acta medica martiniana - uniba.sk · genetics of psoriasis – short resume valentova v. 1 ,...
TRANSCRIPT

JESSENII FACULTAS MEDICA MARTINENSISUniversitatis Comenianae
ACTAMEDICA
MARTINIANAJournal for Biomedical Sciences,
Clinical Medicine and Nursing
201111/1
ISSN 1339 - 4139 (online)ISSN 1335 - 8421


Vydanie ACTA MEDICA MARTINIANA 11/01 bolo podporené projektom
Podpora rozvoja ľudských zdrojov s využitím najmodernejších postupov
a foriem vzdelávania na JLF UK v Martine
spolufinancovaným zo zdrojov EÚ a Európskeho sociálneho fondu.
Publishing of Acta Medica Martiniana 11/01 was supported by project
„Support of human resources development using the most modern methods
and forms of education at JLF UK in Martin“
co-financed from EU sources and European Social Fund.
Moderné vzdelávanie pre vedomostnú spoločnosť/Projekt je spolufinancovaný zo zdrojov EÚModern education for modern society/Project is co-financed from EU sources


ISSN 1335-8421, ISSN 1338-4139 (online) Acta Med Mart 2011, 11(1)
ACTA MEDICA MARTINIANA
Journal for Biomedical Sciences, Clinical Medicine and Nursing
Contents
5Genetics of psoriasis – short resume
Valentova V., Galajda P., Pec M., Mokan M., Pec J.
14Activity of monoamine oxidases in rat female genital organs during
preimplantation period of pregnancy Mihalik J., Kravcukova P., Hodorova I., Vecanova J., Rybarova S.
21Renal ontogeny of P-glycoprotein/MDR1 in rat
Hodorova I., Mihalik J., Vecanova J., Dankova M., Rybarova S.
27Investigating dyspepsia in clinical practice – a trap for Giardia.
Banovcin P. Jr., Demeter M., Bozikova J., Hyrdel R.
35Point prevalence survey of nosocomial infections in University Hospital in Martin
Zabkova E., Murajda L., Hudeckova H.
Published by the Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 14
Editor – in – Chief: Javorka Kamil, Martin, Slovakia
International Editorial Board:
Belej Kamil, Martin, SlovakiaBelova Nina, Sofia, Bulgaria
Bohlin Kajsa, Stockholm, SwedenDanko Jan, Martin, Slovakia
Honzikova Natasa, Brno, Czech RepublicJakus Jan, Martin, Slovakia
Javorka Kamil, Martin, SlovakiaKliment Jan, Martin, SlovakiaLehotsky Jan, Martin, Slovakia
Mares Jan, Praha, Czech RepublicMechirova Eva, Kosice, SlovakiaMistuna Dusan, Martin, SlovakiaMokan Marian, Martin, Slovakia
Mokry Juraj, SlovakiaMusial Jacek, Krakow, PolandPlank Lukas, Martin, SlovakiaStasko Jan, Martin, Slovakia
Stransky Albert, Martin, SlovakiaTatar Milos, Martin, Slovakia
Zibolen Mirko, Martin, SlovakiaZubor Pavol, Martin, Slovakia
Editorial Office:
Acta Medica MartinianaJessenius faculty of Medicine, Comenius University
(Dept. of Physiology)Mala Hora 4
036 01 MartinSlovakia
Instructions for authors: http://www.jfmed.uniba.sk (Acta Medica Martiniana)
© Jessenius Faculty of Medicine, Comenius University, Martin, Slovakia, 2011

5
GEnEtICS OF PSORIASIS – SHORt RESUME
Valentova V.1, Galajda P.2, Pec M.1, Mokan M.2, Pec J.3
1Department of Medical Biology, Jessenius Faculty of Medicine, Comenius University, Martin, 2Clinic of Internal Medicine I., Jessenius Faculty of Medicine, Comenius University, Martin, 3Clinic of
Dermatovenerology, Jessenius Faculty of Medicine, Comenius University, Martin, Slovak Republic
ABStRACtPsoriasis is a disease with a genetic background (4). Several psoriasis susceptibility loci (PSORS) have been found on various chromosomes: PSORS1 on 6p21.3, PSORS2 on 17q, PSORS3 on 4q, PSORS4 on 1q21, PSORS5 on 3q21, PSORS6 on 19p, PSORS7 on 1p, PSORS8 on 16q, PSORS9 on 4q31, PSORS10 on 18p11, PSORS11 on 5q31-q33 and PSORS12 on 20q13. (27). However, the exact genes and their functions, or their respective malfunctions, in psoriasis and arthritis have not been unambiguously identified. Recently, it has been argued that PSORS1 may indeed be the HLA-Cw*06 allele encoding the HLA-Cw6 molecule (35).Psoriasis is a chronic inflammatory disease of skin that also often affects joints and nails. This disorder is characterized by hyperproliferation of keratinocytes, activation of angiogenesis, vasodilatation and mainly by lymphocyte infiltration of dermis and epidermis (45). The process of maturation of keratinocytes is accelerated and thus not quite terminated. Psoriatic lesion appears on skin. Skin manifestations are typically red bounded areas of different size and shape with characteristic silvery scales (9). Lesions appear mostly on the skin of elbows and knees, scalp including genitals. Individual manifestations differ in size and severity from localized lesions to whole body involvement. Very often psoriasis affects nails of hands and feet. It can also cause inflammatory changes on joints, named as psoriatic arthritis. Similarly to rheumatoid arthritis and sclerosis multiplex, psoriasis is classified as an immune mediated inflammatory disorder. Those disorders are characterized by chronic progression of an inflammatory process and important role of TNF alpha. Because of the role of TNF alpha in pathogenesis, we can use its inhibitors in therapy. It also affects progress of different comorbidities such as diabetes mellitus 2 and cardiovascular problems (21). Patients with psoriasis have often other risk factors for atherosclerosis such as lipid metabolism disorders and overweight (37).
Key words: psoriasis, PSORS, HLA-Cw6
IntRODUCtIOn
Psoriasis is characterized by hyperproliferation and abnormal differentiation of epider-mal keratinocytes, by lymphocytary infiltrate composed mainly of T-cells. Other features are change of endothelium, angiogenesis, dilatation and formation of high endothelial venules (HEV) (29).
Exact pathogenesis of this disorder is unknown, but it is supposed that main role plays an immune system (42, 45).
Theory that psoriasis is primarily keratinocyte proliferation disorder is based on ab-normally fast mitotic activity of keratinocytes. T-cell hypothesis imply an abnormal ac-tivation of an acquired immunity. Knowing that TNF alpha therapies are very effective, suggests an important role of innate immunity in pathogenesis (5).
A d d r e s s f o r c o r r e s p o n d e n c e :Mgr. Vanda Valentova, Department of Medical Biology, Jessenius Faculty of Medicine, Comenius UniversityMala Hora Str. 4, 036 01 Martin, Slovak Republic, Phone: +4210434131425, E-mail: [email protected]
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0001-0

