abdominal aortic aneurysm complicated with chronic disseminated intravascular coagulopathy: a case...
TRANSCRIPT

CASE REPORTS
Abdominal aortic ancurysm complicated with chronic disseminated intravascular coagulopathy: A case of surgical treatment H i r o o Mukaiyama, M.D. , Shigehiko Shionoya, M.D. , Te ruo Ikezawa, M.D. , Tadashi Kamiya , M.D. , Mo toh i ro Hamaguch i , M.D. , and H ideh iko Saito, M.D. , Nagoya, Japan
This article reports a case of an infrarenal abdominal aortic aneurysm complicated with chronic disseminated intravascxtlar coagulopathy (DIC). The patient was a 68-year-old man; bleeding of 20 months' duration was reported. Physical examination indicated a pulsating mass in the abdomen. The diagnosis of DIC was made on the basis of standard coagulation studies. Indium 1 l l - labe led platelet scintigraphy demonstrated an increased accumulation of radioactivity over the aneurysm. After preoperative control of the bleed- ing tendency was obtained by continuous intravenous infusion of gabexate mesilate (FOY), the aneurysm was successfully replaced with a prosthetic graft. Gabexate mesilate therapy is useful for DIC as is heparin therapy. I f surgical intervention is required for an abdominal aortic aneurysm with concomitant DIC, preoperative control of bleeding with gabexate mesilate or heparin is recommended to lessen operative bleeding. ( J VAsc SUR~ 1987;6:600-4.)
Disseminated intravascular coagulopathy (DIC) may complicate several clinical entities, including sep- sis, carcinoma, burn, leukemia, and giant hemangi- oma. A variety of aneurysms have also been described as causing DIC since a f rs t report by Fine et al. ~ in 1967. However, a review o f the literature shows that D I C associated with abdominal aortic aneurysm is rare.
This article reports a case of D I C accompanying an asymptomatic abdominal aortic aneurysm. In- dium l 1 l - labeled platelet scintigraphy and the serial changes in coagulation-fibrinolysis parameters showed interesting results.
CASE REPORT A 68-year-old man was admitted to Nagoya University
Hospital in August 1985, for evaluation of a chronic bleed- ing disorder of approximately 20 months' duration.
In November 1983, he had a painful, spontaneous hemarthrosis of the left knee. In April 1985, he had an intramuscular hematoma without trauma, an ecchymosis
From the First Department of Surgery (Drs. Makaiyama, Shio- noya, and Ikezawa) and the First Department of Internal Med- icine (Drs. Kamiya, Hamaguchi, mad Saito), Nagoya Univer- sity, School of Medicine.
Reprint requests: Hiroo Mukaiyama, M.D., Division of Vascular Surgery, First Department of Surgery, Nagoya University, School of Medicine, 65 Tsuramai-cho, Showa-ku, Nagoya City, 466 Japan.
600
over the right upper extremity, and hematuria. He was admitted to a municipal hospital, where he was treated with gabexate mesilate and tranexamic acid, and dis- charged. In July 1985, ecchymoses reappeared over the left hand and the right leg.
On Aug. I, 1985, the patient was referred to Nagoya University Hospital for evaluation of a chronic hemor- rhagic diathesis. He had undergone subtotal gastrectomy to treat carcinoma without hemorrhagic complications 11 years before admission. No liver disease nor weight loss was reported.
On admission, the patient was afebrile and had a bloc: s pressure of 120/74 mm Hg and a pulse rate of 60 beats/rain. Physical examination showed ecchymoses over the left hand and the right leg, a pulsating mass m the abdomen, and a small ulcer on the lower lip.
Laboratory data showed the following values: hemo- globin, 11.2 gm/dl; platelet count, 49,000/ram ~, pro- thrombin time, 17.0 seconds, control, 15 2 seconds); ac- tivated partial thromboplastin time, 57.0 seconds (control, 44.2 seconds); fibrinogen, 80 mg/dl ~normal, 200 to 400 mg/dl); plasminogen activity, 66.4% (normal, 80% to 120%), and fibrin/fibrinogen degradation products (FDP), 10 to 40 t*g/ml ~normal, less than 10 ~g/ml). Antithrom- bin III activity was within normal limits (99.4%). Fibri- nopeptide A (FPA) in the plasma was 34.9 ng/ml (normal. 0.5 to 2.0 ng/ml), fibrinopeptide B~ Ls-~2 (FPBB ~s-42J was 35.8 ng/ml, normal, 0.7 to 4.8 ng/ml), and D-dimer was 5040 ng/ml tnormal, less than 150 ng/ml). Liver function values were normal.
