108lungtransplants(46single,62double)andcompletedits1,070thtransplantsincetheprogram’sinceptionin1990.Morethan 588nationalandinternationalend-stagelungdiseasepatientswere referred to the transplant team for evaluation. The transplant program continues a reputation for accepting and transplanting challenging, complex patients.
Cleveland Clinic’s Lung Transplant Team is involved in a series of multicenter trials aimed at therapy for primary graft dysfunction, acuterejectionandinductiontherapy.Inaddition,oursurgeonshavepioneered certain transplant surgical techniques, including bronchial artery revascularization, that may improve outcomes further by reducingischemicinjury.
The average waiting time for a graft in our program remains stable. The average waiting list time for patients transplanted in 2011 was161days,andthemedianwaitinglisttimewas65days. A continuing emphasis on quality assurance and quality improvement remains central to the program, reflected in the median post-transplant length of stay of 17 days for patients transplanted in 2011.
Another unique feature of Cleveland Clinic’s transplant program is that patients can live within 1,000 miles of the Cleveland area while awaiting an organ, which means they do not have to relocate to Cleveland. We follow our patients for the life of their transplant for continuity of care, and we collaborate with their local physicians. Our transplant physicians are committed to helping transplanted patients receive as much care as possible close to their homes. The goal is to return each transplant patient to his or her primary care physician or referring physician within three to six months after transplant.
Lung and Heart/Lung Transplantation
16

Respiratory Institute Respiratory Institute 17
Primary Lung Transplant
2006 – 2011
The Lung Transplant Program has achieved strong survival rates at or above the national average, with a one-month survival rate of 94.6 percent, one-year survival of 80.3 percent and three-year survival of 72.9 percent.
100
80
0
60
40
20
Survival (%)
0 1 2 3 4 5
N = 485 412 273 158 95
Years Since Transplantation
CC = Cleveland Clinic
SRTR/OPTN = Scientific Registry of Transplant Recipients/Organ Procurement and Transplantation Network
*1-Month and 1-Year Benchmarks = Patients transplanted (single organ) between July 1, 2008, and Dec. 31, 2010.
**3-Year Benchmark = Patients transplanted (single organ) between Jan. 1, 2006, and June 30, 2008.
To obtain comparisons of actual vs. expected outcomes, please visit srtr.org. Survival rates in this book are calculated by a third party, the Scientific Registry of Transplant Recipients (SRTR), and available in the January 2012 release. Survival rates are based on single-organ transplants only.
Adult patient survival
1 Month* 1 Year* 3 Years**
Cleveland Clinic 94.6% 80.3% 72.9%
National registry 96.2% 83.0% 65.8%

Outcomes 201118
Pneumonia Appropriateness of Care
2010 – 2011
This composite metric, based on eight pneumonia hospital quality process measuresdevelopedbytheCentersforMedicareandMedicaidServices(CMS),shows the percentage of patients who received all the recommended care for whichtheywereeligible.ClevelandClinichassetatargetofUHC’s 90th percentile.
Pneumonia — National Hospital Quality Measures
0
60
40
20
* Data source: University HealthSystem Consortium (UHC) Clinical Databasehttps://www.uhc.edu
80
100
Percent
93.7 92.8 95.8 Cleveland Clinic, 2010 (N = 478)Cleveland Clinic, 2011 (N = 516)UHC Top Decile, 2011*
Pneumonia

Respiratory Institute 19
Pneumonia All-Cause 30-Day Mortality (N = 276)
July 2008 – June 2011
Pneumonia Outcome Measures
Pneumonia All-Cause 30-Day Readmissions (N = 305)
July 2008 – June 2011
CMS calculates two pneumonia outcome measures: all-cause mortality and all-cause readmission rates, each based on Medicare claims and enrollment information. Cleveland Clinic’s performance appears below.
Cleveland Clinic’s pneumonia risk-adjusted 30-day mortality rate is the same as the national average. Our pneumonia risk-adjusted readmission rate is higher than the national average; the difference is statistically significant. To further reduce this rate, a multidisciplinary team was tasked with improving transitions from hospital to home or post-acute care facility. Specific initiatives have been implemented in each of these focus areas: communication, education and follow-up.
Pneumonia — National Hospital Quality Measures (continued)
0
15
10
5
20
25
Percent
National Average*
12.012.1
Cleveland Clinic0
5
10
15
20
25
Percent
National Average*
18.5
22.1
Cleveland Clinic
* Source: hospitalcompare.hhs.gov

Outcomes 2011
Cleveland Clinic is dedicated to delivering excellent clinical outcomes and the best possibleexperienceforourpatientsandtheirfamilies.Patientfeedbackiscriticalindriving priorities and assessing results. Based on this feedback, Cleveland Clinic’s OfficeofPatientExperienceimplementstrainingprogramstoimproveserviceandcommunication as well as educational initiatives to help patients understand what to expect when they are in our care.
Outpatient — Respiratory Institute
100
80
0
60
40
20
Percent
Very Good Good Fair Poor Very Poor
Source: Press Ganey, a national hospital survey vendor
2010 (N = 653)2011 (N = 900)
Overall Rating of Outpatient Care and Services During Outpatient Visit 2010 – 2011
20
Patient Experience

Respiratory Institute
Likelihood of Recommending Outpatient Care Provider 2010 – 2011
100
80
0
60
40
20
Percent
Very Good Good Fair Poor Very Poor
Source: Press Ganey, a national hospital survey vendor
2010 (N = 653)2011 (N = 900)
100
80
0
60
40
20
Percent
Very Good Good Fair Poor Very Poor
Source: Press Ganey, a national hospital survey vendor
2010 (N = 653)2011 (N = 900)
Rating of Outpatient Care Provider 2010 – 2011
21

100
80
0
60
40
20
Percent
Rate Hospital Would Recommend
% 9 or 10(0 – 10 scale)
% “definitely yes”
Source: Press Ganey, a national hospital survey vendor
2011 (N = 264)2010 (N = 285)
81%88%
78%74%
HCAHPS Overall Assessment 2010 – 2011
Inpatient — Respiratory Institute
The Centers for Medicare and Medicaid Services (CMS) requires United States hospitals that treat Medicare patients to participate in the national Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey, a standardized tool that measures patients’ perspectives of hospital care. Results collected for public reporting are available at hospitalcompare.hhs.gov.
Outcomes 201122
Patient Experience

HCAHPS Domains of Care 2010 – 2011
100
80
0
60
40
20
Percent
DischargeInformation Given
% yes
Doctor Communication
Nurse Communication
PainManagement
RoomClean
New MedicationsCommunication
Responsivenessto Needs
Quiet atNight
Source: Press Ganey, a national hospital survey vendor
2011 (N = 264)2010 (N = 285)
% always(Options: always, usually, sometimes, never)
Respiratory Institute 23

Outcomes 2011
Innovations
Breath Analysis in Lung Cancer
There is a tremendous need for biomarker development to assist in the evaluation and management of patients with lung
cancer. Biomarkers capable of identifying those at greatest risk for developing lung cancer will help to optimize lung cancer
screening programs and promote chemoprevention research. Biomarkers capable of identifying lung cancer at the earliest
possible stage will lead to advances in lung nodule management and surgical and ablative therapies. Biomarkers able to
predict the nature of the cancer and response to specific therapies will lead to improvements in systemic, targeted and
individualized therapies. Exhaled breath is a unique source of biomarker development.
Exhaledbreathcontainsvolatileorganiccompounds(VOCs)intraceconcentrations.SomebreathVOCsaregeneratedby
the metabolic processes within the body’s tissues. These travel to the lung and are exhausted in our breath. Conditions
thatalterthebody’smetabolicprocesses,suchaslungcancer,mayleadtoauniquesetofbreathVOCs.Supportforthis
premise comes from studies of metabolic changes in lung cancer tissue and the blood of lung cancer patients, as well as
in measurements of VOC off-gassing of lung cancer cell lines.
SeveralstudieshaveassessedthepatternofVOCsinthebreathoflungcancerpatients.Thesestudieshaveeitherused
spectrometry systems or chemical sensor matrices. The studies have been relatively small and early in the evolution of
biomarker development. They have shown promise, with accuracies for the identification of lung cancer reported in the
80to85percentrange.
Wearecurrentlyleadingamulti-institutionprojectwiththegoalofdeterminingtheaccuracyofanadvancedversionof
acolorimetricsensorarraysystem.Ourpreviousresearchshowedthesensorhadanaccuracyof80to85percentinthe
identification of patients with lung cancer. Advances in the sensor and breath collection technology have improved the
sensitivity to low concentrations of VOCs by more than 100 times. It is our hope that these technical advances will
translate into higher accuracy rates for the system.
Inaddition,weareperformingprojectswiththeaimofidentifyingthediscriminatoryVOCsinthebreath,identifying
metaboliteprofilesoflungcanceranddefininglungcancerphenotypestoapplytothebiomarkerprofiles.Ultimately,
we hope this work will lead to validated instruments and metabolic signatures capable of improving the clinical
management of lung cancer patients.
24

RespiratoryInstitute 25
GroupsCompared(N) Sensitivity Specificity
Non-smallcell(83) Controls(137) 70 86
Adenocarcinoma(50) Controls(137) 80 86
Squamouscell(23) Controls(137) 91 73
Adenocarcinoma(50) Squamouscell(22) 90 83
Smallcell(9) Controls(137) 89 85
Smallcell(9) Non-smallcell(83) 78 95
StagesIandII(41) StagesIIIandIV(42) 81 73
Survival<12mo(24) Survival>12mo(68) 70 86
RepresentativeSensitivityandSpecificityoftheMostAccurateModelforEachStudyQuestion
1.00.80.60.4
Specificity
Sens
itivi
ty
0.20.0
0.2
0.0
0.6
0.4
1.0
0.8Non-small cell vs controls, C statistic = 0.811
Adenocarcinoma vs controls, C statistic = 0.825
Squamous cell carcinoma vs controls, C statistic = 0.849
References
MazzonePJ,WangX,XuY,etal.Exhaledbreathanalysiswithacolorimetricsensorarrayfortheidentification and characterization of lung cancer. J Thorac Oncol.2012;7:137-142. MazzonePJ.Exhaledbreathvolatileorganiccompoundbiomarkersinlungcancer.J Breath Res.2012;6:027106.

