a safer future for emily: queensland incidents in transfusion (qiit ... · queensland incidents in...
TRANSCRIPT
Queensland incidents in Transfusion (QiiT) June 2007–2009 Report
A Safer FutureforEmily
QiiTQueensland incidents in Transfusion

Queensland incidents in Transfusion (QiiT) June 2007–2009 report
A Safer FutureforEmily
QiiTQueensland incidents in Transfusion
http://creativecommons.org/licenses/by-nd/2.5/au/
© State of Queensland (Queensland Health) 2012
ISBN: 978-1-921707-81-0
For permissions beyond the scope of this licence contact: Intellectual Property Officer, email [email protected], phone (07) 3234 1479. For further information contact Qld Blood Management Program at [email protected] or 3131 6534.
Design: Biotext, Canberra.
Cover image: Emily receiving a blood transfusion. Photographer: Lyle Radford

iiiQueensland incidents in Transfusion (QiiT) June 2007–2009 report
ForewordWelcome to the June 2007–2009 report of the Queensland incidents in Transfusion (QiiT) haemovigilance system. It is with great pleasure that I present this much-anticipated first report, which is the first step in deepening our understanding of transfusion-associated risks and guiding improvements in transfusion practice within Queensland.
This report, which carries the title A Safer Future for Emily, captures the story of Emily, a regular recipient of blood transfusions. Her story highlights the importance of safe blood transfusions and the experience of the many Queenslanders who receive blood transfusions annually. My sincere thanks to Emily and her family for their invaluable contribution to this report.
The contribution of the 107 Queensland public and private healthcare facilities that are currently participating in QiiT should also be recognised. Clinical staff at these facilities are to be commended for their role in providing QiiT with vital, event-related reporting.
This report provides insight into the types of transfusion-related adverse events in Queensland healthcare facilities between June 2007 and December 2009. Our reporting of these events gives us an opportunity to look further into the factors and conditions that contribute to transfusion adverse events across the state. The report tables some valuable recommendations that may guide improvements in transfusion practice and, indeed, ensure the continued improvement of patient outcomes.
I hope the publication of this report will not only encourage further participation in QiiT, but also build on and extend the culture of patient safety already present in Queensland healthcare facilities through guided improvements in transfusion practice.
Dr Jeannette Young
Chief Health Officer Chair of Queensland Blood Advisory Council

vQueensland incidents in Transfusion (QiiT) June 2007–2009 report
Contents
Foreword ............................................................................................................................... iii
Acknowledgments .................................................................................................................vii
Emily needs safe blood .............................................................................................................1
1. Executive summary and main recommendations ................................................................. 5Main recommendations ..................................................................................................... 6Current work ..................................................................................................................... 8
2. Introduction.....................................................................................................................10
3. System governance .......................................................................................................... 11
4. System outline ................................................................................................................. 12
5. Overview of participation .................................................................................................. 13
6. Summary of events reported ............................................................................................ 15Validated events ..............................................................................................................16Patient demographics ...................................................................................................... 17Blood component ............................................................................................................18Severity and imputability ..................................................................................................18Primary contributory factors and primary site ..................................................................... 19Medical officer review ...................................................................................................... 20
7. Transfusion-transmitted infection ..................................................................................... 21Discussion ...................................................................................................................... 21Summary ........................................................................................................................ 22Practice guidelines ...........................................................................................................23
8. Incorrect blood component transfused ............................................................................. 24Discussion ...................................................................................................................... 24Summary ........................................................................................................................ 26Practice guidelines ...........................................................................................................27
9. ABO haemolytic transfusion reaction ................................................................................ 28Discussion ...................................................................................................................... 28Summary ........................................................................................................................ 29Practice guidelines .......................................................................................................... 29
10. Acute non-ABO haemolytic transfusion reaction and delayed haemolytic transfusion reaction .....30Discussion ...................................................................................................................... 30Summary ......................................................................................................................... 31Practice guidelines ........................................................................................................... 31
11. Febrile non-haemolytic transfusion reactions .....................................................................32Discussion .......................................................................................................................32Summary .........................................................................................................................33Practice guidelines ...........................................................................................................33
vi A Safer Future for Emily
12. Severe allergic reactions and anaphylaxis ......................................................................... 34Discussion ...................................................................................................................... 34Summary ........................................................................................................................ 34Practice guidelines ...........................................................................................................35
13. Acute respiratory reactions ............................................................................................. 36Discussion ...................................................................................................................... 36Summary ........................................................................................................................ 36Practice guidelines ...........................................................................................................37
Appendix A Data set/definitions of transfusion adverse events .............................................. 38
Appendix B QiiT transfusion reaction chart ........................................................................... 40
Appendix C TRALI – information for medical officers ...............................................................41
Appendix D QiiT process (extract from pilot project) ...............................................................45
Appendix E RRMA classification .......................................................................................... 46
Appendix F Imputability and severity scores ........................................................................ 47
Appendix G Blood Products Advisory Committee information developed for IMP notifications .... 48
Abbreviations ....................................................................................................................... 50
References ............................................................................................................................ 51
viiQueensland incidents in Transfusion (QiiT) June 2007–2009 report
Acknowledgments The Queensland Blood Management Program (QBMP) would like to acknowledge the contribution of the following committees, groups, agencies, departments and individuals to the QiiT haemovigilance system and the development of this report:
• haemovigilance coordinators at participating public and private healthcare facilities
• clinical staff at participating public and private healthcare facilities who have reported events and supported the haemovigilance coordinators in the completion of the QiiT follow-up forms
• Haemovigilance Committee members
Dr Bronwyn Williams Royal College of Pathologists of Australasia representative (Co-Chair)
Dr Ann Gillett The Royal Australasian College of Physicians representative
Dr Anne Haughton Australian Association of Pathology Practices representative
Dr Brian Bell Directors of Medical Services Advisory Committee representative
Dr Lance Le Ray Directors of Medical Services Advisory Committee representative
Ms Di Slater Private Hospitals Association of Queensland representative
Ms Glynda Summers Office of the Chief Nursing Officer representative
Dr John Rowell Pathology Queensland representative
Dr John Wakefield Queensland Health Patient Safety and Quality Improvement Service representative
Dr Stewart Bryant Australian Red Cross Blood Service representative
Dr Michael Fanshawe Royal Australasian College of Obstetricians and Gynaecologists representative
Dr Janet Draper Royal Australasian College of Obstetricians and Gynaecologists representative
Ms Wendy Haynes Royal College of Nursing, Australia representative
Prof Michael Humphrey Queensland Health Service District representative
Dr Judy Graves Queensland Health Service District representative
Dr David Slaughter Queensland Health Service District representative
Dr Robert Bird Queensland Health Service District representative and former Chair
Dr Gina Clare Queensland Blood Management Program, Queensland Health
Dr Simon Brown Queensland Blood Management Program, Queensland Health (Co-Chair)
viii A Safer Future for Emily
• QiiT Working Group members
Ms Natasha Kearey Ms Roxina Sharma Ms Anita Booker
Ms Magda Gouws Dr Michelle Bryson Ms Carey Gadischkie
Ms Lynelle Foster Ms Sue Williams Ms Anne Bubbers
Mr Leigh Broad Ms Leanne Hollis Ms Christine Long
Dr Luke Soo Ms Kathy Toumpas Dr Peter Mollee
Ms Rebecca Farrell Ms Cheryl Kann Mr David Stone
Ms Janelle Toombes
• agencies, committees, departments and programs
– Pathology Queensland
– Queensland Medical Laboratories (QML)
– Sullivan Nicolaides Pathology (SNP)
– The Australian Red Cross Blood Service (ARCBS)
– Queensland Health Patient Safety and Quality Improvement Service
• Ms Patricia Pennicott, Integrated Communications, Queensland Health
• Ms Prue Law and Ms Nicole Stephensen, Queensland Health Legal Unit
• Mr Neil Gardiner, Health Statistics Centre, Queensland Health
This report was prepared on behalf of the QBMP, Haemovigilance Committee and QiiT Working Group by
• Dr Simon Brown
• Ms Dal Johal
• Ms Natalie Winter.

1Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Emily needs safe bloodEmily looks at home in the busy and confronting hospital ward, unlike many of the children around her.
Every month for the past 12-and-a-half years, Emily has come to the Royal Children’s Hospital for a blood transfusion.
When she was about three months old, Emily’s parents, Vernon and Tina, sought medical advice because Emily wouldn’t eat. She was diagnosed with thalassaemia.
Thalassaemia is an inherited blood disorder where the body cannot make enough of the globin chains that make up haemoglobin, the protein in red blood cells that carries oxygen. Thalassaemia causes ineffective production of red blood cells.
If untreated, severe thalassaemia can lead to life-threatening anaemia, an enlarged spleen, bone deformities and heart failure.
On a cool, sunny May morning, Emily sits cross-legged on the hospital bed giggling like a typical schoolgirl. This healthy-looking, playful young teenager in denim shorts and T-shirt, with her dark hair loosely pulled back, laughs with her dad about a cheeky little duck on YouTube.
As a Year 8 student, Emily is a typically active 13-year-old who loves netball, hip hop dancing and cheerleading when back home.
Her face lights up as she tells her dad about what her school friends will be up to today. But while her mates are in class, on the netball field, or chatting and giggling on their way home on the bus, Emily will be attached to her intravenous ‘lifeline’ as three to four bags of blood are pumped into her young body over about eight hours.
Thalassaemia is usually treated with regular blood transfusions and folate supplements. But while transfusions can lengthen the patient’s lifespan, they will not cure the disorder.
‘I don’t get tired of having to go through the transfusions. The nurses and doctors are really lovely and it doesn’t hurt at all,’ Emily says.
‘It’s just like staying home for the day and relaxing. I sometimes do my homework, watch TV, play games, or have a little sleep. It’s very comforting and just like a second home to me now.’
Emily receives regular blood transfusions at the Royal Children's Hospital
Photographer: Lyle Radford

2 A Safer Future for Emily
Thalassaemia occurs when there is a defect in a gene that helps control production of one of haemoglobin’s proteins — alpha globin or beta globin. Hence, there are two types of thalassaemia — alpha thalassaemia and beta thalassaemia.
Alpha thalassaemia occurs most commonly in people from Southeast Asia, the Middle East, China and those of African descent. Beta thalassaemia occurs in people of Mediterranean origin, North and West Africa, India and South-East Asia, including Pacific Island populations.
Emily has beta thalassaemia major, which means she inherited one abnormal beta globin gene from each of her parents, who unknowingly were both carriers of the disorder.
Bone marrow transplant — the only definitive cure for thalassaemia — has been used worldwide for about 20 years. But it has risks, depending on availability of a compatible family donor and age and health of the recipient. It also carries very high chances of permanent infertility.
Emily has no siblings and no compatible family donor for bone marrow. The chances of finding a suitable unrelated donor are not very high. Unrelated transplant is also significantly more risky and more expensive.
Emily's dad, Vernon, has been accompanying her every month for more than 12 years
Photographer: Lyle Radford

3Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Emily’s strongest support network — her parents — are well acquainted with what their daughter goes through every month. After more than 12 years of accompanying her to her monthly transfusions and monitoring her ongoing treatment, these very loving parents quite rightly believe they are reasonable experts on what is required and how it should be done.
‘One time after a transfusion Emily got a very high fever, above 40 degrees,’ says Vernon. ‘We had to bring her back to hospital, but the staff insisted it was swine flu. We knew it wasn’t swine flu. We knew it was an infection from the blood transfusion.
‘Getting the quantity of blood right is also important,’ he says. ‘So is the stability of staff. It’s good to have the same people doing the transfusions for Emily.
‘If the nurses or doctors have not done Emily’s transfusions before, I won’t leave her alone at all. It’s important for her to have the same staff who know how to do it.’
Emily pipes in: ‘The worst part is when I have a doctor or nurse who hasn’t been before and they can’t get the needle into my vein.
‘But the best part is that everyone is really nice. It’s a good environment. And it’s easy. If it was hard, I wouldn’t want to come.
‘The transfusions give me more stamina and keep me healthy. And it means I don’t have to have a bone marrow transplant. I prefer the transfusions over the risk of a bone marrow transplant. This is much better for me. And the doctors and nurses are really trustworthy.’
Then with another giggle: ‘But it would be good if they changed the TV programs, instead of repeating the same ones, or the same segments, again and again. I can’t stand watching that talking parrot anymore.’
When she was very young, Emily’s transfusions were done through a port-a-cath surgically inserted under the skin on her chest with a tube connected to a large vein. But when she was old enough, she decided to have the transfusions through an external IV line inserted in her hand, so the port was removed.
‘Emily makes the decisions herself,’ says Vernon. ‘She is the one who goes through it, so she has to feel comfortable.
‘It’s not right for Tina and me to decide on bone marrow. It is up to Emily. But if she hated the transfusions, then obviously we would advise her to look at other options.’
While multiple blood transfusions help control thalassaemia symptoms, they also result in iron overload. If not removed, the excess iron will slowly harm the body’s organs and can result in severe morbidity, such as cardiac disease, diabetes, failure of sexual development, osteoporosis or liver damage, as well as early mortality.
Chelation therapy removes the excess iron and is an integral part of thalassaemia treatment. But it was one of the hardest aspects for Emily in the past.
Her chelation was initially done by desferrioxamine infusion with a thin needle for 8 to 12 hours, five nights a week, using noisy pumps. The needle insertion site can often become painful, with bumps, rashes, bruises and infections occurring.
About two years ago, Emily started on oral iron chelator drugs instead and now finds chelation much easier.
Vernon downplays the impact of Emily’s medical condition on the close-knit family.
‘There is no impact. Apart from the fact that I have to put up with her music on the way to the hospital,’ he laughs.

4 A Safer Future for Emily
‘Seriously, it’s just the way it is. Obviously, we would prefer she didn’t have it, but it has no impact on the family and it doesn’t affect her school work either.’
Emily only recently told her close friends about her thalassaemia and regular blood transfusions.
‘If I get tired at school, I just don’t show it. I just show it at home. I have always kept it a secret. But my friends have been really good. They don’t tease me.’
The family is acutely aware that Emily’s numerous and regular blood transfusions significantly expose her to the risk of adverse reactions or incidents. They rely on the hospital and staff to ensure she receives safe blood and that she stays safe with every transfusion.
According to Medical Officer Simon Brown at the Royal Children’s Hospital’s Haematology and Oncology Department, Australia has one of the safest blood supplies in the world.
‘But voluntary reporting of any haemovigilance incidents across both public and private hospitals can improve the safety of blood transfusions by detecting and detailing the unexpected effects of transfusion.’
A significant proportion of incidents are often unavoidable adverse reactions to fresh blood and blood components, such as allergic reactions and febrile non-haemolytic transfusion reactions (fever).
Other incidents can include bacterial infections, incorrect blood components, inappropriate specification or unnecessary transfusion, haemolytic reactions, transfusion-associated acute lung injuries or graft-versus-host disease and post-transfusion purpura (when the body produces alloantibodies to the introduced platelets).
‘Queensland Health promotes an excellent culture of learning,’ says Simon.
‘Haemovigilance encourages this learning culture where we can learn from what has happened and constantly improve patient care. Through haemovigilance, Queensland Health is taking a leading role in improving patient care in both public and private hospitals.’
Emily’s future depends on it.
5Queensland incidents in Transfusion (QiiT) June 2007–2009 report
1. Executive summary and main recommendations
The implementation of QiiT commenced in the last quarter of 2008. By 31 December 2009, all 15 health service districts in Queensland Health, 107 public and private healthcare facilities and the state’s main pathology providers had agreed to participate in the program.
The role of QiiT is to capture events relating to the administration of fresh blood and blood components in clinical areas and to contribute data to the National Haemovigilance System administered by the National Blood Authority. The information collected by QiiT complements the safety data already collated by the Australian Red Cross Blood Service (ARCBS).
The 230 events reviewed for this report include those reported to QiiT from the start of the pilot project on 1 June 2007 to 31 December 2009. Staff from the Queensland Blood Management Program (QBMP) and the QiiT Working Group have undertaken an analysis and review of these events.
The aim of this review was to validate the events and to allow for recommendations by the QiiT Working Group and the Haemovigilance Committee. The recommendations aim to delineate areas for improvement in transfusion practice and avenues by which these improvements may be addressed in Queensland healthcare facilities.
The review validated 129 of the 230 events reported to QiiT. The summary data for these events is detailed in Chapter 6. The review of the individual categories of events that make up the QiiT data set (Appendix A) are described in detail in Chapters 7–13. The recommendations formulated from the 129 validated events have been divided into the main recommendations and practice recommendations at the end of each specific category chapter.
The current rate of reporting to QiiT is encouraging and compares favourably with reporting rates for the UK haemovigilance scheme, Serious Hazards of Transfusion (SHOT), which has been in operation since 1996. The readiness of facilities to participate and report to QiiT reflects the culture of safety that underpins Queensland’s healthcare systems. This culture reflects the considerable work invested in patient safety by both private and public healthcare providers, in particular the work of the Patient Safety and Quality Improvement Service and patient safety officers in Queensland Health.
Of the validated QiiT events, a significant proportion can be attributed to unavoidable adverse reactions to fresh blood and blood components, such as allergic reactions and febrile non-haemolytic transfusion reactions. The ARCBS, together with all Australian governments, continues to invest in initiatives to minimise the known risks of administering fresh blood and blood components, including universal leucodepletion and the bacterial screening of platelets. Despite this investment, it is imperative that clinical staff appreciate that the avoidance of inappropriate transfusions is equally important in reducing unnecessary adverse events related to blood transfusions.
A survey of the pilot sites during the QiiT pilot project revealed that 11 per cent of the 289 clinical staff surveyed had witnessed a transfusion reaction in the preceding month. While the majority of these transfusion reactions are minor, the overlap in symptoms and signs between both minor and life-threatening transfusion reactions mean that clinical staff need to be able to formulate correct management plans to ensure potentially life-threatening events are not missed; for example, ABO haemolytic transfusion reaction, transfusion-transmitted bacterial sepsis or transfusion-related acute lung injury.
6 A Safer Future for Emily
The events reported to QiiT have shown a marked variation in the management and investigation of transfusion reactions, which has led the Haemovigilance Committee to recommend that further work be undertaken to address inconsistencies in this area.
Finally, it is salient to note that incidents continue to be reported of patients receiving fresh blood and blood components intended for other patients (detailed in Chapter 8 ‘Incorrect blood component transfused’ and Chapter 9 ‘ABO haemolytic transfusion reactions’). This scenario can, in the worst case, result in an ABO haemolytic transfusion reaction and even death.
Evidence from international haemovigilance systems clearly shows that human error is a major factor in both events of incorrect blood component transfused and ABO haemolytic transfusion reactions. On current evidence, the data from QiiT seems to reflect the experience of other haemovigilance systems and suggests that ABO haemolytic transfusion reactions will continue to be reported. This was reinforced by the findings of an audit of the administration of red cell transfusions in Queensland healthcare facilities.1
The UK and French haemovigilance systems estimate that both incorrect blood component transfused and ABO haemolytic transfusion reactions will be fatal in between one in 1.5 million and one in 1.8 million red cell transfusions.2, 3 This means the administration of blood is a comparatively safe procedure, with respect to safety in health care, and is equivalent to the risks of receiving an anaesthetic.4 A challenge for such safe procedures is to ensure healthcare professionals remain diligent to the potential risks, and this forms a significant rationale for haemovigilance systems.
Despite the relative safety of blood transfusions, haemovigilance systems appear to be able to reduce the frequency of transfusion-related fatalities. The SHOT report for 2008 revealed that fatalities related to transfusion have continued to fall after the introduction of the UK haemovigilance system.
These safety improvements are only achievable by the dissemination of reports such as this to all staff involved in the transfusion chain, as well as health service managers. Queensland Health has a commitment to the sharing of information relating to adverse events. Therefore, this report is primarily written for clinical staff employed by private and public healthcare providers in Queensland. However, it is also of value to the wider community, especially those with an interest in the safe delivery of transfusions.
With this in mind, it is important that the health system continues to learn from the experience of countries where haemovigilance has a long pedigree, and that clinical staff realise the importance of adhering to the national guidelines for the administration of blood and blood products, as published by the ANZSBT/RNCA in 2004.5
Main recommendations
The following recommendations have been grouped to reflect the level of the healthcare system best positioned to implement these recommendations.
Clinical staff
1. Clinical staff must ensure that all documentation during the transfusion process is clear and adequate. This includes the correct labelling of blood samples and request forms, prescription of blood and blood components, collection and administration of blood and blood products and patient observations during transfusions. This is essential for ensuring that the correct patient receives the correct blood component and that the blood component, from donor to recipient, is traceable.
2. Clinical staff should consider undertaking the BloodSafe e-Learning Australia program.