From the hematologic abnormalities and clinical
Volume 6 Number 6 December 1987 Abdominal aortic aneurysm with chronic DIC 601
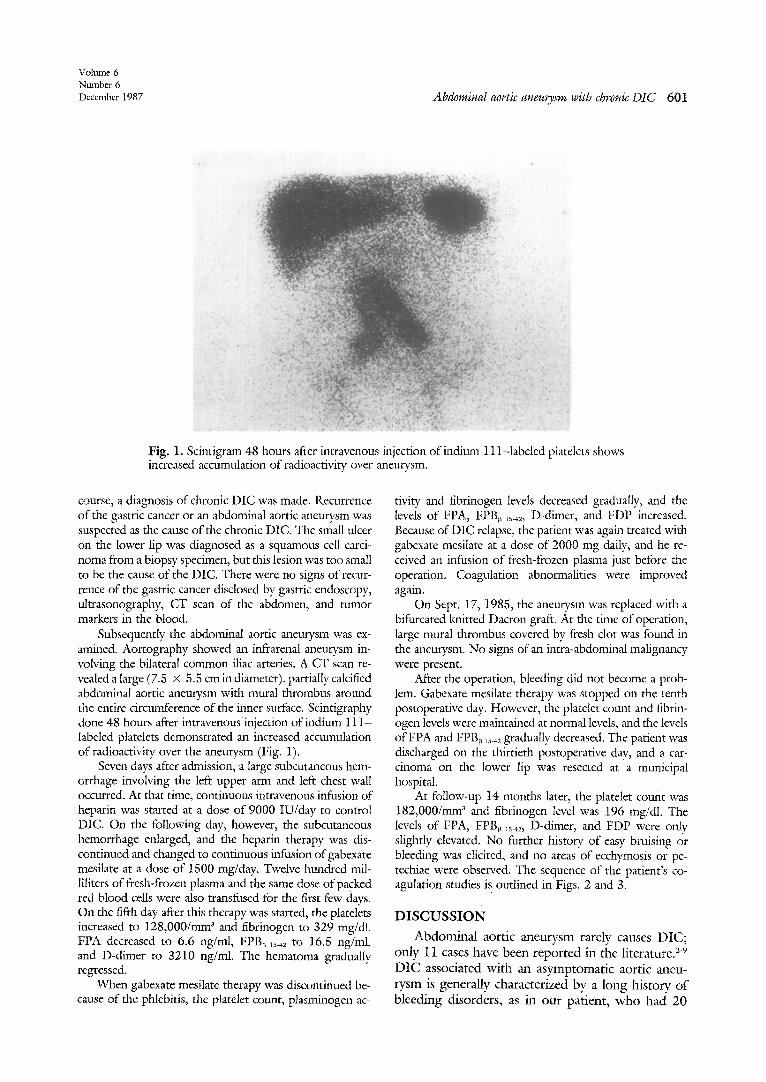
Fig. 1. Scintigram 48 hours after intravenous injection of indium 11 l-labeled platelets shows increased accumulation of radioactivity over aneuusm.
course, a diagnosis of chronic DIC was made. Recurrence of the gastric cancer or an abdominal aortic aneurysm was suspected as the cause of the chronic DIC. The small ulcer on the lower lip was diagnosed as a squamous cell carci- noma from a biopsy specimen, but this lesion was too small to be the cause of the DIC. There were no signs of recur- rence of the gastric cancer disclosed by gastric endoscopy, ultrasonography, CT scan of the abdomen, and tumor markers in the blood.
Subsequently the abdominal aortic aneurysm was ex- amined. Aortography showed an infrarenal aneurysm in- volving the bilateral common iliac arteries. A C T scan re- vealed a large (7.5 x 5.5 cm in diameter), partially calcified abdominal aortic aneurysm with mural thrombus around the entire circumference of the inner surface. Scintigraphy done 48 hours after intravenous injection of indium 11 I - labeled platelets demonstrated an increased accumulation of radioactivity over the aneurysm (Fig. 1).
