2011diagnostic methods in pulmonology methods in pulmonolo… · •any obvious chest or spine...
TRANSCRIPT

1
Diagnostic methods in pulmonology
Dr. A.Torossian, M.D., Ph. D.Department of Respiratory Diseases
History of disease
• Chief complaints• Co morbidities• Past history• Family history• Social status• Occupational history• Risk factors

2
Major pulmonary symptoms
• Cough• Sputum (hemoptysis, hemoptoe)• Dyspnea• Chest pain
Other important complaints
• Intoxication syndrome-fatigue, loss of appetite, weight loss, temperature, profuse sweating
• Other symptoms- mialgia, arthralgia, headache, nausea, sore throat, rhinitis, skin eruptions, diarrhea, urinary symptoms, symptoms of malignancy in other organ, swelling of the ankles, etc.

3
Co morbidities
• Other known diseases-diabetes mellitus, heart failure, resent operation, transplantations, immunologic disorder, HIV status, neoplastic disease
• Symptoms suggesting involvement of other system
• Drugs received
Past history
• Childhood• Recurrent diseases• Previous treatment-immunosuppressive
drugs, radiotherapy, antibiotics, hormones, operations, etc.

4
Family history
• Allergy• Contagious disease• Tuberculosis• Cystic fibrosis• Cancer of the lung
Social status
• Poverty-malnutrition, living in a crowded place
• Prison• Nursing home and other social institutions• Military boarding house, campus, etc.