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 16
SHORt REVIEw OF LOCI AnD CAnDIDAtE GEnES
In the early 1970s psoriasis was placed into associations with the HLA complex on chromosome 6p. Russell et al. in 1972 first reported association with allele HLA-B13. After that, were identified strong associations with other two alleles, Cw6 and DR7 (22, 49). These two alleles were estimated to be relative risk factors for the disease.
There are two types of psoriasis (23): • a familial, early age of onset form (<40 years)• associated with HLA-Cw6, DR7, B13 and B57• a non-familial, later age at onset form • associated with HLA-Cw2 and B27
Psoriasis is a disorder with genetic background and a multifactorial type of heredity. The hypothesis of genetic background is also supported by familial incidence. Chance that a child of nonpsoriatic parents will develop psoriasis is 12 %, if there is a one parent with psoriasis the risk is higher 10-20 % and in a case that both parents are having psoriasis it can be up to 50 % risk. In identical twins the risk that they will develop disease is about 90 %, in nonidentical twins its only 18 % (9). This difference shows a multifactorial type of inheritance and interaction between genetic predisposition and environmental influence (8,14). Based on the study of Bowcock and Barker from 2003 plaque psoriasis can be in small group of patients inherited as an autosomal dominant trait with high penetrance (6).
Fig. 1: Localization of locus PSORS1 in MHC locus, and candidate genes in PSORS1 locus (28).
Recently the results of multiple genetic case–control studies have begun to appear providing convincing statistical evidence for six loci (IL12B, IL13, IL23R, STAT2/IL23A, TNFAIP3, and TNIP1) for psoriasis (32).
In these days 10 loci are known named as PSORS1-10 (psoriasis susceptibility 1-9) and one for psoriatic arthritis, PSORAS1 (1; 13). Exact genes and their function are not yet identified (28). There is a possibility, of location PSPRS1 in allele of HLA-Cw6 coding HLA-Cw6 molecule (15, 36).
Using high-density cDNA microarray to identify psoriatic transcriptome and to set down gene expression in psoriatic lesions elevated expression of different molecules was found. Increased expression of certain mRNA associated with the epidermal differentia-tion complex and hyperproliferation-associated molecules (keratins KRT6A a KRT16) supports hypothesis that psoriasis is keratinocyte disorder, characteristic with their increased proliferation and abnormal differentiation (7, 39, 41, 57).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 7
It is possible that malfunction of CD4+CD25+ regulatory lymphocytes can be partially based on abnormal hematopoietic cells and with genetic background (55).
table 1: PSORS loci (10)
Locus name Chromosomal location Reference
PSORS 1 6p21.3 Zhang et al., 2002
PSORS 2 17q24-25 Samuelsson et al., 1999
PSORS 3 4q34 Samuelsson et al., 1999
PSORS 4 1q21 Capon et al., 1999
PSORS 5 3q21 Enlund et al., 1999
PSORS 6 19p13-q13 Lee et al., 2000
PSORS 7 1p35-p34 Veal et al., 2001
PSORS 8 16q Karason et al., 2003
PSORS 9 4q31 Zhang et al., 2002
PSORS 10 18p11.23 Asumalahlati et al., 2002
PSORS 11 5q31-q33 www.ncbi.nlm.nih.gov/omim
PSORS 12 20q13 www.ncbi.nlm.nih.gov/omim
PSORS1The most studied locus is PSORS1 mapped to MHC complex on chromosome 6. This
region contains genes coding proteins of immunological pathways and is strongly asso-ciated with genes of lymphocyte antigens also situated in this area (1, 11). Main marker of this area is HLA-Cw6 (48). This allele is most frequently mapped in population with early onset psoriasis (36).
Human leukocyte antigenPsoriasis has signs of an autoimmune disease and there is no surprise that there was
found association with certain HLA alleles. Also a role for CD8+ cells is favoured by the observed linkage of psoriasis to certain MHC I alleles, especially HLA Cw6 (20).
Only about 10 % of HLA-Cw6-positive individuals develop psoriasis, suggesting a ma-jor role for additional genes and/or environmental triggers (30).
The observation that a large, multiply affected family demonstrated linkage of pso-riasis susceptibility to 17q25 (50) and not to HLA suggests that other genes can confer susceptibility. In a study of 23 multiply affected families was observed that 25 % are HLA-Cw6 positive. In one family, all three affected members are HLA-B27 (4, 33, 35).
PSORS2Locus is situated near telomeres of chromosome 17q (50). Exact localization of risk al-
lele is not known. In this area at least two candidate genes are expected, but last large study eliminated them both (47).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 18
PSO0RS3Localized is on chromosome 4, in position 4q34. A relation with early onset psoriasis
was found in this area (17). Responsible gene is mapped about 50kb from former marker of PSORS3 locus. The newest localization is for PSORS9 locus, mapped closer to cen-tromere (4q31) in PSORS3 area (25, 56). In this region are situated different genes cod-ing immunologically important proteins, including IL-15 gene (53).
PSORS4Locus PSORS4 mapped to 1q21 of chromosome 4, in area of Epidermal differentiation
complex. This region involves 13 genes coding S100 calcium binding proteins. Some of them, S100A7, S100A8 a S100A9 are known to be increased in keratinocytes of psoriatic patients (44). S100 proteins are responsible for chemotaxis of leukocytes.
PSORS5Localized to 3q21 but his exact position is need to be confirmed by more studies (43).
PSORS6Mapped to 19p13 and his position is also not exact. In this area is mapped also gene
JUNB, which product is member of AP-1 family of transcriptional factors, that control differentiation of keratinocytes (54).
PSORS7Locus is situated in position 1p. Veal et al. (52) referred to fact that gene EPS15
coding intracellular substrate for EGF receptors, highly expressed in psoriatic skin, and is mapped to critical region in position of 1p.
PSORS8This locus is mapped to 16q. Nair et al. (35) referred that PSORS8 area is overlapping
with susceptibility locus for Crohn disease. They found that this locus contains NOD2/CARD15 gene. They also found that psoriasis is more often in patients with Crohn dis-ease, in comparison to control group. It shows a possibility that in this region is local-ized an immunomodulatory locus able to affect both diseases.
PSORS9 Locus is mapped to 4q position.
IL-10IL-10 plays an important role in the pathophysiology of psoriasis. This disease is char-
acterized by a relative IL-10 deficiency that can in part explain the predominance of a Th1 response. The IL-10 promoter region is very polymorphic and controls transcription of the IL-10 gene (3, 24).
While the concept of an allele that makes an individual susceptible to a disease is eas-ily understood, the concept of a protective allele of a predisposing gene is rather new in the genetics of psoriasis.
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 9
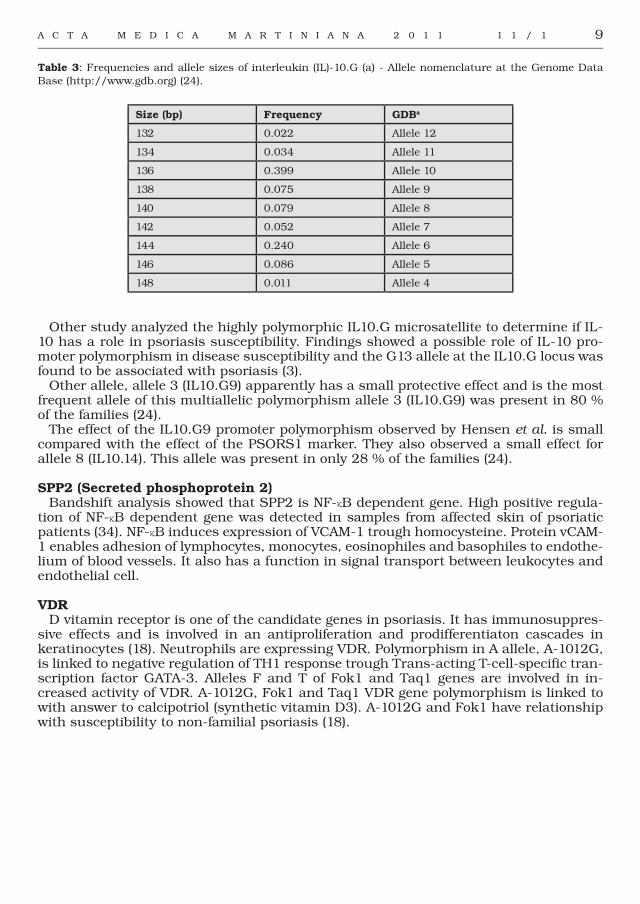
table 3: Frequencies and allele sizes of interleukin (IL)-10.G (a) - Allele nomenclature at the Genome Data Base (http://www.gdb.org) (24).
Size (bp) Frequency GDBa
132 0.022 Allele 12
134 0.034 Allele 11
136 0.399 Allele 10
138 0.075 Allele 9
140 0.079 Allele 8
142 0.052 Allele 7
144 0.240 Allele 6
146 0.086 Allele 5
148 0.011 Allele 4
Other study analyzed the highly polymorphic IL10.G microsatellite to determine if IL-10 has a role in psoriasis susceptibility. Findings showed a possible role of IL-10 pro-moter polymorphism in disease susceptibility and the G13 allele at the IL10.G locus was found to be associated with psoriasis (3).
Other allele, allele 3 (IL10.G9) apparently has a small protective effect and is the most frequent allele of this multiallelic polymorphism allele 3 (IL10.G9) was present in 80 % of the families (24).
The effect of the IL10.G9 promoter polymorphism observed by Hensen et al. is small compared with the effect of the PSORS1 marker. They also observed a small effect for allele 8 (IL10.14). This allele was present in only 28 % of the families (24).
SPP2 (Secreted phosphoprotein 2)Bandshift analysis showed that SPP2 is NF-κB dependent gene. High positive regula-
tion of NF-κB dependent gene was detected in samples from affected skin of psoriatic patients (34). NF-κB induces expression of VCAM-1 trough homocysteine. Protein vCAM-1 enables adhesion of lymphocytes, monocytes, eosinophiles and basophiles to endothe-lium of blood vessels. It also has a function in signal transport between leukocytes and endothelial cell.
VDRD vitamin receptor is one of the candidate genes in psoriasis. It has immunosuppres-
sive effects and is involved in an antiproliferation and prodifferentiaton cascades in keratinocytes (18). Neutrophils are expressing VDR. Polymorphism in A allele, A-1012G, is linked to negative regulation of TH1 response trough Trans-acting T-cell-specific tran-scription factor GATA-3. Alleles F and T of Fok1 and Taq1 genes are involved in in-creased activity of VDR. A-1012G, Fok1 and Taq1 VDR gene polymorphism is linked to with answer to calcipotriol (synthetic vitamin D3). A-1012G and Fok1 have relationship with susceptibility to non-familial psoriasis (18).
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 110
ADAM33 and other genesPolymorphism in locus ADAM33, first gene identified in asthma, is in these days given
to relation with psoriasis (46).Li et al. have tested 15 SNPs form 7 expected psoriatic risk genes: rs597980 in allele
ADAM33, rs6908425 in CDKAL1 and rs3789604 in PtPn22. Results have shown as significant for the same alleles as in previous studies. This data show, that ADAM33, CDKAL1, and PTPN22 are risk genes for psoriasis (32).
Study of Oudota et al. in year 2009, confirmed linkage of other six candidate genes to susceptibility to psoriasis: SCL12A8, belongs to group of free transposing genes; FLG and tGM5, involved in epidermal differentiation; CARD15 and CYLD, that modu-late transcriptional factor NF-κB and IL1Rn, coding antagonist receptor of IL-1. It was proved that an association exists between main risk allele HLA-Cw6 and CARD15, CYLD and TMG5 alleles. Together these results show that etiology of psoriasis and other dis-orders is cooperation of different genetic factors (40).
One region is within the MHC complex on 6p21.3 (51) and includes the non-HLA gene–encoding corneodesmosin (CD) — a protein with homology to keratin-10 (2). The other region includes a cluster of genes on chromosome 1q21 (19, 38). Potential candidate genes encode markers of epidermal differentiation such as corneodesmosin, psoriasin, and CD1d, to name a few (19).
IL-20RComplex of IL-20 receptor is composed from two chains IL20RA and IL20RB. Its li-
gands are three members from IL-19 subfamily, IL-19, IL-20 and IL-24. These cytokines are important for manifestation of psoriatic lesions and recently was described also a relation between IL20 gene polymorphism and psoriasis. In last studies the hypothesis is tested, that genetic variants of IL-20-RI influence susceptibility to psoriasis. To these days there isn’t proved relationship between SNP in that gene and psoriasis. SNPs in two risk haplotypes influence two transcriptional factors leading to differentiation of immune cells. Other studies are necessary to confirm genetic association of IL-20-RA haplotypes with psoriasis (27).
ConclusionIn the last few years, molecular genetics analyses have permitted novel insights into
psoriasis, a disease characterized by uncontrolled proliferation of keratinocytes and recruitment of T cells into the skin. HLA studies revealed an association with certain alleles, notably HLA-Cw6. Despite this HLA component, psoriasis in some families is inherited as an autosomal dominant trait with high penetrance.
Significant progress has been made in the understanding of the genetic, immune and pathogenetic aspects of psoriasis.
Understanding the genetics of psoriasis, and why some people are affected and others are not could lead to more effective treatments. They could work blocking the action of concrete genes, changing their behaviour or by replacing mutated genes with healthy ones via gene therapy.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 11
REFEREnCES
1. Asumalahti K, Veal C, Laitinen T, Suomela S, Allen M, Elomaa O, Moser M, De Cid R, Ripatti S, Vorechovsky I, Marcusson JA, Nakagawa H, Lazaro C, Estivill X, Capon F, Novelli G, Saarialho-Kere U, Barker J, Trembath R, Kere J. Coding haplotype analysis supports HCR as the putative susceptibility gene for psoriasis at the MHC PSORS1 locus. Hum Mol Gene 2002; 11:589–597
2. Allen MH, Veal C, Faassen A, Powis SH, Vaughan RW, Trembath RC, Barker JN. A non-HLA gene within the MHC in psoriasis. Lancet 1999; 353:1589-90
3. Asadullah K, Eskdale J, Wiese A, Gallagher G, Friedrich M, Sterry W. Interleukin-10 promoter polymorphism in psoriasis. J Invest Dermatol 2001; 116:975–978
4. Bhalerao J, Bowcock AM. The genetics of psoriasis: a complex disorder of the skin and immune system. Human molecular genetics 1998; 7:1537-45
5. Bos JD, De Rie MA, Teunissen MB, Piskin G. Psoriasis: dysregulation of innate immunity. Br J Dermatol. 2005; 152:1098-107
6. Bowcock AM, Barker JN. Genetics of psoriasis: the potential impact on new therapies. J Am Acad Dermatol 2003; 49:51–56
7. Bowcock AM, Shannon W, Du F, Duncan J, Cao K, Aftergut K, Catier J, Fernandez-Vina MA, Menter A. Insights into psoriasis and other inflammatory diseases from large-scale gene expression studies. Hum Mol Genet 2001; 10:1793-805
8. Brandrup F, Holm N, Grunnet N, Henningsen K, Hansen HE. Psoriasis in monozygotic twins: variations in expression in individuals with identical genetic constitution. Acta Dermatol 1982; 62:229–36.
9. Braun-Falco O, Plewig G, Wolff H. Dermatológia a venerológia 1. slov. a čes. vyd. Martin, Vydavateľstvo Osveta 2001; 1475s.
10. Campalani E, Barker JNWN. The Clinical Genetics of Psoriasis. Current Genomics 2005; 6:51-6011. Capon F, Munro M, Barker J, Trembath R. Searching for the major histocompatibility complex psoriasis
susceptibility gene. J Invest Dermatol 2002; 118:745–75112. Capon F, Novelli G, Semprini S, Clementi M, Nudo M, Vultaggio P, Mazzanti C, Gobello T, Botta A, Fabrizi
G, Dallapiccola B. Searching for psoriasis susceptibility genes in Italy: genome scan and evidence for a new locus on chromosome 1. J Invest Dermatol 1999; 112:32-35
13. Cookson WOCM, Bowcock AC, Harper JI, Moffat MF. The immunogenetics of inflammatory skin disease. In: Bos JD editor. Skin immune system (SIS): Cutaneous immunology and clinical immunodermatology. 3rd ed. Boca Raton (FL):CRC Press 2005; pp 55-73
14. Duffy DL, Spelman LS, Martin LG. Psoriasis in Australian twins. J Am Acad Dermatol 1993; 29:428–43415. Elder JT. PSORS1: linking genetics and immunology. J Invest Dermatol 2006; 126:1250-616. Enlund F, Samuelsson L, Enerback C, Inerot A, Wahlstrom J, Yhr M, Torinsson A, Riley J, Swanbeck
G, Martinsson T. Psoriasis susceptibility locus in chromosome region 3q21 identified in patients from southwest Sweden. Eur J Hum Genet 1999; 7:783-790
17. Foerster J, Nolte I, Schweiger S, Ehlert C, Bruinenberg M, Spaar K, van der Steege G, Mulder M, Kalscheuer V, Moser B, Kijas Z, Seeman P, Ständer M, Sterry W, te Meerman G. Evaluation of the IRF-2 gene as a candidate for PSORS3. J Invest Dermatol 2004; 122:61-4
18. Halsall JA, Osborne JE, Pringle JH, Hutchinson PE. Vitamin D receptor gene polymorphisms, particularly the novel A-1012G promoter polymorphism, are associated with vitamin D3 responsiveness and non-familial susceptibility in psoriasis. Pharmacogenet Genomics 2005; 15:349-55
19. Hardas BD, Zhao X, Zhang J, Longqing X, Stoll S, Elder JT. Assignment of psoriasin to human chromosomal band 1q21: coordinate overexpression of clustered genes in psoriasis. J Invest Dermatol 1996; 106:753-8
20. Henseler T, Christophers E. Psoriasis of early and late onset: characterization of two types of psoriasis vulgaris. J Am Acad Dermatol 1985; 13:450–456
21. Henseler T, Christophers E. Disease concomitance in psoriasis. J Am Acad Dermatol 1995; 32:982–98622. Henseler T, Koch F, Westphal E. Presence of HLA- DR7 in type I psoriasis. J Invest Dermatol 1992; 98:60723. Henseler T. The genetics of psoriasis. J Am Acad Dermatol 1997; 37:S1-S1124. Hensen P, Asadullah K, Windemuth C, Rüschendorf F, Hüffmeier U, Ständer M, Schmitt-Egenolf M,
Wienker TF, Reis A, Traupe H. Interleukin-10 promoter polymorphism IL10.G and familial early onset psoriasis. Br J Dermatol.2003;149:381-5.
25. Karason A, Gudjonsson JE, Jónsson HH, Hauksson VB, Runarsdottir EH, Stefansson K, Valdimarsson H, Gulcher JR. Genetics of psoriasis in Iceland: evidence for linkage of subphenotypes to distinct loci. J Invest Dermatol 2005; 124:1177-85

