4th year medical students blood component therapy salwa i hindawi msc frcpath ctm director of blood...
Post on 21-Dec-2015
217 views
TRANSCRIPT

4th year medical students
Blood Component Therapy
Salwa I HindawiMSc FRCPath CTM
Director of Blood Transfusion Services
KAUH . Jeddah

4th year medical students
RBC AgglutinationRBC Agglutination

4th year medical students
ABO type Pt Cells Pt Serum
vs vs anti-A anti-B Acells Bcells A + 0 0 + 40% B 0 + + 0 11% AB + + 0 0 4% 0 0 0 + + 45%

4th year medical students
BLOOD COMPONENT THERAPY
It is the transfusion of specific blood components required by the patient.
Principles Use blood products only when it is
essential. Replace only the deficient component, if
possible. Identify the cause and nature of the
deficiency and if possible, treat it.
4th year medical students
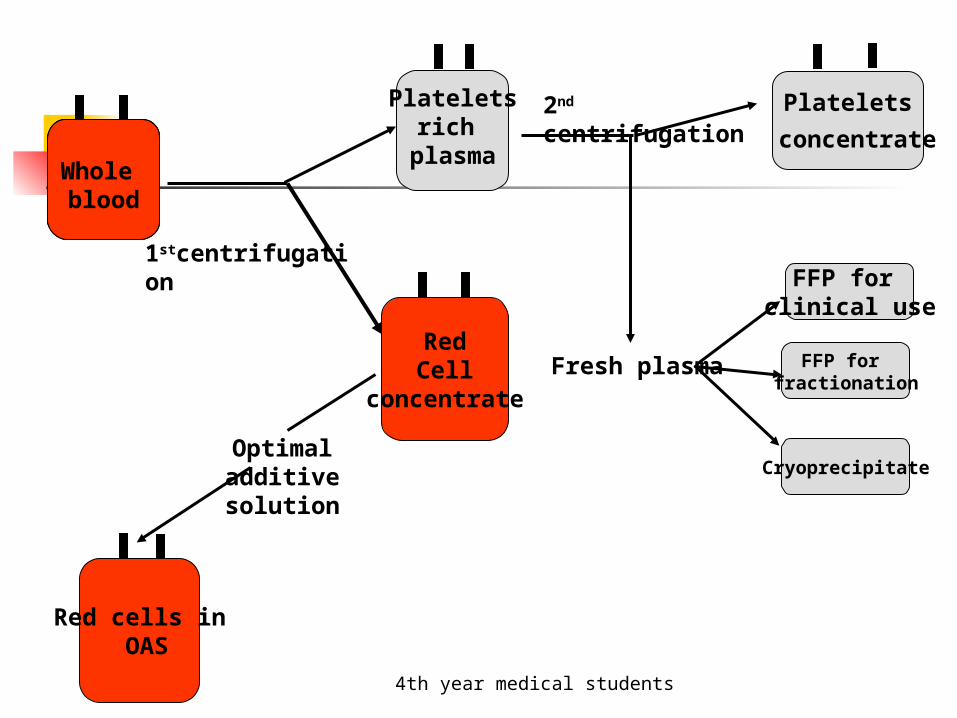
Whole blood
Plateletsrich
plasma
1stcentrifugation
Platelets
concentrateWhole bloodWhole blood
2nd centrifugation
Fresh plasma
FFP for clinical use
FFP for fractionation
Optimal additive solution
Red cells in OAS
Cryoprecipitate
RedCell
concentrate

4th year medical students
Blood COMPONENTS AVAILABLE FROM THE BLOOD BANK
Whole blood Packed RBCs Platelets Single donor platelets (Apheresis) Fresh Frozen Plasma (FFP) Cryoprecipitate

4th year medical students
Indication for Red Blood Cells Transfusion
Red blood cells are component of choice to maintain an adequate supply of oxygen to meet tissue demands.One unit increase the haemoglobin level by 1g/dL in a 70kg recipient.