5
Occupational history
• Toxic gases, fumes, air pollution• Radiation• Infections• Animals, birds, cattle, rats, ticks
Risk factors
• Smoking-package/years• Alcoholism• Drug abuse
6
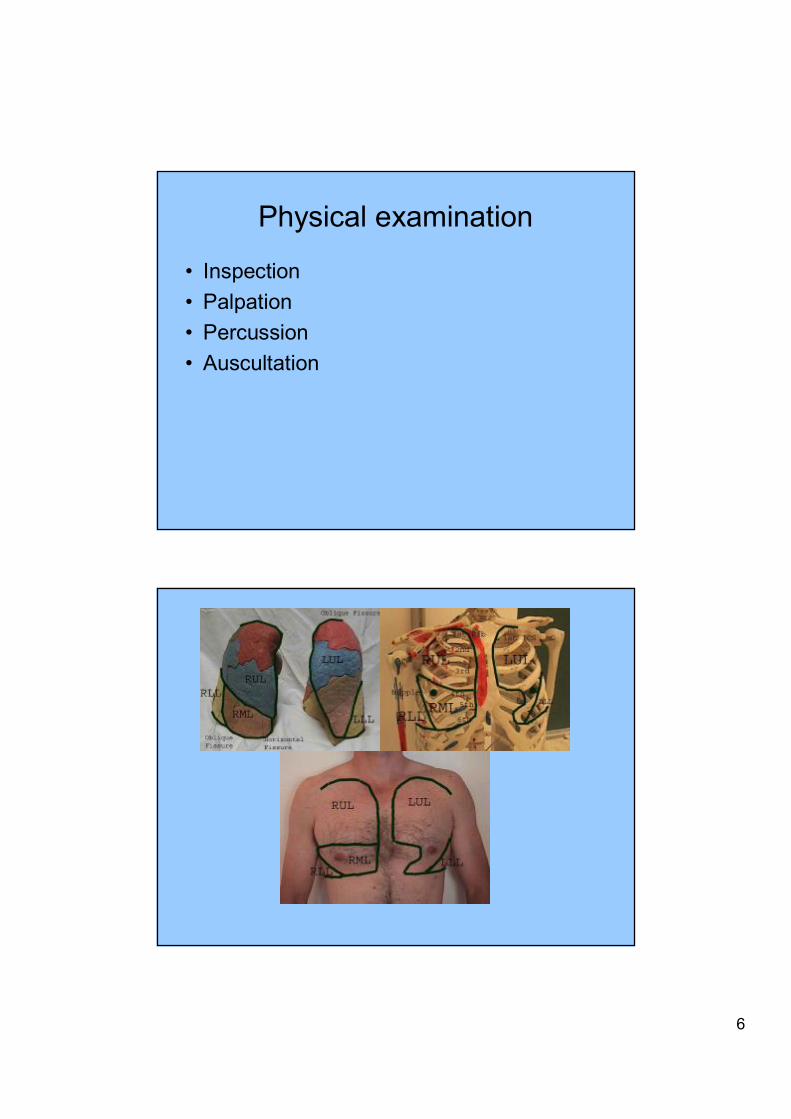
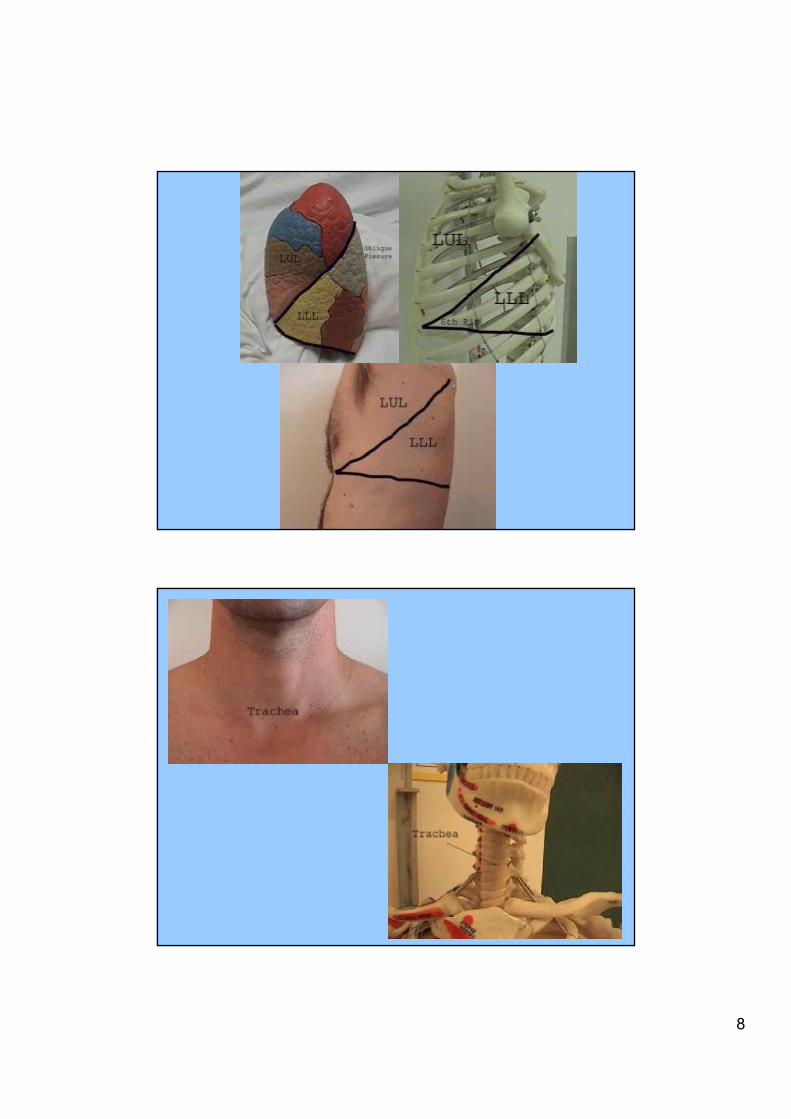
Physical examination
• Inspection• Palpation• Percussion• Auscultation

7
8

9
Inspection
• General comfort and breathing pattern of the patient. Are the breaths regular and deep?
• Use of accessory muscles of breathing (e.g. scalenes, sternocleidomastoids). Their use signifies some element of respiratory difficulty.
• Color of the patient, in particular around the lips and nail beds.

