acute myeloid leukemia marcelo c. pasquini, md, ms associate professor of medicine adult bmt program...
TRANSCRIPT
Acute Myeloid LeukemiaMarcelo C. Pasquini, MD, MS
Associate Professor of MedicineAdult BMT ProgramHeme-Malignancies
Division of Hematology/Oncology
Acute Myeloid Leukemia Outline
• Bone marrow as a blood forming organ• Biology of Acute Myeloid Leukemia• Treatment• Bone marrow Transplant
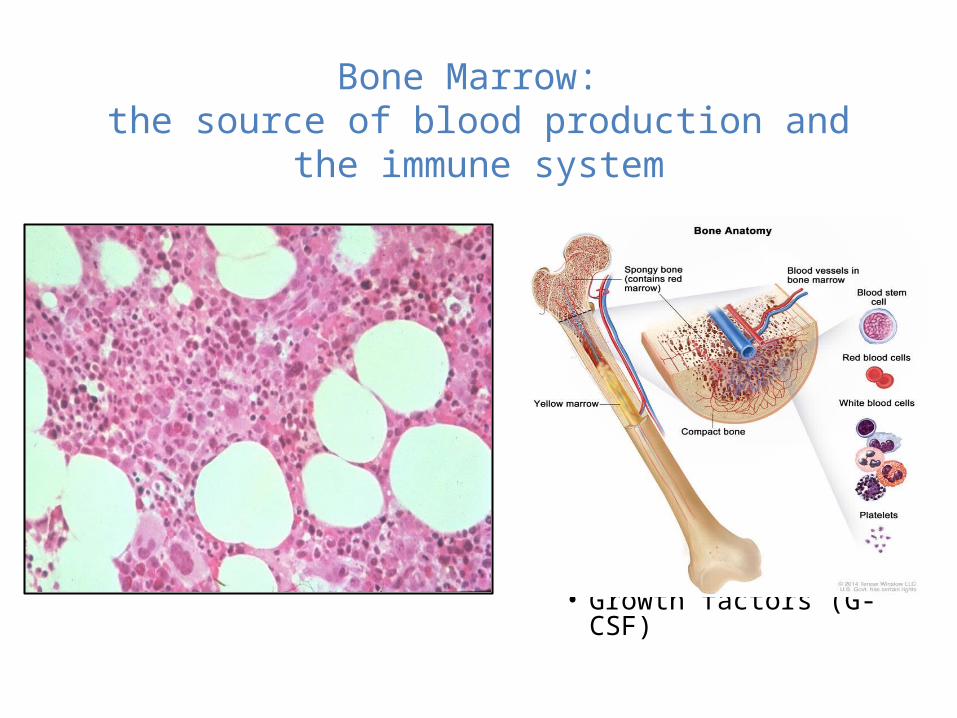
Bone Marrow: the source of blood production and the immune
system• All blood cells arise from
hematopoietic stem cells–Self renewing–Pluripotent
• Blood production is highly regulated–Messages from the body (e.g.
erythropoietin from kidney)–Microenvironments produce
