accuracy in blood pressure measurement importance of site and accuracy
TRANSCRIPT

ACCURACY IN BLOOD PRESSURE
MEASUREMENTImportance of site and accuracy
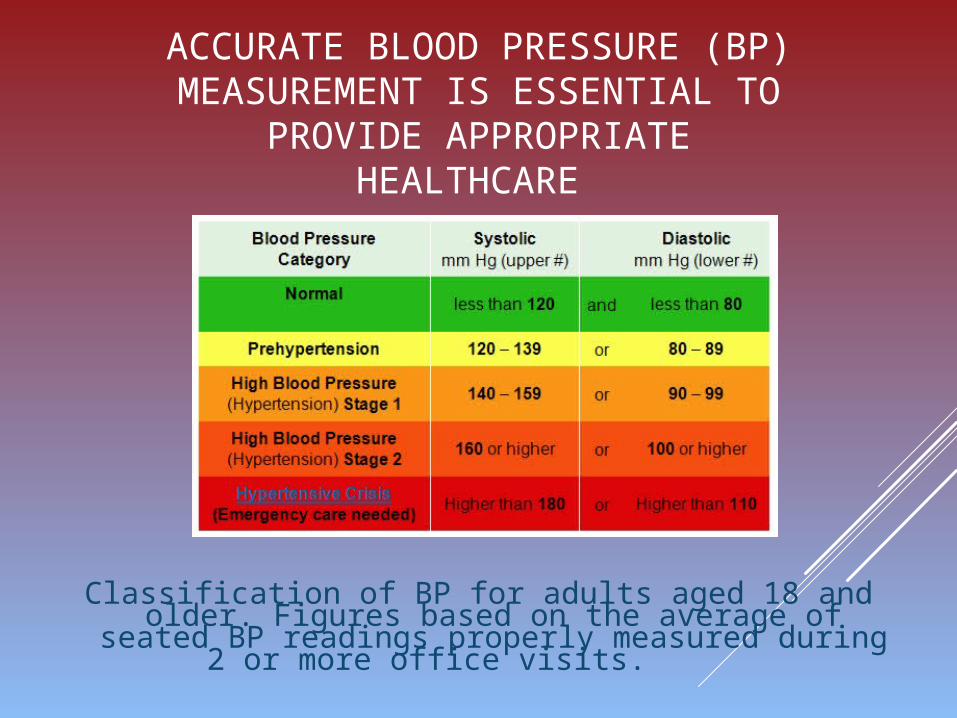
ACCURATE BLOOD PRESSURE (BP) MEASUREMENT IS ESSENTIAL TO
PROVIDE APPROPRIATE HEALTHCARE
Classification of BP for adults aged 18 and older. Figures based on the average of seated BP readings properly measured during 2 or more office visits.
FOR MOST ACCURATE BLOOD PRESSURE RESULTS…
Patient should avoid caffeine, tobacco, or alcohol for 30 minutes prior to measuring.
Patient should rest for 3 to 5 minutes before screening. They should also refrain from talking.
Patient may lie supine or sit erect in a comfortable position, with legs uncrossed and back supported.
Place patient’s arm at heart level, on a stable surface, allowing the arm to remain still.
Wrap the properly sized cuff snugly around a bare arm, leaving enough room for a fingertip under the cuff.
Be certain that the bottom edge of the cuff is 1 inch (2.5 cm) above the antecubital fossa.
Position the cuff on the arm properly by placing the arrow or tubing on the inside of the elbow.
Measure blood pressure in both arms during the initial assessment.
Take multiple readings at least one minute apart and record all the results.
Measure at the same time daily unless otherwise specified. Use the correct sized cuff for your arm.