10
• The position of the patient. Those with extreme pulmonary dysfunction will often sit up-right. In cases of real distress, they will lean forward, resting their hands on their knees in what is known as the tri-pod position

11
• Breathing through pursed lips-often seen in cases of emphysema.
• Ability to speak. At times, respiratory rates can be so high and/or work of breathing so great that patients are unable to speak in complete sentences. If this occurs, note how many words they can speak (i.e. the fewer words per breath, the worse the problem!).
• Any audible noises associated with breathing as occasionally, wheezing or the gurgling caused by secretions in large airways are audible to the "naked" ear.
• Any obvious chest or spine deformities. These may arise as a result of chronic lung disease (e.g. emphysema), occur congenitally, or be otherwise acquired. In any case, they can impair a patient's ability to breathe normally.
1.Barrel chest: associated with emphysema and lung hyperinflation
2.Kyphosis

12
Palpation:
• Accentuating normal chest excursion• Tactile Fremitus• Lung consolidation: Consolidation occurs when the normally air filled lung parenchyma becomes engorged with
fluid or tissue, most commonly in the setting of pneumonia. If a large enough segment of parenchyma is involved, it can alter the transmission of air and sound. In the presence of consolidation, fremitus becomes more pronounced.
• Pleural fluid

13
Percution• striking a surface which covers an air-filled structure (e.g.
normal lung) will produce a resonant note• while repeating the same maneuver over a fluid or tissue
filled cavity generates a relatively dull sound. If the normal, air-filled tissue has been displaced by fluid (e.g. pleural effusion) or infiltrated with white cells and bacteria (e.g. pneumonia), percussion will generate a deadened tone.
• Alternatively, processes that lead to chronic (e.g. emphysema) or acute (e.g. pneumothorax) air trapping in the lung or pleural space, respectively, will produce hyper-resonant (i.e. more drum-like) notes on percussion.

14
Auscultation

15

16
1) Are the breath sounds increased, normal, or decreased?2) Are there any abnormal or adventitious breath sounds?
wheezebronchial
mediastinal crunch (Hamman's sign)
pleural rub
stridorvesicular
rhonchibronchovesicular
crackles (rales)Absent / decreasedtracheal
AdventitiousAbnormalNormal

17
1. Normal Breath Sounds
• organized into categories based on their intensity, pitch, location, and inspiratory to expiratory ratio.
• created by turbulent air flow• expiratory breath sounds are quieter
than inspiratory breath sounds
Tracheal Breath Sound
• very loud and relatively high-pitched• The inspiratory and expiratory sounds
are more or less equal in length.• can be heard over the trachea which is
not routinely auscultated..

18
Vesicular Breath Sound
• is the major normal breath sound and is heard over most of the lungs.
• The inspiratory sounds are longer than the expiratory sounds.
• may be harsher in patients who have thinner chest walls
• may be softer if the patient is frail, elderly, obese, or very muscular
Bronchial Breath Sound• very loud, high-pitched and sound close to
the stethoscope• the expiratory sounds are longer than the
inspiratory sounds• If these sounds are heard anywhere other
than over the manubrium, it is usually an indication that an area of consolidation exists (ie space that usually contains air now contains fluid or solid lung tissue)

19
Bronchovesicular Breath Sound
• The inspiratory and expiratory sounds are equal in length.
• best heard in the 1st and 2nd ICS (anterior chest) and between the scapulae (posterior chest) - i.e. over the mainstem bronchi
• when these are heard anywhere other than over the mainstem bronchi, they usually indicate an area of consolidation.
Abnormal Breath Sounds
• Absent or Decreased Breath Sounds:atelectasis, asthma, pleural effusion, etc.
• Bronchial Breath Sounds in Abnormal Locations: occur over consolidated areas. Further testing of egophony and whispered petroliloquy may confirm your suspicions.

20
Adventitious Breath Sounds
Crackles (Rales)• discontinuous, nonmusical, brief
sounds heard more commonly on inspiration
• fine (high pitched, soft, very brief) or coarse (low pitched, louder, less brief)
Wheeze• continuous, high pitched, hissing
sounds heard normally on expiration but also sometimes on inspiration
• produced when air flows through airways narrowed by secretions, foreign bodies, or obstructive lesions.

