2013 cancer program annual report - johns hopkins hospital · ... (suburban hospital, sibley...
TRANSCRIPT

2013 ANNUAL REPORT
CancerProgram
N O V E M B E R 2 0 1 3

2
2013 has been a memorable year for Howard County General Hospital (HCGH). We have been celebrating 40 years of excellence in health care; we transitioned to Epic, a single, integrated electronic medical record (EMR) that will improve patient care throughout the Johns Hopkins Medicine (JHM) system; and we are saying farewell to Vic Broccolino, our president and CEO of 24 years.
The HCGH Cancer Program has seen many changes and advances during the past year. The most challenging but rewarding change was the transition to Epic, an advance that will literally change the way we care for our cancer patients as well as all other patients. All care providers now have access to vital patient information whenever and wherever they receive treatment throughout the Johns Hopkins Medicine system. In addition, Epic users can access and share records of patients at any hospital where Epic is installed, nationwide. The switch to Epic EMR has improved three major processes in the day-to-day operations of the Cancer Registry: • For abstracting new cancer cases into the registry database, a significant amount of the diagnostic and therapeutic data, as well as data scanned in office notes, H&P’s, diagnostic
imaging and pathology reports from other Johns Hopkins facilities, is readily available to registry staff. This has greatly reduced the number of letters and calls required to complete the abstracts. • Epic has also streamlined the process of preparing for cancer conferences. Needed reports can most often be found without having to call or fax requests to physician offices. Being able to rapidly identify the location of a patient’s outside diagnostic studies provides staff with additional time to obtain the slides and images requested for review. • Follow-up information from physician offices and other facilities is available online. This allows registry staff to obtain more accurate and detailed information on the patient’s current status and any recurrences or additional treatments they may have received. It has reduced the number of follow-up letters being sent to physician offices and other facilities.
Biomedical discovery and research is one of six priorities in the Johns Hopkins Medicine five-year strategic plan, “Leading the Change.” This year, HCGH established a research office that is part of the JHM research network – Capital Area Research (CAPRES) – to develop and nurture research in the three JHM community hospitals (Suburban Hospital, Sibley Memorial Hospital and HCGH) and to expand and coordinate research that was historically based at The Johns Hopkins Hospital. Cancer related studies will be coming in the future.
The Breast Center at HCGH is working to expand its existing range of multidisciplinary breast care services by more closely integrating plastic/reconstructive services and increasing its patient capacity with the addition of a breast health nurse practitioner. (See Focus on Breast Cancer, Page 9, for information about our breast cancer programs.)
In April, the Claudia Mayer Cancer Resource Center (CMCRC) celebrated 15 years of providing support for men and women living with and surviving cancer. To meet the needs of busy care givers and cancer patients, CMCRC has added monthly care giver and patient-focused support group meet-ings on Saturdays. CMCRC also collaborated with the Sidney Kimmel Comprehensive Cancer Center and other JHM system entities to provide a conference that focused on survivorship. Additionally, HCGH offered a Continuing Medical Education program in June with a focus on palliative care.
As we move forward into the next decade of excellent patient care, the HCGH Cancer Program looks forward to leading the change in how we treat, cure and comfort our cancer patients.
C h a i r p e r s o n ’ s R e p o r t
Sally Cheston, M.D. Radiation Oncology, Cancer Committee Chair
Sally Cheston, M.D. Radiation Oncology, Cancer Committee Chair

