a - front cover - nhs doncaster ccg pieri raised the issue relating to the stroke target not being...
TRANSCRIPT

Governing Body
To be held on Thursday 18
th September 2014
from 12.30pm until 3.30pm
in the Boardroom, Sovereign House, Heavens Walk, Doncaster DN4 5HZ
This meeting will be followed by the CCG’s 2013/14 Annual General Meeting at 3:45pm


Governing Body To be held on Thursday 18th September 2014
Commencing at 12.30pm – 3:30pm In the Boardroom, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ
PUBLIC AGENDA
Presenter Enc
1. Welcome and Introductions
Chair
2. Apologies
Chair
3. Declarations of Interest
Chair
4. Questions from Members of the Public
Chair
5. Minutes of the previous meeting held on 21st August 2014
Chair Enc A
6. Matters Arising
Chair
Assurance
7. Quality & Performance Report
Mrs Shepherd & Mrs Leighton
Enc B
8. Finance Report
Mrs Tingle Enc C
9. Annual Audit Letter Mrs Tingle Enc D
Standing Items
10. Chair & Chief Officer Report
Dr Tupper & Mr Stainforth
Enc E
Items to Note / Receipt of Minutes

11. Receipt of Minutes from Committees
• Delivery & Performance Committee – Minutes from the meeting held on 10th July 2014
Dr Tupper Enc F
12. Any Other Business
Dr Tupper
13. Date and Time of Next Meeting Thursday 16th October 2014 at 12:30pm
Dr Tupper
14. To resolve that representatives of the press, and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest Section 1(2) Public Bodies (Admission to Meetings) Act 1960.
Dr Tupper

Enc A
Minutes of the previous meeting


1
Minutes of the Governing Body Held on Thursday 21 August 2014 commencing at 12.30pm
In the Boardroom, Sovereign House Present:
Miss Anthea Morris – Lay Member (Chair) Dr Sam Feeney – Locality Lead, Central Locality Dr Marco Pieri – Locality Lead, North West Locality Dr Niki Seddon – Locality Lead, North West Locality Dr Jeremy Bradley – Locality Lead, North East Locality Dr Andy Oakford – Locality Lead, North East Locality Dr Pat Barbour – Locality Lead, South East Locality Dr Lindsey Britten – Locality Lead, South West Locality Dr Emyr Wyn Jones – Secondary Care Doctor Member Mr Chris Stainforth – Chief Officer Mrs Hayley Tingle – Chief Finance Officer Mrs Mary Shepherd – Chief Nurse Mrs Sarah Atkins Whatley – Chief of Corporate Services Mr David Hamilton – DMBC Representative Dr Tony Baxter – Director of Public Health Mrs Ann Gilbert – Healthwatch Doncaster Representative
In attendance:
Mrs Jayne Satterthwaite – PA (Taking Minutes) Mrs Ailsa Leighton – Head of Performance Mr Ian Carpenter, Communications Manager Dr Nabeel Alsindi, Commissioning Fellow (Observing) Mrs Helen Dabbs, Rotherham, Doncaster and South Humber NHS Foundation Trust (Item 7) Mrs Karen Cvijetic, Rotherham, Doncaster and South Humber NHS Foundation Trust (Item 7)
ACTION
1. Welcome and Introductions Miss Morris welcomed everyone to the Governing Body meeting and introduced Mr David Hamilton, Director of Adults Health and Wellbeing, Doncaster Council, to the Governing Body. Introductions were made around the table. There were 10 members of the public in attendance at the meeting.
2. Apologies Apologies were received from:

2
• Dr Nick Tupper – NHS Doncaster CCG Chairman
• Mr Albert Schofield – Lay Member and Vice Chair of the Governing Body
• Dr Anna Kirkman – Locality Lead, Central Locality
• Mrs Jackie Pederson – Chief of Strategy & Delivery
• Dr Karen Wagstaff – Locality Lead, South West Locality
3. Declarations of Interest There were no declarations of interest made.
4. Questions from Members of the Public/ Patient Stories Patient Story Mr Carpenter introduced Mr John Birkett to the Governing Body and explained that Mr Birkett had agreed to relate his personal experience of the excellent rehabilitation services he received at Mexborough Montagu Hospital following his lung transplant in 2013. Mr Birkett informed the Governing Body that, as a result of double pneumonia as a child, emphysema and the rapid progression of fibrosis, he was referred to the hospital in Newcastle, where following 3 days of assessments, he was included onto the lung transplant list. In October 2013 the lung transplant was performed and Mr Birkett was finally discharged home after a 4 week stay in hospital. A period of rehabilitation followed at Mexborough Montagu Hospital. Mr Birkett gave very high praise to the medical staff at both the hospital in Newcastle and the Mexborough Montagu Hospital for the treatment he received and explained that he had re-applied, and had been accepted for, further rehabilitation in Mexborough which will commence in September. Mr Birkett has raised funds for the family unit at Newcastle hospital which supplies accommodation for family members and is committed to continue his fund-raising in the future. Mrs Shepherd stated that it was rewarding to hear when patients relate positive experiences they have received and the Governing Body noted Mr Birkett’s positive attitude throughout his treatment and that empowering patients to be involved in their treatment is positive. Miss Morris thanked Mr Birkett for his valuable contribution.
5. Minutes of the Previous Meeting held on 17th July 2014 The minutes of the meeting held on 17th July 2014 were agreed as an accurate record subject to the following amendment:
• Page 2,’Minutes of the Previous Meeting held on’, add 17th July

3
2014 in the title.
• Page 3, The Health Needs Assessment for Looked After Children was approved at the Children’s Board, not the Health & Wellbeing Board.
6. Matters Arising Page 3, Diagnostic scanning, the pathway requires a review with Doncaster and Bassetlaw Hospitals NHS Foundation Trust (DBHFT) in order to further clarify the definition of “urgent” requests from primary care. Page 3, Paragraph 3, Finance Report, regarding clarification of the budget book, Mrs Tingle confirmed that a paper will be presented to the Governing Body in September. Page 11, Equalities and Patient Participation Groups, Mrs Atkins Whatley confirmed that a presentation will be given to the Strategy Development Forum in September 2014 in order to raise awareness.
Mrs Leighton Mrs Tingle
7. Quality & Performance Report Mrs Shepherd and Mrs Leighton presented the Quality and Performance Report to the Governing Body. Provider Performance Doncaster and Bassetlaw Hospitals NHS Foundation Trust (DBHFT)
• Friends and Family Test - Although the A&E score improved significantly in June 2014 to 24, the response rate has continued to worsen and was only 2.64% in June 2014. DBHFT is therefore urgently reviewing the methodology used to ensure that patient views are captured in a meaningful way. This mirrors the national consideration being given to the methodology and the appropriateness of the token based approach.
• C Difficile – There were 15 cases in the quarter ending June 2014 against a trajectory of 12. Higher than planned levels of activity placed unexpected pressure on the deep cleaning programme but this returned to plan in June 2014. Assurance meetings are being held with the key care groups at DBHFT in anticipation of the potential risks associated with the rotation of junior medical staff.
• Waiting times – Referral To Treatment (RTT) performance was achieved by DBHFT in all 3 categories for June 2014, (admitted, non-admitted and active waiters) and also for the quarter as a whole. However, it is planned that RTT compliance at DBHFT will drop in Quarter 2, as increased levels of patients waiting over 18 week are treated over the summer period. This is in response to the national incentive to increase the number of long waiting patients treated during the quarter in order to deliver a sustainable

4
18 week position from Quarter 3 onwards. This approach has been supported by NHS England and Monitor. The local plan is focussed on General Surgery, Trauma & Orthopaedics, Ophthalmology and Urology.
• 4 Hour Access Target - DBHFT performance failed against the target in June 2014 at 93.2%, for the first time in 8 months. This in turn resulted in a Quarter 1 position of 94.75%. A significant factor in the drop in performance was the introduction of the new A&E Clinical System, Symphony, on 10 June 2014. The new IT system has significant advantages through electronically capturing a full record of all interventions with the patient to improve the quality of reporting and an accurate record of care provided. However, the launch caused multiple problems in the department due to changes required in data capture and A&E processes. July 2014 performance has also been poor particularly on the Doncaster Royal Infirmary (DRI) site and as a result the NHS England Emergency Intensive Support Team (ECIST) has visited the Trust, with a further visit planned week commencing 18 August 2014. The focus for this is around improving patient flow both within and from the department. NHS Doncaster CCG has been invited to attend the feedback session with ECIST.
• Stroke - Stroke performance in June 2014 continues to fail for direct admission. However, following on from last month’s report the stroke assessment beds identified were not in place until the end of June 2014. Initial indications are that this has had a positive impact in July 2014, although validated figures are awaited. NHS Doncaster CCG also plans to conduct a walk through with Stroke Services to further understand the outcomes of the service provided at DRI.
• Mortality Healthcare Evaluation Data (HED) – The HED for DBHFT differs to the Dr Foster data. Mrs Shepherd has met with Mr Sewa Singh, Medical Director, DBHFT, Mr Richard Parker, Nursing Director, DBHFT and Mrs Margaret Kitching, Director of Nursing and Quality, NHS England and assurance has been given to NHS England on the rolling 12 month picture of mortality improvement using consistent data.
Dr Pieri raised the issue relating to the Stroke target not being met and queried if it would be beneficial to take measures. Mrs Shepherd stated that outcome status was being gathered and that a plan to conduct a walk-through of the pathway was in the process of being arranged. It is proving difficult to obtain morbidity data and would require contact with the national stroke director to obtain the data. Options around obtaining more qualitiative patient experience data were discussed. Mrs Shepherd agreed to discuss this further with Mrs Ann Gilbert, Healthwatch. Dr Seddon raised the issue of the amber rating on pressure ulcers. Mrs Shepherd stated that the total number of pressure ulcers is 20% less than last year and that the ‘ungradeable’ grade is being abolished, and we will explore the possibility of Richard Parker presenting a
Mrs Shepherd / Mrs Gilbert

5
spotlight on pressure ulcers at a future Governing Body meeting. Rotherham Doncaster and South Humber NHS Foundation Trust (RDaSH )
• The RDASH Quality Account for 2013/14 has now been produced.
• Waiting times – there are a number of services, namely Attention Deficit Hyperactivity Disorder (ADHD), Child and Adolescent Mental Health (CAMHS) and Speech and Language Therapy, where waiting times reported are above locally agreed targets. Whilst the issues within each service are understood, the issue as a whole will also be raised with RDASH at the monthly contract meeting on 14 August 2014 in order to understand the potential significance at a whole system level.
• Data quality – there are a number of services, namely Improving Access to Psychological Therapies (IAPT), Neurology and Tissue Viability, where issues have been reported regarding data quality. Whilst the issues within each service are understood, the matter will also be raised with RDASH at the monthly contract meeting on 14 August 2014 in order to understand the potential significance at a whole Trust level.
Other Commissioned Services
• Yorkshire Ambulance Service (YAS) - The ambulance response time for the 8 minute Red 1 target in Doncaster fell slightly during July 2014. The Red 2 response time rose slightly to 66.90% and but remained below target. Red 1 and Red 2 8 minute performance also remains below 70% for the year to date across all CCGs. Despite earlier indications it has now been confirmed by the Co-ordinating Commissioner that the Remedial Action Plan and trajectories subsequently presented by YAS to commissioners on 31 July 2014 did not deliver the required year end performance standards and as such were not agreed by commissioners. A further meeting between the Co-ordinating Commissioner and the YAS Directors will take place on 14 August 2014 to improve the Remedial Action Plan and develop a version that can be agreed before 31 August 2014.
Dr Barbour queried if there was any data available regarding the alternative Patient Transport Service as this could potentially relieve some of the pressure on YAS. Mrs Leighton agreed to investigate how YAS utilise their staff and the number of journeys to DBHFT from GPs.
Other Care Providers
• There are currently 3 embargos against new Care Home admissions within Doncaster. This includes one home that has placed a temporary voluntary embargo.
• The Doncaster Safeguarding Adults Partnership Board (DSAPB) has recommended that a lessons learnt review be undertaken in relation to the care provided to a vulnerable adult. The
Mrs Leighton
6
Safeguarding Adults Review Panel will now consider the appointment of an author and also the Terms of Reference for the review.
• The Doncaster Safeguarding Children’s Board (DSCB) has recommended a Lessons Learnt review be undertaken in relation to the care provided to a child. This has been sent to the Expert Panel (National) to consider prior to a final decision being made.
Local Delivery Plans
• A positive performance against a local priority was noted in relation to cancer against an annual trajectory that there were less than 877 emergency admissions with a primary diagnosis of cancer, during Quarter 1 2013/14 there were 192 emergency admissions against a trajectory of 219.
The Governing Body noted the report. Spotlight Report on the Rotherham, Doncaster and South Humber NHS Foundation Trust (RDaSH) Quality Account Mrs Helen Dabbs and Mrs Karen Cvijetic attended the Governing Body meeting and gave the following presentation regarding the Quality Account.
• The Quality report is nationally mandated and is the sixth report.
• RDaSH is registered with no conditions with the Care Quality Commission (CQC).
• There are a total of 11 inspections with Trust services, 7 of which in Doncaster of Learning Disability and Hospice services and 1 Trust wide inspection all of which have been identified as fully compliant.
• There are a total of 18 monitoring visits of Trust Mental Health Inpatient services, 11 of which are in Doncaster. These have been identified as compliant with some minor improvement actions.
• A programme of 8 commissioner led quality visits has been undertaken in the last year. Positive feedback has been received from patients. Staff demonstrated competence and confidence in care planning, commitment and compassion. Areas for improvement include increasing uptake of statutory/mandatory training, disseminating quarterly Safeguarding Incident Reports to all staff, and ensuring cleaning schedules are up to date and easy to follow and ensuring hand wash/posters are available.
• CQUINS – The majority of patient/carer satisfaction targets have been met, and there is a focus on areas not met such as ward activities and meals and refreshments, improvements in community information and data. Positive feedback has been received regarding One Team Working.
• NHS Safety Thermometer, Harm Free Care – High percentages achieved in harm free care in Inpatient services and Community services. Recovery tools have been identified and implemented in Mental Health and Learning Disability services.

7
• Local Commissioning Improvement Priorities 2014/15 include adults and children’s community nursing, integration and implementation of the recommendations from the Mental Health Review by Attain.
• Quality Improvement Strategy 2014/16 – includes patient’s safety, clinical effectiveness, patient experience and staff.
• The Trust Francis declaration has been jointly signed off by the Board of Directors and Council of Governors in December 2013. The four Francis priorities for 2014 are Culture, Engagement, Non-professionally qualified staff and Whistleblowing.
• The Quality Report 2013/14 and the Forward Strategy 2014/15 will be presented at the Annual Members meeting on 24 September 2014. The Quality Improvement Strategy 2014-2016 and the Annual Plan will be implemented.
Mr Stainforth commented that the presentation was a comprehensive overall summary of the work currently ongoing. The parity of esteem between physical and mental health was clearly noted through the Quality Account and Mr Stainforth emphasised the priority that the CCG has placed upon Mental Health in our Strategic Plan and Delivery Plans. Miss Morris thanked Mrs Dabbs and Mrs Cvijetic for attending the meeting.
8. Finance Report Mrs Tingle presented and gave a detailed overview of the report which sets out the financial position as at the end of June 2014 (Month 3). The CCG is currently achieving all of its financial targets and at this early stage in the year is forecasting full achievement by 31 March 2015. Financial risks are as follows:
• Continuing Healthcare (CHC) - As reported last month, based on the current CHC database information, the projected annual expenditure will be broadly in line with the allocated budget. The timing of invoices sent by Providers is often delayed which results in difficultly during the first few months of the financial year to accurately forecast expenditure. Any pressures however will be reported during the year.
• Doncaster and Bassetlaw Hospitals NHS Foundation Trust (DBHFT) - The latest available information is in respect of Month 3 (June) and the contract is showing a financial overspend as a result of increased performance against elective activity. The majority of the over performance relates to increased activity as the Trust continues to improve against the 18 week target, a targeted non recurrent resource has been allocated to support the 18 Referral to Treatment (RTT) position which is in addition to a £2.2m national funding allocation which is targeting a number of specialities facing RTT pressures.

