2016 world masters weightlifting...
TRANSCRIPT
1
2016 WORLD MASTERS
WEIGHTLIFTING CHAMPIONSHIP (32nd Men’s and 23rd Women’s)
Heinsheim, GERMANY 1st – 8th October 2016
(OFFICIAL ENTRY FORM)
All competitors must complete and submit pages 2, 3, and 4.
National Masters Chairmen must submit a Summary of Entry Fees (page 5) with all
entries. Where a nation has only one or few entries the summary must still be
submitted.

2
2016 IWF-WORLD MASTERS WEIGHTLIFTING CHAMPIONSHIP
(32nd Men's and 23rd Women's Championships) REGISTERED for IWF MASTERS DRUG
TESTING Heinsheim, Germany 1st – 8th October 2016
Return entry forms to - IWF MASTERS SECRETARIAT Dionissiou Solomou 59
2231 Latsia CYPRUS
Email - [email protected] Telephone - + 357 96 710022
Entry Fees - Competition (non-returnable) €106 (includes €1 affiliation) Team Entry (men and women)
(Pay at Technical Conference) €30
Closing Banquet – pay at venue €30 Euros
Venue & address - Josef-Muller-Halle Neckarstr 1, 74906 Bad Rappenau-Heinsheim
CLOSING DATE FOR ENTRIES: Letters postmarked n o later than June 30th , 2016 All forms must be mailed collectively from one sour ce, e.g. your National Masters Chairman NO LATE ENTRIES OR INCOMPLETE ENTRIES ACCEPTED.
Please enter me in the______ kilogram class, age group ______ of the IWF World Masters Weightlifting Championships to be held on 1st Oct.. to 8th Oct. – Heinsheim, Germany. . I hereby accept and acknowledge that all of the rules and regulations of the present competition are solely governed by the applicable rules and regulations of the IWF, IWF Masters, and WADA. I certify that I am an amateur in good standing. In consideration of my entry in the competition, I do hereby waive, and release the 2016 World Masters Weightlifting Championship Organiser (hereafter referred to as the "Organiser"), IWF Masters, their directors, and associated personnel from any and all causes of action, loss, liability, claims, and demands of every kind and nature which I or my heirs or personal representatives may have for bodily injury and expenses of medical treatment. I agree to be filmed and photographed under conditions approved and authorized by the Organiser and IWF Masters to include the use of my name, biographical information, public appearances, interviews, photographs, portrait and motion pictures and television recordings of my weightlifting performances, and grant to the Organiser and the IWF Masters the right to record and make use of the same, and to authorize others to do so in promoting the competition and the success of the weightlifting team on which I compete, to promote the image of the Organiser and the IWF Masters, their sponsors and advertisers, and the sport of amateur weightlifting, and to fund the activities of the Organiser and IWF Masters. I understand all responsibilities for any problems, injuries, etc., arising from my health condition while participating in the IWF Masters Weightlifting Championships. I agree that the Organiser, IWF Masters and their agents, including competition personnel, may make judgments (with appropriate input from available medical personnel), as to my treatment, hospitalization, or other medical care in the event of my illness or accidental injury in connection with my participation in the competition should I be disabled or incompetent to make necessary and appropriate decisions concerning such treatment, hospitalization, or other care. I authorize the Organiser, IWF Masters, their agents and competition personnel to make decisions for me as though they stood in a relationship to me of parent, guardian, or next of kin should circumstances require the Organizer, IWF Masters, their agents and competition personnel to make judgments if my next of kin cannot be timely and conveniently contacted to participate in the making of such judgments. I hereby release and agree not to hold the Organiser, IWF Masters, their agents and competition personnel responsible for all expenses, causes of action, liability, claims, and demands arising from good faith judgments made by the Organiser, IWF Masters, their agents and competition personnel concerning my treatment, hospitalization, and medical care in the event of my illness, injury, and other emergency circumstances in connection with the competition. I agree that I will be financially responsible for treatment and other medical care rendered me in the event of my illness, injury, or other emergent circumstances in connection with the competition, except to the extent of my injuries, and medical expenses, if any, are covered by accidental death, dismemberment and/or loss of sight and medical reimbursement insurance policies, maintained by the Organizer for my benefit, in which event I will nevertheless continue to be financially responsible for expenses of treatment, hospitalization, and other medical care in excess of such policies’ limits.
Further, I declare that I agree to the contents of the IWF MASTERS RULEBOOK and current IWF Anti Doping Rules All lifters must sign on the entry forms a statement that the IWF MASTERS has the authority and the right to test for banned substances at any time during the days of the championship , in our out of competition. The IWF MASTERS recognises the right of any member country to conduct tests on any lifter selected for a drug test at any IWF MASTERS organised event or at any other time.
THE IWF MASTERS DRUG POLICY WILL BE STRICTLY ENFORC ED. *** Please sign below ***
I (the undersigned) accept all such conditions – Name (Print) ______________________________ Signature ______________________________
3
2016 IWF-WORLD MASTERS WEIGHTLIFTING CHAMPIONSHIP
(32nd Men's and 23rd Women's Championships) REGISTERED for IWF MASTERS DRUG
TESTING Heinsheim, Germany 1st – 8th October 2016
I agree to be bound by the Masters rules and declare that I am physically fit to undertake the sport of weightlifting and have no knowledge of any medical condition which will make weightlifting contra-indicated to my well-being. I understand that Travel insurance with health and accident cover is mandatory.
