a14.1 multi institutional approach_christie webster
DESCRIPTION
ÂTRANSCRIPT

A MULTI-INSTITUTIONAL APPROACH TO IMPROVING MATERNAL & FETAL HEALTH
Christie Webster, RNEC, OSFHT
Dr. Hazel Lynn, MD, GBHU
Dr. May Elhajj, MD, GBHS
1

CFPC Conflict of Interest
2
Presenter Disclosure Presenter: Christie Webster Relationships with commercial interests:
• Grants/Research Support: None • Speakers Bureau/Honoraria: None • Consulting Fees: None • Other: None
EXECUTIVE TRAINING FOR RESEARCH APPLICATION (EXTRA)
3
• Program offered by Canadian Foundation for Healthcare Improvement
• Vision: To build leaders in utilizing evidence to guide policy development & decision making in healthcare
• 14 month fellowship: team based • Intervention project
• To engage team in a change strategy • To utilize research based evidence • To focus on a specific issue

The Starting Point: Optimizing Maternal Fetal Health
Planned Pregnancy
Optimal Weight Gain
in Pregnancy
Eliminate Antenatal Smoking
Early Intervention
with Postpartum Depression
4
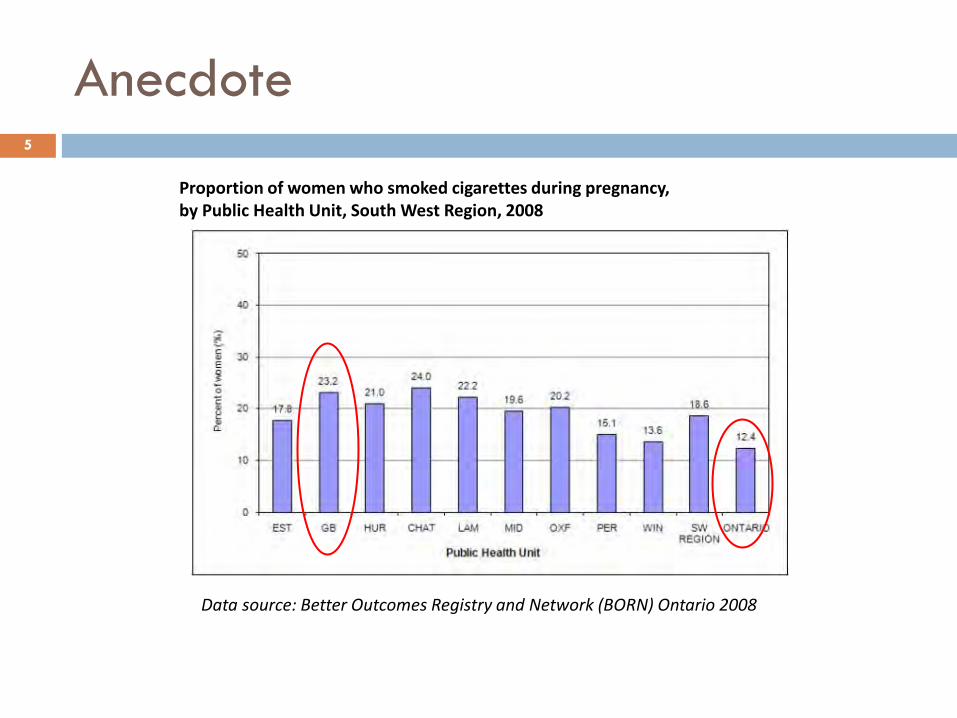
Anecdote
Proportion of women who smoked cigarettes during pregnancy, by Public Health Unit, South West Region, 2008
Data source: Better Outcomes Registry and Network (BORN) Ontario 2008
5
Rates of smoking during pregnancy increased with decreasing maternal age – 44.8% of mothers under
the age of 20 smoked during pregnancy, South West Region of Ontario
BORN, 2008
6

Context: Smoking Cessation
Services a population of 160,000; mandated to address the issue of smoking cessation related to population health with $350,000 of budget provided by smoke free Ontario program
Services 32,000 patients; trained clinical pharmacist & RN in smoking cessation counseling. Participating in Smoking Treatment for Ontario patients (STOP) program
Includes 6 hospitals that provide acute health care to Grey Bruce area. Owen Sound hospital is the only site that provides obstetrical care. Smoking cessation identified as a priority in strategic plan
7

