accp cardiology prn journal club. announcements thank you attending the accp cardiology prn journal...
TRANSCRIPT

ACCP Cardiology PRN Journal Club

Announcements
• Thank you attending the ACCP Cardiology PRN Journal Club– Thank you if you attended last time
• Thank you for doing the survey after second journal club– Changes we made include:
• Only have 1 resident at time• Improve sound• Changed format with mentors• Offering recordings of the presentations
• Our summary article from first journal club will be up soon! I can e-mail if you would like a copy for now.

Spironolactone for Heart Failure with Preserved Ejection Fraction (TOPCAT)
Janna Beavers, PharmDPGY2 Cardiology Resident
WakeMed Health & HospitalsRaleigh, NC
Disclosure Statement
Janna Beavers has no conflicts of interest to disclose.

BackgroundHeart Failure
HF with reduced ejection fraction (HFrEF, EF≤40%)
Evidence-Based Treatment Options: Beta blockers, ACEis/ARBs,
Aldosterone Antagonists, Vasodilators, Diuretics (symptoms)
HF with preserved ejection fraction (HFpEF, EF>40%)
Evidence-Based Treatment Options: Diuretics (symptoms)
JACC; 2013:62(16):e147-239Eur Heart J 2012(33):1787-1847

Background
RAAS Activation
Angiotensin II increased release of aldosterone
Aldosterone: sodium/water retention, fibrosis, vascular inflammation, hypertrophy
JAMA 2013;300(8):781-797
Aldo-DHFNo change in
exercise capacity, symptoms, quality of
life
Improved LV diastolic function at 12
months

TOPCAT Study Objective
Determine whether treatment with spironolactone would improve clinical outcomes in patients with symptomatic heart failure with
preserved ejection fraction.
NEJM 2014;370:1383-1392
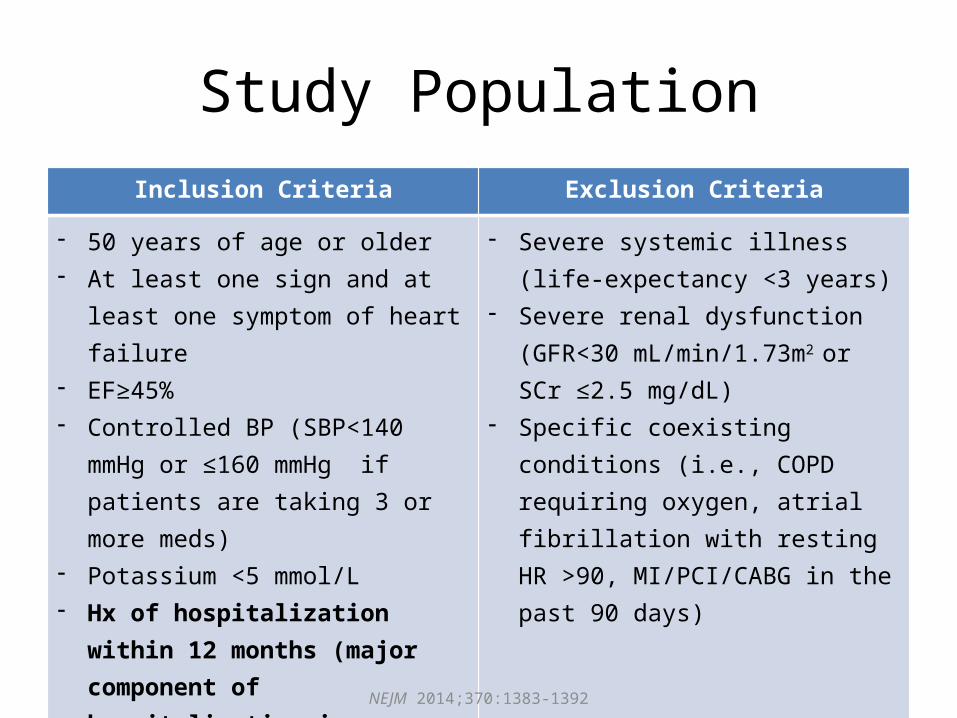
Study PopulationInclusion Criteria Exclusion Criteria
- 50 years of age or older- At least one sign and at least one
symptom of heart failure- EF≥45%- Controlled BP (SBP<140 mmHg or ≤160
mmHg if patients are taking 3 or more meds)
- Potassium <5 mmol/L- Hx of hospitalization within 12
months (major component of hospitalization is management of HF) OR elevated BNP within 60 days (BNP≥100 pg/mL or NT-proBNP≥360 pg/mL)
- Severe systemic illness (life-expectancy <3 years)
- Severe renal dysfunction (GFR<30 mL/min/1.73m2 or SCr ≤2.5 mg/dL)
- Specific coexisting conditions (i.e., COPD requiring oxygen, atrial fibrillation with resting HR >90, MI/PCI/CABG in the past 90 days)
NEJM 2014;370:1383-1392