COMPETITOR’S PERSONAL DETAILS (please print clearly and complete all details marke d *): NAME: First (print) *
Last (print) *
Signature:* Nation (country by passport):* ADDRESS* Line 1 : Line 2 : Line 3 : Date of Birth* – format DD/MM/YYYY / / Age at 31st Dec. 2016*: Age Group*: Body Weight Category* : Gender (M or W)* : Best Total between 20th Sept. 2015 and 30th June 2016* (kg) : Qualifying total for my age group and body weight category (kg) : Email address* : Please indicate if you are a referee (delete as applicable) – IWF CAT I / IWF CAT II / National How long have you held your current status? Years - Months - The above competitor’s details are authorised by me as National Masters Chairman and/or on behalf of the National Federation - Print Name: ______________________________ Signature: ______________________________ Email: _______________________
PLEASE PROVIDE ONE OF THE FOLLOWING * :- Passport number _________________________ Country _________________________ Driver’s license _________________________ Province/state/country of issue ______________________________
4
2016 IWF-WORLD MASTERS WEIGHTLIFTING CHAMPIONSHIP
(32nd Men's and 23rd Women's Championships) REGISTERED for IWF MASTERS DRUG
TESTING Heinsheim, Germany 1st – 8th October 2016
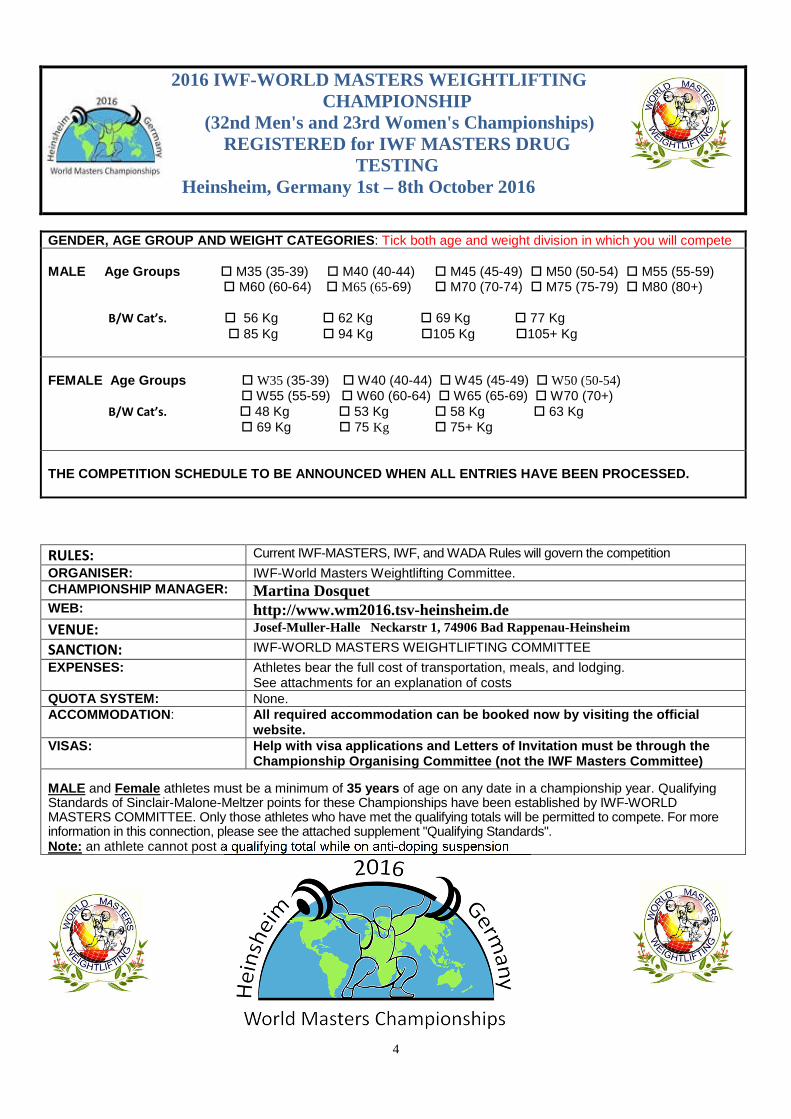
GENDER, AGE GROUP AND WEIGHT CATEGORIES : Tick both age and weight division in which you will compete MALE Age Groups � M35 (35-39) � M40 (40-44) � M45 (45-49) � M50 (50-54) � M55 (55-59)
� M60 (60-64) � M65 (65-69) � M70 (70-74) � M75 (75-79) � M80 (80+)
B/W Cat’s. � 56 Kg � 62 Kg � 69 Kg � 77 Kg � 85 Kg � 94 Kg �105 Kg �105+ Kg
FEMALE Age Groups � W35 (35-39) � W40 (40-44) � W45 (45-49) � W50 (50-54) � W55 (55-59) � W60 (60-64) � W65 (65-69) � W70 (70+)
B/W Cat’s. � 48 Kg � 53 Kg � 58 Kg � 63 Kg � 69 Kg � 75 Kg � 75+ Kg THE COMPETITION SCHEDULE TO BE ANNOUNCED WHEN ALL E NTRIES HAVE BEEN PROCESSED.
RULES: Current IWF-MASTERS, IWF, and WADA Rules will govern the competition ORGANISER: IWF-World Masters Weightlifting Committee. CHAMPIONSHIP MANAGER : Martina Dosquet WEB: http://www.wm2016.tsv-heinsheim.de VENUE: Josef-Muller-Halle Neckarstr 1, 74906 Bad Rappenau-Heinsheim
SANCTION: IWF-WORLD MASTERS WEIGHTLIFTING COMMITTEE EXPENSES: Athletes bear the full cost of transportation, meals, and lodging.