8
• Primary Care Prescribing - The Prescription Pricing Authority (PPA) provides a profile for expected monthly prescribing expenditure. May’s actual data which suggests a slight under spend against profile similar to last year. However, from previous experience the profiles have not been particularly accurate so early in the year so an estimate of breakeven has been included in the forecast figures. The expenditure will be monitored monthly and adjustments made as necessary.
QIPP Programme: The Quality Innovation Productivity & Prevention (QIPP) programme has been developed to encompass a range of areas for disinvestment, re-engineering pathways and cost avoidance measures amounting to £4.5m. Schemes have been identified and are being implemented with leads working on their areas of responsibility. A prudent approach has been taken to the amount of savings that will be achieved at this stage in the year as the evaluation of schemes will take time to process. It is still too early to ascertain if there are any significant variances from the planned profile of savings, however there are no indications that there are any other risks to achieving the QIPP savings, other than those identified in the CCG’s plans. Non-recurrent Headroom: - The CCG has set aside £10.8m (2.5% of the CCG’s recurrent allocation) and plans to fully spend this resource in 2014/15. Commitments relating to waiting list improvements and service redesign costs have been made against this reserve and work is ongoing with managers to determine progress which will result in release of funding into budgets. Further Allocations: - The CCG has been notified of a non-recurrent allocation of £2.2m to support system resilience. A plan of how this is to be invested has been developed through the Operational Resilience Group. The next steps will be to notify our Providers along with required outcome metrics to determine system effectiveness. Mrs Tingle also advised of a new CCG allocation for GP Information Technology (IT), and a transfer from the CCG to NHS England of funding aligned to the registered patient element of the 8-8 contract. Dr Feeney queried where the operating costs and locality budgets were located. Mrs Tingle informed the Governing Body that they were incorporated in the Corporate section within Administration and Business Support. The Governing Body noted the Finance Report.
9. Corporate Assurance Report – Quarter 1 2014/15 Mrs Atkins Whatley presented the Corporate Assurance Report and informed that Governing Body that the report covers the period 1st April to 30th June 2014 (2014/15 Quarter 1) and provides a summary of the key internal corporate assurance and governance activities within NHS Doncaster Clinical Commissioning Group (CCG) during
9
this period. The key points from this report to which the Governing Body’s attention were particularly drawn are: Assurance Framework: There have been no new risks added to the Framework during the last Quarter, with the total remaining at 21. Of these risks, Risk 1.5 relating to commissioning of Continuing Healthcare and Risk 2.4 relating to provider performance were scored at a score of 12 which is above the CCG’s risk toleration threshold and were therefore being treated. 4 additional risks below the risk toleration threshold were also being treated to further strengthen existing controls/assurances (an increase of 2 since the last Quarter). Risk Register: As at quarter-end the CCG Risk Register held 28 risks, of which 3 were rated as High. All of the risks rated High or above (above the CCG risk toleration threshold) were being treated and the action plans were on track. The three high risks relate to Conflicts of Interest, Continuing Healthcare Retrospective Claims, and Safeguarding Children Partnerships. A number of new risks have been identified in Quarter 1, reflecting the fast-moving nature of the risk register. These include risks already noted in Governing Body reports including Financial Risks (Continuing Healthcare, Acute contract over-performance) and Performance Risks (A&E target and stroke improvement trajectory). Five new Corporate Services risks have been added. External Assessments: The Head of Internal Audit Opinion has been received and the Overall Opinion provided significant assurance. The Annual Governance Report / ISA260 was received from the CCG’s External Auditor which reports to those charged with governance and confirmed a positive audit outcome with one low risk recommendation. Committee Activity:
• The Audit Committee had a busy quarter with receipt of Un-audited and Audited Accounts, Annual Report, Annual Governance Statement, Statement of Accountable Officer Responsibilities, Letter of Management Representations, a Shared Business Services (SBS) Audit Report and Commissioning Support Unit Service Auditor Reports
• Quality & Safety Committee considered the usual full range of quality reports, maintained oversight of quality improvements to Continuing Healthcare (CHC), and received the Safeguarding Annual Report.
• The Engagement & Experience Committee planned the launch of the new Talking Points strategy at the June Governing Body meeting, reviewed the Statement of Involvement for 2013/14 and noted a mapping exercise of patient experience to ensure that patient voices are being heard within our commissioning structures.
• Delivery & Performance Committee considered a range of pathway redesigns, business cases and options, noted the organisational processes in place in respect of procurement / tendering / contracts

10
and noted the 2014/15 Choice Framework. Governance Structure: The Corporate Assurance Management Group and the Engagement & Experience Management Group have been added to the governance meeting structure in the last Quarter. The Unplanned Care Working Group has been renamed the System Resilience Group in line with national guidance. Health & Safety, Fire Safety & Security: All required risk assessments (organisational health & safety, fire, first aid) are in date with review dates planned in. A risk has been identified regarding fire seals around the main doors into the top floor of Sovereign House and these are being replaced. Information Governance: The CCG is operating under 4 Section 251 exemptions for the processing of personal confidential data as agreed by the national Confidentiality Advisory Group in line with our status as an Accredited Safe Haven and a Controlled Environment for Finance. These exemptions are time-limited and the national direction of travel is towards anonymised or pseudonymised data only within commissioning. This has been identified as a risk on the Assurance Framework due to a lack of national clarity. Corporate Information Management & Technology (IM&T): Developments include access to corporate email on mobile devices, remote working solutions, and CCG website development. A recent notification on a choice of email solution could impact the CCG having to choose to use NHS Net or a local system and not both, and has been identified as a risk for inclusion on the risk register. Financial Governance: Refreshed Standing Financial Instructions, Standing Orders and a Scheme of Delegation were approved by the Governing Body in May 2014. Organisational Development: Collaborative Leadership Programmes have been running in the last Quarter focussing on:
• Leadership Cohort
• Bands 5/6/7
• Bands 2/3/4
• Governing Body The newly-established Colleague Engagement Group has been meeting regularly. The group has considered and made recommendations arising from the Staff Survey, and are working on a Values into Action workstream which will be incorporated into the Personal Development Review (PDR) process. The Staff Suggestion Scheme has been well received. Dr Seddon commented that it is difficult to understand how best to manage conflicts of interest in clinical commissioning and queried if more work could be done. Mrs Atkins Whatley agreed that conflicts of interest is a key area for the CCG to ensure clinical engagement in key developments whilst effectively managing conflicts of interest, and

11
suggested some timeout to debate the issues may be helpful. Mrs Atkins Whatley also stated that the organisation’s solicitors can provide useful assistance in this matter. The Governing Body noted the report.
10. Chair and Chief Officer Report Mr Stainforth presented the joint report and highlighted the following:
• Better Care Fund - The Better Care Fund (BCF) was announced in June 2013 and the aim of the fund is to provide an opportunity to transform local services so that people are provided with better integrated health care and social care support. Each Health and Wellbeing Board submitted initial plans to NHS England in April 2014. Feedback from the national team states that plans clearly demonstrate a commitment to ensuring more people receive joined-up, personalised care closer to home. They also show that significant progress is being made in bringing together organisations and developing more of a partnership approach to service transformation. Key changes in national guidance for NHS Doncaster CCG to note include:
o Nationally the resource identified for BCF remains at £3.8bn o In the past, £1bn of the fund related to the achievement of
certain local and national metrics o The £1bn will now be utilised differently and a proportion of
the £1bn will be linked to an areas ability to reduce total emergency admissions
o The remaining element of the £1bn will be used by the NHS to commission out of hospital services
o CCGs and the Local Authority will now be asked to set a local target for the reduction of total emergency admissions (minimum expectation is 3.5%)
o CCGs will be required to hold a proportion of the £1bn associated with the reduction of emergency admissions and release this quarterly into a local BCF pooled budget should the reduction in emergency admissions materialise. If not, the funds should pay for the emergency admissions into hospital
o The split between payment for performance and commissioning out of hospital services is dependent upon local ambition for reducing emergency admissions.
o Local providers, in particular acute provide Chief Executives, will be asked sign the plan and provide supporting commentary before submission
The revised plan will now be developed in partnership by the CCG and Local Authority colleagues. It will build on the original April 2014 submission and will also continue to focus on the three transformation programme themes agreed previously.
• Recruitment - Laura Sherburn has been recruited as the new Head of Partnerships Commissioning and is due to commence

12
employment in November 2014 and will report directly to the Chief Officer.
• Unplanned Care Procurement - The CCG continues to move forward with the procurement of GP Out of Hours, Emergency Care Practitioner Service and the unregistered element of the 8-8 Service in Doncaster. The initial aim was for the newly procured services to be in place from 1st April 2105, however, it has become apparent that there are integration and efficiency opportunities if there is alignment with NHS England’s procurement plans for the registered element of the 8-8 Service in Doncaster. In addition, it is has also become necessary to test the flow and number of patients accessing current A&E services to ensure there is greater understanding of acuity and to assess options for streaming patients to appropriate services based on need at presentation. In response to this, current providers were asked if an extension of six months to their current contract was feasible and each provider confirmed that they would accommodate this. The new service model will now go live 1st October 2015.
• Planning Process for 2015/16 – the Planning Process has not yet been clarified nationally however our priorities will be refreshed as necessary.
• Commissioning Support Unit (CSU) Service Level Agreement Review – The focus is on continuing to purchase clinical services and transformational services such as Continuing Healthcare (CHC), Individual Funding Requests and non-recurrent transformational projects, with a principle of considering bringing in-house smaller transactional services.
• The Commissioning Support Unit (CSU) Merger – The CSU merger to create a Yorkshire and Humber CSU is due to take effect on 1st October 2014.
• Transformational Change Programme with Rotherham Doncaster and South Humber NHS Foundation Trust (RDaSH) – A Transformational Change Programme is being undertaken jointly with RDaSH and will focus on Mental Health, Community Nursing and End of Life service provision. This is being led by the NHS Doncaster CCG Chief Officer and RDaSH Chief Executive.
The Governing Body noted the report.
11. Receipt of Minutes from Sub Committees The following draft minutes were received and noted by the Governing Body:
• Quality & Patient Safety Committee – Minutes from the meeting held on 3rd July 2014.
• Delivery & Performance Committee – Minutes from the meeting held on 10th July 2014

13
12. Any Other Business There was no other business discussed.
13. Date and Time of Next Meeting 12:30pm on Thursday 18th September 2014.
14. It was resolved that representatives of the press and other members of the public be excluded from the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest Section 1(2) Public Bodies (Admission to Meetings) Act 1960.

14

Enc B
Quality & Performance Report


1
Meeting name Governing Body
Meeting date 18th September 2014
Title of paper
Quality & Performance Report
Executive / Clinical Lead(s)
Mrs Mary Shepherd, Chief Nurse
Author(s) Mrs Mary Shepherd, Chief Nurse Mrs Ailsa Leighton, Head of Performance
Purpose of Paper - Executive Summary This report sets out the key quality and performance issues to be noted by the NHS Doncaster Clinical Commissioning Group (NHS Doncaster CCG) Governing Body. The format of the report covers 3 main sections this month:
• Provider Performance - main local providers
• Other services commissioned by NHS Doncaster CCG
• Items for escalation regarding Local Delivery Plan in year delivery
Whilst a new contractual year commenced in April 2014, the historic information has been retained in the report in order to enable trends to be identified. However, the performance rating, indicated by Red Amber or Green status, denotes the current month performance and does not reflect the historic trends. This is supported by a detailed appendix (Appendix 1) which highlights performance for NHS Doncaster CCG and all local providers with regards to the main performance indicators. The key areas of change to note since the last report are: Doncaster & Bassetlaw Hospitals NHS Foundation Trust (DBHFT)
• Falls
• Friends and Family Test (FFT)
• C-Difficile
• Waiting times
• 4 Hour Access Target Rotherham, Doncaster & South Humber NHS Foundation Trust (RDASH)
• IAPT Other Commissioned Services
• Child Sexual Exploitation
• Yorkshire Ambulance Service (YAS)
Local Delivery Plan
• Special Educational Needs Assessments
• Dementia Diagnosis
• Children Pathway Changes

2
Recommendation(s) The NHS Doncaster CCG Governing Body is asked to:
• Note the key quality performance areas for attention
Impact analysis
Assurance Framework
2.1, 2.2, 2.4
Risk analysis
Risks are captured in the Executive Summary
Equality impact
Neutral
Sustainability impact
Nil
Financial implications
As identified in the report
Legal implications
Nil
Consultation / Engagement
N/A

3
INTRODUCTION This report sets out the key quality and performance issues to be noted by the Governing Body. The format of the report covers 3 main sections this month:
• Provider Performance - main local providers
• Other services commissioned by NHS Doncaster Clinical Commissioning Group (NHS Doncaster CCG)
• Items for escalation regarding Local Delivery Plan in year delivery
Whilst a new contractual year commenced in April 2014, the historic information has been retained in the report in order to enable trends to be identified. However, the performance rating, indicated by Red Amber or Green status, denotes the current month performance and does not reflect the historic trends. This is supported by a detailed appendix (Appendix 1) which highlights performance for NHS Doncaster CCG and all local providers with regards to the main performance indicators. The key areas of change to note since the last report are:
Doncaster & Bassetlaw Hospital NHS Foundation Trust (DBHFT)
• Falls - Performance has been back on track for serious falls during July. Dr V Barodale consultant Geriatrician is the lead for falls within the trust. Through her analysis a common theme across all falls has been identified (60% association) which is patients falling when going to the toilet in the night. The trust is looking at a proposal to appoint a falls and bone health practitioner who will focus on this work. There will be an 18 month project to address overall falls reduction which we would hope to see a translation into a reduction of serious falls.
• Friends and Family Test - The A&E response rate for Qtr 1 was 11.65% which is below the 15% trajectory set as part of the National CQUIN indicators. In-patients did not achieve the set 25% response rate for Q1 achieving 23.34%. July has seen an improvement in both measures against the previous month, but there still remain issues regarding the A&E response rate although the Trust is currently reviewing methodologies for capturing meaningful patient views. The staff FFT has been undertaken and early indications are that there has been significant improvement from last year’s survey providing positive feedback on recommending the trust to family and friends both for care and treatment and as a place to work. Additionally 90% of staff stated that training and development had helped them to deliver a better service (see CQUIN reports).
• Pressure Ulcers - The incidence of Pressure Ulcers continues to be a challenge within DBHFT and the wider community. The Trust continues to implement their pressure ulcer strategy that also includes the ‘de-escalation’ policy. The impact of these strategies will continue to be monitored through the Contractual Clinical Quality Review meetings. All the necessary resources were in place by April 2014. Embedding of the systems and processes across the organisation is taking longer than anticipated however DBHFT has provided assurance in relation to the priority that this is receiving.

4
NHS Doncaster CCG has co-ordinated and chaired the monthly pressure ulcer Root Cause Analysis meetings but we have now reached the stage where we have good assurance that the internal systems and processes are robust. The Trust now has weekly internal Root Cause Analysis (RCA) meetings with senior team members in order to explore all reported Pressure Ulcers. This increased scrutiny and the implementation of the strategy with increased vigilance, may be contributing to the number of reported incidents. DBHFT have invited a NHS Doncaster CCG representative to this meeting. One significant development found at the RCA panel is the improvement in the nursing documentation relating to patient ‘turn charts’ (how often a patient has their position changed, and how that corresponds to the Integrated Plan of Care in the nursing documentation. As part of this review the number of days without a pressure ulcer is documented Medical Assessment unit (previously an area with high HAPU) have now had 50 + days without any HAPU. The process in place now is that a commissioner will attend the DBHFT internal root cause analysis meeting. One significant advantage of the new strategy within DBHFT is that the intelligence about Pressure Ulcers that have developed outside of the hospital is improved. This l provides a rich source of information and will contribute to improvements in care quality in areas such as domiciliary care and care homes. August 2014 saw a 25% reduction in pressure ulcers designated as Hospital Acquired (HAPU). The strategy advises patients admitted to DBHFT will have a skin assessment within 2 hours of admission, previously where it could not be demonstrated that this had happened the pressure ulcer was recorded as a HAPU. There has been a significant improvement in timely skin assessment at the point of admission and those pressure ulcers present on admission are correctly identified as inherited to the organisation. There has been a 57% increase in inherited pressure ulcers, and of these inherited pressure ulcers the highest denominator is patients admitted from their own home. Due to high activity levels within the organisation the ability to access the correct equipment that will address the complex clinical needs of patients in Emergency departments and Assessment Units e.g. electric 4 sectional profiling beds and (dynamic Alternating pressure) mattresses has been problematic in that these this high specification ‘kit ’is being retained by the wards areas. DBHFT’s response has been to purchase additional bed frames, alternating pressure mattresses, pressure relieving chairs and this should address the deficit
• C Difficile – There were 20 cases in July 2014 against a trajectory of 16. DBHFT have requested a visit from Public Health England. Meetings have

5
taken place with all specialties to discuss antibiotic stewardship and prophylaxis. New processes and robust plans are in place which are expected to directly impact on infection rates.
• Waiting times –Performance for the admitted pathway was 89.2% in July against a target of 90%. This reduction was planned in line with the NHS England initiative to prioritise long waiters in quarter 2. National monies to improve RTT performance locally are supporting additional activity for General Surgery, Urology, Gastroenterology, Ophthalmology and Orthopaedics. The non-admitted and incomplete pathway targets were met in July. DBHFT achieved 90.64% against the 99% target for patients waiting under 6 weeks for a diagnostic test in July. The majority of breaches continue to be in non-obstetric ultrasound as previously reported, although the additional capacity planned for September is now in place. It is expected that waiting times for diagnostics will start to improve as a direct result. During July there was 1 NHS Doncaster CCG patient that waited over 52 weeks, in General Surgery. This has been reported as an incident with a full review being undertaken and a number of process changes made as a result.
• 4 Hour Access Target Following the visit from the NHS England Emergency Intensive Support Team (ECIST) in August 2014 key findings have been shared with the Trust and NHS Doncaster CCG and an action plan created. Areas of focus are pathways for tests, staff rotas, escalation processes and roles in the department. Progress against the action plan will be regularly reviewed. Actions already underway include:
o A new operating procedure has been put in place to strengthen the rapid assessment process.
o A new model has been developed for the resuscitation team to give clearer guidance to staff and management teams.
o A new Matron is due to commence in post. This role will have a key focus on patient flow between the Emergency Department and the Medical Assessment Unit.
The impact of these actions has contributed to improved performance in the second half of August (93.08% for the month compared to 90.2% in July). The range of potential actions to be taken by NHS Doncaster CCG in response to the drop in performance was considered at the Strategy and Development forum meeting in September 2014. It was agreed that NHS Doncaster CCG would look to support the Trust with the transformation required.
Rotherham, Doncaster & South Humber NHS Foundation Trust (RDASH)

6
• IAPT - The external system supplier (TPP) have made changes to the system used by RDASH – namely SystmOne. This has affected the reporting of access and recovery rates and it is currently unreliable. Work is currently being undertaken on an interim solution which is due to be tested in mid September 2014. Until then data for access and recovery rates will be unavailable.
Other Commissioned Services
• Yorkshire Ambulance Service (YAS) - The ambulance response times for both the 8 minute Red 1 and Red 2 targets improved during August 2014 for both Doncaster and YAS as a whole. However they both remain below the 75% target. Performance against the 19 minute target was achieved at 95.89% for August and 95.95% for the year to date for Doncaster. A remedial action plan to deliver Red targets by March 2015 submitted by YAS was rejected by Commissioners due to it not delivering the required standards. A meeting was held on 3rd September at which YAS presented a revised remedial action plan that will deliver targets for YAS as a whole for the quarter ending 31st December and also for the quarter ending 31st March. YAS reported that it was unlikely that targets will be met for the full year 2014-15.
• Other Care Providers - There is currently 1 embargos against admissions within Doncaster. This includes one home that has placed a temporary voluntary embargo.
New embargoes placed in August
Total Providers with embargoes in Place
Embargoes lifted in August
Total Providers with restrictions in Place
Restrictions lifted in July
0 1* 1 1** 0
*Includes 1 Voluntary embargo placed by provider. **Restrictions in place until December 2014.
• The Governing Body was previously informed that the Doncaster Safeguarding Adults Partnership Board (DSAPB) had commissioned a Lessons Learnt Review. The DSAPB have identified an author for this review. The Terms of reference have been developed and a date arranged to for the relevant partners to meet and consider the lessons learnt.
• The Doncaster Safeguarding Children’s Board (DSCB) has recommended a Lessons Learnt review be undertaken in relation to the care provided to a child. This was presented to the Expert Panel (National) on the 8th September to consider prior to a final decision being made. The decision from the meeting will be available in mid September.