7Queensland incidents in Transfusion (QiiT) June 2007–2009 report
3. Clinical staff should read and adhere to the national guidelines on collection and administration of blood and guidelines on the appropriate use of blood and blood components.
4. Clinical staff should ensure that elective transfusions are not performed out of hours unless clinically indicated and in accordance with guidelines on appropriate use of blood components.
Healthcare providers
1. Healthcare providers should consider the provision of local governance structures for transfusion medicine at their facilities (for example, hospital transfusion committees, hospital transfusion teams and a lead clinician for transfusion services).
2. All healthcare facilities and pathology service providers in Queensland should actively participate in the Queensland haemovigilance system.
Tertiary educational institutions and medical colleges
1. Universities and colleges should consider reviewing transfusion practice content in nursing undergraduate courses, specifically about the administration of blood and blood components, correct patient identification and bedside checks, and the accurate and complete documentation of transfusion episodes.
2. Medical colleges and schools should consider reviewing undergraduate and postgraduate course content about the management of transfusion reactions and correct patient identification.
Queensland Health
1. Queensland Health should develop a set of standardised clinical guidelines/pathways for the management of transfusion reactions.
2. Queensland Health should encourage all public and private healthcare facilities and pathology service providers to participate in the Queensland haemovigilance system.
3. Queensland Health should promote the development of appropriate local governance structures for transfusion medicine in public and private healthcare facilities (for example, hospital transfusion committees, hospital transfusion teams and a lead clinician for transfusion services). This will promote the local ownership of transfusion practice through auditing, training, incident review and blood management programs.
4. As part of an overall e-health implementation strategy, Queensland Health should investigate solutions that support the ordering of blood and blood components by clinical staff, and the traceability of blood and blood components, and minimise patient identification errors.
National
1. The National e-Learning Transfusion Advisory Committee should consider the development of a module on the management of transfusion reactions for the BloodSafe e-Learning Australia program.
2. The jurisdictional blood committee should review the need for legislation equivalent to the European Union Blood Directive,6 particularly in relation to Article 14, which relates to the traceability of blood and blood components from the donor to the recipient and vice versa.

8 A Safer Future for Emily
Current work
The process of implementing Queensland’s haemovigilance system, together with the continual review of events submitted to QiiT, have resulted in the identification of several key issues about transfusion practice in Queensland. A considerable body of work has already started to address these issues. This work is outlined below.
a) Documentation and traceability of products
The analysis of QiiT events has identified events where the final fate of the blood component was not recorded in the hospital chart. This means that the blood component cannot be traced categorically to a patient. This issue of traceability is not new, indeed traceability is one of the articles of the European Blood Directive (Article 14 — 2002/98/EC).6 This requires hospital blood banks by law to ‘ensure that blood and blood products … can be traced from donor to recipient and vice versa’. In response to the passing of the European Blood Directive as law in 2005, many National Health Service (NHS) blood banks have invested in technology for the electronic recording of the final fate of blood products — when they are hung and connected to a patient. The Queensland Blood Management Program has facilitated the sharing of relevant information with stakeholders, including the Queensland Blood Advisory Council, Laboratory Information Systems and Solutions, and Clinical and Statewide Services Division.
b) Irradiated blood components
Multiple events of patients receiving non-irradiated blood and blood components, when they are at risk of developing the potentially fatal complication of transfusion-associated graft-versus-host disease, have been reported to QiiT. These events highlight communication problems with the inadequate completion of blood request forms and the transfer of data electronically between blood banks. Discussion of this issue by the Haemovigilance Committee has led to the development of a patient leaflet, card and cognitive aid to empower the patient as an additional advocate for the correct prescription and request of blood and blood components they require.
c) Management of transfusion reactions
Significant variability in the management of transfusion reactions has been identified from events submitted to QiiT. Work in this area includes:
• development of the QiiT transfusion reaction chart (Appendix B)
• distribution of information for medical staff on transfusion-related acute lung injury (Appendix C)
• a request to the national steering group for the BloodSafe e-Learning Australia program to develop a module on the management of transfusion reactions
• commencement of work by the Blood Products Advisory Committee to develop guidelines on transfusion reactions
• surveys of medical schools and junior doctors to inform development and implementation guidelines.
d) Patient identification issues
The Queensland Blood Management Program has worked in conjunction with the Patient Safety and Quality Improvement Service and other key stakeholders to prepare an options paper on patient identification issues. This area continues to be important in blood transfusion, as evidenced by the number of ‘wrong blood in tube’ near-miss events, events of incorrect blood component transfused, ABO haemolytic transfusion reactions as detailed in the previous report — Audit of the collection and administration of blood and blood products (October 2007).1 The
9Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Queensland Blood Management Program has been facilitating the sharing of information about potential IT systems to address patient identification issues and other areas of blood transfusion practice (see (a) above).
e) Appropriate use of blood and blood components
Several side-effects of blood and blood components, such as allergic reactions and febrile non-haemolytic transfusion reactions, are a feature of giving a biological product. However, it is known from national and international studies that the rate of inappropriate transfusion of blood and blood components is 10–50 per cent.7-11 The reduction of inappropriate transfusions offers an opportunity for quality improvement for patients by reducing their exposure to the known risks of blood transfusions. The Queensland Blood Management Program is currently developing strategies to support more effective blood use.
f) Training
In addition to multiple visits by Queensland Blood Management Program team to healthcare facilities during the rollout of QiiT, the team has also delivered several educational talks to healthcare professionals and presentations at scientific meetings. The Queensland Blood Management Program sponsored the BloodSafe e-Learning Australia package on the Queensland Health Electronic Publishing Service (QHEPS) and has promoted this transfusion training package across the state. There has been significant use of this resource, with 9209 clinical staff having completed the package in Queensland. Individual health service districts and healthcare facilities are commended for implementation of this resource as a training tool for staff.
g) Governance
The implementation of adequate governance structures at the hospital level must underpin any effort to improve transfusion safety (for example, hospital transfusion committees (HTCs) or their equivalent). The importance of these governance structures is highlighted in the UK by the Department of Health circular, Better Blood Transfusion: Safe and Appropriate Use of Blood (HSC 2007/001). The initiatives detailed in this circular have led to a steady increase in healthcare facilities implementing HTCs and transfusion teams. This has occurred at a time of decreasing red cell use and transfusion-related fatalities.12 Similar improvements in the local governance of transfusion practice have been evident since the introduction of the mandatory criteria 1.5.5 (relating to blood and blood components) in Evaluation and Quality Improvement Program (EQuIP) 4 by the Australian Council on Healthcare Standards. The Queensland Blood Management Program is now working in conjunction with the Blood Products Advisory Committee to develop appropriate terms of reference, key performance indicators and benchmarking indicators for use by HTCs.
h) Communication
Communication of data back to clinical and laboratory staff is key to the success of any haemovigilance system. In recognition of this, the Queensland Blood Management Program has:
• released quarterly QiiT newsletters
• undertaken a survey of haemovigilance coordinators across the state to gauge the performance of the system and the QiiT team
• developed a Queensland Health forum site for Queensland Health staff on QHEPS
• provided a biannual audit report to participating healthcare facilities
• submitted key performance indicators for the QiiT system to the Queensland Blood Advisory Council.

10 A Safer Future for Emily
2. IntroductionThe Queensland Government, as a cosignatory of the National Blood Agreement, has a responsibility ‘to promote safe, high-quality management and use of blood products, blood-related products and blood-related services…’ In order to meet these and other obligations contained in the agreement, Queensland Health established the Queensland Blood Management Program, within Clinical and Statewide Services (CaSS).
The Queensland Blood Management Program, in meeting its obligations, identified the need to support the clinical governance framework for transfusion practice within Queensland. It proposed the development of a statewide haemovigilance system, which has been defined as ‘the detection, gathering and analysis of information regarding untoward and unexpected effects of blood transfusion’ (Guide on Preparation, Use and Quality Assurance of Blood Components, Recommendation No. R (95)15, 9th ed. 2003). This proposal was supported by public and private health service providers, the ARCBS and pathology providers. A pilot system, modelled on international haemovigilance systems, was trialled during 2007 with positive results.13 This system was later endorsed by the Queensland Health Executive Management Team and the rollout of the system to Queensland’s public and private healthcare facilities began. The system was aptly titled ‘Queensland incidents in Transfusion’ (QiiT).
The QiiT haemovigilance system, together with other Australian states and territories, contributes data to the National Haemovigilance System, as established by the National Blood Authority. The objectives of this national haemovigilance system are to ‘provide documented evidence for improvement of practice, to know what the real risks/hazards of transfusion are in a given community/country, to disseminate the findings and to take appropriate action as well as instigate appropriate education processes to prevent their recurrence’.14 Queensland’s contribution of data to the national system, together with the development of this report and associated recommendations, provide an opportunity to look further into the factors and conditions that contribute to transfusion adverse events.
11Queensland incidents in Transfusion (QiiT) June 2007–2009 report
3. System governanceThe Queensland Blood Advisory Council is an advisory committee which supports the role of the Queensland Blood Management Program. The Queensland Blood Board is chaired by Queensland’s Chief Health Officer and its membership includes representatives from both the public and private healthcare sectors.
The Haemovigilance Committee, a sub-committee of the Queensland Blood Advisory Council, is the governing body for the QiiT system. Membership to this committee is voluntary and currently includes a range of blood sector stakeholders. The work of the Haemovigilance Committee is centred on the provision of high-level strategic direction for the development and maintenance of QiiT. The committee provides policy advice to the Queensland Blood Advisory Council on QiiT, as well as the production and dissemination of information to stakeholders on the operation and findings of QiiT, with the support of the QiiT Working Group.
The QiiT Working Group is a sub-committee of the Haemovigilance Committee and is responsible for the further analysis and review of certain events reported to QiiT, as well as appropriate recommendations on events. Membership of the QiiT Working Group is also voluntary and consists of nursing, pathology, medical and patient safety representatives employed in both the public and private healthcare sectors.

12 A Safer Future for Emily
4. System outlineThe QiiT haemovigilance system collects de-identified data on incidents with the transfusion of fresh blood and blood components (for example, red cell, fresh frozen plasma, cryoprecipitate and platelets) in clinical areas. The ARCBS collects data on adverse events within the blood collection service, therefore this does not form part of the data set collected for QiiT.
QiiT has adopted several strategies to minimise the impact of reporting transfusion-related adverse events on the workload of clinical staff, including:
1. using existing incident reporting systems (for example, PRIME in public healthcare facilities), thus avoiding duplicate reporting
2. limiting the QiiT data set — the type of events reported
3. developing follow-up forms that collect data for the validation and analysis of events, and help clinical staff in the local analysis of events.
The QiiT process is outlined in Appendix D.

13Queensland incidents in Transfusion (QiiT) June 2007–2009 report
5. Overview of participationAs of 31 December 2009, all of Queensland’s health service districts, as well as 75 public healthcare facilities and 32 private healthcare facilities, had agreed to participate in QiiT. Participation in QiiT is voluntary, and nine healthcare facilities have declined participation.
Estimates at this time suggested 36 public and 9 private healthcare facilities that perform blood transfusions were yet to be contacted or yet to agree to participate in the system (Table 1). This estimate represents 30 per cent of all QiiT eligible healthcare facilities.
Table 1 Participation of healthcare facilities in the QiiT haemovigilance system
Eligible to participate Participating Not yet participating Percentage remaining
Public 111 75 36 32%
Private 41 32 9 22%
Overall 152 107 45 30%
The Rural, Remote and Metropolitan Areas system is a classification system that describes the areas of medical practice within Australia (Appendix E). The system divides the rural, remote and metropolitan areas, according to city status, population, rurality and remoteness. The spread of the 107 healthcare facilities currently participating in QiiT is charted in Figure 1.
Figure 1 Distribution of participating healthcare facilities according to Rural, Remote and Metropolitan Areas (RRMA) classification
RRMA 515%
RRMA 410%
RRMA 324%
RRMA 225%
RRMA 126%

