2017 american college of rheumatology guideline … 2017, american college of rheumatology ......
TRANSCRIPT
ARTHRITIS & RHEUMATOLOGY
Vol. 69, No. 8, August 2017, pp 1521–1537
DOI 10.1002/art.40137
VC 2017, American College of Rheumatology
SPECIAL ARTICLE
2017 American College of Rheumatology Guidelinefor the Prevention and Treatment ofGlucocorticoid-Induced Osteoporosis
Lenore Buckley,1 Gordon Guyatt,2 Howard A. Fink,3 Michael Cannon,4 Jennifer Grossman,5
Karen E. Hansen,6 Mary Beth Humphrey,7 Nancy E. Lane,8 Marina Magrey,9 Marc Miller,10
Lake Morrison,11 Madhumathi Rao,12 Angela Byun Robinson,13 Sumona Saha,6 Susan Wolver,14
Raveendhara R. Bannuru,12 Elizaveta Vaysbrot,12 Mikala Osani,12 Marat Turgunbaev,15
Amy S. Miller,15 and Timothy McAlindon12
Guidelines and recommendations developed and/or endorsed by the American College of Rheumatology(ACR) are intended to provide guidance for particular patterns of practice and not to dictate the care of aparticular patient. The ACR considers adherence to the recommendations within this guideline to be vol-untary, with the ultimate determination regarding their application to be made by the physician in light ofeach patient’s individual circumstances. Guidelines and recommendations are intended to promote benefi-cial or desirable outcomes but cannot guarantee any specific outcome. Guidelines and recommendationsdeveloped and endorsed by the ACR are subject to periodic revision as warranted by the evolution of medi-cal knowledge, technology, and practice. ACR recommendations are not intended to dictate payment orinsurance decisions. These recommendations cannot adequately convey all uncertainties and nuances ofpatient care.
The American College of Rheumatology is an independent, professional, medical and scientific society thatdoes not guarantee, warrant, or endorse any commercial product or service.
This article is published simultaneously in Arthritis Care &Research.
The views expressed herein are those of the authors and donot necessarily reflect the position or policy of the Department ofVeterans Affairs or the United States government.
Supported by the American College of Rheumatology.1Lenore Buckley, MD, MPH: Yale University, New Haven,
Connecticut; 2Gordon Guyatt, MD: McMaster University, Hamilton,Ontario, Canada; 3Howard A. Fink, MD, MPH: Geriatric ResearchEducation and Clinical Center, VA Health Care System, Minneapolis,Minnesota; 4Michael Cannon, MD: Arthritis Consultants of Tidewa-ter, Virginia Beach, Virginia; 5Jennifer Grossman, MD: University ofCalifornia, Los Angeles; 6Karen E. Hansen, MD, MS, Sumona Saha,MD: University of Wisconsin, Madison; 7Mary Beth Humphrey, MD,PhD: Oklahoma University Health Sciences Center, Oklahoma City;8Nancy E. Lane, MD: University of California Davis, Sacramento;9Marina Magrey, MD: Case Western Reserve University, Metro-Health System, Cleveland, Ohio; 10Marc Miller, MD: RheumatologyAssociates, Portland, Maine; 11Lake Morrison, MD: Duke UniversityMedical Center, Durham, North Carolina; 12Madhumathi Rao, MD,
Raveendhara R. Bannuru, MD, PhD, Elizaveta Vaysbrot, MD,MS, Mikala Osani, Timothy McAlindon, MD, MPH: Tufts MedicalCenter, Boston, Massachusetts; 13Angela Byun Robinson, MD,MPH: Rainbow Babies and Children’s Hospital, Cleveland, Ohio;14Susan Wolver, MD: Virginia Commonwealth University, Richmond;15Marat Turgunbaev, MD, MPH, Amy S. Miller: American College ofRheumatology, Atlanta, Georgia.
Dr. Cannon has received honoraria from Takeda (less than$10,000). Dr. Hansen has received research grants from Takeda andMerck Sharpe & Dohme. Dr. Lane has received consulting fees fromMerck (less than $10,000) and has served as an expert witness on behalfof Novartis. Dr. Saha has received consulting fees from UCB Biosciences(more than $10,000). Dr. McAlindon has received consulting fees fromPfizer (less than $10,000).
Address correspondence to Lenore Buckley, MD, MPH,Yale University, 300 Cedar Street, TAC #S517, New Haven, CT06520. E-mail: [email protected].
Submitted for publication August 26, 2016; accepted inrevised form April 20, 2017.
1521

Objective. To develop recommendations for pre-vention and treatment of glucocorticoid-induced osteo-porosis (GIOP).
Methods. We conducted a systematic review tosynthesize the evidence for the benefits and harms ofGIOP prevention and treatment options. The Grading ofRecommendations Assessment, Development and Eval-uation methodology was used to rate the quality of evi-dence. We used a group consensus process to determinethe final recommendations and grade their strength.The guideline addresses initial assessment and reassess-ment in patients beginning or continuing long-term (‡3months) glucocorticoid (GC) treatment, as well as therelative benefits and harms of lifestyle modification andof calcium, vitamin D, bisphosphonate, raloxifene, teri-paratide, and denosumab treatment in the general adultpopulation receiving long-term GC treatment, as well asin special populations of long-term GC users.
Results. Because of limited evidence regardingthe benefits and harms of interventions in GC users,most recommendations in this guideline are conditional(uncertain balance between benefits and harms). Rec-ommendations include treating only with calcium andvitamin D in adults at low fracture risk, treating withcalcium and vitamin D plus an additional osteoporosismedication (oral bisphosphonate preferred) in adults atmoderate-to-high fracture risk, continuing calcium plusvitamin D but switching from an oral bisphosphonate toanother antifracture medication in adults in whom oralbisphosphonate treatment is not appropriate, and con-tinuing oral bisphosphonate treatment or switching toanother antifracture medication in adults who completea planned oral bisphosphonate regimen but continue toreceive GC treatment. Recommendations for specialpopulations, including children, people with organ trans-plants, women of childbearing potential, and peoplereceiving very high-dose GC treatment, are also made.
Conclusion. This guideline provides direction forclinicians and patients making treatment decisions. Cli-nicians and patients should use a shared decision-making process that accounts for patients’ values, pref-erences, and comorbidities. These recommendationsshould not be used to limit or deny access to therapies.
INTRODUCTION
Glucocorticoids (GCs) play an important role inthe treatment of many inflammatory conditions. It is esti-mated that 1% of the US population is treated long-termwith GCs (1). However, GC use causes significant toxic-ity, including bone loss and fractures (2,3). More than
10% of patients who receive long-term GC treatment arediagnosed with a fracture, and 30–40% have radio-graphic evidence of vertebral fractures (4,5). The highestrate of bone loss occurs within the first 3–6 months of GCtreatment, and a slower decline continues with persistentuse (6). Both high daily and high cumulative GC dosesincrease risk of fracture, particularly vertebral fracture,due to the greater effects of GCs on trabecular bone thanon cortical bone. Risk factors for GC-induced fractureinclude low bone strength at the beginning of GC treat-ment and the rate of decline in bone mass during treat-ment, which is largely determined by the dose andduration of GC use. In children, GC treatment alsoaffects bone strength, growth, and total adult skeletalmass, with a similar profile of risk factors (7–10).
However, GC treatment is a potentially revers-ible risk factor for glucocorticoid-induced osteoporosis(GIOP); if GC treatment is terminated, bone mineraldensity (BMD) increases and fracture risk declines(6,11,12). In addition, the absolute risk of future frac-ture in an individual is substantially influenced by demo-graphic and other characteristics (age, race, sex, andconcomitant OP risk factors). For these reasons, it isimportant to identify those patients taking GCs forwhom the benefits of preventive therapy sufficiently out-weigh potential harms.
Numerous risk calculators can be applied in clini-cal practice to provide estimates of risk of major OPfracture and hip fracture clinically diagnosed, withadjustment for GC dose in some but not all calculators(13–15). Most stratify GC use into 2 categories: low(prednisone #7.5 mg/day) or high (.7.5 mg/day), basedon data from clinical trials and epidemiologic studies(15,16) demonstrating increasing fracture risk with higherdaily doses. However, these calculators may underesti-mate the fracture risk in patients with prolonged treat-ment with very high doses of GCs for conditions such asgiant cell arteritis, vasculitis, lupus, and dermatomyositis(16,17). Van Staa et al reported a marked increase in rela-tive risk of vertebral and hip fractures in patients who hadreceived treatment with prednisolone $30 mg/day with acumulative dose of .5 gm (15).
There are insufficient data to develop individualprediction tools for children and for adults ,40 years ofage. Nevertheless, observational data indicate a substan-tial risk of clinically diagnosed vertebral fracture amongpremenopausal women $30 years of age receiving veryhigh doses of GCs (10-year risk 5–20%) (18–25).
Despite increasing information about risk factorsfor fracture in GC users and the availability of effectivetherapies to prevent fracture, many long-term GC usersnever receive therapy to prevent bone loss or are treated
1522 BUCKLEY ET AL

only after a fracture has occurred (26,27). The AmericanCollege of Rheumatology (ACR) identified GIOP as animportant public health issue and first published recom-mendations for its prevention and treatment in 1996 (28).The ACR updated these guidelines in 2001 and 2010, asnew techniques for assessing fracture risk and new infor-mation about risk factors and therapies became available(28–30). The present ACR guideline outlines the treat-ment recommendations for GIOP. The guideline wasdeveloped using the Grading of Recommendations As-sessment, Development and Evaluation (GRADE) ap-proach (see below) and included therapies for thetreatment of OP approved by the US Food and DrugAdministration before 2015. No other therapies have beenapproved as of the time of publication of these guidelines.
METHODS
Methodology overview. We developed this guidelineaccording to the ACR guideline development process (http://www.rheumatology.org/Practice-Quality/Clinical-Support/Clini-cal-Practice-Guidelines). This process includes the GRADEmethodology (www.gradeworkinggroup.org) (31–33). Conflictsof interest and disclosures were determined and managedaccording to ACR policy (https://www.rheumatology.org/Portals/0/Files/GIOP-Guidelines-Disclosure-Summary.pdf). The fullmethods are described in detail in Supplementary Appendix 1(available on the Arthritis & Rheumatology web site at http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract). Thiswork involved 4 teams: 1) a Core Leadership Team (4 members),which supervised and coordinated the project and drafted theclinical questions and manuscript; 2) a Literature ReviewTeam, which completed the literature search and abstraction;3) an Expert Panel, which developed the clinical questions(PICO [population/intervention/comparator/outcomes] ques-tions) and the scope of the guideline project; and 4) a VotingPanel, which included adult and pediatric rheumatologists,internists, a nephrologist, a pulmonologist, a gastroenterolo-gist, medical specialists with clinical expertise in treatingGIOP, and a patient who provided input from the patientperspective and voted on the recommendations. Rosters ofthe team and panel members are shown in SupplementaryAppendix 2 (http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract).