7
Safeguarding Child Sexual Exploitation This briefing intends to provide the CCG with an update and areas for local focus and enquiry following the publication of the Independent Enquiry into Child Sexual Exploitation in Rotherham 1997 – 2013. The strategic review of the DSCB in January 2014 led to a stronger focus on CSE Within the new business plan, CSE is identified as part of Strategic Priority 3 as follows: “Doncaster has effective arrangements for responding to key safeguarding risks (particular child sexual exploitation, missing children and neglect, promoting early identification and support to prevent escalation of risk to keep children safe” “To reduce the likelihood of children and young people being sexually exploited and also protect those who are involved by disrupting and bringing to account those who commit this form of child abuse”. Driving these strategic priorities is the CSE sub-group of the DSCB. This sub –group has focused its initial work on:
• Updating the CSE regional strategy to make this more Doncaster Specific
• Embedding effective data systems to capture activity around referrals, assessments, caseloads, investigations and prosecutions.
• Developing revised operational arrangements for receiving and processing referrals
Work is well advanced on the operational elements, and the sub-group has developed a clear referral pathway, a revised referral form, and a detailed operational guide on how the CSE team will handle referrals, assessments and share intelligence. These documents will be finalised by the CSE group in September. Multi-Agency CSE Team In January 2014 the multi-agency CSE team was established and co-located at the Mary Woollett Centre. The team initially comprised of 1 Social worker now to be extended by a further 3, I Detective Sergeant, 5 Detective Constables, 1 senior education welfare office, I worker from Barnardos and I health worker. The remit of the team is around 3 key areas of work: Prevent
• Making it more difficult to exploit children
• Facilitate a co-ordinated response to CSE
• Deliver awareness raising sessions in education settings

8
Protect
• Identify and safeguard children who are at risk
• Support victims
• Identify potential victims and prosecute and identify perpetrators
Pursue
• Identify offenders, disrupt and stop their activity
• Provide specialist support to victims through investigations and court proceedings
• Conduct regular multi-agency reviews and respond to information
CSE Data There have been historic problems in producing reliable data due to the fact that referrals were handled across various work teams and sites. There were also inconsistencies in how staff was classifying cases having regard to the definitions/criteria in Doncaster CSE strategy and procedures. From January it was possible to implement improved systems for recording information with the establishment of the CSE team. CSE Training The DSCB multi agency training has run 6 times since January 2014 and will continue to be run throughout the year. The team have also delivered over 1000 CSE training and awareness sessions. The number of CSE referrals to the police has increased significantl7y over the past 3 years and is likely to be related to increased awareness. Trafficked Children / Missing children Doncaster staff are members of the South Yorkshire wide task and finish group which is currently updating the procedures and operating protocols. Services for longer term support to children At present Doncaster has limited skilled resources to undertake long term interventions with children who are victims of CSE. An important priority will be to explore how these can be developed and resourced. Conclusion The co-ordination and response to concerns about CSE and those children and young people who may be at risk has improved considerably through the co0location of the CSE team, sharing information and intelligence, undertaking immediate risk assessments and providing much more effective engagement with children and their families, and enabling more effective investigations.

9
Local Delivery Plan The following item has been escalated for noting by the Governing Body in relation to the Local Delivery Plan:
• Special educational needs medical assessments completed within 6 weeks of request – In June 0 out of 28 assessments were completed within the targeted timeframe. Commissioners are exploring the reasons for this currently.
• Dementia Diagnosis Rate - This indicator is based on the annual QOF return. The number of people identified with dementia on the QOF list was 2075, an increase of 53; this means that 54.57% of people estimated to have dementia in Doncaster have been identified against a target of 59% at March 2014. This places Doncaster 66th out of 211 CCGs. A band 6 Primary Care Liaison Nurse is currently in place until July 2015 working with RDASH and GP practices to understand the current recording and referral process in place and helping to resolve any issues with data.
The Governing Body is requested to note following area of positive performance in relation to the Local Delivery Plan
• Children - 5% Reduction in acute outpatient tariff activity: New and Follow Up – In quarter one there were 84 new outpatient attendances in an acute setting against a target of 161 and 170 follow-up outpatient attendances in an acute against a target of 229. This demonstrates a significant transfer of activity from acute providers to the new community paediatric service.

10
SECTION 1: PROVIDER PERFORMANCE REPORT The following section of the report details performance for each main local provider, namely DBHFT and RDASH. Performance is across a range of quality and more traditional “performance” measures. As such the report includes performance for each Trust as a whole, and does not simply relate to the service provided to NHS Doncaster CCG.
1.1 Doncaster & Bassetlaw Hospitals NHS Foundation Trust
Governance
Time Period
Q4 2014/15 Q1 2014/15 July 14 August 14
Changes to the board
None applicable None applicable None applicable None applicable
Mortality identified as a risk to quality
Amber Red Amber Amber N/A
There has been a further delay in data being made available to Dr Foster for analysis. The 7 point improvement in the Trust’s rolling HSMR to February 2014 (and the potential improvement once the March data is included), was not due to recoding of practices, but the result of real changes made to care pathways. The Trust’s HSMR figures were monitored on a monthly basis with comparative figures from the preceding year. Revised non-elective pathways were implemented at Doncaster Royal Infirmary (DRI) in December 2013 with greater consultant involvement in care delivery at weekends and out of hours. This appears to have resulted in a significant improvement in non-elective HSMR at DRI.
Further discussion around mortality for the Trust continues to focus efforts on improving the quality of care.
Monitor Governance Rating
Green Green Green Green
Monitor Continuity of Services Rating
4 4 4 4
The continuity of services rating has replaced the financial rating from April 2014.
Contractual actions
2014/15 Contract Queries: no queries issued during August 2014. Performance Notices: zero
Number of serious incidents reported
Q4 2013/14 Q1 2014/15 July 2014 August 2014
47 46 11 5

11
(CCG)
Following a rise in the number of falls resulting in harm the Director of Nursing, Midwifery and Quality has met with falls leads to review all falls occurring since April 2014. As a result further actions will be brought forward with specific projects proposed for any high risk areas which, if successful, will be rolled out across the Trust.
Patient Experience
Time Period
Q3 2013/14 Q4 2013/14 Q1 2013/14 July 14
Complaints Opened 94 115 280 57
There were 60 complaints closed in July (32% within the targeted timescale) with 3 reopened.
Friends & Family Test
Inpatient score Eng. Average (inc. indep.sector) Inpatient response rate
Eng. Average (inc. indep.sector) A&E score Eng. Average A&E response rate
Eng. Average
Dec 13 Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14
81 79 79 76 74 76 77 76
72 73 73 73 73 74 74 74
17.3% 21.6% 25.2% 27.5% 28.7% 21.3% 20.1% 25.4%
28.8% 31.0% 34..2% 34.8% 34.8% 35.9% 38.0% 38.2%
44 53 41 45 54 -3* 24 45
57 57 55 54 55 54 53 53
3.1% 13.7% 23.7% 25.1% 16.5% 16.1% 2.6% 4.8%
15.3% 17.4% 18.6% 18.5% 18.6% 19.1% 20.8% 20.2%
With regards to A&E the response rate for Q1 was 11.65% which is below the 15% trajectory set in the National CQUIN scheme. The Inpatient response rate was 23.34% which did not meet the 25% target. The FFT score for Inpatients remains above the England average. The A&E FFT score improved significantly in July but remains below the England average. It is now mandatory to run the Staff FFT up to four times a year (one of which for DBHFT will be the full annual staff survey in Q3). Q1 results are positive and DBHFT achieved a response rate of 30%. This appears to be the highest response rate of Trusts using Capita to deliver the survey, but comparison against all NHS organisations cannot be undertaken until after the end of July. Results show some significant improvements:
- 78% likely to recommend the Trust as a place for care/treatment (59% in last annual survey)
- 74% likely to recommend Trust as a place to work (59% in last annual survey)
- 90% of staff said their training and development helped them deliver a better patient/user experience (65% in the last annual survey)
In response to the number of staff having had an appraisal in the last 12
12
months the figure remains as per the last annual staff survey at 66%.
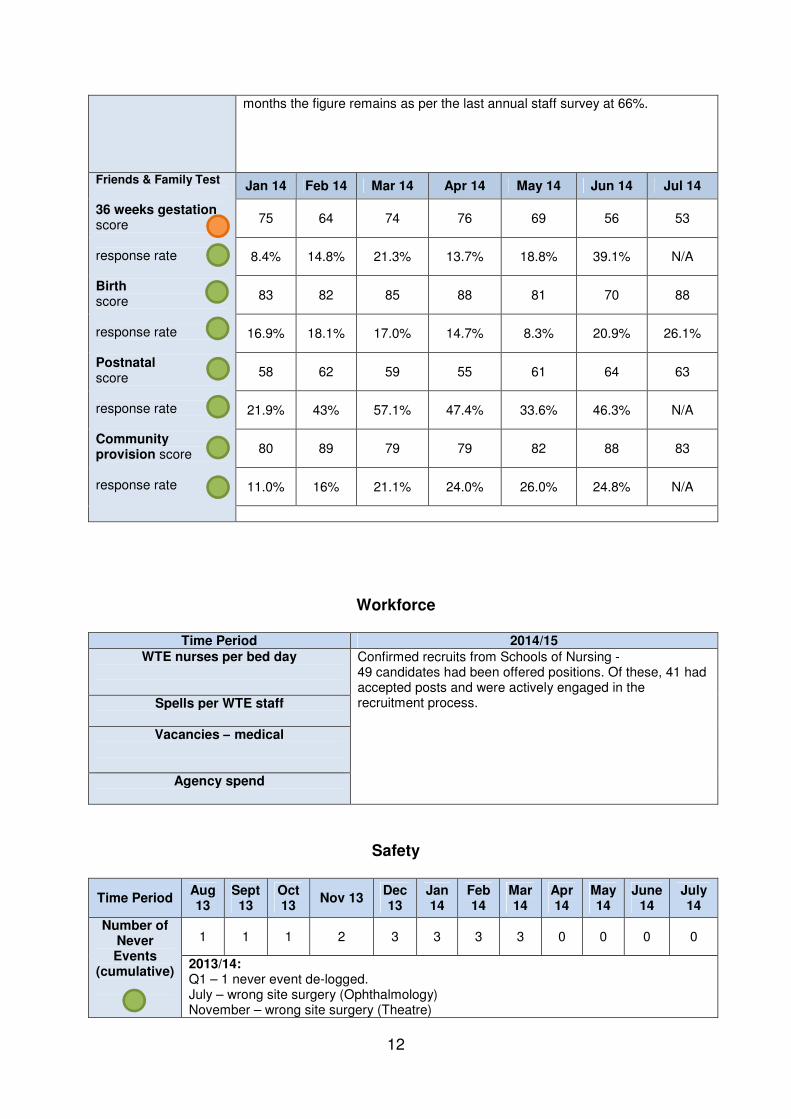
Friends & Family Test
36 weeks gestation score response rate Birth score response rate Postnatal score response rate Community provision score response rate
Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14
75 64 74 76 69 56 53
8.4% 14.8% 21.3% 13.7% 18.8% 39.1% N/A
83 82 85 88 81 70 88
16.9% 18.1% 17.0% 14.7% 8.3% 20.9% 26.1%
58 62 59 55 61 64 63
21.9% 43% 57.1% 47.4% 33.6% 46.3% N/A
80 89 79 79 82 88 83
11.0% 16% 21.1% 24.0% 26.0% 24.8% N/A
Workforce
Time Period 2014/15 WTE nurses per bed day
Confirmed recruits from Schools of Nursing - 49 candidates had been offered positions. Of these, 41 had accepted posts and were actively engaged in the recruitment process.
Spells per WTE staff
Vacancies – medical
Agency spend
Safety
Time Period Aug 13
Sept 13
Oct 13
Nov 13 Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
Number of Never Events
(cumulative)
1 1 1 2 3 3 3 3 0 0 0 0
2013/14: Q1 – 1 never event de-logged. July – wrong site surgery (Ophthalmology) November – wrong site surgery (Theatre)

13
December – retained swab (Women’s and Theatre). 2014/15: No Never Events to date
MRSA (cum.)
1 1 1 2 2 2 2 2 0 0 0 0
2013/14: There were 2 cases of MRSA YTD attributed to DBHFT against a target of 0. 2014/15: No cases of MRSA to date
C-diff Actual
C-diff
Trajectory (NHSE cum.)
17 20 21 26 37 39 40 41 4 11 15 20
15 18 21 24 27 30 33 37 4 8 12 16
DBHFT have requested a visit from Public Health England. Meetings have taken place with all specialties to discuss antibiotic stewardship and prophylaxis. New processes and robust plans are in place.
Pressure Ulcers (total)
Q3 2013/14 – 378 Q4 2013/14 - 387 Q1 2014/15 - 35 July 14 - 4
Please note that the 2013 / 2014 reporting figures are based on all pressure ulcers reported, however 2014 / 2015 figures are focused on all category 3, 4 and ungradeable pressure ulcers. Since the time of reporting in August 7 cases have been reviewed and a revised figure provided for Quarter 1 (35 from 41).
Falls
Q3 464 all falls 7 serious falls
Q4 433 all falls, 5 serious falls
Q1 2014/15 - 13 serious falls
July 14 - 2 serious falls
Performance has been back on track for serious falls during July. Dr V Barodale consultant Geriatrician is the lead for falls within the trust. Through her analysis a common theme across all falls has been identified (60% association) which is patients falling when going to the toilet in the night. The trust is looking at a proposal to appoint a falls and bone health practitioner who will focus on this work. There will be an 18 month project to address overall falls reduction which we would hope to see a translation into a reduction of serious falls
Operational Effectiveness
Time Period
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
Jun 14
Jul 14
Percentage of admitted pathways within 18 weeks for admitted patients
whose clocks stopped during the
period on an adjusted basis (90%
target)
86.4% 85.4% 83.9% 84.6% 86.7% 90.5% 90.7% 90.2% 89.2%
Referral To Treatment (RTT) performance for admitted patients fell below target for DBHFT in July 2014 at 89.2%. This was planned in line with the NHS England initiative to prioritise long waiters in Quarter 2 in preparation for winter.
NHS England has confirmed the Doncaster and Bassetlaw share of national monies to improve RTT performance to be £1.4m. This funding will support additional activity for General Surgery, Urology, Gastroenterology, R

14
Ophthalmology and Orthopaedics. Additional theatre capacity is being put in place and recruitment of Medical Staff for key specialities including Urology and Gastroenterology is in progress to ensure delivery of the targets.
DBHFT achieved 90.64% against the 99% target for patients waiting under 6 weeks for a diagnostic test in July. Of the 626 breaches 520 were for non-obstetric ultrasound and 76 were for DEXA scans. Staff were transferred from DEXA scans to support non-obstetric ultrasound and Computed Tomography (CT). The impact of this change is not expected to continue as from September the Trust have additional sonographers in place as planned, which will directly impact on the waiting times.
52 Week Waits – Incomplete Pathway
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
Jun 14
Jul 14
DCCG 0 0 0 1 0 0 1 0 1
Other 0 0 0 0 0 0 0 0 0
NHSE 1 0 0 0 1 1 3 2 1
DBHFT 1 0 0 1 1 1 4 2 2
At the end of July there were two patients waiting over 52 Weeks.1 was a prisoner and the other was an NHS Doncaster CCG patient waiting for a surgical procedure. A full review of the latter case has been undertaken and a number of process changes made as a result.
4 Hour access - total time in the A&E
department (target 95%)
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
Aug 14
95.6% 96.6% 95.2% 96.5% 95.7% 95.4% 93.2% 91.8% 93.1%
Following the visit from the NHS England Emergency Intensive Support Team (ECIST) in August key findings have been shared and an action plan created. Areas of focus are pathways for tests, staff rotas, escalation processes and roles in the department. Progress against the action plan will be regularly reviewed. Actions already underway include : A new operating procedure has been put in place to strengthen the rapid assessment process. A new model has been developed for the resuscitation team to give clearer guidance to staff and management teams. A new Matron is due to commence in post. This role will have a key focus on patient flow between the Emergency Department and the Medical Assessment Unit. The impact of these actions has contributed to improved performance in the second half of August (93.08% for the month compared to 90.2% in July).
77.0%
82.0%
87.0%
92.0%
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Jul-14
Admitted
Target

15
The range of potential actions to be taken by NHS Doncaster CCG in response to the drop in performance was considered at the Strategy and Development forum meeting in September 2014. It was agreed that NHS Doncaster CCG would look to support the Trust with the transformation required.
Cancelled Operations (target
<0.8%)
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
1.41% 2.91% 1.30% 1.43% 1.09% 0.7% 1.1% 0.9% 1.3%
The target for cancelled operations was not met in July 2014. Reasons for the rise in cancellations are currently being investigated.
All cancer two week wait (target 93%)
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
Jun 14
Jul 14
94.4% 93.7% 91.4% 94.5% 94.3% 94.4% 94.7% 94.0% 95.2%
All cancer 62 days wait for consultant
decision to upgrade their priority status
(target 90%)
85.0% 85.0% 100% 88.2% 100% 88.0% 97.1% 89.3% 85.7%
A review of capacity and demand has been undertaken for breast services and work is taking place to identify capacity which is condition specific. Work is on-going in conjunction with primary care to improve the 62 day pathway for colorectal and lung patients. Direct referral to endoscopy is on track to be in place from September 2014. Collaborative working is also underway with GP colleagues to enable earlier commencement of smoking cessation for patients on the lung cancer pathway.
Outliers (Daily averages)
Medicine to Orthopaedics Medicine to S12 Medicine to surgery Medicine to gynaecology
March 14 April 2014 May 2014 June 2014 July 2014
4 Data not available
6 5 N/A
7 Data not available
3 4 N/A
3 Data not available
3 2 N/A
4 Data not available
5 4 N/A
A number of closed beds within medicine are flexibly opened at certain key points to ensure capacity is maintained.
CQUINs
DBHFT Time Period Q1 2014/15
FFT Staff FFT – Staff FFT was implemented in Q1 and was undertaken by an external company Capita using both electronic and paper methods. The trust are asking the 2 mandated questions
• How likely are you to recommend the organisation as a
place to visit if they (family & friends)need care or
treatment
• How likely they are to recommend the organisation as a
place to work).
Additionally they have asked 2 further questions in relation to
• Staff Education
Notes Achieved Q1 for Staff FFT Payment agreed
(Note encouraging staff
FFT results)