WHY IS THE RIGHT SIZED CUFF IMPORTANT?
The right cuff size is very important.
Blood pressure readings may be wrong if your cuff is the wrong size.
If the cuff is too wide, it will underestimate the BP
While a cuff that is too narrow tends to overestimate the BP.
To ensure proper size, the National Institute of Health and American Heart Association each offer different methods.
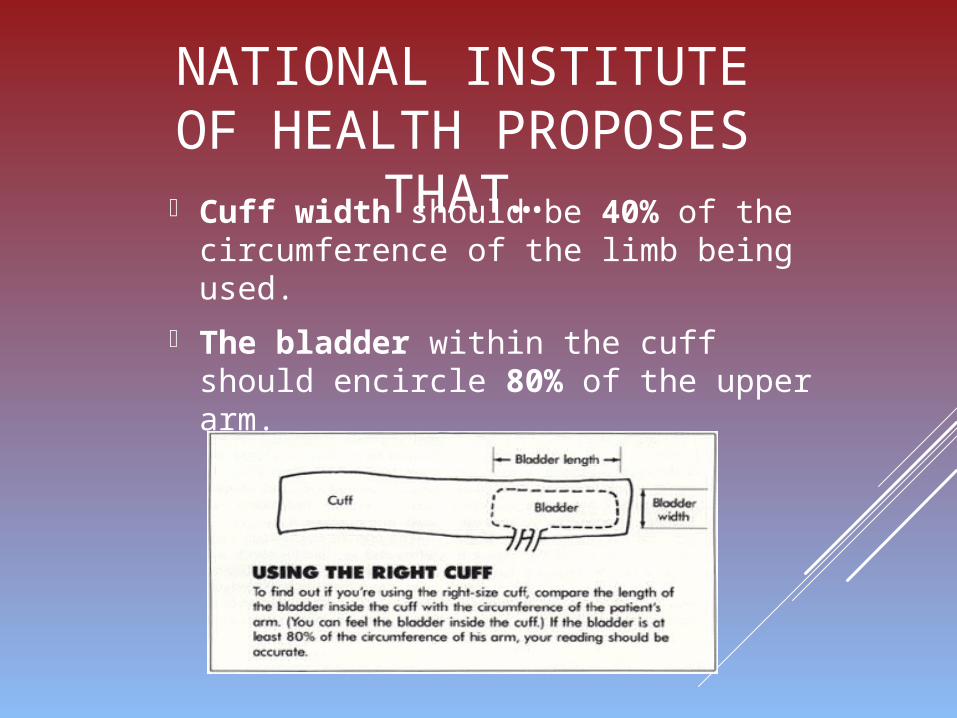
NATIONAL INSTITUTE OF HEALTH PROPOSES
THAT… Cuff width should be 40% of the
circumference of the limb being used.
The bladder within the cuff should encircle 80% of the upper arm.

AMERICAN HEART ASSOCIATIONS (AHA’S)
GUIDELINES ON BP CUFF SIZE Cuff Arm
Circumference NEWBORN <2.5” (< 6 cm) INFANT 2.5-6” (6–15 cm) CHILD 6–8.5” (16-21 cm) SMALL ADULT 8-10” (22-26 cm) ADULT REGULAR 11–13” (27-34 cm) ADULT LARGE 14–17” (35-44 cm) THIGH 18–21” (45-52 cm)
AHA generally recommends larger cuffs be used for borderline measurements (AHA. 1993).
The brachial (upper arm) site is the gold standard for non-invasive BP
monitoring. However, in some situations, this site is inaccessible due to injury, surgery, dialysis shunts, intravenous
devices, and lymphedema. When the upper arm is unavailable to be
used, the forearm site is sometimes the alternative. The increased incidence of obesity also contributes to a heightened
use of forearm BP monitoring.
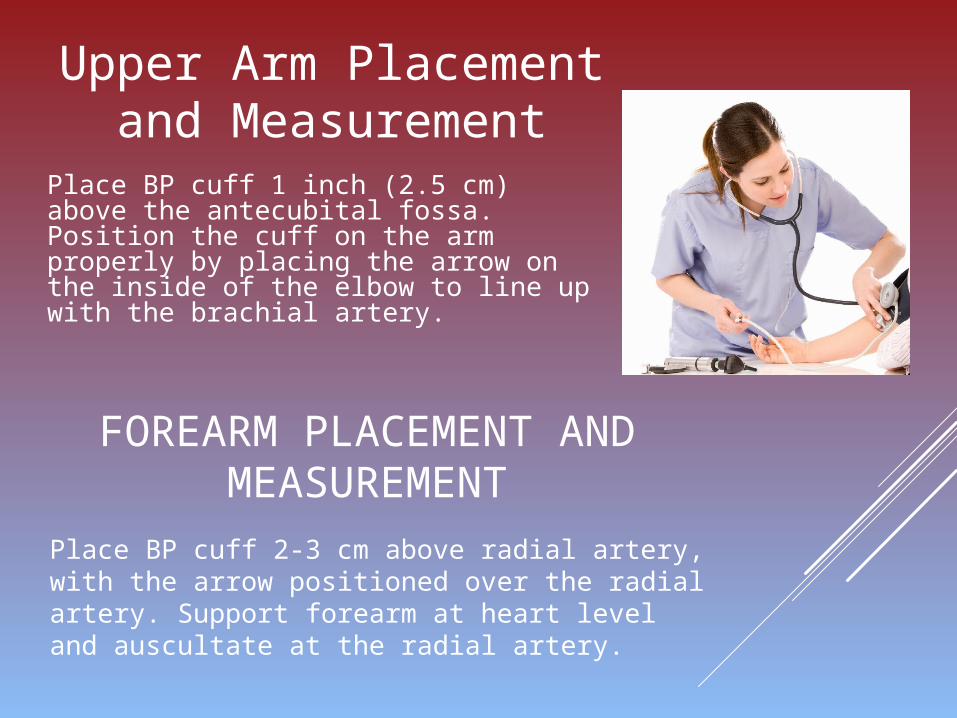
FOREARM PLACEMENT AND MEASUREMENT
Place BP cuff 2-3 cm above radial artery, with the arrow positioned over the radial artery. Support forearm at heart level and auscultate at the radial artery.
Place BP cuff 1 inch (2.5 cm) above the antecubital fossa. Position the cuff on the arm properly by placing the arrow on the inside of the elbow to line up with the brachial artery.
Upper Arm Placement and Measurement