3
C a n c e r C o n f e r e n c e R e p o r tCancer conferences improve the care of patients with cancer by providing multidisciplinary treatment planning and contribute to physician and allied medical staff education.
The HCGH Cancer Program currently offers four cancer conferences (see chart, below). Cases are presented at a point when patient care management can be directly influenced by the discussion. Each discussion includes the patient's medical history; physical findings; diagnostic, pathologic and operative findings; staging; and treatment options. Discussions also include national evidence-based guidelines, protocol updates, literature reviews and presentation of cancer registry data.
General
Conference Breast Conference
Thoracic Conference
Genito-Urinary Conference
All Conferences Combined
Day 2nd and 4th Friday
Every Tuesday
3rd Friday
1st Tuesday
Time 12:15 p.m. 7:30 a.m. 7:30 a.m. Noon
Location: Medical Pavilion Suite G010 Suite G010 Suite G010 Suite G030
Number of Meetings 20 47 10 10 87
Attendance by Surgeon 6 (30%) 47 (100%) 9 (90%) 10 (100%) 72 (83%)
Attendance by Diagnostic Radiology 11 (55%) 47 (100%) 7 (70%) N/A* 65 (84%)*
Attendance by Pathology 20 (100%) 47 (100%) 10 (100%) N/A* 77 (100%)*
Attendance by Medical Oncology 20 (100%) 47 (100%) 10 (100%) 8 (80%) 85 (98%)
Attendance by Radiation Oncology 18 (90%) 47 (100%) 10 (100%) 10 (100%) 83 (95%)
Total Attendance 236 793 109 122 1260
Average Attendance 12 17 11 12 14 Total Number of Patients Discussed 80 302 44 34 460
Average Number of Cases Per Meeting 4 6 4 3 5
Site # of Cases Site # of Cases Lung 19 Male Genital 3
Hodgkin/NHL 17 Unknown / Non-malignant 5 Colorectal 8 H&N 2 Breast 8 CNS 1 Other GI 8 Connective Tissue 1 GYN 3 Hematopoietic 5
TOTAL 80
All conferences are coordinated through the Oncology Data Office. For additional information, contact Sheryl Daugherty at [email protected] or 410-740-7956; or Sharon Tunney at [email protected] or 410-720-8515.
General
Conference Breast Conference
Thoracic Conference
Genito-Urinary Conference
All Conferences Combined
Day 2nd and 4th Friday
Every Tuesday
3rd Friday
1st Tuesday
Time 12:15 p.m. 7:30 a.m. 7:30 a.m. Noon
Location: Medical Pavilion Suite G010 Suite G010 Suite G010 Suite G030
Number of Meetings 20 47 10 10 87
Attendance by Surgeon 6 (30%) 47 (100%) 9 (90%) 10 (100%) 72 (83%)
Attendance by Diagnostic Radiology 11 (55%) 47 (100%) 7 (70%) N/A* 65 (84%)*
Attendance by Pathology 20 (100%) 47 (100%) 10 (100%) N/A* 77 (100%)*
Attendance by Medical Oncology 20 (100%) 47 (100%) 10 (100%) 8 (80%) 85 (98%)
Attendance by Radiation Oncology 18 (90%) 47 (100%) 10 (100%) 10 (100%) 83 (95%)
Total Attendance 236 793 109 122 1260
Average Attendance 12 17 11 12 14 Total Number of Patients Discussed 80 302 44 34 460
Average Number of Cases Per Meeting 4 6 4 3 5
Site # of Cases Site # of Cases Lung 19 Male Genital 3
Hodgkin/NHL 17 Unknown / Non-malignant 5 Colorectal 8 H&N 2 Breast 8 CNS 1 Other GI 8 Connective Tissue 1 GYN 3 Hematopoietic 5
TOTAL 80
Case Distribution for 2012 General Conferences
*Representatives from Diagnostic Imaging and Pathology are not required to attend the GU conferences. Therefore, their average attendance is calculated on a total of 77 meetings.
,

4
The Oncology Data Office at HCGH, a part of the Health Information Management Department, collects data on all cancer patients diagnosed and/or treated at the hospital. Hospital-based cancer registries serve as the nation’s primary source of oncology statistics. This comprehensive collection of patient data facilitates comparisons between individual facilities and the state, or the nation as a whole.
As with all cancer registries, the role of the Oncology Data Office at HCGH continues to grow and evolve. With advances in cancer-related research, technology and treatments, the registry collects more detailed information than ever before. Information collected and analyzed includes demo-graphic, personal and family histories, risk factors, diagnostic procedures, site and histology, tumor markers, prognostic indicators, staging, treatment, follow-up and survival data for each case.
In 2012, 609 analytic cases were accessioned to HCGH's registry database (table 1, page 5). Over the past year, the number of new breast cancer cases increased by 11.5 percent from 157 cases to 175, and remained the most frequently seen primary site at HCGH, making up 28.7 percent of the entire analytic case load, and 46 percent of the female analytic caseload (table 2, page 6). The second most frequently seen primary site in 2012 was lung with 73 cases (12 percent of the total caseload). This represents a decrease of 17 percent from the 88 lung cancer cases accessioned in 2011.
The other top primary sites seen at the hospital were colorectal, melanoma and non-Hodgkin lymphoma (NHL). The number of colorectal cancer cases increased by 2.9 percent, from 69 cases in 2011 to 71 in 2012. Melanoma cases decreased from 39 to 34 over the past year. This is a decrease of 12.8 percent. NHL cases decreased from 37 cases in 2011 to 29 cases in 2012. This is a decrease of 21.6 percent. For 2012, colorectal cancer cases made up 11.7 percent of the total analytic caseload. Melanoma was 5.6 percent and NHL was 4.8 percent of the analytic caseload.
When compared to state and national statistics (table 3, page 7), HCGH continued to see female breast cancer as a significantly higher percentage of its total caseload. The incidence of colorectal and lymphoma cases were also higher at HCGH than for the state of Maryland or the nation. The incidence of melanoma was higher than that of the U.S., but slightly lower than for the state of Maryland. The incidence of lung cancer seen at HCGH was at a lower rate than both the state and nation.
Individual registries help hospital physicians and administrators track quality of care and treatment by monitoring compliance with national evidence-based guidelines. Registry data is also used by the hospital for cancer conference presentations, administrative reports, to evaluate staffing and equipment needs, and guide the development of educational and screening programs for both patients and the community.
The Oncology Data Office staff also compiles the required documentation to insure the HCGH oncology program’s compliance with all standards established by the American College of Surgeons (ACoS) Commission on Cancer (CoC) to maintain its accreditation as a Comprehensive Community Cancer Program (CCCP).
C a n c e r R e g i s t r y R e p o r tFor more information about the HCGH Cancer Registry, please call 410-740-7956.