Innovations
Clinical Intelligence Platform Using Big Data Technology
Socialmediaanduser-generatedcontentontheInternetcontinuetoleadthegrowthoftechnologiestostoreandanalyze
large volumes of data, most of which are unstructured. From the standpoint of data management, these data are similar
toclinicalinformation,whichisoftenunstructuredfreetext.BigDatatechnologiessuchasHBase,Cassandra,MongoDB
and others have certain features in common. They solve the problem of storing large volumes of data by splitting the data
among several computers. Fast data retrieval and analysis are made possible by sharing computational tasks among several
machines. This allows vast amounts of data to be stored and analyzed on clusters of inexpensive, commodity hardware.
TheRespiratoryInstitute’sClinicalIntelligencePlatform(CIP)wasbuiltusingBigDatatechnologytoanalyzeclinical
informationinour53-bedmedicalintensivecareunit.Allclinicaldata,includinglabandtextreportssuchasmicrobiology,
echocardiogramandradiologyreports,arecontinuouslyacquiredbytheCIP.Alertscanbecreatedusingasimpledragand
drop interface to create complex queries. For example, our alert to identify patients who are appropriate candidates for
physical therapy uses more than 40 clinical parameters. The platform continuously evaluates data and matches patients
basedonalertcriteria.SinceDecember2011,wehavereliedonautomatedcriteriatoscreenpatientsforphysicaltherapy
with excellent results, and we are currently evaluating algorithms for early detection of hospital-acquired infection and
acutekidney injuryintheintensivecareunit.
Iron in Pulmonary Arterial Hypertension
Pulmonaryarterialhypertension(PAH)ischaracterizedby increasedpulmonaryvascularresistanceandelevated
pressure leading to right heart failure and death. Therapies to date have focused on pulmonary vasodilation with
limited effect on overall survival.
WerecentlyidentifiedabnormalitiesinthematurationofbonemarrowcellsofpatientswithPAH,includingthebone
marrowcellsthatmaketheredbloodcells [FarhaS,etal.Blood.2011;117:3485-3493].Ironisamasterregulator
for proliferation, differentiation and maturation of all blood cells in the bone marrow. This has led us to investigate
whether there are abnormalities in iron metabolism that could account for the bone marrow abnormalities in pulmonary
hypertension.
Outcomes 201126

RespiratoryInstitute 27
Cellular iron is tightly regulated, as iron plays an essential role in oxygen transport and cellular respiration for energy
production. In general, the body views iron deficiency the same as low levels of oxygen availability or tissue hypoxia.
Themolecularresponsetolowironistoupregulateexpressionofthehypoxiainduciblefactors(HIF),whichcommand
a cascade of responses to increase oxygen delivery to tissues by increasing iron uptake and utilization, red blood
cellproductionandnewbloodvesselformation.OurstudiesandothershaveshownthatHIFisupregulatedinPAH
[FijalkowskaI,etal.Am J Pathol.2010;176:1130-1138;BonnetS,etal.Circulation.2006;113:2630-2641].
HIFinducibleproteins,suchaserythropoietin,whichtriggerredbloodcellproduction,areincreasedinPAHpatients
[FarhaS,etal.Blood.2011;117:3485-3493].
At Cleveland Clinic, we are studying iron metabolism in patients. Iron is essential for productive heme synthesis,
when iron is incorporated into the protoporphyrin ring by the mitochondrial enzyme ferrochelatase to produce heme
for insertion to hemoglobin. In iron deficiency or to block iron incorporation, zinc is inserted in place of iron to form
zincprotoporphyrin(Zn-pp).Totestwhetherabnormalitiesofironmetabolismarepresentandcontributetopulmonary
hypertension,wemeasuredZn-ppinredbloodcellsofpatientswithidiopathicPAH,associatedPAHandsleepapnea-
relatedPAHincomparisontocontrolhealthyandasthmaticindividuals.Despitesimilarlynormalredbloodcellcounts
andhemoglobinlevels,Zn-ppwashighinallPAHpatientsandtrackedwithmeasuresofdiseaseseverity[DeckerI,
et al. Clinical and Translational Science.2011;4(4):253-258].
RedbloodcellsofPAHpatientshadgreatervariation inthesizedistribution,i.e.,anincreaseintheredcell
distributionwidth(RDW),whichwasduethedeficientproductionofheme.RDWmeasurewasstronglyrelatedto
clinicalmeasuresofPAHseverity,includingpulmonaryarterypressuresandsix-minutewalkdistances.Thesefindings
suggest that a decrease in functional iron availability contributes to the pathophysiology of pulmonary hypertension.
Iron supplementation studies are currently under way to determine if iron can affect disease progression.

Outcomes 201128
Innovations
Novel Technique to Restore Patency in Complete Subglottic Stenosis
Subglotticandhightrachealstenosiscanoccurfrommanydifferentetiologiesandcanbeadifficultproblemtomanage.
Congenital and acquired factors may play a role. A suprastomal stenosis can be a troubling complication following a
tracheostomy. In particular, the inability to speak can have a dramatic impact on the patient’s quality of life. We managed
severalcasesofCotton-MyerGradeIVstenosisanddevelopedanalternativeapproachtoitsmanagement.
While an open surgical approach is considered to be the gold standard, often comorbidities, location or length of the lesion
will necessitate endobronchial management. The traditional endoscopic approach is to recannulate orally and has been
describednumeroustimesdatingbacktoChevalierJackson’sdescriptionofplacinganeedlethroughtheairwayfollowed
by airway molds composed of rubber.1,2 In some cases, however, the density and thickness of a stricture may prove to be
too formidable for the traditional approach.
Wedescribeanovelapproachtomanageadense,completelyornearlyoccludedsubglotticstenosis(SGS).Thistechnique
uses a retrograde approach through the prior tracheal stoma, establishing patency from the trachea to the larynx followed
later by more traditional endobronchial maneuvers. This technique is described briefly below.
ArigidbronchoscopeisinsertedtotheleveljustproximaltotheSGS.Thetracheotomytubeisremovedandunderapnea
a large gauge central line insertion needle is inserted cephalad through the stricture. Often the rigid light source may
provide transillumination and thus give a “target,” If the needle is not able to be passed quickly, the tracheotomy tube or
an endotracheal tube is reinserted and ventilation is restored. Once the needle is identified on the proximal side, a guide
wire can be threaded in a retrograde fashion and sequential balloon dilation is initiated. Once an orifice large enough is
established, dilation from above, using a rigid scope and gradually increasing diameter or a balloon, can be used to improve
the lumen size. A sequential rigid dilation is preferred at Cleveland Clinic because it preserves ventilation and can be left in
position to tamponade any bleeding while ventilating. Once a lumen is established, a T-tube may be inserted or a subglottic
stent can be placed above the tracheostomy tube.
A common theme in management of the subglottic or suprastomal stenosis was the recannalization from above. Our
technique provides an alternative approach that in several cases proved to be the only option. This technique will require
further evaluation, but to date has shown to be a reliable, safe and effective alternative for a difficult problem. Our opinion
is consistent with common perceptions that an operative approach should be considered in all patients, but in cases in
which surgery is not an option this technique provides a previously unavailable modality.

RespiratoryInstitute 29
CompleteSGSCotton-Myer grade IV Retrograde balloon dilation through stricture and into rigid scope

Outcomes 201130
Innovations
Laser-safe tube and “new” lumen
T-tube placement

RespiratoryInstitute 31
References
MachuzakM,GildeaT.WorldCongressofBronchologyand
Bronchoesophagoscopy 2012.
Final results

Outcomes 2011
Innovations
Stent Modifications
There are numerous treatment modalities for complex central airway
obstruction,includingplacementofendobronchialstents.Specifically,
silicone stents have been shown to be safe and effective. One feature
of silicone stents is that modifications can be made that improve fit
within the airway or decrease the chance for dislodgement. Although
stents are available in a wide range of sizes and shapes, there are still
problems when the simple tubular structures need to be modified to
serve the purpose of airway manipulation.
The basic techniques are: shortening or notching to accommodate
airway length, punching a hole for stenting across an open lobe, using
custom stent sizes and smoothing the stent’s edges. These techniques
have been employed in a wide range of malignant and nonmalignant
conditions with excellent results.
Modified hour glass stent
32

RespiratoryInstitute 33
Improvement in stenosis after placement of a modified stent
A y-stent sewn shut to occlude tracheoesophageal fistula and hole cut for right upper lobe
Stent modified to create a smaller diameter