AMERICAN HEART ASSOCIATION GUIDELINES RECOMMEND THE FOREARM METHOD
FOR SELECTED BARIATRIC PATIENTSONLY WHEN 1 OF THE FOLLOWING 2 CRITERIA IS
MET:
Upper arm circumference is >20” (50 cm)
Size & shape of upper arm suggest available cuffs will fit extremely poorly
When appropriate (per AHA guidelines), forearm BP’s should be assessed using an ADULT REGULAR cuff at the radial artery (a regular size cuff is appropriate sincemorbid obesity generally spares the wrist).
EVIDENCE BASED PRACTICE SHOWS…
“However, population wide, small inaccuracies in blood pressure measurement can have considerable consequences.
Underestimating true blood pressure by 5 mmHg would mislabel more than 20 million Americans with prehypertension when true hypertension is present. It has been predicted that the consequences of an untreated 5 mmHg of excessive systolic blood pressure would be a 25% increase over current levels of fatal strokes and fatal myocardial infarctions for these individuals.
Conversely, overestimating true blood pressure by 5 mmHg would lead to inappropriate treatment with antihypertension medications in almost 30 million Americans, with attendant exposure to adverse drug effects, the psychological effects of misdiagnosis, and unnecessary cost.”
Many questions remain concerning the accuracy of forearm BP measurements. In fact, many researchers recommend utilizing other alternative BP measures, such as the popliteal (thigh) site, ahead of the forearm.
Research has consistently found that upper arm and forearm BP
readings are NOT interchangeable.
Forearm BP's differ from upper arm BPs. Recent evidence suggests forearm BPs overestimate
systolic, diastolic & mean values anywhere from 10 to 33 mmHg.
Trends in BP readings & patient status will need to be carefully evaluated prior to treatment.
As a result, it is critical that when the forearm method is indicated, all caregivers consistently use the forearm for BP readings.
More so, the difference in BP measurement sites can be used as a basis for a change in current practice to include recording the BP measurement along with the site, as is current practice with temperature measurement.
CONCLUSIONS
NATIONAL PATIENT SAFETY GOALS & QUALITY AND
SAFETY EDUCATION FOR NURSES
Accuracy in Blood Pressure measurement is relied upon for both quality patient care and safe medication administration. Many medications have an impact on not only blood pressure but other vital signs and these measurements are used in determining if the medication should be given and to assess the effect of the medication. Accuracy also plays a part in improving staff communication in that the forearm and the brachial site are not interchangeable. Remember the Brachial Site is the Gold Standard.
Quality and Safety Education for Nurses competencies of Evidence Based Practice play a part of accuracy in blood pressure measurement as the different sites have been researched and tested thoroughly such as in “Clinical Comparison of Automatic, Noninvasive Measurements of Blood Pressure in the Forearm and Upper Arm”
QUIZ TIME…
In what situations should the forearm site be used?