See attachments for an explanation of costs QUOTA SYSTEM: None. ACCOMMODATION : All required accommodation can be booked now by visiting the o fficial
website. VISAS: Help with visa applications and Letters of Invitation must be through the
Championship Organising Committee (not the IWF Mast ers Committee)
MALE and Female athletes must be a minimum of 35 years of age on any date in a championship year. Qualifying Standards of Sinclair-Malone-Meltzer points for these Championships have been established by IWF-WORLD MASTERS COMMITTEE. Only those athletes who have met the qualifying totals will be permitted to compete. For more information in this connection, please see the attached supplement "Qualifying Standards". Note: an athlete cannot post a qualifying total while on anti-doping suspension
5
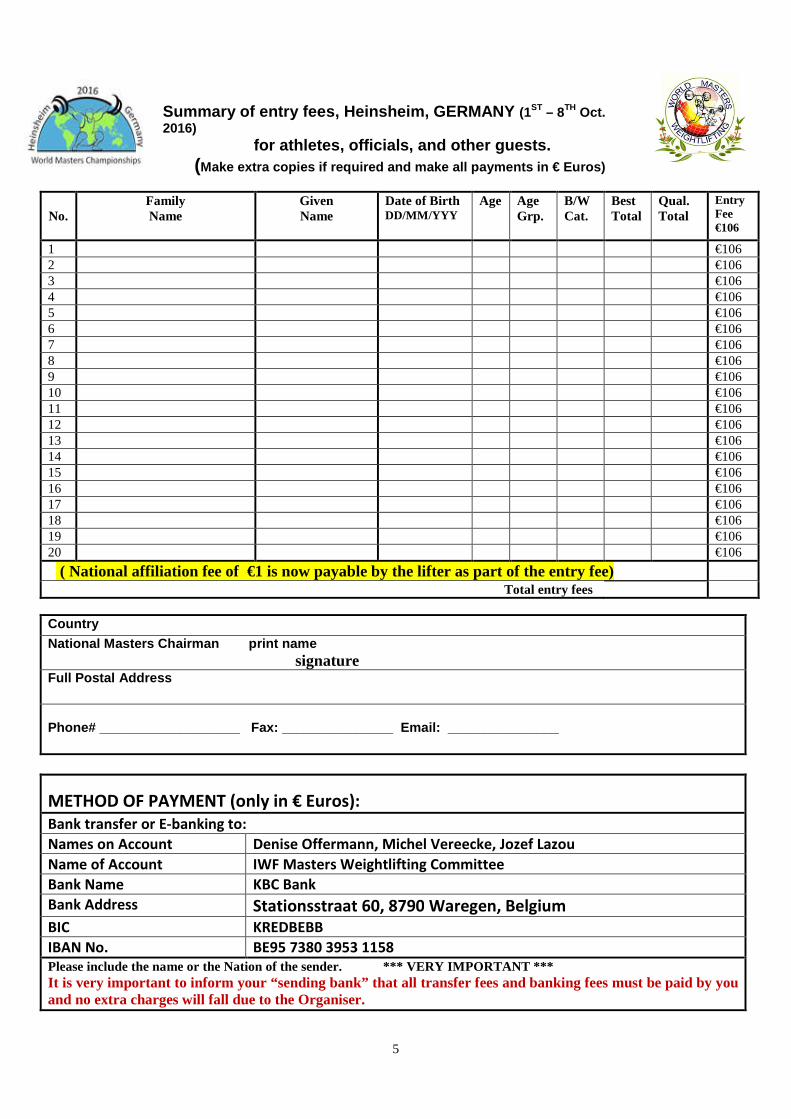
Summary of entry fees, Heinsheim, GERMANY (1ST – 8TH Oct. 2016)
for athletes, officials, and other guests. (Make extra copies if required and make all payments in € Euros)
No. Family Name
Given Name
Date of Birth DD/MM/YYY
Age Age Grp.
B/W Cat.
Best Total
Qual. Total
Entry Fee €106
1 €106 2 €106 3 €106 4 €106 5 €106 6 €106 7 €106 8 €106 9 €106 10 €106 11 €106 12 €106 13 €106 14 €106 15 €106 16 €106 17 €106 18 €106 19 €106 20 €106
( National affiliation fee of €1 is now payable by the lifter as part of the entry fee)
Total entry fees Country National Masters Chairman print name signature Full Postal Address Phone# ___________________ Fax: _______________ Email: _______________
METHOD OF PAYMENT (only in € Euros):
Bank transfer or E-banking to:
Names on Account Denise Offermann, Michel Vereecke, Jozef Lazou
Name of Account IWF Masters Weightlifting Committee
Bank Name KBC Bank
Bank Address Stationsstraat 60, 8790 Waregen, Belgium
BIC KREDBEBB
IBAN No. BE95 7380 3953 1158
Please include the name or the Nation of the sender. *** VERY IMPORTANT *** It is very important to inform your “sending bank” that all transfer fees and banking fees must be paid by you and no extra charges will fall due to the Organiser.

6
2016 IWF-WORLD MASTERS WEIGHTLIFTING CHAMPIONSHIP
(32nd Men's and 23rd Women's Championships) REGISTERED for IWF MASTERS DRUG
TESTING Heinsheim, Germany 1st – 8th October 2016
OFFICIAL TEAM REGISTRATION (for NATIONAL CHAIRMEN O NLY) Please enter the following team (Men’s or Women’s) in this IWF-Masters championship. The payment of the entry fee for this event is €30 and can be paid at accreditation or at the Technical Meeting. All athletes must have registered officially for this event. The men's teams consist of 8 lifters and the women's team 7 lifters. Each nation is only allowed 2 team members competing in the same age group and body weight category.
NATION____________________________________________Date:___________________ NATIONAL CHAIRMAN / COACH _________________________________________
Signature _________________________________________
NAME B/Wght. AGE TOTAL
1.
2.
3.
4.
5.
6.
7.
8.