16
• Appraisal
Response rate in Q1 was 30% The trust is also targeting some staff in Q2 and Q4. In Q3 the FFT questions will be offered to all staff as part of the NHS National Survey. To note – a summary of staff FFT results as summarised by DBH is as follows (not in CQUIN) “We can see some notable improvements compared to the 2013 Staff Survey. People are clearly feeling a bit better about things, as shown by these three key headlines:
• 78% would recommend the Trust to friends and
family if they needed care or treatment,
compared to only 59% last year
• 74% would recommend the Trust as a place to
work up from 59%
• A staggering 90% said their training and
development had helped them deliver a better
service. And we thought we were doing okay
last time with 65”
Increased response rate in A&E and In-patients - We are awaiting the formal results of Q1 FFT in relation to response rates in A&E and In patients. The following are trust reported
• A&E Target 15% Actual 24.9% (over quarter)
• In patients 25% target Actual 23% (over quarter)
As the trust needed to achieve a response rate of 25% for the inpatients element they have not achieved the Q1 indicator.
Q1 payment not achieved.
Note that the token
system in A&E will be
halted nationally from
April 15, affecting
participation in the long
term
Safety Thermometer
Safety Thermometer data continues to be collated. The trust has been reporting the number of harm free care across all areas. There has been a steady de-crease in both the total number of pressure ulcers and new pressure ulcers reported from June to August from 52 in June in total to 45 in August. The trust has been requested to provide data in relation to Pressure Ulcers on the Safety Thermometer as a median figure so the 50% reduction in the median against all pressure ulcers can be monitored in year.
In progress – year-end target against trajectories.
National Dementia
Q1 is on track and the delirium pathway has been completed. In Q1 91.1% of appropriate patients were screened, assessed and referred against a trajectory of 90%. The process for referral is via a direct telephone conversation (or letter if the GP is not contactable at the time by the Geriatrician) with the patients GP by medical staff within the elderly care team. In Q1 24 patients were identified via the process. The trust has a named clinical lead for Dementia and training continues to be rolled out to staff. The audit of carers of dementia patients is due to be carried out in Q2 and will look at the support carers get. The trust has extended the cohort of carers from Dementia wards to include elderly orthopaedic wards also.
Achieved Q1 payment agreed

17
Local Pressure Ulcer scheme
Pressure Ulcer numbers are being collated and monitored against a set baseline for measurement at year end. Q1 saw the following numbers reported for every 1% reduction in hospital acquired 2,3 and 4 (and ungradeable) 5% payment will be agreed
• Ungradeable – 17 against a baseline of 116
• Category 2 – 235 against a baseline of xxx
• Category 3 – 21 against a baseline of 49
• Category 4 – 3 against a baseline of 6
Additionally the trust have established audits to undertake assessment and appropriate action of adult patients admitted via A&E and also to establish correct and timely (within 4 hours) equipment provision for all appropriate patients. Baseline data is currently being established to measure appropriate assessment and timely provision of equipment where clinically indicated.
Q1 reported, Annual trajectory - at risk. Q1 reported
Falls The aim of this CQUIN is to stop multiple falls by patients during an episode of care & support the falls strategy at DBH. A points system is in place which incentivises the trust to prevent multiple falls. (capped at 7) The target is to reduce these by 20% by the year end. Root cause analysis will be completed on all patients who fall multiple (more than 7) times as well as every patient who seriously injures themselves by falling. Themes and trends will be identified with wards being accountable for action plans and reduction measures. Additionally the trust are working to reduce the number of falls that result in a serious injury and a gateway has been introduced which will incentivise the trust to have no more than 22 falls with serious harm within the year. Currently the trust has reported 13 falls with serious injury sustained for Quarter 1. A graduated reduction in payments is triggered from 23 serious falls upwards, so therefore there is a risk to the payment
Work continues – no Q1 payment due as year-end payment. If the provider continues to have serious falls above trajectory some of the payment is at risk
Patient Experience
End of Life – The carer/relative questionnaire used for the 13/14 CQUIN has been revised to include a question in relation to DNA CPR. This will be provided to carers/relatives in Q2 and trajectories will be set against the baseline findings. Adult Experience – Improvement trajectories have been set against specific questions within the adults experience measure undertaken in Q1. These include the following questions and trajectories set
• Sleeping disturbed 90%
• Introduced when met 90%
• Enough help with eating and drinking 95%
• Help to the toilet 95%
• Prompt pain relief 93%
• Everything in reach 95%
• IP&C and hand washing 93% rising to 95% year end
• Informed how treatment/care is progressing 90% raining
to 95% by year end
Q1 achieved payment agreed for all experience questionnaire groups To note – there are some comments picked up in these surveys, particularly in relation to end of life that we would like to see addressed. Therefore it was agreed with DBH that on occasion, instead of a trajectory against the satisfaction score an effective action plan to address particular issues would be accepted

18
Real Time Feed Back System
Children’s Assessment Unit – A questionnaire has been devised to establish views of parents whose children are on the Observation Unit. Almost all (with the exception of informed of progress of care) questions scored 100% in relation to the following:
• Feeling welcome
• Being introduced to Dr and nursing staff
• Having timely observations recorded
• Good control of pain
• Informed of any reasons for delay
• Informed of progress with regards to child’s care (90.9%)
Improvement trajectories have been set to maintain and not drop below 95% Children’s in-patient – Parents experience of in-patient wards has been collated and trajectories for improvement/maintenance will be set against the baseline achieved. All elements achieved over 90% against the following elements
• Knowing who is looking after their child
• Drs and Nurses being caring and compassionate
• Being informed of progress of care
• Feeling safe
• Good pain management
• Tests explained by Drs and Nurses in a way that is
understood
• Cleanliness of the environment
• Giving positive comments on care
Improvement trajectories have been set to maintain and not drop below 95% Young Child and Young persons – Experience from this group of patients has been collated and trajectories for improvement/maintenance will be set against the baselines achieved. There has been a good attainment across the two groups with 100% scores for the following
• Knowing who is looking after them
• That Drs and Nurses are nice or caring
• Understanding how they will try and make them better
• Feeling safe on the ward
• Being informed of changes in care
• Understanding test results
• Pain managed well
• Privacy on the wards
The only score which was lower was in relation to young person’s feeling that staff talked to their parents without including them which scored 85.7% (improvement trajectory for this set at 90%, with the others to maintain and not drop below 95%) Feedback response system – due to the ceasing of the care connect programme the CCG is in discussion about how to move this element forward. The Commissioners are to a replacement proposal to the patient experience group which
No Q1 payment allocated

19
has CCG membership to enable a way forward to be established. Reduction in formal complaints – This indicator is a year-end target to reduce the number of complaints (baseline Q1 and Q2) to the trust and the Ombudsman and also to improve the number of complains resolved within the agreed timescales. In Q1 there were
• 156 complaints
• 42% of complaints resolved within
• 0 complaints referred to the Ombudsman
This will require the steps outlined in “real time feedback system” to take effect. The commissioners have agreed the improvement can measure Q1/2 in 14/15 vs Q3/4, but this still requires a system to be up and running soon
Patient Safety/Deteriorating Patient
The trust has undertaken extensive work to meet this indicator in Q1 in relation to the deteriorating patient and escalation. Assessment of appropriate staff in their competence and skill is being undertaken. The full roll out of this indicator is based on structural, process and outcome measures as follows Structural
• Local leader buy in
• Sufficient equipment
• Competent and skilled staff
• Status at a glance boards to identify patients with EWS
• Obvs and fluid charts at bedside
• SOP
• Individualised monitoring and escalation plans
Process
• 100% compliance with obvs and escalation
• 100% compliance with fluid balance recording
• SBAR use for escalation referrals (observation)
• EWS triggers identified in nursing handover (observation)
• EWS triggers identified at start of ward rounds and
prioritised for review (observation)
Outcome
• 0% failure to escalate (cardiac arrests) in accredited
wards
• 0% failure to identify deterioration and failure to escalate
amongst SI’s in the accredited wards
• Staff report positively about confidence, training, support
and adherence to safe systems and processes.
A roll out of accreditation across acute adult areas of the trust has begun. The Paediatric Advanced Warning Score assessment tool has been rolled out. As there have currently been no SIs attributed the trust are undertaking an audit of the PAWS assessment and recording of this in clinical records.
Achieved Q1 – payment agreed. The work conducted for this CQUIN will be received by the respective Quality and Patient Safety Groups at the CCGs for comment. The principle of having CQUINs led by senior clinicians at DBH looks an exciting one
End of Life On track, but with a risk around GP communications. The DNA CPR question has been included in the End of Life relative/carer questionnaire. Additionally a suite of audits will show DNA CPR discharge information in the discharge summary and that this is communicated to the patients GP (via fax). The audits will also measure the number of patients, carers and relatives recorded as being involved in the DNACPR
Q1 indicator met - No Q1 payment allocated. Strong improvements are needed regarding the communications to GPs.

20
process of the DNACPR to patients GPs. Improvement trajectories have been set in year with a 90% trajectory set for year end. Currently the number of discharge summaries showing DNACPR faxed to GPs in Q1 was 22.8%. Report to be received by the Trust Review of Mortality Meeting.
Cancer Following feedback from GP practices and recent educational events the trust as part of CQUINS agreed to undertake a pilot that will help safely test out a service model which aims to help and support clinical decision making in primary care. During Q1 the pilot process was established for consultants to provide an e-mail advice service to GPs within the following specialities
• Head and Neck
• Haemotology
This advice service commenced in August and GPs have been advised of the process. A mid-point pilot evaluation will be undertaken which will identify the following
• Number of weekly enquiries
• Nature of inquiry
• Nature of advice given
• Outcome of advice (i.e. 2ww referral advised and
received)
• Impact of the pilot over the 2 cancer specialities in terms
of referrals and conversion rates
A report will be provided in Q2 in line with CQUIN agreement however The lead commissioner at DCCG will receive data on a monthly basis in order to track progress and uptake.
On track no Q1 payment allocated.
Carers involvement in Dementia
The trust has introduced an admission pack which is given to all patients admitted to Mallard Ward. Relatives/carers have been invited to attend the ward round. To date relatives/carers have preferred to speak to the consultant on the ward whilst they are visiting the person in hospital. A Ward Quality Assessment Tool has been rolled out and piloted in general rehab wards at Mexborough with Adwick Ward being assessed. The tool is to be rolled out across all wards in the care group and carers/relative representatives will be invited to attend the assessment dates. The tool aims to ensure that the needs of patients with dementia are taken into account when planning care and ward environments. Additionally it covers the following
• Ward profiles
• Patient and staff surveys
• Peer review
• Programme of activities
• PLACE and other audits and action plans
Additionally staff training continues and audit has been undertaken which has established the following
• 62.9% of patients have a named carer
• 100% of care/treatment plans were discussed by the
consultant with the carer/relative
• This occurred daily 11%, Weekly 88% and twice weekly
1% of the time
Achieved Q1 – payment agreed. The commissioners note that the system to invite the patient’s relatives / carer to a ward round has been replaced by the trust with recording that they have had a discussion with the patient’s carer. While this seems sensible we would want confirmation from carers that this conversation happened to their satisfaction

21
• Information was recorded 80% of the time in the medical
records. With 20% in both medical and nursing records.
Safeguarding Indicator being worked through, update to be provided at Q2
No Q1 indicator
Local Intelligence Issues
Time Period Q3 2013/14 Q4 2013/14 Q1 2014/15 July 2014
Stroke : direct admission within 4
hours Target 90%
67.5% 60.2% 55.0% 74.0%
Performance improved in July due to the implementation of the new pathway for direct admission to the Stroke Ward. Due to performance being based on discharges during the month, some patients were admitted prior to the implementation of the new pathway at the end of June. Performance for August is therefore expected to show further improvement as the patients discharged during the month will have been admitted via the new pathway for direct admission Also off track at July 2014:
• Patients spending 90% of their time on stroke unit (72.0% against a target of 80%)
• Patients scanned within 1 hour of arrival (30.0% against a target 50%)
Fractured Neck of
Femur % achieving all best practice tariff criteria
Q1 51% Q2 58% Q3 63.2% Q4 62.7% YTD 65.0%
Performance in July 2014 has decreased within the Trust and DRI, however, performance at BDGH has increased since June 2014. Month Actual (Trust) 52.5% Month Actual (DRI) 40.4% Month Actual (BDGH) 82.3%

22
1.2 Rotherham, Doncaster & South Humber NHS Foundation Trust
Work is taking place with RDASH to develop the suite of reporting currently received. This includes the joint development of a mental health Performance and Quality Outcomes Framework and mental health cluster and team profiles. It is planed that as this work progresses it will be added to future Governing Body reports on an incremental basis.
Governance
Time Period
Q3 2013/14 Q4 2013/14 Q1 2014/15
July 2014
Aug 2014
Number of serious incidents reported
24 16 22 5 2
Monitor Governance Rating
Green Green Green Green Green
Monitor Continuity of Services Rating
3 4 3 3 3
The continuity of services rating has replaced the financial rating from April. Monitor’s view of the risk that the trust will fail to carry on as a going concern. A rating of 1 indicates the most serious risk and 4 the least risk. Since May RDASH’s risk has increased from 4 to 3; as noted at the previous meeting this is expected to be a temporary change and RDASH is still rated as “no evident concerns”.
Contractual Actions
No contractual actions undertaken during August 2014.
Patient Experience
Time Period
Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2013/14 April 2014
Complaints 21 14 20 13 4
Complaints data reporting from May 2014 will be reported on a quarterly basis.
Workforce
Time Period
2014/15
Over view The staffing numbers on each of RDASH’s wards are now being declared monthly on their organisation’s website, in line with national requirements set by NHS England. In addition to this a Clinical Staffing Review Group has been established with key representation from each relevant Business Division. This group meets monthly and has developed a robust approach to ensuring that appropriate staffing levels are in place.

23
Safety
Operational Effectiveness
Time Period
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
Adult Mental Health 18 week Non admitted
98.6% 100% 100% 100% 100% 100% 100% 100% 100%
Older People Mental Health 18 week Non
admitted
100% 100% 100% 100% 100% 100% 100% 100% 100%
Improved access to psychological services - the
proportion of people who complete
treatment who are moving to recovery
(Target – 50%)
The external system supplier (TPP) have made changes to SystmOne which has made the reporting of access and recovery rates unreliable. Work is currently being undertaken on an interim solution which is due to be tested in mid September. Until then data for access and recovery rates will be unavailable.
Improved access to psychological services - the proportion of people
that enter treatment against the level of need in the general population
(cumulative) Q1 target 3.75%
As above.
Time Period
Oct 13
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
Number of Never Events
0 0 0 0 0 0 0 0 0 0
MRSA (cumulative)
0 0 0 0 0 0 0 0 0 0
C-diff Actual
C-diff Trajectory (cumulative)
1 1 0 2 0 0 0 2 2 3
1 2 2 4 4 4 4 6 8 11
These cases are attributed to NHS Doncaster CCG and apportioned to RDaSH. If RDaSH services are involved in the clinical management of the patient the RCA is carried out by RDaSH IPCT

24
CQUINs
Time Period Q1 2014/15
FFT Staff FFT – Working group established and external provider identified. The trust will cover all staff over 4 quarters in 14/15 on a systematic basis and also invite all staff to again answer the question as part of the annual staff survey. The Implementation has begun and a marketing strategy is in place to drive forward the understanding and importance of the survey.
Achieved Q1 Payment agreed
Safety Thermometer
Pressure Ulcers - Data has been provided for Pressure Ulcers as actual, baseline median and target as follows
Area Baseline median Year-end Target
OPMHS Inpatients
0% 0%
DCIS Inpatients 3.64% 3.64%
DCIS Community 9.65% 4.83%
Pressure ulcer prevention plans are in place which includes support for care homes and RCAs are undertaken across the health economy. The trust are also gathering evidence of improving quality in pressure care to measure reduction in deteriorating pressure ulcers from cat 2 to cat 3, Increased use of the IPOC to improve assessment and recording adherence and Improving healing outcomes of pressure ulcers. Falls – The trust are implementing the Fallsafe initiative and baseline data (per 1000 bed days) has been provided
Area Baseline June rolling Target
OPMHS Inpatients 10.86% 13.85%* 8.15%
DCIS Inpatients 9.06% 6.88% 6.80%
* Windermere have seen an increase in falls over the quarter and the trust are looking into the reasons identified in RCAs and will report these back to the CCG. Training events have been held to raise the importance of the initiative and a programme of support events and resources for staff will carry on throughout the year. The Fallsafe leads identified are tasked with undertaking ward based activities to raise the understanding and profile and provide on-going support. Additionally the first set of a rolling programme of care bundles have been implemented with baseline audits being undertaken. As the year progresses all care bundles will be phased so eventually all care bundles are being used simultaneously as part of care planning.
On track at end of Q1– (year end payment)
Improving Physical healthcare for SMI
Cardio metabolic Assessment – The trust have registered for the National audit with the Royal College of Psychiatrists. A policy is in place for physical healthcare of inpatients which includes all elements within the audit criteria. Data collection tool due to be released from the RCP in August. Patients on CPA and communication with GPs (ICD10 codes) – The trust are developing an audit protocol which will be shared with commissioners. A working group has also been established to look at current communication with GPs and the co-hort of patients for this has been agreed.
On track at end of Q1