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 112
26. Karason A, Gudjonsson JE, Upmanyu R, Antonsdottir AA, Hauksson VB, Runasdottir EH, Jonsson HH, Gudbjartsson DF, Frigge ML, Kong A, Stefansson K, Valdimarsson H,Gulcher JR. A susceptibility gene for psoriatic arthritis maps to chromosome 16q: evidence for imprinting. Am J Hum Genet 2003; 72:125-131
27. Kingo K, Mössner R, Rätsep R, Raud K, Krüger U, Silm H, Vasar E, Reich K, Kõks S. Association analysis of IL20RA and IL20RB genes in psoriasis. Genes Immun 2008; 9:445-51
28. Krueger JG, Bowcock A. Psoriasis pathophysiology: current concepts of pathogenesis. Ann Rheum Dis 2005; 64:303-6
29. Krueger JG, Ellis CN. Psoriasis-recent advances in understanding its pathogenesis and treatment. J Am Acad Dermatol 2005; 53:94-100
30. Leder RO and Farber EM. The variable incidence of psoriasis in sub-saharan Africa. Int J Dermatol 1997; 36:911-919
31. Lee YA, Ruschendorf F, Windemuth C, Schmitt-Egenolf M, Stadelmann A, Nurnberg G, Stander M, Wienker TF, Reis A, Traupe H. Genomewide scan in German families reveals evidence for a novel psoriasis-susceptibility locus on chromosome 19p13. Am J Hum Genet 2000; 67:1020-1024
32. Li Y, Begovich AB. Unraveling the genetics of complex diseases: susceptibility genes for rheumatoid arthritis and psoriasis. Semin Immunol 2009; 21:318-27
33. Marcos CY, Fernandez-Vina MA, Barnes R. et al. HLA-B and HLA-C genes in familial psoriasis vulgaris (PV): evidence for genetic heterogeneity. Hum Immunol 1997; 55:51
34. Mechtcheriakova D, Wlachos A, Sobanov J, Kopp T, Reuschel R, Bornancin F, Cai R, Zemann B, Urtz N, Stingl G, Zlabinger G, WoisetschlĂger M, Baumruker T, Billich A. Sphingosine 1-phosphate phosphatase 2 is induced during inflammatory responses. Cell Signal 2007; 19:748-60
35. Nair RP, Henseler T, Jenisch S, Stuart P, Bichakjian CK, Lenk W, Westphal E, Guo SW, Christophers E, Voorhees JJ, Elder JT. Evidence for two psoriasis susceptibility loci (HLA and 17q) and two novel candidate regions (16q and 20p) by genome-wide scan. Hum Molec Genet 1997; 6:1349-56
36. Nair RP, Stuart PE, Nistor I, Hiremagalore R, Chia NV, Jenisch S, Weichenthal M, Abecasis GR, Lim HW, Christophers E, Voorhees JJ, Elder JT. Sequence and haplotype analysis supports HLA-C as the psoriasis susceptibility 1 gene. Am J Hum Genet 2006; 78:827-51
37. Naldi L, Chatenoud I, Linder D, Belloni FA, Peserico A, Virgili AR, Bruni PL, Ingordo V, Lo Scocco G, Solaroli C, Schena D, Barba A, Di Ladro A, Pezzarossa E, Arcangeli F,Gianni C, Betti R, Carli P, Farris A, Barbino GF, La Vecchia C. Cigarette smoking, body mass index, and stressful life events as risk factors for psoriasis: results from an Italian case control study. J Invest Dermatol 2005; 125:61–67
38. Nickoloff BJ. The immunologic and genetic basis of psoriasis. Arch Dermatol 1999; 135:1104-1039. Nomura I, Goleva E, Howell MD, Hamid QA, Ong PY, Hall CF, Darst MA, Gao B, Boguniewicz M, Travers
JB, Leung DY. Cytokine milieu of atopic dermatitis, as compared to psoriasis, skin prevents induction of innate immune response genes. J Immunol 2003; 171:3262-9
40. Oudot T, Lesueur F, Guedj M, de Cid R, McGinn S, Heath S, Foglio M, Prum B, Lathrop M, Prud’homme JF, Fischer J. An Association Study of 22 Candidate Genes in Psoriasis Families Reveals Shared Genetic Factors with Other Autoimmune and Skin Disorders. J Invest Dermatol 2009; 129:2637-45
41. Quekenborn-Trinquet V, Fogel P, Aldana-Jammayrac O, Ancian P, Demarchez M, Rossio P, Richards HL, Kirby B, Nguyen C, Voegel JJ, Griffiths CE. Gene expression profiles in psoriasis: analysis of impact of body site location and clinical severity. Br J Dermatol 2005; 152:489-504
42. Sabat R, Philipp S, Höflich C, Kreutzer S, Wallace E, Asadullah K, Volk H-D,Sterry W, Wolk K. Immunopathogenesis of psoriasis. Exp Dermatol 2007; 16:779–798
43. Samuelsson L, Enlund F, Torinsson A, Yhr M, Inerot A, Enerback C, Wahlstrom J, Swanbeck G, Martinsson T. A genome-wide search for genes predisposing to familial psoriasis by using a stratification approach. Hum Genet 1999; 105:523-529
44. Semprini S, Capon F, Tacconelli A, Giardina E, Orecchia A, Mingarelli R, Gobello T, Zambruno G, Botta A, Fabrizi G, Novelli G. Evidence for differential S100 gene over-expression in psoriatic patients from genetically heterogeneous pedigrees. Hum Genet 2002; 111:310-3
45. Schön MP, Boehncke WH. Psoriasis. N Engl J Med 2005; 352:1899-91246. Siroux V, Bouzigon E, Dizier MH, Pin I, Demenais F, Kauffmann F. Replication of association between
ADAM33 polymorphisms and psoriasis. PLoS ONE 2008; 3:244847. Stuart P, Nair RP, Abecasis GR, Nistor I, Hiremagalore R, Chia NV, Qin ZS, Thompson RA, Jenisch S,
Weichenthal M, Janiga J, Lim HW, Christophers E, Voorhees JJ, Elder JT. Analysis of RUNX1 binding site and RAPTOR polymorphism in psoriasis: no evidence for association despite adequate power and evidence for linkage. J Med Genet 2006; 43:12-7

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 13
48. Suomela S, Kainu K, Onkamo P, Tiala I, Himberg J, Koskinen L, Snellman E, Karvonen SL, Karvonen J, Uurasmaa T, Reunala T, Kivikäs K, Jansén CT, Holopainen P, Elomaa O, Kere J, Saarialho-Kere U. Clinical associations of the risk alleles of HLA- Cw6 and CCHCR1*WWCC in psoriasis. Acta Derm Venereol 2007; 87:127-34
49. Tiilikainen A, Lassus A, Karvonen J, Vartiainen P, Julin M. Psoriasis and HLA-Cw6. Br J Dermatol. 1980; 102:179-84
50. Tomfohrde J, Silverman A, Barnes R, Fernandez-Vina MA, Young M, Lory D, Morris L, Wuepper KD, Stastny P, Menter A et al. Gene for familial psoriasis susceptibility mapped to the distal end of human chromosome 17q. Science 1994; 264:1141-5
51. Trembath RC, Lee Clough R, Rosbotham JL, Jones AB, Camp RDR, Frodsham A, Browne J, Barber R, Terwilliger J, Lathrop GM, Barker JNWN. Identification of a major susceptibility locus on chromosome 6p and evidence for further disease loci revealed by a two stage genome-wide search in psoriasis. Hum Mol Genet 1997; 6:813-820
52. Veal CD, Clough RL, Barber RC, Mason S, Tillman D, Ferry B, Jones AB, Ameen M, Balendran N, Powis SH, Burden AD, Barker JNWN, Trembath RC. Identification of a novel psoriasis susceptibility locus at 1p and evidence of epistasis between PSORS1 and candidate loci. J Med Genet 2001; 38:7-13
53. Villadsen LS, Schuurman J, Beurskens F, Dam TN, Dagnaes-Hansen F, Skov L, Rygaard J, Voorhorst-Ogink MM, Gerritsen AF, van Dijk MA, Parren PW, Baadsgaard O, van de Winkel JG. Resolution of psoriasis upon blockage of Il-15 biologic activity in a xenograft mouse model. J Clin Invest 2003; 112:1571-80
54. Zenz R, Eferl R, Kenner L, Florin L, Hummerich L, Mehic D, Scheuch H, Angel P, Tschachler E, Wagner EF. Psoriasis-like skin disease and arthritis caused by inducible epidermal deletion of Jun proteins. Nat 2005; 437:369-75
55. Zhang K, Li X, Yin G, Liu Y, Niu X, Hou R. Functional characterization of CD4+CD25+ regulatory T cells differentiated in vitro from bone marrow-derived haematopoietic cells of psoriasis patients with a family history of the disorder. Br J Dermatol 2008; 158:298–305
56. Zhang XJ, He PP, Wang ZX, Zhang J, Li YB, Wang HY, Wei SC, Chen SY, Xu SJ, Jin L, Yang S, Huang W. Evidence for a major psoriasis susceptibility locus at 6p21 (PSORS1) and a novel candidate region at 4q31 by genome-wide scan in Chinese hans. J Invest Dermatol 2002; 119:1361-6
57. Zhou X, Krueger JG, Kao MC, Lee E, Du F, Menter A, Wong WH, Bowcock AM; Novel mechanism of T-cell and dendritic cell activation revealed by profiling of psoriasis on the 63,100-element oligonucleotide array. Physiol Genomics 2003; 13:69-78
Received: December,6,2010Accepted: January,7,2011

14
ACtIVItY OF MOnOAMInE OxIDASES In RAt FEMALE GEnItAL ORGAnS DURInG PREIMPLAntAtIOn PERIOD OF PREGnAnCY
Mihalik J.1, Kravcukova P.2, Hodorova I.1, Vecanova J.1, Rybarova S.1
1 Department of Anatomy, P.J.Safarik University, Medical Faculty, Kosice, Slovak Republic 2 Neurobiological Institute, Slovak Academy of Sciences, Kosice, Slovak Republic
ABStRACtOur objectives in the present study were to determine the activity of monoamine oxidases A and B (MAO AB) in rat ovary, oviduct and uterus during preimplantation period of pregnancy. It should help us to clarify and better understand possible involvement of both MAO enzymes in the reproductive process. Pregnant females were killed employing a lethal dose of thiopental on the first (D1), on the third (D3), and on the fifth (D5) days of pregnancy. Rats were perfused transcardially with the PBS to rinse out of the body as much blood as possible. Ovaries, oviducts and uteri were immediately removed and stored until the measurement was done. MAO activity was determined by fluorescent monoamine oxidase detection kit. In the ovaries we have found the highest MAO activity at D3, followed by D1, and the lowest levels were recorded at D5 of pregnancy. In the oviducts, the highest MAO activity was detected again at D3, followed by D5, and by D1 of pregnancy. But statistical analysis did not reveal any difference between individual days of pregnancy nor in the ovaries, neither in uterine tubes. Uteri were the only organs, in which statistically significant differences were detected (p<0.001). The highest activity of MAO was observed at D5, followed by D1, and by D3 of pregnancy. Potential mechanisms responsible for the changed MAO activity in gonads during preimplantation period of pregnancy are proposed.
Key words: MAO, ovary, oviduct, uterus
IntRODUCtIOn
Monoamine oxidases (MAO) are flavoprotein enzymes located in the mitochondrial outer membrane. The enzymes exist as two forms, MAO-A and MAO-B, which are dif-ferent gene products and have different substrate specificities. MAO-A preferentially oxidizes noradrenaline (NA) and serotonin (5HT), while MAO-B has a greater affinity for phenylethylamine and benzylamine. Dopamine (DA) is a common substrate of both MAO-A and MAO-B. The two MAO isoforms can also be differentiated according to their inhibition by synthetic compounds. MAO-A is selectively inhibited by clorgyline whereas MAO-B is selectively inhibited by L-deprenyl (selegiline). MAO are involved in many be-havioral processes and their inhibition has a marked effect on brain function, blood pressure regulation and the detoxification of potentially harmful exogenous amines [1].
In attempt to understand the role of MAO enzymes in brain, many studies have inves-tigated their distribution and cellular localization [2]. Recently, an increasing number of claims have been made about involvement of these enzymes in many psychiatric and neurological diseases, such as depression, bulimia, schizophrenia, Parkinson’s disease, Alzheimer’s disease, neurodegenerative diseases in general, etc. Although the molecular base of these diseases are often complex, the fact that most of them have been linked with abnormal MAO activity provides a biochemical rationale for further pursuit of their investigation [3]. In contrast, little is known about distribution of MAO in peripheral tis-sues. The enzymes have been identified outside the central nervous system in organs such as liver, kidney and intestine [4]. Studies of the biochemical properties of MAO are
A d d r e s s f o r c o r r e s p o n d e n c e :MVDr. Jozef Mihalik, CSc., Department of Anatomy, P.J. Safarik University, Medical FacultySrobarova Str. N. 2, 040 01 Kosice, Slovak Republic, Phone: ++ 421 055 6228866; e-mail: [email protected]
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0002-z