specific cells• Cytokines (SCF, IL3)• Growth factors (G-CSF)
Normal bone marrow
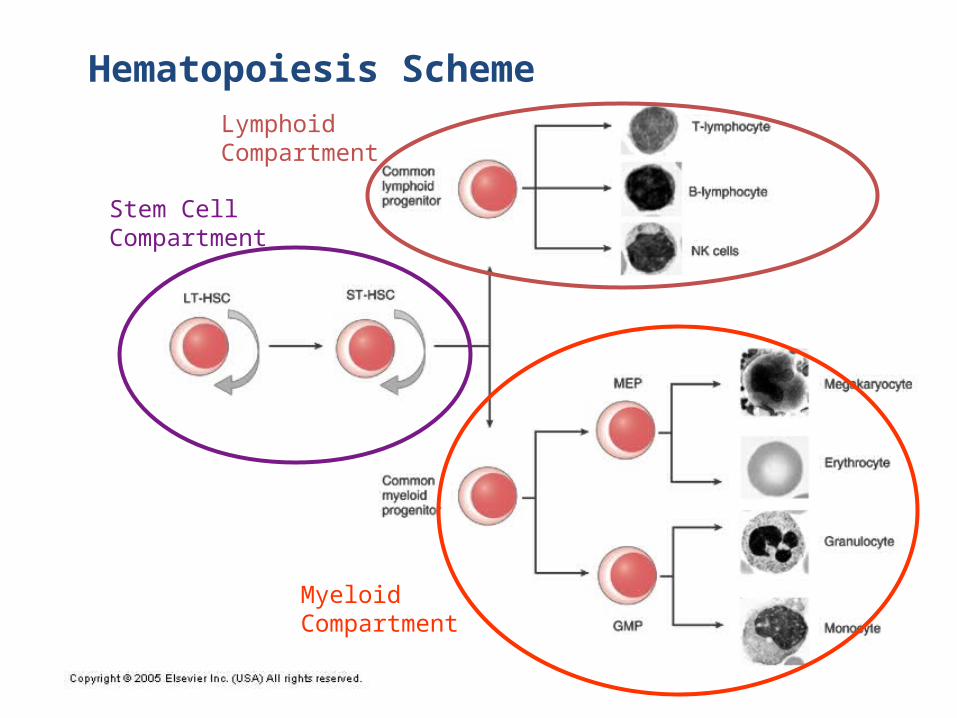
Hematopoiesis Scheme
Stem CellCompartment
LymphoidCompartment
MyeloidCompartment
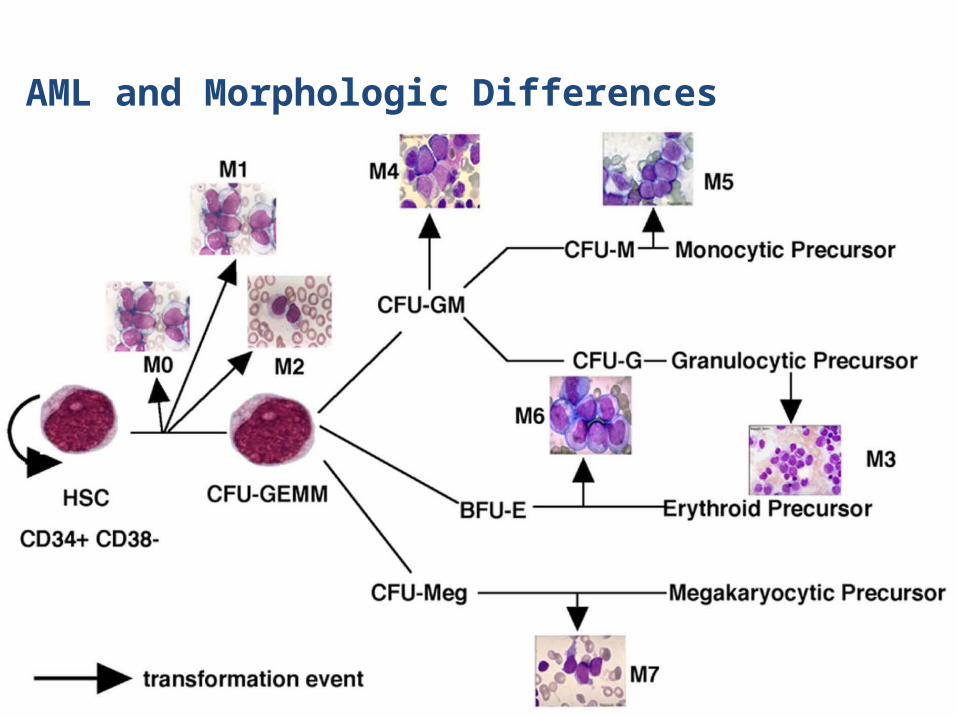
AML and Morphologic Differences
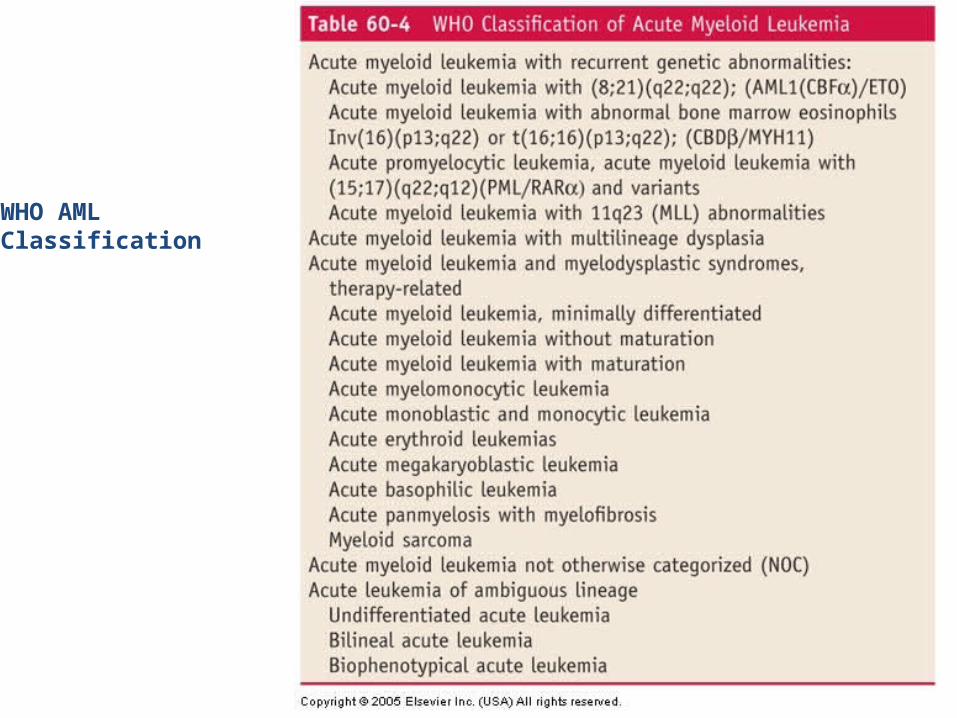
WHO AMLClassification
Prognostic factors in AML
• Disease markers
– Chromosomes– Genetic markers
• Performance status• Age
Juliusson G et al. Blood 2012;119:3890-3899
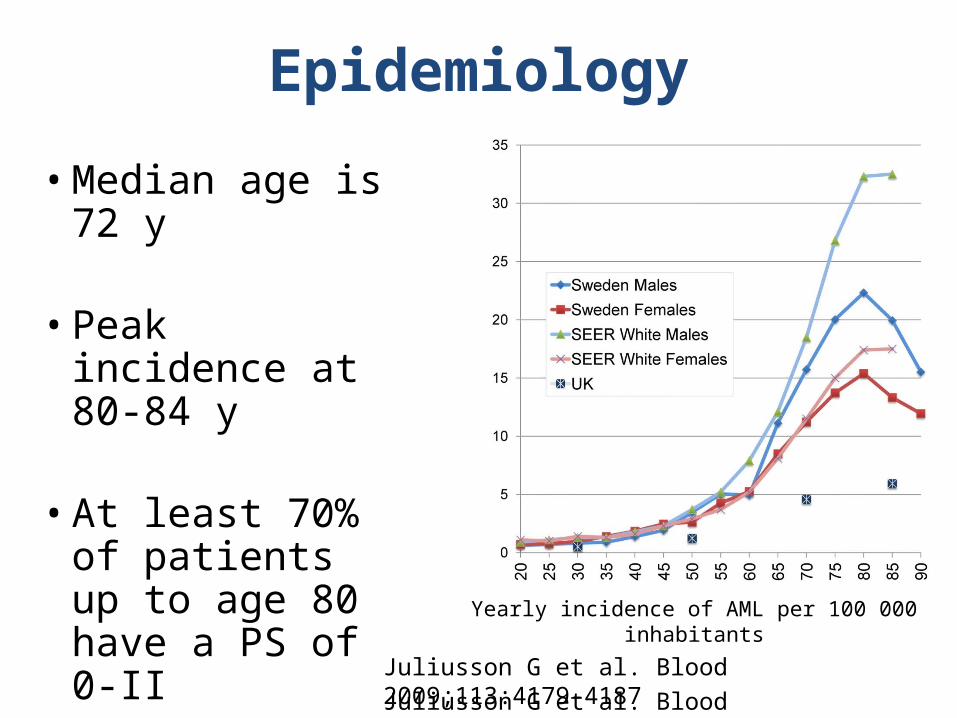
• Median age is 72 y
• Peak incidence at 80-84 y
• At least 70% of
patients up to age 80 have a PS of 0-II
Yearly incidence of AML per 100 000 inhabitants
Epidemiology