Reserves:-
1
2
3
7
2016 IWF-WORLD MASTERS WEIGHTLIFTING CHAMPIONSHIP
(32nd Men's and 23rd Women's Championships) REGISTERED for IWF MASTERS DRUG
TESTING Heinsheim, Germany 1st – 8th October 2016
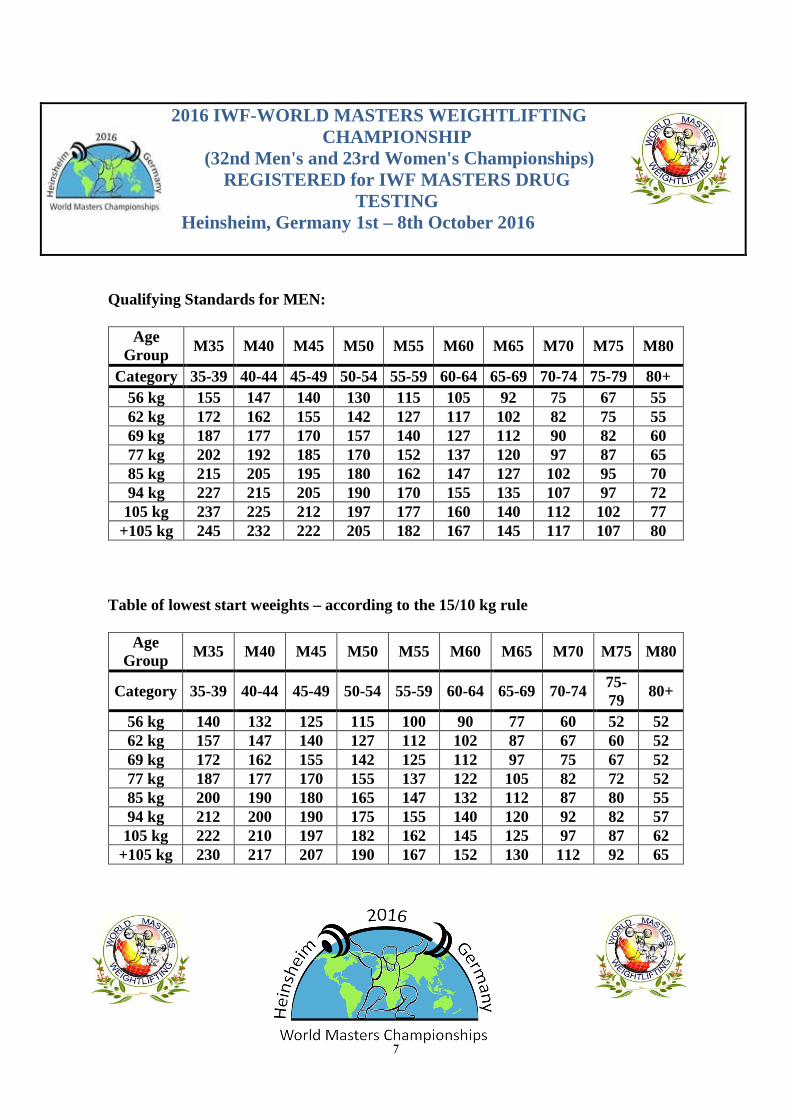
Qualifying Standards for MEN:
Age Group M35 M40 M45 M50 M55 M60 M65 M70 M75 M80
Category 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80+ 56 kg 155 147 140 130 115 105 92 75 67 55 62 kg 172 162 155 142 127 117 102 82 75 55 69 kg 187 177 170 157 140 127 112 90 82 60 77 kg 202 192 185 170 152 137 120 97 87 65 85 kg 215 205 195 180 162 147 127 102 95 70 94 kg 227 215 205 190 170 155 135 107 97 72 105 kg 237 225 212 197 177 160 140 112 102 77
+105 kg 245 232 222 205 182 167 145 117 107 80 Table of lowest start weeights – according to the 15/10 kg rule
Age Group
M35 M40 M45 M50 M55 M60 M65 M70 M75 M80
Category 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79
80+
56 kg 140 132 125 115 100 90 77 60 52 52 62 kg 157 147 140 127 112 102 87 67 60 52 69 kg 172 162 155 142 125 112 97 75 67 52 77 kg 187 177 170 155 137 122 105 82 72 52 85 kg 200 190 180 165 147 132 112 87 80 55 94 kg 212 200 190 175 155 140 120 92 82 57 105 kg 222 210 197 182 162 145 125 97 87 62
+105 kg 230 217 207 190 167 152 130 112 92 65
8
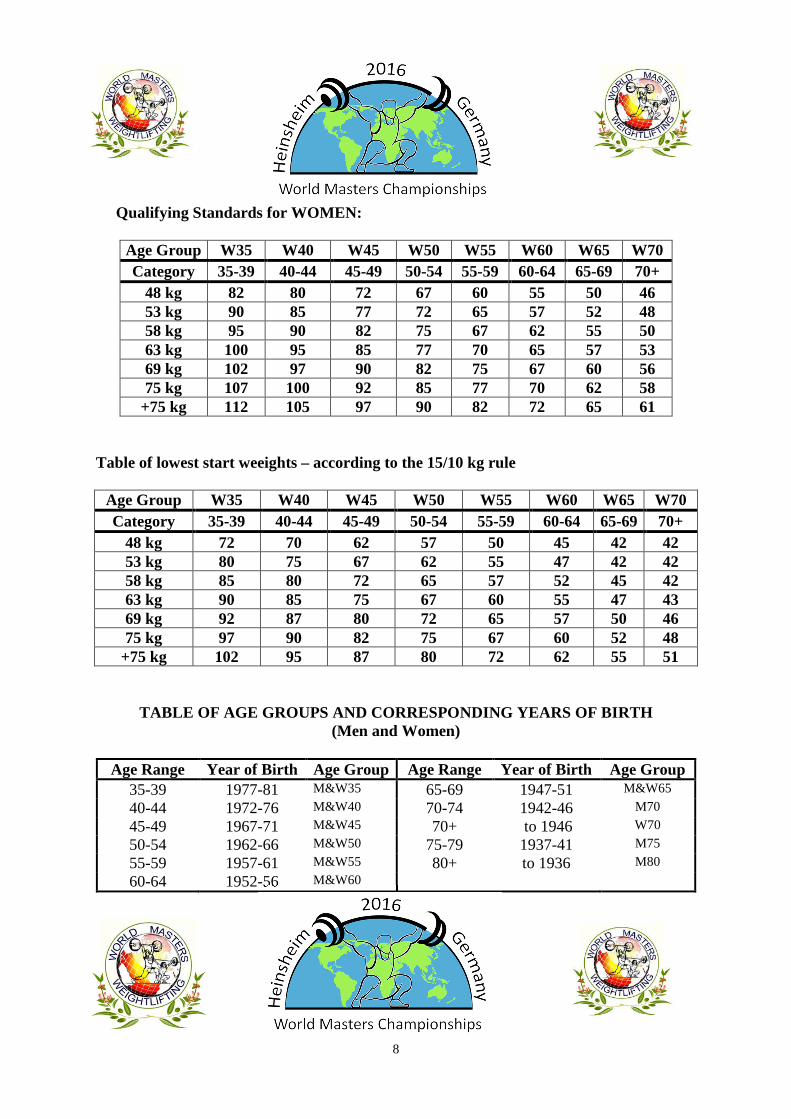
Qualifying Standards for WOMEN:
Age Group W35 W40 W45 W50 W55 W60 W65 W70 Category 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70+
48 kg 82 80 72 67 60 55 50 46 53 kg 90 85 77 72 65 57 52 48 58 kg 95 90 82 75 67 62 55 50 63 kg 100 95 85 77 70 65 57 53 69 kg 102 97 90 82 75 67 60 56 75 kg 107 100 92 85 77 70 62 58
+75 kg 112 105 97 90 82 72 65 61
Table of lowest start weeights – according to the 15/10 kg rule
Age Group W35 W40 W45 W50 W55 W60 W65 W70 Category 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70+
48 kg 72 70 62 57 50 45 42 42 53 kg 80 75 67 62 55 47 42 42 58 kg 85 80 72 65 57 52 45 42 63 kg 90 85 75 67 60 55 47 43 69 kg 92 87 80 72 65 57 50 46 75 kg 97 90 82 75 67 60 52 48
+75 kg 102 95 87 80 72 62 55 51
TABLE OF AGE GROUPS AND CORRESPONDING YEARS OF BIRTH (Men and Women)