Seven days after admission, a large subcutaneous hem- orrhage involving the left upper arm and left chest wall occurred. At that time, continuous intravenous infusion of heparin was started at a dose of 9000 IU/day to control DIC. On the following day, however, the subcutaneous hemorrhage enlarged, and the heparin therapy was dis- continued and changed to continuous infusion of gabexate mesilate at a dose of 1500 rag/day. Twelve hundred mil- liliters of fresh-frozen plasma and the same dose of packed red blood cells were also transfused for the first few days. On the fifth day after this therapy was started, the platelets increased to 128,000/mm 3 and fibrinogen to 329 mg/dl. FPA decreased to 6.6 ng/ml, FPB~ 15-,2 to 16.5 ng/ml, and D-dimer to 3210 ng/ml. The hematoma gradually regressed.
When gabexate mesilate therapy was discontinued be- cause of the phlebitis, the platelet count, plasminogen ac-
tivity and fibrinogen levels decreased gradually, and the levels of FPA, FPB~ ls-42, D-dimer, and FDP increased. Because of DIC relapse, the patient was again treated with gabexate mesilate at a dose of 2000 mg daily, and he re- ceived an infusion of fresh-frozen plasma just before the operation. Coagulation abnormalities were improved again.
On Sept. 17, 1985, the aneurysm was replaced with a bifurcated knitted Dacron graft. At the time of operation, large mural thrombus covered by fresh clot was found in the aneurysm. No signs of an intra-abdominal malignancy were present.
After the operation, bleeding did not become a prob- lem. Gabexate mesilate therapy was stopped on the tenth postoperative day. However, the platelet count and fibrin- ogen levels were maintained at normal levels, and the levels of FPA and FPB~ is-,2 gradually decreased. The patient was discharged on the thirtieth postoperative day, and a car- cinoma on the lower lip was resected at a municipal hospital.
At follow-up 14 months later, the platelet count was 182,000/mm 3 and fibrinogen level was 196 mg/dl. The levels of FPA, FPB~ is.42, D-dimer, and FDP were onty slightly elevated. No further history of easy bruising or bleeding was elicited, and no areas of ecchymosis or pe- techiae were observed. The sequence of the patient's co- agulation studies is outlined in Figs. 2 and 3.
DISCUSSION
Abdominal aortic aneurysm rarely causes D I C ; only 11 cases have been reported in the literature. 2-9 D I C associated with an asymptomatic aortic aaleu- rysm is generally characterized by a long history o f bleeding disorders, as in our patient, w h o had 20

602 Mukaiyama et al.
[oum£ o:-/" VASCULAR
SURGERY
Oate 8/211985 8/8 8/20 9/1 9/17 9/26 10/1 10/9 I'0/141~1/14/1986 Heparin ~]9o0o ,U/d op~ation
FOY [ '500,e/d I FOY[ "' 2000.~/d 11500m~d[ .,o_ Fibrinogen
Fibrinogen (meN) /o~......,._o,,.~ . ' ' ~
400. Fibrinogen
300 P'-~o
FDP 10-4010-40 <I0 I0-40 10-40 40< 40< I0-4040( 40< 10-40 10-40 10-40 10.40 (llg/ml)
Platelets (xlO4/cmm)
40
3O
20
10
0
Fig. 2. Serial coagulation studies show response of fibrinogen, FDP, antithrombin III, and platelet counts to gabexate rnesilate (FOY) therapy.
Date 8/211985 8/8 8/20 9/1 9/17 9/26 10/1 10/14 1111411986 ! , , ,
Heparin~9oo0 ig/e t . operation FOX I ,500.,/d fl FOY[.'.; 2000mg/d I 1500me/d [
FPA (n~/ml) I, s' \ FPB <5.42 (ng/ml) /,, \ 40
g~-'- - .~. ,," ~ FPBm5.4~ 30 " / \
-
\ \ / J
-x- - a~. . . . . ._ - - - -~ --- ,o , . ......... .-.x--
0
g.dimer (ng/~l)
-I0000
Fig. 3. Serial coagulation studies show response of FPA, FPB~ ls.42, and D-dimer to gabexate mesilate therapy.
months' duration of bleeding before admission. Sic- bert and Natelson 3 proposed four criteria for ac- cepting stable aortic aneurysms as the primary, etio- logic factors evoking DIC; they include (1) presence of a chronic acquired bleeding disorder, (2) labora- tory evidence of consumptive coagulopathy, (3) dis- appearance of the hemostatie defect after aneurysm repair, and (4) maintenance of normal coagulation for at least 3 months postoperatively. Our patient meets all these criteria.