Juliusson G et al. Blood 2009;113:4179-4187
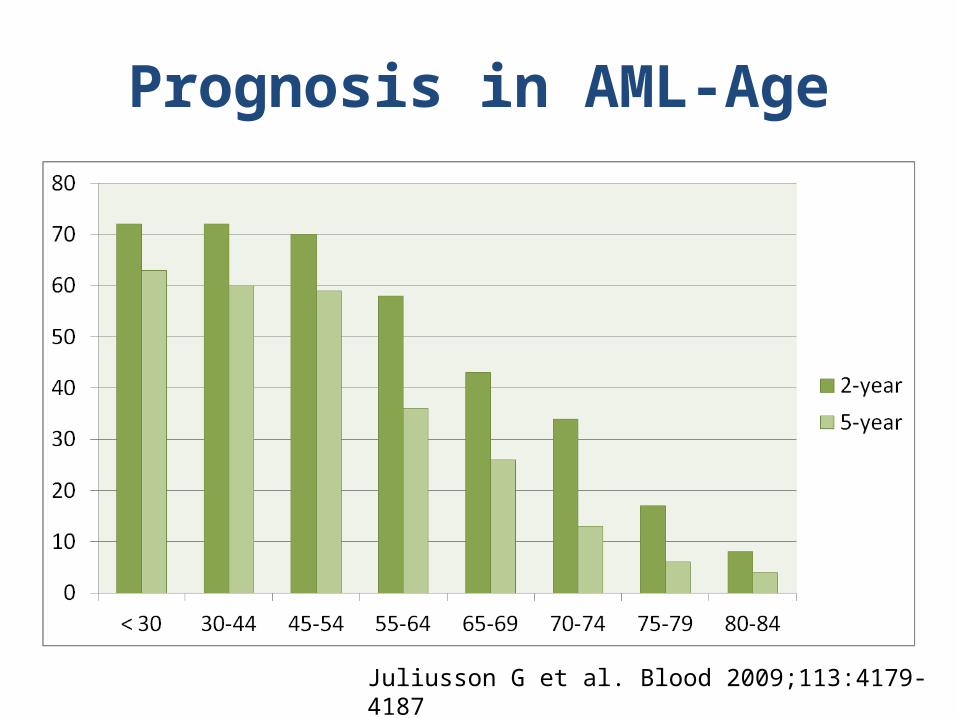
Prognosis in AML-Age
Juliusson G et al. Blood 2009;113:4179-4187
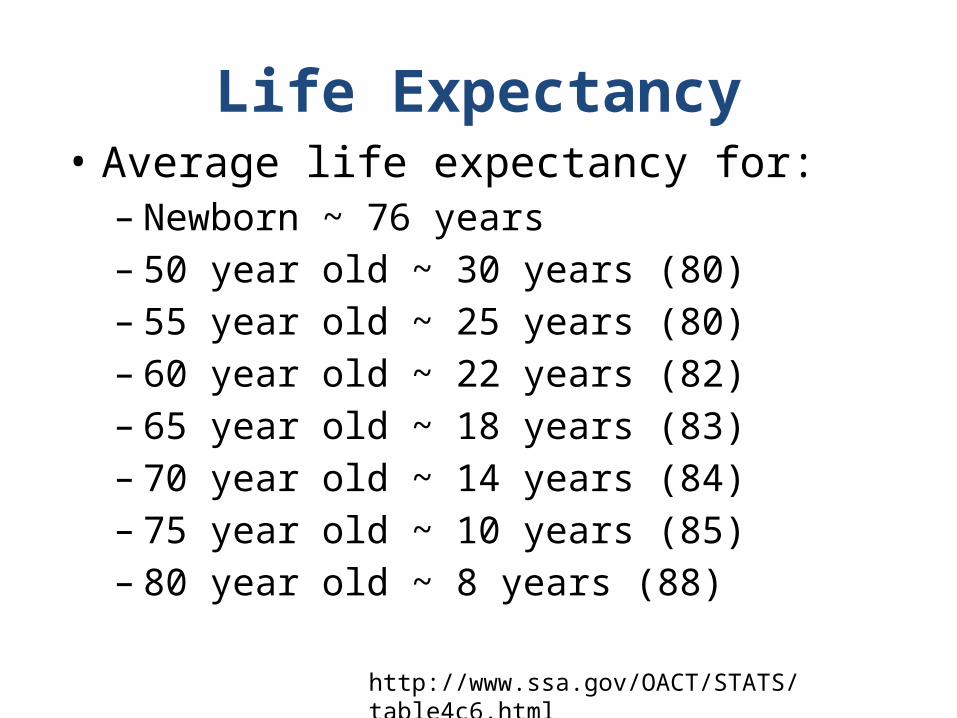
Life Expectancy• Average life expectancy for:
– Newborn ~ 76 years– 50 year old ~ 30 years (80)– 55 year old ~ 25 years (80)– 60 year old ~ 22 years (82)– 65 year old ~ 18 years (83)– 70 year old ~ 14 years (84)– 75 year old ~ 10 years (85)– 80 year old ~ 8 years (88)
http://www.ssa.gov/OACT/STATS/table4c6.html
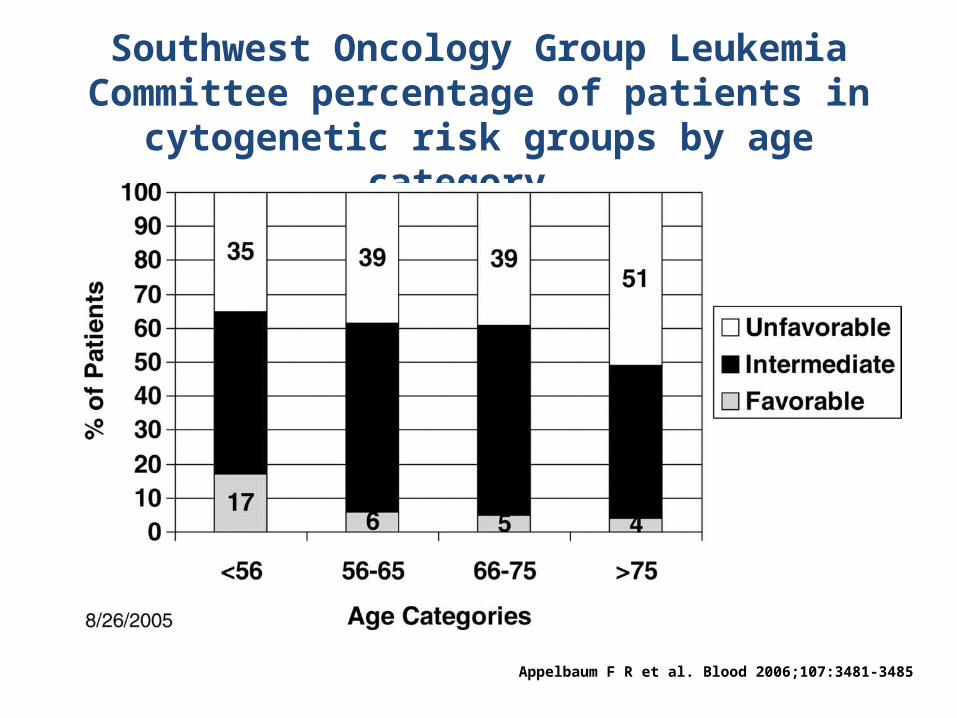
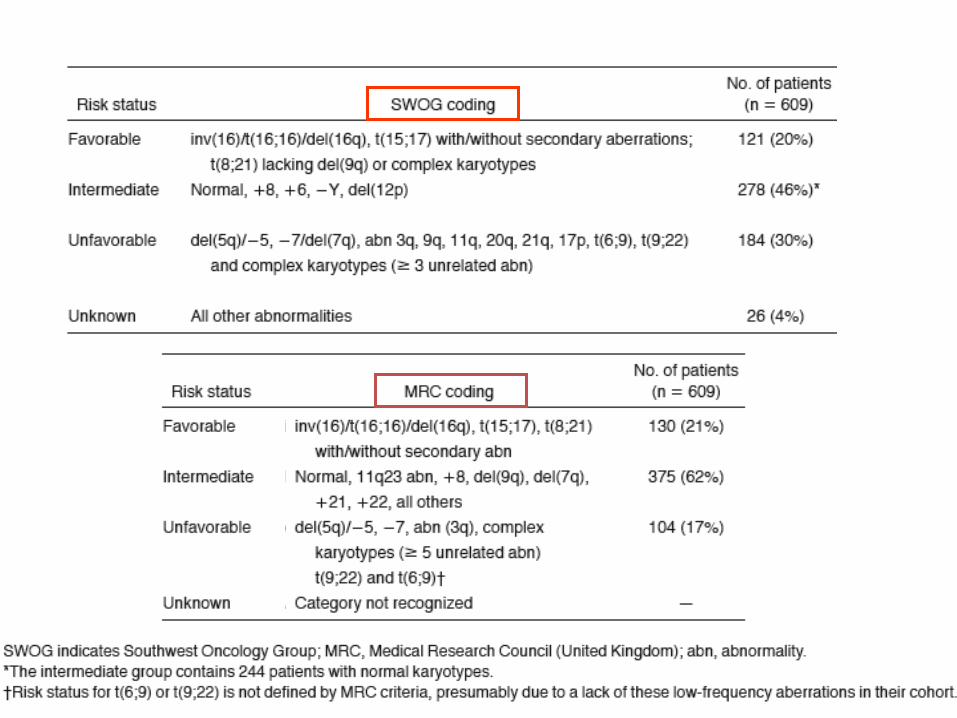
Southwest Oncology Group Leukemia Committee percentage of patients in cytogenetic risk groups by age
category.