25
Patient Experience
Mental Health and Community Patients and Carers – The trust have undertaken a review of the surveys completed in 2013/14 and where necessary changes to the pro-forma have been agreed. The areas of focus for each service have been identified and action plans have been written. The reports against attainment are due in Q2. GP Survey - The trust have liaised with commissioners and the survey will focus on the understanding of the crisis pathway as it stands and then look at understanding and benefits on the changed crisis pathway which is due to be undertaken.
On track at end of Q1
Recovery CAMHS – Outcome measure training been undertaken for staff and more sessions have been arranged for new staff and to ensure its well embedded. A self-assessment questionnaire on the routine outcome measures tool is available to test knowledge and reporting systems for the outcome measures have been set up on Silverlink. Champions have been identified and baselines set. Improvement trajectories will need to be agreed as the next steps in Q2. LD – The LD Health Equalities Framework continues to be rolled out. A pilot and mid-point review has been undertaken which gathers both staff feedback and has reviewed some early outcomes. There has been positive feedback from staff particularly in relation to outcomes being linked to care goals and provision of evidence to steer audits/assessment/reviews against care management plans and clinically targeted interventions. There have however been some concerns that the tool is quite time consuming, not attached to a clinical system and that it isn’t useful for maintenance of patients. The trust is working through resolving the issues identified and working with clinical teams to link outcomes to individual care goals and also developing a suite of plans/goals relating to outcomes so they fit with the wider suite of clinical assessments. Additionally the trust are considering a wider roll out to inpatients with LD. Early outcomes from the use of the tool have identified at 100% of Doncaster patients who have been reviewed showed improvement in their individual needs and for 3 patients who have had final scores undertaken all three demonstrated significant improvement. AMH and OPMH – The 4 factor model is the agreed recovery tool for these patients and builds onto last year’s CQUIN. The coverage of patients having a HoNOS completed at discharge has continued to improve to over 70% and is on track for 90% target by end of Q2. Reporting has been developed in Q1 using the 4 factor model and this supports clinicians in managing both an individual patients care and understanding the 4 factor models cores per cluster. Charts at patient level are included in the patient record in Silverlink it is easily accessible by the treating team to track progress and begin to link the scores to care planning.
Achieved Q1 payment agreed
LD Dementia The screening checklist, tool and pathway have been reviewed to ensure it meets the requirements of the CQUIN for those patients showing signs of cognitive issues. The pathway has been mapped and appropriate changes to the pathway have been made. A pre-screen based on the carer checklist of signs and symptoms for LD patients over 50s and patients aged over 35 with
On track at end of Q1 (year end payment against trajectory)

26
Downs Syndrome is in place. A template for TPP has been implemented and staff were notified of the screening which began in June. The trust have identified clinical leads and training materials are currently being sought and designed to ensure appropriate staff are trained in understanding and treating Dementia within LD patients.
Community Dementia
Hawthorne and Hazel wards – Screening has begun on these wards using the Addenbrooks screening tool and a template on TPP allows recording of the process. Where the screen indicates possible dementia, the patients are referred to memory clinic if relevant tests have been undertaken on the ward while the patient is an in-patient, or to the GP if tests need to be completed. The trust are formulating a roll out of this programme to community patients and will also investigate a way to be able to gain understanding from GPs on outcomes from referral for assessments and any diagnosis made as part of this process.
Achieved Q1 payment agreed
Care Planning and Risk Assessments
Care planning audit protocols have been developed and are tailored to meet the differing divisions i.e. OPMH, LD and AMH. Baseline audits have been completed and will be available in Q2. Audits will also be repeated in December 14. A community audit protocol is being devised based on the same principles as outlined in the CQUIN indicator. This will cover a number of areas including
• outcomes of screens and risk assessments being
evidenced in the care plan development
• Patients having an understanding of their care plan
• Actions have been reviewed in the care plan
• The care co-ordinator has been involved in the process.
On track at end of Q1
Community Nursing and OTW
Community Nursing – A skills gap analysis has been completed against the skills required to meet the new specification. This has formed the basis of the training which is well underway. Trajectories against these along with the 6c’s action plan have also been agreed. The trust are confident that the skills gap will be filled and the CQUIN indicator met in year. Currently there are 2 minor elements that have been RAG rated Amber by the trust. These are Doppler training and Bandaging and compression training. These will be on track in Q2. End of Life training is currently being identified and the learning package will be implemented at the end of Q2. OTW – Progress report has been provided and is on track. The trust are re-visiting GPs and practice teams and are working on agreeing an information sharing agreement to allow comparison between OTW caseload data, A&E data and LoS data.
Achieved Q1 payment agreed
Safeguarding The trust have undertaken the benchmarking exercise against the safeguarding standards as per statutory requirement. The outcomes from this have been RAG rated and action plans developed for any areas that are not rated as green. Of the full set of standards 4 are rated amber. Three of these are where policies are being updated and one is linked to improving the capture of patient experience.
Achieved Q1 payment agreed

27
The design of a methodology of capturing patient experience has been challenging for the trust and it has been agreed that the trust will meet with the safeguarding adults and children leads within the CCG to establish the process and formulate the next steps to move this forward. The ‘What about the children’ document has been reviewed to understand what actions were required. Areas identified for further work included both AMH and drug and alcohol services. Work completed to date for AMH includes
• Named nurses for safeguarding with AMH division
formulated a Child assessment tool for pilot
implementation in agreed teams
• Concerns raised from the pilot in relation to the quality of
information gathered, the time constraints of the
assessment and recording in the electronic records have
been reviewed.
• The tool has been reviewed in terms of how it could
include the assessment of child need and subsequent
actions and an aide memoire has been devised that
reference all the key issues relating to children that
required exploring during the assessment
• Aide memoire on silverlink recording guide issued to all
AMH clinical staff and a guide identifies what elements of
child assessment should be recorded and where on the
electronic record.
Next steps
• Clinical audit to be undertaken against recording guide
standards
• Further exploration of the silverlink functionality to take
place through Q2 and Q3 to address specific data capture
and extraction such as child carer figures.
Local Intelligence Issues
Time Period
Oct 13
Nov 13
Dec 13
Jan 14
Feb 14
Mar 14
Apr 14
May 14
June 14
July 14
ADHD waiting times
Performance in July for the waiting time between Connors (ADHD test) to therapy or medication has improved to 100% waiting less than 18 weeks. This is the first time in 2014/15 where performance targets have been met.
CAMHS - Percentage of
non-urgent referrals assessed
within 4 weeks (95%)
98.6% 100% 56.9% 100% 90.9% 82.8% 95.7% 95.0% 86.4% 94.4%
Data is reported on a monthly basis to enable timely understanding of performance as a whole. However the monthly data includes a number of potential exceptions, which if excluded would improve the performance. Therefore a second stage has been added to the process - a quarterly reconciliation whereby all exceptions are reviewed between NHS Doncaster CCG and RDASH. Once this process has been undertaken and exceptions agreed a final position is confirmed. Based on July’s likely outcome following exception reporting the likely figure will be 94.4%, just below the monthly target of 95%. 2 children were seen out of timeframe, each by 1 day. Investigations on whether this may have been an error with calculating cut off is underway.

28
Speech and language
Waiting Times
As at July 85.0% of people had been seen within 18 weeks with 22 active waiters waiting over 18 weeks. The high number of referrals into the service has created capacity issues which have in turn has meant high numbers of patients on the waiting list. The team are triaging patients according to clinical prioritisation and risk, therefore the patients with the longest waits have been assessed as lower clinical priority. It has been recognised that there has been a large increase in the number of referrals to both RDASH and DBHFT and a joint working party has been convened to review the issues in both areas. In addition as internal review is underway with RDASH AHP lead and team looking into options for increased agile working.

29
SECTION 2: OTHER COMMISSIONED SERVICES Nursing / Care Homes / Domiciliary Care Providers The information provided within this section is taken up to the 31st August 2014. Since the last Governing body meeting there have been 0 new embargoes against admissions/new care packages. There is currently one voluntary embargo against admissions within one care home within Doncaster. There is on-going work within across the Doncaster Partnership to support the necessary improvements within this home. As previously reported, CQC have taken additional actions against a care home provider in relation to removal of registration. This related to on-going concerns about the quality of care. In light of these concerns and actions by CQC, a decision was made to find alternate homes for residents. This process was led by the Local Authority with support from all relevant partners as necessary. New embargoes placed in August
Total Providers with embargoes in Place
Embargoes lifted in August
Total Providers with restrictions in Place
Restrictions lifted in July
0 1* 1 1** 0 *Includes 1 Voluntary embargo placed by provider. **Restrictions in place until December 2014. Doncaster Safeguarding Adults Partnership Board As previously reported, the Serious Case Review being undertaken by the Doncaster Safeguarding Adults Partnership Board (DSAPB) in relation to the Solar Centre continues. Publication of this report took place on the 17th of June 2014. Serious Case Reviews / Lesson Learnt Reviews The Governing Body was previously informed that the Doncaster Safeguarding Adults Partnership Board (DSAPB) had commissioned a Lessons Learnt Review. The DSAPB have identified an author for this review. The Terms of reference have been developed and a date arranged to for the relevant partners to meet and consider the lessons learnt.
The LSCB has recommended a Lessons Learnt review be undertaken in relation to the care provided to a child. This was presented to the Expert Panel (National) on the 8th September to consider prior to a final decision being made. The decision from the meeting will be available mid September.
There is one Lessons Learnt Review underway that is due to be reported to the September DSAPB meeting.

30
Yorkshire Ambulance Service (YAS) The ambulance response times for both the 8 minute Red 1 and Red 2 targets improved during August 2014. However both remain below target. Performance against the 19 minute target remains on track at 95.89% for August and 95.95% for the year to date. A remedial action plan to deliver both Red targets by March 2015 was submitted by YAS but rejected by Commissioners due to it not delivering the required standards. A meeting was held on 3rd September at which YAS presented a revised remedial action plan that will deliver targets for YAS as a whole for the quarter ending 31st December and also for the quarter ending 31st March. YAS reported that it was unlikely that targets will be met for the full year 2014-15. Doncaster CCG YAS Performance: March April May June July August
R1 MTD 67.05% 62.28% 61.40% 62.02% 61.05% 64.35% R1 YTD 79.03% 62.28% 62.01% 62.01% 61.81% 62.32% R2 MTD 71.11% 66.64% 68.18% 66.53% 66.90% 68.37% R2 YTD 74.47% 66.64% 67.39% 67.10% 67.05% 67.32%
SECTION 3: NHS Doncaster CCG Local Delivery Plans- Items to note The following item has been escalated for noting by the Governing Body in relation to the Local Delivery Plan: Special educational needs medical assessments completed within 6 weeks of request – In June 0 out of 28 assessments were completed within the targeted timeframe. Commissioners are exploring the reasons for this currently. Dementia Diagnosis Rate - This indicator is based on the annual QOF return. The number of people identified with dementia on the QOF list was 2075, an increase of 53; this means that 54.57% of people estimated to have dementia in Doncaster have been identified against a target of 59% at March 2014. This places Doncaster 66th out of 211 CCGs. A band 6 Primary Care Liaison Nurse is currently in place until July 2015 working with RDASH and GP practices to understand the current recording and referral process in place and helping to resolve any issues with data etc.
The Governing Body is requested to note following area of positive performance in relation to the Local Delivery Plan: Children - 5% Reduction in acute outpatient tariff activity: New and Follow Up. – In quarter one there were 84 new outpatient attendances in an acute setting against a target of 161 and 170 follow-up outpatient attendances in an acute setting against a target of 229. This demonstrates a significant transfer of activity from acute providers to the new community paediatric service.

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
11432 11432 11432 11432 11432 11432 11432 11432 11432 11432 11432 11432
11432 12004 11663 12632 12129 12449
14320 14320 14320 14320 14320 14320 14320 14320 14320 14320 14320 14320
14320 15036 14746 15855 15131 15510
A&E Attendances (All) DBHFT for last year 2013-2014 14375 15094 14380 14651 14578 15528 14261 14205 14336 13557 14392 13601 13061 15292
T Total Longest Wait in A&E department (hh:mm) 4 Hours > 4.2 Hours 13:37:00 13:39:00 16:03:00 15:44:00
T A&E waiting time - total time in the A&E department >=95% <95% 95.71% 95.35% 93.18% 91.79%
C Ambulance clinical quality – Category A (Red 2) 8 minute response time YAS >=75% <71.25% 70.65% 69.45% 68.38% 69.17% 70.29%
C Ambulance clinical quality – Category A (Red 2) 8 minute response time DONC >=75% <71.25% 66.64% 61.40% 62.02% 66.90% 68.37%
C Ambulance clinical quality – Category A (Red 1) 8 minute response time DONC >=75% <71.25% 66.64% 68.18% 66.53% 67.96% 64.35%
TAll handovers between ambulance and A&E must take place within 15 minutes -
those over 30 minutes0 >1 86 112 168 137
TAll handovers between ambulance and A&E must take place within 15 minutes -
those over 60 minutes0 >1 7 14 13 5
CPercentage of patients receiving first definitive treatment for cancer within 62-
days of a consultant decision to upgrade their priority status>=90% <85% 94.74% 100.00% 66.70% 81.48%
<= > 4 8 12 16 20 24 28 32 36 39 42 45
22 23 4 11 15 5
Maternity
C Maternal smoking at delivery <=21% >21% 22.30% 19.50% 18.90% 22.20%
TCancelled Operations - All patients who operations cancelled for non clinical
reasons to be offered another binding date within 28 days0 >0 3 2 0 6
T Time to initial assessment (95th percentile) hh:mm 15 Mins > 15 Mins 00:15 00:13 00:28 00:40
T Time to treatment in department (median) hh:mm 1 Hour >1 Hour 5 Mins 00:44 00:50 01:20 01:15
CImplementation of Stroke Strategy - Patients spending 90% Time on a Stroke
Unit (CCG)80% <80% 62.50% 57.60% 80.00% 70.30%
TImplementation of Stroke Strategy - Patients spending 90% Time on a Stroke
Unit80% <80% 68.9% 61.50% 81.30% 72.0%
CPeople who have had a stroke and are admitted to an acute stroke unit with
four hours of arrival to hospital90% 85.50% 56.3% 51.50% 56.00% 73.0%
TPeople who have had a stroke and are admitted to an acute stroke unit with
four hours of arrival to hospital90% 85.50% 60.0% 51.9% 53.1% 74.0%
Waiting Times
Other
Stroke & TIA
Cancer
Infection Control
Ambulance
Accident & Emergency
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Indicators Currently reported as RED or OFF TRACK
TBaseline
TBaseline
A&E Attendances (All) DBHFT
A&E Attendances (Type1) DBHFT
T Incidence of healthcare associated infection: C. difficile
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
T
Number of 52 week Referral to Treatment Pathways - the number of admitted
pathways greater than 52 weeks for admitted patients whose clocks stopped
during the period on an un-adjusted basis
0 0 0 0 3 ND
T
Number of 52 week Referral to Treatment Pathways - the number of non-
admitted pathways greater than 52 weeks for non-admitted patients whose
clocks stopped during the period
0 0 1 0 1 ND
T Diagnostic test waiting times >99% <99% 91.80% 89.40% 92.60% 90.60%
C Diagnostic test waiting times >99% <99% 92.60% 89.60% 92.90% 91.60%
C Ambulance clinical quality – Category A (Red 1) 8 minute response time YAS >75% <71.25% 69.78% 69.57% 68.01% 61.05% 71.33%
81 103 49 61 51 55 87 106 135 76 77 84
80 83 67 59
T
Number of 52 week Referral to Treatment Pathways - the number of
incomplete pathways greater than 52 weeks for patients on incomplete
pathways at the end of the period
0 >10 1 4 2 2
C
Number of 52 week Referral to Treatment Pathways - the number of
incomplete pathways greater than 52 weeks for patients on incomplete
pathways at the end of the period
0 >10 0 1 0 1
TThe percentage of admitted pathways within 18 weeks for admitted patients
whose clocks stopped during the period on an adjusted basis>=90% <85% 90.5% 90.7% 90.2% 89.2%
CPercentage of admitted pathways within 18 weeks for admitted patients whose
clocks stopped during the period on an adjusted basis>=90% <85% 90.2% 90.3% 89.8% 88.7%
3730 3916 3783 3831 3809 ND
T
Unplanned re-attendance rate - Unplanned re-attendance at A&E within 7 days
of original attendance (including if referred back by another health
professional)
5.00% 5.25% 0.6% 0.6% 0.2% 0.5%
T A & E - Left department without being seen rate 5% >5.25% 1.90% 2.40% 1.10% 0.40%
T Trolley waits in A&E <=12 Hours > 12 Hours 0 0 0 0
C Trolley waits in A&E <=12 Hours > 12 Hours 0 0 0 0
C Ambulance clinical quality - Category A 19 minute transportation time YAS >=95% <95% 96.19% 95.90% 95.54% 95.05%
C Ambulance clinical quality - Category A 19 minute transportation time DONC >=95% <95% 96.66% 99.80% 96.20% 95.02%
C All cancer two week wait >=93% <88% 95.70% 95.96% 95.12% 95.89%
Cancer
Accident & Emergency
Indicators Currently reported as GREEN or ON TRACK
Waiting Times
Ambulance
Childrens Plan On Page
C5% Reduction in emergency admissions for upper respiratory tract infections by
April 2015
5% Reduction or
MoreLess Than
Indicators Currently reported as AMBER or AT RISK
Ambulance
C Elective finished first consultant episodes (FFCEs)Baseline