The pathogenesis of DIC accompanying ancu- rysm has not been fully established. Straub and Kessler 1° injected 131I-labcled fibrinogcn and dem-
onstrated the accumulation of radioactivity, in an ab- dominal aortic aneurysm by surface scan. They also showed a large, radioactive fibrin mass within the electively resected aneurysm. Prentice, McNicol, and Douglas ~1 showed that the adhesion of platelets was greater to atheromatous areas of the aortic intima than to the normal aortic intima. In our case, indium i l l - labeled platelet scintigraphy showed an in- creased accumulation of radioactivity over the an- eurysm, and fresh clot was found in the aneurysm during the operation. Judging from these facts, we concluded that exposure of the subendothelial layer of the aortic wall and the relative stasis of blood

Volume 6 Number 6 December 1987 Abdominal aortic aneurysm with chronic DIC 603
within the aneurysm stimulate the deposition of fi- brin and adherence of platelets and result in intra- vascular coagulation and secondary fibrinolysis. In most cases, there appears to be a compensated state between the dynamic process of production and de- struction of platetets, fibrinogen, and other clotting factors. In a few cases, when an additional factor is present, such as hepatic disease or rapid aneurysm expansion, decompensation of this balance may oc- cur, leading to manifestation of DIC. Fisher, Yawn, and Crawford ~2 reported that the incidence rate of clinically manifested DIC with ecchymoses and pe- techiae is low (probably less than 5% of all patients with aortic aneurysms).
The cardinal laboratory signs of DIC are throm- bocytopenia and a quantitative or qualitative change in the plasma fibrinogen. The fibrinogen level is usu- ally decreased but may be in the normal range. The levels of FDP, FPA, FPB¢ ~5-42, and D-dimer are in- creased. An increased level of FPA reflects activation of the coagulation system, and increased levels of FDP, FPB¢ ~5-42, and D-dimer reflect secondary ac- tivation of the fibrinolytic system. In our patient, the levels ofFPA, FPB~ ~542, and D-dimer on admission were remarkably increased, indicating a hyperco- agulable and hyperfibrinolytic state. With gabexate mesilate therapy, these values promptly decreased. On the tenth day after discontinuation of the gabex- ate mesilate therapy, however, the levels of FPB~ x5-42 and D-dimer compared with FPA were remarkably elevated, indicating that activation offibrinolysis was predominant over activation of coagulation. When gabexate mesilate therapy was started again, the levels of FPB~ ls-42 and D-dimer gradually decreased but did not return to their normal ranges. At follow-up ~4 months later, the levels of FPA, FPB~ ~s-42, D-dimer, and FDP were still slightly elevated, probably because of activation of the coagulation- fibrinolysis system on the inner surface of the pros- thetic graft. Thus, FPA, FPB~ 15-42, and D-dimer are useful indices for assessing the efficacy of the treatment and for analyzing the changes in the coagulation-fibrinolysis system.
Gabexate mesilate is a synthetic protease inhibitor and has been used for the treatment of pancreatitis and DIC in Japan. A low dose of gabexate mesilate has inhibitory effects on plasma kallikrein, thrombin, C1 esterase, and trypsin, while a relatively high dose is required to inhibit plasmin and factor Xa. It in- hibits the activities of thrombin, plasmin, and fac- tor Xa without requiring antithrombin III. It has a small molecular weight of approximately 417 and is rapidly inactivated by plasma esterases (half-life of 70
to 80 seconds). For DIC therapy, it may be admin- istered by continuous intravenous infusion within a dose of 20 to 39 mg/kg over a 24-hour period in adults. High infusion speed or high concentration may produce pain and thrombophlebitis at the in- fusion site. Therefore central intravenous infusion is recommended. Hypersensitivity reaction (e.g., rash and itching, increased bleeding tendency, hypoten- sion, and nausea) is also occasionally seen. Shock is rare.