5
Primary Site Cases M F 0 I II III IV N/A UNK
Oral Cavity, Pharynx 9 8 1 2 4 0 1 2 0 0Tongue 4 4 0 2 1 0 0 1 0 0Salivary Gland 1 1 0 0 1 0 0 0 0 0Floor of Mouth 1 1 0 0 0 0 0 1 0 0Gum & Other Parts of Mouth 2 1 1 0 2 0 0 0 0 0Tonsil 1 1 0 0 0 0 1 0 0 0
Digestive Organs 140 68 72 1 24 24 34 44 3 10Esophagus 6 3 3 0 2 2 0 2 0 0Stomach 17 11 6 0 3 0 3 6 2 3Small Intestine 7 3 4 0 0 0 4 2 0 1Colon 46 19 27 0 12 10 14 10 0 0Rectosigmoid 8 5 3 0 1 1 4 2 0 0Rectum 17 12 5 1 1 3 5 5 0 2Anus & Anal Canal 5 1 4 0 1 1 2 1 0 0Liver & Intrahep Bile Ducts 5 3 2 0 2 0 1 2 0 0Gallbladder 1 0 1 0 0 0 0 1 0 0Other Biliary 4 3 1 0 0 1 0 0 1 2Pancreas 23 9 14 0 4 6 0 11 0 2Peritoneum, Omentum & Mesentery 1 0 1 0 0 0 0 1 0 0
Respiratory System 75 33 42 0 11 10 12 39 0 3Larynx 2 1 1 0 0 0 0 1 0 1Lung & Bronchus 73 32 41 0 11 10 12 38 0 2
Skin (Excludes Squamous & Basal Cell) 35 19 16 19 11 1 3 0 0 1Melanoma 34 19 15 19 11 1 3 0 0 0Other Non-Epithelial Skin 1 0 1 0 0 0 0 0 0 1
Soft Tissue 1 1 0 0 0 0 1 0 0 0
Breast 175 3 172 44 67 44 12 6 2 0
Female Genital Organs 18 0 18 0 8 0 4 2 0 4Cervix 3 0 3 0 1 0 0 1 0 1Uterus 11 0 11 0 6 0 2 0 0 3Ovary 4 0 4 0 1 0 2 1 0 0
Male Genital Organs 27 27 0 0 11 12 2 2 0 0Prostate 22 22 0 0 8 12 0 2 0 0Testis 5 5 0 0 3 0 2 0 0 0
Urinary Tract 35 27 8 17 8 2 4 2 0 2Urinary Bladder 24 22 2 17 4 1 1 0 0 1Kidney & Renal Pelvis 11 5 6 0 4 1 3 2 0 1
Brain / Other Nervous System 19 6 13 0 0 0 0 0 19 0Meninges/Brain/CNS Benign & Borderline 15 3 12 0 0 0 0 0 15 0Brain, Malignant 4 3 1 0 0 0 0 0 4 0
Endocrine System 17 7 10 0 8 3 3 1 1 1Thyroid 16 7 9 0 8 3 3 1 0 1Thymus 1 0 1 0 0 0 0 0 1 0
Lymphoma 35 19 16 0 6 9 3 16 0 1Hodgkin Lymphoma 6 1 5 0 1 3 0 2 0 0Non-Hodgkin Lymphoma 29 18 11 0 5 6 3 14 0 1
Myeloma 4 3 1 0 0 0 0 0 4 0
Leukemia 6 5 1 0 0 0 0 0 6 0Lymphocytic 1 1 0 0 0 0 0 0 1 0Myeloid & Monocytic 5 4 1 0 0 0 0 0 5 0
Unknown Primary Site 14 6 8 0 0 0 0 0 14 0
ALL SITES 609 232 377 83 159 105 77 114 49 22
Abbreviations: M=Male, F=Female, UNK=Unknown or Unstageable, N/A=Not Applicable *Carcinoma in situ/CIN-III of the cervix is no longer reported nationally or to the state
HCGH 2012 Site Distribution Table Ana l y t i c Cases
TABLE 1
Sex AJCC Stage at Dx
Abbreviations: M=Male, F=Female,
UNK=Unknown or Unstageable, N/A=Not Applicable
*Carcinoma in situ/CIN-III of the
cervix is no longer reported nationally or to the state

