3d printing: additive processes in dentistry - bego · may 2016 laboratory 13 techica 3d printing:...
TRANSCRIPT
May 2016 Laboratory 13
TECHNICAL
3D printing: Additive processes in dentistryFollowing metal casting and dental ceramics,3D printing is the latest step in in the manufacture of replacement teeth. Professor Dr Constantin von See and Dr Maximilian Meindorfer provide an overview of additive manufacturing technologies for the dental laboratoryThe ultimate effects of this new technology can only be imagined at present. The article summarises existing technologies under the catch-all term 3D printing and presents conditions and technical options for the various additive processes. In addition, its application in the dental technology field is introduced. The manufacture of milled/ subtractively created replacement teeth made its way into everyday dental practice years ago. Constructive–additive processes have only recently become available for day-to-day use by dental laboratories. Although research has been done on additive processes using plastic materials since the early 1980s, they have only been used in dental technology for the last few years. This can be explained by, among other things, the high precision requirements of the objects to be created as well as the specific materials.
What actually is 3D printing? Various additive technical processes are used to manufacture technical dental restorations. Generally it involves the manufacture of semi-finished or finished parts. These are generated by joining, bonding, sintering or polymerising together small volume elements.
The term 3D printing is used here as a catch-all term for various additive processes (Figure 1). Thanks to the joining
technology, the freedom of form in 3D printing is virtually unlimited. Small volume elements are joined together layer by layer. An illustrative comparison is that of constructing a building block tower, in which the individual building blocks are firmly bonded together. In addition to freedom of form, the advantages of additive manufacturing compared to subtractive manufacturing are lower consumption of materials and decreased manufacturing time. With increasing research into 3D printing, various processes have emerged as practical depending on the field of application.
In the dental field, stereolithography (SL, SLA), the masking process and selective laser melting (SLM) have established themselves. For example, in template-guided surgery, drill templates have been printed using SL processes for years. Prerequisites for the application of 3D printing in dental medicine are a high
degree of manufacturing precision and the use of medically harmless materials. The materials used must at least fulfil the requirements for class 1 medical products if they are to be placed in patients’ mouths. 3D printing can only be used in the medical field with suitable materials and after adequate testing (Figures 2 - 3).
The history and development of 3D printingThe additive - often described as generative - manufacturing processes have undergone enormous development recently. However, research into the computer–supported manufacture of printed 3D objects has been going on for 30 years. Additive manufacturing is generally classified as computer aided manufacturing (CAM) (Figure 4). The ‘founder’ of 3D printing was Charles Hull of the University of Colorado, USA.
It started in the early 1980s with work on the 3D printing process, using ultraviolet (UV) light to harden the surface coatings. In 1986 Hull filed his first patent related to this process and called it stereolithography (SL). The 3D printing process was originally used to manufacture prototypes and models. Objects and shapes designed on the computer were manufactured individually as display models. The rapid industrial spread and application in various
Educational aims and objectives To give the reader an overview of the recent advances in 3D printing / additive manufacturing and to evaluate the uses and advantages/disadvantage of the various methods for use in dentistry.
Expected outcomes To understand the various processes of 3D printing and how there are best utilised in the dental laboratory. Subscribers can answer the questions on page 46 to earn one hour of verifiable CPD.
Professor Dr Constantin von See is head of the CAD/CAM and digital technologies in dentistry centre at Danube Private University, Krems, Germany.
Dr med dent Maximilian Meindorfer studied dentistry at the Danube Private University, Krems in parelel with medical journalism.
14 Laboratory May 2016
TECHNICAL
industrial fields meant that, as the additive manufacturing process became increasingly well established, its costs fell significantly. The portfolio of materials to be printed also significantly expanded.
As a result, materials are now available that are suitable for dental medicine applications. The printers have improved significantly in terms of speed, possible component size and the precision of the components, which ultimately determines the fields of application. One example is the 3D-printer from the company BEGO, which can currently be used to manufacture castable casting moulds (CAD/casting moulds), splints, drilling templates, individual moulding trays and models. Further possible application areas should follow in future.