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 15
numerous, but information about the quantification of MAO in female gonads during pregnancy is limited.
Recently we have observed an antagonistic effect of chronic treatment with deprenyl, a potent MAO-B inhibitor, at the dose 0.25 mg/kg on embryo development in rats. Sig-nificantly less degenerated embryos were isolated from experimental females, but on the other hand, a decreased mean cell number in blastocysts was recorded [5]. Our objectives in the present study were to determine the activity of MAO in rat ovary, oviduct and uterus during preimplantation period of pregnancy, which should help us to clarify and better understand possible involvement of both MAO enzymes in the reproductive process.
MAtERIAL AnD MEtHODS
AnimalsAll procedures performed with animals adhered to the permission granted by the Com-
mittee for Ethical Control of Animal Experiments at Safárik University and the permis-sion of the State Veterinary and Food Administration of the Slovak Republic (permission No. 715/08-221b). All efforts were made to minimize both the number of animals and their suffering.
Experiments were carried out on 15 young, virgin female Wistar rats (200-240 g, 85-90 days old) obtained from the animal facility of the University. The animals were given free access to standard diet and water and were maintained in a 12 h light/12 h dark cycle. Fe-males were mated for two hours from 07:00-09:00 a.m. with males of the same strain. The first day on which a vaginal plug was present was designated as day 1 of pregnancy. Preg-nant rats were killed by a lethal dose of thiopental (40 mg/kg; ICN Czech Pharma, Prague, Czech Republic) on the first (D1), on the third (D3), and on the fifth (D5) day of pregnancy.
After a lethal injection of thiopental rats were perfused transcardially with 100 ml of room-temperature PBS (ph 7.4) to rinse out as much blood as possible. Ovaries, ovi-ducts, and uteri were immediately removed and stored in Eppendorf tubes at -80 °C until the measurement was done.
MAO AB activityActivity of MAO was measured by fluorescent monoamine oxidase detection kit (Ba-
chem; Cat. No. S-90092) based on detection of H2O2 released from the conversion of a substrate to its aldehyde via both forms MAO A and MAO B. H2O2 oxidizes the detection reagent in a 1:1 stoichiometry to produce the fluorescent product. A standard curve was prepared from resorufin to determine moles of product produced.
Briefly, organs were homogenized in five volumes (w/v) of the 25mmol/l TRIS-HCL (pH 7.4) mixed with 1mmol/l EDTA and subsequently were centrifuged at 10,000xg for 15 min at 4 °C. To a black 96 well plate 100 ml of samples and 100 ml of reaction cocktail were added into individual wells to incubate at room temperature for 30-60 minutes. Reaction cocktail was prepared obeying the manufacturer’s instructions and consisted of the detection reagent, horse radish peroxidase and dimethyl sulfoxide (DMSO). Sam-ples were read using excitation at 570 nm and fluorescence was measured at 590-600 nm employing the fluorescence plate reader. Activity of MAO expressed as the µmol/l resorufin was normalized on the basis of total protein content (µmol/l of resorufin/mg of protein). Chemicals used for assessing of enzymes activity were purchased from Sigma-Aldrich (St. Louis, MO, USA).
Statistical analysisData are expressed as the mean ± SD. Differences in the MAO AB activity were analyzed by
the Kruskal-Wallis test for multiple comparisons. P<0.05 was considered as significant. The data presented here are pooled from two independent replications of the same experiment.
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 116
RESULtS
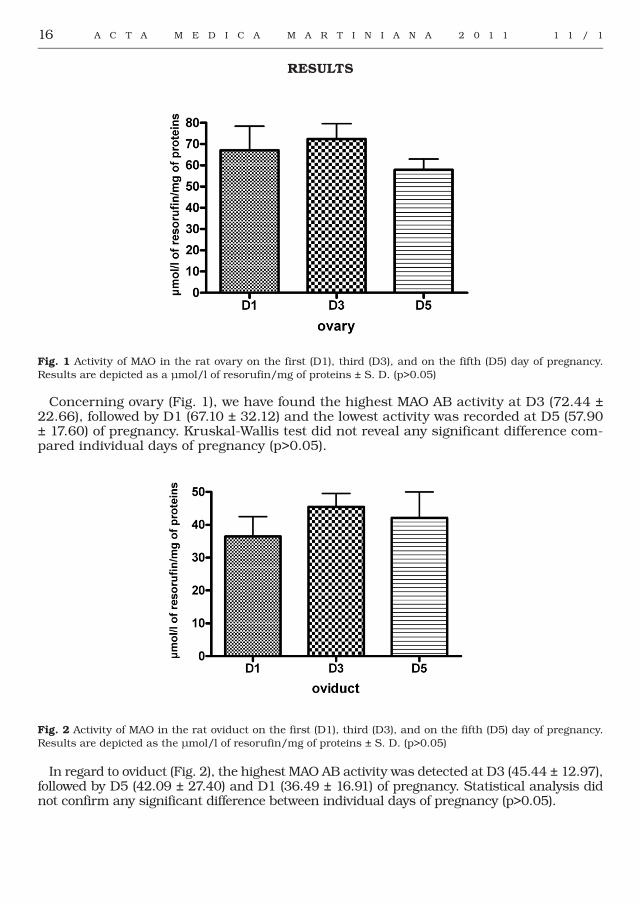
Fig. 1 Activity of MAO in the rat ovary on the first (D1), third (D3), and on the fifth (D5) day of pregnancy. Results are depicted as a µmol/l of resorufin/mg of proteins ± S. D. (p>0.05)
Concerning ovary (Fig. 1), we have found the highest MAO AB activity at D3 (72.44 ± 22.66), followed by D1 (67.10 ± 32.12) and the lowest activity was recorded at D5 (57.90 ± 17.60) of pregnancy. Kruskal-Wallis test did not reveal any significant difference com-pared individual days of pregnancy (p>0.05).
Fig. 2 Activity of MAO in the rat oviduct on the first (D1), third (D3), and on the fifth (D5) day of pregnancy. Results are depicted as the µmol/l of resorufin/mg of proteins ± S. D. (p>0.05)
In regard to oviduct (Fig. 2), the highest MAO AB activity was detected at D3 (45.44 ± 12.97), followed by D5 (42.09 ± 27.40) and D1 (36.49 ± 16.91) of pregnancy. Statistical analysis did not confirm any significant difference between individual days of pregnancy (p>0.05).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 17
Fig. 3 Activity of MAO in the rat uterus on the first (D1), third (D3), and on the fifth (D5) day of pregnancy. Results are depicted as the µmol/l of resorufin/mg of proteins ± S. D. (* it means p<0.001)
Uterus (Fig. 3) was the only organ, in which statistically significant differences were detected (p<0.001). The highest activity of MAO AB was observed at D5 (75.48 ± 53.24), followed by D1 (13.94 ± 6.09) and D3 (6.30 ± 3.19) of pregnancy.
DISCUSSIOn
We have found that monoamine oxidases activity undergo changes during early stages of pregnancy in all female reproductive organs examined, but their levels statistically differ only in the uterus.
Sympathetic nerve fibers are the largest source of NA in the ovary, but not the only one. Ovarian granulose cells, after taking up catecholamines, can serve as an intrao-varian catecholamine-storing compartment, releasing them in a regulated way [6]. High concentrations of both catecholamines NA and DA were found in the stroma of bovine ovaries and corpora lutea (CL), too [7]. NA given into the abdominal aorta affected the secretory function of the corpus luteum by stimulation of the luteal adrenoreceptors [8] in cattle and also in other species [9]. Tonic beta-adrenoreceptor stimulation of the CL ensures the basal secretion of progesterone, whereas acute noradrenergic activa-tion supports the CL during stressful situations that could impair its function [10]. NA was also determined in the preovulatory follicular fluid of women undergoing in vitro fertilization. All of the follicular samples contained NA at concentrations substantially higher than those in the corresponding plasma samples. The data indicate that NA ac-cumulates in follicular fluid, supporting the physiological significance of NA in the local regulation of human ovarian functions [11].
High levels of DA were described in the human ovary, raising question about its role in the female gonad [12]. It has been reported that monkey (Macaca mulatta) oocytes are able to take up DA and use it as a precursor for the synthesis of NA with the help of the dopamine-β-hydroxylase [13]. Bovine luteal cells are reported to perform synthesis of NA in a similar way [14], and presumably this occurs also in intraovarian nerve fibers, which likewise express dopamine-β-hydroxylase [15]. Recent study revealed dopamine 1,2,4,5 receptors expressed by endocrine cells of the follicle and the corpus luteum, which suggests a complex role of DA in the regulation of ovarian processes [16].
In the light of findings described above there is no surprise that the activity of MAO enzymes, which are responsible for the degradation of the catecholamines, was observed

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 118
in the CL of rat ovary employing enzymatic histochemical method [17]. In our work we found the highest MAO activity on the D3 of pregnancy, when corpora lutea are already formed. Similar results were recorded in women employing monoclonal antibodies. MAO-A was intensely expressed in CL of pregnancy, especially in large luteal cells [18]. MAO enzymes were also detected in the intersticial gland cells and in the blood vessels of rat ovary [17]. It has been recorded [19], that MAO activities in the vessels of ovarian pedicle of pigs were the highest on the 13-14 day of the estrous cycle. Authors suggest that high MAO activity in the vessels may be a significant factor in the regulation of the ovarian vasotone and might be responsible for increasing in the ovarian blood flow during the luteal phase of ovarian cycle. Interstitial glands are situated near to the blood vessels in the ovarian stroma, and arise from the follicles, which undergo atrophic process. Prob-ably this is the reason why the further catecholamine accumulation is not needed and these substances are rather metabolized through MAO enzymes. Taken together, results suggest that MAO activity in the ovary might be involved in follicular development and progesterone metabolism.
High concentrations of NA have been detected in the human and cow oviductal com-partments [20, 21]. The highest concentrations were found in the isthmus, where the adrenergic nerves are primarily related to smooth muscles [20]. Recently we have found that high doses of deprenyl (2.5 mg/kg), a potent MAO-B inhibitor, significantly slow down the movement of rat embryos through the female reproductive tract [22]. These findings need another investigation, because MAO-B and MAO-A are responsible for the DA degradation and DA was also detected in the human [20] and cow [21] oviduct com-partments. Moreover, the addition of DA into the incubation bath significantly reduced the strength and frequency of spontaneous rhythmic contractions of the rat uterus [23]. NA was also identified in bovine oviductal fluid [24], and it could influence the oviduct epithelium via adrenergic receptors, which have been shown in the oviduct epithelian cells of several species [25, 26]. Recently, it was clearly demonstrated that mouse oo-cytes and embryos express α2C- and β2-adrenergic receptors, too [27]. As one could ex-pect, MAO activity in the human oviduct has been detected on the same places, as their catecholamine substrates are located. It means in the epithelium and in the muscular layer [28]. Despite the fact that we have recorded the highest activity of monoamine oxi-dases on D3 and on D5, when embryo goes through the oviduct into the uterus, activity of MAO did not differ significantly compared the individual days of pregnancy. Probably, it could be the sign of similar metabolic MAO activity, as the oviduct almost permanently moves during the transport of spermatozoa in the time of fertilization and subsequently during the embryo passage down into the uterine cavity. Based on the works mentioned above, catecholamines play the pivotal role in this process.
Uterus is the only one reproductive organ, in which significantly different MAO activity during preimplantation period of pregnancy was recorded. In the time, when the oocytes and subsequently embryos are located in the oviduct, extremely low MAO activity in rat uterus was detected. However, on the D5, when embryos are present in the uterine cavity and their implantation into the uterine wall occurs, MAO activity significantly increased several times. Successful implantation depends both on the quality of the embryo and on the endometrial receptivity. The later depends on the progesterone-induced changes in gene expression. One of the genes whose transcription appears to be enhanced during the receptive period is probably gene for MAO. Similar results were obtained in women [29]. MAO-A transcript levels increased in human uterus between the pre-receptive and recep-tive phase with a median increase of 25-fold. Conversely, prior failure of embryo implan-tation was associated with a 29-fold decrease in MAO-A mRNA levels and a substantial reduction in MAO-A protein immunofluorescent label score. These results show a strong association between endometrial receptivity and MAO-A expression in the endometrial epithelium, suggesting an important role for this enzyme in normal implantation.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 19
In the present study, we determined activity of monoamine oxidases in rat ovary, oviduct and uterus on the first, on the third and on the fifth day of pregnancy. We can conclude that significant elevation of MAO activity was recorded in the rat uterus in the time of embryonic implantation. The data obtained extend our knowledge about MAO enzymes in rat reproductive organs during early period of embryo development. To our knowledge this is the first paper describing the MAO activity in female reproductive or-gans during the whole preimplanation period of pregnancy in mammals.
Acknowledgement: This research work was supported by the VEGA Agency [grant 1/4227/07].
REFEREnCES
1. Singer TP, Ramsay RR. Monoamine oxidases; old friends hold many surprises. FASEB J 1995; 9: 605-10.2. Saura J., Bleuel Z., Ulrich J., Mendelowitsch A., Chen K., Shih J. C., Malherbe P., Da Prada M., Richards
J. G. Molecular neuroanatomy of human monoamine oxidase A and B revealed by quantitative enzyme radioautography and in situ hibridization histochemistry. Neuroscience 1996; 70: 755-74.
3. Keung WM. Monoamine oxidase inhibitors. Expert Opin. Ther Pat 2002; 12: 1813-29.4. Rodríguez M. J., Saura J., Billet E. E., Finch Ch. C., Mahy N. Cellular localization of monoamine oxidase
A and B in human tissues outsider of the central nervous system. Cell Tissue Res 2001; 304: 215-20.5. Mihalik J, Špakovská T, Prokopčáková L, Schmidtová K. Antagonistic effect of low deprenyl dose on the
preimplantation embryo development in rat. Bratislava Medical Journal 2008a; 109: 151-1546. Greiner M, Paredes A, Rey-Ares V, Saller S, Mayerhofer A, Lara HE. Catecholamine uptake, storage, and
regulated release by ovarian granulosa cells. Endocrinology 2008; 149(10): 4988-96.7. Denning-Kendall PA, Wild ML, Wathes DC. Regional differences in catecholamine concentrations in
bovine ovaries analysed by high-performance liquid chromatography. J Endocrinol 1991; 129(2): 221-6.8. Miszkiel G, Kotwica J. Mechanism of action of noradrenaline on secretion of progesterone and oxytocin
by the bovine corpus luteum in vitro. Acta Vet Hung 2001; 49(1): 39-51.9. Kotwica J. Role of the noradrenergic system in the secretory function of the corpus luteum. J Physiol
Pharmacol 1992; 43(4 Suppl 1): 131-42.10. Kotwica J, Bogacki M. Physiological importance of dopamine as a noradrenaline precursor in the corpus
luteum. Clin Exp Pharmacol Physiol Suppl 1999; 26:S29-35.11. Itoh MT, Ishizuka B, Kuribayashi Y, Abe Y, Sumi Y. Noradrenaline concentrations in human preovulatory
follicular fluid exceed those in peripheral plasma. Exp Clin Endocrinol Diabetes 2000; 108(8): 506-9.12. Bodis J, Bognar Z, Hartmann G, Török A, Csaba IF. Measurement of noradrenaline, dopamine and
serotonin contents in follicular fluid of human Graafian follicles after superovulation treatment. Gynecol Obstet Invest 1992; 33: 165-7.
13. Mayerhofer A, Smith GD, Danilchik M, Levine JE, Wolf DP, Dissen GA, Ojeda SR. Oocytes are a source of catecholamines in the primate ovary: evidence for a cell-cell regulatory loop. Proc Natl Acad Sci USA 1998; 95: 10990-5.
14. Kotwica J, Bogacki M, Rekawiecki R. Neural regulation of the bovine corpus luteum. Domest Anim Endocrinol 2002; 23: 299-308.
15. D’Albora H, Anesetti G, Lombide P, Dees WL, Ojeda SR. Intrinsic neurons in the mammalian ovary. Microsc Res Tech 2002; 59: 484-9.
16. Rey-Ares V, Lazarov N, Berg D, Berg U, Kunz L, Mayerhofer A. Dopamine receptor repertoire of human granulose cells. Reprod Biol Endocrinol 2007; 5: 40.
17. Yoshimoto Y, Sakumoto T, Arai R, Miyake A, Kimura H, Aono T, Tanizawa O, Maeda T. Monoamine oxidase in rat ovary during the estrous cycle. A histochemical study by a new coupled peroxidatic oxidation method. Endocrinology 1986; 119(4): 1800-4.
18. Takao Y, Fujiwara H, Yoshioka S, Fujii S, Ueda M. Monoamine oxidase A is highly expressed by the human corpus luteum of pregnancy. Reproduction 2008; 136(3): 367-75.
19. Dynarowicz I, Szurmiński M. Monoamine oxidase activity in the uterine and mesenteric arteries, vessels of ovarian pedicle and myometrium of pigs during the oestrous cycle. Arch Vet Pol 1995; 35(1-2): 45-52.
20. Helm G, Owman CH, Rosengren E, Sjöberg NO. Regional and cyclic variations in catecholamine concentration of the human Fallopian tube. Biol Reprod 1982; 26: 553-8.
21. Kotwica G, Kurowicka B, Franczak A, Grzegorzewski W, Wrobel M, Mlynarczuk J, Kotwica J. The concentrations of catecholamines and oxytocin receptors in the oviduct and its contractile activity in cows during the estrous cycle. Theriogenology 2003; 60: 953-64.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 120
22. Mihalik J, Kravčuková P, Špakovská T, Mareková M, Schmidtová K. Study of high deprenyl dose on the preimplantation embryo development and lymphocyte DNA in rat. Gen Physiol Biophys 2008; 27: 121-6.
23. Czerski A, Zawadzki W, Zawadzki M, Czerska Z. Influence of dopamine on rat uterine motility in vitro. Acta Vet Brno 2005; 74: 9-15.
24. Way AL, Barbato GF, Killian GJ. Identification of norepinephrine in bovine oviductal fluid by high performance liquid chromatography. Life Sciences 2001; 70: 567-76.
25. Tolszczuk M, Pelletier G. Autoradiographic localization of beta-adrenergic receptors in rat oviduct. Mol Cell Endocrinol 1988; 60: 95-9.
26. Einspanier R, Gabler C, Kettler A, Kloas W. Characterization and localization of B2-adrenergic receptors in the bovine oviduct: indication for progesterone-mediated expression. Endocrinology 1999; 140: 2679-84.
27. Čikoš Š, Veselá J, Iľková G, Rehák P, Czikková S, Koppel J. Expression of beta adrenergic receptors in mouse oocytes and preimplantation embryos. Mol Reprod Dev 2005; 71: 145-53.
28. Donnez J, Goenen E, Casanas-Roux F, Caprasse J, Ferin J, Thomas K. Monoamine oxidase reactivity in the human fallopian tube. Fertil Steril 1995; 43(3): 488-90.
29. Henriquez S, Tapia A, Quezada M, Vargas M, Cardenas H, Rios M, Salvatierra AM,Croxatto H, Orihuela P, Zegers-Hochschild F, Munroe DJ, Velasquez L. Deficient expression of monoamine oxidase A in the endometrium is associated with implantation failure in women participating as recipients in oocyte donation. Mol Hum Reprod 2006; 12(12): 749-54.
Received: December,14,2010Accepted: January,10,2011