6
Occu
rren
ce o
f C
an
cer
by S
ite a
nd
Sex
20
12
AN
ALY
TIC
CA
SE
S
Ho
wa
rd C
ou
nty
Ge
ne
ral
Ho
sp
ita
l
Lip
, Ora
l C
avit
y, P
hary
nx, L
aryn
x
Eso
phag
us
Sto
mac
h
Oth
er D
iges
tive
Org
ans
Col
on, R
ectu
m
Pan
crea
s
Lun
g
Mel
anom
a sk
in
Bre
ast
Fem
ale
Ova
ry
Cor
pus
Ute
ri
Cer
vix
Pro
stat
e
Uri
nary
Bla
dder
Kid
ney
Bra
in &
Ner
vous
Sys
tem
Non
-Hod
gkin
Lym
phom
a
Leu
kem
ia
Ben
ign
Bra
in a
nd C
NS
All
Oth
er S
ites
Bre
ast
- M
ale
10 (
4.30
%)
3 (1
.29%
)1
(0.2
7%)
12 (
3.18
%)
3 (1
.29%
)
9 (3
.88%
)2
(0.5
4%)
3 (1
.29%
)3
(0.8
0%)
33 (
14.2
2%)
40 (
10.6
1%)
11 (
4.74
%)
6 (1
.59%
)
9 (3
.88%
)14
(3.
71%
)
35 (
15.0
8%)
36 (
9.55
%)
5 (2
.16%
)5
(1.3
3%)
22 (
9.48
%)
2 (0
.53%
)
172
(45.
62%
)
4 (1
.06%
)
11 (
2.92
%)
3 (0
.80%
)
3 (1
.29
%)
22 (
9.48
%)
12 (
3.19
%)
19 (
8.19
%)
15 (
3.98
%)
18 (
7.76
%)
11 (
2.92
%)
5 (2
.15%
)
22 (
9.49
%)
1 (0
.27%
)
27 (
7.20
%)
To
tal
Mal
es:
Tot
al F
emal
es:
232
(100
.00%
)37
7 (1
00.0
0%)
609
Rep
orte
d C
ases
Rep
ort
#2-2
0-03
0
9/1
2/2
013
For
mat
Cop
yri
ght
(c)
2011
, On
co,
Inc.
ver
4.2
Pre
pa
red
by
: S
her
yl D
au
gh
erty
Da
ta S
et:
Tem
p F
ilte
r R
esu
lts
by
Pag
e 1
of 2
Per
cen
tage
s sh
own
are
gen
der
/col
um
n s
pec
ific
Occ
urre
nce
of C
ance
r by
Site
and
Sex
20
12 A
naly
tic
Ca
ses
HO
WA
RD
C
OU
NT
Y
GE
NE
RA
L
HO
SP
IT
AL
TAB
LE 2

7
US and MD statistics from ACS Facts and Figures
0 5 10 15 20 25 30
Breast
Lung
Colorectal
Melanoma
NHL
PERCENTAGE OF TOTAL CASELOAD
US
MD
HCGH
PErCEnTAGE of ToTAL CASELoAD
US and MD statistics from ACS Facts and Figures
HCGH Top 5 Site Comparison 2012 Analytic Cases
TABLE 3
Non-Hodgkin Lymphoma

8
Ongoing quality reviews monitor HCGH's compliance with nationally established evidence-based treatment guidelines for the management of care for cancer patients. This review includes six measures and compares our performance rate with those from the state of Maryland and the entire U.S. This data is compiled by the National Cancer Data Base (NCDB) using information submitted by cancer registries at all CoC accredited hospitals countrywide (table 4, below).
This year’s review includes data from 2011 (table 5, below). HCGH scored higher than the overall state and national rates for all six monitors.
N C D B P e r f o r m a n c e M e a s u r e s
Measure
BCS/RT
MAC
HT
ACT
12 RLN
Ajd RT
Definition
Radiation therapy is administered within one year (365 days) of diagnosis for women under age 70 receiving breast conserving surgery for breast cancer.
Combination chemotherapy is considered or administered within four months (120 days) of diagnosis for women under 70 with AJCC T1c N0 M0, or Stage II or III ERA and PRA negative breast cancer.
Tamoxifen or third generation aromatase inhibitor is considered/administered within one year (365 days) of diagnosis for women with AJCC T1c N0 M0, or Stage II or III ERA and/or PRA positive breast cancer.
Adjuvant chemotherapy is considered or administered within four months (120 days) of diagnosis for patients under the age of 80 with Stage III (lymph node positive) colon cancer.
At least 12 regional lymph nodes are removed and pathologically examined for resected colon cancer.
Radiation therapy is administered within six months (180 days) of diagnosis for patients under the age of 80 with clinical or pathologic AJCC T4 N0 M0 or Stage III receiving surgical resection for rectal cancer.
Performance rate HCGH MD US
97.50% 83.90% 84.60%
100% 86.80% 86.40%
95% 77% 77%
100% 77.50% 80.70%
95% 89.20% 87.50%
100% 90.50% 88.50%
Measure Definition HCGH MD US
Radiation therapy is administered within one year (365 days) of diagnosis for women under age 70
receiving breast conserving surgery for breast cancer
Combination chemotherapy is considered or administered within four months (120 days) of diagnosis for
women under 70 with AJCC T1c N0 M0, or Stage II or III ERA and PRA negative breast cancer
Tamoxifen or third generation aromatase inhibitor is considered/administered within one year (365 days)
of diagnosis for women with AJCC T1c N0 M0, or Stage II or III ERA and/or PRA Positive breast cancer
Adjuvant chemotherapy is considered or administered within four months (120 days) of diagnosis for
patients under the age of 80 with Stage III (lymph node positive) colon cancer
At least 12 regional lymph nodes are removed and pathologically examined for resected colon cancer
Radiation therapy is administered within six months (180 days) of diagnosis for patients under the age
of 80 with clinical or pathologic AJCC T4N0M0 or Stage III receiving surgical resection for rectal cancer
89.20% 87.50%
100%MAC
HT
ACT
12 RLN
Ajd RT
100%
95%
86.80% 86.40%
95% 77.00% 77.00%
100% 90.50% 88.50%
77.50% 80.70%
NCDB Performance Measures2011 Analytic Cancer Cases
97.50% 83.90% 84.60%
Performance Rate
BCS/RT
0
0.2
0.4
0.6
0.8
1
1.2
BCS/RT MAC HT ACT 12 RLN Ajd RT
Compliance
Rate
Performance Measure
HCGH
Maryland
US
PErforMAnCE MEASUrE
Co
MP
LiA
nC
E r
AT
E
2011 Analytic Cases
TABLE 5
TABLE 4