Framework for the GIOP guideline development. ThePanel ranked fracture (hip, vertebral, nonvertebral) as thecritically important outcome measure for treatment evaluation.Important outcome measures included adverse effects oftreatments, in particular the incidence of serious and totaladverse events (see Supplementary Appendix 3 [http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract] for alist of adverse events).
At the initial meeting, the Voting Panel and ExpertPanel agreed that the scope of the project should be theassessment, prevention, and treatment of OP and fractures inchildren and adults taking glucocorticoids (prednisone at.2.5 mg/day for $3 months), including patients with organtransplants, women of childbearing potential, and peoplereceiving very high-dose GCs. Treatment of people using
inhaled GCs and those with a glomerular filtration rate of,30 ml/minute were not addressed in these guidelines.
Adult men and women were divided into 2 groupsbased on age ($40 years or ,40 years). After population riskgroups were defined, interventions and comparators for eachclinical scenario were specified using a PICO question (see listof PICO questions in Supplementary Appendix 3). PICOquestions included assessment and reassessment of fracturerisks, treatment comparisons, and questions about durationand reassessment of treatment. When it was necessary to useBMD to support a recommendation (which was the case inonly 4 PICO questions, all addressing pediatric patients withGIOP), the Voting Panel downgraded the quality of evidencefor indirectness, since BMD provides only indirect evidence ofthe impact on fracture.
Systematic synthesis of the literature. We performedsystematic searches of the published English-language litera-ture including OVID Medline, PubMed, Embase, and theCochrane Library (including Cochrane Database of SystematicReviews, Database of Abstracts of Reviews of Effects,Cochrane Central Register of Controlled Trials, and HealthTechnology Assessments) from the beginning of each databasethrough October 6, 2015 (Supplementary Appendix 4, on theArthritis & Rheumatology web site at http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract), and update searches wereconducted on April 23, 2016. We performed duplicate screen-ing of literature search results using DistillerSR software(https://distillercer.com/products/distillersr-systematic-review-software/) (Supplementary Appendix 5, http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract). Data were extractedinto RevMan software (http://tech.cochrane.org/revman), andthe quality of each study was evaluated using the Cochranerisk of bias tool (http://handbook.cochrane.org/). We exportedRevMan files into GRADEpro software to formulate aGRADE summary of findings table (Supplementary Appendix3) for each PICO question (34). The overall quality of evidencewas evaluated using GRADE quality assessment criteria (31).
In clinical scenarios not addressed by data from ran-domized clinical trials, data from observational cohort studieswere used to estimate relative effects. In situations in whichthe question had not been tested in a sample of patients takingGCs but had been tested in a non-GIOP population, weapplied the relative risk values from that study, making theassumption that the effect was generalizable, but wedowngraded the quality of evidence for indirectness.
We projected absolute risk reduction within each riskstratum according to hypothetical baseline fracture risk rang-ing from 1% to 20%. The following cut points were used tostratify levels of risk: ,5% incidence of vertebral fracturesover 5 years, between 5% and ,10%, and $10%. The VotingPanel then made recommendations based on absolute fracturereduction with treatment in each of these strata. We focusedon vertebral fracture rates because this outcome was moreconsistently reported in the literature and because of thegreater effects of GCs on trabecular bone.
Moving from evidence to recommendations. GRADEmethodology specifies that panels make recommendationsbased on the balance of relative benefits and harms of thetreatment options under consideration, the quality of the evi-dence (i.e., confidence in the effect estimates), and patients’values and preferences. Key to the recommendation is the
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1523

tradeoff between desirable and undesirable outcomes andcost; recommendations require estimating the relative valuepatients place on the outcomes. We are unaware of publishedliterature exploring patient values and preferences regardingthese issues. Our judgments were based on the experience ofthe Panel members (which included a patient) in shareddecision-making with their patients. Below we outline the Vot-ing Panel’s assessment of these tradeoffs that informed thefinal recommendations.
Consensus building. The Voting Panel voted on thedirection and strength of the recommendation related to eachPICO question. An 80% level of agreement was used as thethreshold for a recommendation; if 80% agreement was notachieved during an initial vote, the Panel members held addi-tional discussions before re-voting. Consistent with GRADEguidance, in some instances the Voting Panel chose to providea strong recommendation despite a low quality rating of evi-dence (33). In such cases, a written explanation is provided,describing the reasons for this decision.
Moving from recommendations to practice. Whenapplying these risk-stratified recommendations in clinicalsettings, adults $40 years of age receiving long-term GCsshould be designated as being at moderate-to-high risk or lowrisk of fracture (Table 1) based on BMD, history of fracture, and10-year risk of major OP fracture and hip fracture calculatedusing a tool that combines risk factors with GC dose. Althoughmany tools that incorporate GC use are available, the VotingPanel suggested using FRAX (https://www.shef.ac.uk/FRAX/tool.jsp) for fracture risk assessment. When GC use is includedas a risk factor in FRAX, the fracture risk generated is the
risk associated with a prednisolone dose of 2.5–7.5 mg/day(prednisolone and prednisone doses are nearly equivalent).For people receiving doses of .7.5 mg/day, the fracture riskgenerated with FRAX should be increased by a relative 15%for major osteoporotic fracture and 20% for hip fracture risk(13). For example, if the 10-year hip fracture risk is 2.0% withGC use entered in FRAX, the risk estimate should be increasedto 2.4% if the prednisone dose is .7.5 mg.
There are no tools available to estimate absolute frac-ture risk in children or in adults ,40 years of age. Thesegroups were considered to be at high fracture risk if they havepreviously sustained an OP fracture. The Voting Panel desig-nated men and women ,40 years of age to be at moderate riskif they were expected to continue GC treatment at .7.5 mg/day for 6 months and had either 1) a hip or spine BMD Zscore of ,23 or 2) a rapid decline in hip or spine BMD(equivalent to $10% in 1 year) during GC treatment.
RESULTS/RECOMMENDATIONS
How to interpret the recommendations
1. The Voting Panel’s assessment was that patientswould be willing to take calcium and vitamin D withonly a very small absolute risk reduction, that all orvirtually all would be willing to take bisphos-phonates to achieve a 5-year absolute reduction invertebral fracture risk of 5%, and that most wouldchoose to take oral bisphosphonates if the fracture
Table 1. Fracture risk categories in GC-treated patients
Adults $40 years of age Adults ,40 years of age
High fracture risk Prior osteoporotic fracture(s)Hip or spine bone mineral density
T score #22.5 in men age$50 years and postmenopausalwomen
FRAX* (GC-adjusted†) 10-yearrisk of major osteoporoticfracture‡ $20%
FRAX* (GC-adjusted†) 10-yearrisk of hip fracture $3%
Prior osteoporotic fracture(s)
Moderate fracture risk FRAX* (GC-adjusted†) 10-yearrisk of major osteoporoticfracture‡ 10–19%
FRAX* (GC-adjusted†) 10-yearrisk of hip fracture .1% and,3%
Hip or spine bone mineraldensity Z score ,23orrapid bone loss ($10% at thehip or spine over 1 year)
andContinuing GC treatment at
$7.5 mg/day for $6 months
Low fracture risk FRAX* (GC-adjusted†) 10-yearrisk of major osteoporoticfracture‡ ,10%
FRAX* (GC-adjusted†) 10-yearrisk of hip fracture #1%
None of above risk factors otherthan GC treatment
* https//www.shef.ac.uk/FRAX/tool.jsp.† Increase the risk generated with FRAX by 1.15 for major osteoporotic fracture and 1.2 for hip fractureif glucocorticoid (GC) treatment is .7.5 mg/day (e.g., if hip fracture risk is 2.0%, increase to 2.4%).‡ Major osteoporotic fracture includes fractures of the spine (clinical), hip, wrist, or humerus.
1524 BUCKLEY ET AL
reduction were $3% to ,5% (leading to a condi-tional recommendation in favor). The 5-year timeperiod was chosen because few clinical trials havedata on fracture risk reduction past 3–5 years. Fur-ther, the Panel members thought that mostpatients would decline oral bisphosphonates with
an absolute reduction in 5-year risk of vertebralfractures of 1.6–2.9% (leading to a conditional rec-ommendation against), and all or virtually all woulddecline if the risk reduction were ,1.5% (leading,in the presence of high- or moderate-quality evi-dence, to a strong recommendation against).