Outcomes 201134
Innovations
Improved Forceps for Stent Placement
In the management of complex central airway
obstruction, we frequently have anatomic challenges
that require airway stenting. The problem with airways
as opposed to other tubular structures is that central
airways are not cylindrical and the branches of the
airways can be distorted and compressed, causing,
for example, cone-shaped airways or tortuous airways.
Often, when placing a stent, there is a need to adjust its
position and perhaps move it slightly more proximally
or distally. Because we only have instruments to pull
on a stent and pushing a stent risks causing further
airway trauma, we often favor initially placing a stent
distally, then trying to pull it back. When a stent gets
dislodged or if it does not seat properly and needs to
be adjusted distally, we have few options but to remove
the stent and replace it. With silicone stents, this is
relatively easily done with small risk, but metallic
stents cannot be reloaded. Sometimes we find that a
simple adjustment or a quick pull on the lower end of
the stent would be the ideal solution, but there are no
instruments designed for this purpose.
Steve Hoffman, RT, has watched us struggle with this
challenge for many years in the bronchoscopy suite.
He designed and patented backward grasping forceps
that will allow us to reach down below a lesion, foreign
body or stent to grasp it from an entirely different angle.
This will allow us an entirely new degree of freedom in
maneuvering in the airway and a new tool to care for
our patients.
Selected numerical references appear in the illustration
to the right and are in the patent abstract.
12
1030
124
44
118
110
114
116
114
34
112104
102
42 100
100
126
122
106120

RespiratoryInstitute 35
(12)
(54)
Hoffman
APPARATUS FOR INSERTION INTO A BODYLUMEN
(10) Patent No.:(45) Date of Patent:
US 7,559,946 B2Jul. 14, 2009
(75) Inventor: Steven William Hoffman, N. Olmsted,OH (US)
(73) Assignee: The Cleveland Clinic Foundation,Cleveland,OH (US)
(21) Appl. No.: 10/803,245
(22) Filed:
(51) Int. Cl.A61F 2/06A61B 10/00A61D 1/12
(56)
5,295,990 A * 3/1994 Levin 606/49
(2006.01)(2006.01)(2006.01)
U.S. PATENT DOCUMENTS
(60) Provisional application No. 60/455,642, files on Mar.18, 2003.
US 2004/0204718 A1 Oct. 14, 2004
See application file for complete search history.
Mar. 18, 2004
(65) Prior Publication Data ABSTRACT
3 Claims, 6 Drawing Sheets
Related U.S. Application Data
( * ) Notice: Subject to any disclaimer, the term of thispatent is extended or adjusted under 35U.S.C. 154(b) by 848 days.
6,136,006 A * 10/20005,928,263 A * 7/1999 606/2055,755,723 A * 5/1998 606/170
United States Patent
5,725,532 A * 3/1998
Johnson et al.Hoogeboom
7,105,016 B2 * 9/2006 623/1.12Shiu et al.6,261,308 B1 * 7/2001 606/207Saavedra
LombardoShoemaker 623/1.11
(58) Field of Classification Search
References Cited
600/108(52) U.S. Cl. 623/1.11; 600/564; 606/106
600/110, 205, 207, 170, 174, 106; 623/9,623/1.11; 600/562, 564
* cited by examiner
Primary Examiner—Todd E ManahanAssistant Examiner—Victor X Nguyen(74) Attorney, Agent or Firm—Tarolli, Sundheim, Covell &Tummino LLP
(57)
An Apparatus (10) for insertion into a body lumen (16)Includes an elongate member (30) having a proximal end (32)and a distal end (34) insertable into the body lumen (16). Atleast one clamping arm (100) includes a first end (102) havinga pivitol connection with the distal end (34) of the elongatemember (30). The pivotal connection provides pivotal move-ment of at least one clamping arm (100) relative to theelongate member (30). The at least one clamping arm (100)extends away from the pivotal connection toward the proxi-mal end (32) of the elongate member (30). The apparatus (10)also includes a control mechanism (40) for controlling thepivotal movement of the at least one clamping arm (100)relative to the elongate member (30). The apparatus (10) mayalso include an assembly (150) for controlling advancementof the member (30) in the body lumen (16).

Outcomes 2011
Innovations
36
Revised Training Model for Bronchoscopy
The apprentice model used to train physicians has remained virtually unchanged for decades, if not longer. The student
typically learns from the mentor by passive observation, with the famous saying at hand: “see one, do one, teach one.”
The apprentice model may not be sustainable, as learning medical procedures is a complex process. Competency in
bronchoscopy training still relies heavily on the number of procedures performed during fellowship training and a faculty
assessment often based on a grading system. In addition, novice fellows are often trained by more senior fellows or
pulmonologists who are not full-time bronchoscopists.
In the academic year 2011/2012, first-year fellows at Cleveland Clinic started working exclusively with our most
experiencedbronchoscopists.Simulation-basedtraininghasbeenshowntobeeffectiveandtoprovideincreasedpatient
comfort in a number of studies. We are currently in the process of incorporating simulation training in bronchoscopy prior
to patient contact. A new document stating the specific expectations for first-year trainees has been created. Because of
thecomplexityofbronchoscopyinthe21stcentury(frombasicprocedurestoadvanceddiagnosticandcomplextherapeutic
ones),anewevaluationformforanygivenbronchoscopyrotationhasbeencreated.Thegradingsystemnowevaluates
traineesinalesssubjectivemanner:novice,advancedbeginner,competentorproficient.Traineesareevaluatednotonly
for the specific technique, but also for the procedure planning, from the initial patient evaluation to the actual procedure
preparation, assessment and management of any complications, and short- and long-term follow-ups. The number-based
competency assessment alone is no longer acceptable.
The next step in the bronchoscopy training evaluation is the assessment of specific techniques used in addition to
theglobalrotationevaluation(e.g.,transbronchialbiopsies,endobronchialultrasound,transbronchialneedlebiopsies).
We hope that a more standardized training, both with simulation and on patients, will increase the confidence of our
trainees in addition to improving their skill, and thus improve the quality of care provided to our patients.

RespiratoryInstitute 37
Advanced Diagnostic Bronchoscopy Program
In recent years, there has been a relative explosion in technology in the bronchoscopy arena. From navigational
bronchoscopy to endobronchial ultrasound, advances in technology are more frequently finding their way into the
bronchoscopy suite. The challenge with cutting-edge technology is to balance its cost against the benefits it can
provide for patients.
TheAdvancedDiagnosticBronchoscopyProgramatClevelandClinichaspossiblythelargestexperienceinthese
new technologies, and through this experience we have been able to use these technologies, both individually and in
combination,tostreamlineapatient’scare,reducingunnecessary(andsometimesinvasive)procedures,enhancing
diagnostic accuracy and reducing the time to effective diagnoses. For example, our team has used radial probe ultrasound
inconjunctionwithnavigationalbronchoscopytoenhancetheyieldofthisprocedure.Thisinnovativetechniqueof
combining two cutting-edge technologies in complementary fashion is used by only a handful of institutions in the
UnitedStates.
Anotherexampleisusingendobronchialultrasound-guidedtransbronchialneedleaspiration(EBUS-TBNA)asafirst
stepinthediagnosisofsuspectedlungcancer.EBUS-TBNAofmediastinalnodesinthesepatientsnotonlycanachieve
diagnosis, but also can stage the cancer at the same sitting, thus potentially obviating other additional, and occasionally
more invasive, biopsy procedures. If a patient has a lung nodule that is suspicious for lung cancer, we have shown that
performinganEBUS-TBNAprocedureasafirstdiagnostictestcanresultinavoidingsubsequenttestinginmorethan
50 percent of patients, thereby also avoiding the additional cost and risk of these other testing procedures.
In addition to being at the forefront in bronchoscopic technology and a leader in procedural volume, we are especially
proud of how we are making these procedures work for our patients in cost-effective ways, enhancing patient outcome
byimprovingyieldandreducingtimetodiagnosis(andstaging)whileatthesametimeminimizingrisk.Duetoour
exposure to these technologies and our procedural volume, we are able to use our expertise and experience in
innovative ways to provide unparalleled patient care.

Outcomes 201138
Innovations
Bronchial Thermoplasty
Bronchialthermoplasty(BT)isanondrugtherapyforsevereasthmathatisavailableatClevelandClinic
RespiratoryInstitute’sAsthmaCenter.Thisnoveltherapeuticmodalityinvolvesthreesessionsofbronchoscopy
during which excess smooth muscle in airway walls is reduced by the application of thermal energy. Approved
in 2010 by the FDA, BT is meant for use in patients who have persistent asthma symptoms despite maximal
medical therapy. Clinical trials have demonstrated improvement in asthma quality-of-life scores as well
asareductioninsevereexacerbationsandemergencyroomvisits.Recentreportsdemonstratesafetyand
persistence of effectiveness two years after the procedure.
In our experience, carefully selected and medically optimized severe asthma patients who have undergone BT
have experienced improvements in their asthma symptoms, quality-of-life scores and exacerbations. We are
continuing to track patient characteristics and outcomes of treated patients to determine certain phenotypes
of patients who may experience most favorable responses to this therapy.
Currently, there is no cure for asthma. Comprehensive management of asthma with optimal medical therapy,
lifestyleadjustments,controlofconfoundingconditions(e.g.,GERD,sinusdisease,sleepapnea)andpatient
empowerment is essential to ensure the best possible patient outcomes. BT should be considered as one of
the components in a comprehensive management plan for severe asthmatics. Not all patients may be good
candidates; because the most common complication is exacerbation of asthma, patients must have symptoms
severe enough to qualify for BT but be well enough to tolerate the procedure. After careful consideration and
patient selection, BT offers a targeted approach to the smooth muscle dysfunction and hyperactivity in asthma.
References
GildeaTR,KhatriSB,CastroM.Bronchialthermoplasty:Anewtreatmentforsevererefractoryasthma.Cleve Clin J Med. 2011 Jul;78(7):477-485.