Appelbaum F R et al. Blood 2006;107:3481-3485
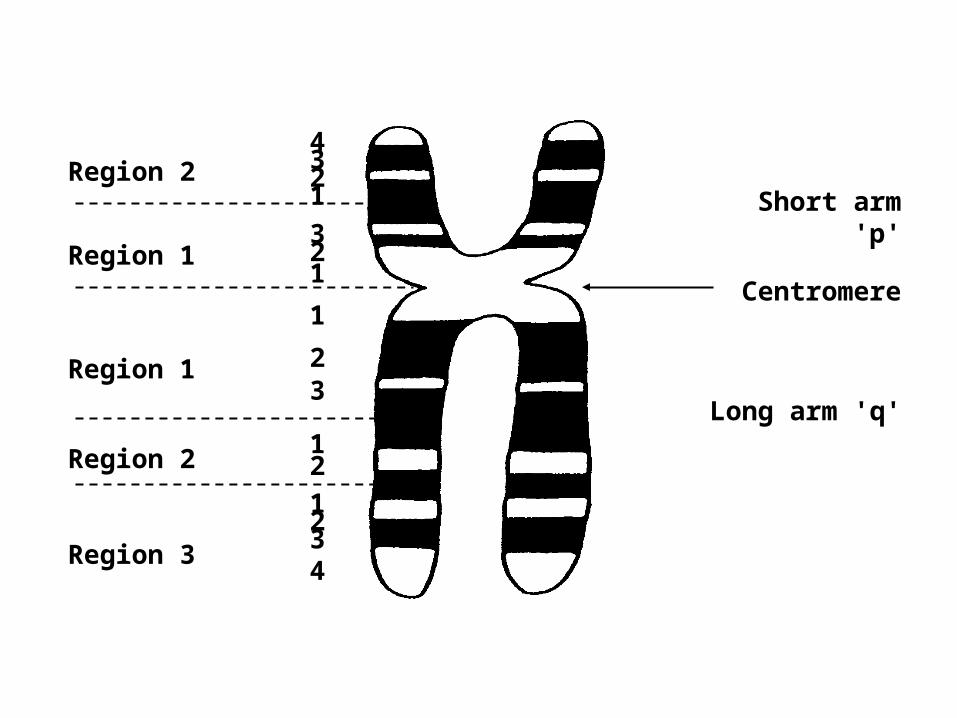
Region 2
Region 1
Region 1
Region 2
Region 3
4321
321
1
23
21
1234
Short arm 'p'
Centromere
Long arm 'q'
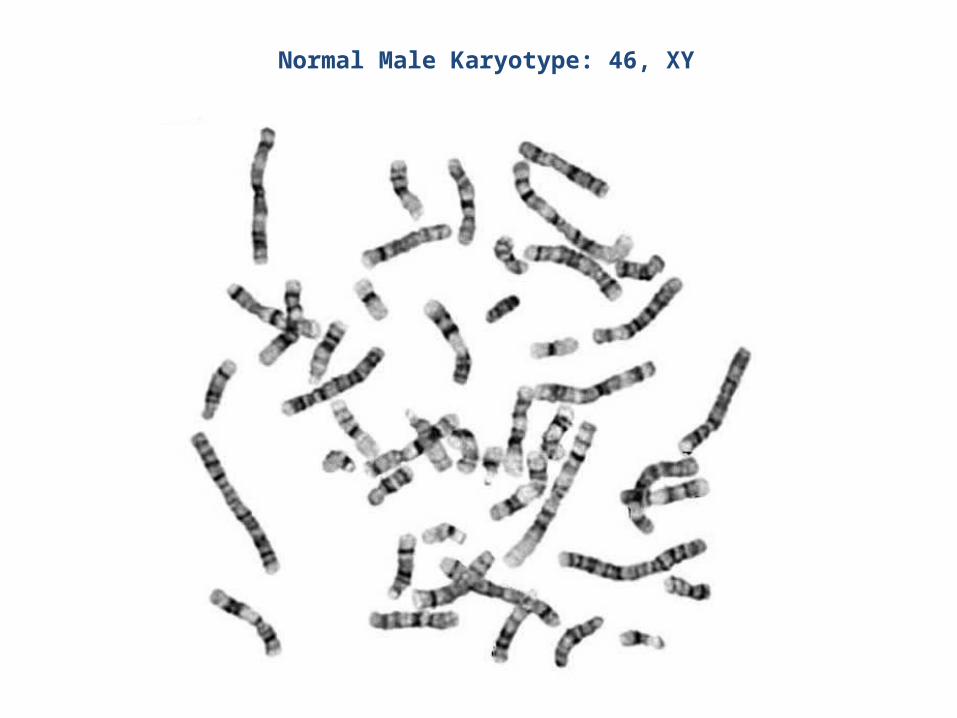
Normal Male Karyotype: 46, XY

47, XY, +8
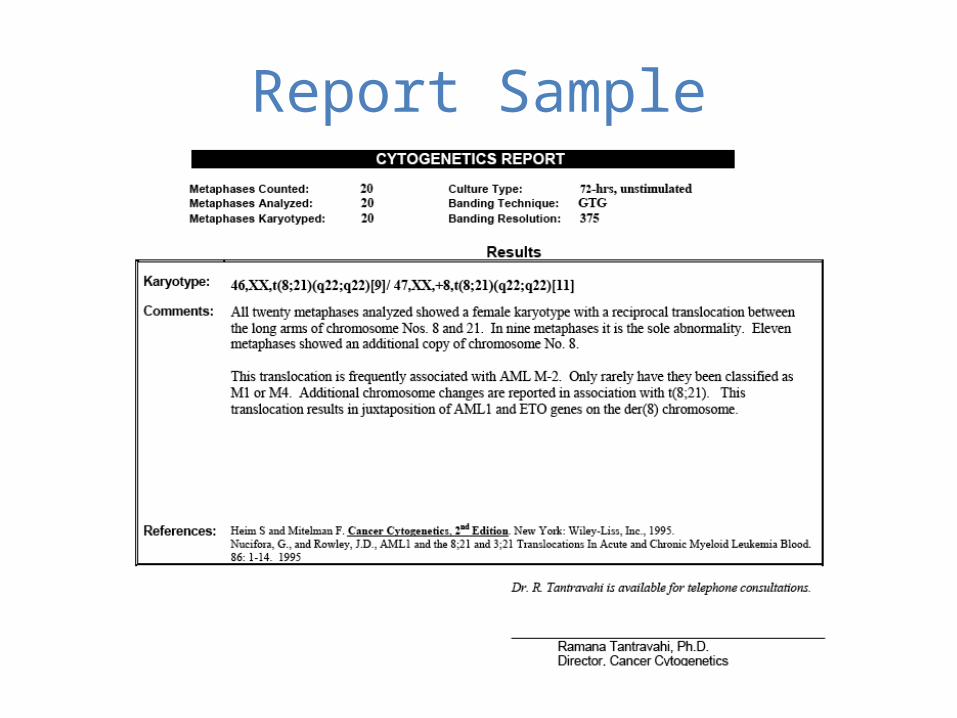
Report Sample
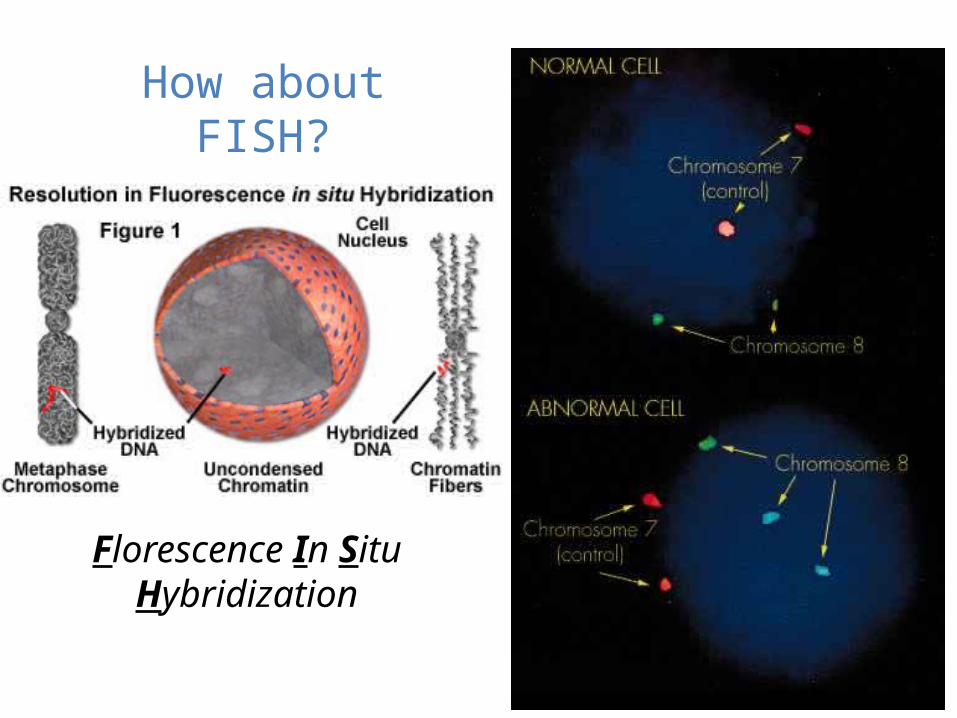
How about FISH?