Critical Summary of Evidence
ACOG and SOGC strongly endorse obstetricians being involved in smoking cessation programs
Economic evaluations of smoking cessation and relapse prevention programs for pregnant women: a systematic review. Ruger, et al. Value Health. 2008 Mar-Apr;11(2):180-90.
For every dollar invested in smoking cessation programs, $3 are saved in downstream health-related costs.
Interventions for promoting smoking cessation during pregnancy. Lumley J. et al. Cochrane Database of Systematic Reviews, 3, 2009.
Positive impact as far as pregnancy and fetus - less risk of complications
Neonatal care for infants born to smoking mothers: extra $700.
Adams et al: Health Econ 2002
8

Critical Summary of Evidence – cont’d
EMRs-potentially valuable component to support smoking cessation
Boyle R, Solberg L, Fiore M. Cochrane Database System Rev. 2011 Dec 7;(12):CD008743.
An office-based protocol that systematically identifies pregnant women who smoke and offers treatment or referral has been proved to increase quit rates.
Obstet Gynecol. 2010 Nov;116(5):1241-4
9
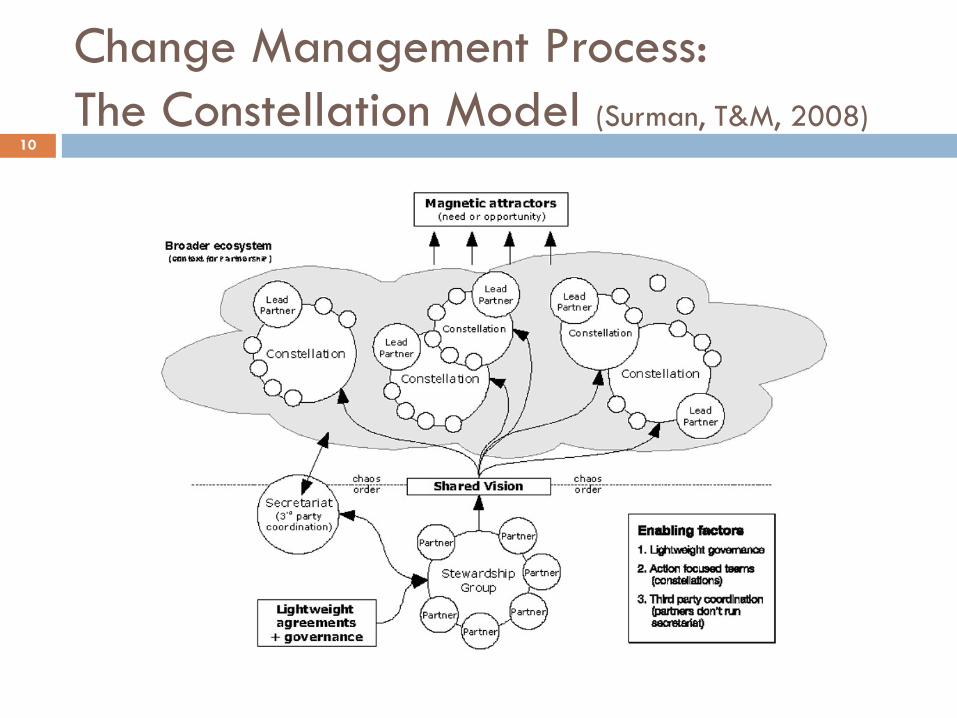
Change Management Process: The Constellation Model (Surman, T&M, 2008)
10

11
Need & Opportunity
Extra team: Vision & Plan
Constellations: Self
organizing action teams
Enabling Factors
Foundational agreement-EXTRA program No cost (our time) Collaborative partnerships Shared vision Feedback loops (stats, PHC providers, HCPs) Simple tools applied in practice
EMR Smoking status reminder EMR message for smoking cessation counseling Highlighted section in antenatal record#1
12

13
Smoking history is highlighted – if “yes” –refer for smoking cessation counseling

Barriers
Communication challenges Large geographic area of Grey Bruce Multiple HCPs with varying levels of
administrative support HCPs who lack skill in with dealing with a
younger population High rate of “No Show/No Response” to
smoking cessation counseling
14