RespiratoryInstitute 39
References
MillerJD,CoxG,VincicL,LombardCM,LoomasBE,DanekCJ.Aprospectivefeasibilitystudyofbronchialthermoplasty in the human airway. Chest.2005Jun;127(6):1999-2006.MedicalIllustrator:MarkSabo,CCF.
Bronchial thermoplasty for severe refractory asthma
Bronchial thermoplasty involves delivery of radiofrequency energy to the airway wall which ablates the smooth muscle layer, lessening bronchoconstriction and improving symptoms.
Treatments are done in three separate procedures, with meticulous mapping of the areas treated. The right lower lobe is treated in the first procedure, the left lower lobe in the second, and the two upper lobes in the third. The right middle lobe is not treated.
Rightmiddlelobe is not treated
Procedure3: Upperlobes
Procedure1: Rightlowerlobe
Procedure2: left lower lobe

Outcomes 2011
Selected Publications
40
Albashir S, Olansky L, Sasidhar M. Progressive muscle weakness: More there than meets the eye. Cleve Clin J Med. 2011 Jun;78(6):385-391.
Almeida FA, Bruno DS, Faiz S, Hinrichs B, Eapen GA, Bashoura L. Hemothorax treated with indwelling tunneled pleural catheter: Are all hemothoraces the same? J Bronchology Interv Pulmonol. 2011 Jul;18(3): 261-264.
Amann A, Corradi M, Mazzone P, Mutti A. Lung cancer biomarkers in exhaled breath. Expert Rev Mol Diagn. 2011 Mar;11(2):207-217.
Aytekin M, Dweik RA. Low-molecular-mass of hyaluronan was detected in PASMCs from the patients with idiopathic pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol. 2011 Jan;300(1):L148.
Balzar S, Fajt ML, Comhair SAA, Erzurum SC, Bleecker E, Busse WW, Castro M, Gaston B, Israel E, Schwartz LB, Curran-Everett D, Moore CG, Wenzel SE. Mast cell phenotype, location, and activation in severe asthma: data from the severe asthma research program. Am J Respir Crit Care Med. 2011 Feb 1;183(3):299-309.
Batal O, Khatib OF, Bair N, Aboussouan LS, Minai OA. Sleep quality, depression, and quality of life in patients with pulmonary hypertension. Lung. 2011 Apr;189(2):141-149.
Bauer EM, Zheng H, Comhair S, Erzurum S, Billiar TR, Bauer PM. Complement C3 deficiency attenuates chronic hypoxia-induced pulmonary hypertension in mice. PLoS ONE. 2011;6(12):e28578.
Bauer SR, Culver DA, Abraham S, Lam SW, Fissell WH, Wiedemann HP, Reddy AJ. Detectability of vasopressin in continuous venovenous hemodialysis effluent of patients with vasodilatory shock treated with exogenous arginine vasopressin. Pharmacotherapy. 2011 Sep;31(9):857-862.
Baughman RP, Culver DA, Judson MA. A concise review of pulmonary sarcoidosis. Am J Respir Crit Care Med. 2011 Mar 1;183(5):573-581.
Baumgartner M, Ashton R. Diffuse alveolar hemorrhage. South Med J. 2011 Apr;104(4):274-275.
Bencsath KP, Reu F, Dietz J, Hsi ED, Heresi GA. Idiopathic systemic capillary leak syndrome preceding diagnosis of infiltrating lobular carcinoma of the breast with quiescence during neoadjuvant chemotherapy. Mayo Clin Proc. 2011 Mar;86(3):260-261.
Respiratory Institute staff authored
more than
100 publications in 2011.
clevelandclinic.org/outcomes.

RespiratoryInstitute 41
BrozekJL,AklEA,CompalatiE,KreisJ,TerraccianoL,FiocchiA,UeffingE,AndrewsJ,Alonso-CoelloP, MeerpohlJJ,Lang DM,JaeschkeR,WilliamsJW,Jr.,PhillipsB,LethabyA,BossuytP,GlasziouP,HelfandM,WatineJ,AfilaloM,WelchV,MontedoriA,AbrahaI, HorvathAR,BousquetJ,GuyattGH,SchunemannHJ. Gradingqualityofevidenceandstrengthofrecommendations in clinical practice guidelines. Part3of3.TheGRADEapproachtodevelopingrecommendations. Allergy.2011May;66(5):588-595.
BulekK,LiuC,SwaidaniS,WangL,PageRC,GulenMF,HerjanT,AbbadiA,QianW,SunD,LauerM,HascallV,MisraS,ChanceM,Aronica M,HamiltonT,LiX.TheinduciblekinaseIKKiisrequiredforIL-17-dependentsignaling associated with neutrophilia and pulmonary inflammation. Nat Immunol.2011;12(9):844-852.
BusseWW,PetersSP,FentonMJ,MitchellH,BleeckerER,CastroM,WenzelS,Erzurum SC,FitzpatrickAM,TeagueWG,JarjourN,MooreWC,SuminoK,SimeoneS,RatanamaneechatS,PenugondaM,GastonB,RossTM,SigelmanS,SchiepanJR,ZaccaroDJ,CrevarCJ, CarterDM,TogiasA.Vaccinationofpatientswith mildandsevereasthmawitha2009pandemicH1N1 influenza virus vaccine. J Allergy Clin Immunol. 2011 Jan;127(1):130-137.e3.
CastroM,FainSB,HoffmanEA,GieradaDS, Erzurum SC,WenzelS.Lungimaginginasthmaticpatients: The picture is clearer. J Allergy Clin Immunol. 2011Sep;128(3):467-478.
Chatburn RL,Mireles-CabodevilaE.Closed-loopcontrolof mechanical ventilation: description and classification of targeting schemes. Respir Care.2011Jan;56(1):85-102.
Chatburn RL,GoleS,SchenkP,HoisingtonER,Stoller JK. Respiratorycareworkassignmentbasedonworkrateinstead of work load. Respir Care.2011Nov;56(11): 1785-1790.
ChengG,SwaidaniS,SharmaM,LauerME,HascallVC,Aronica MA.Hyaluronandepositionandcorrelationwithinflammation in a murine ovalbumin model of asthma. Matrix Biol.2011Mar;30(2):126-134.
CoghillM,AmbalavananN,Chatburn RL,HibberdPL,Wright LL, Carlo WA. Accuracy of a novel system for oxygen delivery to small children. Pediatrics. 2011 Aug;128(2):e382-e387.
ComhairSAA,GastonBM,RicciKS,HammelJ,Dweik RA, TeagueWG,MeyersD,AmplefordEJ,BleeckerER, BusseWW,CalhounWJ,CastroM, ChungKF, Curran-EverettD,IsraelE,JarjourWN,MooreW,PetersSP,WenzelS,HazenSL,Erzurum SC. Detrimental effects of environmental tobacco smoke in relation to asthma severity. PLoS ONE.2011;6(5):e18574.
CoxL,NelsonH,LockeyR,CalabriaC,ChackoT, FinegoldI,NelsonM,WeberR,BernsteinDI, Blessing-MooreJ,KhanDA,Lang DM,NicklasRA,OppenheimerJ,PortnoyJM,RandolphC,SchullerDE,SpectorSL,TillesS,WallaceD.Allergenimmunotherapy:a practice parameter third update. J Allergy Clin Immunol. 2011Jan;127(1Suppl):S1-S55.
Culver DA,BaughmanRP.TNF-alphaantagonistsandsarcoidosis. QJM.2011Apr;104(4):374.
Cumbo-NacheliG,Ashton RW.Mucoidplugsineosinophilic pneumonia. J Bronchology Interv Pulmonol. 2011Jul;18(3):257-258.
Cumbo-NacheliG,SamavatiL,Guzman JA. Bioavailability of fondaparinux to critically ill patients. J Crit Care. 2011 Aug;26(4):342-346.
DaVeigaSP,LiuX,CarusoK,GolubskiS,XuM,Lang DM. Systemicreactionsassociatedwithsubcutaneousallergenimmunotherapy: timing and risk assessment. Ann Allergy Asthma Immunol.2011Jun;106(6):533-537.