21
REnAL OntOGEnY OF P-GLYCOPROtEIn/MDR1 In RAt
Hodorova I.1, Mihalik J.1, Vecanova J.1, Dankova M.2, Rybarova S.1
1Department of Anatomy, P. J. Safarik University, Faculty of Medicine, Kosice, Slovak Republic; 2Department of Histology and Embryology, P. J. Safarik University, Faculty of Medicine, Kosice, Slovak Republic
ABStRACtBACKGROUND: P-glycoprotein (Pgp/MDR1) is an ATP-dependent, integral plasma-membrane efflux pump that is constitutively expressed on adult apical brush-border epithelium of renal proximal tubules. This Pgp/MDR1 tissue distribution and localization affects the absorption, distribution, metabolism, and excretion of Pgp/MDR1 substrates. The ontogeny of rat Pgp/MDR1 is still doubtful, and such knowledge may be helpful in understanding age-related pharmacokinetics. The purpose of this study was to determine, whether Pgp/MDR1 expression is altered during development.METHODS: Postnatal expression of Pgp was determined using immunohistochemical method. Tissue from Wistar rat were isolated on the 1st day (D1), 7th day (D7), 14th day (D14), 21st day of life (D21) and from adult animals (60 days old; Ad). RESULTS: Our ontogeny study illustrated that expression of Pgp was relatively constant from birth to adulthood.CONCLUSIONS: Knowledge of the ontogeny of transport proteins involved in distribution and elimination of drugs is important for adequate interpretation of the results of toxicity studies in juvenile animals.
Key words: Pgp/MDR1, rat, immunohistochemistry
IntRODUCtIOn
ATP-binding cassette (ABC) superfamily now includes about 300 proteins, among the transporters of quite different compounds (1,2,3). Proteins of this family are present in all living organisms. About fifty ABC proteins have been found in man and approximate-ly the same number in mouse (4). Since a great number of ABC proteins were discovered only recently, many of them are still poorly studied. Studies of ABC proteins are impor-tant both for medicine and biology because they concern problems of protection of all living cells. Human proteins of the ABC family are divided to seven subfamilies (class A to G) (4,5). The affiliation of each protein to a subfamily is determined by its domain or-ganization, namely by the number and combination of transmembrane domains (TMDs) and ATP-binding domains (NBDs, nucleotide-binding domains) (6). In total, there are 49 protein members in this family, but only three are well known for their multidrug resist-ance (7). There are P-glycoprotein (Pgp/MDR1, ABCB1), MDR-associated protein (MRP1, ABCC1) and breast cancer resistance protein (BCRP, ABCG2). Pgp, paradigm ABC drug efflux transporter, is the first detected and to date the best characterized of the family of ABC drug efflux transporters. It gained worldwide attention about three decades ago for its role in the phenomenon of multidrug resistance in tumor cells (8,9). Subsequently, constitutive expression of Pgp/MDR1 has been described in a variety of other tissues in-cluding liver, intestine, kidney, pancreas, adrenal, capillary endothelium of blood-brain and blood-testis barrier, choroid plexus, placental trophoblast and others (10). The po-larized, apical membrane localization of Pgp/MDR1 causes that its substrates are prefe- erentially translocated from basolateral to the apical side of the epithelium. Thus, Pgp/MDR1 limits the influx and facilitates the efflux of its substrates, eventually preventing their intracellular accumulation. Many in vitro and in vivo studies demonstrated high
A d d r e s s f o r c o r r e s p o n d e n c e :Hodorova Ingrid, MD, PhD, Department of Anatomy, P.J. Safarik University, Medical FacultySrobarova Str. N. 2, 040 01 Kosice, Slovak Republic, Phone: ++ 421 055 6228866; e-mail: [email protected]
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0003-y

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 122
impact of Pgp/MDR1 on drug pharmacokinetics in these organs (10). It is likely that Pgp/MDR1 and other ABCs have evolved in these “normal” tissues to protect them from potentially damaging effect of toxic compounds.
In the kidney, Pgp/MDR1 is expressed mainly at the apical (luminal) brush-border mem-brane of proximal tubular cells (11) and to lesser extent in the thick limb of Henle’s loop, collecting ducts, and glomerular mesangium. Many substances are actively transported by Pgp/MDR1, e.g. calcium channel blockers, immunosuppressants, cardioactive glycosides, antibiotics, antineoplastic and severel others peptides and steroids (12,13). Thus Pgp/MDR1 functions as an efflux pump which represents a protective mechanism to exclude endog-enous and exogenous toxins from normal cells and to ultimately excrete them into the bodily secretions. In humans, two genes (MDR1 and MDR2) encode this protein, whereas in rodents there are three homologs of this protein, mdr1 (mdr1b), mdr2, mdr3 (mdr1a) (14,15,16).
The aim of the present study was to determine postnatal expression of Pgp/MDR1 in rat kid-ney by two widely used monoclonal antibodies for Pgp/MDR1: C219 and UIC2 .These antibodies are known to detect Pgp/MDR1 in paraffin-embedded histological tissue in many histopatho-logical laboratories. The neonatal rat is a useful model for kidney developmental studies since rats are born with immature kidneys and there is considerable postnatal renal development.
MAtERIAL AnD MEtHODS
AnimalsAll procedures performed with animals adhered to the permission of the Committee for
Ethical Control of Animal Experiments at Safarik University and the permission of the State Veterinary and Food Administration of the Slovak Republic (permission No. 7881/04-220/3). All efforts were made to minimize both the number animals and their suffering.
To acquire rat cubs, female Wistar rats were mated with males of the same strain over-night. Tissue from Wistar rat were isolated on the 1st day (D1), 7th day (D7), 14th day (D14), 21st day of life (D21) and from adult animals (60 days old; Ad) by ether anaesthesia. Three animals were killed on each day examined. The kidneys were obtained by medial laparotomy carried out in deeply anaesthetised animals. At the end of surgery rats were killed by overdose of ether. Rat kidneys were immersed in a neutral buffered formalin solu-tion for 72 hours at room temperature. Tissue blocks were dehydrated in increasing alco-hols and embedded in paraffin. Seven-micron-thick serial sections were cut and attached to the slide with alum gelatine. The slides were processed for immunohistochemistry.
Antibodies:We have used the following primary monoclonal antibodies: mouse anti-MDR1, clone
C219 (Signet Laboratories, Inc.) and mouse anti-MDR1, UIC2 – clone C494 (Santa Cruz Biotechnology, Inc.).
Immunohistochemical detection of Pgp:For immunohistochemistry, paraffin embedded sections of the rat kidney were deparaffinized
with xylene and rehydrated in decreasing ethanols to water. The slides were finally washed in phosphate-buffered saline containing 0.05 % Tween-20 (PBS-Tw), pH 7.6. Endogenous peroxi-dase activity was blocked by 0.3 % H202 in methanol for 30 minutes at room temperature. To re-establish an original conformation of epitopes modified after fixation, we performed antigen retrieval using a microwave (in sodium citrate solution for 2x5 minutes at 500 watts). Pgp/MDR1 staining procedure continued by blocking nonspecific staining with milk buffer (5 % dry milk in TRIS buffer) for 30 minutes at room temperature. Primary antibodies were applied overnight in humidified chamber at 4˚C. After rinsing in PBS-Tw (3x5 minutes) the sections were subsequently incubated with the secondary antibody (30 minutes) and strepatavidin-