14 A Safer Future for Emily
A computer monitor and blood treatment equipment in a hospital pathology lab
Photographer: Michael Marston
15Queensland incidents in Transfusion (QiiT) June 2007–2009 report
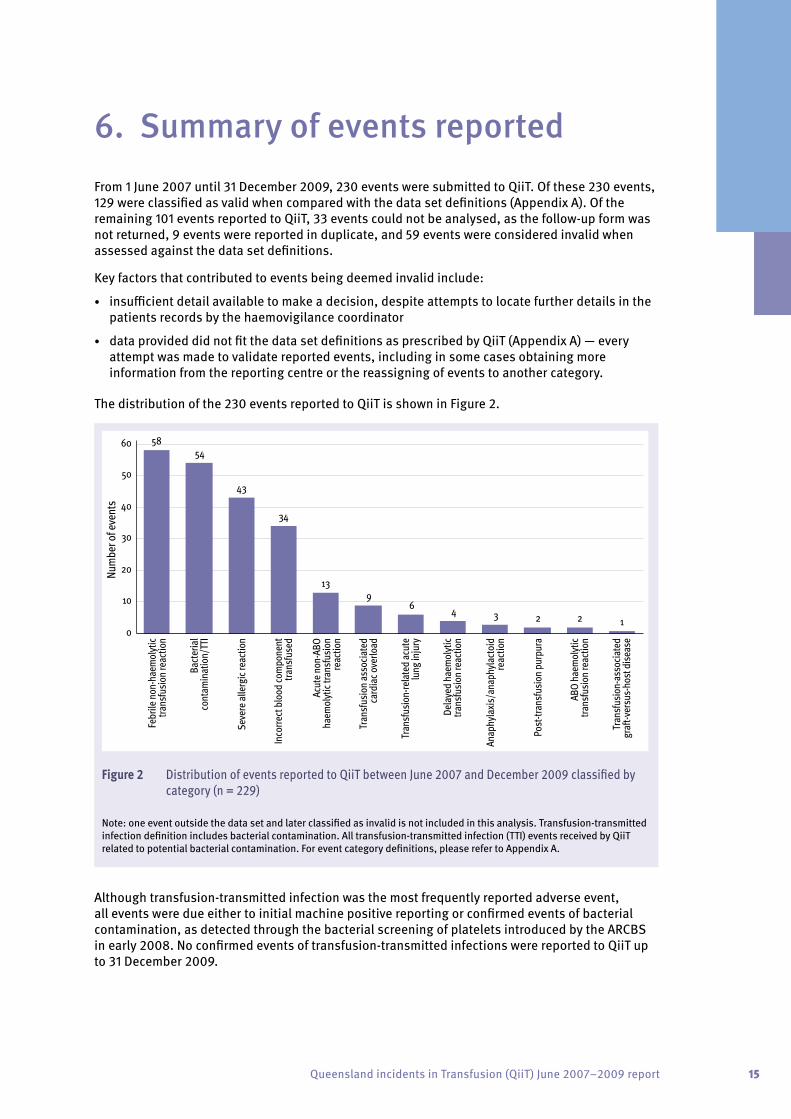
6. Summary of events reported From 1 June 2007 until 31 December 2009, 230 events were submitted to QiiT. Of these 230 events, 129 were classified as valid when compared with the data set definitions (Appendix A). Of the remaining 101 events reported to QiiT, 33 events could not be analysed, as the follow-up form was not returned, 9 events were reported in duplicate, and 59 events were considered invalid when assessed against the data set definitions.
Key factors that contributed to events being deemed invalid include:
• insufficient detail available to make a decision, despite attempts to locate further details in the patients records by the haemovigilance coordinator
• data provided did not fit the data set definitions as prescribed by QiiT (Appendix A) — every attempt was made to validate reported events, including in some cases obtaining more information from the reporting centre or the reassigning of events to another category.
The distribution of the 230 events reported to QiiT is shown in Figure 2.
5854
43
34
139
6 4 3 2 2 10
10
20
30
40
50
60
Febr
ile n
on-h
aem
olyt
ictra
nsfu
sion
reac
tion
Bact
eria
lco
ntam
inat
ion/
TTI
Seve
re a
llerg
ic re
actio
n
Inco
rrect
blo
od co
mpo
nent
trans
fuse
d
Acut
e no
n-AB
Oha
emol
ytic
trans
fusi
onre
actio
n
Tran
sfus
ion
asso
ciate
dca
rdia
c ove
rload
Tran
sfus
ion-
rela
ted
acut
elu
ng in
jury
Dela
yed
haem
olyt
ictra
nsfu
sion
reac
tion
Anap
hyla
xis/
anap
hyla
ctoi
dre
actio
n
Post
-tran
sfus
ion
purp
ura
ABO
haem
olyt
ictra
nsfu
sion
reac
tion
Tran
sfus
ion-
asso
ciate
dgr
a�-v
ersu
s-ho
st d
isea
se
Num
ber o
f eve
nts
Figure 2 Distribution of events reported to QiiT between June 2007 and December 2009 classified by category (n = 229)
Note: one event outside the data set and later classified as invalid is not included in this analysis. Transfusion-transmitted infection definition includes bacterial contamination. All transfusion-transmitted infection (TTI) events received by QiiT related to potential bacterial contamination. For event category definitions, please refer to Appendix A.
Although transfusion-transmitted infection was the most frequently reported adverse event, all events were due either to initial machine positive reporting or confirmed events of bacterial contamination, as detected through the bacterial screening of platelets introduced by the ARCBS in early 2008. No confirmed events of transfusion-transmitted infections were reported to QiiT up to 31 December 2009.
16 A Safer Future for Emily
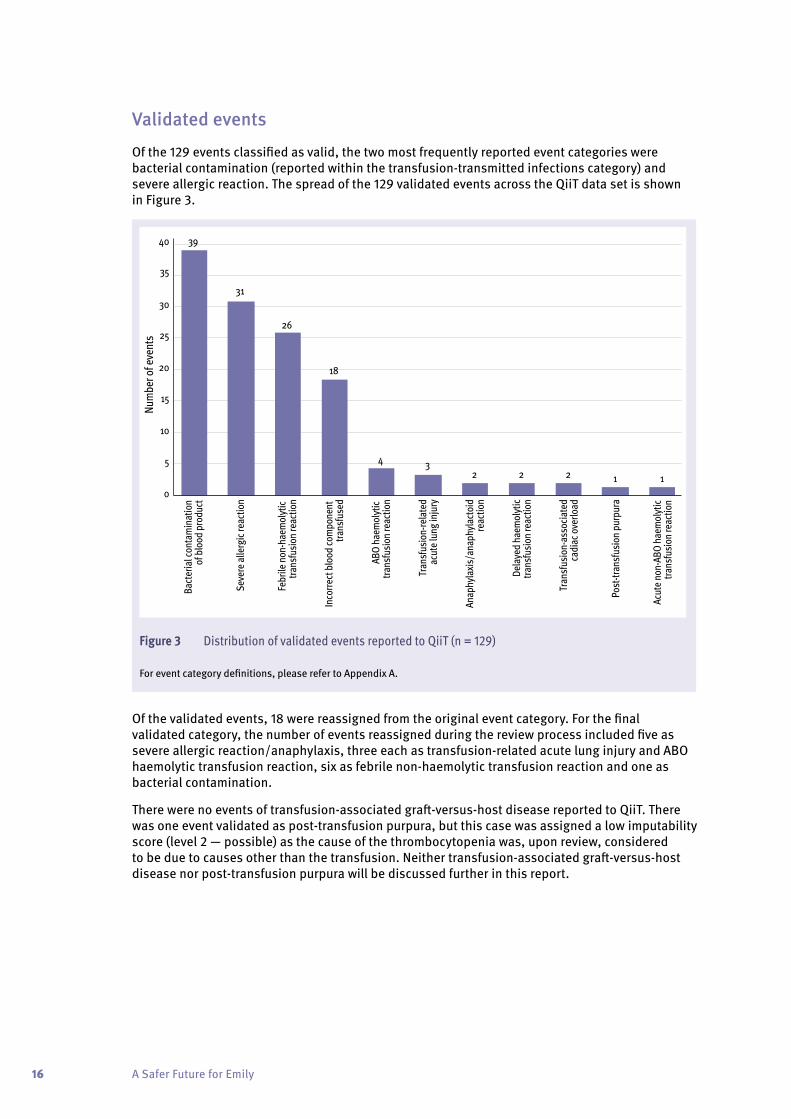
Validated events
Of the 129 events classified as valid, the two most frequently reported event categories were bacterial contamination (reported within the transfusion-transmitted infections category) and severe allergic reaction. The spread of the 129 validated events across the QiiT data set is shown in Figure 3.
0
5
10
15
20
25
30
35
40
Num
ber o
f eve
nts
Bact
eria
l con
tam
inat
ion
of b
lood
pro
duct
Seve
re a
llerg
ic re
actio
n
Febr
ile n
on-h
aem
olyt
ic tra
nsfu
sion
reac
tion
Inco
rrect
blo
od co
mpo
nent
tra
nsfu
sed
ABO
haem
olyt
ic tra
nsfu
sion
reac
tion
Tran
sfus
ion-
rela
ted
acut
e lu
ng in
jury
Anap
hyla
xis/
anap
hyla
ctoi
dre
actio
n
Dela
yed
haem
olyt
ictra
nsfu
sion
reac
tion
Tran
sfus
ion-
asso
ciate
dca
diac
ove
rload
Post
-tran
sfus
ion
purp
ura
Acut
e no
n-AB
O ha
emol
ytic
trans
fusi
on re
actio
n
39
31
26
18
4 32 2 2 1 1
Figure 3 Distribution of validated events reported to QiiT (n = 129)
For event category definitions, please refer to Appendix A.
Of the validated events, 18 were reassigned from the original event category. For the final validated category, the number of events reassigned during the review process included five as severe allergic reaction/anaphylaxis, three each as transfusion-related acute lung injury and ABO haemolytic transfusion reaction, six as febrile non-haemolytic transfusion reaction and one as bacterial contamination.
There were no events of transfusion-associated graft-versus-host disease reported to QiiT. There was one event validated as post-transfusion purpura, but this case was assigned a low imputability score (level 2 — possible) as the cause of the thrombocytopenia was, upon review, considered to be due to causes other than the transfusion. Neither transfusion-associated graft-versus-host disease nor post-transfusion purpura will be discussed further in this report.
17Queensland incidents in Transfusion (QiiT) June 2007–2009 report
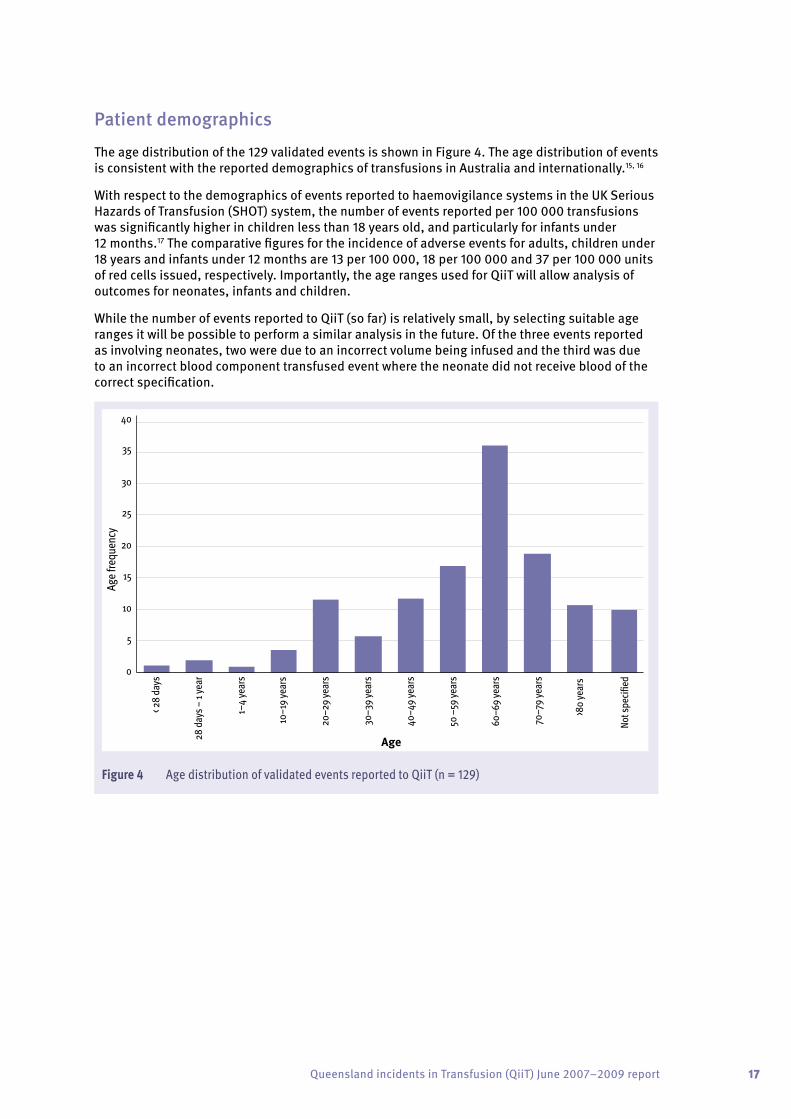
Patient demographics
The age distribution of the 129 validated events is shown in Figure 4. The age distribution of events is consistent with the reported demographics of transfusions in Australia and internationally.15, 16
With respect to the demographics of events reported to haemovigilance systems in the UK Serious Hazards of Transfusion (SHOT) system, the number of events reported per 100 000 transfusions was significantly higher in children less than 18 years old, and particularly for infants under 12 months.17 The comparative figures for the incidence of adverse events for adults, children under 18 years and infants under 12 months are 13 per 100 000, 18 per 100 000 and 37 per 100 000 units of red cells issued, respectively. Importantly, the age ranges used for QiiT will allow analysis of outcomes for neonates, infants and children.
While the number of events reported to QiiT (so far) is relatively small, by selecting suitable age ranges it will be possible to perform a similar analysis in the future. Of the three events reported as involving neonates, two were due to an incorrect volume being infused and the third was due to an incorrect blood component transfused event where the neonate did not receive blood of the correct specification.
0
5
10
15
20
25
30
35
40
Age
frequ
ency
< 28
day
s
28 d
ays –
1 ye
ar
1–4
year
s
10–1
9 ye
ars
20–2
9 ye
ars
30–3
9 ye
ars
40–4
9 ye
ars
50 –
59 ye
ars
60–6
9 ye
ars
70–7
9 ye
ars
>80
year
s
Not s
peci�
ed
Age
Figure 4 Age distribution of validated events reported to QiiT (n = 129)
18 A Safer Future for Emily
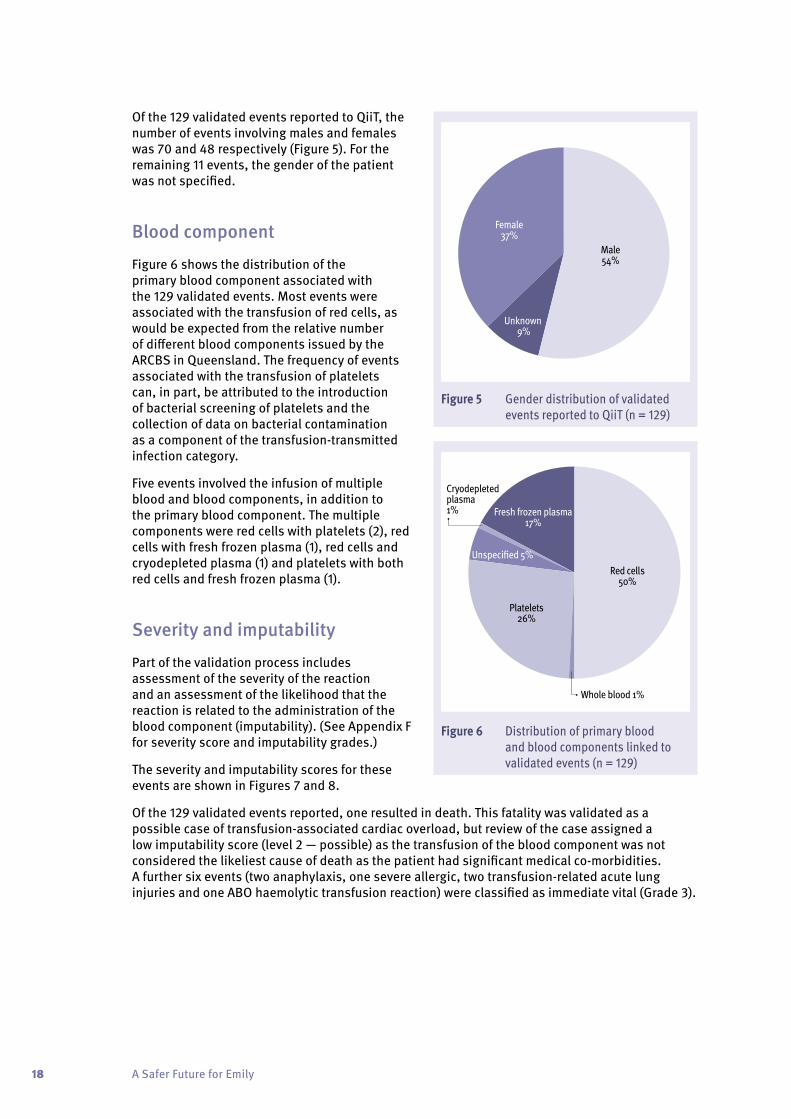
Of the 129 validated events reported to QiiT, the number of events involving males and females was 70 and 48 respectively (Figure 5). For the remaining 11 events, the gender of the patient was not specified.
Blood component
Figure 6 shows the distribution of the primary blood component associated with the 129 validated events. Most events were associated with the transfusion of red cells, as would be expected from the relative number of different blood components issued by the ARCBS in Queensland. The frequency of events associated with the transfusion of platelets can, in part, be attributed to the introduction of bacterial screening of platelets and the collection of data on bacterial contamination as a component of the transfusion-transmitted infection category.
Five events involved the infusion of multiple blood and blood components, in addition to the primary blood component. The multiple components were red cells with platelets (2), red cells with fresh frozen plasma (1), red cells and cryodepleted plasma (1) and platelets with both red cells and fresh frozen plasma (1).
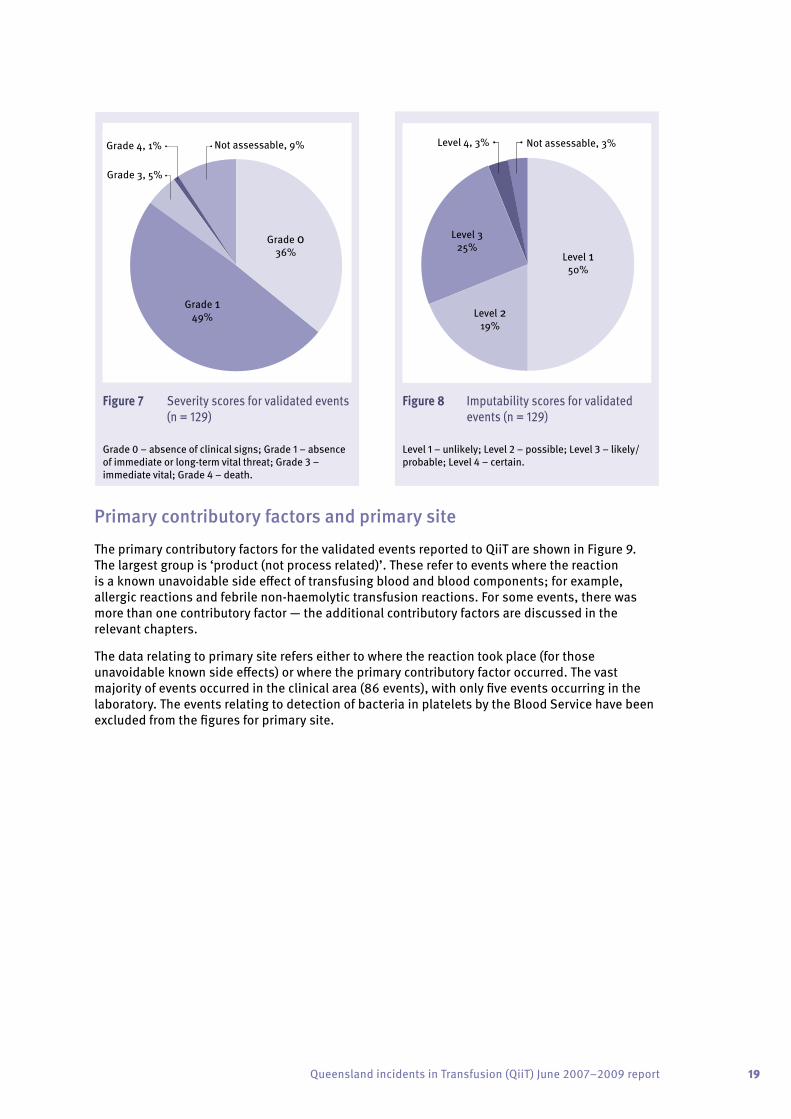
Severity and imputability
Part of the validation process includes assessment of the severity of the reaction and an assessment of the likelihood that the reaction is related to the administration of the blood component (imputability). (See Appendix F for severity score and imputability grades.)
The severity and imputability scores for these events are shown in Figures 7 and 8.
Of the 129 validated events reported, one resulted in death. This fatality was validated as a possible case of transfusion-associated cardiac overload, but review of the case assigned a low imputability score (level 2 — possible) as the transfusion of the blood component was not considered the likeliest cause of death as the patient had significant medical co-morbidities. A further six events (two anaphylaxis, one severe allergic, two transfusion-related acute lung injuries and one ABO haemolytic transfusion reaction) were classified as immediate vital (Grade 3).
Figure 5 Gender distribution of validated events reported to QiiT (n = 129)
Male54%
Female37%
Unknown 9%
Figure 6 Distribution of primary blood and blood components linked to validated events (n = 129)
Fresh frozen plasma17%
Cryodepletedplasma1%
Unspeci�ed 5%
Platelets26%
Whole blood 1%
Red cells50%
19Queensland incidents in Transfusion (QiiT) June 2007–2009 report
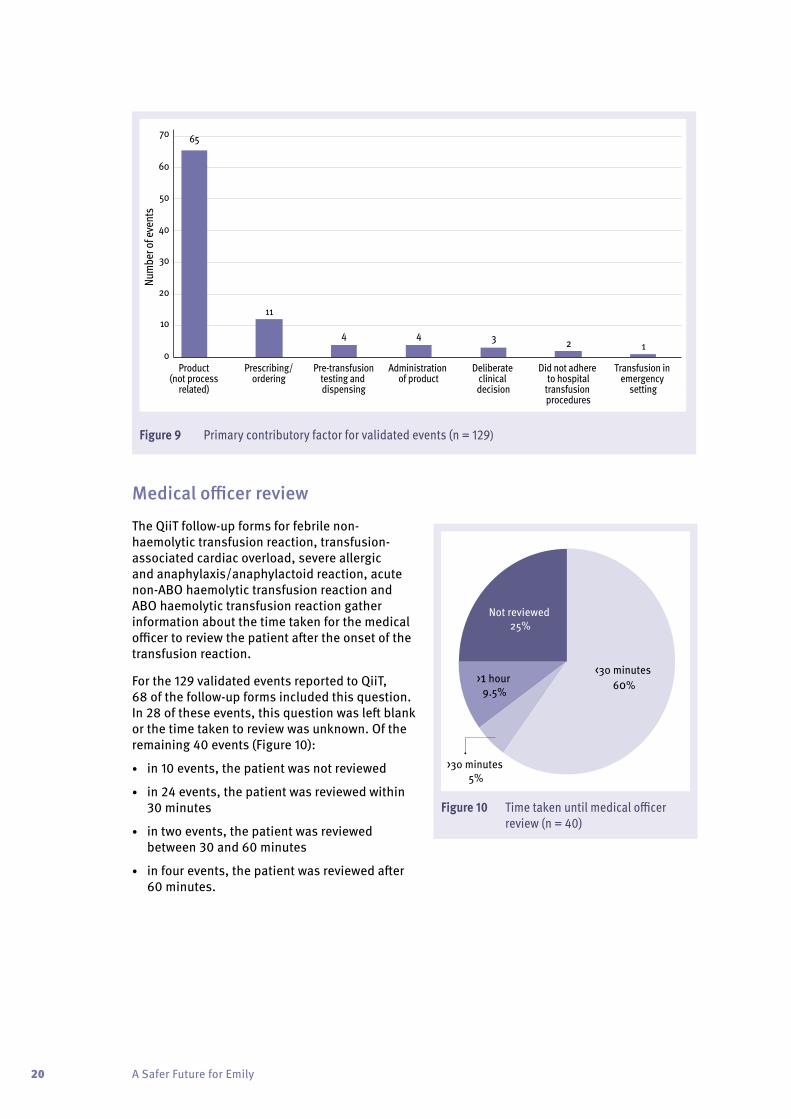
Primary contributory factors and primary site
The primary contributory factors for the validated events reported to QiiT are shown in Figure 9. The largest group is ‘product (not process related)’. These refer to events where the reaction is a known unavoidable side effect of transfusing blood and blood components; for example, allergic reactions and febrile non-haemolytic transfusion reactions. For some events, there was more than one contributory factor — the additional contributory factors are discussed in the relevant chapters.
The data relating to primary site refers either to where the reaction took place (for those unavoidable known side effects) or where the primary contributory factor occurred. The vast majority of events occurred in the clinical area (86 events), with only five events occurring in the laboratory. The events relating to detection of bacteria in platelets by the Blood Service have been excluded from the figures for primary site.
Figure 7 Severity scores for validated events (n = 129)
Grade 0 – absence of clinical signs; Grade 1 – absence of immediate or long-term vital threat; Grade 3 – immediate vital; Grade 4 – death.
Not assessable, 9%Grade 4, 1%
Grade 3, 5%
Grade 149%
Grade 036%
Figure 8 Imputability scores for validated events (n = 129)
Level 1 – unlikely; Level 2 – possible; Level 3 – likely/probable; Level 4 – certain.
Not assessable, 3%Level 4, 3%
Level 325%
Level 219%
Level 150%
20 A Safer Future for Emily
0
10
20
30
40
50
60
70Nu
mbe
r of e
vent
s
Product (not process
related)
Prescribing/ordering
Pre-transfusiontesting and dispensing
Administration of product
Deliberate clinical decision
Did not adhere to hospital
transfusion procedures
Transfusion in emergency
setting
65
11
4 4 3 2 1
Figure 9 Primary contributory factor for validated events (n = 129)
Medical officer review
The QiiT follow-up forms for febrile non-haemolytic transfusion reaction, transfusion-associated cardiac overload, severe allergic and anaphylaxis/anaphylactoid reaction, acute non-ABO haemolytic transfusion reaction and ABO haemolytic transfusion reaction gather information about the time taken for the medical officer to review the patient after the onset of the transfusion reaction.
For the 129 validated events reported to QiiT, 68 of the follow-up forms included this question. In 28 of these events, this question was left blank or the time taken to review was unknown. Of the remaining 40 events (Figure 10):
• in 10 events, the patient was not reviewed
• in 24 events, the patient was reviewed within 30 minutes
• in two events, the patient was reviewed between 30 and 60 minutes
• in four events, the patient was reviewed after 60 minutes.
Figure 10 Time taken until medical officer review (n = 40)
Not reviewed 25%
>1 hour 9.5%
>30 minutes 5%
<30 minutes 60%
21Queensland incidents in Transfusion (QiiT) June 2007–2009 report
7. Transfusion-transmitted infection
Data summary
Cate
gory
/ ca
tego
ries Transfusion-transmitted
infection (TTI)
Total number of events: 39
Gend
er Male/female ratio 20:15
Unknown 4
Age
<28 days 0
28 days – 1 year 0
1–9 years 1
10–29 years 0
30–49 years 6
50–69 years 16
70–79 years 7
80+ years 3
Unknown 6
Tim
e of
tra
nsfu
sion
In core hours (8.30am – 5.30pm) 23
Out of core hours (5.30pm – 8.30am) 11
Unknown 5
Impu
tabi
lity
Level 1 0
Level 2 9
Level 3 0
Level 4 26
Not assessable 4
Impl
icat
ed b
lood
co
mpo
nent
s
Red cells 6
Platelets 22
Fresh frozen plasma 1
Multiple components 1
Unknown 9
Seve
rity
Grade 0 29
Grade 1 0
Grade 2 0
Grade 3 0
Grade 4 0
Not assessable 10
Prim
ary
erro
r Product not process 1
Other 38
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.
Discussion
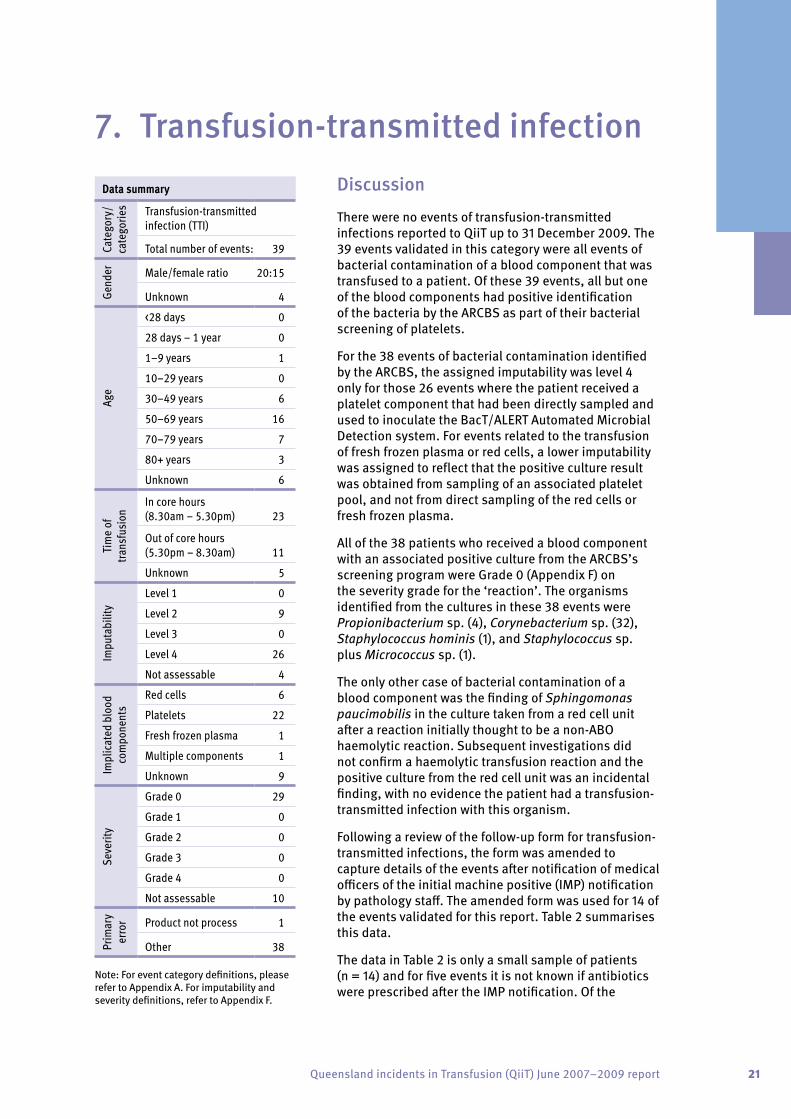
There were no events of transfusion-transmitted infections reported to QiiT up to 31 December 2009. The 39 events validated in this category were all events of bacterial contamination of a blood component that was transfused to a patient. Of these 39 events, all but one of the blood components had positive identification of the bacteria by the ARCBS as part of their bacterial screening of platelets.
For the 38 events of bacterial contamination identified by the ARCBS, the assigned imputability was level 4 only for those 26 events where the patient received a platelet component that had been directly sampled and used to inoculate the BacT/ALERT Automated Microbial Detection system. For events related to the transfusion of fresh frozen plasma or red cells, a lower imputability was assigned to reflect that the positive culture result was obtained from sampling of an associated platelet pool, and not from direct sampling of the red cells or fresh frozen plasma.
All of the 38 patients who received a blood component with an associated positive culture from the ARCBS’s screening program were Grade 0 (Appendix F) on the severity grade for the ‘reaction’. The organisms identified from the cultures in these 38 events were Propionibacterium sp. (4), Corynebacterium sp. (32), Staphylococcus hominis (1), and Staphylococcus sp. plus Micrococcus sp. (1).
The only other case of bacterial contamination of a blood component was the finding of Sphingomonas paucimobilis in the culture taken from a red cell unit after a reaction initially thought to be a non-ABO haemolytic reaction. Subsequent investigations did not confirm a haemolytic transfusion reaction and the positive culture from the red cell unit was an incidental finding, with no evidence the patient had a transfusion-transmitted infection with this organism.
Following a review of the follow-up form for transfusion-transmitted infections, the form was amended to capture details of the events after notification of medical officers of the initial machine positive (IMP) notification by pathology staff. The amended form was used for 14 of the events validated for this report. Table 2 summarises this data.
The data in Table 2 is only a small sample of patients (n = 14) and for five events it is not known if antibiotics were prescribed after the IMP notification. Of the