Different processes and their application The most important process technologies, summed up by the term 3D printing, are (Figure 1): • Stereolithography • 3D printing with powder (3DP) • Selective laser melting (SLM) • Fused deposition modelling (FDM) • Masking processes• Laser polymerisation
Stereolithography The oldest, already mentioned CAM process, stereolithography (SL) is distinguished by its high precision. In the original SL process, 3D objects are polymerised from a light-curing plastic bath. For this purpose a support plate is lowered into the bath and always moved down by the corresponding thickness of
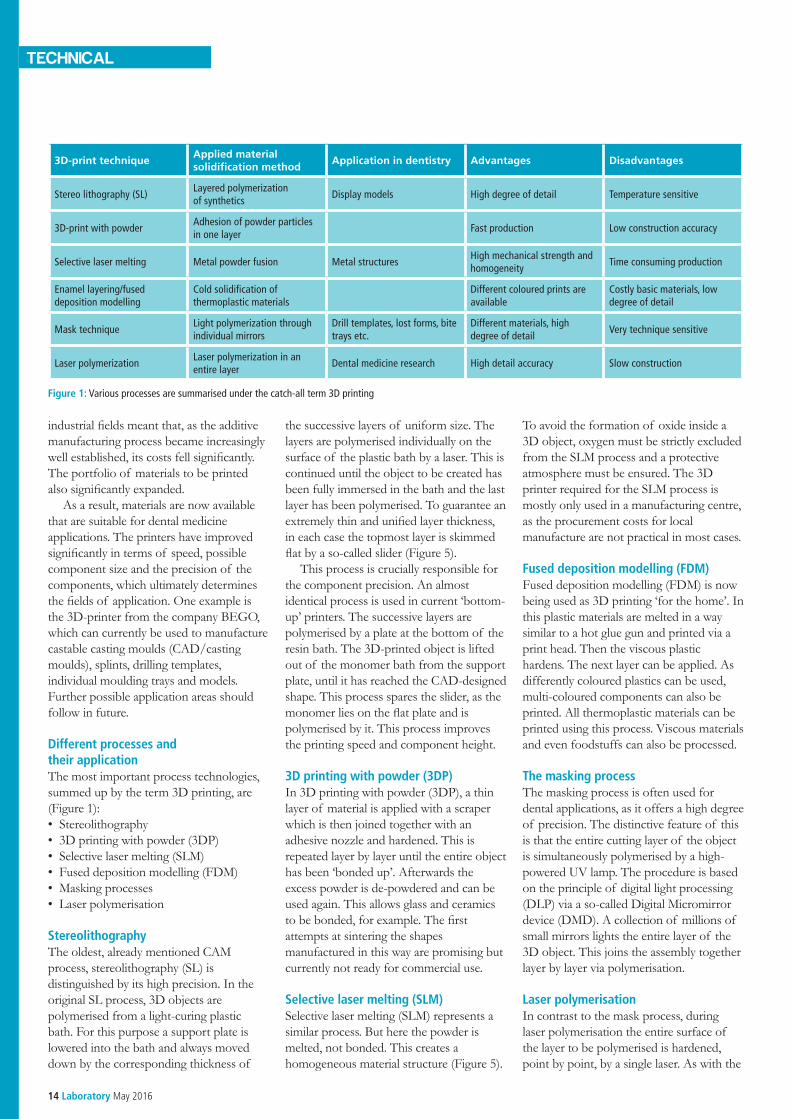
Figure 1: Various processes are summarised under the catch-all term 3D printing
the successive layers of uniform size. The layers are polymerised individually on the surface of the plastic bath by a laser. This is continued until the object to be created has been fully immersed in the bath and the last layer has been polymerised. To guarantee an extremely thin and unified layer thickness, in each case the topmost layer is skimmed flat by a so-called slider (Figure 5).
This process is crucially responsible for the component precision. An almost identical process is used in current ‘bottom-up’ printers. The successive layers are polymerised by a plate at the bottom of the resin bath. The 3D-printed object is lifted out of the monomer bath from the support plate, until it has reached the CAD-designed shape. This process spares the slider, as the monomer lies on the flat plate and is polymerised by it. This process improves the printing speed and component height.
3D printing with powder (3DP) In 3D printing with powder (3DP), a thin layer of material is applied with a scraper which is then joined together with an adhesive nozzle and hardened. This is repeated layer by layer until the entire object has been ‘bonded up’. Afterwards the excess powder is de-powdered and can be used again. This allows glass and ceramics to be bonded, for example. The first attempts at sintering the shapes manufactured in this way are promising but currently not ready for commercial use.
Selective laser melting (SLM) Selective laser melting (SLM) represents a similar process. But here the powder is melted, not bonded. This creates a homogeneous material structure (Figure 5).
To avoid the formation of oxide inside a 3D object, oxygen must be strictly excluded from the SLM process and a protective atmosphere must be ensured. The 3D printer required for the SLM process is mostly only used in a manufacturing centre, as the procurement costs for local manufacture are not practical in most cases.
Fused deposition modelling (FDM) Fused deposition modelling (FDM) is now being used as 3D printing ‘for the home’. In this plastic materials are melted in a way similar to a hot glue gun and printed via a print head. Then the viscous plastic hardens. The next layer can be applied. As differently coloured plastics can be used, multi-coloured components can also be printed. All thermoplastic materials can be printed using this process. Viscous materials and even foodstuffs can also be processed.