9
Breast cancer is the most common cancer to occur in women and, after lung cancer, the second most common cause of cancer death in women. Over 200,000 women are diagnosed with breast cancer every year, but the good news is that there are 2.6 million breast cancer survivors in the United States. Breast cancer awareness is highly visible in the United States due to active breast cancer support groups and everything turning pink in the month of October. That visibility has been used to promote breast cancer screening as a way to improve survival. The success of screening is demonstrated by the large percent of women that are diagnosed with early stage breast cancer: stage 0, 1 or 2 (table 6, page 10). That early diagnosis has resulted in fewer complications from breast cancer treatment and more survivors.
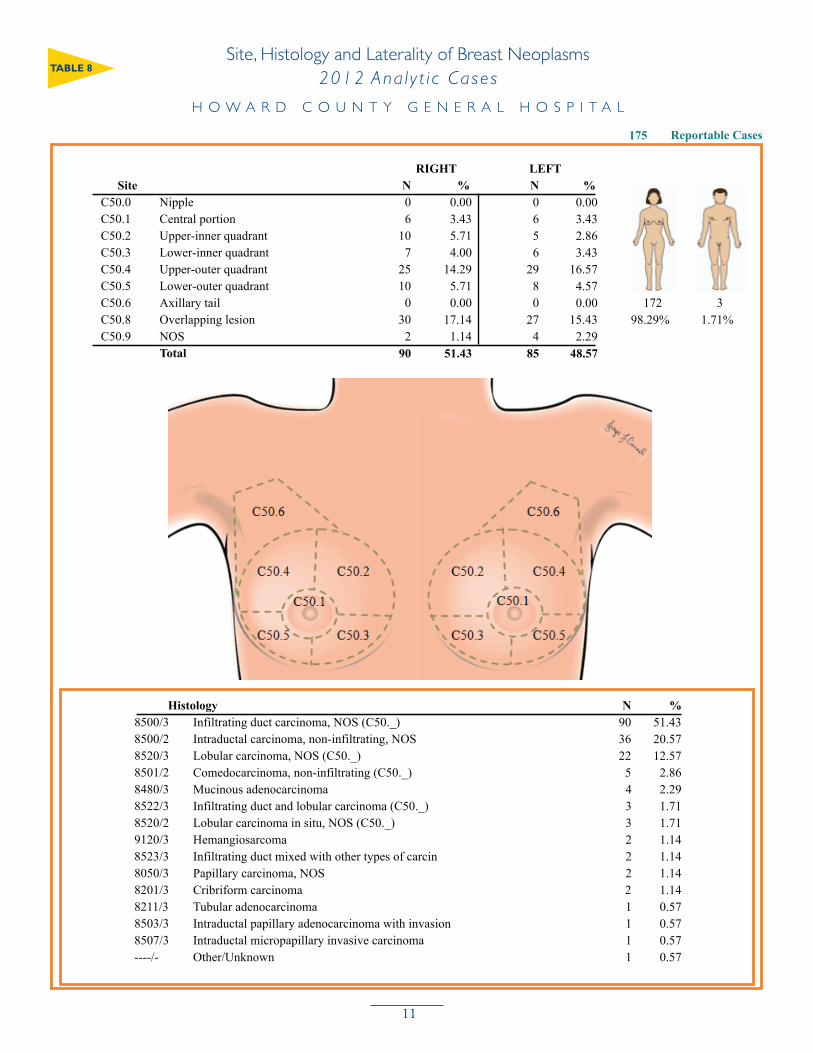
Breast cancer arises in the portion of the breast that makes milk. This is termed the breast lobule and ductal system. There are approximately 15 lobular units in each breast which open onto the nipple through eight to 10 sites. The lining of these ductal lobular units is the cell that results in breast cancer. The two most common types of breast cancer are ductal carcinoma (which accounts for 72 percent) and lobular carcinoma (accounting for 14 percent) (table 8, page 11). A number of impor-tant features of breast cancer are used to determine an individual’s prognosis. The most important is the cancer’s stage, which is determined by the size of the invasive tumor and the presence of lymph nodes involved with tumor. In Howard County, the majority of women are diagnosed at an early stage. Other important features in determining treatment and survival are the estrogen and proges-terone receptor status, the presence of Her-2-neu receptors on the cell surface, and estimates of the rate of growth of the tumor. Each of these features is used to personalize the treatment of the cancer to the specific features that the cancer exhibits. This allows us to select treatments that are more likely to be effective and, therefore, limit the complications and risks of treatment.
The most gratifying aspect of taking care of breast cancer patients is that the majority of them will survive. This allows the doctors and nurses involved to approach every patient with a positive perspective and an expectation that they will do well. In developing the Breast Center at HCGH, we have taken the view that high-quality breast cancer screening coupled with compassionate, well-coordinated, state-of-the-art care will result in more breast cancer survivors in our community. Despite heightened awareness and availability of mammography, only 50 percent of women get the recommended yearly mammogram. At the Breast Center at HCGH, we have a goal to increase our screening and diagnostic mammography rates by providing high-quality services in a convenient setting. We have begun to see steady increases in the number of women diagnosed and treated for breast cancer in the county.
The key to increased survival in breast cancer is early detection and up-to-date management once a diagnosis is made. We work to improve early detection through community education events emphasizing availability of screening services. We are also fortunate to have health care providers whose primary practice is focused on breast cancer care. This allows us to offer our patients the best treatment options available that are specifically targeted to their tumor. The results of these efforts (table 7, page 10) demonstrate that Howard County has a much higher breast cancer survival rate than the remainder of the United States.
Lisa Jacobs, M.D. Medical Director, Breast Center at Howard County General Hospital
F o c u s o n B r e a s t C a n c e r
Lisa Jacobs, M.D. Medical Director, Breast Center, Howard County General Hospital