Outcomes 201142
Selected Publications
DeckerI,GhoshS,ComhairSA,Farha S,TangWHW, ParkM,WangS,LichtinAE,Erzurum SC.High levels of zinc-protoporphyrin identify iron metabolic abnormalities in pulmonary arterial hypertension. Clin Transl Sci.2011Aug;4(4):253-258.
DemirjianS,TeoBW,Guzman JA,HeykaRJ,PaganiniEP,FissellWH,ScholdJD,SchreiberMJ.Hypophosphatemiaduring continuous hemodialysis is associated with prolonged respiratory failure in patients with acute kidney injury.Nephrol Dial Transplant.2011Nov;26(11): 3508-3514.
DemirjianSG,RainaR,BhimrajA,NavaneethanSD,GordonSM,SchreiberMJ,Jr.,Guzman JA. 2009 influenzaAinfectionandacutekidneyinjury:incidence,risk factors, and complications. Am J Nephrol. 2011;34(1):1-8.
DrakeKM,ZygmuntD,MavrakisL,HarborP,WangL,ComhairSA,Erzurum SC,AldredMA.AlteredmicroRNAprocessing in heritable pulmonary arterial hypertension: AnimportantroleforSmad-8.Am J Respir Crit Care Med. 2011Dec15;184(12):1400-1408.
DummerJ,StorerM,SwanneyM,McEwanM, Scott-ThomasA,BhandariS,ChambersS,Dweik R, EptonM.Analysisofbiogenicvolatileorganiccompoundsin human health and disease. Trends Analyt Chem. 2011 Jul;30(7):960-967.
DuongHT,Erzurum SC,AsosinghK.Pro-angiogenichematopoietic progenitor cells and endothelial colony-forming cells in pathological angiogenesis of bronchial and pulmonary circulation. Angiogenesis. 2011 Dec;14(4):411-422.
Dweik R. Bulletin Board: Breathe easy? Exhaled molecules may reveal those who have been infected with influenza. Therapy.2011Sep;8(5):511-514.
Dweik R. The great challenge for exhaled breath analysis: embracing complexity, delivering simplicity. J Breath Res. 2011Sep;5(3):030201.
Dweik R, Erzurum SC.Updateonpulmonaryvasculardiseases 2010. Am J Respir Crit Care Med. 2011 Jul1;184(1):26-31.
EpsteinSK,Chatburn RL.Patient-ventilatorinteraction.Foreword. Respir Care.2011Jan;56(1):13-14.
Farha S,AsosinghK,XuW,SharpJ,GeorgeD,ComhairS, ParkM,TangWHW,LoydJE,TheilK,TubbsR,HsiE,LichtinA,ErzurumSC.Hypoxia-induciblefactorsin human pulmonary arterial hypertension: a link to the intrinsic myeloid abnormalities. Blood. 2011 Mar31;117(13):3485-3493.
Fernandez-BussyS,MajidA,CaviedesI,Akindipe O, BazM,JantzM.Treatmentofairwaycomplicationsfollowing lung transplantation. Arch Bronconeumol. 2011Mar;47(3):128-133.
GangopahyayA,OranM,BauerEM,WertzJW, ComhairSA,Erzurum SC,BauerPM.Bonemorphogeneticprotein receptor II is a novel mediator of endothelial nitric-oxide synthase activation. J Biol Chem. 2011Sep23;286(38):33134-33140.
GarchaPS,SantacruzJF,Machuzak MS, Budev MM, Mehta A. Clinical course after successful double lung transplantation in a patient with severe scoliosis. J Heart Lung Transplant.2011Feb;30(2):234-235.
GhoshS,Erzurum SC. Nitric oxide metabolism in asthma pathophysiology. Biochim Biophys Acta. 2011 Nov;1810(11):1008-1016.
Gildea TR, Khatri SB,CastroM.Bronchialthermoplasty:A new treatment for severe refractory asthma. Cleve Clin J Med.2011Jul;78(7):477-485.

RespiratoryInstitute 43
GreenhawtMJ,LiJT,BernsteinDI,Blessing-MooreJ,CoxL,KhanD, Lang DM,NicklasRA,OppenheimerJ,PortnoyJM,RandolphC,SchullerDE,SpectorSL,TillesSA,WallaceD.Administeringinfluenzavaccinetoegg allergic recipients: a focused practice parameter update. Ann Allergy Asthma Immunol.2011Jan;106(1):11-16.
GudavalliR,Diaz-GuzmanE,ArrossiAV,Chapman JT, Mehta AC. Fleeting alveolar infiltrates and reversed halo sign in patients with breast cancer treated with tangential beam irradiation. Chest.2011Feb;139(2):454-459.
Guzman JA, Sasidhar M, Stoller JK.CaringforVIPs:Nineprinciples. Cleve Clin J Med.2011Feb;78(2):90-94.
Guzman JA,TchokonteR,SobelJD.Septicshockduetocandidemia:outcomes and predictors of shock development. J Clin Med Res. 2011 Apr4;3(2):65-71.
HaserodtS,AytekinM,Dweik RA. A comparison of the sensitivity, specificity, and molecular weight accuracy of three different commercially availableHyaluronanELISA-likeassays.Glycobiology.2011Feb;21(2): 175-183.
Heresi GA, Dweik RA.Strengthsandlimitationsofthesix-minute- walk test: a model biomarker study in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med.2011May1;183(9):1122-1124.
Heresi GA. Clinical perspective: biomarkers in pulmonary arterial hypertension. Int J Clin Pract Suppl.2011Jan;(169):5-7.
HoitBD,DaltonND,GebremedhinA,JanochaA,ZimmermanPA,ZimmermanAM,StrohlKP,Erzurum SC,BeallCM.Elevatedpulmonaryartery pressure among Amhara highlanders in Ethiopia. Am J Hum Biol. 2011Mar-Apr;23(2):168-176.
HolguinF,BleeckerER,BusseWW,CalhounWJ,CastroM,Erzurum SC, FitzpatrickAM,GastonB,IsraelE,JarjourNN,MooreWC,PetersSP,Y onasM,TeagueWG,WenzelSE.Obesityandasthma:an association modified by age of asthma onset. J Allergy Clin Immunol. 2011Jun;127(6):1486-1493.

Outcomes 2011
Selected PublicationsSelected Publications
44
HossainM,Mazzone P, Tierney W, Cucullo L. In vitro assessment of tobacco smoke toxicity at the BBB: do antioxidant supplements have a protective role? BMC Neurosci. 2011;12:92.
HuangP,ChengG,LuH,Aronica M,RansohoffRM, Zhou L. Impaired respiratory function in mdx and mdx/utrn(+/-)mice.Muscle Nerve.2011Feb;43(2):263-267.
HunterGW,XuJC,Biaggi-LabiosaAM,LaskowskiD, DuttaPK,MondalSP,WardBJ,MakelDB,LiuCC, Chang CW, Dweik RA.Smartsensorsystemsfor human health breath monitoring applications. J Breath Res.2011Sep;5(3):037111.
Isiguzo M,BrunkenR,TchouP,XuM,Culver DA. Metabolism-perfusionimagingtopredictdisease activity in cardiac sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis.2011Jul;28(1):50-55.
JainA,McCarthyK,XuM,Stoller JK. Impact of a clinical decision support system in an electronic health record to enhancedetectionofalpha(1)-antitrypsindeficiency. Chest.2011Jul;140(1):198-204.
JamieS,TylerCV,Jr.,Parambil JG.Sarcoidosispresentingas symptomatic hypercalcemia in an octogenarian. Clin Geriatr.2011Apr;19(4):43-46.
JanochaAJ, KochCD,TisoM,PonchiaA,DoctorA, GibbonsL,GastonB,BeallCM,Erzurum SC. Nitric oxide during altitude acclimatization. N Engl J Med. 2011 Nov17;365(20):1942-1944.
KawR,PasupuletiV,DeshpandeA,HamiehT, Walker E, Minai OA.Pulmonaryhypertension: An important predictor of outcomes in patients undergoing non-cardiac surgery. Respir Med. 2011Apr;105(4):619-624.

RespiratoryInstitute 45
Mashir A,PaschkeKM,vanDuinD,ShresthaNK, LaskowskiD,StorerMK,Yen-LiebermanB,GordonSM,AytekinM,Dweik RA.EffectoftheinfluenzaA(H1N1) liveattenuatedintranasalvaccineonnitricoxide(FE(NO))and other volatiles in exhaled breath. J Breath Res. 2011Sep;5(3):037107.
MasonDP,MurthySC,YunJJ,Machuzak M,ShresthaR,AveryRK,McCurryKR,Budev MM,PetterssonGB. Lung transplantation in a recipient with novel 2009 H1N1influenza:Lessonslearned.Thorac Cardiovasc Surg.2011Mar;59(2):126-127.
McCormackFX,InoueY,MossJ,SingerLG, StrangeC,NakataK,BarkerAF,Chapman JT, BrantlyML,StocksJM,BrownKK,LynchJP,III, GoldbergHJ,YoungLR,KinderBW,DowneyGP, SullivanEJ,ColbyTV,McKayRT,CohenMM, KorbeeL,Taveira-DaSilvaAM,LeeHS,KrischerJP, Trapnell BC. Efficacy and safety of sirolimus in lymphangioleiomyomatosis. N Engl J Med. 2011Apr28;364(17):1595-1606.
MezianeM,ObuchowskiNA,LababedeO,LieberML,PhilipsM,Mazzone P. A comparison of follow-up recommendations by chest radiologists, general radiologists, and pulmonologists using computer-aided detection to assess radiographs for actionable pulmonary nodules. AJR Am J Roentgenol.2011May;196(5):W542-W549.
ModrykamienA,Minai O.A 60-yearoldman presenting with yellow nail syndrome. Respir Care. 2011Jul;56(7):1043-1045.
ModrykamienA,ChatburnRL,Ashton RW. Airway pressure release ventilation: An alternative mode of mechanical ventilation in acute respiratory distress syndrome [Erratum in: Cleve Clin J Med 2011Apr;78(4):240].Cleve Clin J Med. 2011 Feb;78(2):101-110.
KostikasK,MinasM,PapaioannouAI,PapirisS, Dweik RA. Exhaled nitric oxide in asthma in adults: The end is the beginning? Curr Med Chem. 2011;18(10):1423-1431.
LababedeO,MezianeM,Rice T.Seventhedition of the cancer staging manual and stage grouping of lung cancer: quick reference chart and diagrams. Chest.2011Jan;139(1):183-189.
LiX,HowardTD,MooreWC,AmplefordEJ,LiH, BusseWW,CalhounWJ,CastroM,ChungKF, Erzurum SC,FitzpatrickAM,GastonB,Israel E, JarjourNN,TeagueWG,WenzelSE,PetersSP, HawkinsGA,BleeckerER,MeyersDA.Importance of hedgehog interacting protein and other lung function genes in asthma. J Allergy Clin Immunol. 2011Jun;127(6):1457-1465.
LiuC,SwaidaniS,QianW,KangZ,SunP,HanY, WangC,GulenMF,YinW,ZhangC,FoxPL,Aronica M, HamiltonTA,MisraS,DengJ,LiX.ACC’loopdecoypeptideblockstheinteractionbetweenAct1andIL-17RAto attenuate IL-17- and IL-25-induced inflammation. Sci Signal.2011;4(197):ra72.
LiuL,TeagueWG,Erzurum S,FitzpatrickA,MantriS,Dweik RA,BleeckerER,MeyersD,BusseWW, CalhounWJ,CastroM,ChungKF,Curran-EverettD, IsraelE,JarjourWN,MooreW,PetersSP,WenzelS, HuntJF,GastonB.DeterminantsofexhaledbreathcondensatepHinalargepopulationwithasthma. Chest.2011Feb;139(2):328-336.
MahajanAK,DietteGB,Hatipoglu U, Bilderback A, RidgeA,HarrisVW,DalapathiV,BadlaniS,LewisS,CharbeneauJT,NaureckasET,KrishnanJA.High frequency chest wall oscillation for asthma and chronic obstructive pulmonary disease exacerbations: a randomized sham-controlled clinical trial. Respir Res. 2011;12:120.