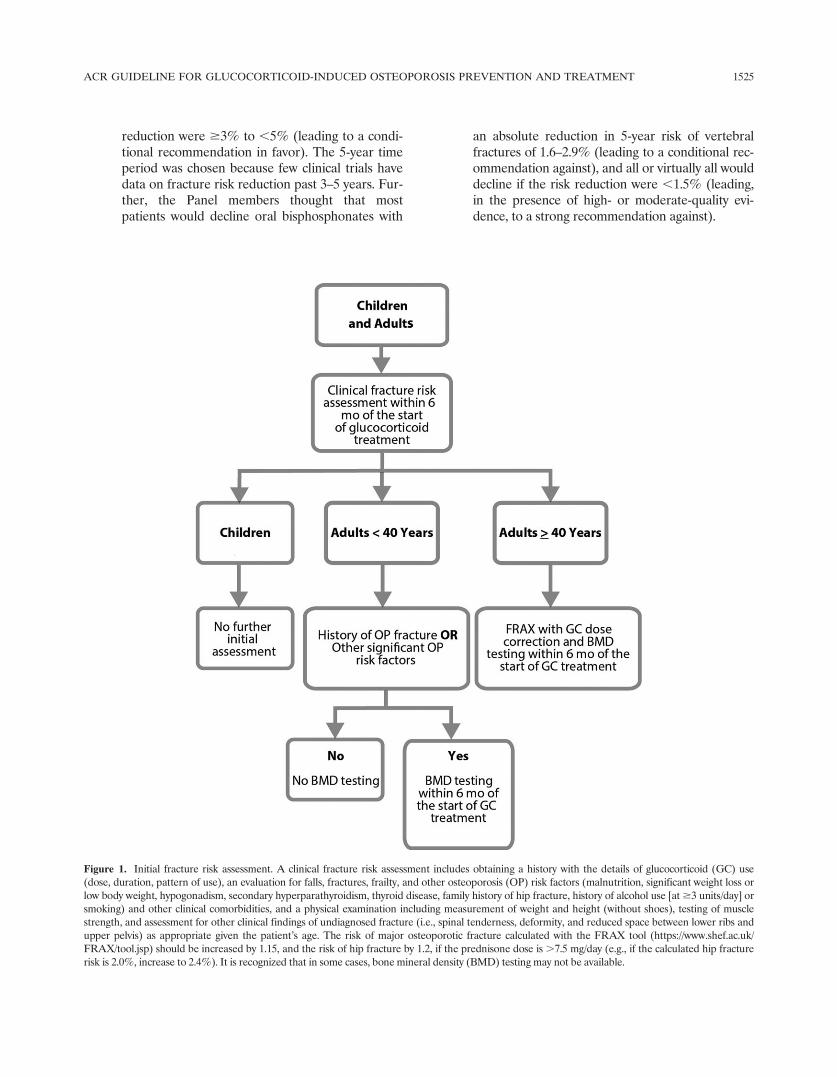
Figure 1. Initial fracture risk assessment. A clinical fracture risk assessment includes obtaining a history with the details of glucocorticoid (GC) use(dose, duration, pattern of use), an evaluation for falls, fractures, frailty, and other osteoporosis (OP) risk factors (malnutrition, significant weight loss orlow body weight, hypogonadism, secondary hyperparathyroidism, thyroid disease, family history of hip fracture, history of alcohol use [at $3 units/day] orsmoking) and other clinical comorbidities, and a physical examination including measurement of weight and height (without shoes), testing of musclestrength, and assessment for other clinical findings of undiagnosed fracture (i.e., spinal tenderness, deformity, and reduced space between lower ribs andupper pelvis) as appropriate given the patient’s age. The risk of major osteoporotic fracture calculated with the FRAX tool (https://www.shef.ac.uk/FRAX/tool.jsp) should be increased by 1.15, and the risk of hip fracture by 1.2, if the prednisone dose is .7.5 mg/day (e.g., if the calculated hip fracturerisk is 2.0%, increase to 2.4%). It is recognized that in some cases, bone mineral density (BMD) testing may not be available.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1525
For intravenous (IV) bisphosphonates, denosu-mab, raloxifene, and teriparatide, which have great-er harms or burden of treatment, the threshold washigher, although the Panel did not specify a thresh-old value. Because raloxifene may increase the riskof death due to stroke in postmenopausal womenwith documented coronary heart disease or atincreased risk of major coronary events and/or mayincrease the risk of deep vein thrombosis and pul-monary embolism (35), and there is no evidence ofits benefit in fracture reduction in GC-treatedpatients, the Voting Panel considered the drug as atreatment option only for postmenopausal womenwith contraindications to all other treatments. Weare unaware of published literature exploringpatient values and preferences regarding theseissues. The judgments are based on the experienceof the Panel members (which included a patient) inshared decision-making with their patients.
2a. A strong recommendation means that the Panel wasconfident that the desirable effects of following therecommendation outweigh the undesirable effects(or vice versa), so the course of action would apply toall or almost all patients, and only a small proportionwould not want to follow the recommendation.
2b. A conditional recommendation means that thePanel believed the desirable effects of followingthe recommendation probably outweigh the unde-sirable effects, so the course of action wouldapply to the majority of the patients, but somemay not want to follow the recommendation.Because of this, conditional recommendations arepreference sensitive and always warrant a shareddecision-making approach.
2c. A good practice recommendation (36) means thatalthough the Panel believed the benefits of proceed-ing according to the guidance far outweigh theharms, the supporting evidence is indirect, and thePanel did not formally assess the relevant evidence.The logic for the good practice statements is asfollows: Appropriate management regarding bonehealth is based on an initial assessment and reas-sessment of fracture risk. However, there are inade-quate data directly addressing outcomes in patientswhose cases were managed with, versus those with-out, initial and follow-up fracture risk assessments.The chain of evidence—limited antifracture treat-ment with limited adverse effects in those at lowrisk; more aggressive antifracture treatment withresultant decrease in fractures in those at highrisk—is nevertheless compelling, though without a
structured review of the evidence for the benefitsand harms, the statement in question does not war-rant a formal GRADE recommendation.
3. For each recommendation, details regarding thePICO questions and the GRADE evidence tablesare listed in Supplementary Appendices 1 and3 (on the Arthritis & Rheumatology web site athttp://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract).
4. Recommendations for BMD testing are based onthe assumption that it is available in the regionwhere the patient receives treatment and thatthere are no significant barriers, including thepatient’s functional status or financial barriers, thatpreclude testing, and that the results are likely tohave an impact on clinical decision-making.
Recommendations for fracture risk assessment andreassessment
Initial fracture risk assessment. All of the frac-ture risk assessment and reassessment recommenda-tions are made as good practice recommendations. Inall adults and children, an initial clinical fracture riskassessment should be performed as soon as possible, butat least within 6 months of the initiation of long-term GCtreatment (Figure 1). This assessment should include ahistory with the details of GC use (dose, duration, pat-tern of use), an evaluation for falls, fractures, frailty,and other risk factors for fracture (malnutrition, signifi-cant weight loss or low body weight, hypogonadism,secondary hyperparathyroidism, thyroid disease, familyhistory of hip fracture, history of alcohol use [at $3units/day] or smoking) and other clinical comorbidities,and a physical examination including measurement ofweight and height (without shoes), testing of musclestrength, and assessment for other clinical findings ofundiagnosed fracture (i.e., spinal tenderness, deformity,and reduced space between lower ribs and upper pelvis)as appropriate given the patient’s age.
In addition, for adults $40 years of age, the initialabsolute fracture risk should be estimated using FRAX(https://www.shef.ac.uk/FRAX/tool.jsp) with the adjust-ment for GC dose and BMD testing (if available, or with-out BMD if it is not available) as soon as possible, but atleast within 6 months of the initiation of GC treatment.
For adults ,40 years of age, BMD testingshould be done as soon as possible but at least within6 months of the initiation of GC treatment if thepatient is at high fracture risk because of a historyof previous OP fracture(s) or if the patient has othersignificant OP risk factors (malnutrition, significant
1526 BUCKLEY ET AL
weight loss or low body weight, hypogonadism, sec-ondary hyperparathyroidism, thyroid disease, familyhistory of hip fracture, smoking, alcohol use at $3units/day).
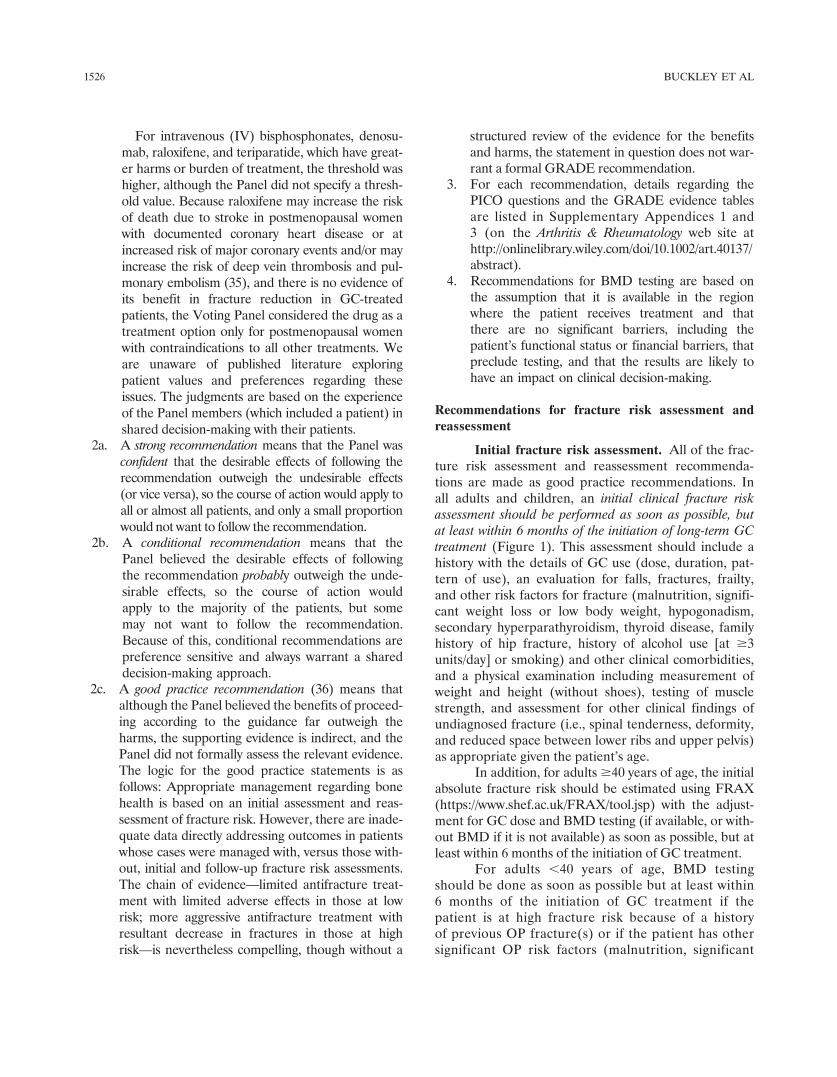
Reassessment of fracture risk. In all adults andchildren who continue GC treatment, a clinical fracture
risk reassessment should be performed every 12 months(Figure 2).