21
Rhonchi• low pitched, continuous, musical
sounds that are similar to wheezes • usually imply obstruction of a larger
airway by secretions
Stridor• an inspiratory musical wheeze heard
loudest over the trachea during inspiration. Stridor suggests an obstructed trachea or larynx and therefore constitutes a medical emergency that requires immediate attention.

22
Pleural Rub• creaking or brushing sounds produced when
the pleural surfaces are inflamed or roughened and rub against each other. They may be discontinuous or continuous sounds.
• They can usually be localized at a particular place on the chest wall and are heard during both the inspiratory and expiratory phases.
Mediastinal Crunch (Hamman’s sign)• crackles that are synchronized with the
heart beat and not respiration. They are heard best with the patient in the left lateral decubitus postion.
• As with stridor, mediastinal crunches should be treated as medical emergencies.
23
Physical examination of other systems
Sometimes the lung problem is a result of a primary disease in another system
• Heart rhythm, murmurs, swellings, ascites, enlarged liver, enlarged lymph nodes (especially supraclavicular area)
• Local status -urological, gynecological, etc.
Laboratory methods• Clinical laboratory- Biochemical l Methods: blood tests,
enzyme tests, mineral content tests, glucose, urea, etc. -in blood plasma, in pleural effusion, liquor, urine....ESR (erythrocyte sedimentation rate), etc.
• Microbiology- Gram staining, cultures- bacteria, fungi, viruses, radiometric test- Bactec
• Immunology-ELISA, complement fixation test, immune status etc.
• Cytology-tumor cells in sputum, pleural effusion, bronchial secretion
• Genetics-cystic fibrosis

24
Imaging methodsX-ray imaging: TV-scopy, chest radiograph/chest X-ray (CXR), Classic Tomography, Computed tomography (CT), etc.Ultrasound imagingRadioisotopes (scintigraphy)Nuclear Magnetic Resonance Imaging (MRI)Pozitron Emmision Tomography (PET)Pulmonary angiography
25
Pulmonary Function Tests: Spirometry
• Spirometry (measuring of breath) is the most common of the Pulmonary Function Tests (PFTs), measuring lung function, specifically the measurement of the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled.
• Spirometry is an important tool in diagnosing COPD, asthma, pulmonary fibrosis, etc.
• Forced Vital Capacity (FVC)-the volume of air that can forcibly be blown out after full inspiration, measured in liters. FVC is the most basic maneuver in spirometry tests.
• Forced Expiratory Volume in 1 second (FEV1)-Average values for FEV1 in healthy people depend mainly on sex and age. Values of between 80% and 120% of the average value is considered normal.
• FEV1/FVC ratio (FEV1%)• Peak Expiratory Flow (PEF)-the maximal flow (or speed) achieved during
the maximally forced expiration initiated at full inspiration, measured in liters per minute.
• Diffusion capacity (DLCO)
A modern PC based spirometer printout