Florescence In Situ Hybridization
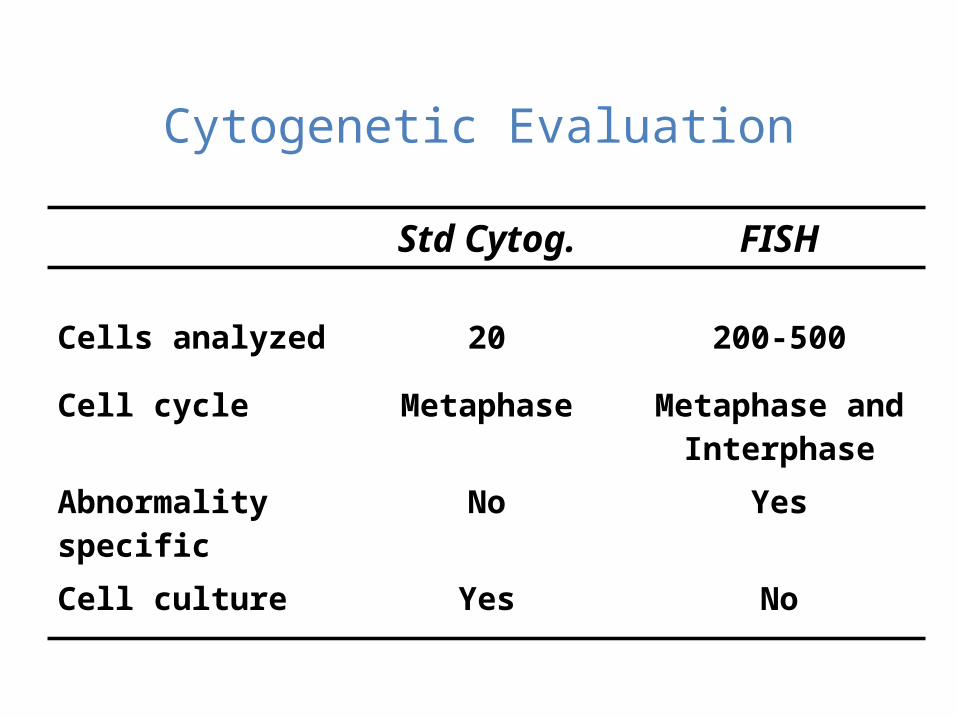
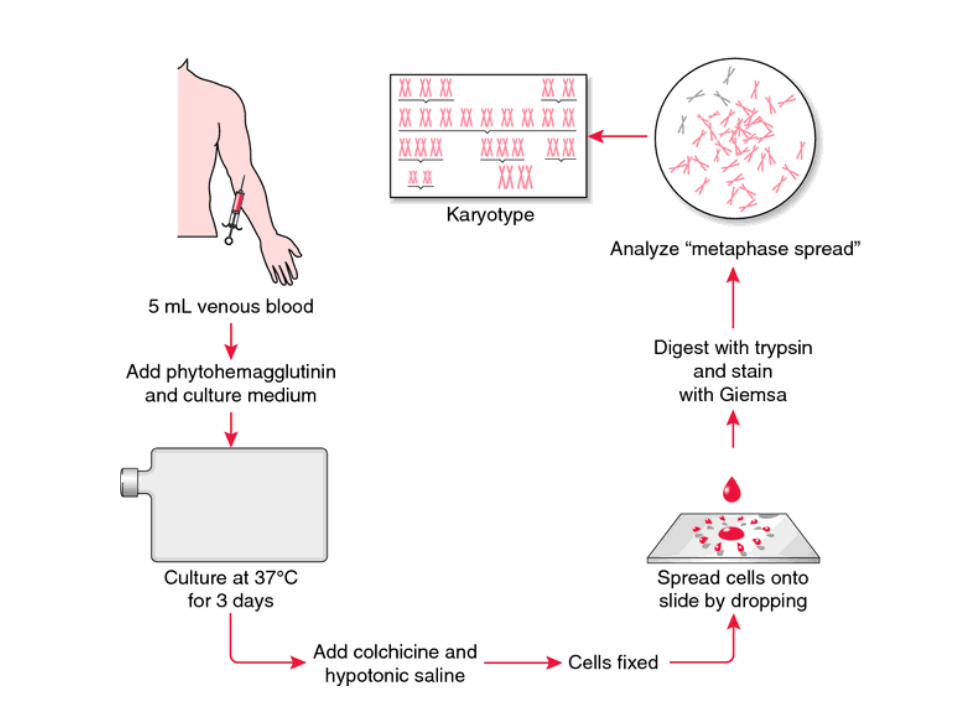
Cytogenetic Evaluation
Std Cytog. FISH
Cells analyzed 20 200-500
Cell cycle Metaphase Metaphase and Interphase
Abnormality specific
No Yes
Cell culture Yes No
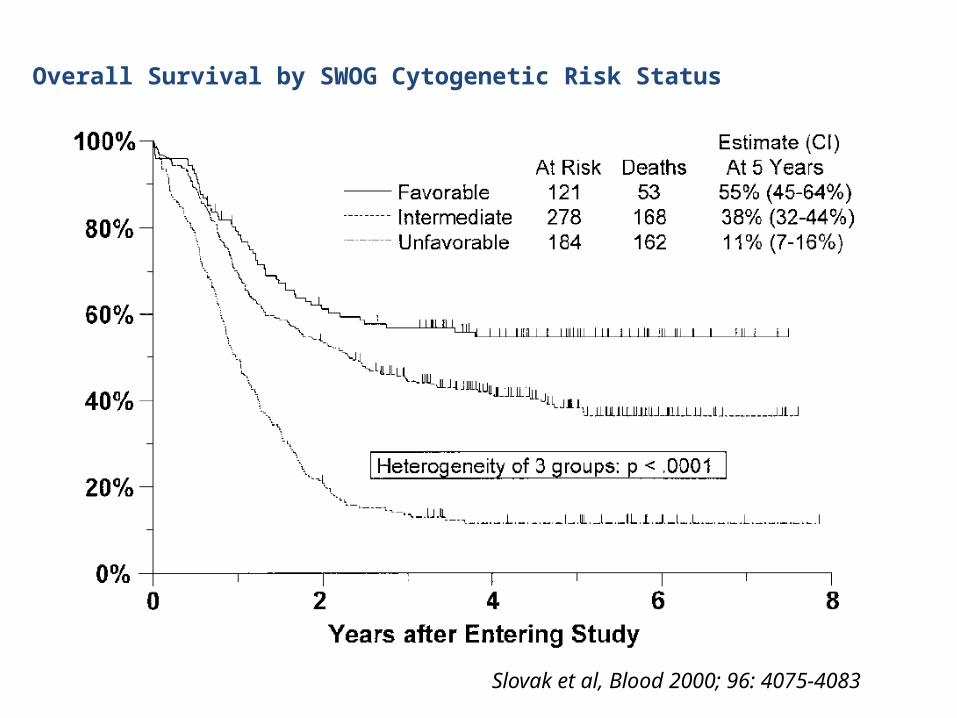
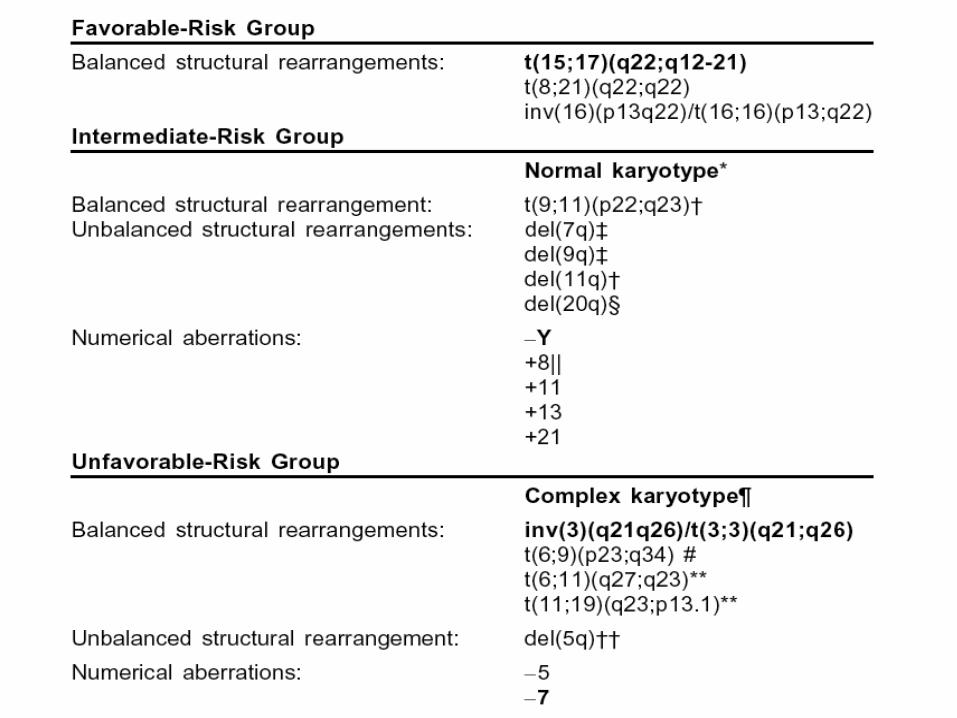
Overall Survival by SWOG Cytogenetic Risk Status
Slovak et al, Blood 2000; 96: 4075-4083
Genetic markers in AML
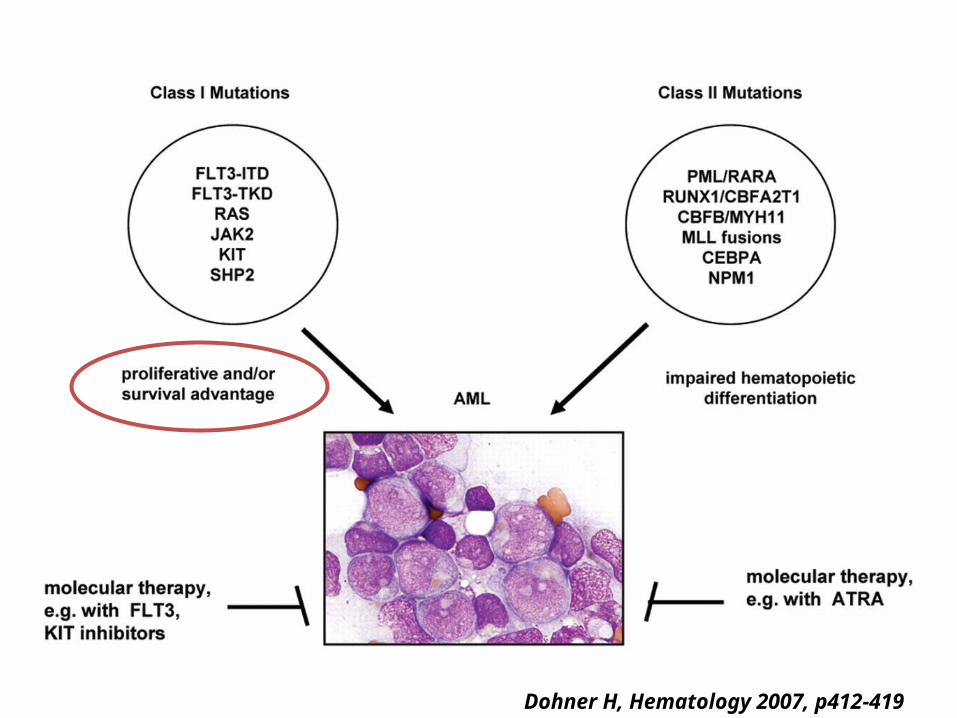
Dohner H, Hematology 2007, p412-419
Molecular Markers and Prognosis