Adults $40 years of age. For adults $40 years ofage who continue GC treatment and are not treatedwith an OP medication beyond calcium and vitamin D,reassessment with FRAX, with BMD testing if available,
Figure 2. Reassessment of fracture risk. A clinical fracture risk reassessment includes obtaining a history with the details of glucocorticoid (GC)use (dose, duration, pattern of use), an evaluation for falls, fractures, frailty, and other osteoporosis (OP) risk factors (malnutrition, significantweight loss or low body weight, hypogonadism, secondary hyperparathyroidism, thyroid disease, family history of hip fracture, history of alcoholuse [at $3 units/day] or smoking) and other clinical comorbidities, and a physical examination including measurement of weight and height(without shoes), testing of muscle strength, and assessment for other clinical findings of undiagnosed fracture (i.e., spinal tenderness, deformity,and reduced space between lower ribs and upper pelvis) as appropriate given the patient’s age. Very high-dose GC treatment was defined astreatment with prednisone $30 mg/day and a cumulative dose of .5 gm in the past year. Reliability of FRAX (https://www.shef.ac.uk/FRAX/tool.jsp) after OP treatment is debated, but FRAX calculation can be repeated in adults age $40 years who have not received treatment. It isrecognized that in some cases, bone mineral density (BMD) testing may not be available.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1527
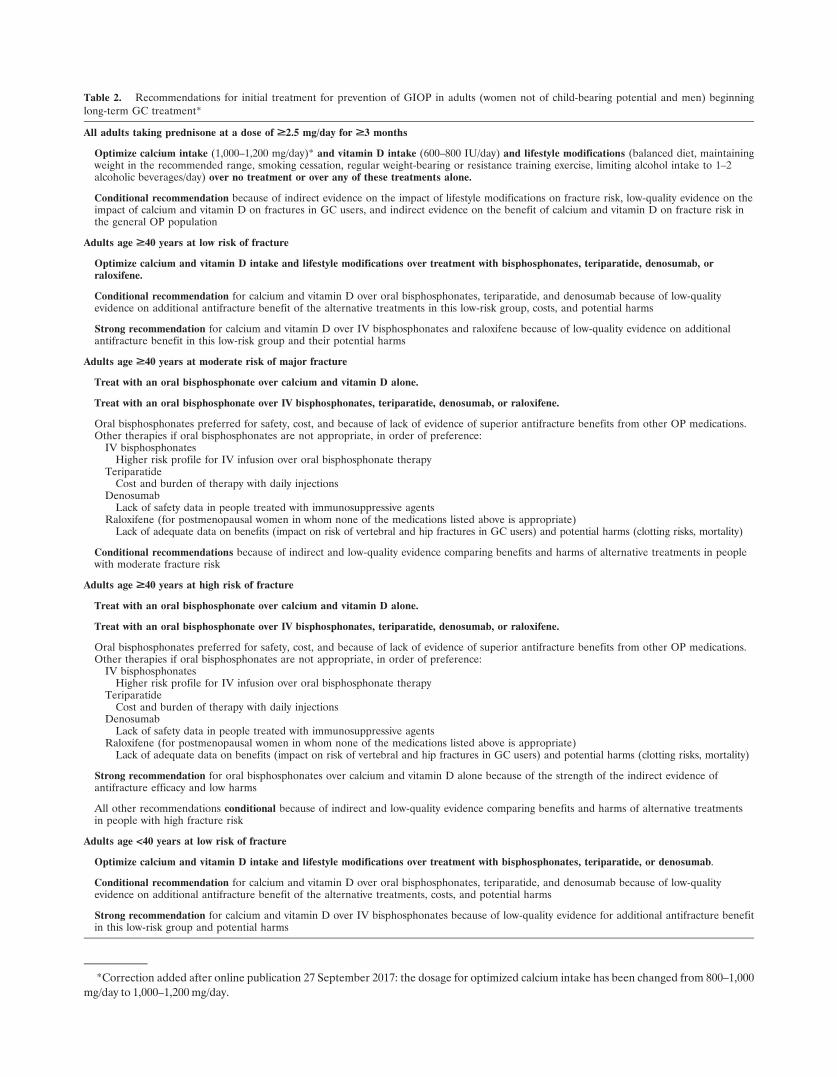
Table 2. Recommendations for initial treatment for prevention of GIOP in adults (women not of child-bearing potential and men) beginninglong-term GC treatment*
All adults taking prednisone at a dose of ‡2.5 mg/day for ‡3 months
Optimize calcium intake (1,000–1,200 mg/day)* and vitamin D intake (600–800 IU/day) and lifestyle modifications (balanced diet, maintainingweight in the recommended range, smoking cessation, regular weight-bearing or resistance training exercise, limiting alcohol intake to 1–2alcoholic beverages/day) over no treatment or over any of these treatments alone.
Conditional recommendation because of indirect evidence on the impact of lifestyle modifications on fracture risk, low-quality evidence on theimpact of calcium and vitamin D on fractures in GC users, and indirect evidence on the benefit of calcium and vitamin D on fracture risk inthe general OP population
Adults age ‡40 years at low risk of fracture
Optimize calcium and vitamin D intake and lifestyle modifications over treatment with bisphosphonates, teriparatide, denosumab, orraloxifene.
Conditional recommendation for calcium and vitamin D over oral bisphosphonates, teriparatide, and denosumab because of low-qualityevidence on additional antifracture benefit of the alternative treatments in this low-risk group, costs, and potential harms
Strong recommendation for calcium and vitamin D over IV bisphosphonates and raloxifene because of low-quality evidence on additionalantifracture benefit in this low-risk group and their potential harms
Adults age ‡40 years at moderate risk of major fracture
Treat with an oral bisphosphonate over calcium and vitamin D alone.
Treat with an oral bisphosphonate over IV bisphosphonates, teriparatide, denosumab, or raloxifene.
Oral bisphosphonates preferred for safety, cost, and because of lack of evidence of superior antifracture benefits from other OP medications.Other therapies if oral bisphosphonates are not appropriate, in order of preference:
IV bisphosphonatesHigher risk profile for IV infusion over oral bisphosphonate therapy
TeriparatideCost and burden of therapy with daily injections
DenosumabLack of safety data in people treated with immunosuppressive agents
Raloxifene (for postmenopausal women in whom none of the medications listed above is appropriate)Lack of adequate data on benefits (impact on risk of vertebral and hip fractures in GC users) and potential harms (clotting risks, mortality)
Conditional recommendations because of indirect and low-quality evidence comparing benefits and harms of alternative treatments in peoplewith moderate fracture risk
Adults age ‡40 years at high risk of fracture
Treat with an oral bisphosphonate over calcium and vitamin D alone.
Treat with an oral bisphosphonate over IV bisphosphonates, teriparatide, denosumab, or raloxifene.
Oral bisphosphonates preferred for safety, cost, and because of lack of evidence of superior antifracture benefits from other OP medications.Other therapies if oral bisphosphonates are not appropriate, in order of preference:
IV bisphosphonatesHigher risk profile for IV infusion over oral bisphosphonate therapy
TeriparatideCost and burden of therapy with daily injections
DenosumabLack of safety data in people treated with immunosuppressive agents
Raloxifene (for postmenopausal women in whom none of the medications listed above is appropriate)Lack of adequate data on benefits (impact on risk of vertebral and hip fractures in GC users) and potential harms (clotting risks, mortality)
Strong recommendation for oral bisphosphonates over calcium and vitamin D alone because of the strength of the indirect evidence ofantifracture efficacy and low harms
All other recommendations conditional because of indirect and low-quality evidence comparing benefits and harms of alternative treatmentsin people with high fracture risk
Adults age <40 years at low risk of fracture
Optimize calcium and vitamin D intake and lifestyle modifications over treatment with bisphosphonates, teriparatide, or denosumab.
Conditional recommendation for calcium and vitamin D over oral bisphosphonates, teriparatide, and denosumab because of low-qualityevidence on additional antifracture benefit of the alternative treatments, costs, and potential harms
Strong recommendation for calcium and vitamin D over IV bisphosphonates because of low-quality evidence for additional antifracture benefitin this low-risk group and potential harms
*Correction added after online publication 27 September 2017: the dosage for optimized calcium intake has been changed from 800–1,000
mg/day to 1,000–1,200 mg/day.

should be completed every 1–3 years. This reassessmentshould be performed earlier within this 1–3-year timerange for adults age $40 years who are receiving veryhigh doses of GCs (initial prednisone dose $30 mg/day,cumulative dose .5 gm in the previous year) or thosewith a history of OP fracture(s). Later or less frequenttesting within this range can be done for adults age $40years who are taking lower doses of GCs with no otherOP risk factors.
For adults $40 years old who continue GC treat-ment and are currently treated with an OP medication inaddition to calcium and vitamin D, BMD testing shouldbe completed every 2–3 years during treatment in high-risk patients such as those receiving very high-dose GCs(initial prednisone dose $30 mg/day, cumulative dose.5 gm in the previous year), a history of OP fractureoccurring after $18 months of treatment with anti-fracture medication (other than calcium and vitamin D),risks for poor medication adherence or absorption, orother significant OP risk factors.
For adults $40 years old who received an OP treat-ment in the past but are no longer being treated with an OPmedication other than calcium and vitamin D, BMD testingshould be done every 2–3 years. Within this range, reassess-ment should be conducted earlier in patients receivinghigher doses of GCs and those with a history of fracture orlow BMD, and later in those receiving lower doses of GCs,with higher BMD and no other OP risk factors.
Adults ,40 years of age. For all adults ,40years of age who continue GC treatment and are atmoderate-to-high fracture risk (history of previous fracture,BMD Z score ,23, received very high-dose prednisone[$30 mg/day and cumulative dose .5 gm] in the previousyear, risks for poor medication adherence or absorption,
or multiple OP risk factors), BMD testing should be doneevery 2–3 years.
Recommendations for treatment
The Voting Panel’s rationale and strength of rec-ommendations for treatment are detailed in Table 2.
Calcium and vitamin D intake and lifestylemodifications. Optimizing calcium intake (1,000–1,200 mg/day) and vitamin D intake (600–800 IU/day;serum level $20 ng/ml) (37) as well as lifestyle modi-fications (a balanced diet, maintaining weight in the rec-ommended range, smoking cessation, regular weight-bearing or resistance training exercise, limiting alcoholintake to 1–2 alcoholic beverages/day) are conditionallyrecommended for all patients receiving GC treatment.
Initial pharmacologic treatment. Adults $40years of age. Women $40 years of age and not ofchildbearing potential and men $40 years of age (Fig-ure 3) who are at moderate-to-high risk of fractureshould be treated with an oral bisphosphonate (strongrecommendation for those at high risk; conditional rec-ommendation for those at moderate risk). For patientsin whom oral bisphosphonates are not appropriate (forexample, due to comorbidities, patient preference, orconcerns about adherence with an oral medication regi-men), IV bisphosphonates should be used rather thanthe patient receiving no additional treatment beyondcalcium and vitamin D. If bisphosphonate treatmentis not appropriate, teriparatide should be used ratherthan the patient receiving no additional treatmentbeyond calcium and vitamin D. If neither oral nor IVbisphosphonates nor teriparatide treatment is appropri-ate, denosumab should be used rather than the patientreceiving no additional treatment beyond calcium and
Table 2. (Cont’d)
Adults age <40 years at moderate-to-high risk of fracture
Treat with an oral bisphosphonate over calcium and vitamin D alone.