Outcomes 201146
Selected Publications
RiceBL,FarverCF,PohlmanB,BurkeyBB,Parambil JG. Concomitant Castleman’s disease and sarcoidosis. Am J Med Sci.2011Mar;341(3):257-259.
RiceBL,Culver DA,SantacruzJF,LazarCA,McCarthyK,Gildea TR. Obstructive fibrinous tracheal pseudomembrane. Ann Thorac Surg.2011Dec;92(6):e115-e117.
SahinerUM,BirbenE,Erzurum S,SackesenC,KalayciO.Oxidative stress in asthma. World Allergy Organiz J. 2011 Oct;4(10):151-158.
SahooDH,BandyopadhyayD,XuM,PearsonK,Parambil JG, Lazar CA, Chapman JT, Culver DA. Effectiveness and safety of leflunomide for pulmonary and extrapulmonary sarcoidosis. Eur Respir J.2011Nov;38(5):1145-1150.
Siles RI, Hsieh FH. Allergy blood testing: A practical guide for clinicians. Cleve Clin J Med.2011Sep;78(9):585-592.
SwaidaniS,BulekK,KangZ,GulenMF,LiuC,YinW, Abbadi A, Aronica M,LiX.Tcell-derivedAct1isnecessaryfor IL-25-mediated Th2 responses and allergic airway inflammation. J Immunol.2011Sep15;187(6):3155-3164.
SwaisgoodCM,Oswald-RichterK,MoellerSD,KlemencJM, RupleLM,FarverCF,DrakeJM,Culver DA,DrakeWP.Development of a sarcoidosis murine lung granuloma model usingMycobacteriumsuperoxidedismutaseApeptide. Am J Respir Cell Mol Biol.2011Feb;44(2):166-174.
TarabishyAB,KhatibOF,NoceroJR,Budev M,KaiserPK.Ocular complications in patients with lung transplants. Br J Ophthalmol.2011Sep;95(9):1295-1298.
TarboxJA,GuttaRC,Radojicic C, Lang DM.Utility of routine laboratory testing in management of chronic urticaria/angioedema. Ann Allergy Asthma Immunol. 2011Sep;107(3):239-243.
MondalSP,DuttaPK,HunterGW,WardBJ, Laskowski D, Dweik RA. Development of high sensitivity potentiometric NOx sensor and its application to breath analysis. Sens Actuators B Chem.2011Nov15;158(1):292-298.
MurthySC,NowickiER,MasonDP,Budev MM, Nunez AI, Thuita L, Chapman JT,McCurryKR, PetterssonGB,BlackstoneEH.Pretransplantgastroesophageal reflux compromises early outcomes after lung transplantation. J Thorac Cardiovasc Surg. 2011Jul;142(1):47-52.
Parambil JG,TaveeJO,ZhouL,PearsonKS, Culver DA. Efficacy of intravenous immunoglobulin for small fiber neuropathy associated with sarcoidosis. Respir Med.2011Jan;105(1):101-105.
PatelDC,Ashton RW. Inhaled therapy for acute COPDexacerbationinthehospital:Arewemissing the low-hanging fruit? South Med J. 2011 Nov;104(11):746.
PaulM,JohnS,Ashton RW.Recurrentpneumoniaina51-year-old woman due to congenital bronchoesophageal fistula. Respir Care.2011Aug;56(8):1203-1205.
PinneyMF,RosenbergAF,HamppC,SchainD, Akindipe O,BazM.Invasivefungalinfectionsin lung transplant recipients not receiving routine systemic antifungal prophylaxis: 12-year experience at a university lung transplant center. Pharmacotherapy. 2011 Jun;31(6):537-545.
RainaR,SimonJF,MarionCR,ValeriaA,NavaneethanSD,Heresi GA, Guzman JA,WehbeE,NallyJV.Unusualcases of hydronephrosis with retroperitoneal fibrosis: mystery revealed. NDT Plus.2011Oct;4(5):313-317.

47RespiratoryInstitute
TaveeJ,Culver D.Sarcoidosisandsmall-fiberneuropathy.Curr Pain Headache Rep.2011Jun;15(3):201-206.
Taylor C, Farver C, Stoller JK.Perspective:Canemotionalintelligence training serve as an alternative approach to teaching professionalism to residents? Acad Med. 2011 Dec;86(12):1551-1554.
Tonelli AR,AlnuaimatH,LiN,CarrieR,MubarakKK.Value of impedance cardiography in patients studied for pulmonary hypertension. Lung. 2011 Oct;189(5):369-375.
Tonelli AR,Mubarak KK,LiN,CarrieR,AlnuaimatH.Effect of balloon inflation volume on pulmonary artery occlusion pressure in patients with and without pulmonary hypertension. Chest. 2011 Jan;139(1):115-121.
TorgersonDG,AmplefordEJ,ChiuGY,GaudermanWJ,GignouxCR,GravesPE,HimesBE,LevinAM, MathiasRA,HancockDB,BaurleyJW,EngC,SternDA,CeledonJC,RafaelsN,CapursoD,ContiDV,RothLA, Soto-QuirosM,TogiasA,LiX,MyersRA,RomieuI, VanDenBergDJ,HuD,HanselNN,HernandezRD, IsraelE,SalamMT,GalanterJ,AvilaPC,AvilaL, Rodriquez-SantanaJR,ChapelaR,Rodriguez-CintronW,Diette GB,AdkinsonNF,AbelRA,RossKD,ShiM, FaruqueMU,DunstonGM,WatsonHR,ManteseVJ,Ezurum SC,LiangL,RuczinskiI,FordJG,HuntsmanS,ChungKF,VoraH,LiX,CalhounWJ,CastroM, Sienra-MongeJJ,delRio-NavarroB,DeichmannKA,HeinzmannA,WenzelSE,BusseWW,GernJE, LemanskeRF,Jr.,BeatyTH,BleeckerER,RabyBA, MeyersDA,LondonSJ,GillilandFD,BurchardEG, MartinezFD,WeissST,WilliamsLK,BarnesKC,OberC,NicolaeDL.Meta-analysisofgenome-wideassociationstudies of asthma in ethnically diverse North American populations. Nat Genet.2011;43(9):887-892.
VakilN,MasonDP, YunJJ,MurthySC,Budev MM, PetterssonGB.Third-timelungtransplantationina patient with cystic fibrosis. J Thorac Cardiovasc Surg. 2011Jan;141(1):e3-e5.
Wang D, Olman MA,StewartJ,Jr.,TippsR,HuangP, SandersPW,TolineE,PraysonRA,LeeJ,WeilRJ, PalmerCA,GillespieGY,LiuWM,PieperRO,GuanJL,GladsonCL.DownregulationofFIP200inducesapoptosisof glioblastoma cells and microvascular endothelial cells by enhancingPyk2activity.PLoS ONE.2011;6(5):e19629.
WangKP,Feller-KopmanD,Mehta A,SharmaM,YarmusL.Endobronchialultrasoundandesophagealultrasound:justbecause we can, does not necessarily mean we should. Chest.2011Jul;140(1):271-272.
WedesSH,WuW,ComhairSAA,McDowellKM, DiDonatoJA, Erzurum SC,HazenSL.Urinarybromotyrosinemeasures asthma control and predicts asthma exacerbations in children. J Pediatr.2011Aug;159(2):248-255.
WheelerDM,Stoller JK. Teamwork, teambuilding and leadership in respiratory and health care. Canadian Journal of Respiratory Therapy.2011Spring;47(1):6-11.
Wiedemann HP.Fishoilisnotthefixforacutelunginjury.Crit Care Med.2011Jul;39(7):1829-1830.
ZamoraMR,Budev M,RolfeM,GottliebJ,HumarA,DeVincenzoJ,VaishnawA,CehelskyJ,AlbertG,NochurS,Gollob JA,GlanvilleAR.RNAinterferencetherapyinlungtransplant patients infected with respiratory syncytial virus. Am J Respir Crit Care Med.2011Feb15;183(4):531-538.