4th year medical students
Indication for Transfusion of Whole Blood
Fresh whole blood<5 days old is often used for exchange transfusion in newborns.
Stored whole blood can be used in actively bleeding patients who have lost > 30-40% of their blood volume.
4th year medical students
Indication for red blood cells Transfusion
Symptomatic anaemia Acute blood loss>30-40% of blood volume. Pre-operative Hb< 8g/dl and operative
procedure associated with major blood loss.
Evidence of inadequate oxygen delivery.
4th year medical students
Administration and Dose
Red blood cells transfusion has to be grouped specific & Rh specific, if not one of alternative compatible group.
This component must be administered through a suitable transfusion set (170 mM filter).
Dose of 4ml/kg raises venous Hb by about 1g/dl.

4th year medical students
Specifications
Whole blood volume 450mls+63mls of CPD-A1 anticoagulant.
Packed RBCs volume 250mls±50mls. Hct=0.55-0.75. Anticoagulant CPD-A1 store at 4c°±2c° for 35
days. SAG-M for 42 days.

4th year medical students
Indication for Platelet Transfusion
Decrease platelet production (Bone marrow failure)
Therapeutic:for patient who are bleeding associated with BMF caused by either disease, therapy or irradiation.
Prophylactic: >10x 109/L to decrease morbidity in patients with thrombocytopenia due to B.M.F.
4th year medical students
Cont, Platelet Transfusion
In acute D.I.C (Disseminated intravasculr coagulation).
In neonatal alloimmune thrombocytopenia (NAIT) from donor known to be negative for the appropriate HPA or mother platelet.
Platelet function disorders or thrombocytopenia <50x 109/L going for invasive procedure, for operation in critical sites such as the brain or eyes the platelet count should be raised to 100x109/L.
In massive blood transfusion, the platelet count to be maintained above 50x109 /L.

4th year medical students
Administration of Platelet Concentrate:
ABO compatible platelet are preferred but not necessary.
Platelet concentrate should be transfused as soon as possible after reaching the ward with standard blood transfusion sets with 170 mm filters.
The transfusion should normally be completed within 30 minutes.
Observation during platelet transfusion should include pulse& temperature before& after transfusion.

4th year medical students
Indications For The Use Of FFP
Definite indication: Replacement of single factor deficiencies Immediate reversal of warfarin effect Vitamin K deficiency Acute disseminated intravascular coagulation Thrombotic thrombocytopenic purpura Inherited deficiencies of inhibitors of
coagulation:at, protein S, protein C. CI esterase inhibitor deficiency

4th year medical students
Conditional uses of FFP
FFP is only indicated in the presence of bleeding and disturbed coagulation.
Massive transfusion Liver disease Cardiopulmonary bypass surgery Special Paediatric indications: sever sepsis, DIC.

4th year medical students
Administration of FFP
1unit of FFP= APPROXIMATELY 200 ML Dose = 12-15 ml/kg Should be administered within 2 hours of thawing. PT & PTT used for monitoring in addition to the clinical
assessment. ABO compatible FFP should be used. Compatibility
testing is not required. Group O should only be given to group O recipient. Group A or B FFP can be given to group O recipient. Group AB FFP should be reserved for group AB
recipients and for emergencies.

4th year medical students
Indications for The Use Of Cryoprecipitate
1-congenital or Acquired Fibrinogen Deficiency.
2-Haemophilia A, vonWillebrand’s Disease.
3-factor X111 Deficiency
4-disseminated intravascular coagulopathy(DIC).

4th year medical students
Administration of Cryoprecipitate
1 unit of cryo= approximately 10-20ml Adult dose equivalent to 10 units of cryo For factor replacement the dose can be calculated
according to the volume of the factor in the concentrate.
Fibrinogen 150-300mg/pack Von Willebrand factor 80-120u/pack Factor V111c 80-120u/pack Factor X111 20-30% of factor X111 present in the
FFP. Should be ABO compatible to avoid risk of
haemolysis caused by donor antiA or antiB. Should be administered within 4 hours of thawing.

4th year medical students
Platelet, Apheresis
An adult dose of Platelets prepared from anticoagulated blood which is separated into
components by apheresis machine with retention of the platelets and a portion of the plasma.
The remaining elements may be returned to the donor

4th year medical students
Specification
Volume 200 – 800 mlsPlatelet count > 240 x 109 / unitLeucocyte count < 5 x 108 / unit
PH at end of shelf life 6.4-7.4 Availability: On request.
Shelf life storage: 5 days at 22 2c gently agitated

4th year medical students