Treat with an oral bisphosphonate over IV bisphosphonates, teriparatide, or denosumab.
Oral bisphosphonates preferred for safety, cost, and because of lack of evidence of superior antifracture benefits from other OP medications.Other therapies if oral bisphosphonates are not appropriate, in order of preference:
IV bisphosphonatesHigher risk profile for IV infusion over oral bisphosphonate therapy
TeriparatideCost and burden of therapy with daily injections
DenosumabLack of safety data in people treated with immunosuppressive agents
Conditional recommendations because of low- to very low-quality evidence on absolute fracture risk and indirect and low-quality evidencecomparing relative harms and benefits of alternative treatments in this age group
* GIOP 5 glucocorticoid (GC)–induced osteoporosis; IV 5 intravenous.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1529
vitamin D. For postmenopausal women in whom noneof these medications is appropriate, raloxifene shouldbe used rather than the patient receiving no additionaltreatment beyond calcium and vitamin D. The order ofthe preferred treatments was determined based on acomparison of efficacy (fracture reduction), toxicity, andcost. These are conditional recommendations.
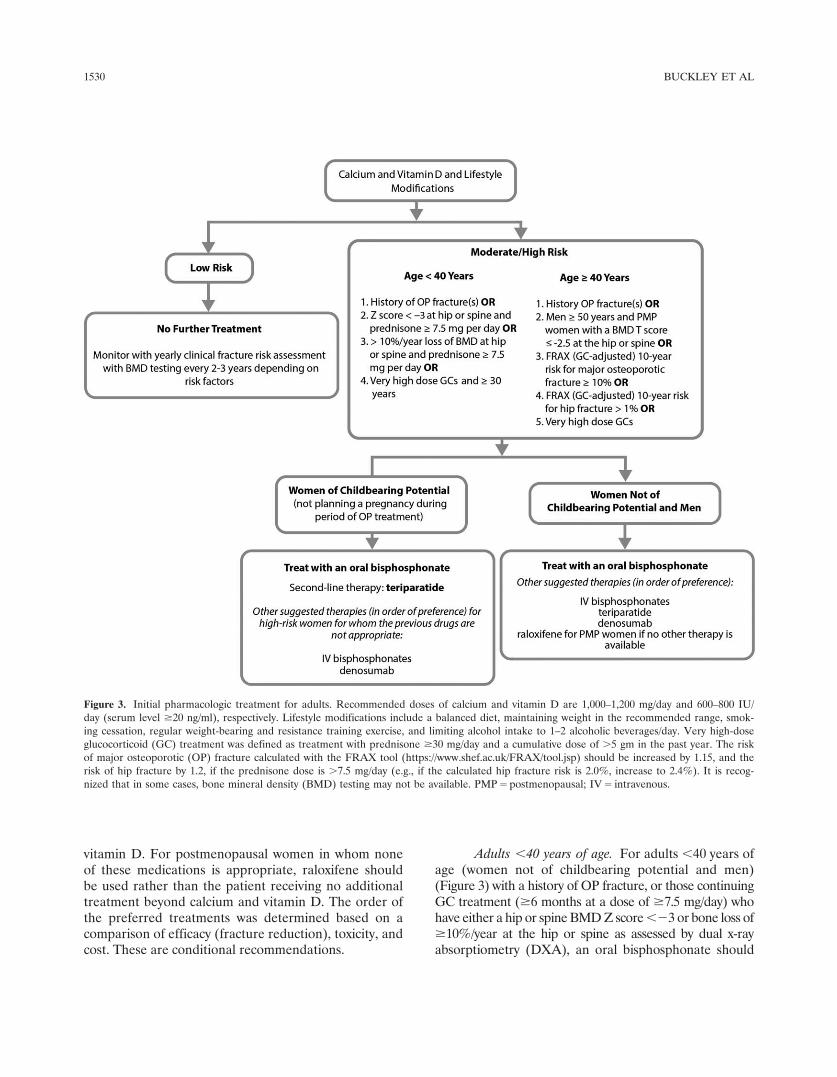
Adults ,40 years of age. For adults ,40 years ofage (women not of childbearing potential and men)(Figure 3) with a history of OP fracture, or those continuingGC treatment ($6 months at a dose of $7.5 mg/day) whohave either a hip or spine BMD Z score ,23 or bone loss of$10%/year at the hip or spine as assessed by dual x-rayabsorptiometry (DXA), an oral bisphosphonate should
Figure 3. Initial pharmacologic treatment for adults. Recommended doses of calcium and vitamin D are 1,000–1,200 mg/day and 600–800 IU/day (serum level $20 ng/ml), respectively. Lifestyle modifications include a balanced diet, maintaining weight in the recommended range, smok-ing cessation, regular weight-bearing and resistance training exercise, and limiting alcohol intake to 1–2 alcoholic beverages/day. Very high-doseglucocorticoid (GC) treatment was defined as treatment with prednisone $30 mg/day and a cumulative dose of .5 gm in the past year. The riskof major osteoporotic (OP) fracture calculated with the FRAX tool (https://www.shef.ac.uk/FRAX/tool.jsp) should be increased by 1.15, and therisk of hip fracture by 1.2, if the prednisone dose is .7.5 mg/day (e.g., if the calculated hip fracture risk is 2.0%, increase to 2.4%). It is recog-nized that in some cases, bone mineral density (BMD) testing may not be available. PMP 5 postmenopausal; IV 5 intravenous.
1530 BUCKLEY ET AL
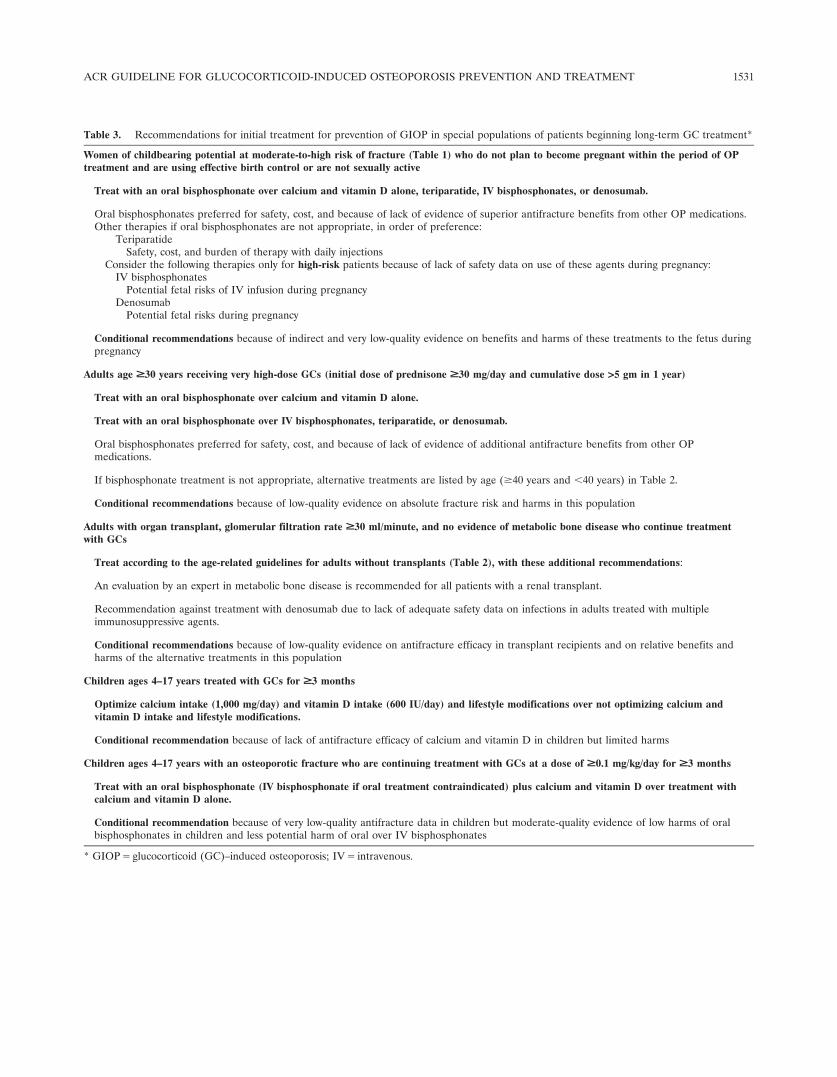
Table 3. Recommendations for initial treatment for prevention of GIOP in special populations of patients beginning long-term GC treatment*
Women of childbearing potential at moderate-to-high risk of fracture (Table 1) who do not plan to become pregnant within the period of OPtreatment and are using effective birth control or are not sexually active
Treat with an oral bisphosphonate over calcium and vitamin D alone, teriparatide, IV bisphosphonates, or denosumab.
Oral bisphosphonates preferred for safety, cost, and because of lack of evidence of superior antifracture benefits from other OP medications.Other therapies if oral bisphosphonates are not appropriate, in order of preference:
TeriparatideSafety, cost, and burden of therapy with daily injections
Consider the following therapies only for high-risk patients because of lack of safety data on use of these agents during pregnancy:IV bisphosphonates
Potential fetal risks of IV infusion during pregnancyDenosumab
Potential fetal risks during pregnancy
Conditional recommendations because of indirect and very low-quality evidence on benefits and harms of these treatments to the fetus duringpregnancy
Adults age ‡30 years receiving very high-dose GCs (initial dose of prednisone ‡30 mg/day and cumulative dose >5 gm in 1 year)
Treat with an oral bisphosphonate over calcium and vitamin D alone.
Treat with an oral bisphosphonate over IV bisphosphonates, teriparatide, or denosumab.
Oral bisphosphonates preferred for safety, cost, and because of lack of evidence of additional antifracture benefits from other OPmedications.
If bisphosphonate treatment is not appropriate, alternative treatments are listed by age ($40 years and ,40 years) in Table 2.