The definitive treatment for DIC is removal of the cause, that is, replacement of the aneurysm with a prosthetic graft in this setting. The infusion of ga- bexate mesilate may be of temporary benefit, but it will be useful as a preoperative treatment for DIC accompanying aneurysm as well as heparin therapy. In our patient, the infusion of gabexate mesilate at a dosc of 1500 to 2000 mg daily was beneficial for preoperative control of the bleeding disordcr. Ga- bexate mesilate therapy may be superior to heparin therapy, when activation of fibrinolysis is predomi- nant over activation of coagulation or when anti- thrombin III activity is low.
If surgical therapy is required for an abdominal aortic aneurysm with DIC, proper preoperative con- trol of the [bleeding disorder with gabexate mesilate ofheparin along with replacement of the blood com- poncnts is rccommended to lessen operative bleed- ing. Special care after the operation is also neccssary because DIC has occasionally been reported occur- ring after placement of a prosthetic graft 13~16 or the thromboexclusion method 17 for aortic aneurysm.
REFERENCES 1. Fine NL, Applebaum )', Elguezabal A, Castleman L. Multiple
coagulation defects in association with dissecting ancurysm. Arch Intern Med 1967;119:522-6.
2. Kazmier F, Didisheim P, Fairbanks VE, Ludwig l, Payne WS, Bowie JW. Intravascular coagulation an d arterial disease. Thrornb Diath Hacmorrh (Suppl) 1969;36!295-303.
3. Siebert WT, Natelson EA. Chronic consumption coagulop- athy accompanying abdominal aortic aneurysm. Arch Surg 1976;111:539-41.
4. Satiani B; Savrin R, Evans WE. Consumption coagulopathy associated with arterial aneurysms. J" Cardiovasc Surg 1979; 20:273-8.
5. Diskin C], Weitberg AB. Minidose heparin therapy: treat- ment of chronic intravascular coagulation syndrome. Arch Intern Med 1980;140:263-6.
6. Fouser LS, Morrow NE, Davis RB. Platelet dysfunction as- sociated with abdominal aortic aneurysm. Am J Clin Patho! 1980;74:701-5.
7. Keagy BA, Pharr WF, Bowes DE. Unusual presentations of abdominal aortic aneurysms. J Cardiovasc Surg 1981;22: 41-6.
604 Mukaiyama et al.
Yourn~ of VASCULAR
SURGERY
8. Goto H, Kimoto A, Kawaguchi H, et al. Surgical treatment of abdominal aortic aneurysm complicated with chronic dis- seminated intravascular coagulopathy. J Cardiovasc Surg 1985;26:280-2.
9. Thompson RW, Adams DH, Cohen JR, Mannick JA, Whitte- more AD. Disseminated intravascular coagulation caused by abdominal aortic aneurysm. J VAsc SURG 1986;4:186-9.
10. Straub PW, Kessler S. Umsatz und Lokalisation von mI- fibrinogen bei chronischer intravasaler Gerinntmg. Schweiz Med Wschr 1970;100:2001-3.
11. Prentice CRM, McNicol GP, Douglas AS. Effects on blood coagulation of normal and atheromatous aortic tissue. J Clin Pathol 1966;19:154-8.
12. Fisher DF, Yawn DH, Crawford ES. Preoperative dissemi- nated intravascular coagulation associated with aortic aneu- rysms: a prospective study of 76 cases. Arch Surg 1983;118: 1252-5,
13, Phillips LL. Alterations in ~e blood clotting system in dis:~i seminated intravascular coagulation. Am J Cardiol 1967;20: 174-84.
14. Mulcare RJ, Royster TS, Weiss HJ, Phillips LL. Disseminated intravascular coagulation as a complication of abdominal aor- tic aneurysm repair. Ann Surg I974;180:343-9.
15. Phillips LL, Mulcare RJ, Royster TS. Coagulation and ~bri- nolytic changes in aortic gra~ operations. Thromb Diath Hae- morrh 1975;34:587.
16. Collins GJ, Rich NR, Scialla S, Andersen CA, McDonald PT. Pitfalls in peripheral vascular surgery: disseminated intravas- cular coagulation. Am J Surg 1977;134:375-80.
17. Ishibe R, Morishita Y, Toyohira H, Saigenji H, Tabata F, Taira A. Disseminated intravascular coagulopathy associated with thromboexdusion for DeBakey III b dissecting aneu- rysm: a case report. Nippon Kyobu Geka Gakkai Zasshi 1985;33:1996-9.