26

27
Other functional tests
• Bronchodilator test• Bronchoprovocation testing• Monitoring PEF
Invasive methods of diagnosis
• Bronchoscopy• Percutaneous fine-needle biopsy• Cutting-needle biopsy• Video-assisted thoracoscopic surgery
(VATS) • Mediastinoscopy• Open lung biopsy• Biopsy of other sites
28
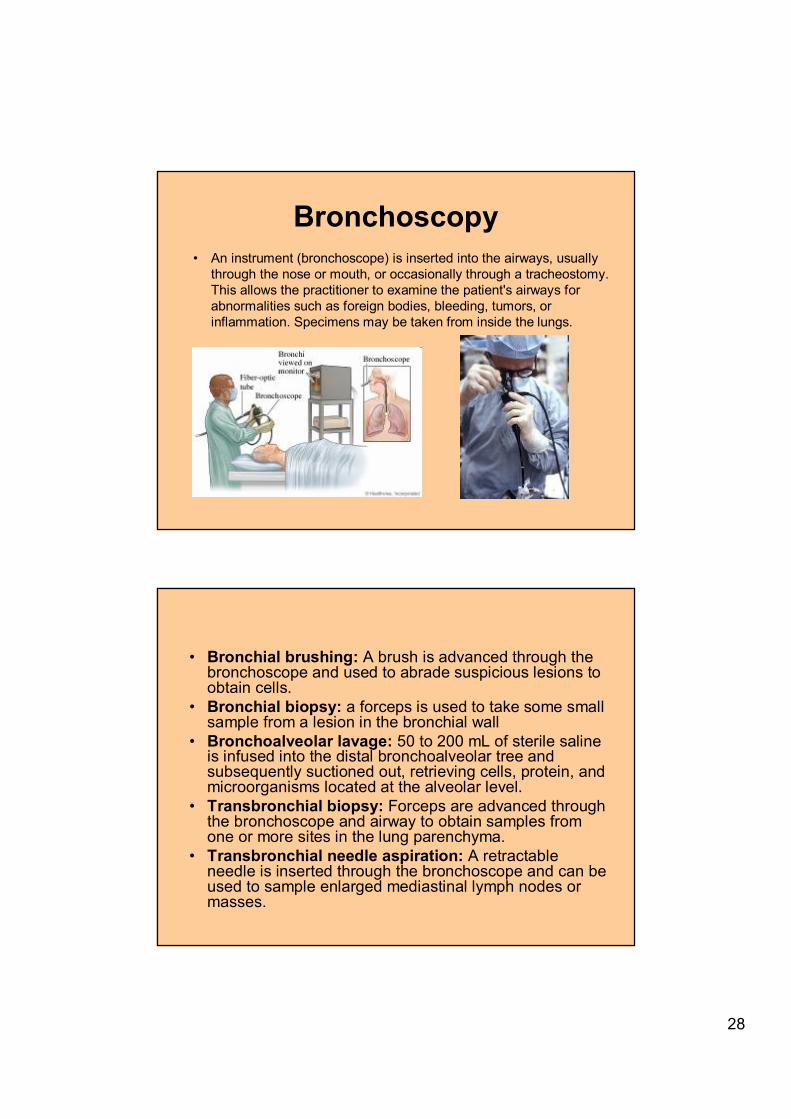
Bronchoscopy• An instrument (bronchoscope) is inserted into the airways, usually
through the nose or mouth, or occasionally through a tracheostomy. This allows the practitioner to examine the patient's airways for abnormalities such as foreign bodies, bleeding, tumors, or inflammation. Specimens may be taken from inside the lungs.
• Bronchial brushing: A brush is advanced through the bronchoscope and used to abrade suspicious lesions to obtain cells.
• Bronchial biopsy: a forceps is used to take some small sample from a lesion in the bronchial wall
• Bronchoalveolar lavage: 50 to 200 mL of sterile saline is infused into the distal bronchoalveolar tree and subsequently suctioned out, retrieving cells, protein, and microorganisms located at the alveolar level.
• Transbronchial biopsy: Forceps are advanced through the bronchoscope and airway to obtain samples from one or more sites in the lung parenchyma.
• Transbronchial needle aspiration: A retractable needle is inserted through the bronchoscope and can be used to sample enlarged mediastinal lymph nodes or masses.

29
Percutaneous fine-needle biopsy
Video-assisted thoracoscopic surgery (VATS)a type of thoracic surgery performed using a small video camera that
is introduced into the patient's chest via a scope.

30
Other methods• Arterial blood gas (ABG)• ECG• Echocardiography• Skin tests for allergy- A small amount of a
suspected allergen is placed on or below the skin to see if a reaction develops.
• Skin prick test- placing a drop of a solution containing a possible allergen on the skin, and a series of scratches or needle pricks allows the solution to enter the skin
• Intradermal test-a small amount of the allergen solution is injected into the skin
• Skin patch test- the allergen solution is placed on a pad that is taped to the skin for 24 to 72 hours.

31