Age Range Year of Birth Age Group Age Range Year of Birth Age Group
35-39 1977-81 M&W35 65-69 1947-51 M&W65
40-44 1972-76 M&W40 70-74 1942-46 M70
45-49 1967-71 M&W45 70+ to 1946 W70
50-54 1962-66 M&W50 75-79 1937-41 M75
55-59 1957-61 M&W55 80+ to 1936 M80
60-64 1952-56 M&W60

9
Medical Information
Since the 2004 World Championships in Baden, Austria, the IWF Masters has encouraged athletes to share their medical information with our medical team. In the past it has been included with the registration packet. This form was developed purely to assist the medical personnel in the event of an injury, sickness or emergency of an athlete, official, or coach. It must be completed in ENGLISH but it can be filled out by the athlete, athlete’s representative, or physician.
This questionnaire is strictly confidential and will be used by the IWF Masters medical team in case of injury/illness during the competition. This form will NOT be used to qualify or disqualify a lifter in terms of their health status or be used by anti-doping. All lifters are recommended to see their own personal physician to address their health status prior to engaging in a world competition.
This form will be destroyed at the end of the competition!
The athlete MUST do either
1) OPTION 1: Fill out the attached Medical Information Form (MIF) (preferred) OR 2) OPTION 2: Sign the waiver in the MIF refusing to share their medical information with the
competition’s medical provider.
One of the two options MUST (mandatory) be returned along with the athlete’s registration to their country’s national chairman.
The National Masters Chairman may do one of two things with the forms he/she has collected from all competitors.
1) Mail the documents (both MIF and declinations) with the registration forms to the meet organizer, who will then turn them over the meet Medical Director on the first day of the competition.
2) Carry all their country’s MIF’s and declinations to the competition and personally deliver them to the Medical Director on the first day of the competition.
No registration will be accepted unless one of the two options has been completed!