The masking process The masking process is often used for dental applications, as it offers a high degree of precision. The distinctive feature of this is that the entire cutting layer of the object is simultaneously polymerised by a high-powered UV lamp. The procedure is based on the principle of digital light processing (DLP) via a so-called Digital Micromirror device (DMD). A collection of millions of small mirrors lights the entire layer of the 3D object. This joins the assembly together layer by layer via polymerisation.
Laser polymerisation In contrast to the mask process, during laser polymerisation the entire surface of the layer to be polymerised is hardened, point by point, by a single laser. As with the
3D-print techniqueApplied material solidification method
Application in dentistry Advantages Disadvantages
Stereo lithography (SL)Layered polymerization of synthetics
Display models High degree of detail Temperature sensitive
3D-print with powderAdhesion of powder particles in one layer
Fast production Low construction accuracy
Selective laser melting Metal powder fusion Metal structuresHigh mechanical strength and homogeneity
Time consuming production
Enamel layering/fused deposition modelling
Cold solidification of thermoplastic materials
Different coloured prints are available
Costly basic materials, low degree of detail
Mask techniqueLight polymerization through individual mirrors
Drill templates, lost forms, bite trays etc.
Different materials, high degree of detail
Very technique sensitive
Laser polymerizationLaser polymerization in an entire layer
Dental medicine research High detail accuracy Slow construction

May 2016 Laboratory 17
TECHNICAL
masking process, very high precision can be achieved with this technology too. Both processes permit the manufacture of very small objects, for which reason they are also of great significance in experimental medicine for so-called tissue engineering.
Applications in dental technology For dental technology applications, it is the masking process in particular that is used. To speed this up, the reverse ‘bottom-up manufacturing’ process described in the stereolithography section is used. This allows taller components to be manufactured. Commercially available stereolithographs currently work with precisions of 25 to 50μm (for example Varseo, BEGO).
Stereolithographs that are used for research purposes have a precision of up to 5μm, which, as a corollary, means that the construction speed is slowed down enormously. With stereolithography, it is not physical parameters but the technical machine implementation that is the limiting factor. Alongside the diameter of the laser radiation or the precision of the impacting UV light source, the natural oscillation through the motors and the size of the construction chamber play a decisive role. The UV light source or the laser beam determine the width of the contours in the X-Y layer to be polymerised. The layer thicknesses and thus the structural height of the layers of the individual layers to be polymerised in the Z direction are limited by the wettability of the preceding, polymerised layer. This is not a limitation in dental medicine. In this respect, the viscosity and the surface tension of the plastic material used play a decisive role.
3D printing material facts In masking processes for technical dental stereolithography applications, it is mainly acrylic resins that are used. These exhibit a high degree of reactivity to light and also have the medical plastics reference data required for the application of UV light. Polymerisation takes place in a way comparable to condensible plastics, in which the initiators contained in the acrylic resin break down into their radicals through photonic effect. The more initiators react in the monomer, the greater the number of the simultaneously initiated chain reactions.
This results in shorter chain lengths. However the chain lengths are decisively
responsible for the characteristics and the polymerisation shrinkage of a plastic.
As chain length or the size of the macromolecules increases, the usability at high temperatures and durability characteristics improve, which is an important aspect for models (Figure 9). In addition, the material characteristics such as the elastic modulus, strength or brittleness can be optimised for the particular indication via the resin selection and the possible addition of filling materials. In recent years many studies were done based on the interplay of output materials and chain lengths, enabling targeted control of material characteristics and compensation for polymerisation shrinkage.
Without this fundamental understanding of material characteristics, comprehensive use in dental technology would be inconceivable. In close interaction of
printable materials and the development of printers, many new application options and indications are created for additive manufacturing.
3D printer environmentA digital model in three-dimensional space is created in the CAD program; for this the spatial planning on the computer screen requires practice and experience. To simplify the design and contouring, semi-automatic processes and digital-design proposals have therefore established themselves in the day-to-day work of dental engineering. For the CAD design of an object to be printed, programs are used that are familiar from the grinding (subtractive) processing. Before computer-aided design (CAD) process work is generated, the intraoral situation of the patient must be digitally available. For this reason a digital
Figure 3: Splint immediately after the 3D printing process with the printing base and support structure. The CAD design is done using ‘Splint designer’. The implementation was performed in the CAM process using stereolithography (3D printer Varseo, BEGO)
Figure 2: Example of a drilling template from 3D printing (Varseo, BEGO)

18 Laboratory May 2016
TECHNICAL
intraoral impression is recommended. Alternatively the plaster model can be scanned extraorally. When capturing the entire jaw, according to current studies, the model scanner is still significantly better than the intraoral scanner.