Results: Provider Initiated Referrals to Smoking Cessation Counseling
15
TIME FRAME IDENTIFIED ANTENATAL SMOKERS ON EMR
# PROVIDER INITIATED REFERRALS
# NO SHOW &/OR NO RESPONSE
2010 0
2011 2
Jan - Aug 2012 ** 30 2 (6.7%)
Sept 2012 – Jan 2013
43 16 (37.2%) 7
Feb – March 2013 6 1 (16.7%)
April – Dec 2013 28 14 (50%) 8
Jan – April 2014 29 13 (44.8%) 4
**Pre EXTRA IP

Organizational Impact
Increased uptake of an available resource within an organization (smoking cessation counseling)
Heightened awareness of the problem Workshop “A Woman-Centered Approach to Tobacco Use &
Pregnancy”-June 2013 (GBHU)
Momentum for other organizations – role model Collaborative partnerships—beyond the project
Breaking down the silos
Focus on a Modifiable risk factor – smoking cessation Reduce duplication of work between institutions Health Links—identification of factors that make
pregnancy more expensive…reduce risk!
16
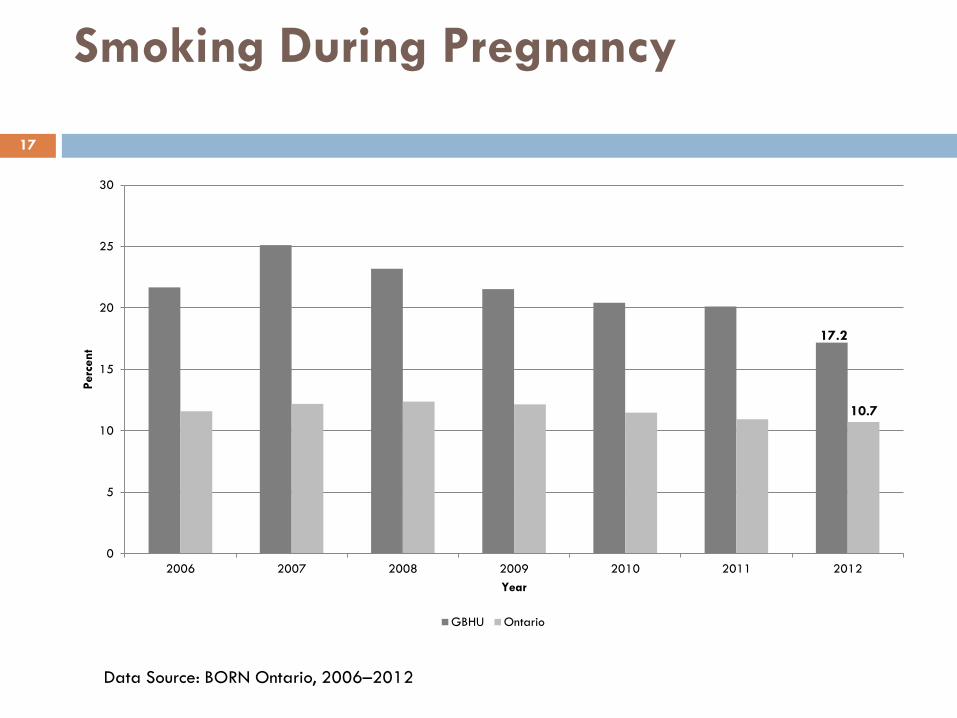
Smoking During Pregnancy
17
0
5
10
15
20
25
30
2006 2007 2008 2009 2010 2011 2012
Perc
ent
Year
GBHU Ontario
17.2
10.7
Data Source: BORN Ontario, 2006–2012
Sustainability
Feedback to MDs, HCPs (referral rates)- accountability No structural reorganization; no redesigning patterns of
delivery of care Patient focused - developed around the woman’s
preconception/pregnancy journey
18

Next Steps 19
Partnership with Keystone Child, Youth & Family Services, host to Healthy Beginnings (CPNC) sessions for teenage pregnant families Fall 2014 “lunch & learn” joint pilot project by OSFHT clinical pharmacist to
address stress mgmt & smoking cessation with interested clients (with or without partners); captive audience with food, transportation provided
3 sessions/year planned
Smoking cessation “swag” donated by GBHU
Host site application submitted to RNAO Best Practice Champions for Smoke-Free Pregnancies Workshop
If accepted, to be offered to OSFHT and community partners
Electronic pre/postnatal resource document-developing (OSFHT) Plan to educate HCPs on this resource
Questions? 20