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 23
biotin (30 minutes) (Universal detection kit LSAB+KIT/HRP, Dako). Next, the sections were visualized with DAB (3.3’- diaminobenzidine tetrahydrochloride) at a concentration of 0.5 mg/ml in Tris buffer, pH 7.6 and 0.015 % H2O2. Slides were stream-rinsed with tap water, coun-terstained with Mayer’s hematoxylin for 2 minutes, washed in tap water, dried, mounted and coverslipped. Sections processed with omission of primary antibody served as control.
Semiquantitative evaluationImmunostaining was assessed by two independent observers blinded to animal
characteristics.Expression of Pgp/MDR1 was evaluated separately using the following scale: 3+ =
high level (91-100 % of positive cells), 2+ = medium level (11-90 % of positive cells), 1+ = low level (up to 10 % of positive cells), – = negative cells (0 % of positive cells). Samples with high [3+] and medium level [2+] of proteins expression were considered as positive. Samples scored as [1+] and [–] were considered as negative.
RESULtS
Kidney of rat cubsUsing monoclonal antibody mouse anti-MDR1 clone C219 we have detected moderate
immunopositivity for Pgp/MDR1 in all developmental stages (D1, D7, D14, D21). Em-ploying semiquantitative evaluation of tissue samples we have found no differences in expression of Pgp/MDR1 in epithelial cells of proximal tubules. The remaining structures (epithelial cells of distal tubules, glomerulus and glomerular capsule) did not show any positivity for Pgp/MDR1.
Using monoclonal antibody mouse anti-MDR1 UIC2 – clone C494 we have detected in all de-velopmental stages the same spatial protein distribution but its signal was significantly weaker.
Kidney of rat adultsUsing both monoclonal antibodies (mouse anti-MDR1:clone C219 and mouse anti-
MDR1:UIC2 – clone C494) we have observed expression of Pgp/MDR1 in epithelial cells of proximal tubules in adult kidney, too. Employing semiquantitative evaluation we have found no differences in expression of Pgp/MDR1 in all tissue samples. The immunoreactivity for this protein was strongly restricted to the apical membrane and weakly to the cytoplasm of proximal tubular cells. No signal for this protein in the other cells of rat kidney was found.
A B
Fig. 1. 1-day old rat kidney – D1. Immunohistochemical detection of Pgp/MDR1 by monoclonal antibody: mouse anti-MDR1 - clone C219 (A), UIC2 – clone C494 (B). Positive expression of Pgp/MDR1 in proximal tubular epithelial cells of rat kidney – cytoplasmic staining (A, B).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 124
A B
Fig. 2. Pgp/MDR1 was expressed in epithelial cells of proximal tubules in 7-day old rat kidney - D7 (A) and adult kidney (B) by mononoclonal antibody: mouse anti-MDR1 – clone C219. The remaining structures (epithelial cells of distal tubules, glomerulus and glomerular capsule) did not show any positivity for Pgp/MDR1.
DISCUSSIOn
Knowledge of the ontogeny about transport proteins involved in distribution and elimi-nation of drugs is important for adequate interpretation of the results of safety studies in juvenile animals. Since rat is one of the most frequently species used in non-clinical testing we used this species in our study on the age-dependent changes in Pgp/MDR1 expression. We focused on the age shortly after birth until early adulthood of the animals (D1, D7, D14, D21, Ad). The transport proteins in the kidney are involved in the passage of compound through the tubular epithelial cells, prior to urinary excretion. Urinary excre-tion of drugs is a complex interplay of three mechanisms: glomerular filtration, tubular secretion, and tubular reabsorption. The basic prerequisite for excretion into urine is water solubility of drug and/or its metabolites as no transporting carrier is available in this body fluid. Accordingly, the primary mechanism for drug excretion is glomerular filtration, a passive process influenced by molecule size, concentration of unbound fraction of drug in plasma and renal blood perfusion. Tubular secretion and partly also reabsorption are ac-tive mechanisms requiring transporters. The function of renal proximal tubular epithelial cells is the most significant factor for active drug renal excretion (17).
The large differences in ontogeny of the individual transport proteins were observed, with some transporters having the highest expression at birth (MRP1 and MRP3), and other having a more or less constant expression during development (MRP2 and BCRP) (18). It was reported that Pgp/MDR expression increased up to Day 26, with a subse-quent decrease to adult levels at Day 42 (18). On the other hand, other authors found continuously increasing level of Pgp/MDR1 up to Day 60 (19). In our study we have found relatively constant levels of Pgp/MDR1 protein from the birth to the adulthood.
It should be noted that all our data on transport protein is limited to actual func-tionality of Pgp/MDR1. The mRNA expression of this transporter was not studied such as in previous mentioned publications. The reason for the differences between the data obtained in our study and those already published, as well as the differences between individual publications, are most likely related to differences in methodology (sample preparation, differences in diet, etc.).
Despite these differences, the results indicate that expression of majority of the trans-port proteins studied vary during development. Cellular and tissue distribution as well as elimination of transported substrates will therefore also change during development. Knowledge of these ontogenic differences in absorption, distribution, metabolism and excretion (ADME) processes of test compound in development may help to interpret dif-ferences in toxicity observed between adult, neonate and young animals.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 25
REFEREnCES
1. Ambudkar SV, Dey S, Hrycyna CA, Ramachandra M, Pastan I, Gottesman MM. Biochemical, cellular, and pharmacological aspects of the multidrug transporter. Annu Rev Pharmacol Toxicol. 1999; 39:361-98. Review.
2. Stavrovskaya AA. Cellular mechanisms of multidrug resistance of tumor cells. Biochemistry (Mosc). 2000; 65(1):95-106. Review.
3. Higgins C. F. Multiple molecular mechanisms for multidrug resistance transporters.4. Nature 2007; 446, 749-757.5. Dean M, Rzhetsky A, Allikmets R. The human ATP-binding cassette (ABC) transporter superfamily.
Genome Res. 2001; 11(7):1156-66. Review. 6. Neyfakh AA. Mystery of multidrug transporters: the answer can be simple. Mol Microbiol. 2002;
44(5):1123-30. Review.7. Sarkadi B, Homolya L, Szakács G, Váradi A. Human multidrug resistance ABCB and ABCG transporters:
participation in a chemoimmunity defense system. Physiol Rev. 2006; 86(4):1179-236. Review. 8. Stavrovskaya AA, Stromskaya TP. Transport proteins of the ABC family and multidrug resistance of
tumor cells. Biochemistry (Mosc). 2008; 73(5):592-604. Review. 9. Bosch I, Croop J. P-glycoprotein multidrug resistance and cancer. Biochim Biophys Acta. 1996;
1288(2):F37-54. Review.10. Goldstein LJ, Gottesman MM, Pastan I. Expression of the MDR1 gene in human cancers. Cancer Treat
Res. 1991; 57:101-119. Review. 11. Schinkel AH, Jonker JW. Mammalian drug efflux transporters of the ATP binding cassette (ABC) family:
an overview. Adv Drug Deliv Rev. 2003; 55(1):3-29. Review. 12. Thiebaut F, Tsuruo T, Hamada H, Gottesman MM, Pastan I, Willingham MC. Cellular localization of the
multidrug-resistance gene product P-glycoprotein in normal human tissues. Proc Natl Acad Sci U S A. 1987; 84(21):7735-7738.
13. Ernest S, Bello-reuss E. P-glycoprotein functions and substrates: possible roles of MDR1 gene in the kidney. Kidney Int 1998; 65: S11-S17.
14. Shinkel AH. The physiological function of drug-transporting P-glycoproteins. Semin Cancer Biol 1997; 8:161-170.
15. Eraly SA, Blantz RC, Bhatnagar V, Nigam SK. Novel SK. Novel aspects of renal organic anion and cation transporters. Curr Opin Nephrol Hypertens 2003; 12: 551-558.
16. Gottesman MM and Pastan I. Biochemistry of multidrug resistance mediated by multidrug transporter. Annu Rev Biochem 1993; 62: 385-427.
17. Inui KI, Masuda S, Saito H. Cellular and molecular aspects of drug transport in the kidney. Kidney Int 2000; 58: 944-958.
18. Lash LH, Putt DA, Cai H. Drug metabolism enzyme expression and activity in primary cultures of human proximal tubular cells. Toxicology 2008, 244:56-65.
19. de Zwart L, Scholten M, Monbaliu JG, Annaert PP, Van Houdt JM, Van den Wyngaert I, De Schaepdrijver LM, Bailey GP, Coogan TP, Coussement WC, Mannens GS. .The ontogeny of drug metabolizing enzymes and transporters in the rat. Reprod Toxicol. 2008, 26(3-4):220-230.
20. Rosati A, Maniori S, Decorti G, Candussio L, Giraldi T, Bartoli F. Physiological regulation of P-glycoprotein, MRP1, MRP2 and cytochrome P450 3A2 during rat ontogeny. Dev Growth Differ. 2003 Aug;45(4):377-387.
Acknowledgement: This work was supported partly by grant VEGA 1/0388/08 and partly by grant VVGS 25/10-11.
Received: November,12,2010Accepted: December,16,2010
26
InVEStIGAtInG DYSPEPSIA In CLInICAL PRACtICE – A tRAP FOR GIARDIA
Banovcin P. Jr., Demeter M., Bozikova J., Hyrdel R.
Department of Internal Medicine - Gastroenterology, Jessenius Faculty of Medicine, Commenius University and University Hospital Martin, Slovak Republic
ABStRACtIntroduction: Dyspepsia is a very common condition with significant morbidity and economic implications. Dyspeptic symptoms have heterogeneous pathogenic mechanisms, including several organic, systemic or extragastrointestinal causes, however, origin of the most cases of dyspepsia remains unclear. This study aimed to focus on potential causes in patients with nonspecific dyspeptic symptoms in absence of organic, systemic or biochemical and hematological findings that readily explain their symptoms. Methods: We studied presence of persistent abdominal symptoms (heartburn, dull epigastric pain, epigastric cramps, epigastric fullness, flatulence, diarrhoea), weight loss. All patients (116 patients, 29 males/87 females) had normal laboratory tests, negative abdominal ultrasound evaluation and upper endoscopy findings. Presence of Giardia intestinalis (GI), Helicobacter pylori (HP) infection and coeliac disease (CD) was evaluated by obtaining biopsy samples and duodenal fluid aspiration during upper endoscopy. We determined the effect of eradication treatment on dyspepsia symptoms 2 months after therapy. Results: HP infection was present in 28 %, coeliac disease in 6 %, GI infection was diagnosed in 27 % patients GI and HP in 12 %, CD and HP in 1 %, GI and CD in 2 %. None of these causes were presented in 39 %. Most frequent symptoms were epigastric fullness (69 %), dull epigastric pain (38 %), heartburn (35 %), flatulence (34 %), abdominal cramps (31 %) and diarrhoea (16 %). We documented the remission of symptoms in 79 % examined patients 2 month after eradication therapy. Conclusion: The most common cause of dyspepsia was Helicobacter pylori infection and chronic giardiasis. Although H. pylori and coeliac disease are widely well known, we pointed out Giardia intestinalis as another possible cause of dyspepsia. Chronic giardiasis leads in selected individuals to dyspeptic symptomatology that mimics functional dyspepsia and irritable bowel syndrome. We recommend test for G. intestinalis infection in all patients with chronic dyspeptic complaints of unknown origin.
Key words: Dyspepsia, functional dyspepsia, Giardia intestinalis, Helicobacter pylori, coeliac disease
IntRODUCtIOn
Dyspepsia is a very common condition with significant morbidity and economic implica-tions. Around 25-40 % of adults in the general population have dyspepsia, but the preva-lence and incidence depend on population study design, observation period, and defini-tion of dyspepsia, itself (1,2). According to the Czech study, the prevalence of long-lasting dyspeptic symptoms in uninvestigated dyspepsia was 17 % (3). Dyspepsia accounts for 2-5 % of primary care consultations, but patients that are most affected often do not seek medical care (4). A large number of patients in clinical practice present symptoms such as epigastric pain, abdominal cramps, excessive belching, early satiation, postprandial fullness or nausea. The dyspeptic symptoms can have several organic, systemic or ex-tragastrointestinal causes. However, the origin of most of the cases of dyspepsia remains unclear. When these symptoms are chronic and occur in the absence of organic disease that readily explains them, patients are considered to have a functional gastroduodenal disorder (5). Functional dyspepsia remains a diagnosis of exclusion. The therapeutical
A d d r e s s f o r c o r r e s p o n d e n c e :Banovcin P.Jr. MD, Clinic of Internal Medicine, Gastroenterology Dept., Jessenius Faculty of MedicineCU and University Hospital in Martin, Kollarova Str. N. 2, 03601 Martin, Slovak Republic email: [email protected]
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0004-x

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 27
and diagnostical processes are often not optimal and still controversial. Due to these facts we focused on potential causes of non-specific dyspeptic symptomatology.
Giardia intestinalis (also known as Giardia lamblia and Giardia duodenalis) is an enteric protozoan pathogen found in a variety of mammalian hosts, including humans, and causes one of the most common parasitic infections worldwide. It contributes to estimate of 280 million symptomatic human infections per year (6). One of the major sources of infection in humans is contaminated water; however, there is evidence that the parasite is transmitted by human-to-human contact or by the contact with the domestic or wild animals (7). The symptoms of human giardiasis are highly variable. They vary from asymptomatic to severe form with diarrhoea, fever, weight loss and ma-labsorbtion. Most prominent clinical symptoms are abdominal pain, vague abdominal discomfort, bloating, flatulence and diarrhoea. Various extra-intestinal manifestations have been reported such as maculopapular rush, pulmonary infiltrates, polyarthritis and urticaria (8, 9). Chronic courses are common, but are mostly asymptomatic or pre-sented by non-specific mild symptoms that may result in a low clinical index of suspi-cion for the diagnosis. Chronic infection may be linked to the phenomenon of antigenic variation and individual response of the host. Recent data show that Giardia intestinalis infection has been found to trigger abdominal symptoms of functional gastrointestinal disorder such as irritable bowel syndrome or functional dyspepsia. (10,11,12)
MAtERIAL AnD MEtHODS
We enrolled to our study 116 patients (29 males/87 females) aged 18 years and over at-tending Gastroenterology Outpatient Unit due to chronic dyspeptic symptoms. Patients with persistent abdominal dyspeptic symptoms in duration at least 3 months were con-sidered for the study. Patient with the alarm features (such as dysphagia, odynophagia, vomiting, bleeding or rapid weight loss) as well pregnant women and patients familiarly for malignant disease were excluded. All patients underwent complex physical examina-tion, routine biochemical and hematological blood laboratory tests.
Furthermore, ultrasound evaluation including hepatobiliary tract, pancreas, kidneys and upper endoscopy were performed. All examination had not produced relevant explanation
for dyspepsia. Upper gastrointestinal endoscopy was accompanied by obtaining of multiplied biopsy samples from gastric antrum to investigate presence of Helicobacter pylori (H. pylori) infection. Duodenal biopsy samples (D2-D3) and serum anti-gliadin, anti-endomysial and anti-transglutaminase antibodies estimation was used to evalu-ate coeliac disease. Presence of Giardia intestinalis infection was performed by direct examination of duodenal juice aspirate. Aspiration of duodenal fluid was performed on the fasting patient, during the endoscopy so the position of the aspiration tube was cor-rectly placed in the distal duodenum or proximal jejunum. Aspirates were immediately transported in sterile containers in a tempered medium to microbiology laboratory. The samples were processed within 2 hours for microscopic examination.
We studied presence of H. pylori infection, G. intestinalis and coeliac disease and its relative contribution to overall dyspeptic symptoms (heartburn, dull epigastric pain, epi-gastric cramps, epigastric fullness, flatulence, diarrhoea). After identification of possible cause, appropriate treatment was initiated (eradication of H. pylori, gluten-free diet in coe-liac disease and therapy with metronidazole 250 mg tid. In the case of giadriasis, we de-termined the effect of eradication treatment on functional dyspepsia symptoms 2 months after therapy. Statistical analysis was performed using the program PAST version 1.80.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 128
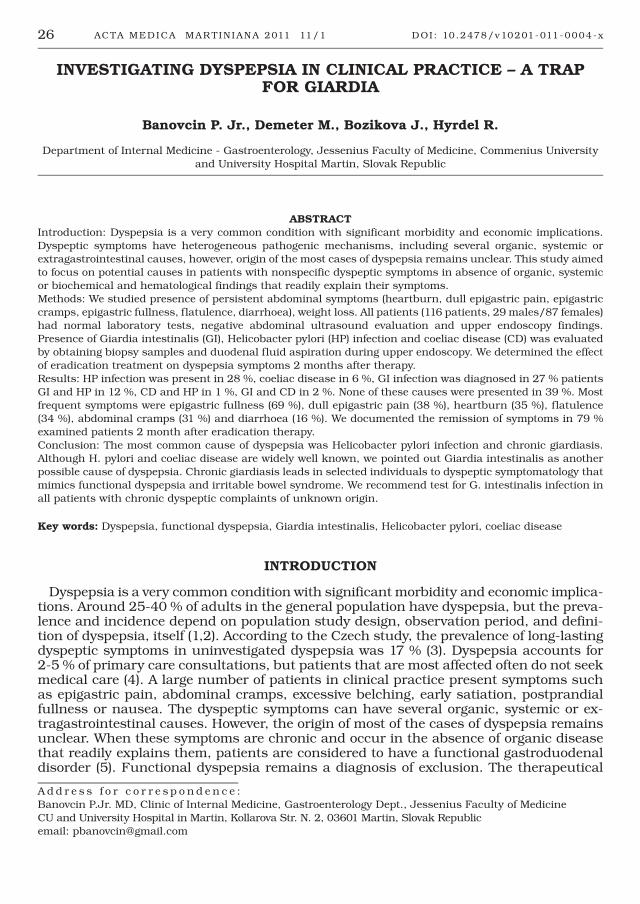
RESULtS
One hundred and sixteen patients (87F, 29M) fulfilled the inclusion criteria. The mean age of patients was 37.3 (18-67years). Giardia intestinalis infection was diagnosed in 27 % of the patients. H. pylori infection was found in 28 %, coeliac disease in 6 %. Both G. intestinalis and H. pylori were present in 12 %, coeliac disease and H. pylori in 1 %, giardiasis and coeliac disease in 2 %. There were 39 % of the patients that did not exem-plify any of the causes mentioned. Figure1. Most frequent symptoms were epigastric full-ness (69 %), dull epigastric pain (38 %), heartburn (35 %), flatulence (34 %), abdominal cramps (31 %), and diarrhoea (16 %) Figure 2. Comparing frequency of symptoms, we didn’t confirmed statistically significant differences among investigated groups. Average lenght of dyspeptic syndrome history was 18.5 months and average weight loss was 2 kg.
28%
6%
12%
1%2%
39%
27%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
GI -total HP - total CD - total HP + GI HP + CD GI + CD Unkonwn
Fig. 1. Summary of potential dyspepsia causes in study patients (totally). Giardia intestinalis (GI), Helicobacter pylori (HP) and coeliac disease (CD).
0%
10%
20%
30%
40%
50%
60%
70%
80%
Dull pain Cramps Heartburn Epigastricfullness
Flatulence Diarrhoea
Total=116Females n=87Males n=29
Fig. 2. Prevalence of selected dyspepsia symptoms in study patients (totally)
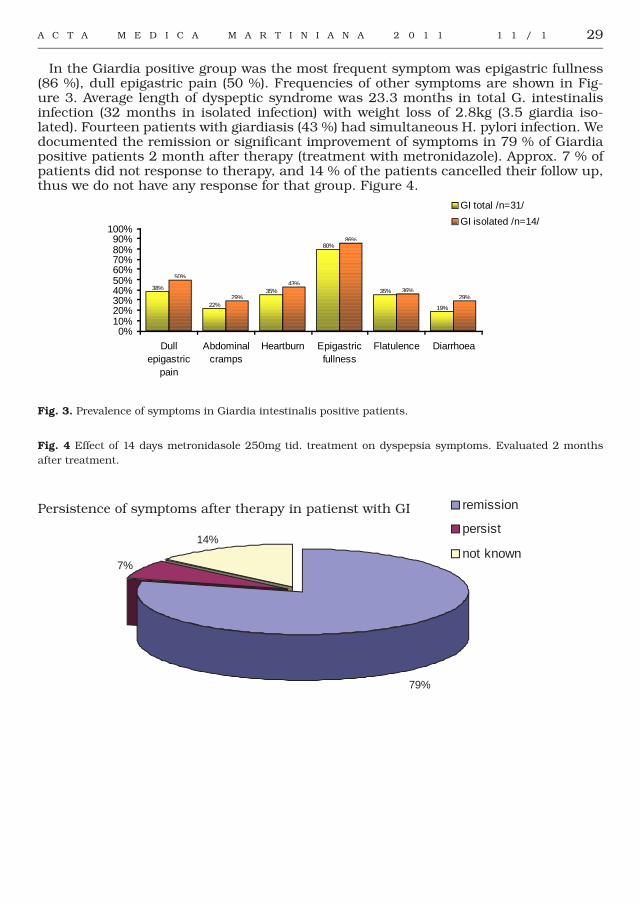
A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 29
In the Giardia positive group was the most frequent symptom was epigastric fullness (86 %), dull epigastric pain (50 %). Frequencies of other symptoms are shown in Fig-ure 3. Average length of dyspeptic syndrome was 23.3 months in total G. intestinalis infection (32 months in isolated infection) with weight loss of 2.8kg (3.5 giardia iso-lated). Fourteen patients with giardiasis (43 %) had simultaneous H. pylori infection. We documented the remission or significant improvement of symptoms in 79 % of Giardia positive patients 2 month after therapy (treatment with metronidazole). Approx. 7 % of patients did not response to therapy, and 14 % of the patients cancelled their follow up, thus we do not have any response for that group. Figure 4.
38%
22%
35%
80%
35%
19%
50%
29%
43%
86%
36%29%
0%10%20%30%40%50%60%70%80%90%
100%
Dullepigastric
pain
Abdominalcramps
Heartburn Epigastricfullness
Flatulence Diarrhoea
GI total /n=31/
GI isolated /n=14/
Fig. 3. Prevalence of symptoms in Giardia intestinalis positive patients.
Fig. 4 Effect of 14 days metronidasole 250mg tid. treatment on dyspepsia symptoms. Evaluated 2 months after treatment.
79%
7%
14%
remission
persist
not known
Persistence of symptoms after therapy in patienst with GI