22 A Safer Future for Emily
remaining nine events, five patients were already on antibiotics and three had antibiotics prescribed following the IMP notification. The data shows some variation in practice that likely reflects the patient’s medical co-morbidities and variation in medical practice to this new clinical scenario.
Only one patient developed a fever 24 hours after the infusion of platelets. This patient had a positive blood culture from the day before the platelet transfusion and was already receiving broad-spectrum antibiotics.
Table 2 Analysis of 14 events of bacterial contamination. All 14 patients received platelets.
No antibiotics prescribed after IMP
notification
Antibiotics prescribed after IMP notification
On antibiotics before IMP notification Unknown Total
Total 1 3 5 5 14
Inpatient/outpatient/unknown 1/ 0 / 0 2 / 1 / 0 5 / 0 / 0 4 / 0 / 1 12 / 1 / 1
Reviewed by medical officer yes/no/unknown 0 / 0 / 1 3 / 0 / 0 4 / 0 / 1 0 / 0 / 5 7 / 0 / 7
Blood culture done/not done/unknown 0 / 1 / 0 2 / 1 / 0 0 / 5 / 0 0 / 4 / 1 2 / 11 / 1
Pyrexia yes/no/unknown 0 / 0 / 1 0 / 3 / 0 1 / 3 / 1 0 / 0 / 5 1 / 6 / 7
IMP – initial machine positive
Of the 38 events identified from positive cultures by the ARCBS, follow-up of the events for QiiT evidence for administration of the blood component was not documented in the medical charts for six patients. As these ‘contaminated’ components randomly enter the healthcare system, the lack of traceability for the final fate of 16 per cent of these components is likely to reflect the true error rate in traceability, using the current paper-based methods of documentation.
Summary
The introduction of bacterial screening of platelets by the ARCBS is an important advance in minimising the risk of bacterial-transmitted transfusion reactions. Bacterial contamination of platelet components occurs in about one in 3000 platelet products, and the rate of septic transfusion reactions following platelet transfusions is about one in 25 000.18, 19
The introduction of bacterial screening has reduced the exposure of patients to blood components contaminated with bacteria. Even in those patients who receive contaminated components as defined by a positive culture in the screening system (BacT/ALERT), the risks of developing a septic transfusion reaction are low.18, 19 In the Netherlands, one patient out of 158 patients who received a transfusion of platelets found to be culture-positive developed a reaction, and this reaction was thought unlikely to be due to the bacterial contamination.
The data submitted to QiiT, and the more extensive data collected by the ARCBS are consistent with the data from the Netherlands, and reflect the low pathogenicity of the diphtheroids (Propionibacterium sp. and Corynebacterium sp.), the most common organisms grown.
The implementation of the BacT/ALERT screening of platelet products does not totally protect recipients against developing a septic transfusion reaction18 and clinical staff must continue to be vigilant for this often fatal complication of transfusion.
When the platelet screening program was implemented by the ARCBS, the Blood Product Advisory Committee developed clinical guidelines that were distributed to all pathology providers

23Queensland incidents in Transfusion (QiiT) June 2007–2009 report
(Appendix G). This guidance was to be distributed by pathology providers when they notified clinical staff of the IMP to aid the management of the patient who has received the potentially contaminated blood component.
Finally, the 16 per cent lack of traceability of the final fate of the bacterially contaminated components is similar to previously reported rates of traceability.20, 21 Electronic systems to track and manage blood product stocks both within and after they are issued from the blood bank have the potential to dramatically improve traceability.22 Implementation of these systems has occurred in European countries after the introduction of the EU Directive (Directive 2002/98/EC).6
Practice guidelines
• Healthcare facilities should have procedures in place based on the national guidelines for the administration of blood5 that specify the standards for recording and documenting transfusions of blood products in medical charts.
• Clinical staff should refer to the advice from pathology providers when notified of an IMP (potentially contaminated blood component) for guidance in the management of the patients who have received the implicated blood component.

24 A Safer Future for Emily
Discussion
Eighteen events were validated under the incorrect blood component transfused category. Analysis of these 18 events identified four broad contributory factors that had led to the events — failures of checking processes and procedures, failure to share clinical information, events related to deliberate clinical decisions and one case that highlighted the need for forward planning. Each of these four areas is discussed below.
By definition, no incorrect blood component transfused events were associated with any adverse outcome for the patient.
Although the QiiT data set does not include near-miss events related to the incorrect labelling of blood samples or wrong blood in tube (WBIT) events, the collection of data from a subset of the healthcare facilities participating in QiiT has allowed the inclusion of some data on WBIT events. The number of WBIT events reported to QiiT up until 31 December 2009 is 273. These WBIT events are only those that have been detected by pathology laboratories due to inconsistencies in laboratory results; for example, a change in ABO blood group between tests.
International data has shown that labelling errors of blood samples are very common, with one in 165 samples affected, and that WBIT events occur in one in 2000 blood samples.23 To put this in a local context, Pathology Queensland registers about 2.2 million blood samples each year. Therefore, although a significant proportion of WBIT samples are detected by pathology providers, it is likely that many samples are not detected and this could result in:
• prescribing of blood products for test results that do not belong to the intended patient, leading to inappropriate transfusions
• missing an alloantibody on the antibody screen
• potentially an ABO or Rh D mismatched transfusion.
Clinical staff should be aware of the potential consequences of mislabelling samples sent to pathology.
Data summary
Cate
gory
/ ca
tego
ries Incorrect blood component
transfused
Total number of events: 18
Gend
er Male/female ratio 10:7
Unknown 1
Age
<28 days 1
28 days – 1 year 2
1–9 years 0
10–29 years 3
30–49 years 2
50–69 years 8
70–79 years 2
80+ years 0
Unknown 0
Tim
e of
tra
nsfu
sion
In core hours (8.30am – 5.30pm) 13
Out of core hours (5.30pm – 8.30am) 5
Impu
tabi
lity
Level 1 0Level 2 0Level 3 0Level 4 18Not assessable 0
Impl
icat
ed b
lood
co
mpo
nent
s
Red cells 11Platelets 2Fresh frozen plasma 2Multiple components 1Whole blood 1Unknown 1
Seve
rity
Grade 0 17Grade 1 1Grade 2 0Grade 3 0Grade 4 0
Not assessable 0
Prim
ary
erro
r
Administration of product 2
Deliberate clinical decision 2
Prescribing/ordering 11
Pre-transfusion testing and dispensing 3
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.
8. Incorrect blood component transfused

25Queensland incidents in Transfusion (QiiT) June 2007–2009 report
1. Failure of checking processes and procedures
There were five events that fell into this broad category of incorrect blood component transfused. Two events related to the failure of checks to identify incorrect settings on infusion devices resulting in the wrong volume being infused. This was a particular problem for neonates and children where pumps are routinely used to deliver the correct volume of the blood component.
Two patients received the wrong blood component. In one case, a patient was prescribed and administered a blood component that was required by another patient on the ward.
In one case, the cross-match labels for two units of red cells were transposed in the laboratory. The first unit was transfused without the error being detected by the bedside checks, but when the second unit was taken to the ward the correct bedside checking process detected the discrepancy between the blood unit number on the blood bag and the cross-match label. Fortunately, both units were intended for the same patient, but a similar labelling error and failure of bedside checks could have resulted in a patient receiving blood of the incorrect blood group.
2. Information-sharing
There were 10 events where the lack of sharing of clinical information resulted in the incorrect blood component being transfused. In eight of these events, patients received blood of the incorrect specification; for example, non-irradiated or CMV-negative blood components (total of 20 units). These transfusions potentially could have resulted in transfusion-associated graft-versus-host disease or CMV infections in susceptible patient groups; for example, patients receiving chemotherapy. In two events, clinical staff failed to follow hospital protocols and inform the blood bank staff of special requirements for patients undergoing specific medical procedures.
Case one*
A blood bank was contacted at midnight for an emergency supply of blood for a neonate born prematurely with hydrops due to haemolytic disease. The supply of red cells was complicated by the emergency nature of the situation. According to ANZSBT guidelines, the red cells should be less than five days old and used within 24 hours following irradiation. The existing blood stocks in the hospital did not hold irradiated blood compatible with these national guidelines, and in view of the clinical urgency, red cells that did not meet the criteria for age or time from irradiation had to be transfused. No adverse effect was experienced by the neonate.
Further analysis of this case could highlight issues about communication, planning of blood bank inventories, facilities for irradiation of blood components or supply issues. Appropriate local analysis of such events is required to identify system failures that could help to prevent similar situations in the future. There are opportunities for improving clinical and laboratory services by learning from events where no harm is caused to the patient. It is recommended that all healthcare staff attend appropriate training (for example, the HEAPS course offered by the Patient Safety Centre) and participate in incident reporting and local analysis of events.
Case two*
A 24-year-old woman (blood group A) was transfused group O red cells meant for another patient on another ward. Both patients shared the same surname. Fortunately, the error was picked up when the blood was collected for the other patient (blood group O). If the error had not been picked up when the blood was collected for the other patient it could have resulted in a potentially fatal transfusion of group A red cells to an individual who required group O red cells.
So how did this happen? When the blood was collected from the blood bank, the wrong unit was picked up from the blood fridge due to the identical surnames. The laboratory staff then issued the unit using the surname on the cross match label (which was stuck to red cell unit), rather than the patient ID which had been brought to the blood bank by the nursing staff. This meant that the discrepancy in the first name, date of birth and UR number was not picked up. This error then continued to the bedside where adequate bedside checks were not performed and the blood was transfused. All these events occurred within core working hours on a weekday.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY

26 A Safer Future for Emily
Case three*
A 65-year-old man receiving fludarabine for non-Hodgkin’s lymphoma should have received irradiated blood components to prevent possible transfusion-associated graft-versus-host disease. However, the request forms sent to the blood bank failed to contain the information that the patient required irradiated blood components and the patient received 10 units of non-irradiated red blood cells. The need for irradiated blood had been placed on the patient’s laboratory file as a ‘flag’ to remind laboratory staff to select irradiated blood. But the patient’s care was transferred to another hospital and the flag indicating the need for irradiated blood did not automatically transfer between the laboratory information systems.
The request form and prescription should indicate the need for irradiated blood each time blood
components are requested. This is the responsibility of the staff requesting the blood components. Patient groups who require irradiated blood components are listed in the national ANZSBT guidelines.
The laboratory IT system flag serves as an additional check to remind laboratory staff to issue irradiated blood. But such ‘flags’ may not be transferred between blood bank laboratories at different healthcare facilities, so medical staff must ensure their local blood bank staff are aware of these special requirements. Transfusion-associated graft-versus-host disease has been associated with use of red cells, platelets and whole blood, but not fresh frozen plasma or cryoprecipitate. The mortality rate is high (90 per cent) if transfusion-associated graft-versus-host disease develops.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE
STU
DY
Where patients received non-irradiated or CMV-negative blood components contrary to their medical requirements, the main contributory factor was the medical officers’ failure to detail the need for these products on the request form to blood bank staff. Another contributory factor was the lack of transfer of relevant alerts stored on pathology laboratory information systems between laboratories.
3. Deliberate clinical decision
Sometimes the supply of blood components does not match demand. In these situations, clinicians may make deliberate clinical decisions to administer Rh D positive blood components to patients who are Rh D negative. This could potentially result in a patient developing anti-D antibodies that could complicate cross-matching for future transfusions. This is of particular concern in Rh D
negative women of child-bearing age due to the risk of the development of Rh haemolytic disease of the newborn due to anti-D.
All attempts are made to minimise the risks of these deliberate clinical decisions, including the administration of anti-D prophylaxis within 72 hours of the transfusion to prevent allo-anti-D forming, when clinically appropriate.
In one case reported to QiiT, the prophylactic anti-D was not administered within 72 hours, but allo-anti-D did not subsequently develop in the patient. In one case, the Rh D positive red cells were given when the pre-transfusion haemoglobin was more than 100 g/L, and potentially the transfusion could have been delayed until Rh D negative red cells were available.
Summary
Incorrect blood component transfused events are among those events most commonly reported to haemovigilance systems.24, 25 Such events, and those of wrong blood in tube events, highlight the errors that occur across the pathway of administering blood products, and have allowed discussion of the common errors and potential solutions to some of the weaknesses in the system.3, 26
Data from Serious Hazards of Transfusion (SHOT) shows that about 70 per cent of incorrect blood component transfused events occur in the clinical area and that more than 50 per cent of events involve more than one contributory factor.25 The most common single contributory factor is failure of the final patient identification check (27 per cent of events). Of note, in 87 per cent of these

27Queensland incidents in Transfusion (QiiT) June 2007–2009 report
events, previous contributory factors could have been detected by the correct procedure during the bedside check. This data from SHOT is mirrored by the findings of an audit of the collection and administration of blood and blood product transfusions in Queensland.1
The events reported to QiiT are consistent with the findings from other haemovigilance systems and show that the clinical area is associated with most of the contributory factors in events of incorrect blood component transfused (14 of 18 events).
On review of the events to QiiT, some potential future solutions to reduce the frequency of incorrect blood component transfused events include:
• adaptation of the 3Cs (ensuring correct patient, correct site and side, correct procedure) to the final bedside check
• ensuring transmission of relevant transfusion alerts between pathology laboratories
• electronic ordering of blood products with in-built forcing functions to ensure special requirements and appropriateness of transfusion are dealt with when ordering blood products
• engaging consumers of healthcare services to be aware of and participate in procedures, such as patient identification checks
• full implementation of written informed consent for transfusions, to allow a further opportunity to review the appropriateness of the transfusion by the clinical staff and patient
• use of technology to reduce human errors at critical steps in the transfusion pathway, such as the administration of blood products at the bedside
• zero tolerance of mislabelled samples received by pathology.
Practice guidelines
• Healthcare facilities should develop and implement procedures:
– that outline the minimum standards of patient identification and procedure required for the collection of blood products
– for formally checking the identification of the patient against the blood component label at the bedside. This procedure should reference the national administration guidelines.5
• The blood component should be spiked and the transfusion connected to the patient’s intravenous line (hung) immediately after the correct checks are performed at the bedside. If for any reason there is a delay between performing the checks at the bedside and the blood component being spiked and hung, the checks should be repeated at the bedside immediately before the component is spiked and hung.
• The blood component should be hung by one of the staff members participating in the bedside checks.
• Blood products should always be administered against a written prescription.
• Laboratory IT systems should be checked for special requirements for each patient receiving blood products.
• Hospital procedures for ordering and administering blood products should ensure that irradiated and other special requirement blood components are always given where appropriate. The procedure must clearly state the need for a medical officer to clearly request and prescribe these products when indicated.
• Where Rh D positive blood components have to be administered to Rh D negative patients in emergency situations, and where administration of anti-D prophylaxis is clinically indicated to prevent allo-anti-D formation, the anti-D prophylaxis should be administered within 72 hours.

28 A Safer Future for Emily
9. ABO haemolytic transfusion reaction
Data summary
Cate
gory
/ ca
tego
ries ABO haemolytic transfusion
reaction (ABO HTR)
Total number of events: 4
Gend
er Male/female ratio 2:2
Unknown 0
Age
<28 days 0
28 days – 1 year 0
1–9 years 0
10–29 years 0
30–49 years 0
50–69 years 3
70–79 years 1
80+ years 0
Unknown 0
Tim
e of
tra
nsfu
sion In core hours
(8.30am – 5.30pm) 2
Out of core hours (5.30pm – 8.30am) 2
Impu
tabi
lity
Level 1 0
Level 2 1
Level 3 0
Level 4 3
Not assessable 0
Impl
icat
ed b
lood
co
mpo
nent
s Red cells 3
Unknown 1
Seve
rity
Grade 0 0
Grade 1 3
Grade 2 0
Grade 3 1
Grade 4 0
Not assessable 0
Prim
ary
erro
r
Administration of product 1
Deliberate clinical decision 1
Did not adhere to hospital transfusion procedures 2
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.
Discussion
There were four validated events within the ABO haemolytic transfusion reaction category. In three of the four events, the reaction was related to the transfusion of ABO incompatible red cells, with an imputability score of four (certain). None of these three events were fatal.
The fourth case involved a reaction after infusion of major ABO mismatched stem cells. In this case, the reaction was felt unlikely to be an ABO haemolytic transfusion reaction, although this could not be fully excluded. The hospital protocol was followed and appropriate steps were taken to minimise the risks of an ABO haemolytic transfusion reaction.
Contributory factors for the three ABO incompatible transfusions were:
1. two of the three red cell transfusions occurred outside working hours
2. final ‘bedside’ checks were performed in a side room distant to the patient
3. staff hanging the blood were not involved in the final checking process
4. emergency situation
5. poor communication between team members
6. lack of a prescription/IV order form for the transfusions
7. failure to verify and cross-check the patient identification on red cell unit label and wristband with the patient’s verbal verification of their name and date of birth
8. incorrect patient identification taken to blood bank
9. bedside checks were only performed between the red cell unit and cross-match form, not with the patient’s ID.
The signs and symptoms presented in these events included a marked drop in blood pressure, characteristic haemoglobinuria and a drop in haptoglobin. In one case, the patient reported back pain, was experiencing rigors and became tachycardic and pyrexial after receiving 20 mL of blood.

29Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Summary
The incidence of ABO haemolytic reactions is about one in 150 000 transfusions and a fatal case occurs in about one in 1.5 million allogeneic red cell units transfused.2 Like many events of incorrect blood component transfused, the events of acute ABO haemolytic transfusion reactions highlight the many errors that can occur in administering blood. Particularly relevant are the human factors involved. These three events highlight many of the contributory factors in ABO haemolytic transfusion reactions and incorrect blood component transfused events, and which have been observed in other haemovigilance systems.2, 3, 24, 25
An audit of the collection and administration of blood and blood products has previously catalogued the numerous near-misses during this complex pathway.1 In these audits, only one out of 37 had the correct checks performed. Therefore, the combination of human factors and a complex pathway both contribute to the observed incidence of incorrect blood component transfused events and ABO haemolytic transfusion reactions.
Practice guidelines
• Healthcare facilities should develop and implement procedures:
– that outline the minimum standards of patient identification and procedure required for the collection of blood products
– for formally checking the identification of the patient against the blood component label at the bedside. This procedure should reference the national administration guidelines.5
• The blood component should be spiked and the transfusion connected to the patient’s intravenous line (hung) immediately after the correct checks are performed at the bedside. If for any reason there is a delay between performing the checks at the bedside and the blood component being spiked and hung, the checks should be repeated at the bedside immediately before the component is spiked and hung.
• The blood component should be hung by one of the staff members participating in the bedside checks.
• Out-of-hours elective transfusions are best avoided and should be performed only when clinically indicated and in accordance with guidelines on appropriate use of blood components.
Case one*
A 36-year-old man who had been operated on that afternoon was found to have a haemoglobin level of 70 g/L. The medical officer asked for a two-unit transfusion of red cells that evening.
When the blood was due for collection, the registered nurse (RN) caring for the patient was called to a second patient in the four-bed bay who was receiving a transfusion and had developed acute shortness of breath and dropped their oxygen saturations to 80 per cent on room air.
The RN asked the agency nurse whose patient she had been called to see, to go to the blood bank and collect the blood for the post-operative patient. The agency nurse asked the name of the patient and requested a sticker with the patient’s identification. However, the RN was busy with the patient suffering an acute reaction and said the medical chart was on the desk outside. The agency nurse
picked up a patient’s sticker and collected the blood and cross-match form from Blood Bank.
On returning to the ward, the two RNs on night duty were drawing up hydrocortisone for the patient who had suffered the acute transfusion reaction. The agency nurse gave the unit of red cells to the RNs who performed the checks of the blood unit against the cross-match form in the side room. They then called the agency nurse and asked her to hang the blood. The bedside checks were not completed at the bedside, and the 36-year-old man who was blood group O was transfused group A red cells meant for another patient. Despite developing signs and symptoms of a haemolytic reaction, the patient made a full recovery.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY
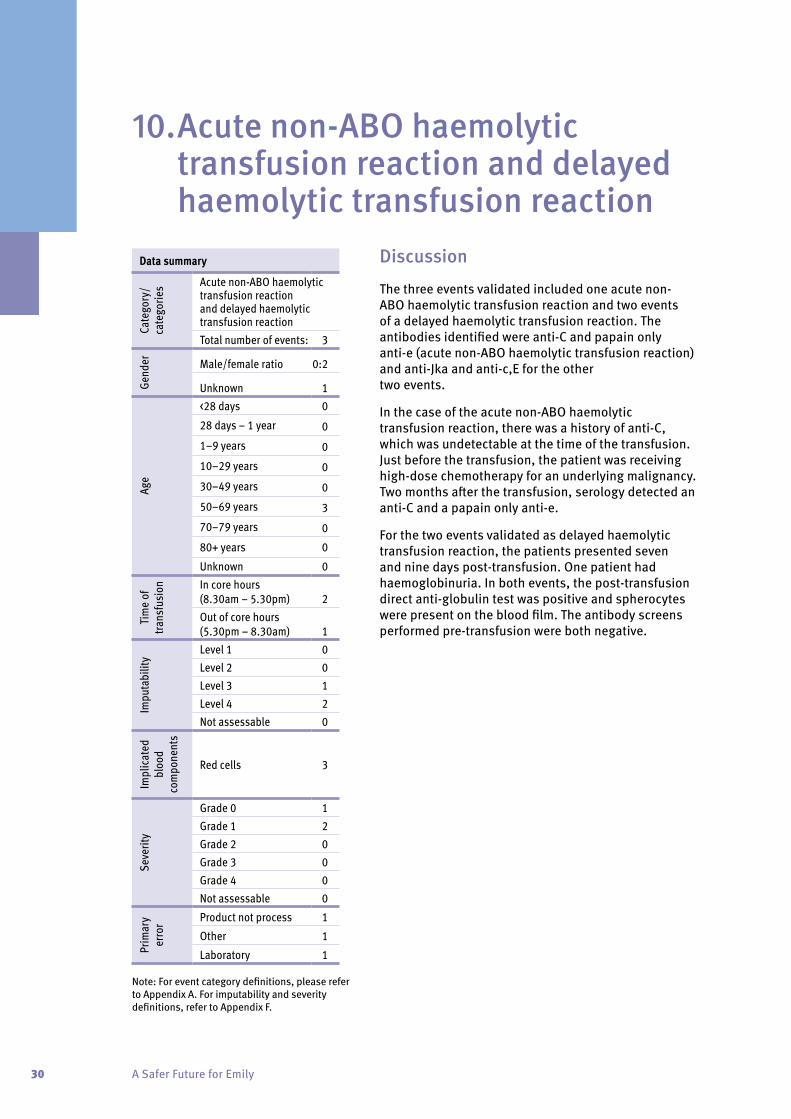
30 A Safer Future for Emily
Discussion
The three events validated included one acute non-ABO haemolytic transfusion reaction and two events of a delayed haemolytic transfusion reaction. The antibodies identified were anti-C and papain only anti-e (acute non-ABO haemolytic transfusion reaction) and anti-Jka and anti-c,E for the other two events.
In the case of the acute non-ABO haemolytic transfusion reaction, there was a history of anti-C, which was undetectable at the time of the transfusion. Just before the transfusion, the patient was receiving high-dose chemotherapy for an underlying malignancy. Two months after the transfusion, serology detected an anti-C and a papain only anti-e.
For the two events validated as delayed haemolytic transfusion reaction, the patients presented seven and nine days post-transfusion. One patient had haemoglobinuria. In both events, the post-transfusion direct anti-globulin test was positive and spherocytes were present on the blood film. The antibody screens performed pre-transfusion were both negative.
10. Acute non-ABO haemolytic transfusion reaction and delayed haemolytic transfusion reaction
Data summary
Cate
gory
/ ca
tego
ries Acute non-ABO haemolytic
transfusion reaction and delayed haemolytic transfusion reactionTotal number of events: 3
Gend
er Male/female ratio 0:2
Unknown 1
Age
<28 days 0
28 days – 1 year 0
1–9 years 0
10–29 years 0
30–49 years 0
50–69 years 3
70–79 years 0
80+ years 0
Unknown 0
Tim
e of
tra
nsfu
sion In core hours
(8.30am – 5.30pm) 2Out of core hours (5.30pm – 8.30am) 1
Impu
tabi
lity
Level 1 0Level 2 0Level 3 1Level 4 2Not assessable 0
Impl
icat
ed
bloo
d co
mpo
nent
s
Red cells 3
Seve
rity
Grade 0 1Grade 1 2Grade 2 0Grade 3 0Grade 4 0Not assessable 0
Prim
ary
erro
r Product not process 1
Other 1
Laboratory 1
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.

31Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Summary
These three events are characteristic of haemolytic transfusion reactions caused by antibodies to non-ABO blood group antigens. In the first 10 years of Serious Hazards of Transfusion (SHOT), antibodies to Kidd and Rh blood groups accounted for 53 per cent and 38 per cent of all delayed haemolytic transfusion reactions reported.25
Practice guidelines
• Previous laboratory transfusion records, including previous antibodies detected, should be available at all times.
Case one*
A 70-year-old man had recently been diagnosed with myelodysplasia and had started regular red cell transfusions. Ten days after his latest transfusion of three units of allogeneic red cells, the man called the day unit to say his urine was dark and his wife had noticed his eyes were yellow. The haematologist reviewed the patient that day. The patient was jaundiced and his urine was red and positive for blood on urinalysis. A full blood count and blood film revealed the haemoglobin had fallen to the pre-transfusion level and there were spherocytes on the blood film. The direct anti-globulin test (DAT) was positive and an antibody screen identified an anti-Fya that had not been present in the antibody screen pre-transfusion.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY
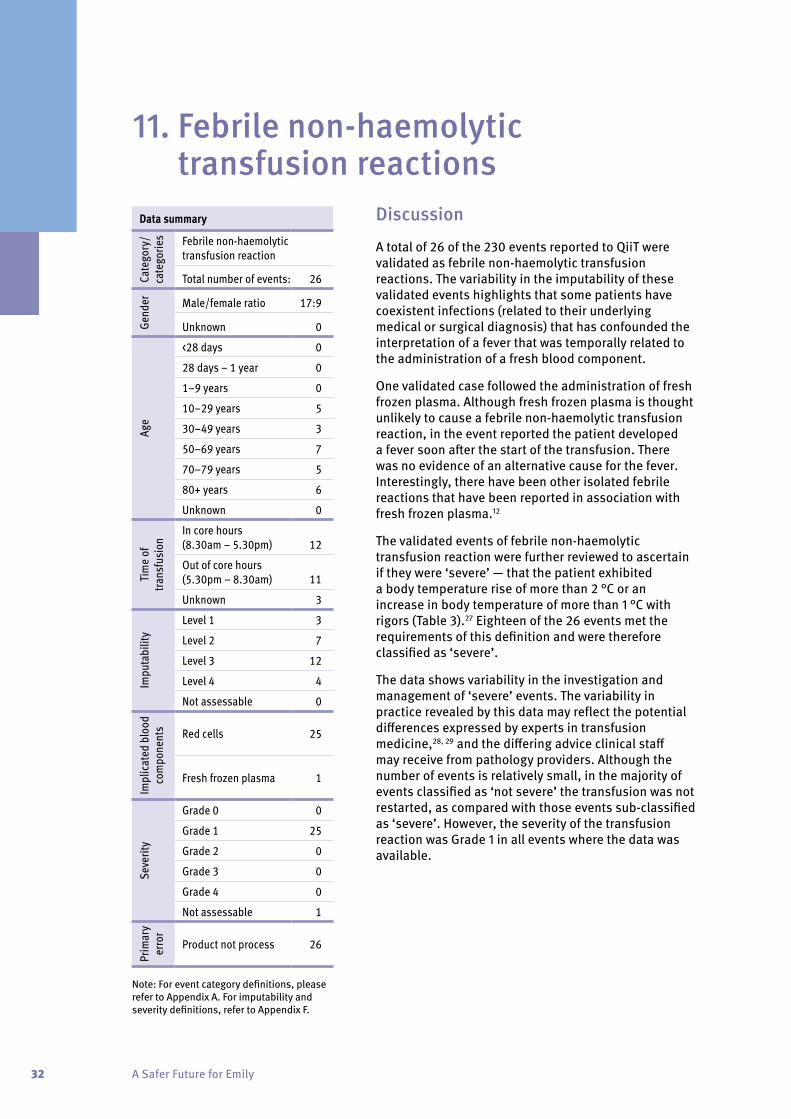
32 A Safer Future for Emily
Discussion
A total of 26 of the 230 events reported to QiiT were validated as febrile non-haemolytic transfusion reactions. The variability in the imputability of these validated events highlights that some patients have coexistent infections (related to their underlying medical or surgical diagnosis) that has confounded the interpretation of a fever that was temporally related to the administration of a fresh blood component.
One validated case followed the administration of fresh frozen plasma. Although fresh frozen plasma is thought unlikely to cause a febrile non-haemolytic transfusion reaction, in the event reported the patient developed a fever soon after the start of the transfusion. There was no evidence of an alternative cause for the fever. Interestingly, there have been other isolated febrile reactions that have been reported in association with fresh frozen plasma.12
The validated events of febrile non-haemolytic transfusion reaction were further reviewed to ascertain if they were ‘severe’ — that the patient exhibited a body temperature rise of more than 2 °C or an increase in body temperature of more than 1 °C with rigors (Table 3).27 Eighteen of the 26 events met the requirements of this definition and were therefore classified as ‘severe’.
The data shows variability in the investigation and management of ‘severe’ events. The variability in practice revealed by this data may reflect the potential differences expressed by experts in transfusion medicine,28, 29 and the differing advice clinical staff may receive from pathology providers. Although the number of events is relatively small, in the majority of events classified as ‘not severe’ the transfusion was not restarted, as compared with those events sub-classified as ‘severe’. However, the severity of the transfusion reaction was Grade 1 in all events where the data was available.
11. Febrile non-haemolytic transfusion reactions
Data summary
Cate
gory
/ ca
tego
ries Febrile non-haemolytic
transfusion reaction
Total number of events: 26
Gend
er Male/female ratio 17:9
Unknown 0
Age
<28 days 0
28 days – 1 year 0
1–9 years 0
10–29 years 5
30–49 years 3
50–69 years 7
70–79 years 5
80+ years 6
Unknown 0
Tim
e of
tra
nsfu
sion
In core hours (8.30am – 5.30pm) 12
Out of core hours (5.30pm – 8.30am) 11
Unknown 3
Impu
tabi
lity
Level 1 3
Level 2 7
Level 3 12
Level 4 4
Not assessable 0
Impl
icat
ed b
lood
co
mpo
nent
s Red cells 25
Fresh frozen plasma 1
Seve
rity
Grade 0 0
Grade 1 25
Grade 2 0
Grade 3 0
Grade 4 0
Not assessable 1
Prim
ary
erro
r
Product not process 26
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.

33Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Table 3 Sub-classification of febrile non-haemolytic transfusion reaction events. (Severe events had either a body temperature rise of more than 2 °C, or an increase in body temperature of more than 1 °C associated with rigors. )
Investigated for HTR Product cultured Patient culturedDid not restart
transfusion Reviewed by MO
Severe 16/18 (88.9%) 8/18 (44.4%) 10/18 (55.6%) 10/18 (55.6%) 10/18 (55.6%)
Not severe 5/8 (62.5%) 1/8 (7.8%) 4/8 (50%) 6/8 (75%) 3/8 (37.5%)
HTR = haemolytic transfusion reaction, MO = medical officer
The introduction of universal pre-storage leucodepletion for red cells and platelets by the ARCBS will have reduced the frequency of febrile non-haemolytic transfusion reactions.30 The overall incidence of febrile non-haemolytic transfusion reactions with pre-storage leucodepleted blood and blood components is more than 1 per cent, but as seen from the events reported to QiiT, it makes up the second largest group of transfusion-related adverse events.
Summary
Febrile non-haemolytic transfusion reactions remain a common side-effect of transfusions. A febrile non-haemolytic transfusion reaction is considered a diagnosis of exclusion (where other causes for a fever post-transfusion have been investigated and found to be negative).
The rarity of alternative causes for a post-transfusion fever may impact on the experience of clinical staff and this may be reflected in the variation of investigation and management of this common post-transfusion scenario.
If this bias is influencing clinical decision-making, an alternative to the current guidelines for the management of a post-transfusion fever is needed to aid clinical staff and ensure the correct management.
Practice guidelines
• The definition of febrile non-haemolytic transfusion reaction in the QiiT data set includes the statement ‘or change of more than 1 °C from pre-transfusion level’ in reference to body temperature. This increase in body temperature only applies in events where the pre-transfusion body temperature is more than 37 °C.
• The investigation and management of transfusion reactions should adhere to hospital procedures.
Case one*
A 24-year-old female developed rigors and a fever while receiving the second unit of red blood cells. Her temperature rose from 36.4 °C to 38.1 °C during the transfusion and there was no preceding history of fever or infection. Although a haemolytic transfusion reaction (HTR) was considered, review of the patient’s chart failed to find clear documentation of the time the reaction occurred or whether the patient was reviewed by a medical officer. Despite the fever and consideration of an HTR, no laboratory investigations for an HTR were undertaken and no blood cultures were taken from the patient or the blood bag. The patient was given paracetamol, antihistamine and hydrocortisone for this reaction. The red cell transfusion was restarted and subsequently completed.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY

34 A Safer Future for Emily
Discussion
Allergic reactions complicating transfusions are common adverse events and this is reflected in the 30 validated events of severe allergic reactions and 3 validated events of anaphylaxis reported to QiiT. The incidence of urticaria during transfusion is known to be up to 3 per cent,31 while anaphylaxis is much rarer, with an incidence of about one in 50 000 transfusions.32 The events below highlight the heterogeneity of allergic reactions complicating transfusion.
Two events of anaphylaxis complicating transfusions were validated. In the first case, the patient received intravenous (IV) adrenaline, while in the second case the patient received IV fluids, IV steroids and an oral antihistamine.
In the first case, the investigations included a chest X-ray and in the second case (where the patient's blood pressure fell to 60/20 mmHg and oxygen saturations fell to less than 93 per cent), only blood cultures were performed. IgA deficiency may be a contributing factor in such cases, but IgA levels were not checked in either case.
Summary
Allergic reactions during transfusions are common. As with the events of febrile non-haemolytic transfusion reaction and acute respiratory reactions reported to QiiT, the two most severe events of severe allergic reactions/anaphylaxis highlight the variability in the investigation of transfusion reactions.
12. Severe allergic reactions and anaphylaxis
Data summary
Cate
gory
/ ca
tego
ries Severe allergic reaction and
anaphylaxis/anaphylactoid reaction
Total number of events: 33
Gend
er Male/female ratio 17:11
Unknown 5
Age
<28 days 028 days – 1 year 01–9 years 010–29 years 530–49 years 750–69 years 1570–79 years 280+ years 1Unknown 3
Tim
e of
tra
nsfu
sion
In core hours (8.30am – 5.30pm) 17
Out of core hours (5.30pm – 8.30am) 15Unknown 1
Impu
tabi
lity
Level 1 0Level 2 4Level 3 17Level 4 12Not assessable 0
Impl
icat
ed b
lood
co
mpo
nent
s
Red cells 10Platelets 4Fresh frozen plasma 13Cryoprecipitate 1Cryoprecipitate plasma 1Multiple components 3Unknown 1
Seve
rity
Grade 0 0Grade 1 30Grade 2 0Grade 3 3Grade 4 0Not assessable 0
Prim
ary
erro
r Product not process 32
Administration of product 1
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.

35Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Practice guidelines
• Patients with significant severe allergic reactions and all patients suffering anaphylaxis/anaphylactoid reactions associated with transfusions should be investigated for the underlying cause, particularly anti-IgA antibodies complicating IgA deficiency.
• An alert should be placed in the patient’s medical chart if they have suffered a significant severe allergic reaction or anaphylaxis/anaphylactoid reaction associated with a transfusion of a blood component. This alert will help guide the future management of transfusions in such patients.
• The investigation and management of transfusion reactions should adhere to hospital procedures.
Case one*
A 27-year-old woman received two units of red cells post-operatively. During the second unit, she complained of itchiness over both arms, which then spread over her back and finally to the rest of her body. A red rash, with a few hives, then developed and she complained of a ‘burning tongue’. Examination of the tongue revealed no swelling. There was no alteration in her blood pressure, pulse or oxygen saturations during or after the reaction. She was given an oral antihistamine, and the symptoms resolved within two hours. No investigations were performed.
Case two*
A 43-year-old man received a pool of platelets for chemotherapy-induced thrombocytopenia. During the transfusion, he developed an urticarial rash, pruritus and shortness of breath. His blood pressure fell from 120/70 mmHg to 96/45 mmHg and his pulse increased from 86 to 138. He remained apyrexial and his oxygen saturations did not drop. Both an antihistamine and intravenous hydrocortisone were administered. Investigations revealed negative blood cultures and a normal chest X-ray. His symptoms resolved within three hours.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY

36 A Safer Future for Emily
Discussion
Five events were validated as transfusion-associated cardiac overload (2) or transfusion-related acute lung injury (3). Of these five events, four had evidence of hypoxia, with a significant fall in oxygen saturation measured by pulse oximetry. The trough oxygen saturations in these four events were 43 per cent, 79 per cent (2) and 86 per cent.
The three lowest oxygen saturations were seen in the three events that were subsequently reclassified as possible events of transfusion-related acute lung injury. Transfusion-related acute lung injury was not considered in the differential diagnosis of these four events with hypoxia, and the three events that were reclassified had been reported to QiiT as a severe allergic reaction, anaphylaxis and a febrile non-haemolytic transfusion reaction.
Two of the four events had a chest X-ray at the time of the reaction; one was reported as showing bilateral pleural effusions (validated as possible transfusion-associated cardiac overload) and the other as showing pulmonary oedema (validated as possible transfusion-related acute lung injury).
Although there was insufficient evidence to conclude that the two events of transfusion-associated cardiac overload were definitely related to the transfusion, both patients were more than 70 years of age, had positive fluid balances before the transfusion started, and had a history of cardiac disease. Neither case was prescribed diuretics as pre-medication for the transfusion.
The differential diagnoses considered in these five events were transfusion-associated cardiac overload, allergic reaction/anaphylaxis, pulmonary embolism and febrile reaction (with negative patient blood cultures).
Summary
Acute respiratory complications after transfusions of fresh blood components are significant causes of morbidity. Transfusion-related acute lung injury was the leading cause of transfusion-associated death in data collected by the United States Food and Drug Administration33 and both transfusion-related acute lung injury and transfusion-associated cardiac overload accounted for 25 per cent each of the fatal transfusion reactions reported to the French haemovigilance system in 2002 and 2003.24
13. Acute respiratory reactions
Data summary
Cate
gory
/ ca
tego
ries
Transfusion-related acute lung injury (TRALI) and Transfusion-associated cardiac overload (TACO)
Total number of events: 5
Gend
er Male/female ratio 4:1
Unknown 0
Age
<28 days 0
28 days – 1 year 0
1–9 years 0
10–29 years 2
30–49 years 0
50–69 years 1
70–79 years 1
80+ years 1
Unknown 0
Tim
e of
tra
nsfu
sion In core hours
(8.30am – 5.30pm) 4
Out of core hours (5.30pm – 8.30am) 1
Impu
tabi
lity
Level 1 1
Level 2 2
Level 3 2
Level 4 0
Not assessable 0
Impl
icat
ed b
lood
co
mpo
nent
s Red cells 1
Platelets 1
Fresh frozen plasma 3
Seve
rity
Grade 0 0
Grade 1 0
Grade 2 2
Grade 3 2
Grade 4 1
Not assessable 0
Prim
ary
erro
r Product not process 1
Administration of product 4
Note: For event category definitions, please refer to Appendix A. For imputability and severity definitions, refer to Appendix F.