Outcomes 2011
Staff Listing
Chairman
HerbertWiedemann,MD,MBA
Quality Improvement Officer
UmurHatipoglu,MD
Pulmonary and Critical Care Medicine
LoutfiAboussouan,MD
JafarAbunasser,MD Medical Director, ReSCU
MuzaffarAhmad, MD
OlufemiAkindipe,MD
FranciscoAlmeida,MD,MS Director, Interventional Pulmonary Medicine Fellowship Program
RendellAshton,MD Associate Director, Medical Intensive Care Unit Director, Pulmonary and Critical Care Fellowship Program
JamesBlackburn,DO
MarieBudev,DO,MPH Medical Director, Lung Transplantation
RobertCastele,MD
ChiragChoudhary,MD
JosephCicenia,MD
Daniel Culver, DO Director, Sarcoidosis Program
JeanLouisDupiton,MD
RaedDweik,MD Director, Pulmonary Vascular Disease Program
SerpilErzurum,MD Chair, Department of Pathobiology Co-Director, Asthma Center
HanyFarag,MD
SamarFarha,MD
AndrewGarrow,MD
Puneet,Garcha,MD
ThomasGildea,MD,MS Section Head, Bronchoscopy
JorgeGuzman,MD Director, Medical Intensive Care Unit Section Head, Critical Care Medicine
TarikHanane,MD
GustavoHeresi,MD
DavidHolden,MD
AanchalKapoor,MD
SumitaKhatri,MD,MS Co-Director, Asthma Center
SudhirKrishnan,MD
CharlesLane,MD
MichaelMachuzak,MD Medical Director, Center for Major Airway Disease
PeterMazzone,MD,MPH Director, Lung Cancer Program
GlennMeden,MD
AtulMehta,MD
4848

RespiratoryInstitute
OmarMinai,MD
KathrinNicolacakis,MD
ThomasOlbrych,MD
MitchellOlman,MD
BeverlyO’Neill,MD
AmanPande,MD
JosephParambil,MD Director, HHT Center
BohdanPichurko,MD Director, Pulmonary Function Lab
JenniferRamsey,MD,MS
DeborahRathz,MD,PhD
AnitaReddy,MD
RaymondSalomone,MD
MadhuSasidhar,MD Section Head, Respiratory Therapy
DavidSkirball,MD
JamesStoller,MD,MS Chairman, Education Institute
AdrianoTonelli,MD
JoeZein,MD
Allergy and Clinical Immunology
DavidLang,MD Section Head Co-Director, Asthma Center Director, Allergy and Immunology Fellowship Program
SheilaArmogida,MD
MarkAronica,MD
4949
JamesFernandez,MD,MPH
SandraHong,MD
FredHsieh,MD
LilyPien,MD
CristineRadojicic,MD
RoxanaSiles,MD
RachelSzekely,MD
Somephysiciansmaypracticeinmultiplelocations. For a detailed list including staff photos, please visit clevelandclinic.org/staff.

Outcomes 2011
General Patient Referral
24/7 hospital transfers or physician consults
800.553.5056
Pulmonary Appointments/Referrals
216.444.6503or800.223.2273,ext.46503
Allergy Appointments/Referrals
216.444.3386or800.223.2273,ext.43386
On the Web at clevelandclinic.org/pulmonary
Contact Information
5050

RespiratoryInstitute 5151
Additional Contact Information
General Information 216.444.2200
Hospital Patient Information 216.444.2000
General Patient Appointments 216.444.2273or800.223.2273
Referring Physician Center and Hotline ClevelandClinic’sReferringPhysicianCenterhasestablisheda24/7hotline—855.REFER.123(855.733.3712)—tostreamline access to our array of medical services. Contact theReferringPhysicianHotlineforinformationonourclinicalspecialties and services, to schedule and confirm patient appointments, for assistance in resolving service-related issues, and to connect with Cleveland Clinic specialists.
Request for Medical Records 216.444.2640or800.223.2273,ext.42640
Medical Concierge Complimentary assistance for out-of-state patients and families
800.223.2273,ext.55580,[email protected]
Global Patient Services/International Center Complimentary assistance for international patients and families
001.216.444.8184orvisitclevelandclinic.org/gps Cleveland Clinic Florida 866.293.7866 For address corrections or changes, please call 800.890.2467

Institute Locations
Outcomes 20115252
Cleveland Clinic Main Campus
9500 Euclid Ave. Cleveland,OH44195 216.444.6503 PulmonaryandAllergy
Beachwood Family Health and Surgery Center
26900CedarRoad Beachwood,OH44122 216.839.3820 Pulmonary
Brunswick Family Health Center
3574CenterRoad Brunswick,OH44212 330.225.8886 Pulmonary
Chagrin Falls Family Health Center
551E.WashingtonSt. ChagrinFalls,OH44022 440.893.9393 800.232.0263 PulmonaryandAllergy
Euclid Hospital
EuclidMedicalOfficeBuilding 99NorthlineCircle,Suite235 Euclid,OH44119 216.692.7848 Pulmonary
Hillcrest Hospital
HillcrestAtrium 6780MayfieldRoad,Suite323 MayfieldHeights,OH44124 440.312.7140 Pulmonary
Independence Family Health Center
Crown Centre II 5001RocksideRoad Independence,OH44131 216.986.4000 PulmonaryandAllergy
Medina Medical Office Building – South
970E.WashingtonSt. Medina,OH44256 330.721.5700 Allergy
Mentor Physician Office
9500MentorAve. Mentor,OH44060 440.639.0448 Pulmonary
Richard E. Jacobs Family Health Center
33100ClevelandClinicBlvd. Avon,OH44011 440.695.4000 PulmonaryandAllergy
Institute Locations

RespiratoryInstitute
South Pointe Hospital Charles B. Miner Medical Office Building
20050HarvardRoad WarrensvilleHeights,OH44122 216.295.1010 Pulmonary
Strongsville Family Health and Surgery Center
16761SouthParkCenter Strongsville,OH44136 440.878.2500 PulmonaryandAllergy
Twinsburg Family Health and Surgery Center
8701DarrowRoad Twinsburg,OH44087 330.888.4000 PulmonaryandAllergy
Willoughby Hills Family Health Center
2550&2570SOMCenterRoad WilloughbyHills,OH44094 440.943.2500 800.807.2888 PulmonaryandAllergy
Wooster Family Health Center
1740ClevelandRoad Wooster,OH44691 330.287.4500 800.451.9870 PulmonaryandAllergy
5353

Outcomes 20115454
Improving Quality, Safety and the Patient Experience
Overview
Cleveland Clinic uses a scorecard approach to measure quality, safety and patient experience. In addition, real-time dashboard data are leveraged to drive performance improvement. Although not an exact match to publicly reported data, more timely internal data provide transparency for leaders at all levels of the organization to support improved care in their clinical locations. The following are examples of Cleveland Clinic’s 2011 focus areas and main campus results.
Appropriateness of Care 2010 – 2011
ClevelandClinic’sobserved/expected(O/E)mortalityratiooutperformedtheUniversityHealthSystemConsortium(UHC)academicmedicalcenter50thpercentile throughout 2011.
Cleveland Clinic’s goal is for all patients to receive all the recommended care for which they are eligible. An aggregated “all or nothing” measurement approach to monitoring multiple publicly reported process-of-care measures for heart failure, acute myocardial infarction, pneumonia and surgical patients is trending positively.
Mortality 2010 – 2011
98
96
100
86Q1 Q2
2010 2011
Q3 Q4 Q1 Q2 Q3 Q4
94
92
90
88
Percent of Patients
Cleveland Clinic performanceCleveland Clinic target
*Source: Performance Accelerator Suite Program maintainedby the University HealthSystem Consortium (UHC)https://www.uhc.edu/
0.8
1.0
0.6
0.0Q1 Q2
2010 2011
Q3 Q4 Q1 Q2 Q3 Q4
0.4
0.2
O/E Ratio
Cleveland Clinic*UHC academic medicalcenter 50th percentile*

RespiratoryInstitute 5555
Patient Safety Indicators (PSIs) 2011
ClevelandClinicestablisheda2011targetICUsurveillancerateof1.33centralline-associatedbloodstreaminfections(CLABSIs)per1,000central line days, with the goal of reducing our rate by an additional 50 percent over the 2010 results. This 2011 target was met by the end of the year.
Cleveland Clinic focused on reducing the incidence of10AgencyforHealthcareResearchandQualityPSIs.ClevelandClinicachievedareductionofmorethan60percentinthetotalnumberofthesePSIsin 2011 through a combination of clinical and documentation improvement activities.
Central Line-Associated Bloodstream Infections — ICUs 2010 – 2011
3
4
2
0Q1 Q2
2010 2011
Q3 Q4 Q1 Q2 Q3 Q4
1
Rate per 1,000 Line Days
Cleveland Clinic performanceCleveland Clinic target
*PSI3StageIII/IVPressureUlcers,PSI6IatrogenicPneumothorax,PSI7CLABSI,PSI8Post-OpHipFracture,PSI9Post-OpHemorrhage/Hematoma,PSI11Post-OpRespiratoryFailure,PSI12Post-OpPEorDVT,PSI13Post-OpSepsis,PSI14Post-OpWoundDehiscence,PSI15AccidentalPuncture/Laceration
150
200
100
0Jan Mar May July Sep Nov
50
Number of PSIs*