10
NCDB Data used for comparisonTable #2
78
80
82
84
86
88
90
92
94
96
98
100
1 2 3 4 5
SURVIVAL PERCENTAGE
YEARS SINCE DIAGNOSIS
OVERALL SURVIVIAL RATE COMPARISON 2003-2006 ANALYTIC BREAST CANCER CASES
HCGH
US
SUrV
iVA
L P
Er
CE
nTA
GE
YEArS SinCE DiAGnoSiSNCDB data used for comparison
Table #1
0
5
10
15
20
25
<40 40 - 49 50 - 59 60 - 69 70 - 79 80+
NUMBER OF CASES
AGE AT DIAGNOSIS
AGE BY STAGE DISTRIBUTION HCGH 2012 ANALYTIC BREAST CANCER CASES
0
I
II
III
IV
NA/UNK
overall Survival rate Comparison 2003-2006 Analytic Breast Cancer Cases
Age by Stage Distribution HCGH 2012 Analytic Breast Cancer Cases
AGE AT DiAGnoSiS
nU
MB
Er
S o
f C
ASE
S
TABLE 6
TABLE 7
11
Site, Histology and Laterality of Breast Neoplasms
2012 ANALYTIC CASES
Reportable Cases
Howard County General Hospital
175
N %Site
Histology %N
RIGHT LEFT
%N
C50.0
C50.1
Nipple
Central portion
C50.2
C50.3
C50.4
C50.5
C50.6
C50.8
C50.9
Upper-inner quadrant
0 0.00
Lower-inner quadrant
Upper-outer quadrant
Lower-outer quadrant
Axillary tail
Overlapping lesion
NOS
6
10
7
25
10
0
30
2
3.43
5.71
4.00
14.29
5.71
0.00
17.14
1.14
0
6
5
6
29
8
0
27
4
0.00
3.43
2.86
3.43
16.57
4.57
0.00
15.43
2.29
Total 90 85
3 172
8500/3
8500/2
8520/3
8501/2
8480/3
8522/3
8520/2
9120/3
8523/3
8050/3
8201/3
8211/3
8503/3
8507/3
----/-
Infiltrating duct carcinoma, NOS (C50._)
Intraductal carcinoma, non-infiltrating, NOS
Lobular carcinoma, NOS (C50._)
Comedocarcinoma, non-infiltrating (C50._)
Mucinous adenocarcinoma
Infiltrating duct and lobular carcinoma (C50._)
Lobular carcinoma in situ, NOS (C50._)
Hemangiosarcoma
Infiltrating duct mixed with other types of carcin
Papillary carcinoma, NOS
Cribriform carcinoma
Tubular adenocarcinoma
Intraductal papillary adenocarcinoma with invasion
Intraductal micropapillary invasive carcinoma
Other/Unknown
90
36
22
5
4
3
3
2
2
2
2
1
1
1
1
51.43
20.57
12.57
2.86
2.29
1.71
1.71
1.14
1.14
1.14
1.14
0.57
0.57
0.57
0.57
98.29% 1.71%
51.43 48.57
Page 1 of 2Report #2-01-02 sv_1 09/12/2013
Format Copyright (c) 2011, Onco, Inc. ver 4.2
Prepared by: Sheryl Daugherty
Data Set: Temp Filter Results by
Site, Histology and Laterality of Breast Neoplasms 2012 Ana l y t i c Cases
H O W A R D C O U N T Y G E N E R A L H O S P I T A L
TABLE 8