37Queensland incidents in Transfusion (QiiT) June 2007–2009 report
The five events reported to QiiT highlight several issues:
1. Transfusion-related acute lung injury is often overlooked in the differential diagnosis of acute respiratory complications of transfusion.
2. Clinical indicators suggesting a risk of developing transfusion-associated cardiac overload may not be acted on.
3. The low imputability scores for these events reflect the lack of appropriate investigations at the time of the reaction and prevent a clear conclusion on the nature of the reaction.
4. None of the possible events of transfusion-related acute lung injury were referred to the ARCBS at the time of the reaction for serological investigation of the donors.
As with other categories of events reported to QiiT, there is an indication that the investigation and management of these acute respiratory transfusion reactions may not be optimal. As a result of these concerns and the experience of underreporting of transfusion-related acute lung injury in other countries, information about transfusion-related acute lung injury was circulated to senior medical staff within Queensland in 2009. The information circulated is reproduced in Appendix C.
Practice guidelines
• In events of suspected transfusion-related acute lung injury, the transfusion laboratory that supplied the blood component should be notified so they can inform the ARCBS. This will allow for the investigation of implicated donors and appropriate management of donors who have positive serology by the Blood Service.
• Patients at risk of cardiac overload (for example, due to age, pre-existing co-morbidities, current fluid balance etc) need to be identified and medically reviewed before transfusion to allow appropriate management (for example, rate of transfusion, prophylactic diuretics) to prevent transfusion-associated cardiac overload.
• Transfusion-related acute lung injury should be considered in all patients receiving fresh blood components that contain plasma, who exhibit relevant signs and/or symptoms of acute lung injury (hypoxia, bilateral infiltrates on chest x-ray and no signs of heart failure) within six hours of a transfusion.
Case one*
A 55-year-old man on ICU with multiple fractures was prescribed fresh frozen plasma (FFP). The patient was fully conscious and receiving 30 per cent inspired oxygen to maintain his oxygen saturations at 95 per cent. Within 15 minutes of starting the fresh frozen plasma, the oxygen saturations fell to 48 per cent. This was associated with an increase in body temperature by 1 °C and rigors. The patient was reviewed promptly and received hydrocortisone. It took nine hours for the oxygen saturations and inspired oxygen requirements to return to the pre-FFP levels. Blood cultures were taken and subsequently found to be negative. Review of routine chest X-rays (CXR) performed each morning revealed a normal CXR before the reaction and a CXR showing bilateral shadowing the morning after the reaction.
* The data in this case study has been used in a de-identified manner to create this typical case example. This is not an actual case, however, it can be used to accurately illustrate key findings.
CASE STUDY
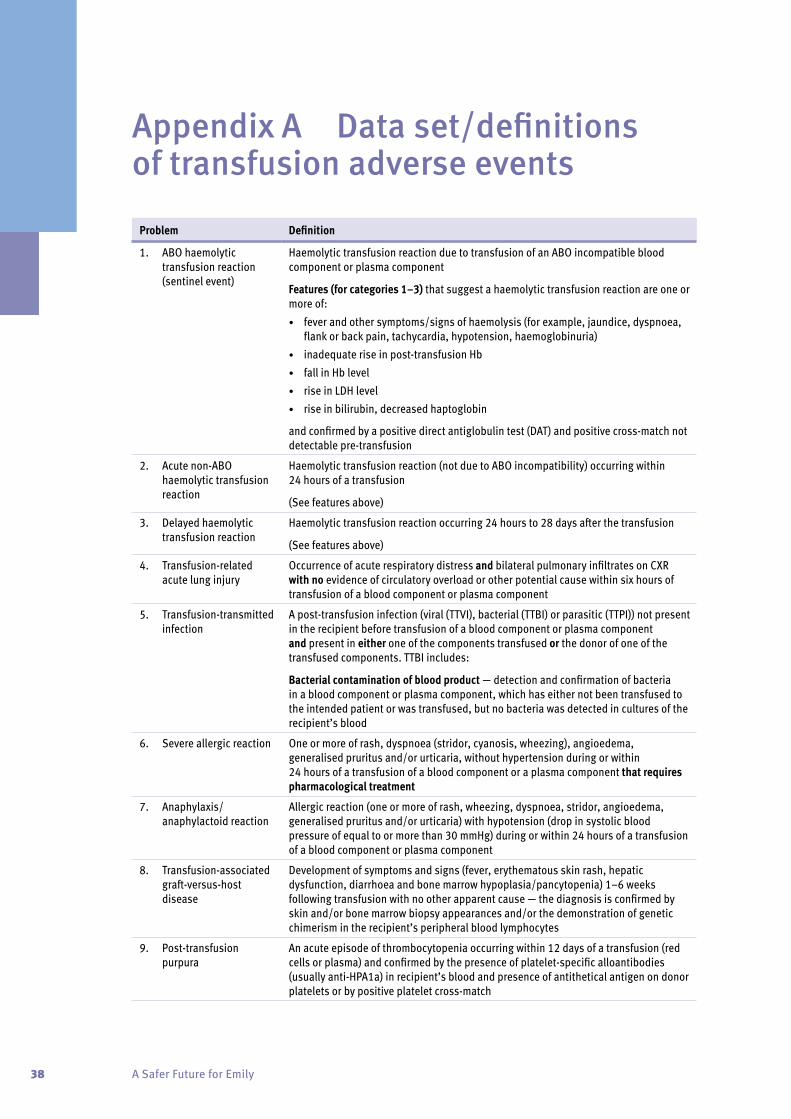
38 A Safer Future for Emily
Appendix A Data set/definitions of transfusion adverse events
Problem Definition
1. ABO haemolytic transfusion reaction (sentinel event)
Haemolytic transfusion reaction due to transfusion of an ABO incompatible blood component or plasma component
Features (for categories 1–3) that suggest a haemolytic transfusion reaction are one or more of:• fever and other symptoms/signs of haemolysis (for example, jaundice, dyspnoea,
flank or back pain, tachycardia, hypotension, haemoglobinuria)• inadequate rise in post-transfusion Hb• fall in Hb level • rise in LDH level• rise in bilirubin, decreased haptoglobin
and confirmed by a positive direct antiglobulin test (DAT) and positive cross-match not detectable pre-transfusion
2. Acute non-ABO haemolytic transfusion reaction
Haemolytic transfusion reaction (not due to ABO incompatibility) occurring within 24 hours of a transfusion
(See features above)
3. Delayed haemolytic transfusion reaction
Haemolytic transfusion reaction occurring 24 hours to 28 days after the transfusion
(See features above)
4. Transfusion-related acute lung injury
Occurrence of acute respiratory distress and bilateral pulmonary infiltrates on CXR with no evidence of circulatory overload or other potential cause within six hours of transfusion of a blood component or plasma component
5. Transfusion-transmitted infection
A post-transfusion infection (viral (TTVI), bacterial (TTBI) or parasitic (TTPI)) not present in the recipient before transfusion of a blood component or plasma component and present in either one of the components transfused or the donor of one of the transfused components. TTBI includes:
Bacterial contamination of blood product — detection and confirmation of bacteria in a blood component or plasma component, which has either not been transfused to the intended patient or was transfused, but no bacteria was detected in cultures of the recipient’s blood
6. Severe allergic reaction One or more of rash, dyspnoea (stridor, cyanosis, wheezing), angioedema, generalised pruritus and/or urticaria, without hypertension during or within 24 hours of a transfusion of a blood component or a plasma component that requires pharmacological treatment
7. Anaphylaxis/anaphylactoid reaction
Allergic reaction (one or more of rash, wheezing, dyspnoea, stridor, angioedema, generalised pruritus and/or urticaria) with hypotension (drop in systolic blood pressure of equal to or more than 30 mmHg) during or within 24 hours of a transfusion of a blood component or plasma component
8. Transfusion-associated graft-versus-host disease
Development of symptoms and signs (fever, erythematous skin rash, hepatic dysfunction, diarrhoea and bone marrow hypoplasia/pancytopenia) 1–6 weeks following transfusion with no other apparent cause — the diagnosis is confirmed by skin and/or bone marrow biopsy appearances and/or the demonstration of genetic chimerism in the recipient’s peripheral blood lymphocytes
9. Post-transfusion purpura
An acute episode of thrombocytopenia occurring within 12 days of a transfusion (red cells or plasma) and confirmed by the presence of platelet-specific alloantibodies (usually anti-HPA1a) in recipient’s blood and presence of antithetical antigen on donor platelets or by positive platelet cross-match
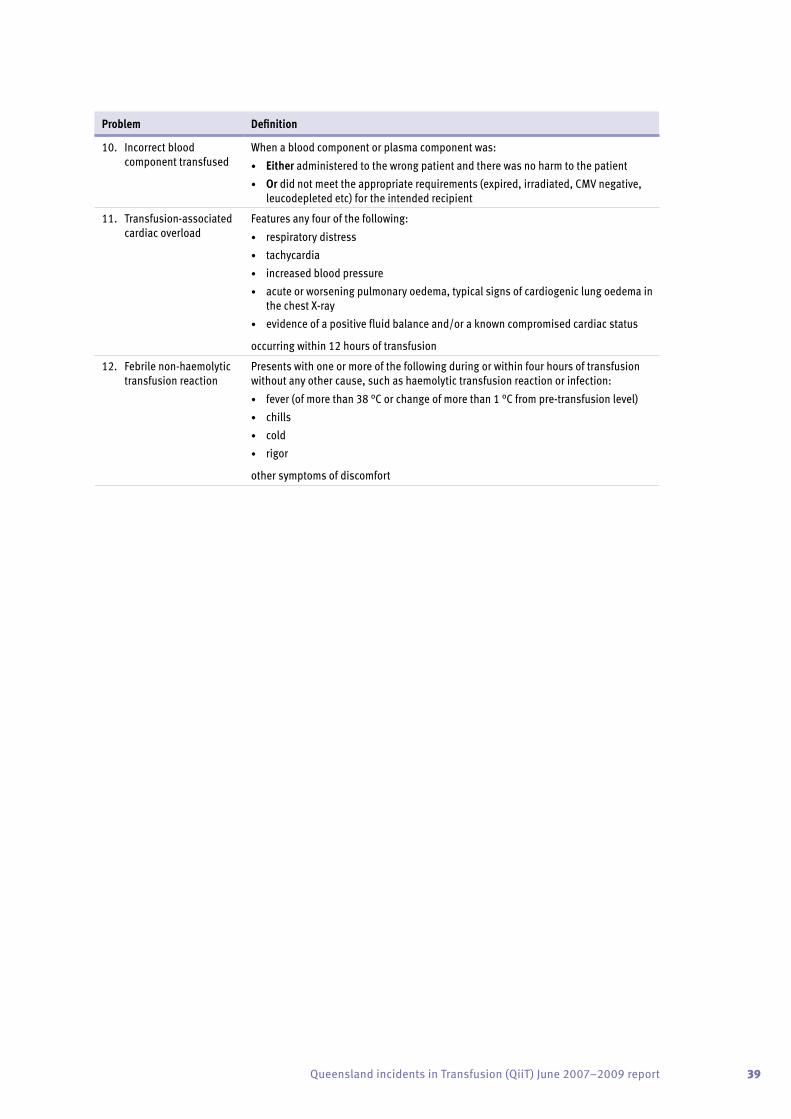
39Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Problem Definition
10. Incorrect blood component transfused
When a blood component or plasma component was:• Either administered to the wrong patient and there was no harm to the patient• Or did not meet the appropriate requirements (expired, irradiated, CMV negative,
leucodepleted etc) for the intended recipient
11. Transfusion-associated cardiac overload
Features any four of the following:• respiratory distress• tachycardia• increased blood pressure• acute or worsening pulmonary oedema, typical signs of cardiogenic lung oedema in
the chest X-ray• evidence of a positive fluid balance and/or a known compromised cardiac status
occurring within 12 hours of transfusion
12. Febrile non-haemolytic transfusion reaction
Presents with one or more of the following during or within four hours of transfusion without any other cause, such as haemolytic transfusion reaction or infection:• fever (of more than 38 °C or change of more than 1 °C from pre-transfusion level)• chills• cold• rigor
other symptoms of discomfort
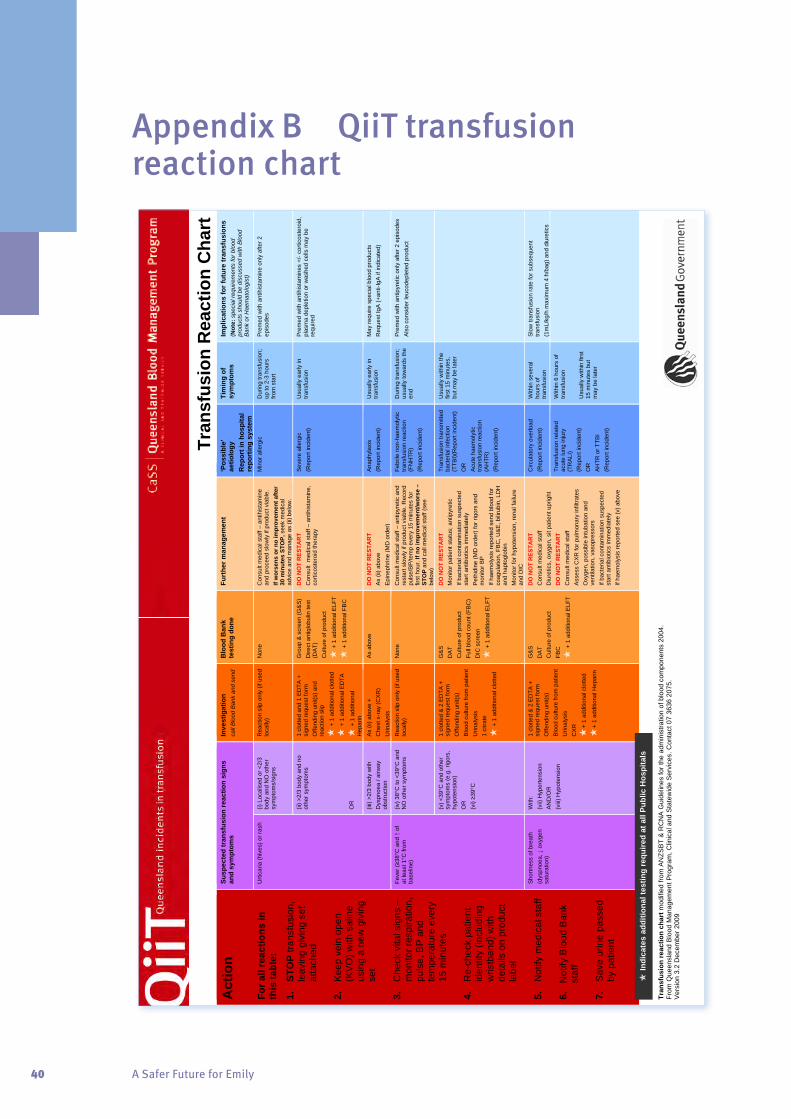
40 A Safer Future for Emily
Appendix B QiiT transfusion reaction chart
Tran
sfus
ion
reac
tion
char
t mod
ified
from
AN
ZSB
T &
RC
NA
Gui
delin
es fo
r the
adm
inis
tratio
n of
blo
od c
ompo
nent
s 20
04.
From
Que
ensl
and
Blo
od M
anag
emen
t Pro
gram
, Clin
ical
and
Sta
tew
ide
Ser
vice
s. C
onta
ct 0
7 36
36 2
075.
V
ersi
on 3
.2 D
ecem
ber 2
009
Act
ion
For a
ll re
actio
ns in
th
is ta
ble:
1.
STO
P tra
nsfu
sion
, le
avin
g gi
ving
set
at
tach
ed
2.
Kee
p ve
in o
pen
(KV
O) w
ith s
alin
e us
ing
a ne
w g
ivin
g se
t 3.
C
heck
vita
l sig
ns –
m
onito
r res
pira
tion,
pu
lse,
BP
and
te
mpe
ratu
re e
very
15
min
utes
4.
R
e-ch
eck
patie
nt
iden
tity
(incl
udin
g w
ristb
and)
with
de
tails
on
prod
uct
labe
l 5.
N
otify
med
ical
sta
ff 6.
N
otify
Blo
od B
ank
staf
f 7.
S
ave
urin
e pa
ssed
by
pat
ient
Susp
ecte
d tr
ansf
usio
n re
actio
n si
gns
and
sym
ptom
s In
vest
igat
ion
call
Blo
od B
ank
and
send
B
lood
Ban
k te
stin
g do
ne
Furt
her m
anag
emen
t ‘P
ossi
ble’
ae
tiolo
gy
Rep
ort i
n ho
spita
l re
port
ing
syst
em
Tim
ing
of
sym
ptom
s Im
plic
atio
ns fo
r fut
ure
tran
sfus
ions
(N
ote:
spe
cial
requ
irem
ents
for b
lood
pr
oduc
ts s
houl
d be
dis
cuss
ed w
ith B
lood
B
ank
or H
aem
atol
ogis
t)
Urti
caria
(hiv
es) o
r ras
h (i)
Loc
alis
ed o
r <2/
3 bo
dy a
nd N
O o
ther
sy
mpt
oms/
sign
s
Rea
ctio
n sl
ip o
nly
(if u
sed
loca
lly)
Non
e C
onsu
lt m
edic
al s
taff
– an
tihis
tam
ine
and
proc
eed
slow
ly if
pro
duct
via
ble.
If
wor
sens
or n
o im
prov
emen
t afte
r 30
min
utes
STO
P, s
eek
med
ical
ad
vice
and
man
age
as (i
i) be
low
.
Min
or a
llerg
ic
Dur
ing
trans
fusi
on;
up to
2-3
hou
rs
from
sta
rt
Pre
med
with
ant
ihis
tam
ine
only
afte
r 2
epis
odes
(ii) >
2/3
body
and
no
othe
r sym
ptom
s O
R
1 cl
otte
d an
d 1
ED
TA +
si
gned
requ
est f
orm
O
ffend
ing
unit(
s) a
nd
reac
tion
slip
+
1 a
dditi
onal
clo
tted
+
1 a
dditi
onal
ED
TA
+
1 a
dditi
onal
H
epar
in
Gro
up &
scr
een
(G&
S)
Dire
ct a
ntig
lobu
lin te
st
(DA
T)
Cul
ture
of p
rodu
ct
+
1 a
dditi
onal
ELF
T
+
1 a
dditi
onal
FB
C
DO
NO
T R
ESTA
RT
Con
sult
med
ical
sta
ff –
antih
ista
min
e,
corti
cost
eroi
d th
erap
y
Sev
ere
alle
rgic
(R
epor
t inc
iden
t) U
sual
ly e
arly
in
trans
fusi
on
Pre
med
with
ant
ihis
tam
ines
+/-
corti
cost
eroi
d,
plas
ma
depl
etio
n or
was
hed
cells
may
be
requ
ired
(iii)
>2/3
bod
y w
ith
Dys
pnoe
a / a
irway
ob
stru
ctio
n
As
(ii) a
bove
+
Che
st x
-ray
(CX
R)
Urin
alys
is
As
abov
e D
O N
OT
RES
TAR
T A
s (ii
) abo
ve
Epi
neph
rine
(MD
ord
er)
Ana
phyl
axis
(R
epor
t inc
iden
t) U
sual
ly e
arly
in
trans
fusi
on
May
requ
ire s
peci
al b
lood
pro
duct
s R
eque
st Ig
A (+
anti-
IgA
if in
dica
ted)
Feve
r (≥3
8°C
and
↑ o
f at
leas
t 1°C
from
ba
selin
e)
(iv) 3
8°C
to <
39°C
and
N
O o
ther
sym
ptom
s R
eact
ion
slip
onl
y (if
use
d lo
cally
) N
one
Con
sult
med
ical
sta
ff –
antip
yret
ic a
nd
rest
art s
low
ly if
pro
duct
via
ble.
Rec
ord
puls
e/B
P/te
mp
ever
y 15
min
utes
for
first
hou
r. If
no im
prov
emen
t/wor
se –
ST
OP
and
call
med
ical
sta
ff (s
ee
belo
w)
Febr
ile n
on-h
aem
olyt
ic
trans
fusi
on re
actio
n (F
NH
TR)
(Rep
ort i
ncid
ent)
Dur
ing
trans
fusi
on;
usua
lly to
war
ds th
e en
d
Pre
med
with
ant
ipyr
etic
onl
y af
ter 2
epi
sode
s A
lso
cons
ider
leuc
odep
lete
d pr
oduc
t
(v) <
39°C
and
oth
er
sym
ptom
s (e
.g. r
igor
s,
hypo
tens
ion)
O
R
(vi) ≥3
9°C
1 cl
otte
d &
2 E
DTA
+
sign
ed re
ques
t for
m
Offe
ndin
g un
it(s)
B
lood
cul
ture
from
pat
ient
U
rinal
ysis
1
citra
te
+
1 a
dditi
onal
clo
tted
G&
S
DA
T C
ultu
re o
f pro
duct
Fu
ll bl
ood
coun
t (FB
C)
DIC
scr
een
+
1 a
dditi
onal
ELF
T
DO
NO
T R
ESTA
RT
Mon
itor p
atie
nt s
tatu
s; a
ntip
yret
ic
If ba
cter
ial c
onta
min
atio
n su
spec
ted
star
t ant
ibio
tics
imm
edia
tely
P
ethi
dine
(MD
ord
er) f
or ri
gors
and
m
onito
r BP
If
haem
olys
is re
porte
d se
nd b
lood
for
coag
ulat
ion,
FB
C, U
&E
, bili
rubi
n, L
DH
an
d ha
ptog
lobi
n M
onito
r for
hyp
oten
sion
, ren
al fa
ilure
an
d D
IC
Tran
sfus
ion
trans
mitt
ed
bact
eria
l inf
ectio
n (T
TBI)(
Rep
ort i
ncid
ent)
OR
A
cute
hae
mol
ytic
tra
nsfu
sion
reac
tion
(AH
TR)
(Rep
ort i
ncid
ent)
Usu
ally
with
in th
e fir
st 1
5 m
inut
es,
but m
ay b
e la
ter
Sho
rtnes
s of
bre
ath
(dys
pnoe
a, ↓
oxy
gen
satu
ratio
n)
With
: (v
ii) H
yper
tens
ion
AN
D/O
R
(viii
) Hyp
oten
sion
1 cl
otte
d &
2 E
DTA
+
sign
ed re
ques
t for
m
Offe
ndin
g un
it(s)
B
lood
cul
ture
from
pat
ient
U
rinal
ysis
C
XR
+ 1
addi
tiona
l clo
tted
+
1 ad
ditio
nal H
epar
in
G&
S
DA
T C
ultu
re o
f pro
duct
FB
C
+
1 a
dditi
onal
ELF
T
DO
NO
T R
ESTA
RT
Con
sult
med
ical
sta
ff D
iure
tics,
oxy
gen,
sit
patie
nt u
prig
ht
DO
NO
T R
ESTA
RT
Con
sult
med
ical
sta
ff A
sses
s C
XR
for p
ulm
onar
y in
filtra
tes
Oxy
gen,
pos
sibl
e in
tuba
tion
and
vent
ilatio
n, v
asop
ress
ors
If ba
cter
ial c
onta
min
atio
n su
spec
ted
star
t ant
ibio
tics
imm
edia
tely
If
haem
olys
is re
porte
d se
e (v
) abo
ve
Circ
ulat
ory
over
load
(R
epor
t inc
iden
t) W
ithin
sev
eral
ho
urs
of
trans
fusi
on
Slo
w tr
ansf
usio
n ra
te fo
r sub
sequ
ent
trans
fusi
on
(1m
L/kg
/h m
axim
um 4
h/b
ag) a
nd d
iure
tics
Tran
sfus
ion
rela
ted
acut
e lu
ng in
jury
(T
RA
LI)
(Rep
ort i
ncid
ent)
OR
A
HTR
or T
TBI
(Rep
ort i
ncid
ent)
With
in 6
hou
rs o
f tra
nsfu
sion
U
sual
ly w
ithin
firs
t 15
min
utes
but
m
ay b
e la
ter
Tr
ansf
usio
n R
eact
ion
Cha
rt
In
dica
tes
addi
tiona
l tes
ting
requ
ired
at a
ll Pu
blic
Hos
pita
ls

41Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Appendix C TRALI – information for medical officers
Dear Colleague, Re: Transfusion related acute lung injury (TRALI) TRALI is the leading cause of death related to transfusion of blood and blood components, and I am writing to you to:
1. help increase awareness of this potentially fatal complication of transfusion, which is often overlooked in patients developing respiratory problems post-transfusion,
2. emphasise that reducing inappropriate use of blood and blood components is an essential measure in reducing the occurrence of TRALI and preventing deaths due to this complication, and
3. ensure that you are aware of the need to report cases to the ARCBS for investigation (via your hospital Blood Bank) to identify implicated donors as a method to reduce the incidence of TRALI.
Background TRALI is a significant cause of mortality and morbidity in patients who receive blood products, particularly plasma-containing products. If TRALI is not recognised and treated appropriately, it can frequently result in death. Despite the growing recognition of TRALI it is clear that TRALI is often misdiagnosed or overlooked. For example, data from the Queensland Health incident reporting system (PRIME) show that no cases of TRALI were reported during the 12 months to December 2007. Given that in Queensland, approximately 250,000 units of blood products are transfused each year, a conservative estimate for the expected number of reports of TRALI in QH hospitals would be 12 cases per year. Data from the US Food and Drugs Administration (FDA) for 2005 and 2006 show that of all transfusion related fatalities reported to the FDA, TRALI was the leading cause of death, accounting for 56% of transfusion related deaths. The exact frequency of TRALI is not known, but international haemovigilance systems have demonstrated increased numbers of cases reported as clinicians become more aware of this potentially lethal complication.