• New Good Guys– NPM1 mutation without FLT3 ITD– CEBPA mutation
• New Bad Guys– FLT3 ITD– MLL PTD– KIT mutation (Associated with t(8;21) or inv(16))– Overexpression of BAALC– WT1 mutations– IDH1/2
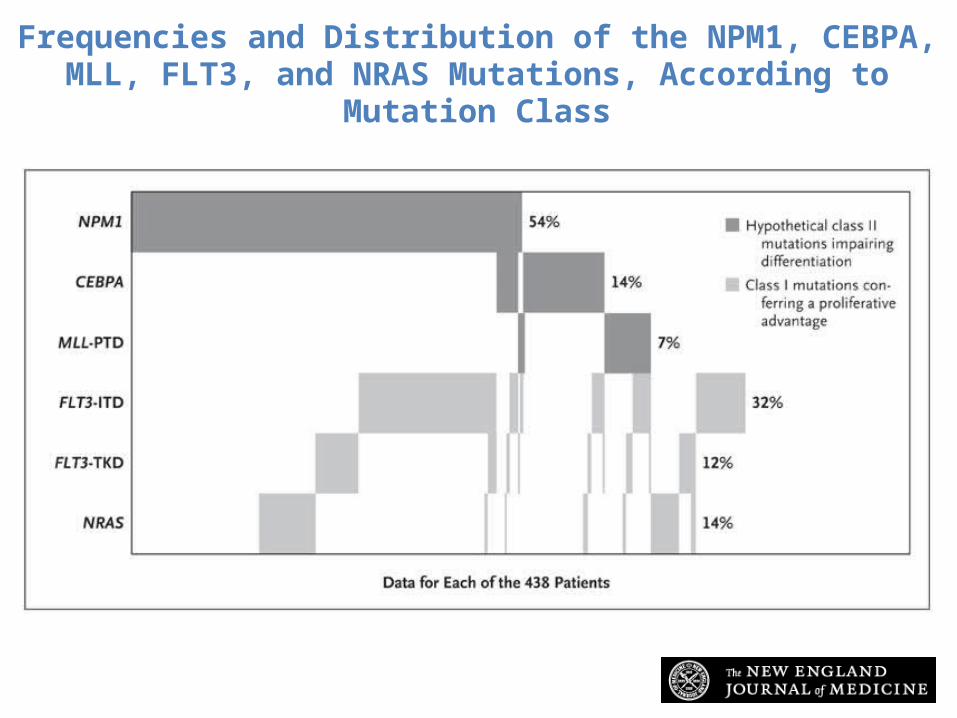
Schlenk R et al. N Engl J Med 2008;358:1909-1918
Frequencies and Distribution of the NPM1, CEBPA, MLL, FLT3, and NRAS Mutations, According to
Mutation Class
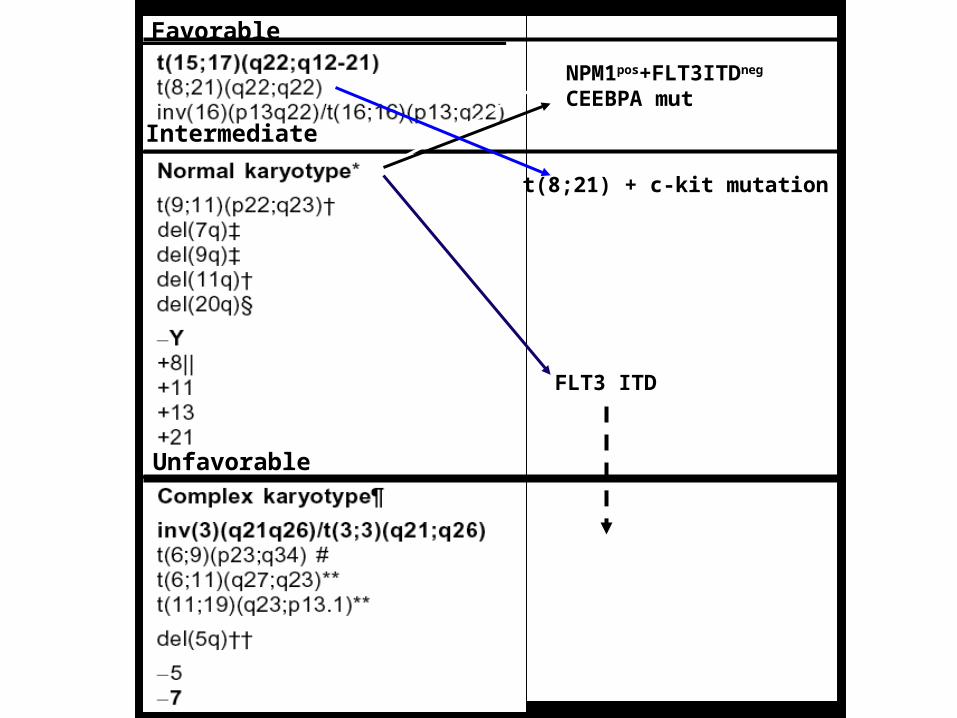
Favorable
Intermediate
Unfavorable
NPM1pos+FLT3ITDneg
CEEBPA mut
t(8;21) + c-kit mutation
FLT3 ITD
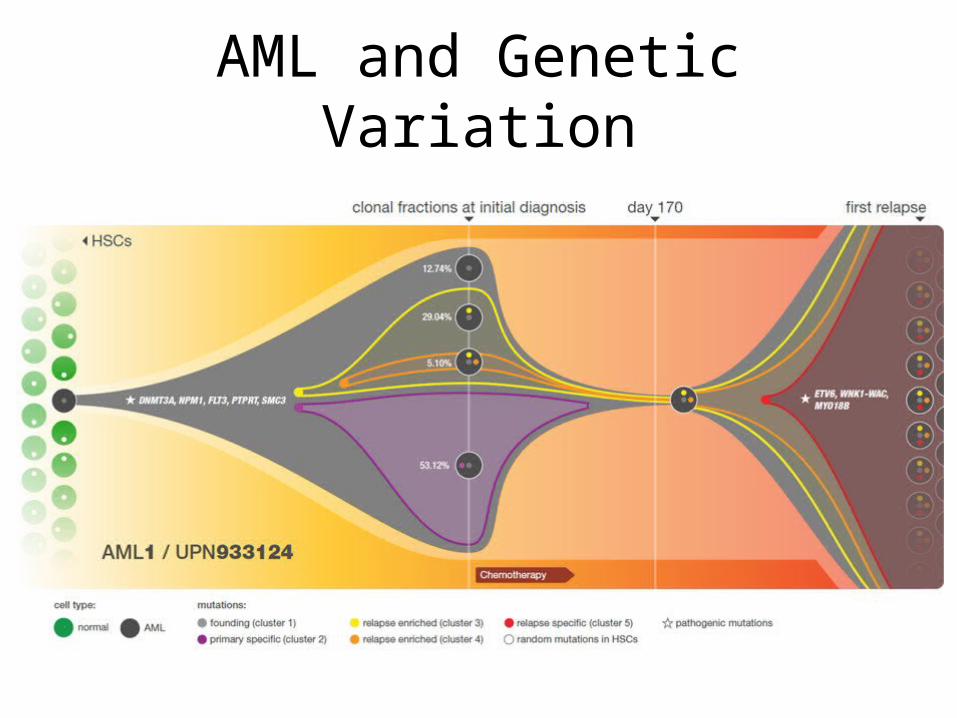