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 130
DISCUSSIOn
Dyspepsia is common and global problem with board differential. This study aimed to focus on patients with nonspecific dyspeptic symptoms in absence of organic, sys-temic or biochemical and hematological findings that explain their symptoms. In order to prevent serious illness, patient complaining of alarm symptoms were excluded. The negative aspect of this study was our failure to fulfill the diagnosis of functional gastro-intestinal disorders according to ROME III criteria. However, the aim of the study was to identify other possible agents that may contribute to development of gastrointestinal symptoms. The role of H. pylori in functional disease has been controversial. Recent meta-analyses suggest some benefit from H. pylori eradication (13). In our findings was the H. pylori infection most common agent. After eradication therapy, 72 % of patients reported benefits from this therapy.
Coeliac disease was diagnosed in 6 %. As expected, flatulence fullness and diarrhoea were the dominant symptoms, but not significantly different from other groups. On the other hand, in our study were not sufficiently many patients with coeliac disease to conclude any decision.
Incidence of giardiasis varies from 20 % to 60 % in endemic areas and 2-7 % in indus-trialized countries depending on region and age (6). We found out that 27 % of studied patients had giardia infection. The rate is higher compared to general population in western countries mostly due to selection of symptomatic patients.
Traditional diagnosis of giardiasis is set by the direct detection of trophozoites or cysts in a stool sample; however, repeated stool examinations are needed to avoid false-nega-tive results, because cyst excretion may be intermittent. This may be difficult sometime in outpatient units because of patient compliance. The data show that histological ex-amination of duodenal biopsies is unsuitable (15,16,17). In recent years, rapid diagnos-tic tests that use antigen detection methods or PCR have been employed. These tests are both highly specific and sensitive, but still expensive (14). The specificity and sensitivity is also questionable in case of chronic giardiasis. Diagnosis of Giardia intestinalis in our study was performed by microscopic evaluation of duodenal juice aspirate. There are studies that show yields of microscopic examination of duodenal aspirate that vary from 0.7 % to 47.6 % (15,16). There is disadvantage to duodenal fluid aspiration in that it is performed during endoscopy therefore it is not suitable for routine screening. Another disadvantage of this evaluation is that aspirate should be preceded within 2 hours of aspiration and transported in temperate medium.
Giardia intestinalis infection in humans has a wide spectrum of clinical manifestation ranging from asymptomatic to serious diarrhoea. In our study the most frequent symp-tom was abdominal fullness and diarrhoea followed by heartburn, dull epigastric pain abdominal cramps, and flatulency. There were no symptoms or symptom-complex that reliably allowed the recognition of giardiasis. Again our results were similar to previ-ously published studies. (17,18)
The pathophysiology of these symptoms in giardia infection has not been well un-derstood. The possible mechanisms include direct damage to the intestinal brush and mucosa resulting in secondary lactose intolerance, reduced intestinal absorption and deconjugation of bile salts. Recent hypothesis also suggests induction of apoptosis in intestinal epithelial cells and disruption of tight junctional zona-occludens followed by increased epithelial permeability across epithelial monolayers. (19,20, 23) Compared to other studies, diarrhoea was not so common feature in our study. as reported from in endemic areas. This difference might be caused by low initial dose of giardia cysts, in non-endemic area therefore the host is able to maintain parasite count at very low level, or it may be due to the distribution of different pathogenic strains. But this assumption is highly speculative. The association with clinical manifestation and parasite genotype is not definitive to date (18,21,22).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 31
In our study, the mean age of patients with giardiasis was slightly lower (not signifi-cantly) compared to patients with H. pylori infection and in the group without any find-ings. It is well know, that giardiasis is more common in children and adolescents (28). From this point of view, age may have some attribution in diagnostic process in uninves-tigated dyspepsia and related symptoms.
Duration of symptoms was longest in patients with giardiasis. Possible reason of de-layed diagnosis is that the G.intestinalis is generally considered to be on low degree of suspicion in non-endemic countries in comparison with the well-known H. pylori.
Importantly, we documented total remission of symptoms in 79 % examined patients with G. intestinalis infection after 14-days course treatment with metronidazole at 250mg tid. There were no statistically significant differences in symptoms distribution or metronidazole therapy effect on them in all G. intestinalis positive patients.
Another finding was that giardiasis was associated with H. pylori infection. H. pylori was found in 14 patients of the 31 patients with giardiasis. This possibly reflects the fact that both G. intestinalis and H. pylori share similar risk factors (24). There is exist-ing literature and data supporting possible synergy effect of infections, however, in our study were no significant differences between the giardia groups in symptoms presenta-tion or distribution. Some authors suggest possible synergistic participation leading to metronidasole resistance and gastrointestinal neoplasia (24,25,26,27).
Causal treatment of dyspesia led to resolution of dyspeptic symptoms; however in almost 39 % patients we did not find the cause of dyspepsia. Such patients are hypoth-esized to have functional gastrointestinal disorder. Given that functional gastrointestinal disorders are the diagnosis per exlusionem, further examinations are needed to proof the diagnosis according to ROME III criteria.
COnCLUSIOn
Chronic dyspeptic syndrome is a frequent problem of patients visiting gastroenterol-ogy outpatient unit. In our study most common cause of dyspepsia were Helicobacter pylori infection, chronic giardiasis and coeliac disease. Although H. pylori and coeliac disease are widely well known, we pointed out another possible cause of dyspepsia. Ac-cording to our data, we are suggesting that chronic Giardia intestinalis infection leads to nonspecific dyspeptic symptomatology in selected individuals that mimics functional dyspepsia and irritable bowel syndrome. We recommend test GI infection in all patients with chronic dyspeptic complaints of unknown origin,
REFEREnCES
1. Talley NY, Vakil NB, Moayyedi P. American Gastroenterological Association technical review on the evaluation of dyspepsia. Gastroenterology2005;129:1756-80.
2. McQuaid KR. Dyspepsia. In: Feldman M, Friedmann LS, Brandt LJ, editors. Sleisenger & Fordtran’s gastrointestinal and liver disease. 8th ed. Philadelphia: Saunders Elsevier; pp. 2006;121–142.
3. Rejchrt S, Koupil I, Kopacova M, Vorisek V, Seifert B, Pozler O, Zivny P, Douda T, Palicka V, Holcik J, Bures J, European society for Primary care Gastroenterology. Prevalence and sociodemografic determinants of uninvestigated dyspepsia in the Czech republic.; Eur J gastroenterol Hepatol. 2008;Sep;20(9):898-905
4. Baron JH, Sonnenberg A. Hospital admissions and primary care attendances for non ulcer dyspepsia, reflux oesophagitis and peptic ulcer in Scotland 1981-2004. Eur J Gastroenterol Hepatol 2008;20:180-6.
5. Tack J, Talley NJ, Camilleri M et al. Functional gastroduodenal disorders. Gastroenterology 2006;130:1466–1479.
6. WHO Protozoan Parasites (Cryptosporidium, Giardia, Cyclospora). Microbiological Agents in Drinking Water, 2nd edition. Addendum; 2002.
7. Hunter PR, Thompson RC. The zoonotic transmission of Giardia and Cryptosporidium.Int J Parasitol. 2005; Oct;35(11-12):1181-90.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 132
8. M. Letts, D. Davidson and F. Lalonde, Synovitis secondary to giardiasis in children, Am J Orthop 1998;27 pp. 451–454
9. Nenoff P, Domula E, Willing U, Herrmann J.Giardia lamblia-cause of urticaria and pruritus or accidental association? Hautarzt. 2006;Jun;57(6):518-20, 521-2.
10. Hanevik K, Dizdar V, Langeland N, Hausken T. Development of functional gastrointestinal disorders after Giardia lamblia infection. BMC Gastroenterol.2009; 9: 27.
11. D’Anchino M, Orlando D, De Feudis L. Giardia lamblia infections become clinically evident by eliciting symptoms of irritable bowel syndrome. J Infect 2002; 45:169-172.
12. Grazioli B, Matera G, Laratta C, Schipani G, Guarnieri G, Spiniello E, et al. Giardia lamblia infection in patients with irritable bowel syndrome and dyspepsia: a prospective study. World J Gastro-enterol 2006; 12:1941-1944.
13. Moayyedi P, Soo S, Deeks J, Delaney B, Harris A, Innes M, Oakes R, Wilson S, Roalfe A, Bennett C, Forman D. Eradication of Helicobacter pylori for non-ulcer dyspepsia. Cochrane Database Syst Rev. 2006 Apr 19;(2):CD002096.
14. Garcia LS, Shimizu RY. Evaluation of nine immunoassay kits (enzyme immunoassay and direct fluorescence) for detection of Giardia lamblia and Cryptosporidium parvum in human fecal specimens. J Clin Microbiol 1997; 35:1526-1529
15. Diagnostic yield of duodenal aspirate for G. lamblia and comparison to duodenal mucosal biopsies.Gupta SK, Croffie JM, Pfefferkorn MD, Fitzgerald JF. Dig Dis Sci. 2003 Mar;48(3):605-7.
16. McHenry R, Bartlett MS, Lehman GA, O’Connor KW: The yield of routine duodenal aspiration for Giardia lamblia during esophagogastroduodenoscopy. Gastrointest Endosc 1987; 6:425–426.
17. Yakoob J, Jafri W, Abid S, Jafri N, Hamid S, Shah HA, Rizvi L, Islam M, Shaikh H. Giardiasis in patients with dyspeptic symptoms. World J Gastroenterol. 2005;Nov 14;11(42):6667-70
18. Read CM, Walters J, Robertson ID, Thompson RCA Correlation between genotype of Giardia duodenalis and diarrhoea. Int J Parasitol 2002; 32:229–231
19. Chin AC, Teoh DA, Scott KG, et al. Strain-dependent induction of enterocyte apoptosis by Giardia lamblia disrupts epithelial barrier function in a caspase-3-dependent manner. Infect Immun 2002; 70:3673-3680
20. Scott KG, Meddings JB, Kirk DR, et al. Intestinal infection with Giardia spp. reduces epithelial barrier function in a myosin light chain kinase-dependent fashion. Gastroenterology 2002; 123:1179-1190
21. Homan WL, Mank TG. Human giardiasis. genotype linked differences in clinical symptomatology. Int J Parasitol 2001; 31:822-826
22. Sahagun J, Clavel A, Goni P, Seral C, Llorente MT, Castillo FJ, Capilla S, Arias A, Gomez-Lus R. Correlation between the presence of symptoms and the Giardia duodenalis genotype. Eur J Clin Microbiol Infect Dis 2008; 27(1):81-83
23. Das S, Schteingart CD, Hofmann AF, Reiner DS, Aley SB, Gillin FD. Giardia lamblia: evidence for carrier-mediated uptake and release of conjugated bile acids..Exp Parasitol. 1997; Oct;87(2):133-41.
24. Moreira ED Jr, Nassri VB, Santos RS, Matos JF, de Carvalho WA, Silvani CS, Santana CS. Association of Helicobacter pylori infection and giardiasis: results from a study of surrogate markers for fecal exposure among children. World J Gastroenterol 2005; 11: 2759-2763
25. Abou Holw SA, Anwar MM, Heshmat MG, Enany AY, Rashad MM. Effect of concommitant Helicobacter pylori infection in patients with Giardia lamblia in Egypt. J Egypt Soc Parasitol. 2009; Aug;39(2):439-46.
26. Land KM, Johnson PJ. Molecular basis of metronidazole resistance in pathogenic bacteria and protozoa. Drug Resist Update 1999; 2: 289-294
27. Patterson MM, Schrenzel MD, Feng Y, Fox JG. Gastritis and intestinal metaplasia in Syrian hamsters infected with Helicobacter aurati and two other microaerobes. Vet Pathol 2000; 37: 589-596
28. Farthing MJ. Giardiasis. Gastroenterol Clin North Am 1996; 25: 493–515
Received: December,1,2010Accepted: January,6,2011