42 A Safer Future for Emily
.
2
Estimates of the incidents of TRALI are 1 in 1000 to 1 in 5000 units transfused, and the mortality rate is between 5% and 25%. Once recent study of critically ill patients demonstrated 8% of patients developed acute lung injury with 6 hours of transfusion (1). Why is it important to recognise TRALI? As dyspnoea after a transfusion is often believed to be due to another cause, e.g. circulatory overload, allergic reaction etc., or because there are other risk factors present for acute lung injury, TRALI is often overlooked. Criteria for the clinical diagnosis of TRALI (see attached) have been published (2). Typical clinical features are hypoxaemia, hypotension, fever and severe bilateral pulmonary infiltrates within 6 hours of completing a transfusion. Early recognition allows the transfusion to be stopped immediately and commencement of oxygen and supportive therapy. As the underlying pathology involves microvascular injury, use of diuretics may be detrimental and some patients benefit from fluid administration. Recognising TRALI allows notification of the Australian Red Cross Blood Service (ARCBS) and testing of the blood component and/or donor for anti-HLA and anti-granulocyte antibodies. Donors of blood products implicated in cases of TRALI often contain anti-leukocyte allo-antibodies (anti-HLA and anti-granulocyte) that are thought to be important in the pathogenesis of TRALI in a significant number of cases. Recognition of these donors by the ARCBS allows appropriate exclusion of implicated blood products. What can you do?
• Reduce the exposure of patients to fresh frozen plasma, platelets and red cells by ensuring appropriate use of blood products. All blood products used should be prescribed in accordance with the National Health and Medical Research Council (NHRMC) national guidelines.
• Ensure clinical colleagues are aware of TRALI, as a complication of transfusing fresh blood products, e.g. fresh frozen plasma, cryoprecipitate, platelets and red cells.
• Notify your blood bank if TRALI is clinically suspected, so that testing of the blood component and/or donor can be arranged through ARCBS.
• Notify cases of TRALI to the Queensland haemovigilance system (Queensland incidents in Transfusion – QiiT) via your hospital clinical incident reporting system.
The ARCBS has introduced a minimisation strategy that aims to increase to the proportion of clinical fresh frozen plasma (FFP) that is sourced only from male donors (who have lower incidence of anti-leukocyte antibodies). Currently, the ARCBS has been able to collect 90% of all clinical FFP from male donors. This will help reduce the likelihood of TRALI. Other strategies identified as reducing the risk of TRALI, e.g. use of solvent detergent treated FFP, are not currently available in Australia.
43Queensland incidents in Transfusion (QiiT) June 2007–2009 report
3
However, ensuring appropriate use of fresh blood products will form an important part of avoiding patient’s exposure to unnecessary transfusions (3,4) and can be effected through local governance of transfusion practice. Yours sincerely, Dr Simon A Brown Clinical Advisor Queensland Blood Management Program On behalf of Queensland Blood Advisory Council 07/04/2009 References
1. Gajic O et al. Am J Resp Crit Care Med 2007, 176; 886-891. 2. Kleinmann S et al. Transfusion 2004, 44; 1774-1789. 3. Rubin GL et al. Med J Aust 2001, 175; 354-358. 4. Schonfield WN et al. Med J Aust 2003, 178; 117-121.

44 A Safer Future for Emily
Transfusion related acute lung injury (TRALI) 1. Recommended criteria for TRALI and possible TRALI
a) Criteria for TRALI
(i) Acute lung injury (ALI)* (ii) No pre-existing ALI* before transfusion (iii) During or within 6 hours of transfusion (iv) No temporal relationship to other risk factor for ALI
b) Possible TRALI
(i) ALI* (ii) No pre-existing ALI* before transfusion (iii) During or within 6 hours of transfusion (iv) Temporal relationship to other risk factor for ALI
* Acute lung injury (ALI) – definition of ALI:
1. Acute onset 2. Hypoxia – oxygen saturation <90% on air measured by pulse oximetry
or other clinical evidence of hypoxaemia 3. Bilateral infiltrates on chest X-ray 4. No evidence of circulatory overload (left atrial hypertension)
2. Comparison of features of TRALI and transfusion associated cardiac overload
Feature TRALI Overload Body temperature Blood pressure Neck veins Ejection fraction PA occlusion pressure Fluid balance Response to diuretic WBC
Can be raised Hypotension Unchanged Normal, decreased ≤ 18mmHg Any Minimal Transient reduction
Unchanged Hypertension Can be distended Decreased > 18 mmHg Positive Significant Unchanged
Adapted from: Skeate & Eastlund. Curr Opin Hematol 2007, 14: 682-687; Kleinman et al. Transfusion 2004, 44: 1774-1789.

45Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Appendix D QiiT process (extract from pilot project)The QiiT haemovigilance system DOES NOT replace the existing hospital incident reporting system. QiiT works in conjunction with the existing hospital incident-reporting system.
Figure 2.2 describes the process of reporting a transfusion incident through QiiT. The QiiT process is based on established procedures for incident-reporting and is operated by the QiiT staff at the Queensland Blood Management Program (QBMP).
Figure 2.2 QiiT process of incident-reporting and analysis
The medical, nursing or hospital staff who responded to the transfusion incident, report the incident according to the local hospital procedures. Systems within the hospital initiate (i) a local systems analysis of the incident and (ii) the QiiT process. In the public sector, the QiiT process initiates automatically through an electronic feed from PRIME to the QiiT staff. In the private sector, the hospital’s haemovigilance coordinator contacts the QiiT staff by mail, phone or email.
The QiiT staff at the QBMP log the incident and provide the hospital’s haemovigilance coordinator with the appropriate follow up form. The haemovigilance coordinator facilitates the local haemovigilance follow-up activities and then returns the completed form to the QiiT staff for further analysis at a state and national level.
QBMP QiiT ProgramParticipating Facility
incident
immediate action
local haemovigilance coordinator receives and facilitates completion
of the follow up form
incident reported incident notified to QiiT staff at QBMP
initial data entered into QiiT database
incident assigned unique QiiT number
QiiT incident feedback indicating final assessment of incident is
sent to facility
QiiT report distributed to stakeholders
follow up form entered into QiiT database
QiiT team performs incident analysis and validation of incident with assistance from QiiT working
group as required
QiiT team prepares QiiT report biennially

46 A Safer Future for Emily
Appendix E RRMA classification
Department of Health and Ageing
RRMA 1 Capital cities
RRMA 2 Other metropolitan centres (urban centre population of more than 100 000)
RRMA 3 Large rural centres (urban centre population 25 000 to 99 000)
RRMA 4 Small rural centre (urban centre population 10 000 to 24 999)
RRMA 5 Other rural centres (urban centre population of fewer than 10 000)
RRMA 6 Remote centres (urban centre population of more than 4999)
RRMA 7 Other remote centres (urban centre population of fewer than 5000)

47Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Appendix F Imputability and severity scoresSeverity scores
Grade 0 no effect; absence of clinical signs
Grade 1 absence of immediate or long-term vital threat
Grade 2 long-term morbidity
Grade 3 immediate vital
Grade 4 death
Imputability scores
Level 0 excluded
Level 1 unlikely
Level 2 possible
Level 3 likely/probable
Level 4 certain
N/A not assessable

48 A Safer Future for Emily
Appendix G Blood Products Advisory Committee information developed for IMP notifications
June 2009
Dear Doctor,
Clinician Advisory — Bacterial Contamination Screening
You have been alerted that a unit of platelets transfused to your patient is potentially contaminated with bacteria (initial machine positive (IMP) notification). In May 2008, the ARCBS commenced bacterial screening of platelet products to decrease the incidence of transfusion of contaminated units.
Recommendations
• The clinical condition of the patient should be urgently appraised. This might involve delegation of a clinician to urgently review inpatients or rapid contact with outpatients to ascertain whether they have symptoms suggesting sepsis.
• Asymptomatic patients should then be followed up at their next routine review, but told to report for urgent medical review should they develop fever or other symptoms suggesting sepsis.
• Patients with symptoms or signs suggesting possible bacterial sepsis should be managed urgently with blood cultures and other septic screens as clinically indicated and rapid initiation of broad spectrum intravenous antibiotics (e.g. in neutropenic patients ticarcillin/clavulanate plus gentamicin, in non neutropenic patients ticarcillin/clavulanate, If penicillin allergic an alternative such as vancomycin plus gentamicin or ceftazidime should be considered).
Please note: Currently, about 75 per cent IMP notifications will be found to be false positive (no bacteria confirmed).
In the initial six months of bacterial screening (April to October 2008), Australian Red Cross ARCBS (ARCBS) tested 60,868 platelet components. Of these, 732 (1.2 per cent) were IMP, with 72 (0.11 per cent) confirmed to be positive, with organism identification.
Causes of bacterial contamination*
The most common organisms cultured in bacterial screening of platelets in Australia in order of frequency were: Propionibacterium (73.1 per cent), Staphylococcus (11.1 per cent), Corynebacterium (6.5 per cent), Micrococcus (2.8 per cent), Streptococcus (2.8 per cent), Klebsiella (1.9 per cent) and Ralstonia (0.9 per cent). The largest group, Propionibacterium, only grows in anaerobic media, with a mean time to detection of 101 hours after incubation. This organism is generally regarded as clinically insignificant. The mean time to detection of all other organisms was 42 hours in aerobic, and 61 hours in anaerobic culture. This means that 45 per cent of platelet units which are confirmed to be contaminated or indeterminate can be withdrawn from inventory before transfusion.
Subsequent notification of the veracity of the result, with Gram stain, identification and sensitivities will be provided.

49Queensland incidents in Transfusion (QiiT) June 2007–2009 report
Bacterial contamination usually occurs at venipuncture, with the most common organisms being skin commensals. Less commonly, donors might have been bacteraemic or less commonly again, bacteria might have been introduced during product handling.
For further assistance and advice, please contact:
• Your local haematologist
• Your local infectious diseases physician
• ARCBS transfusion medicine specialist 07 3838 9234 (office hours) or 07 3838 9010 (after hours)
*Reference for all data quoted in this document: Finding the bugs in platelets: bacterial contamination screening in Australia 2009, Presentation from ISBT ARCBS, Melbourne Victoria. P Hetzel, S Winzar, J Derks, R Burfoot, T Johnson, P Mock, T Smith, S Ismay, P Rodgers. M Borosak
50 A Safer Future for Emily
AbbreviationsANZSBT Australian and New Zealand Society of Blood Transfusion
ARCBS The Australian Red Cross Blood Service
BPAC Blood Products Advisory Committee
EU European Union
FNHTR febrile non-haemolytic transfusion reaction
HEAPS human error and patient safety
HTR haemolytic transfusion reaction
IMP initial machine positive
PRIME Queensland Health Clinical Incident Management Information System
RRMA Rural, Remote and Metropolitan Areas classification
SHOT Serious Hazards of Transfusion
TRALI transfusion-related acute lung injury
UK United Kingdom
QBMP Queensland Blood Management Program
QHEPS Queensland Health Electronic Publishing Service
QiiT Queensland incidents in Transfusion
51Queensland incidents in Transfusion (QiiT) June 2007–2009 report
References1. QBMP, PSC. Audit of the collection and administration of blood and blood products.
Queensland Health; October 2007.
2. Andreu G, Morel P, Forestier F, et al. Haemovigilance network in France: organization and analysis of immediate transfusion incident reports from 1994 to 1998. Transfusion. Oct 2002;42(10):1356-1364.
3. Stainsby D, Russell J, Cohen H, Lilleyman J. Reducing adverse events in blood transfusion. Br J Haematol. Oct 2005;131(1):8-12.
4. Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. 2005 May 3;142(9):756-64.
5. Aiello J, Thorp D, Davis K. Guidelines for the Administration of Blood Components. Australian & New Zealand Society of Blood Transfusion, Royal College of Nursing Australia; October 2004.
6. Cox P, Drys G. Directive 2002/98/EC setting standards of quality and safety for the collection, testing, processing, storage and distribution of human blood and blood components and amending Directive 2001/83/EC. 2003:p. 30.
7. Brien WF, Butler RJ, Inwood MJ. An audit of blood component therapy in a Canadian general teaching hospital. CMAJ. 1989;140(7):812-815.
8. Parker J, Thompson J, Stanworth S. A retrospective one-year single-centre survey of obstetric red cell transfusions. Int J Obstet Anesth. Oct 2009;18(4):309-313.
9. Schofield WN, Rubin GL, Dean MG. Appropriateness of platelet, fresh frozen plasma and cryoprecipitate transfusion in New South Wales public hospitals. Med J Aust. Feb 3 2003;178(3):117-121.
10. Schots J, Steenssens L. Blood usage review in a Belgian university hospital. Int J Qual Health Care. Mar 1994;6(1):41-45.
11. Tuckfield A, Haeusler MN, Grigg AP, Metz J. Reduction of inappropriate use of blood products by prospective monitoring of transfusion request forms. Med J Aust. Nov 3 1997;167(9):473-476.
12. Taylor CE, Cohen H, Mold D, et al. The 2008 Annual SHOT Report 2009.
13. QBMP. Final Report of the Queensland Incidents in Transfusion (QiiT) Haemovigilance Pilot Project May 2008.
14. NBA. Initial Australian Haemovigilance Report 2008: National Blood Authority Haemovigilance Project Working Group; January 2008.
15. Shortt J, Polizzotto MN, Waters N, et al. Assessment of the urgency and deferability of transfusion to inform emergency blood planning and triage: the Bloodhound prospective audit of red blood cell use. Transfusion. Nov 2009;49(11):2296-2303.
16. Wallis JP, Wells AW, Chapman CE. Changing indications for red cell transfusion from 2000 to 2004 in the North of England. Transfus Med. Dec 2006;16(6):411-417.
17. Stainsby D, Jones H, Wells AW, Gibson B, Cohen H. Adverse outcomes of blood transfusion in children: analysis of UK reports to the serious hazards of transfusion scheme 1996-2005. Br J Haematol. Apr 2008;141(1):73-79.

52 A Safer Future for Emily
18. Eder AF, Kennedy JM, Dy BA, et al. Bacterial screening of apheresis platelets and the residual risk of septic transfusion reactions: the American Red Cross experience (2004-2006). Transfusion. Jul 2007;47(7):1134-1142.
19. Koopman MM, van’t Ende E, Lieshout-Krikke R, Marcelis J, Smid WM, de Korte D. Bacterial screening of platelet concentrates: results of 2 years active surveillance of transfused positive cultured units released as negative to date. Vox Sang. Nov 2009;97(4):355-357.
20. Dike AE, Christie JM, Kurtz JB, Teo CG. Hepatitis C in blood transfusion recipients identified at the Oxford Blood Centre in the national HCV look-back programme. Transfus Med. Jun 1998;8(2):87-95.
21. Pawson R, Rajan S, Hazlehurst G, et al. Hepatitis C lookback programme: a single hospital experience. Transfus Med. Sep 1999;9(3):189-193.
22. Murphy MF. Application of bar code technology at the bedside: the Oxford experience. Transfusion. Aug 2007;47(2 Suppl):120S-124S; discussion 130S-131S.
23. Dzik WH, Murphy MF, Andreu G, et al. An international study of the performance of sample collection from patients. Vox Sang. Jul 2003;85(1):40-47.
24. Rebibo D, Hauser L, Slimani A, Herve P, Andreu G. The French Haemovigilance System: organization and results for 2003. Transfus Apher Sci. Oct 2004;31(2):145-153.
25. Stainsby D, Jones H, Asher D, et al. Serious hazards of transfusion: a decade of hemovigilance in the UK. Transfus Med Rev. Oct 2006;20(4):273-282.
26. Pagliaro P, Rebulla P. Transfusion recipient identification. Vox Sang. Aug 2006;91(2):97-101.
27. Chiu EK, Yuen KY, Lie AK, et al. A prospective study of symptomatic bacteremia following platelet transfusion and of its management. Transfusion. Nov-Dec 1994;34(11):950-954.
28. Oberman HA. Controversies in transfusion medicine: should a febrile transfusion response occasion the return of the blood component to the blood bank? Con. Transfusion. Apr 1994;34(4):353-355.
29. Widmann FK. Controversies in transfusion medicine: should a febrile transfusion response occasion the return of the blood component to the blood bank? Pro. Transfusion. Apr 1994;34(4):356-358.
30. Yazer MH, Podlosky L, Clarke G, Nahirniak SM. The effect of prestorage WBC reduction on the rates of febrile nonhemolytic transfusion reactions to platelet concentrates and RBC. Transfusion. Jan 2004;44(1):10-15.
31. Stephen CR, Martin RC, Bourgeois-Gavardin M. Antihistaminic drugs in treatment of nonhemolytic transfusion reactions. J Am Med Assoc. Jun 18 1955;158(7):525-529.
32. Gilstad CW. Anaphylactic transfusion reactions. Curr Opin Hematol. Nov 2003;10(6):419-423.
33. United States Food and Drug Administration. Topic II: Transfusion Related Acute Lung injury (TRALI). http://www.fda.gov/ohrms/dockets/AC/07/briefing/2007-4300B2_01.htm.