QUIZ TIME…
How do you properly measure a cuff for fit?

QUIZ TIME…
How far from the Antecubital Fossa should the cuff be placed?

QUIZ TIME…
What happens if the cuff is too small or too large?

QUIZ TIME…
What is the Gold Standard location?
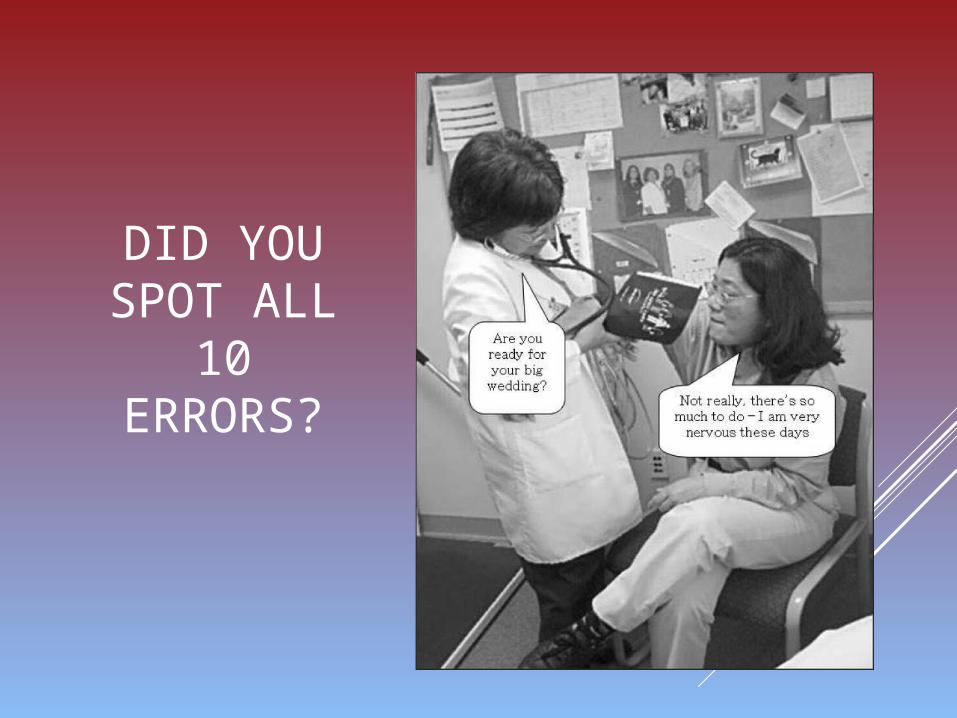
DID YOU SPOT ALL
10 ERRORS?

1. Pt’s arm is unsupported above heart level2. Pt’s back is unsupported3. Pt is talking4. Pt is engaged in active listening5. Wrong cuff size in use (too big)6. BP is too low on upper arm, appears to be
over elbow, likely that arterial marker is malpositioned as well
7. Cuff is over clothing8. Observer is not eye level with the monitor.
Where is the monitor?9. Pt’s legs are crossed10.End of stethoscope is in coat pocket

Barnason, S., Williams, J., & Patrick, V. (2012, December 1). Clinical Practice Guideline : Non - Invasive
Blood Pressure Measurement with Automated Devices. Retrieved from
https://www.ena.org/practice-research/research/CPG/Documents/NIBPMCPG.pdf
How to Monitor and Record Your Blood Pressure. (2014, August 4). Retrieved from
http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/SymptomsDiagnosisMonitori
ngofHighBloodPressure/How-to-Monitor-and-Record-Your-Blood-
Pressure_UCM_303323_Article.jsp
Potter, P. A., & Perry, A. G. (2013). Fundamentals of nursing (13th ed.). Philadelphia, PA: F. A. Davis
Company
Schimanski, K., Jull, A., Mitchell, N., & McLay, J. (2014). Comparison study of upper arm and forearm
non-invasive blood pressures in adult Emergency Department patients. International Journal Of
Nursing Studies, 51(12), 1575-1584. doi:10.1016/j.ijnurstu.2014.03.008
Wilson, S.F. & Giddens, J.F. (2009). Health assessment for nursing practice (4th ed.). Saint Louis, MO:
Eselvier
References