AML and Genetic Variation
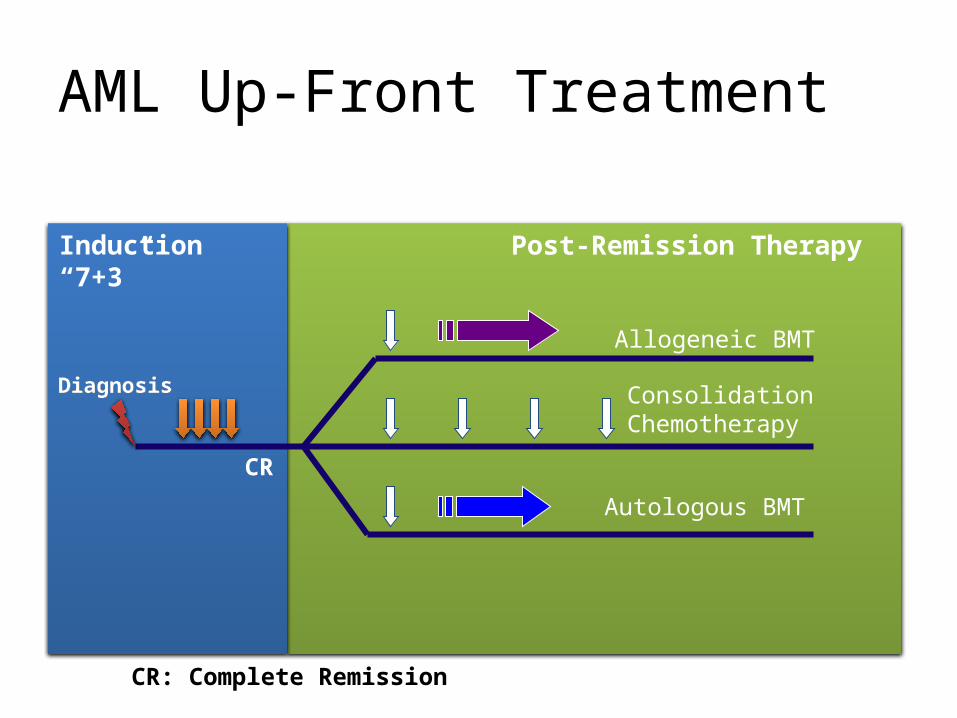
AML Up-Front Treatment
Induction“7+3”
Post-Remission Therapy
CR
Allogeneic BMT
ConsolidationChemotherapy
Autologous BMT
DiagnosisDiagnosis
CR: Complete Remission
First report of “7 + 3”
Cancer Chemotherapy reports Part 1 Vol. 57, No. 4, Nov/Dec 1973
Induction therapy
• 7 + 3• Azacitidine• Decitabine• Clofarabine
DRL
RRL
RR D
DDD
HSCT
D
D
D
D
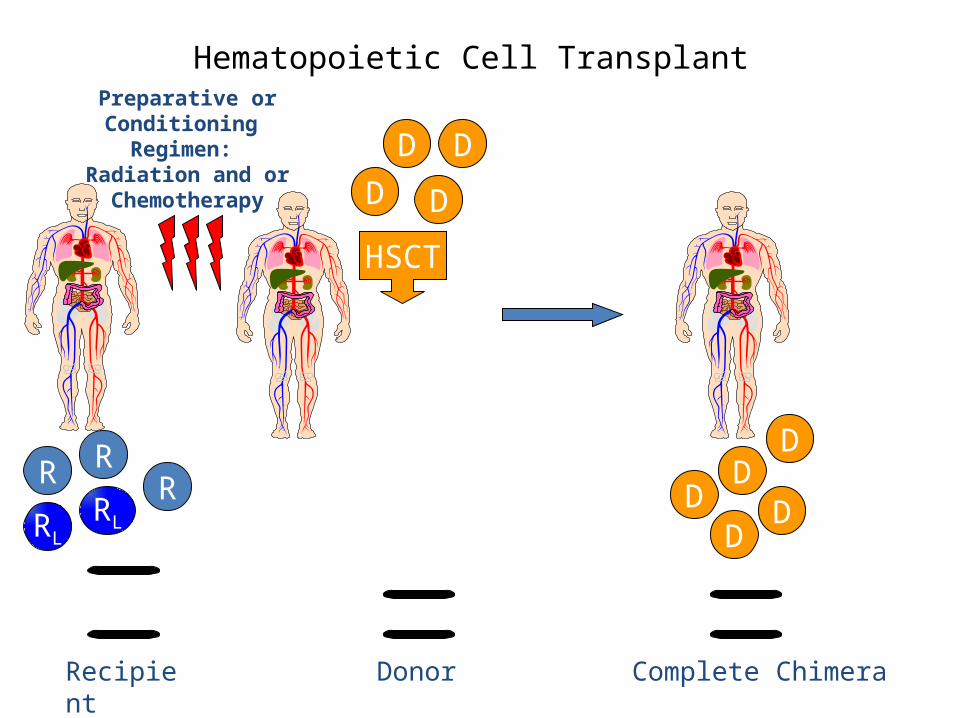
Complete ChimeraRecipient
Donor
Hematopoietic Cell TransplantPreparative or Conditioning
Regimen: Radiation and or Chemotherapy