Study Design• International, multi-center, double-blind, placebo-controlled,
randomized trial• Randomization
– Study Groups• Spironolactone 15 mg once daily (max 45 mg/day)• Placebo
– Stratification• Previous hospitalization or BNP elevation
• Patients received other heart failure medications throughout study
NEJM 2014;370:1383-1392
Medication Spironolactone Placebo
Diuretics 81.4% 82.3%
Beta blocker 84.3% 84.2%
ACEi or ARB 78.2% 77.3%

Outcomes
Primary Outcome• Composite – death from CV causes, aborted cardiac arrest,
hospitalization for management of HF
Secondary Outcomes• Death from any cause• Hospitalization for any cause• Hyperkalemia (K≥5.5 mmol/L) or hypokalemia (K<3.5 mmol/L)• Elevated SCr (≥2 times above the upper limit of normal OR SCr
≥3 mg/dL)
NEJM 2014;370:1383-1392
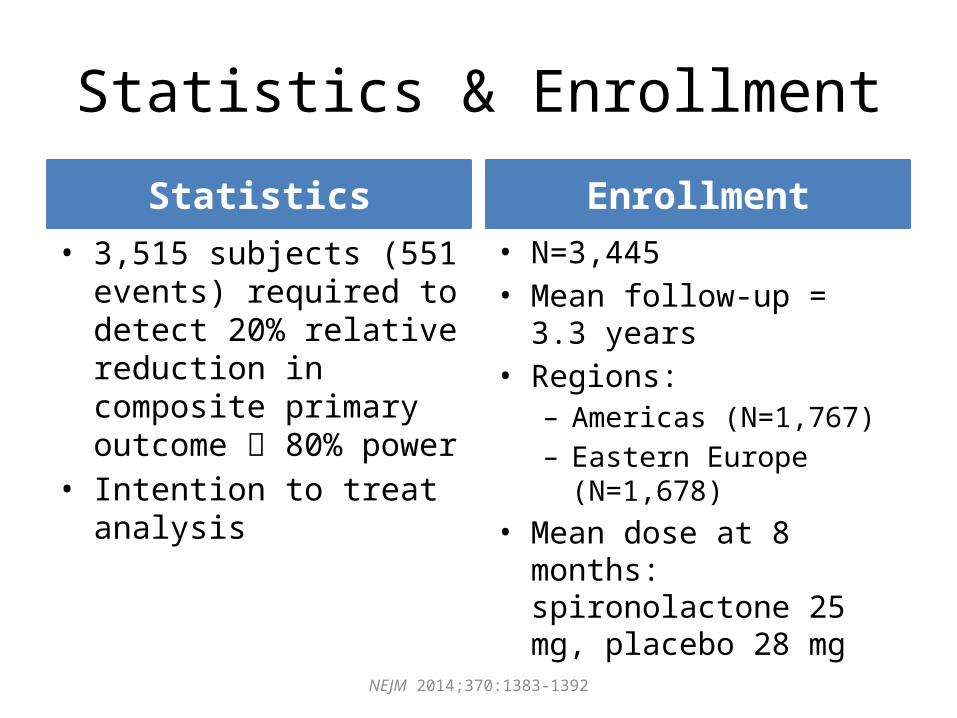
Statistics & Enrollment
Statistics• 3,515 subjects (551 events)
required to detect 20% relative reduction in composite primary outcome 80% power
• Intention to treat analysis
Enrollment• N=3,445• Mean follow-up = 3.3 years• Regions:
– Americas (N=1,767)– Eastern Europe (N=1,678)
• Mean dose at 8 months: spironolactone 25 mg, placebo 28 mg
NEJM 2014;370:1383-1392