12
• Sponsored the Cancer Survivors Reception at the American Cancer Society’s Relay for Life. HCGH was a corporate sponsor and sponsored a team, which raised over $13,000. • Free monthly meeting space was provided for the American Cancer Society Leadership Council and Man-to-Man prostate cancer support group.• The hospital provided space for Nicotine Anonymous meetings every Sunday.• Focus on Your Total Health: Your Seasonal Check-Up was held in September and provided cervical cancer information, BMI calculations, breast self-exam demonstrations and information on women’s health issues to 72 participants.• On-site breast health demonstrations and lectures were held at Howard County businesses and organizations through Personally Speaking: A Breast Health Education Program funded through the Howard County General Hospital Volunteer Auxiliary. In addition, related flyers were placed in the bathrooms of 45 area organizations.• Spring Into Health was held in June, with 62 participants receiving information on healthy eating, the risks of prostate, testicular and colon cancers, as well as BMI calculations. • You’re a Breast Cancer Survivor – Now What? was held in October at the HCGH Wellness Center with 45 participants. It was also recorded and posted online.• The Great American Smokeout was held in November in the HCGH front lobby, providing tobacco prevention information to over 50 staff and visitors.• Through the Let Go of Tobacco program, HCGH provided patients in Labor and Delivery brochures listing local resources and websites available for smoking cessation. Another phase provides anti-tobacco resources in local faith communities through the hospital’s Community Cardiovascular Project. Parish-based volunteer nurses are provided with posters and brochures on smoking cessation to share while screening for hypertension. Tobacco prevention information was distributed to maternal-child health classes.• Mammograms: Best Practices for Women for Healthier Exams was held in September at the Wellness Center. Experts presented information on breast health, cancer prevention, genetics, mammogram myths and surgical options in this program. This program is available online at hcgh.org/mammogram. • Provided information on cancer risk reduction and the importance of early detection at health fairs throughout the year.• The hospital’s speakers bureau filled numerous requests for presentations on cancer risk reduction and the dangers of tobacco use.• Two members of the HCGH staff served as active members on the Leadership Council of the American Cancer Society.• Multiple Claudia Mayer Cancer Resource Center (CMCRC) fundraisers: month-long Blossoms of Hope events, annual Signature Fretz Autumn Extravaganza event as well as many smaller, community events. Our newest fundraising program, Team CONQUER Cancer, participated in several running and triathlon events which helped raise even more funds and awareness for the center. All of these events raised approximately $210,000. • Nutrition and Cancer, individual counseling with a registered dietitian, helped high-risk people modify their diets and assisted those undergoing cancer treatment meet nutritional needs. • Thirteen prostate cancer screenings were performed by urologists at the HCGH Wellness Center in April.• Distributed seven free colorectal cancer screening kits to the community.• In May, 52 skin cancer screenings were performed at the HCGH Wellness Center.
T h e Ye a r i n R e v i e w 2 0 1 2

13
• The Howard County Cancer and Smoke Free Tobacco Coalition is represented by a member of HCGH’s Wellness Center Staff. • The monthly Care Giver Support Group at CMCRC provided support to 27 family care givers.• Smoke-Free Lungs, a free monthly program for those who want to quit using tobacco, provided support and education to those in any stage of the quit process. • Participated in the Latino Health Fair. Clinical breast exams, skin cancer information, colorectal cancer education, fecal occult blood testing kits and general cancer education and materials provided in March to more than 550 participants. Prostate and oral cancer screenings as well as smoking cessation information were also provided.• HCGH was a sponsor of Get Active Howard County, an annual healthy lifestyle program, with over 1,000 participants.• Cosponsored the 50+ Expo for thousands of seniors, offering breast health, blood pressure, BMI, pulmonary function tests, stroke screenings, tobacco prevention and other wellness programs at Wilde Lake High School in October.• In October, a Cancer Prevention and Early Detection Clinic was sponsored by HCGH at The Mall in Columbia. Over 200 participants received information on breast health, HPV and cervical cancer, tobacco prevention, lymphedema, oral health and pancreatic cancer; conferred with cancer specialists; and had their BMI measured. • The CMCRC continued to offer programs to cancer patients such as yoga, quilting, knitting and crocheting, acupuncture and Ask-the-Pharmacist. Other support programs offered at CMCRC are Teens Together, Stage IV Breast Cancer Group, Survivors Offering Support and the Care Givers Support Group.• Healthy Families, Healthy Kids Clinic was sponsored by HCGH in September at The Mall in Columbia. Information on tobacco prevention, skin cancer, healthy lifestyles and cancer prevention was available to 170 attendees. • In February, the community Cardiovascular Clinic was held at The Mall in Columbia where the hospital provided screenings, including pulmonary function tests; physician experts were on-site and smoking cessation information was available for 117 participants. • The annual Healthy Howard Day highlighted healthy lifestyles, physical activity and wellness. HCGH provided more than 100 BMI measurements.• Over 1,200 BMI calculations were performed by the HCGH Wellness Center staff at numerous community events and health fairs. • In May, the Asian-Pacific Islander American Heritage Fair was held for several hundred participants with HCGH providing BMI calculations. • In May, over 2,000 people attended the Howard County Public School System’s Employee/ Family Wellness Day. HCGH staffed this first annual event and provided BMI calculations.• In June, the Howard County Men’s Health Fair featured health awareness programs specific to men with 200 attending.• HCGH sponsored the Red Cross Blood Drive and Health Fair at the Wellness Ce nter in June. Over 90 people attended. • The Fitness and Sports Medicine Clinic, held at The Mall in Columbia in June, featured physician experts, and cancer prevention and education materials to over 100 attendees.• In September, the Healthy Kids, Healthy Families Clinic at The Mall in Columbia featured health resources for children and families. Over 170 families registered.
T h e Ye a r i n R e v i e w 2 0 1 2