To implement the design in the 3D object, the use of a computer-aided manufacturing (CAM) process is required with corresponding information processing. Once the digitalisation is
complete, the scan data will be initially converted into a so called STL (Surface tesselation language file or Standard triangulation language file) file with the CAD program (Figure 7). The STL formula encodes all surfaces into triangles and for every triangle saves the coordinates of the corner points and their positive normal vectors. The more corners the system assigns to a surface, the more precisely it is supplied to the
corresponding CAM system. However this means the amount of data to be processed is greater. The amounts of data that are generated can be processed on any modern PC and represent no limitation for additive or subtractive CAD/CAM processes (for example 3D printing).
Furthermore, the data can be sent digitally within a reasonable time and thus made available everywhere. The technical dental work can be designed on the digital models that have been generated; the technical dental workpiece created (drilling template, splint, model, etc) is again saved as an STL file. No additional transformation or conversion of the data is required. The generated STL file can be exported from most CAD programs and fed into a CAM process. During 3D printing of technical dental designs, supports still need to be inserted that prevent warping of the plastic. The printer software of the particular device now ‘slices’ the workpiece according to the structural height - this means that the individual layers to be printed are divided up. The data can now be fed into the printer. As for different indications – for example castable model casting frameworks (CAD/cast) or individual moulding trays - a different manufacturing precision is required, the manufacturing speed is adapted to the plastic. For
Rapid Prototyping
SubtractiveApplication in dentistry
CNC-supported erosive techniquesThe product is milled out of a solid body
Additive/subtractive Shape deposition manufacturingCombination of CNC-milling and layering techniques
Adhesion of powder particles in one layer Stereolithography (SLA or STL)The product is created layer by layer through laser polymerization
Additive
Liquid
Photo polymer
Poly Jet methodLayers of hardening bonding agents are applied to a liquid medium
Multi Jet Modelling (MJM), model makerInjectors applying layers of material (support structure needed)
Thermic materials
Fused Layer Modelling (FLM)Injectors apply melted material to defined spots
Powder
Selective Laser Sintering (SLS)/ Melting (SLM)The product is constructed layer by layer using the powder-pack method and laser
3D- powder printingThe product is constructed layer by layer using the powder-pack method and a bonding agent
Layering Laminated Layer Modeling (LLM)Individual layers are created and placed on top of each other
Figure 4: Overview of the various computer-aided manufacturing (CAM) processes
Figure 5: Diagrammatic representation of the SL process. In this respect the 3D data represent the STL file and the prototype of the factory object that will be lowered into the monomer bath after polymerisation

20 Laboratory May 2016
TECHNICAL
example, individual moulding trays can be manufactured significantly more quickly than precision components such as those for model casting frameworks. The width of the components in the X-Y plane only plays a subordinate role in the masking process. For that reason several components can be manufactured alongside one another without loss of time. This improves the efficiency of the 3D printing when there is an optimal arrangement of the objects to be printed on the support plate. With the Varseo 3D printer, the build-up rate at 50μm is 20 mm/hour and at 100μm it is 40mm/hour. After the printing the additively created objects are manually separated from the support and hardened afterwards to maintain their final physical characteristics. Then the printed objects are processed further (for example CAD/cast frameworks (Figure 8), bite block splints, drilling templates or moulding trays).
Why now? Why has 3D printing has taken off so greatly in the recent past? There are various reasons.
On the one hand, patents for various printing processes have expired, enabling further dissemination and open innovation. On the other hand, from the industrial side, the 3D print process promises high growth rates and a major growth market. The additive technology is now also mature enough that in respect both of precision and the materials used, the requirements for dental applications can be satisfied. As it becomes increasingly established in the marketplace, the manufacturing costs of 3D-printed objects become ever smaller. Thanks to mature processes, procedures can also be arranged more efficiently and the investment of time and effort can be kept down. Other grounds for its current popularity are the almost universal availability of model scanners and the increasing dealings with digital design processes in dental technology. This is of especial benefit to young dental technicians who generally have a low inhibition threshold for dealing with 3D computer programs. The intuitive learning of new CAD computer programs and the basic understanding of
digital data transfer simplifies the work of the new generation of dental technicians in the area of digital design and manufacturing processes.
SummaryThe data quantities to be processed and CAD programs for dental technology have become effective support tools in recent years. This is the basis for the use of 3D printing technology in the dental laboratory. In addition, high-performance programs and processors have been developed that enable rapid mirror control and a high degree of manufacturing precision. These internal control units are already mature and work very reliably. Even more crucial developments can be expected in the years to come, particularly in the sphere of additional application options and new materials. 3D printer processes still have lots of potential to open up in dental technology, which today is still far from exhausted.
Figure 7: CAD representation of a splint. The digital representation has been overlain with the associated STL description
Figure 6: A 14-unit bridge manufactured in the SLM process made from the alloy Wirobond C+ (BEGO)
Figure 9: Example of a printed model
Figure 8: Example of a Varseo CAD/Cast framework created in the 3D printer for the manufacture of a model casting base
Figure 10: Example of an individual moulding tray manufactured in the Varseo 3D printer