Baseline Characteristics
Age 68.7 yrs (median)
~89% white race
NYHA II (~64%) & III (~33%)
Ejection fraction 56% (median)
SCr ~1 (median)
Eligibility based on hospitalization (71.5%) or elevated BNP (28.5%)
NEJM 2014;370:1383-1392

Outcomes
NEJM 2014;370:1383-1392

Subgroup AnalysisOutcome Hospitalization (n=2464) Elevated BNP (n=981)
Spiro(n=1232)
Placebo (n=1232)
HR (p-value)
Spiro (n=490)
Placebo (n=491)
HR (p-value)
Primary Outcome 19.6% 19.1% 1.01 (p=0.923)
15.9% 23.6% 0.65 (p=0.003)
CV Mortality 9.7% 9.5% 1.01 (p=0.924)
8.2% 12% 0.69 (p=0.069)
Aborted cardiac arrest
0.1% 0.4% 0.2 (p=0.138)
0.4% 0 N/A
Hospitalization for heart failure
12.3% 13.1% 0.92 (0.44)
11.2% 16.9% 0.64 (p=0.011)
NEJM 2014;370:1383-1392

Post-hoc Analysis
Outcome Americas Eastern Europe
Spiro (n=886)
Placebo (n=881)
HR (p-value)
Spiro (n=836)
Placebo (n=842)
HR (p-value)
Primary Outcome
27.3% 31.8% 0.82 (p=0.026)
9.3% 8.4% 1.1 (p=0.576)
Adjusted Cox Model: HR 3.96, p<0.001
NEJM 2014;370:1383-1392

Safety
Spironolactone Placebo
Doubling of SCr
D/C due to breast tenderness
↓ Systolic BP
↑ Hyperkalemia
↑ Hypokalemia
NEJM 2014;370:1383-1392

Author’s Conclusions
In patients with HFpEF, spironolactone did NOT significantly reduce the incidence of
the primary outcome.
Spironolactone -> reduced hospitalizations
NEJM 2014;370:1383-1392

Study CritiqueStrengths Limitations
• First large study of aldosterone antagonists in HFpEF to look at morbidity and mortality
• Doses achieved similar to other HF studies (i.e., RALES)
• Fewer HF hospitalizations in spironolactone group
• Mild adverse event profile for spironolactone
• Inclusion criteria for hospitalization: Major component of hospitalization was heart failure but no standard diagnosis
• Different standards of care and definitions of heart failure in different countries
• Not powered to detect differences in subgroup or post-hoc analyses

Impact on Clinical Practice
• Increased use of aldosterone antagonists in patients with HFpEF?– Particularly those with elevated BNP
• Future Studies– Geographic regions– Include only patients with elevated BNP

Acknowledgements
• Carolyn Hempel, PharmD, BCPS– State University of New York at Buffalo, School of
Pharmacy and Pharmaceutical Sciences• Jenna Huggins, PharmD, BCPS-AQ Cardiology
– WakeMed Health & Hospitals • Herb Patterson, PharmD, FCCP
– UNC Eshelman School of Pharmacy• Craig Beavers, PharmD, AACC, BCPS-AQ Cardiology
– TriStar Centennial Medical Center

Questions??

Thank you for attending!
• If you would like to have your resident present, would like to be a mentor, or have questions or comments please e-mail the journal club at [email protected] or [email protected]
• Our next Journal Club will be November 25th, same time.– Robert Tunny from Vanderbilt Medical Center will be
presenting PARADIGM-HF