Conditional recommendations because of low-quality evidence on absolute fracture risk and harms in this population
Adults with organ transplant, glomerular filtration rate ‡30 ml/minute, and no evidence of metabolic bone disease who continue treatmentwith GCs
Treat according to the age-related guidelines for adults without transplants (Table 2), with these additional recommendations:
An evaluation by an expert in metabolic bone disease is recommended for all patients with a renal transplant.
Recommendation against treatment with denosumab due to lack of adequate safety data on infections in adults treated with multipleimmunosuppressive agents.
Conditional recommendations because of low-quality evidence on antifracture efficacy in transplant recipients and on relative benefits andharms of the alternative treatments in this population
Children ages 4–17 years treated with GCs for ‡3 months
Optimize calcium intake (1,000 mg/day) and vitamin D intake (600 IU/day) and lifestyle modifications over not optimizing calcium andvitamin D intake and lifestyle modifications.
Conditional recommendation because of lack of antifracture efficacy of calcium and vitamin D in children but limited harms
Children ages 4–17 years with an osteoporotic fracture who are continuing treatment with GCs at a dose of ‡0.1 mg/kg/day for ‡3 months
Treat with an oral bisphosphonate (IV bisphosphonate if oral treatment contraindicated) plus calcium and vitamin D over treatment withcalcium and vitamin D alone.
Conditional recommendation because of very low-quality antifracture data in children but moderate-quality evidence of low harms of oralbisphosphonates in children and less potential harm of oral over IV bisphosphonates
* GIOP 5 glucocorticoid (GC)–induced osteoporosis; IV 5 intravenous.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1531

be used rather than the patient receiving no additionaltreatment beyond calcium and vitamin D. If treatmentwith an oral bisphosphonate is not appropriate, the samealternative medications listed for adults $40 years of ageare recommended with the exception of raloxifene, whichis not used in men and premenopausal women. Theseare conditional recommendations.
Special populations. For women who meet crite-ria for moderate-to-high risk of fracture (Table 1) and areof childbearing potential (Table 3 and Figure 3), but donot plan to become pregnant within the period of OP treat-ment and are using effective birth control or are not sexu-ally active, an oral bisphosphonate should be used ratherthan the patient receiving no additional treatmentbeyond calcium and vitamin D. If oral bisphosphonatetreatment is not appropriate, teriparatide should beused rather than the patient receiving no additionaltreatment beyond calcium and vitamin D. Becauseof the lack of safety data and the potential fetal harmassociated with denosumab in animal studies and withhigh-dose IV bisphosphonates (38–53), these therapiesshould be used only in women who are at high risk of frac-ture in whom treatment with an oral bisphosphonate and
teriparatide is not appropriate. Denosumab or IV bis-phosphonate treatment should be initiated only after adiscussion with the patient about the very low quality ofevidence about fetal harms in the event of an unplannedpregnancy. These are conditional recommendations.
There is a lack of data on the safety of currentlyavailable OP treatments during pregnancy. Therefore, theseguidelines do not include recommendations about OP pre-vention or treatment, other than calcium and vitamin Dintake and lifestyle modification, in women who arepregnant.
For adults �30 years of age who are receiving veryhigh-dose GC treatment (initial prednisone dose of$30 mg/day [or equivalent GC exposure] and a cumulativeannual dose of .5 gm) (Table 3), oral bisphosphonatetreatment should be initiated. If treatment with an oral bis-phosphonate is not appropriate, the age-related recom-mendations for second-line therapy (Table 2) should befollowed (with adjustments for women of childbearingpotential as outlined in these guidelines). These are condi-tional recommendations.
For adults who have received an organ transplantand who are continuing treatment with GCs (Table 3),
Table 4. Recommendations for follow-up treatment for prevention of GIOP*
Adults age ‡40 years continuing GC treatment who have had a fracture that occurred after ‡18 months of treatment with an oralbisphosphonate or who have had a significant loss of bone mineral density (‡10%/year)
Treat with another class of OP medication (teriparatide or denosumab; or, consider IV bisphosphonate if treatment failure is judged to bedue to poor absorption or poor medication adherence) with calcium and vitamin D over calcium and vitamin D alone or over calcium andvitamin D and continued oral bisphosphonate.
Conditional recommendation because of very low-quality evidence comparing benefits and harms of the compared treatment options in thisclinical situation
Adults age ‡40 years who have completed 5 years of oral bisphosphonate treatment and who continue GC treatment and are assessed to be atmoderate-to-high risk of fracture
Continue active treatment (with an oral bisphosphonate beyond 5 years or switch to IV bisphosphonate [if concern with regard to adherenceor absorption] or switch to an OP treatment in another class) over calcium and vitamin D alone.
Conditional recommendation because of very low-quality data on benefits and harms in GC-treated patients, but moderate-quality data in thegeneral OP literature on benefits and harms of continuing treatment with oral bisphosphonates past 5 years for people at high risk of fracture
Adults age ‡40 years taking an OP medication in addition to calcium and vitamin D who discontinue GC treatment and are assessed to be atlow risk of fracture
Discontinue the OP medication but continue calcium and vitamin D over continuing the OP medication.
Conditional recommendation made by expert consensus; evidence informing it too indirect for the population and very low-quality
Adults age ‡40 years taking an OP medication in addition to calcium and vitamin D who discontinue GC treatment and are assessed to be atmoderate-to-high risk of fracture
Complete the treatment with the OP medication over discontinuing the OP medication.
Strong recommendation for high-risk patients based on expert consensus that patients who are at high risk should continue an OP treatmentin addition to calcium and vitamin D
Conditional recommendation for moderate-risk patients because of lower fracture risk compared to potential harms
* GIOP 5 glucocorticoid (GC)–induced osteoporosis; IV 5 intravenous.
1532 BUCKLEY ET AL

the age-related treatment recommendations outlined inthese guidelines for men and women who do not havetransplants should be followed if the glomerular filtra-tion rate is $30 ml/minute and there is no evidence ofmetabolic bone disease. An evaluation by an expert inmetabolic bone disease is recommended before initiat-ing pharmacologic treatment in adults with a renaltransplant (54). The Panel made a recommendationagainst the use of denosumab because of lack of safetydata in this population of patients who are treated withmultiple immunosuppressive agents. These are condi-tional recommendations.
For GC-treated children 4–17 years of age, a calciumintake of 1,000 mg/day and vitamin D intake of 600 IU/dayis recommended. For children who have had an OP frac-ture who continue GC treatment at a dose of $0.1 mg/kg/day for $3 months, treatment with an oral bisphospho-nate (or an IV bisphosphonate if oral treatment is notappropriate) is recommended (Table 3). These are con-ditional recommendations.
Follow-up treatment recommendations. Initialtreatment failure. For adults $40 years of age who arecontinuing GC treatment who have had a fracturethat occurred $18 months after beginning treatment withan oral bisphosphonate or had a significant decline inBMD ($10%/year) after 1 year of treatment (Table 4),treatment with another class of OP medication (teriparatide,denosumab) or an IV bisphosphonate (if treatment failure isjudged to be due to poor absorption or poor medicationadherence) is recommended rather than the patient receiv-ing no additional treatment beyond calcium and vitamin Dalone or continuing oral bisphosphonate treatment. Theseare conditional recommendations.
Treatment if moderate-to-high fracture risk persistsafter bisphosphonate therapy. For adults $40 years ofage who have completed 5 years of oral bisphosphonatetreatment (Table 4) who are continuing GC treatmentand are assessed to be at moderate-to-high risk of frac-ture (Table 1), continuation of active OP treatment (inaddition to calcium and vitamin D) is recommendedrather than the patient receiving no additional treatmentbeyond calcium and vitamin D. Suggested treatmentoptions include continuing the oral bisphosphonate for7–10 years, switching to an IV bisphosphonate if absorp-tion or adherence is a problem, or treatment with anotherclass of OP medication (teriparatide or denosumab),depending on the response to the initial bisphosphonatetreatment (change in BMD, new fractures) and with con-sideration of rare risks, including jaw necrosis and atypi-cal femur fractures, which might increase with theduration of antiresorptive therapy. These are conditionalrecommendations.
Treatment if GCs are discontinued. For adults$40 years of age who are treated with OP medication inaddition to calcium and vitamin D and are discontinuingGC treatment (Table 4), discontinuation of the OP medica-tion is recommended if fracture risk at the time of GC dis-continuation is assessed to be low. Otherwise, the OPtreatment course should be completed or continued untilthe fracture risk is assessed to be low. Continuation of OPtreatment in the setting of high risk is a strong recommen-dation. The others are conditional recommendations.
Application of these treatment recommenda-tions. These recommendations are made for average ortypical GC-treated patients. They may not be applicableto GC-treated patients with multiple risk factors orfeasible for patients with financial or social barriers totesting and treatment.
DISCUSSION
This report presents the updated ACR recommen-dations for the prevention and treatment of osteoporosisand fractures in patients receiving glucocorticoid treatment.The goal is to optimize identification of patients at risk ofGC-induced fractures so that they can be appropriatelytreated while limiting the risk and the burden of testingand treatment. The guiding principle for these guide-lines was to use outcome measures that are clinicallyrelevant to patients and providers, so in decision-making, data about absolute fracture risk reduction weregiven priority over BMD changes. The recommenda-tions on the order of first-line treatments were based onthe Voting Panel’s assessment of antifracture efficacy,potential harms, and costs. Thus, oral bisphosphonateswere recommended as the preferred first-line therapy inmost clinical situations given their antifracture benefit,safety, and low cost, unless there are contraindications,intolerance, or concerns about patient adherence totreatment.
Robust methodology was used in the literaturesearch. The Voting Panel had a broad representation ofclinicians, both primary care providers and sub-specialists, with experience in bone health and in pre-scribing GC medications. In addition, these guidelinesinclude recommendations for the assessment and reas-sessment of fracture risk and antifracture therapy dur-ing GC treatment and for special populations, such aschildren, people with organ transplants, people receiv-ing very high doses of GCs, and women of childbearingpotential.
There are limitations to these recommendations.First, many important clinical situations could not beaddressed given the limited scope of this guideline
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1533

project. Recommendations addressing initial assessmentand reassessment of fracture risk were made as goodpractice recommendations (36) because, although thePanel believes that the benefits of proceeding accordingto the guidance far outweigh the undesirable conse-quences, the supporting evidence is indirect or not avail-able, and the Panel did not formally gather, summarize,or assess the relevant evidence.