Outcomes 20115656
Improving Quality, Safety and the Patient Experience
Hospital-Acquired Pressure Ulcers — ICUs 2010 – 2011
Patient Falls — Stepdown Units 2010 – 2011
Hospital-acquiredpressureulcersinClevelandClinicICUpatientswerebelowthenationalaverage in 2010 and 2011.
Falls in Cleveland Clinic stepdown unit patients were below the national average for most of 2010 and 2011. In 2011, Cleveland Clinic supplemented proactive falls- reduction strategies with after-event huddles to evaluate causality and develop prevention strategies.
*TheNationalDatabaseofNursingQualityIndicators®(NDNQI®)isownedbythe American Nurses Association. The database collects and evaluates unit-specific nurse-sensitive data from hospitals domestically and globally with over 1800hospitalsparticipating.ThecomparisondatarepresentedherearebasedonathirdofallhospitalsintheU.S.participating.© 2012 American Nurses Association,AllRightsReserved.https://www.nursingquality.org/
12
14
8
10
0Q1 Q2
2010 2011
Q3 Q4 Q1 Q2 Q3 Q4
6
4
2
Pressure Ulcer Prevalence (%)
Cleveland Clinic ICUsBenchmark: NDNQI* ICUs
3.0
4.0
2.0
3.5
2.5
0Q1 Q2
2010 2011
Q3 Q4 Q1 Q2 Q3 Q4
1.5
1.0
0.5
Fall Rate per 1,000 Patient Days
Cleveland Clinic Stepdown UnitsBenchmark: NDNQI* Stepdown Units

RespiratoryInstitute
Medical Emergency Team Event Volume* 2009 – 2011
Critical Response Outcomes
Percent of Medical Emergency Team Events Resulting in ICU Transfer 2009 – 2011
MedicalEmergencyTeams(METs)bringcriticalcareexperiencetopatientsacrossthehospitalandprovideearlyinterventionthatcanpreventunplannedtransferstoICUs.AsadultMETactivationsincreasedfrom2009through2011,post-eventadultICUtransfersdecreased.
3,000
2,500
0
2,000
1,500
1,000
500
Events
2009 2010 2011
*Excluding events originating in ORs and ICUs
40
30
0
20
10
Percent
2009 2010 2011
5757

Outcomes 20115858
Improving Quality, Safety and the Patient Experience
HCAHPS Hospital Domain Scores 2010 – 2011
HCAHPS Rate and Recommend Hospital 2010 – 2011
Patient Experience — Cleveland Clinic
100
80
0
60
40
20
Percent (Best Response)
DischargeInformation Given
% yes
Doctor Communication
Nurse Communication
PainManagement
RoomClean
New MedicationsCommunication
Responsivenessto Needs
Quiet atNight
% always(Options: always, usually, sometimes, never)
“PatientsFirst”istheguidingprincipleofClevelandClinic,whichwasamongthe firstmajoracademicmedicalcenterstomakeimprovingthepatientexperienceastrategicgoal.TheOfficeofPatientExperiencecollaborateswithphysicianandnursingleadership to establish best practices and implement standardized protocols that ensure delivery of patient-centered care. Campus-wideHCAHPSsurveyresultsaretrendingfavorablyineverydomain.
TheHospitalConsumerAssessmentofHealthcareProvidersandSystems(HCAHPS)surveyisthestandardnationaltoolformeasuringpatients’perspectivesofhospitalcare.Resultsareavailableathospitalcompare.hhs.gov.
100
80
60
0
40
20
Percent (Best Response)
Rate Hospital Would Recommend Hospital
% 9 or 10(0 – 10 scale)
% “definitely yes” Cleveland Clinic 2010*Cleveland Clinic 2011*
National Average 7/1/2010 – 6/30/2011
*Source: Press Ganey, a national hospital survey vendor
Source: hospitalcompare.hhs.gov.

5959RespiratoryInstitute
About Cleveland Clinic
Overview
Cleveland Clinic is a nonprofit multispecialty academic medical center that integrates clinical and hospital care with research and education. Acrossthehealthsystem,2,800ClevelandClinicphysiciansandscientistspractice in 120 medical specialties and subspecialties, annually recording morethan4.6millionphysicianvisitsandnearly188,000surgeries.Patientscomefortreatmentfromeverystateandfrommorethan 125countries annually. ClevelandClinic’smaincampus,with50buildingson180acresinCleveland, Ohio, includes a 1,400-bed hospital, outpatient clinic, specialty institutes, and supporting labs and facilities. The hospital currently has the highestCMScase-mixindexinAmerica.ClevelandClinicalsooperates18family health centers, eight community hospitals, one affiliate hospital, a rehabilitation hospital for children, Cleveland Clinic Florida, Cleveland Clinic LouRuvoCenterforBrain HealthinLasVegas,ClevelandClinicCanada,andSheikhKhalifaMedicalCity.ClevelandClinicAbuDhabi(UnitedArabEmirates),amultispecialtycarehospitalandclinic,isscheduledtoopenin2013.With41,000employees,ClevelandClinicisthesecondlargestemployerinOhioandisresponsibleforanestimated$9billionofeconomicactivity every year.
The Cleveland Clinic Model
Cleveland Clinic was founded in 1921 by four physicians who had served in World War I and hoped to replicate the organizational efficiency of military medicine. The organization has grown through the years by adhering to the model set forth by the founders. All Cleveland Clinic staff physicians receive a straight salary with no bonuses or other financial incentives. The hospital and physicians share a financial interest in controlling costs, and profits are reinvested in research and education. In 2007, Cleveland Clinic restructured its practice, bundling all clinical specialties into integrated practice units called institutes. An institute combines all the specialties surrounding a specific organ or disease system under a single roof. Each institute has a single leader and focuses the energies of multiple professionals on the patient. Institutes are improving the patient experience at Cleveland Clinic.

Outcomes 20116060
Cleveland Clinic Lerner Research Institute AttheLernerResearchInstitute,hundredsofprincipalinvestigators,projectscientists,researchassociatesand postdoctoral fellows are involved in laboratory-based, translational and clinical research. Total research expenditures from external and internal sources exceeded $240millionin2010.Researchprogramsincludecardiovascular, cancer, neuralgic, musculoskeletal, allergic and immunologic, eye, metabolic, and infectious diseases.
Cleveland Clinic Lerner College of Medicine Celebrating its 10th anniversary in 2012, the Lerner College ofMedicineofCaseWesternReserveUniversityisknownfor its small class size, unique curriculum and full-tuition scholarshipsforallstudents.Theprogramgraduated31students as physician investigators in 2011.
Graduate Medical Education In2011,nearly1,800residentsandfellowstrainedatCleveland Clinic and Cleveland Clinic Florida, the most ever hosted by Cleveland Clinic and part of a continuing upward trend.
U.S.News & World Report Ranking Cleveland Clinic is consistently ranked among the top hospitals in America by U.S.News & World Report, and our heart and heart surgery program has been ranked No. 1 since 1995.
For more information about Cleveland Clinic, please visit clevelandclinic.org.
About Cleveland Clinic

6161RespiratoryInstitute
prescriptions and review test results and medications from theirpersonalcomputers.MyChartprovidesalinktoMicrosoftHealthVault,afreeonlineservicethathelpspatientssecurelygather and store health information. It connects to Cleveland Clinic’s social media and Internet site, currently the most visited hospital website in America. For more information, visit clevelandclinic.org/mychart.
Critical Care Transport Worldwide Cleveland Clinic’s critical care transport team and fleet of mobileICUvehicles,helicoptersandfixed-wingaircraftservecritically ill and highly complex patients across the globe.
ToarrangeatransferforSTEMI(STelevatedmyocardialinfarction),acutestroke,ICH(intracerebralhemorrhage),SAH(subarachnoidhemorrhage)oraorticsyndrome,calltoll-free877.379.CODE(2633).
Forallothercriticalcaretransfers,call216.444.8302or800.553.5056.
CME Opportunities: Live and Online Cleveland Clinic’s Center for Continuing Education operates oneofthelargestandmostsuccessfulCMEprogramsinthecountry.TheCenter’swebsite(ccfcme.com)isaneducational resource for healthcare providers and the public. Available24/7,ithousesprogramsthatcovertopicsin30areas – if not from A to Z, at least from Allergy to Wellness – with a worldwide reach. Among other resources, the websitecontainsavirtualtextbookofmedicine(DiseaseManagementProject)andmyCME,asystemforphysicianstomanagetheirCMEportfolios.Livecourses,however,remainthebackboneoftheCenter’sCMEoperation.Mostlive courses are held in Cleveland, but outreach plans are under way. In 2011, the Center offered 15 simultaneous coursesatArabHealth,amajorworldhealthcareforum.
Referring Physician Center and Hotline
ClevelandClinic’sReferringPhysicianCenterhasestablished a 24/7 hotline – 855.REFER.123(855.733.3712) – to streamline access to our array of medicalservices.ContacttheReferringPhysicianHotlinefor information on our clinical specialties and services, to schedule and confirm patient appointments, for assistance in resolving service-related issues, and to connect with Cleveland Clinic specialists.
Remote Consults
Online medical second opinions from Cleveland Clinic’s MyConsultareparticularlyvaluableforpatientswhowishto avoid the time and expense of travel. Cleveland Clinic offers online medical second opinions for more than 1,000 life-threatening and life-altering diagnoses. For more information, visit clevelandclinic.org/myconsult, email [email protected], ext.43223.
Request Medical Records 216.444.2640or800.223.2273,ext.42640
Track Your Patient’s Care Online DrConnect offers referring physicians secure access to their patients’ treatment progress while at Cleveland Clinic. To establish a DrConnect account, visit clevelandclinic.org/drconnect or email [email protected].
Medical Records Online Cleveland Clinic continues to expand and improve electronic medicalrecords(EMRs)toprovidefaster,moreefficientand accurate care by sharing patient data through a highlysecurenetwork.PatientsusingMyChartcanrenew
Resources


© The Cleveland Clinic Foundation 2012

9500 Euclid Avenue, Cleveland, OH 44195 ClevelandClinic.org

63