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
C Two week wait for breast symptoms (where cancer was not initially suspected) >=93% <88% 97.41% 90.48% 91.97% 93.60%
CPercentage of patients receiving first definitive treatment within one month of
a cancer diagnosis>=96% <91% 98.67% 100.00% 97.44% 96.36%
C 31-day standard for subsequent cancer treatments- surgery >=94% <89% 96.60% 85.30% 100.00% 100.00%
C 31-day standard for subsequent cancer treatments- radiotherapy >=94% <89% 98.10% 97.10% 100.00% 100.00%
C 31-day standard for subsequent cancer treatment - anti cancer drug regimens >=98% <87% 100.00% 100.00% 100.00% 100.00%
CPercentage of patients receiving first definitive treatment for cancer within two
months (62 days) of an urgent GP referral for suspected cancer>=85% <80% 84.60% 84.50% 86.30% 86.4%
CPercentage of patients receiving first definitive treatment for cancer within 62-
days of referral from an NHS Cancer Screening Service>=90% <85% 100.00% 100.00% 100.00% 100.00%
C Number of emergency admissions as a result of cancer (Primary diagnosis)877 Per Year
219 Per QuarterHigher 64
T All cancer two week wait. >=93% <88% 94.40% 94.7% 94.0% 95.30%
T Two week wait for breast symptoms (where cancer was not initially suspected) >=93% <88% 96.30% 89.0% 92.2% 93.90%
TPercentage of patients receiving first definitive treatment within one month of
a cancer diagnosis>=96% <91% 100.00% 100.0% 98.1% 97.20%
T 31-day standard for subsequent cancer treatments-surgery >=94% <89% 95.00% 94.7% 100.0% 100.00%
T 31-day standard for subsequent cancer treatments-anti cancer drug regimens >=98% <87% 100.00% 100.0% 100.0% 100.00%
TPercentage of patients receiving first definitive treatment for cancer within two
months (62 days) of an urgent GP referral for suspected cancer>=85% <80% 87.40% 85.0% 87.8% 91.60%
TPercentage of patients receiving first definitive treatment for cancer within 62-
days of referral from an NHS Cancer Screening Service>=90% <85% 100.00% 100.0% 94.6% 96.70%
TPercentage of patients receiving first definitive treatment for cancer within 62-
days of a consultant decision to upgrade their priority status>=90% <85% 88.00% 97.1% 89.3% 85.2%
81 103 49 61 51 55 87 106 135 76 77 84
80 83 67 59
15 9 14 7
<= > 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0
<= > 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0
<= > 0 0 0
0 0 0 0 0 ND
<= > 10 19 26 33 39 45 52 59 66 75 84 91
Infection Control
Less Than
Childrens
C5% Reduction in emergency admissions for upper respiratory tract infections by
April 2015
5% Reduction or
More
C Incidence of healthcare associated infection: MRSA bacteraemia
CEmergency admissions for children with lower respiratory tract infections
(LRTIs)
<114 at Q4, <423
per annumMore than
38
306
T Incidence of healthcare associated infection: MRSA bacteraemia
T Incidence of healthcare associated infection: MRSA bacteraemia
C Incidence of healthcare associated infection: C. difficile

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
35 36 4 10 9 12 3
<= > 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 ND
T
Mental Health Measure – Care Programme Approach (CPA) - The proportion of
those patients on Care Programme Approach (CPA) discharged from inpatient
care who are followed up within 7 days (stretch local target)
95% <90.25% 98% 100.0% 100% 100%
=> <
3.92%
T Maternal smoking at delivery <=21% >21% 22.30% 19.20% 18.30% 20.00%
T Antenatal assessments <13 weeks >=85% <85% 83.7% 85.5% 84.3% 90.3%
C Antenatal assessments <13 weeks >=85% <85% 86.7% 85.1% 82.6% 90.3%
C Mixed Sex Accommodation (MSA) Breaches CCG 0 >0 0 0 0 0
T Mixed Sex Accommodation (MSA) Breaches (DBHFT) 0 >0 0 0 0 0
T Mixed Sex Accommodation (MSA) Breaches (RDASH) 0 >0 0 0 0 ND
C Percentage of Call backs within 20 Minutes (Triage of urgent calls) >=95% <90% 89.05% 96.32% 97.60% 96.40%
C Percentage of Call backs within 60 Minutes (Triage of all other calls) >=95% <90% 96.88% 98.74% 99.86% 99.73%
C Percentage of Home visits made within 2 Hours (urgent) >=95% <90% 100.00% 100.00% 100.00% 100.00%
C Percentage of Home visits made within 6 Hours (less urgent) >=95% <90% 100% 100.00% 100.00% 100.00%
C Percentage of Consultations Made within 2 Hours (UCC) - Urgent >=95% <90% 100.00% 100.00% 100.00% 100.00%
C Percentage of Consultations Made within 6 Hours (UCC) - Less Urgent >=95% <90% 100% 99.93% 100.00% 99.90%
C Total Number of calls made to service 6290 6319 5279 5127
CImplementation of Stroke Strategy - TIA Patients Assessed and Treated within
24 Hours (CCG)60% <60% 82.80% 74.30% 85.70% 73.30%
TImplementation of Stroke Strategy - TIA Patients Assessed and Treated within
24 Hours60% <60% 82.9% 70.00% 81.80% 78%
C
Number of 52 week Referral to Treatment Pathways - the number of admitted
pathways greater than 52 weeks for admitted patients whose clocks stopped
during the period on an un-adjusted basis
0 0 0 0 1 0
C
Number of 52 week Referral to Treatment Pathways - the number of non-
admitted pathways greater than 52 weeks for non-admitted patients whose
clocks stopped during the period
0 0 0 0 1 0
Out Of Hours
Stroke & TIA
Mixed Sex Accomodation
Mental Health
T
Mental Health Measure- Improved access to psychological services - The
proportion of people that enter treatment against the level of need in the
general population (the level of prevalence addressed or ‘captured’ by referral
routes)
3.75% 7.50% 11.25% 15.00%
2.75%
Maternity
C Incidence of healthcare associated infection: C. difficile
T Incidence of healthcare associated infection: C. difficile
Waiting Times

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
TThe percentage of non-admitted pathways within 18 weeks for non-admitted
patients whose clocks stopped during the period>=95% <90% 95.52% 95.35% 95.42% 95.20%
CPercentage of non-admitted pathways within 18 weeks for non-admitted
patients whose clocks stopped during the period>=95% <90% 95.96% 95.42% 95.38% 95.88%
TThe percentage of incomplete pathways within 18 weeks for patients on
incomplete pathways at the end of the period>=92% <87% 92.4% 92.95% 92.58% 92.40%
CPercentage of incomplete pathways within 18 weeks for patients on incomplete
pathways at the end of the period>=92% <87% 92.06% 92.69% 92.27% 92.17%
3199 3359 3163 3259 3199 ND
8136 8543 7010 7603 7939 8040
2013 2014
5% Reduction or
moreMore than 7
C 100% completion IHA within 60 working days all LAC 31/03/14 100 Less Than 85.00% 57% ND ND
C90% Initial Health Assesments (in area) completed within 28 working days by
31/03/1540% Less Than 38.00% 29.00% ND ND
CPercentage of patients receiving first definitive treatment for cancer within 62-
days of a consultant decision to upgrade their priority status. CCG>=90% <85% 94.74% 100.00% 66.70% 81.48%
3149 3129 3041 3225 3139 3059 3169 3146 3222 3232 2736 3167
< = 3099 > 3253 3163 3269 3206 ND
248 248 248 248 248 248 248 248 248 248 248 248
< = 236 > 248 219 273 200 ND
C All cancer two week wait. CCG >=93% <88% 95.70% 95.96% 95.12% 95.89%
CTwo week wait for breast symptoms (where cancer was not initially suspected).
CCG>=93% <88% 97.40% 90.48% 91.97% 93.60%
CPercentage of patients receiving first definitive treatment within one month of
a cancer diagnosis CCG>=96% <91% 100.00% 100.00% 97.44% 96.36%
C 31-day standard for subsequent cancer treatments-surgery >=94% <89% 96.60% 85.30% 100.00% 100.00%
Cancer Plan On Page
Unplanned Care Plan On Page
Childrens Plan On Page
PLANS ON A PAGE
Indicators Currently reported as RED or OFF TRACK
Cancer Plan On Page
C Non-elective FFCEs (First Finished Consultant Episode)Baseline
C All first outpatient attendancesBaseline
C 5% reduction in emergency admissions - LRTI
42 17 166 80
38
Indicators Currently reported as AMBER or AT RISK
Indicators Currently reported as GREEN or ON TRACK
C Zero growth In Emergency Hospital admissions against 13/14 outtun13/14 Baseline
C Zero growth in emergency admissions for Chronic ACSC against 13/14 outturn 13/14 Baseline

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
C 31-day standard for subsequent cancer treatments-radiotherapy >=94% <89% 98.10% 97.10% 100.00% 100.00%
C 31-day standard for subsequent cancer treatments-anti cancer drug regimens >=98% <87% 100.00% 100.00% 100.00% 100.00%
CPercentage of patients receiving first definitive treatment for cancer within two
months (62 days) of an urgent GP referral for suspected cancer. CCG>=85% <80% 84.62% 84.48% 87.93% 86.44%
CPercentage of patients receiving first definitive treatment for cancer within 62-
days of referral from an NHS Cancer Screening Service. CCG>=90% <85% 100.00% 100.00% 100.00% 100.00%
C Improve 39% treatment from 2ww 39% <37.05%
C 82% patients having curative treatments 82% <77.9%
C 66% one or two GP attendances prior to referral 66% Less Than
C Reduction in Emergency admissions as a result of cancer 220 per Quarter Higher Than 63 70 59
192 186 162 129
9.11
23
CWe will ensure that readmission rates back to mental health services up to 30
days post discharge are less than 10%< 10% Greater Than ND
C15% of people with anxiety and depression will access psychological therapies
by 2014/15 6.50% Q2 1.1% 1.87% 2.75% 3.92%
>=20.87% <21.91% ND ND
< = 23258 > 24420 ND
C No Ambulance delays over 30 minutes at ED 0 >0 ND
C Achievement of 95% A&E 4 hour access target >=95% <95% 95.71% 95.35% 93.18% 91.79%
Dementia Plan On Page
74.00%
Continuing Health Care
Indicators Currently reported with no RAG rating
56.99%
82.25%
C Admissions to DRI against 13/14 outturn 124 Greater Than
517 466 525 511
540
Mental Health
C Average length of stay (DRI) against 13/14 outturn Greater Than10.13 11.05 10.27 10.40
11.20
C Hospital readmissions to DRI within 30 days against 13/14 outturn Greater Than93 79 89 101
105
2.86%
ND
CZero growth in conversion rate of ED attendances to admissions from 13/14
baseline
13/14 Baseline 20.87% 20.87% 20.87% 20.87%
C People with dementia who had an episode of crisis against 13/14 outturn < 3 Greater Than0 0 0 ND
0 0
Unplanned Care Plan On Page
C Zero growth in A&E attendance against 13/14 outturn Doncaster Patients 13/14 Baseline 23258 23258 23258 23258
ND
20.35%

LOC Indicator Pass Condition Fail Condition Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Doncaster CCG 2014/15 Performance Report Q1 Q2 Q3 Q4
Doncaster CCG 2014/15 Performance ReportCCG
DBHFT
RDaSH
Misc Delivery Plans
Key:T = Trust Targets
C = CCG related Targets
ND No Data Available
C Reduce national benchmarking ranking by quarter 4 submitted results (Activity)
C Reduce national benchmarking ranking by quarter 4 submitted results (Cost)
CDevelop mechanisms to ensure that total spend against budget is full
understood and reported against on a monthly basis
C
Develop robust and detailed understanding of patient flow at aggregate and
individual level, with appropriate targets being agreed by 31 March 2014 for
14/15
CQuarterly review of % of Fast Tracks over 90 days, leading to the development
and agreement of an appropriate target for 14/15 (Cum)
CUnplanned hospitalisation for asthma, diabetes and epilepsy in under 19s
9 20 20 18
T Friends and Family Test (Inpatients) 74 76 77 45
T Friends and Family Test (A&E) 54 -3 24 35
TPatient Reported Outcome Measures (PROMS) for elective procedures – Live:
Unilateral Hip Replacements (Primary and Revisions),No Target No Target
TPatient Reported Outcome Measures (PROMS) for elective procedures – Live:
Unilateral Knee Replacements (Primary and Revisions)No Target No Target
TPatient Reported Outcome Measures (PROMS) for elective procedures – Live:
Groin Hernia Surgery,No Target No Target
TPatient Reported Outcome Measures (PROMS) for elective procedures – Live:
Varicose Vein SurgeryNo Target No Target
1st 2nd 2nd
All Other
5th 1st 1st
Under Development
Under Development
8.12%


Enc C
Finance Report


1
Meeting name Governing Body
Meeting date 18th September 2014
Title of paper
2014/15 Finance Report June 2014 (Month 4) Executive Summary
Executive / Clinical Lead(s)
Hayley Tingle Chief Finance Officer
Author(s) Hayley Tingle
Chief Finance Officer
Purpose of Paper – Executive Summary This report sets out the financial position as at the end of July 2014. The CCG is currently achieving all of its financial targets and at this early stage in the year is forecasting full achievement by 31 March 2015. The report also outlines:
• The key risk areas relating to primary care prescribing, the Doncaster and Bassetlaw Hospitals NHS Foundation Trust contract and Continuing Healthcare including specialist placements
• A summary of the CCG Efficiency Savings plan for 2014/15 (Appendix 2)
• A summary of the CCG’s Resource Allocation (Appendix 3)
• A summary of the CCG’s Reserve position (Appendix 4)
• A summary of the CCGs scheme of delegation authorisation threshold (Appendix 5)
• Annual Audit Letter 2013/14 (Appendix 6)

2
Recommendation(s) Members are asked to receive the report and note the financial position.
Impact analysis
Assurance Framework
1.2, 1.4, 2.4, 3.1, 3.2, 6.2
Risk analysis
The CCG continues to identify a number of risks in 2014/15. These include:
• Additional costs arising from the growth in continuing healthcare packages
• Potential over performance against the main acute contracts
• Unforeseen prescribing costs
• Potential non delivery of parts of the Efficiency Savings programme
However the CCG has sufficient flexibility within the overall CCG allocation to meet these challenges whilst still achieving the target surplus. The 0.5% contingency will be used to mitigate against any financial risks as they arise in year together with flexing the non recurrent head room reserve if required.
Equality impact
None Identified
Sustainability impact
Nil
Financial implications
Highlighted within the Report
Legal implications
None identified
Consultation / Engagement
N/A

3
NHS DONCASTER CCG 2014/15 FINANCE REPORT MONTH 04 JULY 2014 1. Introduction
This report provides an update on the financial position for NHS Doncaster CCG for 2014/15 as at July (Month 4). Overall, the CCG is achieving all financial targets year to date and is forecasting achievement for the financial year 2014/15, although at this stage of the year it is important to note this is based on very early information. The report also includes appendices which give a brief overview of the threshold values included with the Scheme of Delegation and copy of the Annual Audit letter summarising the audit outcome for 2013/14. 2. Current Position The year to date position reflects a surplus of £2,194k which is consistent with the profiled surplus. In line with the agreed control total, the CCG is forecasting a £6.6m surplus. The current position is summarised in the Operating Cost Statement included at Appendix 1. 3. Key Messages and Risks
The largest financial risk facing the CCG continues to be Continuing Healthcare. Following the comprehensive review of the service all the action plans continue to be enacted and delivered during 2014/15 and will be revised as necessary, the financial implications of this will be reported during the year. Other risks include the over performance on acute contracts, unforeseen prescribing costs and the non delivery of parts of the Efficiency Programme. To help manage and offset these risks a contingency fund has been established. Further mitigation includes the ability to flex the non recurrent expenditure including the 2.5% headroom. Taking each risk in turn: Continuing Care As reported last month, based on the current CHC database information, the projected annual expenditure will be broadly in line with the allocated budget. The timing of invoices sent by Providers is often delayed which results in difficultly during the first few months of the financial year to accurately forecast expenditure. Any pressures however will be reported during the year. At this stage in the year no significant financial risks are being highlighted.

4
Doncaster and Bassetlaw Hospitals NHS Foundation Trust The latest available information is in respect of Month 4 (July) and the contract is showing a financial overspend as a result of increased performance against elective activity. The majority of the over performance relates to increased activity as the trust continues to improve against the 18 week target, a targeted non recurrent resource has been allocated to support the 18 RTT position which is in additional to national funding allocation which is targeting a number of specialities facing RTT pressures. Primary Care Prescribing The Prescription Pricing Authority provides a profile for expected monthly prescribing expenditure. We are in receipt of June’s actual data which suggests a slight under spend against profile similar to last year. However, from previous experience the profiles have not been particularly accurate so early in the year so an estimate of breakeven has been included in the forecast figures. The expenditure will be monitored monthly and adjustments made as necessary. 4. Efficiency Savings Programme
The efficiency savings programme has been developed to encompass a range of areas for disinvestment, re-engineering pathways and cost avoidance measures amounting to £4.5m (See Appendix 2). Schemes have been identified and are being implemented with leads working on their areas of responsibility. A prudent approach has been taken to the amount of savings that will be achieved at this stage in the year as the evaluation of schemes will take time to process. It should be noted that the budget lines and contract values shown in Appendix 1 are after the efficiency saving targets have been deducted. All contract values negotiated with providers were agreed net of efficiency saving targets where appropriate. Detailed discussions with managers continue to take place to ensure that the savings programme and its delivery remains “high profile”. It is still too early to ascertain if there are any significant variances from the planned profile of savings, however there are no indications that there are any other risks to achieving the savings, other than those identified in the CCG’s plans. More detailed information will be available shortly as a detailed review is being undertaken of the first quarter’s complete activity. 5. 2.5% Non Recurrent Headroom The CCG has set aside £10.8m (2.5% of the CCG’s recurrent allocation) and plans to fully spend this resource in 2014/15. Commitments relating to waiting list improvements and service redesign costs have been made against this

5
reserve and work is ongoing with managers to determine progress which will result in release of funding into budgets. 6. Further Allocations The CCG has been notified of a non recurrent allocation of £452k to support secondary care prison health; this is an interim position until the commissioning arrangements are clarified with NHS England. Two further transfers of £593k and £67k have been agreed with NHS England and largely relate to a realignment of overheads within the RDASH contract and is a further refinement of the former PCTs legacy arrangements. However this has no impact on the CCG financial position. 7. Capital Resource
No further updates to report. 8. Other Key Financial Targets Revenue spend maintained within Resource Limit
The risk of breaching the revenue resource limit total at the year end is assessed as low.
9. Better Payment Policy Performance against the better payment policy is managed by the Commissioning Support Unit and information is now provided on a monthly basis. As at the end of July the CCG has achieved 99.99% of NHS invoices paid within 30 days and 98.53% of non NHS invoices within 30 days giving an overall total of 99.73% 10. Conclusion and Recommendations Members are asked to: Receive and note the Finance Report for July 2014 (month 4).