We adopted generally accepted thresholds todefine high, medium, and low levels of absolute risk ofincident fracture (i.e., ,10%, 10–19%, and $20% 10-year risk of major osteoporotic fracture). These cutpoints were used to stratify PICO questions and weighpotential benefits versus harms in those different clinicalsituations. However, the application of these recom-mendations to a clinical setting requires that the physi-cian assign the individual patient into a risk stratum.For adults age $40 years, this can be accomplishedusing fracture risk calculators that take the GC doseinto account, such as the FRAX tool. However, FRAXhas important limitations. First, the fracture risk gener-ated when GC use is included as a risk factor estimatesthe risk that would be associated with moderate-doseprednisone (2.5–7.5 mg/day). To accurately estimate therisk associated with doses of .7.5 mg/day, the clinicianmust multiply the risk of major osteoporotic fractureand the risk of hip fracture generated with the FRAXby 1.15 and by 1.2, respectively. This adjustment maynot adequately estimate the risk associated with veryhigh-dose GC use. FRAX uses hip BMD to calculatefracture risk, but GC use has a greater impact on spineBMD. For GC-treated patients with discordant spine andhip BMD (with lower spine BMD), the Fracture RiskCalculator, which includes spine BMD in absolute frac-ture risk estimation, is available (https://riskcalculator.fore.org). Finally, there is debate about the validity ofFRAX fracture risk estimates after pharmacologic treat-ment for OP, which should be considered in the reassess-ment of fracture risk in treated patients.
The available evidence about fracture risk andrisk reduction was particularly limited with regard totreatment recommendations in adults ,40 years of ageand children, and there are no tools available to esti-mate absolute fracture risk in these age groups. Youn-ger people are often treated with higher doses of GCs,but they have higher bone mass and greater potentialfor recovery of bone mass when the GC treatment is dis-continued. To try to better categorize fracture risk inadults ,40 years of age, the Panel considered severalrisk factors as indicators of moderate-to-high fracturerisk—including history of previous fragility fracture, sig-nificant decrease in BMD, or low BMD Z score with
continued use of prednisone (limiting the recovery ofbone mass) at a dose of $7.5 mg/day for at least 6months—in patients ,40 years old, as well as in patients$30 years old treated with very high doses of GCs (ini-tial prednisone dose $30 mg/day with a cumulative doseof .5 gm) (15,18,21–25). The lack of data on long-termoutcomes with OP treatment in this age group may leadto under- or overtreatment, but the possible benefits tolong-term bone health and the relatively low risks asso-ciated with the recommended OP treatments led to therecommendation of treatment with an oral bisphospho-nate in addition to calcium and vitamin D. There is aneed for more research about absolute risk of fracturein this age group during and after GC use and into lateradult life.
Fracture data are very limited in GIOP-specificclinical trials and population studies. Lacking thesedata, the relative fracture reduction associated with OPmedications was extrapolated from the risk reductionascertained in clinical trials of many different treatmentsfor OP in general. While this step introduced indirect-ness into the quality of evidence for many PICO ques-tions, it is reassuring that where parallel data fromGIOP and non-GIOP trials exist, the derived relativerisks for treatment effects from the same interventionare often similar, indicating that the assumption of gen-eralizability may be reasonable (Supplementary Appen-dix 3 [Summary of Findings Tables 1.4a/b/c, 1.9a/b/c],available on the Arthritis & Rheumatology web siteat http://onlinelibrary.wiley.com/doi/10.1002/art.40137/abstract). Imprecision in the estimate of benefits oftreatment is increased by these extrapolations. Futureclinical trials in GC-treated patients should include frac-ture as a primary outcome measure.
The Panel faced low-quality evidence regardingthe magnitude of benefit GC-treated patients wouldrequire as a tradeoff for assuming the burden and risksof treatment for lowering fracture risk, particularlygiven the uncertainties associated with estimates of ben-efit. Awareness of the need to attain “minimally disrup-tive medicine” (55) has increased in recent years, andmany of the candidate patients already bear the burdenof multiple medications. This burden may influencetheir willingness to tolerate yet additional treatment.The Panel’s assessment was that patients would be will-ing to take calcium and vitamin D with only a very smallabsolute risk reduction, that all or virtually all would bewilling to take bisphosphonates to achieve a 5-year abso-lute reduction in vertebral fracture risk of 5%, and thatmost would choose to take oral bisphosphonates ifthe fracture reduction were between $3% and ,5%.Patients who value these small absolute reductions less
1534 BUCKLEY ET AL

highly than the Panel estimated may decide against rec-ommended treatment after discussion of risks andbenefits with their providers.
There are concerns about the potential harmsof calcium and vitamin D supplementation with regard tocardiovascular risks (56,57). Optimizing calcium intake,however, may be even more important in GC-treatedpatients because of the increase in urinary calcium excretionduring GC use. For this reason, the guidelines suggest opti-mizing dietary intake of calcium. More research about thebenefits and harms of supplemental calcium and vitamin Din GC-treated patients is needed.
Because of these limitations, most of the recom-mendations in this guideline are conditional or goodclinical practice recommendations. Further studies areneeded to examine differences in fracture risk in peoplewith different OP risk factors (age, race, and sex), therole of spine imaging using vertebral fracture assess-ment with DXA or radiography in assessing fracturerisk in GC users, the risk of OP medications to the fetusin women of childbearing potential, and the impact ofOP treatment versus no treatment on adult bone healthand fracture risk in GC-treated children.
GIOP is not a problem that is unique to rheumatol-ogy; GCs are widely prescribed by primary care providersand subspecialists. The Panel’s judgments regardingpatients’ values and preferences were informed by inputfrom the primary care physicians, non-rheumatology spe-cialists, and the patient who served on the Panel. Thispatient highlighted the significant challenges that patientsand clinicians confront when making decisions about opti-mizing bone health during GC treatment of chronic inflam-matory conditions.
ACKNOWLEDGMENTS
We thank Jonathan (Rick) Adachi, MD, Robert Adler,MD, Marcy Bolster, MD, Roberto Civitelli, MD, Jeffrey Curtis,MD, MPH, Chad Deal, MD, Michael Maricic, MD, CliffordRosen, MD, Kenneth Saag, MD, MSc, Emily von Scheven,MD, and Barton Wise, MD for serving on the Expert Panel. Wethank Tom Nickolas, MD, MS, and Elizabeth Shane, MD forproviding expert advice. We thank the Arthritis Foundation forits assistance with patient involvement in this guideline project,as well as the patients who participated in this project. Wethank the ACR staff, including Ms Regina Parker for assistancein organizing the face-to-face meeting and coordinating theadministrative aspects of the project, Ms Robin Lane for assis-tance in manuscript preparation, and Ms Lauren Evans forassistance throughout the literature review process. We thankMs Janet Joyce for help in developing the literature searchstrategy and performing the literature search and updates, andMs Tamara Radar for peer reviewing the literature searchstrategy.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors approvedthe final version to be published. Dr. Buckley had full access to all ofthe data in the study and takes responsibility for the integrity of thedata and the accuracy of the data analysis.
Study conception and design. Buckley, Guyatt, Fink, Cannon,Grossman, Hansen, Humphrey, Lane, Magrey, M. Miller, Morrison,Rao, Robinson, Saha, Wolver, Bannuru, Vaysbrot, Osani, Turgunbaev,A. S. Miller, McAlindon.
Acquisition of data. Buckley, Guyatt, Fink, Bannuru, Vaysbrot,Osani, Turgunbaev, A. S. Miller, McAlindon.
Analysis and interpretation of data. Buckley, Guyatt, Fink,Cannon, Grossman, Hansen, Humphrey, Lane, Magrey, M. Miller,Morrison, Rao, Robinson, Saha, Wolver, Bannuru, Vaysbrot, Osani,Turgunbaev, A. S. Miller, McAlindon.
REFERENCES
1. Fardet L, Petersen I, Nazareth I. Monitoring of patients onlong-term glucocorticoid therapy: a population-based cohortstudy. Medicine (Baltimore) 2015;94:e647.
2. Saag KG, Koehnke R, Caldwell JR, Brasington R, BurmeisterLF, Zimmerman B, et al. Low dose long-term corticosteroidtherapy in rheumatoid arthritis: an analysis of serious adverseevents. Am J Med 1994;96:115–23.
3. Lane NE, Lukert B. The science and therapy of glucocorticoid-induced bone loss. Endocrinol Metab Clin North Am 1998;27:465–83.
4. Curtis J, Westfall AO, Allison J, Bijlsma JW, Freeman A,George V, et al. Population-based assessment of adverse eventsassociated with long-term glucocorticoid use. Arthritis Rheum2006;55:420–6.
5. Angeli A, Guglielmi G, Dovio A, Capelli G, de Feo D, GianniniS, et al. High prevalence of asymptomatic vertebral fractures inpost-menopausal women receiving chronic glucocorticoid ther-apy: a cross-sectional outpatient study. Bone 2006;39:253–9.
6. Laan RF, van Riel PL, van de Putte LB, van Erning LJ, van’tHof MA, Lemmens JA. Low-dose prednisone induces rapidreversible axial bone loss in patients with rheumatoid arthritis: arandomized, controlled study. Ann Intern Med 1993;119:963–8.
7. Hansen KE, Kleker B, Safdar N, Bartels CM. A systematicreview and meta-analysis of glucocorticoid-induced osteoporosisin children. Semin Arthritis Rheum 2014;44:47–54.
8. Van Staa TP, Cooper C, Leufkens HG, Bishop N. Children andthe risk of fractures caused by oral corticosteroids. J Bone MinerRes 2003;18:913–8.
9. Rodd C, Lang B, Ramsay T, Alos N, Huber AM, Cabral DA,et al. Incident vertebral fractures among children with rheumaticdisorders 12 months after glucocorticoid initiation: a nationalobservational study. Arthritis Care Res (Hoboken) 2012;64:122–31.
10. LeBlanc CM, Ma J, Taljaard M, Roth J, Scuccimarri R,Miettunen P, et al. Incident vertebral fractures and risk factorsin the first three years following glucocorticoid initiation amongpediatric patients with rheumatic disorders. J Bone Miner Res2015;30:1667–75.
11. Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C.Use of oral corticosteroids and risk of fractures. J Bone MinerRes 2000;15:993–1000.
12. Hall GM, Spector TD, Griffin AJ, Jawad AS, Hall ML, DoyleDV. The effect of rheumatoid arthritis and steroid therapy onbone density in postmenopausal women. Arthritis Rheum 1993;36:1510–6.