33
POInt PREVALEnCE SURVEY OF nOSOCOMIAL InFECtIOnS In UnIVERSItY HOSPItAL In MARtIn
Zabkova E., Murajda L., Hudeckova H.
Department of Public Health, Jessenius Faculty of Medicine, Comenius University, Slovak Republic
AbstractNosocomial infections (NI) are a serious problem not only in Slovakia but in all countries. The European Commission decided on their standardized surveillance in the whole European Union. According methodology elaborated by experts from the European Centre for Disease Control and Prevention (ECDC) in Stockholm we performed a point prevalence survey in the University Hospital Martin (UHM). In this article we present the results which show that the prevalence of NI in UHM (5.5 %) is comparable with the average in other European hospitals. In comparison with occurrence of NI (0.64 %) reported through the Epidemiological Information System of the Slovak Republic, our results are 8.5-times higher. The highest point prevalence of NI was found at the Clinic of Hematology and Transfusiology – 7 patients (out of 15 hospitalized) which is 46.7 %. The most common type of NI was sepsis (25.9 %) and urological infection (22.2 %). Based on the results obtained we recommend to continue in international projects of NI surveillance, so that it would be possible to acquire more accurate data on NI prevalence in UHM and do the benchmarking among hospitals in countries of the European Union.
Key words: nosocomial infection, prevalence, University Hospital Martin
IntRODUCtIOn
A nosocomial infection (NI) is defined in Slovak legislation as an infection of internal or external origin, which occurred in direct relation with hospital stay or healthcare performance in a healthcare facility or social care facility (1).
Centers for Disease Control and Prevention (CDC) in USA defines nosocomial infec-tions as infections which occurred in a healthcare facility, were not present at admission and the patient was not in incubation period of the relevant infection at admission. If incubation period is unknown, an infection is considered nosocomial when occurred later than 48-72 hours after admission to hospital. Infection present at admission can be considered as nosocomial only if it is epidemiologically related to a precedent hospi-talization. All other infections are considered as community acquired. The CDC has also specific diagnostic criteria for the infection types. Using these criteria and same meth-ods of surveillance enables mutual comparability of the acquired data (2).
The NI occurrence is watched in Slovakia through an obligatory reporting. Regulation of the Ministry of Health of Slovak Republic No. 553/2007 on requirements for health-care facilities about health protection, sets for providers of healthcare and for healthcare workers a duty to avoid NI and to register NI in patient records and in a diary of NI, to perform an analysis of NI occurrence and of the reasons of their occurrence and to apply measures to decrease the occurrence, stop spread of NI and prevent them.
The chief doctor of a ward has to inform the Regional Public Health Authority in 48 hours by a written form. If there is an outbreak or clinically serious NI, death or suspi-cion of death for NI, reporting is performed immediately – personally, by telephone, fax or email. NI outbreak is an incidence of at least three cases of the same NI, which are in epidemiological relationship (3).
A d d r e s s f o r c o r r e s p o n d e n c e :Eva Zabková, Department of Public Health JFM CUSklabinská Str. N. 26, 036 01 Martin, Slovak Republic, e-mail: [email protected].
ACTA MEDICA MAR T IN IAN A 2011 11/1 DOI : 10 .2478/v10201-011-0005-9

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 134
Analysis of occurrence of NI is annually published in the Annual report on activities of public health authorities in the Slovak Republic, published by the Public Health Au-thority of the Slovak Republic. Through the Regional Public Health Authority in Banská Bystrica the information on NI has been published since 2006 on web pages of the Epi-demiological Information System (EPIS), too.
MEtHODS
We used a point prevalence survey to estimate prevalence of nosocomial infections in University Hospital Martin.
The survey was realized from June 22nd till July 8th, 2010. Performing of the study was approved by the Ethical Committee of the Regional Public Health Authority in Mar-tin.
Collection of data at each ward had to be finished during the same day it started. The maximum lenght of survey for the whole hospital was set to three weeks. For privacy protection, every patient in the survey was given a code and his/her data were registered in database only under this code.
We used the definitions of different types of NI from the Codebook by ECDC (4).There were two criteria for the study group. First, regarding the wards – only the acute
care wards were included and the long-term care wards were excluded. The second was about patients – all patients admitted to the ward before 8.00 am and not discharged from the ward at the time of the survey were included.
Our team consisted from researchers from the Department of Public Health of the Jess-enius Faculty of Medicine, Comenius University, Regional Public Health Authority in Martin and the University Hospital Martin. These visited in three weeks according a set schedule all acute care wards of the hospital and in collaboration with appointed doctors at the wards they assessed data from patient records and registered active nosocomial infections according the definitions used in the survey. We processed and analyzed the results in Microsoft Excel.
RESULtS
There were 495 patients included in the survey, 268 men (54.1 %) and 227 women (45.9 %), with average age 51.5 years (min. 0, max. 89 years).Out of all patients included in the survey, there were 5.5 % patients found with an active NI. The average age of pa-tients with NI was 50 years (min.0, max.85 years). We found NI in 44.4 % of women (12 NI) and in 55.6 % of men (15 NI).
18.6%
22.2%
25.9%
11.1%
22.2%
P N
UTI
B S I
E E NT
OTH
Fig. 1. Prevalence of nosocomial infections at University Hospital Martin Legends for Fig.1 and Fig.5:PN – Pneumonia; UTI – Urinary tract infection; BSI – Bloodstream infection; EENT – Eye, Ear, Nose or Mouth infection; OTH – other; (according CDC definitions).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 35
The NI prevalence according age groups is on Figure 2.
0
1
2
3
4
5
6
7
0-4 5-9 10-14 15-19 20-24 25-34 35-44 45-54 55-64 65-74 75-84 85-
a g e g roups
HI (
abs.
)
Fig. 2. Prevalence of nosocomial infections according age groups
We present character distribution of NI found at the clinics visited on the following picture.
14,81%
25,93%
11,11% 11,11%
11,11%
11,11%
14,81%P E D
O R T HO
I.INT
II. INT
NE O N
HAE M
O T H
Fig. 3. Proportion of nosocomial infections at clinics of University Hospital Martin
Legends for Fig. 3, Fig. 4 and Fig. 5: PED – Paediatrics; ORTHO – Orthopaedics and Traumatology; I. INT – General Medicine; II. INT – Gastroenterology; NEON – Neonatol-ogy; HAEM – Haematology; NEUROL – Neurology; I.SUR - General Surgery; II.SUR – Transplant and Vascular Surgery; OTH – Other.
On Figure 4 there is prevalence of NI at the clinics of UHM. At nine clinics the preva-lence of NI was from 2.8 % to 46.7 %. At other clinics there was not found any NI during the survey.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 136
46,7
10,31068
2,85,98,1
11,8
05
101520253035404550
P ED
OR THO
NE UR OL
I. SUR
II. S UR
I.INT
II. IN
T
NE ON
HAE M
HI%
Fig. 4. Prevalence of nosocomial infections at clinics of University Hospital Martin.
On Figure 5 we present character of found NI according clinics of the hospital.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PE D
OTR HOI.IN
TII.I
NT
NEON
HAE MI. S
UR
II. S UR
NEUR O L
P N
UTI
B S I
E E NT
OTH
Fig. 5. Character of nosocomial infections at clinics of University Hospital Martin.
DISCUSSIOn
The European Union put an effort on harmonisation of policies of surveillance of com-municable diseases including nosocomial infections. In this context, the EU-funded HELICS project in 1993-2004 undertook a systematic overview of the national surveil-lance policies and organisation to identify similarities and discrepancies and to plan further progress to be made. Totally, around 2000 European hospitals participate in a surveillance network. The participation is voluntary and the estimated coverage is quite high: around 30 % (5).
Based on the IPSE project (Improving Patient Safety in Europe) in hospitals in the European Union a need was defined for a surveillance of nosocomial infections on Eu-ropean level to estimate and watch the burden of nosocomial infections.
Because a general continuous incidence surveillance is very expensive, the prevalence hospital surveys are considered efficient.

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 1 37
In 2009 the experts from European Centre for Disease Control and Prevention (ECDC) and experts from member states of the European Union elaborated a protocol of the European point prevalence survey (6).
Prevalence here means the number of all cases – new and also old but still present in popu-lation. Because this number is counted for a specific date, it is a point prevalence study (7).
Currently, the average NI incidence among hospitalized patients in hospitals in devel-oped countries is about 6-8 %. In less developed countries it is even more than 25 %. Infections, deaths and economic costs related to acquiring NI have been growing mainly in past thirty years. Although estimations of proportion of preventable NI differ, there is a general consent that it could be more than 20 % in developed countries and even more than 40 % from all NI in less developed countries (8).
The biggest proportion of NI was the sepsis (25.9 %). In men it was 33.0 % from all found NI, in women 16.0 %. Then there were urological infections, which occurred in 22.2 %. In men in 20.0 % and in women 25.0 % of all NI. Other infections were found in 22.2 % of all NI. To this group we put the infections of gastrointestinal system, central nervous system, surgical site infections (SSI) and bone and joint infections.
It results from the data from EPIS that in 2009 the most common reported NI were the SSI (22.96 %) and urological infections (20.41 %).
We found most of the NI in the age group of 65-84 years, 12 cases (22.2 %). High number of NI occurred also in children under one year of age – 4 cases (14.8 %). In both these groups there was the highest number of hospitalized patients, too. We think that one of the most important causes underlying the high prevalence in these is the weak immune system.
The highest proportion of NI found at the University Hospital Martin (UHM) was from the Clinic of Hematology and Transfusiology (25.9 %). There occurred all types of seri-ous NI. This was probably due to characteristic weak immune system of the patients hospitalized at the clinic and to an aggressive chemotherapy.
At the Clinic of Children and Adolescents there were 14.8 % of all NI in the hospi-tal and equally 11.1 % at the Clinic of Orthopedics and Traumatology, Clinic of Inter-nal Medicine I, Clinic of Internal Medicine-Gastroenterology and Clinic of Neonatology. Some clinics with lower NI prevalence (Clinic of Neurology, Clinic of Surgery, Clinic of Transplant and Vascular Surgery) represent 14.8 % from total number of found NI. There were no found NI at other clinics. When looking at data from EPIS, the highest number of NI in 2009 was reported from the Clinic of Surgery (25.51 %).
The highest point prevalence - the proportion of NI from the total number of hospital-ized patients at a clinic – was at the Clinic of Hematology and Transfusiology: 7 patients (46.7 %). In 2009 there was no NI reported to EPIS from this clinic. We assume that it was due to insufficient reporting. Similarly, in the Annual report on activities of public health authorities in the Slovak Republic in 2009 we may read that the low number of reported NI from all healthcare facilities in Slovakia is probably due to insufficient reporting, too.
At the Clinic of Children and Adolescents we found 4 cases of NI (11.8 %), at Clinic of Neonatology we found 3 NI cases (10.3 %) and at Clinic of Internal Medicine-Gastroen-terology 3 NI cases (10.0 %). We found less than 10 % of NI cases among the patients at the Clinic of Orthopedics and Traumatology, Clinic of Neurology, Clinic of Surgery, Clinic of Transplant and Vascular Surgery and Clinic of Internal Medicine I.
Summarizing, the prevalence of NI found in patients at the University Hospital Martin was higher (5.5 %) in comparison with the reported occurrence in the Epidemiological information system where NI represent 0.64 % (9). We are convinced that this is due to insufficient reporting of NI. There could be more reasons for that. Our main assumption is that there is a belief that a higher number of reported NI could lead to a negative as-sessment of quality of healthcare of the hospital.
However, our results are in accord with data on reported NI in developed countries. Mar-cel et al. (10) state that the prevalence of NI in European hospitals is about 6-12 % (10).

A C T A M E D I C A M A R T I N I A N A 2 0 1 1 1 1 / 138
We suggest that the reporting of NI would be improved at the University Hospital Martin and that there would continue the participation in international projects of sur-veillance of NI and the infection control, so that it would enable benchmarking and consecutive improvement.
REFEREnCES
1. Act of the Parliament of the Slovak Republic No. 355/2007 on protection, promotion and development of public health. Code of laws, 2007 (154): 2402-75.
2. Centers for Disease Control and Prevention: Definitions of Nosocomial Infections. [online ] [cit. 2009-03-10] Available on Internet: http://www.health2k.state.nv.us/sentinel/Forms/ UpdatedForms105/CDC_Defs_Nosocomial.pdf
3. Regulation of Ministry of Health of the Slovak Republic No. 553/2007 on requirements for health protection in healthcare facilities.
4. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals, Pilot Protocol 3.3 - Codebook, ECDC, June 2010.
5. IPSE, Improving Patient Safety in Europe, IPSE Annual Report 2005. Available on Internet: http://helics.univ-lyon1.fr/deliverables/IPSE_Annual_Report_2005_25oct06.pdf
6. Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals, Pilot Protocol (final), Version 3.3, ECDC, June 2010.
7. Bakoss, P. et al.: Epidemiológia. Bratislava, Univerzita Komenského, 2005. 488 p.8. Stefkovicova, M.: Prevencia nozokomiálnych nákaz je ako beh na dlhé trate. In: Nozokomiálne nákazy,
2003 (2): 1-2.9. Annual Report on Activities of Regional Public Health Authorities in the Slovak Republic in 2009.
Bratislava, Public Health Authority of the Slovak Republic, 2009. 776 p. Available on Internet: http://www.slovanet.sk/uvzsr/docs/vs/vyrocna_sprava_SR_09.pdf
10. Marcel, J.P. et al.: Healthcare-associated infections: think globally, act locally. Clin Microbiol Infect. October 2008;14(10):895-907.
Received: November,30,2010Accepted: February,14,2011



JESSENII FACULTAS MEDICA MARTINENSISUniversitatis Comenianae
ACTAMEDICA
MARTINIANAJournal for Biomedical Sciences,
Clinical Medicine and Nursing
IS S N 1 3 3 5 - 8 4 2 1
201010/3