6

NHS DONCASTER CLINICAL COMMISSIONING GROUP Appendix 1
2014/15 FINANCE REPORT JULY 2014
Recurrent
Budget
£000s
Non Rec
Budget
£000s
Total
Budget
£000s
Forecast
Outturn
£000s
Variance
(Under)/
Over
£000s
Recurrent
Budget
£000s
Non Rec
Budget
£000s
Total
Budget
£000s
YTD Actual
£000s
Variance
(Under)/
Over
£000s
Baseline Allocation -414,774 -7,130 -421,904 -421,904
Running Cost Allowance -7,639 -7,639 -7,639
Initial Allocation -422,413 -7,130 -429,543 0 -429,543
Transfer to NHS England 0 0
GP IT -785 -785 -785
8 to 8 Registered Patients 753 753 753
Colposcopy 67 67 67
RDASH Community HV 593 593 593
Offender Health -452 -452 -452
TOTAL ALLOCATIONS -421,000 -8,367 -429,367 0 -429,367 -138,362 -138,362 0
Acute Contracts - DBHFT 175,988 21 176,009 176,009 0 59,094 0 59,094 59,952 859
Acute Contracts - Other NHS 32,096 452 32,548 32,548 0 11,765 0 11,765 10,846 -919
Acute Contracts - Other Providers Non NHS 3,918 58 3,976 4,130 154 1,364 0 1,364 1,569 205
Acute - Non Contract Activity 2,656 0 2,656 2,564 -92 885 0 885 838 -48
Total Acute Services 214,658 531 215,190 215,252 62 73,108 0 73,108 73,205 97
Mental Health Contracts - RDaSH FT 35,696 0 35,696 35,696 0 11,899 0 11,899 11,881 -18
Mental Health Contracts - Other NHS 309 0 309 334 26 103 0 103 129 26
Mental Health Contracts - Other Providers 11,985 0 11,985 12,014 29 3,995 0 3,995 4,005 10
Mental Health - Non Contract Activity 177 0 177 177 0 59 0 59 52 -7
Total Mental Health Services 48,167 0 48,167 48,221 54 16,056 0 16,056 16,066 10
Community Contracts - RDaSH FT 27,604 0 27,604 27,610 5 9,201 0 9,201 9,201 0
Community Contracts - Other NHS 377 0 377 374 -2 125 0 125 125 -1
Community Contracts - Other Providers 3,173 553 3,725 3,722 -4 1,232 0 1,232 1,228 -4
Total Community Services 31,153 553 31,706 31,706 -1 10,559 0 10,559 10,555 -5
Prescribing 57,460 0 57,460 57,460 0 19,192 0 19,192 19,150 -41
Oxygen Services 511 0 511 558 47 170 0 170 190 19
Other Primary Care Services 2,233 0 2,233 2,218 -15 744 0 744 748 3
GPIT 0 785 785 785 0 0 0 0 0 0
Medical Recommendations 135 0 135 149 14 45 0 45 26 -19
Primary Care Services 60,339 785 61,124 61,170 46 20,151 0 20,151 20,114 -37
Continuing Healthcare 38,154 0 38,154 38,193 39 12,718 0 12,718 12,746 28
Continuing Healthcare Services 38,154 0 38,154 38,193 39 12,718 0 12,718 12,746 28
Medicines Management 550 0 550 537 -14 183 0 183 176 -8
Admin & Business Support 2,007 -102 1,905 1,905 1 489 0 489 510 21
Contract Management 363 0 363 381 18 121 0 121 145 24
Finance 653 14 667 600 -67 225 0 225 181 -44
Patient & Public Involvement 159 12 171 163 -7 57 0 57 54 -3
Performance 426 0 426 415 -10 142 0 142 124 -18
Quality Assurance 632 0 632 623 -9 211 0 211 205 -6
Strategy & Development 895 70 964 867 -97 333 0 333 290 -43
Governing Body 1,292 6 1,298 1,286 -12 436 0 436 430 -7
CSU recharge 1,769 0 1,769 1,739 -30 590 0 590 560 -30
NHS Property Services Recharge 2,337 0 2,337 2,348 12 779 0 779 783 4
Total Corporate Costs 11,081 0 11,081 10,864 -217 3,565 0 3,565 3,457 -109
Winter Pressures 0 121 121 121 0 0 0 0 26 26
Winter Pressures 0 121 121 121 0 0 0 0 26 26
2.5% Non Recurrent Headroom Reserve 10,117 10,117 10,117 0 0 0 0 0 0
Contingency Reserve 0.5% 2,148 0 2,148 2,148 0 0 0 0 0 0
Investments 4,947 0 4,947 4,947 0 0 0 0 0 0
Total Reserves 7,095 10,117 17,212 17,212 0 0 0 0 0 0
TOTAL APPLICATION OF FUNDS 410,648 12,107 422,755 422,739 -16 136,158 0 136,158 136,168 10
SURPLUS 1% REQUIREMENT* 6,612 0 -6,612 2,204 0 -2,204
TOTAL 429,367 422,739 -6,628 138,362 136,168 -2,194
* As directed by NHS England - All CCGs are required to make a surplus of at least 1%
OPERATING COST STATEMENT
YEAR TO DATE

Appendix 2
NHS DONCASTER CLINICAL COMMISSIONING GROUP
Savings / Efficiency Programme 2014/15
Programme Project Transformational / Transactional Lead Clinical Lead 2014/15 Target Risk
Elective Care Reduction in Face to Face Patient contacts work stream Transactional
Richard Metcalfe Dr. Marco Pieri 50 Medium
Paediatrics Service redesign - reduction in outpatients Transactional Lee Golze Dr. Pat Barbour 121 Medium
Alternative Ophthalmology Pathway FYE Transformational Richard Metcalfe Dr. Marco Pieri 25 Low
Telederm Scheme FYE Transformational Richard Metcalfe Dr. Marco Pieri 30 Low
Urology pathways (Acute retention & LUTS) Transformational Richard Metcalfe Dr. Marco Pieri 60 Medium
Methotrexate (weekly patients) Transactional Richard Metcalfe Dr. Marco Pieri 20 Low
Cancer Follow Up Pathways FYE Transformational Richard Metcalfe Dr. Marco Pieri 30 Low
Total Schemes 336
Unplanned Care Assessment Tariff in Paeds, Medicine & Surgery Transformational
Lee Golze Dr. Pat Barbour 0 High
Children's service redesign reduction in NEL activity Transactional Lee Golze Dr. Pat Barbour 12 Low
Reduction in Emergency admissions - Care of the frailty , ECP , care home admissions Transformational tbd Dr. Andy Oakford 640 Medium
Reduction in Emergency Readmissions - Cancer Schemes Richard Metcalfe Dr. Marco Pieri 92 Low
Reduction in Emergency Readmissions - COPD Schemes Jo Forrestall Dr. Andy Oakford 75 Low
Total Schemes 819
Prescribing All Prescribing schemes including : Mark Randerson Dr. Jeremy Bradley 600 Low
Waste reduction TransactionalMark Randerson Dr. Jeremy Bradley 700 Medium
Repeat Prescribing TransactionalMark Randerson Dr. Jeremy Bradley 700 High
Total Schemes 2,000
Vulnerable People MH Schemes to be determined Transformational Wayne Goddard Dr. Niki Seddon 50 Medium
Implementation of CHC commissioning criteria & Fast Tracks Transactional Claire Hudson Dr. Lindsey Britten 900 High
Total Schemes 950
Other Schemes Property Utilisation Transactional Hayley Tingle - 400 Medium
Risk Mitigation - - - -5 Low
2014/15 TOTAL 4,500

NHS DONCASTER CLINICAL COMMISSIONING GROUP APPENDIX 3
SUMMARY OF RESOURCE ALLOCATIONS AS AT MONTH 4 JULY 2014
Recurrent Non Recurrent Total
£000's £000's £000's
Recurrent Baseline -414,774 -414,774
Non Recurrent Surplus from 2013/14 -7,130 -7,130
Running Cost Allowance -7,639 -7,639
Total Resources Available at Plan Stage -422,413 -7,130 -429,543
Adjustments to the Resource Limit:
Month 01 April
No adjustments 0 0 0
0 0 0
Month 02 May
No adjustments 0 0 0
0 0 0
Month 03 June
GPIT Allocation -785 -785
Transfer to NHS England for registered population of 8-8 centre 753 753
753 -785 -32
Month 04 July
Transfer to NHS England for overheads associated with Health
Visiting service provided by RDASH
593 0 593
Transfer to NHS England for colposcopy 67 67
Transfer of funding for Offender Health -452 -452
660 -452 208
Revised Resources available as at Month 12 March 2015 -421,000 -8,367 -429,367

NHS DONCASTER CLINICAL COMMISSIONING GROUP APPENDIX 4
SUMMARY OF RESERVES AS AT MONTH 4 JULY 2014
RESERVES Recurrent Non Total
Recurrent
£000's £000's £000's
INVESTMENT RESERVES
Inital Plan 5,000 0 5,000
Budget Transfers
New GP LES Schemes 14/15 -53 -53
0
0
0
0
4,947 0 4,947
RISK RESERVES AND CONTINGENCIES
2.5% Non Recurrent Headroom
Initial Plan 0 10,870 10,870
Complex Assessment Beds (April - June) -86 -86
Complex Assessment Beds (July-March) -467 -467
Discharge Planning Support to DRI -21 -21
Patient Transport (additional crew) -58 -58
Extension of winter schemes -121 -121
0 10,117 10,117
0.5% Contingency
Initial Plan 2,148 0 2,148
No transfers as at Month 4
2,148 0 2,148
2,148 10,117 12,265
7,095 10,117 17,212
Cross Check to Operating Cost Statement 7,095 10,117 17,212

NHS DONCASTER CCG AUGUST 2014
Scheme of Delegation - Paragraph 13.3.1 Budgetary Delegation
Chief Officer - Chris Stainforth ) - for single transactions of expenditure over £150,000 within the CCG's approved budgets two signatures required
Deputy Chief Officer - Jackie Pederson )
Chief Finance Officer - Hayley Tingle )
Chief Officer - Chris Stainforth ) - may authorise single transactions of expenditure up to £150,000
Deputy Chief Officer - Jackie Pederson )
Chief Finance Officer - Hayley Tingle - may authorise single transactions of expenditure up to £100,000
Group 1 - Sarah Atkins Whatley / Mary Shepherd ( - may authorise single transactions of expenditure up to £50,000
( - may authorise budget virements between non pay lines up to £25,000
(
(
Group 2 -
Mark Randerson / Wayne Goddard / Julia Holmes / Claire Hudson / ) - may authorise single transactions of expenditure up to £10,000
Ailsa Leighton / Martha Coulman / Richard Metcalfe / Lee Golze ) - as delegated by a member of Group 1 (up to maximum of their delegated authority) in the absence of the member
Jo Forrestall / Suzannah Cookson / Tina Greaves / Tracy Wyatt )
Budget Managers (Band 7 and above) ) - may authorise single transactions of expenditure up to £5,000
) - may authorise budget virements between non pay lines up to £5,000)
)
Other Staff (Bands 4,5 and 6) ) - may authorise single transactions of RDC and print room expenditure up to £1,000
) - may authorise single transactions of other expenditure up to £250
NHS DONCASTER CLINICAL COMMISSIONING GROUP
The following Scheme of Delegation applies to nominated officers working on behalf of the Doncaster Clinical Commissioning Group.
SBS Thresholds for the Authorisation of Requisitions and ad hoc Invoices (where approval in principle has been given in line with the Procurement Strategy)
INTRODUCTION
Tendering and Contracting - Single Quote / Tender Waivers
(See Section 17 of Standing Orders, Reservation and Delegation of Powers and Standing Financial Instructions)
The full scheme of Reservation and Delegation of Powers is included in Section C of the NHS Doncaster CCG Standing Orders, Reservation and Delegation of Powers and Standing Financial
Instructions located on the NHS Doncaster website.
Budget Holders and Budget Managers must adhere to the rules contained in the Standing Orders, Reservation and Delegation of Powers and Standing Financial Instructions when managing their
delegated budget.
The thresholds up to which Budget Holders and Budget Managers may authorise expenditure (in a single transaction or several transactions to the same company / provider for the same service), the
movements (virements) between pay and non-pay and the movements (virements) between lines which are management costs are detailed below.
ALIGNMENT WITH PROCUREMENT STRATEGY (please refer to full document for further detail)
If estimated expenditure is expected to exceed £50,000 then formal tendering procedures apply. If estimated expenditure is expected to exceed £10,000 but not exceed £49,999.99, competitive quotation
procedures apply. In certain circumstances (see paragraphs 17.8.1 and 17.5.4), both formal tendering and competitive quotation procedures may be waived. In these circumstances, a Single
Quote/Tender Waiver Request Form must be completed and submitted to the Chief Finance Officer for approval. Tender waivers also require Chief Officer approval.
Capital or Revenue Healthcare or Non Healthcare contracts exceeding the following thresholds over a period of 3 years (or the period of contract if longer) must be approved by the following:
- £10 million and above = The Governing Body
- Up to £9,999,999.99 = Chief Officer
of Group 1, for extended periods of annual leave and sickness
- must have approval of Chief Finance Officer before moving budget between pay and non pay lines or lines involving running
costs
- must have approval of Chief Finance Officer before moving budget between pay and non pay lines or lines involving running
costs
Enc C3 Copy of Scheme of budgetary R and D of P CCG August 2014

Commissioning :
Chief Officer - Chris Stainforth - may authorise single transactions of healthcare and non healthcare expenditure up to £20m
Deputy Chief Officer - Jackie Pederson - may authorise single transactions of healthcare and non healthcare expenditure up to £20m
Chief Finance Officer - Hayley Tingle - may authorise single transactions of healthcare and non healthcare expenditure up to £20m
Deputy Chief Finance Officer - Tracy Wyatt
Assistant Head of Finance - Julia Holmes - may authorise single transactions of healthcare expenditure up to £20m in line with contract value
Head of Contracting - Claire Hudson - may authorise single transactions of healthcare expenditure up to £20m in line with contract value
Head of Strategy & Delivery (Vulnerable People) - Wayne Goddard - may authorise single transactions of healthcare expenditure up to £4m in line with contract value
Mark Randerson / Wayne Goddard / Julia Holmes / Claire Hudson / ) - may authorise single transactions of healthcare and non healthcare expenditure up to £10,000
Ailsa Leighton / Martha Coulman / Richard Metcalfe / Lee Golze )
Jo Forrestall / Suzannah Cookson / Tracy Wyatt )
Commissioning :
Chief Officer - Chris Stainforth - may sign SLAs and authorise CVs within the CCG's approved budgets
Deputy Chief Officer - Jackie Pederson - may sign SLAs and authorise CVs within the CCG's approved budgets
Chief Finance Officer - Hayley Tingle - may sign SLAs and authorise CVs within the CCG's approved budgets
Deputy Chief Finance Officer - Tracy Wyatt
Assistant Head of Finance - Julia Holmes - may sign SLAs and authorise CVs within the CCG's approved budgets
Head of Contracting - Claire Hudson - may sign SLAs and authorise CVs within the CCG's approved budgets
Chief of Corporate Services - Sarah Atkins Whatley - may sign non-healthcare corporate services SLAs and authorise CVs within the CCG's approved budgets
Head of Strategy & Delivery (Vulnerable People) - Wayne Goddard - may sign SLAs (including individual care packages) and authorise CVs up to £50k within the CCG's approved budgets
Mark Randerson / Ailsa Leighton / Martha Coulman / Richard Metcalfe ) - may authorise CVs up to £50k within the CCG's approved budgets
Jo Forrestall / Suzannah Cookson / Lee Golze )
Weekly Pay Runs (BACS and payable orders) - see list attached
Schedule of payments to other NHS Bodies (RFT Transfer) - see list attached
Tax, NI and Pension payment schedules - see list attached
CHAPS payments (same day payment into creditors bank account) - see list attached
Chief Finance Officer - Hayley Tingle - may authorise any item of expenditure against balance sheet codes
Deputy Chief Finance Officer - Tracy Wyatt
Assistant Head of Finance - Julia Holmes - may authorise any item of expenditure against balance sheet codes
Head of Contracting - Claire Hudson - may authorise any item of expenditure against balance sheet codes
Chief Officer - Chris Stainforth - may authorise any items of capital expenditure within the CCG's approved capital budgets
Deputy Chief Officer - Jackie Pederson - may authorise any items of capital expenditure within the CCG's approved capital budgets
Chief Finance Officer - Hayley Tingle - may authorise any items of capital expenditure within the CCG's approved capital budgets
Deputy Chief Finance Officer - Tracy Wyatt - may authorise single transactions of capital expenditure up to £10,000 for approved projects
Assistant Head of Finance - Julia Holmes - may authorise single transactions of capital expenditure up to £10,000 for approved projects
Head of Contracting - Claire Hudson - may authorise single transactions of capital expenditure up to £10,000 for approved projects
Budget Managers (Band 8b and above) - may authorise single transactions of capital expenditure up to £10,000 for approved projects
The Audit Committee - may authorise single items of loss or a special payment up to £10,000
The Governing Body - may authorise single items of loss or a special payment in excess of £10,000Chief Officer and Chair of the Audit Committee (ratify at next meeting) - may authorise URGENT special payments up to £10,000 Chief Officer and Chair of the Governing Body (ratify at next meeting) - may authorise URGENT special payments in excess of £10,000
Balance Sheet
SBS Thresholds for the Authorisation of Invoice payments relating to agreed healthcare and non healthcare contracts
(where approval in principle has been given in line with the Procurement Strategy)
Service Level Agreements (SLAs) (including individual care packages) and Contract Variations (CV's) - healthcare and non healthcare
- may sign SLAs and authorise CVs within the CCG's approved budgets EXCLUDING DONCASTER & BASSETLAW
HOSPITAL NHS FOUNDATION TRUST
- may authorise any item of expenditure against balance sheet codes EXCLUDING those associated with DONCASTER &
BASSETLAW HOSPITAL NHS FOUNDATION TRUST
Writing off Losses and authorising Special Payments
Single items of Loss or Expenditure
Capital
Payment Schedules
Items of expenditure over £5,000 (or inter-dependant items of lesser value but with a group value over £5,000) are classified as capital.
- may authorise single transactions of healthcare expenditure up to £4m in line with contract value EXCLUDING DONCASTER
& BASSETLAW HOSPITAL NHS FOUNDATION TRUST
Enc C3 Copy of Scheme of budgetary R and D of P CCG August 2014
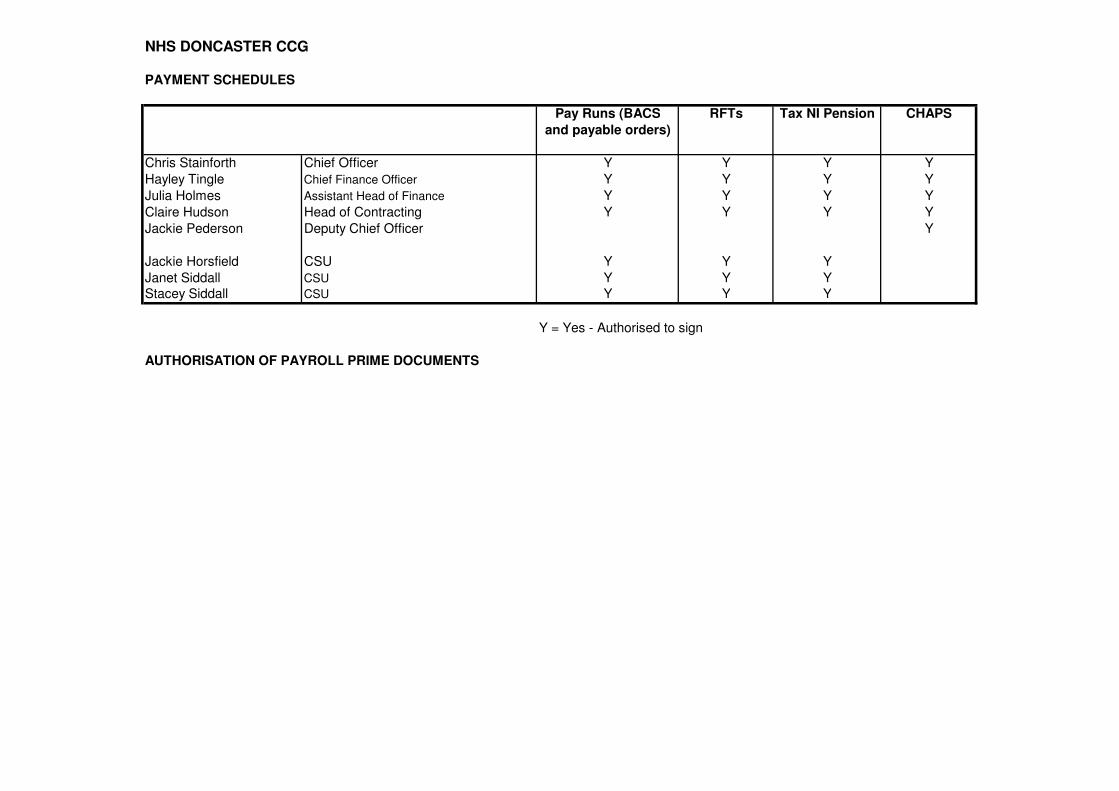
NHS DONCASTER CCG
PAYMENT SCHEDULES
Pay Runs (BACS RFTs Tax NI Pension CHAPS
and payable orders)
Chris Stainforth Chief Officer Y Y Y Y
Hayley Tingle Chief Finance Officer Y Y Y Y
Julia Holmes Assistant Head of Finance Y Y Y Y
Claire Hudson Head of Contracting Y Y Y Y
Jackie Pederson Deputy Chief Officer Y
Jackie Horsfield CSU Y Y Y
Janet Siddall CSU Y Y YStacey Siddall CSU Y Y Y
Y = Yes - Authorised to sign
AUTHORISATION OF PAYROLL PRIME DOCUMENTS