10
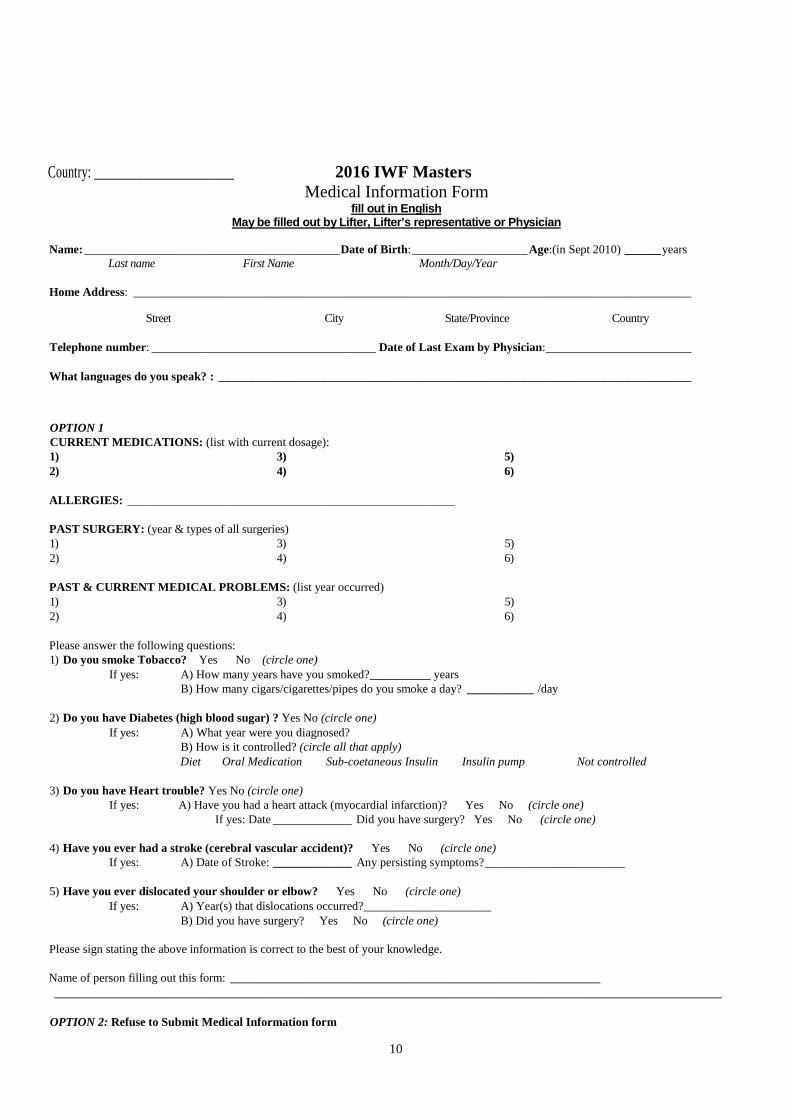
Country: _______________________ 2016 IWF Masters
Medical Information Form fill out in English
May be filled out by Lifter, Lifter’s representativ e or Physician
Name: __________________________________________ Date of Birth: ___________________ Age:(in Sept 2010) ______ years Last name First Name Month/Day/Year
Home Address: ____________________________________________________________________________________________
Street City State/Province Country
Telephone number: _____________________________________ Date of Last Exam by Physician: ________________________
What languages do you speak? : ______________________________________________________________________________
OPTION 1 CURRENT MEDICATIONS: (list with current dosage): 1) 3) 5) 2) 4) 6)
ALLERGIES: ______________________________________________________
PAST SURGERY: (year & types of all surgeries) 1) 3) 5) 2) 4) 6)
PAST & CURRENT MEDICAL PROBLEMS: (list year occurred) 1) 3) 5) 2) 4) 6)
Please answer the following questions: 1) Do you smoke Tobacco? Yes No (circle one)
If yes: A) How many years have you smoked? __________ years B) How many cigars/cigarettes/pipes do you smoke a day? ___________ /day
2) Do you have Diabetes (high blood sugar) ? Yes No (circle one) If yes: A) What year were you diagnosed?
B) How is it controlled? (circle all that apply) Diet Oral Medication Sub-coetaneous Insulin Insulin pump Not controlled
3) Do you have Heart trouble? Yes No (circle one) If yes: A) Have you had a heart attack (myocardial infarction)? Yes No (circle one)
If yes: Date _____________ Did you have surgery? Yes No (circle one)
4) Have you ever had a stroke (cerebral vascular accident)? Yes No (circle one) If yes: A) Date of Stroke: _____________ Any persisting symptoms? _______________________
5) Have you ever dislocated your shoulder or elbow? Yes No (circle one) If yes: A) Year(s) that dislocations occurred? _____________________
B) Did you have surgery? Yes No (circle one)
Please sign stating the above information is correct to the best of your knowledge.
Name of person filling out this form: _____________________________________________________________ ______________________________________________________________________________________________________________
OPTION 2: Refuse to Submit Medical Information form

11
/ decline filling out the medical information form and realize that by choosing not to share my health information it may impair my potential treatment by medical personnel if injured or ill at the competition.
Signature of athlete: _____________________________________ date _______________
At every international IWF Masters championship doping
control will be conducted!!!
How can you spare yourself from an unnecessary positive Doping result?? 1) BE FAIR!
Be part of the example that believes clean sport is one of the fairest and most powerful tools for positive change and growth on that embraces fair play and respect. 2) You are entitled to be sick, but don’t get caugh t! Other prohibited substances are often found in medications you can buy at the pharmacy without prescription so if you have a cold etc. YOU must check first before taking any medication. Even in your country your usual medication can change anytime with added substances. You need to read and/or ask your physician each time you open a new package, whether no changes have been made to your usual medication. 3) What should you do if you get sick while travell ing in a foreign country? Medications are usually commercialized under different names in different countries, and even if they have the same brand names, they may have a different composition in order to respect each country's laws on availability of certain substances. You need to make a little research or consulting your physician. Check yourself at the WADA website: www.wada-ama.org and IWF website under Anti Doping section: http://www.iwf.net/anti-doping/rules 4) TUE APPLICATION PROCESS:
YOU CAN FIND A TUE FORM TRHOUGH YOUR NATIONAL WEIGH TLIFTING BODY; FROM THE
MASTERS ENTRY FORM or FROM OUR MASTERS WEBSITE: www.europeanmasterswl.com + www.iwfmasters.net
12
IWF-Masters Anti-Doping Sub Committee
Therapeutic Use Exemptions
TUE – 2016
A) An Athlete who needs a TUE should apply as soon as possible. For substances prohibited In-Competition only, the Athlete should apply for a TUE at least 30 days before his/her next Competition, unless it is an
emergency or exceptional situation. The Athlete should apply to his/her National Anti-Doping Organization,
International Federation and/or a Major Event Organization (as applicable), using the TUE application form
provided.
Standard TUE
For all other substances and methods, a standard TU E form is required.
The following medical evidence is required: • History of medical condition • Evidence of diagnosis (such as hospital review lett ers, test results, examinations and investigations) • Evidence of using alternative permitted medications
Any TUE is valid for four (4) years by the IWF Masters Anti Doping committee. If an athlete has a TUE
granted for life, he will be asked to provide an updated medical report every 4 years until otherwise
noted.