14
Claudia Mayer Cancer Resource Center (CMCRC): provides educational, aesthetic, emotional and psychosocial support services through center resources, which include a lending library; classes and support programs for patients, families and care givers; a full-service salon; a prosthesis specialist, oncology social worker and navigation; and acupuncture and therapeutic massage. For more infor-mation, call 410-740-5858.
Breast Cancer Support Group: meets the third Wednesday of the month from 7 to 8:30 p.m. Free, but registration is required. For more information, call 410-740-5858.
Care Givers Support Group: meets the first Tuesday of each month from 3:30 to 4:30 p.m. or the second Saturday of each month from 10 to 11 a.m. at CMCRC. Call 410-740-5858 for more information.
Living with Breast Cancer – Stage IV Breast Cancer Support Group: meets the fourth Thursday of each month from 7 to 8:30 p.m. Free, but registration is required. For more information call 410-740-5858.
Together We Thrive: a support group for men and women diagnosed with cancer, meets the first Saturday of each month from 10 to 11:30 a.m. Call 410-740-5858 for more information.
Red Devils: services for breast cancer patients coordinated through CMCRC. Call 410-740-5858 for more information.
Advance Directives classes to educate patients, families and the community about advance directives. Sponsored by CMCRC and the Wellness Center. For additional information, call 410-740-7601.
Yoga for Patients, Care Givers and Survivors: offered Tuesdays from 10 to 11 a.m. from an experienced and clinically trained instructor. For information or to register, call 410-964-9100.
Knitting and Crochet Support Group: meets weekly on Wednesdays from 10 a.m. to noon. Instruction, directions and good times for the beginning or advanced needler. Free. Call 410-740-5858 for more information.
Quilting Support Group: second and fourth Tuesdays of each month, 1 to 3 p.m. Quilting and hand-piecing techniques and time to work on projects. Free. Call 410-740-5858 for more information.
Programs through American Cancer Society (ACS) at the Claudia Mayer Cancer Resource Center Look Good Feel Better: This ACS program provides a free workshop by a licensed cosmetologist. Women undergoing cancer treatment learn to manage the appearance-related side effects of cancer treatment and receive a complimentary bag of cosmetics. Meets monthly. To register, call ACS at 888-535-4555.
Road to Recovery: sponsored by the ACS, volunteer drivers provide transportation for cancer patients undergoing treatment. Call 888-227-6333.
Programs and Suppor t Groups for Pat ients and thei r Famil ies

15
Other Community ResourcesBreast and Cervical Cancer Screening Program: for women age 40 and over who meet income requirements and have no health insurance or are under-insured. For more information, call 410-313-2333.
Cancer Information Service of the National Cancer Institute: 800-422-6237.
Gilchrist Hospice Care: services for the terminally ill, their families and the bereaved. Call 410-730-5072.
Howard County General Hospital Wellness Center: programs include screenings, health fairs, support groups and smoking cessation classes. For information, call 410-740-7601.
The Bolduc Family Outpatient Center (including lymphedema and oncology rehabilitation management): 443-718-3000
Howard County General Hospital Ostomy Nurse: 410-740-7767
Howard County General Hospital Pastoral Care: 410-740-7898
Advanced Disease and Symptom Management Program (formerly HCGH Palliative Care Program): 410-720-8500
Eric Aldrich, M.D., Ph.D., AdministrationRennae Anderson, M.D., PathologyDianne Braun, P.T., The Bolduc Family Outpatient Center, clinical program manager Sally Cheston, M.D., Radiation Oncology, Cancer Conference coordinator, chairpersonSheryl Daugherty, R.H.I.T., C.T.R., Oncology Program coordinatorSandra Dawson, R.H.I.A., director, Health Information Management, quality review coordinatorHeather Dworski, Pharm.D., PharmacySuzi Ford, American Cancer SocietyPaul Gleichauf, Administration Leslie Hack, PA-C, quality review coordinatorJohn Kishel, M.D., Urology/SurgeryMartha Koch, M.D., Colorectal SurgeryMichelle Morgan, Clinical ResearchAndrew Morton, M.D., Diagnostic ImagingStanley Podlasek, M.D., PathologySandy Roemer, R.N., Community EducationLeslie Rogers, M.S.W., LCSW-C, Claudia Mayer Cancer Resource Center, oncology social workerTeji Sastry, M.D., Medical Oncology, cancer liaison physicianJudy Siegelman, R.N., O.C.N., nurse manager, 4 SouthSharon Tunney, C.T.R., cancer registrarDavid Van Echo, M.D., Advanced Disease and Symptom Management
Programs and Suppor t Groups for Pat ients and thei r Famil ies
2 0 1 3 C a n c e r C o m m i t t e e

1
5755 Cedar Lane Columbia, MD 21044410-740-7890 • hcgh.org