Appendix 5 NHS DONCASTER CCG Scheme of Delegation Authorisation threshold limits Introduction
This report provides a brief summary of how the authorisation limits are set within the Budgetary Scheme of Delegation (SoD), as attached within this document. Methodology The amounts in the Scheme of Delegation for Healthcare Contract invoices (page 2 of the SoD) are based on the monthly contractual amounts payable to each Provider. The financial ledger cannot distinguish between Healthcare Contract invoices and Non Healthcare Contract invoices and so the authorisation threshold is set at such a level to enable the highest value invoice (the Doncaster & Bassetlaw Hospital FT monthly invoice) to be paid. Regarding Non Healthcare invoices (page 1 of the SoD), the authorisation thresholds are largely historic and have been rolled forward from the previous year. The values have been based on historical PCT budgets. The membership of each Group is updated for changes in CCG staff. The SoD is presented to the DCCG managers meeting at regular intervals. CCG authorised signatories must adhere to the Scheme of Delegation and only authorise invoices in financial ledger to the maximum allowed per the Scheme of Delegation, even if the electronic threshold is higher. Summary The SoD has been fully audited in 2013/14 and no recommendations arose relating to the thresholds and thresholds will be reviewed each year in line with both Healthcare and Non Healthcare contract values. Members are asked to note the report.

KPMG LLP Tel: 0113 231 3935 Audit Email: [email protected] 1 The Embankment
Leeds LS1 4DW
KPMG LLP, a UK limited liability partnership, is a subsidiary of KPMG Europe LLP and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative, a Swiss entity.
Registered in England No OC301540 Registered office: 15 Canada Square, London, E14 5GL
Hayley Tingle Chief Finance Officer Doncaster CCG Sovereign House Ten Pound Walk Doncaster DN4 5DJ
14 July 2014
Our ref JP/GL/JIB/LET-966
To the Governing Body members of Doncaster Clinical Commissioning Group
Annual Audit Letter 2013/14 We are pleased to submit our annual audit letter which summarises our 2013/14 audit for Doncaster CCG (“the CCG”). It summarises the key issues arising from our 2013/14 audit at the CCG. Although this letter is addressed to the Governing Body members of the CCG it is also intended to communicate the issues arising from the audit of the CCG to external stakeholders, such as members of the public. It is the responsibility of the CCG to publish this letter on its website.
Scope of our audit
The statutory responsibilities and powers of appointed auditors are set out in the Audit Commission Act 1998. Our main responsibility is to carry out an audit that meets the requirements of the Audit Commission’s Code of Audit Practice (“the Code”). On 5 June 2014 we presented our report under auditing standard ISA 260 to those charged with governance to the Audit Committee which summarised our conclusions from the 2013/14 audit and outlined our auditor responsibilities under statute and the Code. Following the presentation of our ISA 260 report to the Audit Committee we have:
• issued an unqualified opinion on the CCG’s 2013/14 financial statements on 5 June 2014 meeting the Department of Health’s deadline of 6 June;
• concluded that there were no matters arising from our use of resources work that we need to report for the year ending 31 March 2014; and
• issued an unqualified Group Audit Assurance Certificate to the National Audit Office regarding the Whole of Government accounts submission with no exceptions.

ABCD
KPMG LLP Annual Audit Letter 2013/14 14 July 2014
JP/GL/JIB/LET-966 2
Public Interest Reporting
We have a responsibility to consider whether there is a need to issue a public interest report or whether there are any issues which require referral to the Secretary of State. There were no matters in the public interest that we needed to report or refer to the Secretary of State in 2013/14. Key findings The CCG has generally sound processes in place for the production of the accounts and in relation to use of resources. We did raise one low priority recommendation. This is detailed within our ISA260 report to those charged with governance. Fees
Our fee for the 2013/14 external audit was £99,000 excluding VAT. This was in line with the fee agreed at the start of the year with the CCG’s Audit Committee. The Audit Commission made a rebate of £9,000 to the CCG to cover the first year audit costs included within the fee for 2013/14.
Closing remarks
I have discussed and agreed this letter with the Chief Finance Officer of the CCG and confirmed that all Governing Body members of the CCG have received a copy. I would like to thank the finance team, senior officers and the Audit Committee for their support and cooperation throughout the 2013/14 audit. Yours sincerely
John Prentice Director For, and on behalf of, KPMG LLP

Enc D
Chair & Chief Officer Report


Meeting name Governing Body
Meeting date 18th September 2014
Title of paper
Chair and Chief Officer Report
Executive / Clinical Lead(s)
Dr Nick Tupper, Clinical Chair Mr Chris Stainforth, Chief Officer
Author(s) Mrs Jackie Pederson, Chief of Strategy and Delivery
Purpose of Paper - Executive Summary The purpose of this report is to update the Governing Body on issues relating to the activity of NHS Doncaster Clinical Commissioning Group of which the Governing Body needs to be aware, but which do not themselves warrant a full Governing Body paper. This month the paper includes progress on the following areas:
− CQC Review of services for looked after children and safeguarding
− CCG Constitution amendments
− NHS Doncaster CCG Quarter 1 Assurance meeting
− Forward Locality Lead Election Programme
Recommendation(s) The Governing Body is asked to
- Note the report

Impact analysis
Assurance Framework
3.2, 5.1, 6.2
Risk analysis
None
Equality impact
Neutral
Sustainability impact
Nil
Financial implications
Nil
Legal implications
Nil
Consultation / Engagement
N/A

1
1. CQC Review of services for looked after children and safeguarding NHS Doncaster CCG was notified Thursday 4th September 2014 that a Care Quality Commission (CQC) inspection of services for looked after children and safeguarding in Doncaster would commence Monday 8th September 2014. The inspection lasted 5 days and ended with a feedback session to the health and social care community Friday 12th September. The review focussed on the quality of health services for looked after children and the effectiveness of safeguarding arrangements for all children in the area. The review was conducted under section 48 of the Health and Social Care Act 2008 and focussed on evaluating the experiences and outcomes for children, young people and their families who receive health services within the boundaries of Doncaster. The NHS Doncaster CCG Chief Nurse will inform the Governing Body of outcomes from the review once feedback has been formally received from CQC colleagues. 2. CCG Constitution amendments In accordance with published timescales, any amendments to the CCG’s Constitution must be consulted upon and submitted to NHS England by 3rd November 2014. Governing Body Members are asked to highlight any recommended changes for debate by the Governing Body and recommendation to Member Practices. The next opportunity for Constitutional amendments after 3rd November date will be June 2015. 3. NHS Doncaster CCG Quarter 1 Assurance meeting The NHS Doncaster CCG quarter 1 assurance meeting with the Area Team took place on Friday 5th September 2014. Confirmation was given by Area Team colleagues that emphasis will be placed on performance and assurance in the future in addition to the transformation agenda. Concerns were raised by the Area Team in relation to a number of NHS Constitutional standards and national priorities. In particular, a lengthy discussion focussed on non-compliance with the A&E 4 hour wait, diagnostic 6 week wait and Yorkshire Ambulance Service performance targets. Feedback from Area Team colleagues was positive in relation to the improved position on Hospital Standardised Mortality Ratios performance at Doncaster and Bassetlaw Hospitals NHS Foundation Trust. There was further discussion relating to primary care commissioning opportunities and the successes achieved by the CCG in the last 12 months.

2
Formal feedback from Area Team colleagues will be presented to the Governing Body in due course. This will also be made available to the general public via the CCG website. 4. Forward Locality Lead Election Planner The following table details the Locality Lead election planner. Please note that the scheduled September 2014 elections are due to be held in October 2014.
Locality Locality
September 2013 North East Dr Oakford
(Lead A) South West
Dr Harding
(Lead A)
March 2014 Central ---------- North West Dr Pieri
(Lead A)
September 2014 South East Vacancy
(Lead A) North East
Dr Bradley
(Lead B)
March 2015 South West Dr Britten
(Lead B) Central
Dr Feeney
(Lead B)
September 2015 North West Dr Seddon
(Lead B) South East
Dr Barbour
(Lead B)
March 2016 North East Dr Oakford
(Lead A) South West
Dr Wagstaff
(Lead A)
September 2016 Central Dr Kirkman
(Lead A) North West
Dr Pieri
(Lead A)
March 2017 South East Vacancy
(Lead A) North East
Dr Bradley
(Lead B)
September 2017 South West Dr Britten
(Lead B) Central
Dr Feeney
(Lead B)
March 2018 North West Dr Seddon
(Lead B) South East
Dr Barbour
(Lead B)
5. Recommendation The Governing Body is asked to:
- Note the report

Enc E
Receipt of Minutes from Committees


1
Delivery and Performance Committee
Held on Thursday 10 July 2014 Board Room, Sovereign House
Present: Mr Stainforth, Chief Officer (Chair)
Dr Tupper, CCG Chairman Mrs Shepherd, Chief Nurse Mrs Leighton, Head of Performance
In attendance: Mrs Satterthwaite, PA (Minutes) Mrs Wyatt, Deputy Chief Finance Officer (attending on behalf of
Mrs Tingle) Mr Metcalfe, Head of Strategy & Delivery (Item 5) Mr Carpenter, Communications Manager Miss Katie Chester (Observing)
ACTION
1. Apologies
Apologies were received from:
Dr Oakford, North East Locality Lead Dr Barbour, South East Locality Lead Mrs Tingle, Chief Finance Officer Mrs Pederson, Head of Strategy and Delivery
2. Minutes of the last meeting The minutes of the meeting held on Thursday 12 June 2014
were agreed as a true record.
3. Matters Arising not on the Agenda
Delivery & Performance Committee Self-Assessment Dr Tupper stated that certain scores had been altered on the self-assessment form and Mr Stainforth confirmed that he was in agreement with the changes. Choice Framework – Choosing to access required treatment in another European Economic Area country Mr Metcalfe confirmed that this also applies to the unplanned care element and that extra medical insurance will be needed when travelling to these countries. Mr Metcalf is in the process

2
of updating the Choice Framework which will be presented to the Senior Management Team for a decision as to where it will be presented for ‘sign off’ and will liaise with Mr Carpenter to ascertain how this information will be communicated. Unscheduled agenda Item regarding Individual Funding Requests (IFR) Mrs Hudson is in the process of arranging a meeting with DBHFT and the policies have been checked.
Mr Metcalfe
4. Declarations of Interest
There were no Declarations of Interest received.
5. Oncology Business Case
Mr Metcalfe presented the business case.
More patients in Doncaster are being identified with the symptoms of Cancer, patients are accessing treatment earlier and more patients are being treated with curative intent. This also means demand is increasing for treatments such as Radiotherapy and more services being centralised at tertiary centres also means increasing numbers of Doncaster CCG patients are travelling to Sheffield for their treatment. Currently there are 12,500 attendances for Doncaster CCG patients, related to Cancer (Clinical & Medical oncology) outpatient, face to face outpatient attendances in Sheffield per year. Of those 12,500 attendances currently 20% (5100 journeys) which Doncaster CCG patients make for treatment related to Cancer are ‘Eligible’ for Patient Transport Service (PTS) journeys and are funded by the CCG and provided by the Yorkshire Ambulance Service (YAS) PTS contract. Eligible patients are frequently part of a multiple pick up which can result in extended travelling times. Mr Metcalfe informed the Committee of the options as follows:
• Do nothing. If we do nothing patients will continue to access transport via the contracted YAS service. If Radiotherapy services are developed in Doncaster a portion of the journeys to Sheffield will move to Doncaster, although this could be 3 years away
• Invest further with YAS for a period to see if they can deliver a more personalised service. If Radiotherapy services are developed in Doncaster a portion of the journeys to Sheffield will move to Doncaster
• Offer patients a choice through Booking & Screening of YAS PTS, existing taxi contract or Voluntary Community.

3
Doncaster CCG would continue to fund eligible patients only. This option would lead to a more personalised service than group transport with increased choice for patients and could commence immediately. As the current contract is with YAS there may be a potential for challenge and would need to serve notice or treat as a ‘pilot’, incremental in the year and activity and costs taken out in March 2015 as part of the next contracting round
• For patients who need to be in Sheffield at a particular time and need a more personalised car service, choice for patients of current provision plus taxi or Voluntary Community e.g. Fire Fly and Aurora similar to the Bassetlaw model. This model is not restricted to patients who are only eligible therefore there is a risk that Doncaster CCG would end up paying for the majority of journeys not currently funded
• Decommission YAS PTS, procure from an independent contractor and specify they work with Voluntary Community to deliver the contract. This could potentially be time consuming and an expensive use of commissioning time is the service is only viable for 3 years and would require 6-12 month notice to YAS
• Decommission and re-commission all PTS services. This would be time consuming, an expensive use of commissioning time and would require 6-12 month notice to YAS. The risk is high and evidence from Nottinghamshire shows a poor experience
Mr Stainforth stated that historically there have been problems with the PTS. A patient has recently related his own personal experience in one of the Governing Body meetings. Cancer is one of Doncaster CCGs priorities and we would wish to eliminate any difficulties for patients who are experiencing 9-12 weeks of treatment, out-patient and review appointments. Mrs Wyatt informed the Committee that funding had been identified. The Committee discussed and agreed the business case.
Unscheduled Agenda Item regarding Premature Ejaculation (PE)
Dr Tupper informed the Committee that this had been previously discussed in this forum in May 2014 and that a decision had been deferred pending further investigations. A brief synopsis of the paper was given. Dapoxetine is a controlled drug and is the first oral treatment for PE to be licensed in the UK and could potentially be used as a leisure drug similar to Viagra. There are 3 potential options as follows:

4
• It stays within Primary Care
• All referrals for PE go to the Leger Clinic for assessment of need and prescribing
• All referrals for PE go to the Leger Clinic for assessment of need and prescribing is done in Primary Care
This has been discussed by the Area Prescribing Committee and the Medicines Management Group which recommended Option 3 as this would give the CCG some control over numbers without making the pathway too onerous and suggested a dosage of between 4-6 tablets/ month. There is also the Psycho/Social aspect to consider. The Committee agreed Option 3 and to review again in 18 months through the Area Prescribing Committee. The Medicines Management Committee will closely monitor prescribing levels.
6. Any Other Business
There was no other business discussed.
7. Date and Time of Next Meeting
Thursday 14 August 2014 at 12.30pm, Dr Nick Tupper’s Office, Sovereign House.