B) Medical conditions and TUEs
Certain medical conditions are more likely to require Certain medical conditions are more likely to require Certain medical conditions are more likely to require Certain medical conditions are more likely to require medications that will be on the Prohibited medications that will be on the Prohibited medications that will be on the Prohibited medications that will be on the Prohibited
List, or have special conditions on their use.List, or have special conditions on their use.List, or have special conditions on their use.List, or have special conditions on their use.
You HAVE TO APPLY FOR A TUE.You HAVE TO APPLY FOR A TUE.You HAVE TO APPLY FOR A TUE.You HAVE TO APPLY FOR A TUE.
Asthma and asthma medications (BetaAsthma and asthma medications (BetaAsthma and asthma medications (BetaAsthma and asthma medications (Beta----2 agonists)2 agonists)2 agonists)2 agonists)
ADHDADHDADHDADHD
HypertensionHypertensionHypertensionHypertension

13
RETROACTIVE TUE APPLICATION PROCESS SHORTLY BEFORE OR
DURING COMPETITION:
C) An Athlete may only be granted retroactive approval for his/her Therapeutic Use of a Prohibited Substance or Prohibited Method (i.e., a retroactive TUE) if: - a. Emergency treatment or treatment of an acute medical condition was necessary; - b. Due to other exceptional circumstances, there was insufficient time or opportunity for the Athlete to submit, or for the TUEC to consider, an application for the TUE prior to Sample collection.
THE RETROACTIVE TUE APPLICATION, IF GRANTED, IS ONLY VALID FOR THE CURRENT
COMPETITION!
MEANING IT WILL EXPIRE IMMEDIATELY AFTER THE LAST DAY OF THE NEAREST DATED
COMPETITION!
The IWF Masters Anti Doping Sub Committee expects all participants selected for drug testing, who are using therapeutic medicine to submit an IWF Masters TUE or WADA TUE Form and a medical report signed and stamped by their doctor to the Doping Control Officer at the time of the test. A TUE form and the medical report from the athletes physician will be checked through only by a positive result. CAUTION: Applying for a Masters TUE Form doesn’t automatic mean that it is granted. The IWF Masters Anti-Doping Sub Committee will at its discretion seek the advice and assistance of an appointed qualified medical practitioner to verify that an alternative therapy is not available. The IWF Masters Anti-Doping Sub Committee may at its discretion seek the advice and assistance of the appointed qualified medical practitioner to enable a decision to be reached in the hearing. Where therapeutic/inadvertent use of a banned substance or substances is proven, the IWF Masters Anti-Doping Sub Committee may:
1. take no further action, 2. provide counseling and take no additional action, or 3. impose a suitable sanction.
Incomplete Applications will be returned and will need to be
totally resubmitted.
The IWF Masters TUE Form and your physician’s report is to hand over only to the Doping
officer if you have been selected for doping control.
The 2 documents are invalid after 4 years from the date and year of the TUE form and the
doctor’s report which must be identical.

14
Please note that only a physician should fill out the (IWF Masters) TUE Form!!
The IWF Masters Anti Doping Sub Committee accepts the 2 documents only if it is filled out,
stamped and signed by the same physician.
At every International Masters Championship you must bring a copy of your TUE Form and
report in case you will be selected for dope testing.
Note: The refusal by a participant to provide a sample will make any medical certificate inadmissible. Any refusal to provide a sample will be an automatic positive result and will be punished with a 4 year ban from your sport.
BEWARE OF SUPPLEMENTS! EDUCATE YOURSELF!
From 1 January 2015 the risks associated with suppl ement use increase as bans could get longer. • There is no guarantee that any supplement product is free from banned substances • You are strongly advised to be very cautious if you choose to use any supplement product
• You must undertake thorough internet research of any supplement products before use, including the name of
the product and the ingredients/substances listed. Information revealed as a result should be further investigated and we advise athletes to keep evidence of their research
What are the risks? • Supplements can contain banned substances • Contamination (where banned substances are accidentally mixed in with the supplement) can occur during the
manufacturing process • Ingredients on the label may be listed differently to how they are shown on the Prohibited List
• Supplements may be sold as counterfeit products. The risk of fake supplement products is greatest when buying
over the internet • A label saying ‘Safe for Sports People’, or ‘Approved by WADA ‘ is meaningless. WADA do not approve any
supplement products
Our advice Before you take a supplement you should: • assess the need - all athletes should seek advice from a medical professional or nutritionist on their need to use
supplement products • assess the risk - undertake thorough research of all supplement products you are considering taking
• assess the consequences - you could receive a four-year ban
You can reduce the risks by: • undertaking thorough internet research
• only using batch-tested products • checking on the Informed-Sport risk minimisation programme that a supplement has been batch-tested or
contact your National Anti Doping Organization
All athletes are advised to be vigilant in using any supplement. No guarantee can be given that any particular supplement is free from prohibited substances. An important principle of the Code is that of strict liability, which states that athletes are solely responsible for any prohibited substances they use, attempt to use or is found in their system regardless of how it got there and if there was an intention to cheat. Before taking supplements, athletes must therefore assess the need, risk and consequences to their careers. Diet, lifestyle and training should all be optimised before athletes consider supplements and they should always consult a medical professional or nutritionist and seek advice.

15
Supplements may claim to be drug-free or safe for drug-tested athletes. It is not possible to guarantee that specific supplements will be free of prohibited substances and athletes can only reduce the risk of inadvertent doping by making informed decisions. There is an array of supplements available for athletes to purchase that have no prohibited substances listed as ingredients. Despite this, there have been several cases whereby supplement products have been contaminated with prohibited substances as defined by the World Anti-Doping Code (the Code) Prohibited List. In the UK, LGC has taken the initiative to create a scheme to support athletes in assessing the risk. The Informed-Sport programme is designed to evaluate supplement manufacturers for their process integrity and screening of supplements and raw ingredients for the presence of substances that are on the WADA Prohibited List. For further information, visit the Informed-Sport website. The IWF Masters believes this risk minimisation service to be a positive step and welcomes the approach being taken by industry and the LGC Informed-Sport programme. However, we wish to remind athletes that strict liability will still apply and the appropriate sanctions imposed on any athlete returning an adverse analytical finding from any supplement product, as with all other cases of doping.