13. Kanis JA, Johansson H, Oden A, McCloskey EV. Guidance forthe adjustment of FRAX according to the dose of glucocorti-coids. Osteoporos Int 2011;22:809–16.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1535

14. Ettinger B. A personal perspective on fracture risk assessmenttools. Menopause 2008;15:1023–6.
15. Van Staa TP, Geusens P, Pols HA, de Laet C, Leufkens HG,Cooper C. A simple score for estimating the long-term risk offracture in patients using oral glucocorticoids. QJM 2005;98:191–8.
16. De Vries F, Bracke M, Leufkens HG, Lammers JW, Cooper C,van Staa TP. Fracture risk with intermittent high-dose oral glu-cocorticoid therapy. Arthritis Rheum 2007:56:208–14.
17. Bultink IE, Lems WF, Kostense PJ, Dijkmans BA, Voskuyl AE.Prevalence of and risk factors for low bone mineral density andvertebral fractures in patients with systemic lupus erythematosus.Arthritis Rheum 2005;52:2044–50.
18. Sugiyama T, Suzuki S, Yoshida T, Suyama K, Tanaka T, SueishiM, et al. Incidence of symptomatic vertebral fractures in womenof childbearing age newly treated with high-dose glucocorticoid.Gend Med 2010;7:218–29.
19. Almehed K, Hetenyi S, Ohlsson C, Carlsten H, Forsblad-d’EliaH. Prevalence and risk factors of vertebral compression fracturesin female SLE patients. Arthritis Res Ther 2010;12:R153.
20. Li EK, Tam LS, Griffith JF, Zhu TY, Li TK, Li M, et al. Highprevalence of asymptomatic vertebral fractures in Chinesewomen with systemic lupus erythematosus. J Rheumatol 2009;36:1646–52.
21. Borba VZ, Matos PG, da Silva Viana PR, Fernandes A, SatoEI, Lazaretti-Castro M. High prevalence of vertebral deformityin premenopausal systemic lupus erythematosus patients. Lupus2005;14:529–33.
22. Sugiyama T, Tatsuno I, Suzuki S, Yoshida T, Tanaka T, SueishiM, et al. Incidence of symptomatic vertebral fracture with high-dose glucocorticoid treatment in the Chiba-Shimoshizu Rheu-matic Cohort between 1986 and 2006. Endocr J 2009;56:591–9.
23. Tatsuno I, Sugiyama T, Suzuki S, Yoshida T, Tanaka T, SueishiM, et al. Age dependence of early symptomatic vertebral frac-ture with high-dose glucocorticoid treatment for collagen vascu-lar diseases. J Clin Endocrinol Metab 2009;94:1671–7.
24. Sugiyama T, Suzuki S, Yoshida T, Mayama T, Hashimoto N,Suyama K, et al. Age, initial dose and dose increase are inde-pendent risk factors for symptomatic vertebral fractures inglucocorticoid-treated male patients. Intern Med 2011;50:817–24.
25. Kumagai S, Kawano S, Atsumi T, Inokuma S, Okada Y, KanaiY, et al. Vertebral fracture and bone mineral density in womenreceiving high dose glucocorticoids for treatment of autoimmunediseases. J Rheumatol 2005;32:863–9.
26. Solomon DH, Katz JN, Jacobs JP, La Tourette AM, Coblyn J.Management of glucocorticoid-induced osteoporosis in patientswith rheumatoid arthritis: rates and predictors of care in an aca-demic rheumatology practice. Arthritis Rheum 2002;46:3136–42.
27. Feldstein AC, Elmer PJ, Nichols GA, Herson M. Practice pat-terns in patients at risk for glucocorticoid-induced osteoporosis.Osteoporos Int 2005;16:2168–74.
28. American College of Rheumatology Task Force on OsteoporosisGuidelines. Recommendations for the prevention and treatmentof glucocorticoid-induced osteoporosis. Arthritis Rheum 1996;39:1791–801.
29. American College of Rheumatology Ad Hoc Committee onGlucocorticoid-Induced Osteoporosis. Recommendations for theprevention and treatment of glucocorticoid-induced osteoporosis:2001 update. Arthritis Rheum 2001;44:1496–503.
30. Grossman JM, Gordon R, Ranganath VK, Deal C, Caplan L,Chen W, et al. American College of Rheumatology 2010 recom-mendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheum 2010;62:1515–26.
31. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y,Alonso-Coello P, et al. GRADE: an emerging consensus on rat-ing quality of evidence and strength of recommendations. BMJ2008;336:924–6.
32. Andrews J, Guyatt G, Oxman AD, Alderson P, Dahm P, Falck-Ytter Y, et al. GRADE guidelines: 14. Going from evidence torecommendations: the significance and presentation of recom-mendations. J Clin Epidemiol 2013;66:719–25.
33. Andrews JC, Schunemann HJ, Oxman AD, Pottie K, MeerpohlJJ, Coello PA, et al. GRADE guidelines: 15. Going from evidenceto recommendation-determinants of a recommendation’s direc-tion and strength. J Clin Epidemiol 2013;66:726–35.
34. GRADEpro web site. URL: https://gradepro.org/.35. EVISTA (raloxifene hydrochloride) tablet for oral use initial US
approval: 1997 prescribing information. Indianapolis (IN): EliLilly and Company; 2007. URL: http://www.accessdata.fda.gov/drugsatfda_docs/label/2007/022042lbl.pdf.
36. Guyatt GH, Sch€unemann HJ, Djulbegovic B, Akl EA. Guidelinepanels should not GRADE good practice statements. J ClinEpidemiol 2015;68:597–600.
37. Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clin-ton SK, et al. The 2011 report on dietary reference intakes forcalcium and vitamin D from the Institute of Medicine: what cli-nicians need to know. J Clin Endocrinol Metab 2011;96:53–8.
38. Bussiere JL, Pyrah I, Boyce R, Branstetter D, Loomis M,Andrews-Cleavenger D. Reproductive toxicity of denosumab incynomolgus monkeys. Reprod Toxicol 2013;42:27–40.
39. Patlas N, Golomb G, Yaffe P, Pinto T, Breuer E, Ornoy A.Transplacental effects of bisphosphonates on fetal skeletal ossifi-cation and mineralization in rats. Teratology 1999;60:68–73.
40. Ornoy A, Wajnberg R, Diav-Citrin O. The outcome of preg-nancy following pre-pregnancy or early pregnancy alendronatetreatment. Reprod Toxicol 2006;22:578–9.
41. Illidge TM, Hussey M, Godden CW. Malignant hypercalcaemiain pregnancy and antenatal administration of intravenous pami-dronate. Clin Oncol (R Coll Radiol) 1996;8:257–8.
42. Levy S, Fayez I, Taguchi N, Han JY, Aiello J, Matsui D, et al.Pregnancy outcome following in utero exposure to bisphosphonates.Bone 2009;44:428–30.
43. Green SB, Pappas AL. Effects of maternal bisphosphonate useon fetal and neonatal outcomes. Am J Health Syst Pharm 2014;71:2029–36.
44. Stathopoulos IP, Liakou CG, Katsalira A, Trovas G, Lyritis GG,Papaioannou NA, et al. The use of bisphosphonates in womenprior to or during pregnancy and lactation. Hormones (Athens)2011;10:280–91.
45. McNicholl DM, Heaney LG. The safety of bisphosphonate usein pre-menopausal women on corticosteroids. Curr Drug Saf2010;5:182–7.
46. Briggs GG, Freeman RK, Yaffe SJ. Drugs in pregnancy and lac-tation: a reference guide to fetal and neonatal risk. Philadelphia:Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011.
47. Djokanovic N, Klieger-Grossmann C, Koren G. Does treatmentwith bisphosphonates endanger the human pregnancy? J ObstetGynaecol Can 2008;30:1146–8.
48. Okazaki A, Matsuzawa T, Takeda M, York RG, Barrow PC,King VC, et al. Intravenous reproductive and developmental tox-icity studies of cimadronate (YM175), a novel bisphosphonate,in rats and rabbits. J Toxicol Sci 1995;20 Suppl 1:1–13.
49. Graepel P, Bentley P, Fritz H, Miyamoto M, Slater SR. Repro-duction toxicity studies with pamidronate. Arzneimittelforschung1992;42:654–67.
50. Sakiyama Y, Tada I, Yamamoto H, Nakanishi T, Yasuda Y,Soeda Y, et al. The effect of ethane-1-hydroxy-1,1-diphosphonate(EHDP) on fetal mice during pregnancy: with emphasis onimplantation and fetal weight. J Osaka Dent Univ 1986;19:87–90.
51. Ibrahim A, Scher N, Williams G, Sridhara R, Li N, Chen G,et al. Approval summary for zoledronic acid for treatment ofmultiple myeloma and cancer bone metastases. Clin Cancer Res2003;9:2394–9.
52. Boyce RW, Varela A, Chouinard L, Bussiere JL, Chellman GJ,Ominsky MS, et al. Infant cynomolgus monkeys exposed to den-osumab in utero exhibit an osteoclast-poor osteopetrotic-like
1536 BUCKLEY ET AL

skeletal phenotype at birth and in the early postnatal period.Bone 2014;64:314–25.
53. Minsker DH, Manson JM, Peter CP. Effects of the bisphospho-nate, alendronate, on parturition in the rat. Toxicol ApplPharmacol 1993;121:217–23.
54. Kidney Disease: Improving Global Outcomes (KDIGO) CKD–MBD Work Group. KDIGO clinical practice guideline for thediagnosis, evaluation, prevention, and treatment of chronic kid-ney disease–mineral and bone disorder (CKD–MBD). KidneyInt Suppl 2009;76 Suppl 113:S1–130.
55. May C, Montori VM, Mair FS. We need minimally disruptivemedicine. BMJ 2009;11;339:b2803.
56. Bolland MJ, Grey A, Avenell A, Gamble GD, Reid IR. Calciumsupplements with or without vitamin D and risk of cardiovascu-lar events: reanalysis of the Women’s Health Initiative limitedaccess dataset and meta-analysis. BMJ 2011;342:d2040.
57. Hsia J, Heiss G, Ren H, Allison M, Dolan NC, Greenland P,et al. Calcium/vitamin D supplementation and cardiovascularevents. Circulation 2007;115:827–8.
ACR GUIDELINE FOR GLUCOCORTICOID-INDUCED OSTEOPOROSIS PREVENTION AND TREATMENT 1537