THE 2015 IWF ANTI DOPING CODE STATES THAT YOU are responsible for what is in your system and the Punishment for a positive RESULT, ESPECIALLY ANABOLIC SUBSTANCES are a 4 year ban from your sport.
IWF MASTERS Anti Doping Sub Committee: Denise Offerman: [email protected] + [email protected]
DECLARATION: I hereby declare that I read and understand all the above and acknowledge with my signature:
NATION:____________________________________________ FULL NAME:___________________________________________________ DATE:______________________ SIGNATURE:___________________________________________________
16
THERAPEUTIC/INADVERTENT USAGE OF BANNED SUBSTANCES Participants subjected to drug testing who give an adverse analytical finding for the use of a banned substance or substances, and who have a medical certificate issued to them by a qualified medical practitioner may:
1. Refer the medical certificate to the appointed Anti-Doping Commission hearing. 2. Provide additional verifying facts and information that may support the particulars in the medical certificate and
substantiate the use of such banned substance or substances by the participant for therapeutic and/or medical purposes only.
3. Complete the attached TUE form and submit with a medical certificate from their doctor. 4. Your application does not necessarily guarantee acceptance.
The IWF Masters Anti Doping Sub Committee expect all participants selected for drug testing who are using therapeutic medicine to submit an IWF Masters TUE Form and a medical certificate from their doctor to the Doping Control Officer at the time of the test. Keep these documents with you at championships and produce them if selected for testing. The IWF Masters Anti-Doping Sub Committee may at its discretion seek the advice and assistance of the appointed qualified medical practitioner to enable a decision to be reached in the hearing. Where therapeutic/inadvertent use of a banned substance or substances is proven, the IWF Masters Anti-Doping Commission may:
4. take no further action, 5. provide counseling and take no additional action, or 6. impose a suitable sanction.
Note: The refusal by a participant to provide a sample will make any medical certificate inadmissible. EDUCATION: The IWF Masters will promote the education of Masters participants with regard to drugs in Sports. In particular, the IWF Masters will affirm that no one should cease taking prescribed medication to compete in any IWF Masters sanctioned event unless their personal physician recommends they cease the medication.
17
IWF-Masters Anti-Doping Committee Therapeutic Use Exemptions
TUE - 2016 Appendix 1
Please complete all sections, both sides, in capital letters or typing 1. ATHLETE INFORMATION: Surname (Family Name): ____________________________ ____________ Given Names: ____________________________________ ____
Date of Birth (d/m/y): ______________________________ Female □ Male □ Street Address : __________________________________________________ City: ____________________ State/Province: ___________________Country: ________ ________ Postal-code: _______________ Telephone: (country code) ______________________________ E-mail: _________________________@_________________ ________ National Sport Organization : Name, Address , & e-mail: ______________________________ _____________________________________________________________________________ 2. MEDICAL INFORMATION:
Diagnosis with sufficient medical information (see Note: next section): …………………………………………………………………………………………..............................…………… …………………………………………………………………………………………………………..……................. ………………………………………………………………………………………………………..…………………..... …………………………….……………………………………………………………………………………..……….... If there are any “permitted medication/s” that are indicated, or being used, in the treatment of this type of medical condition, provide clinical justification for the r equested use of the “prohibited” medication. …………………………………………………………………………………….............................…………………. …………………………………………………………………………………………………………............................ ………………………………………………………………………………………………………..………………….....
NOTE: Diagnosis
Evidence confirming the diagnosis must be attached and forwarded with this applicatio n. The medical evidence should include a comprehensive medical history and the results of all relevant examinations, laboratory investigations and imaging studies. Copies of the original reports or letters should be included when possible. Evidence should be as objective as possible in the clinical circumstances and in the case of non-demonstrable conditions independent supporting medical opinion will assist this application.
18
3. MEDICATION DETAILS: Generic Name -- mandatory Prohibited substance(s)
Dose Route Frequency
Intended duration of treatment: (Please tick appropriate box)
Once only □ Emergency□ Ongoing Duration □ state length: (week/s—month/s): ……………………start date: ……………………
Have you previously submitted any TUE applications?: yes □ no □ Which substance(s)?
……………………………..To whom?……………………………When?…………………Approved □ Not approved □
……………………………..To whom?……………………………When?…………………Approved □ Not approved 4. MEDICAL PRACTITIONER’S DECLARATION: ( Please attach page from prescription pad) I certify that the above-mentioned treatment is medically appropriate/necessary and that the use of alternative medication, that is not on the prohibited list, would be unsatisfactory for this condition. Name:……………………………………………………..................................................... Medical Specialty: ______________________________ Degree: _________________________________ Address: __________________________________________ _____________________________________ Tel.: (country code) ______________________ Fax: _______________________________ E-mail: __________________________________________ ___ Signature of Medical Practitioner: ________________ ___________________ .Date: _________________________
5. ATHLETE’S DECLARATION: I, ________________________________________ certify that the information under section “1.” Is accurate and that I am requesting approval to use a Substance or Method from the WADA Prohibited List. I authorize the release of personal medical information to the IWF and its representative Anti-Doping Organization/s (ADO) as well as to WADA staff, to the WADA TUEC (Therapeutic Use Exemption Committee) and to other ADO’s under the provisions of the Code. I understand that if I ever wish to revoke the right of these organizations to obtain my health information on my behalf, I must notify my medical practitioner and my ADO/s in writing of that fact.
Athlete’s signature: ______________________________ Date: __________________
Incomplete Applications will be returned and will need to be totally resubmitted. Please submit the completed form to the applicable