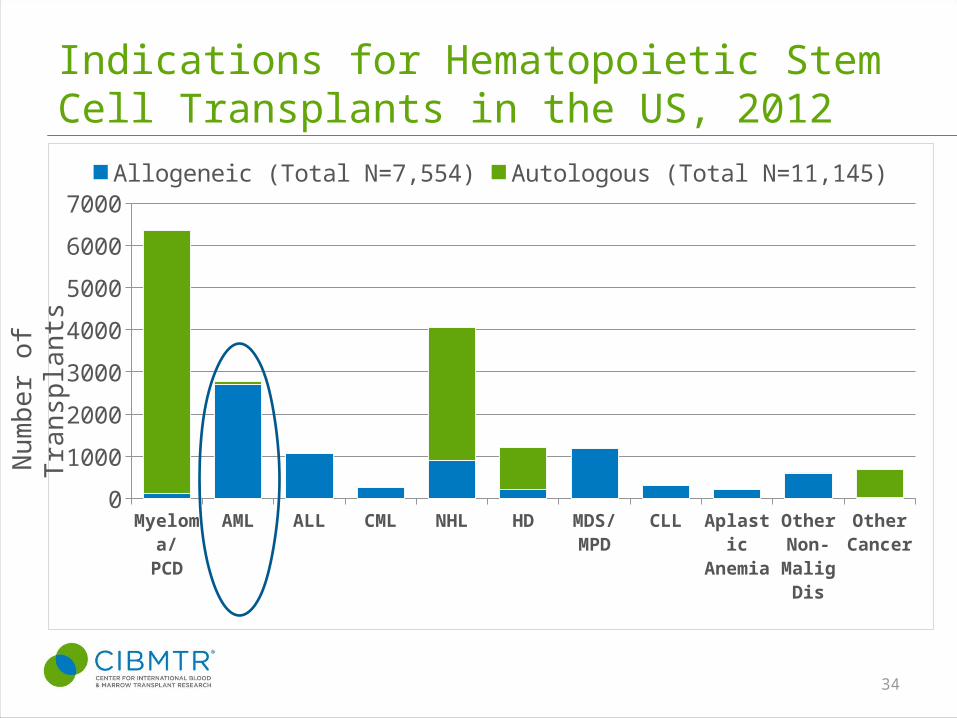
Indications for Hematopoietic Stem Cell Transplants in the US, 2012
Myeloma/PCD
AML ALL CML NHL HD MDS/MPD
CLL Aplastic Anemia
Other Non-Ma-lig Dis
Other Cancer
0
1000
2000
3000
4000
5000
6000
7000
Allogeneic (Total N=7,554) Autologous (Total N=11,145)
34
Nu
mb
er
of T
ran
spla
nts
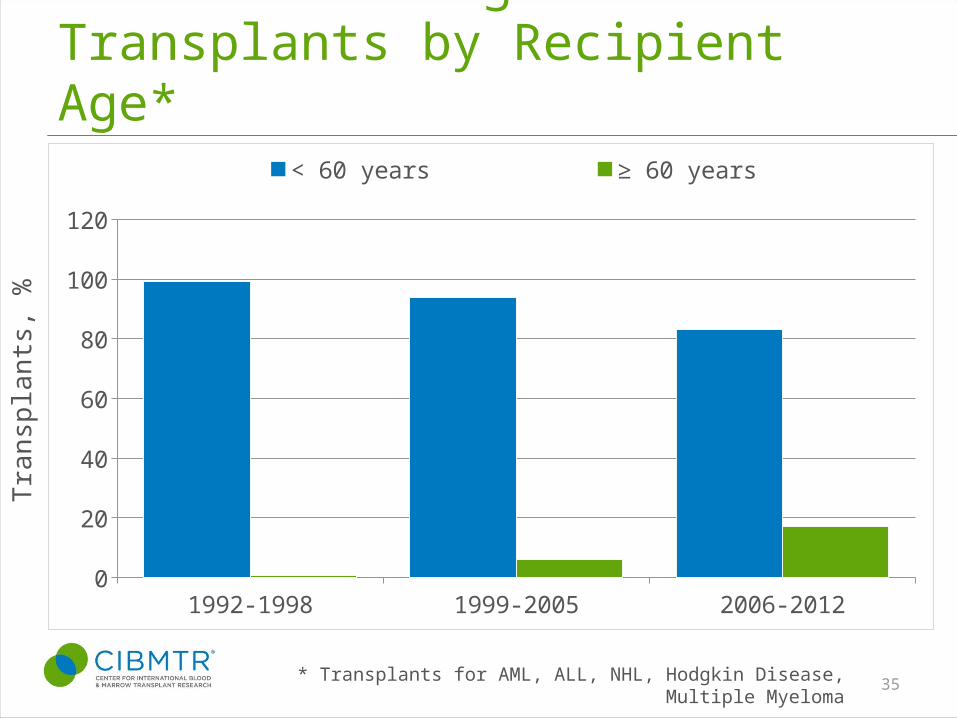
Trends in Allogeneic Transplants by Recipient Age*
1992-1998 1999-2005 2006-20120
20
40
60
80
100
120
< 60 years ≥ 60 years
* Transplants for AML, ALL, NHL, Hodgkin Disease, Multiple Myeloma 35
Tra
nsp
lant
s, %
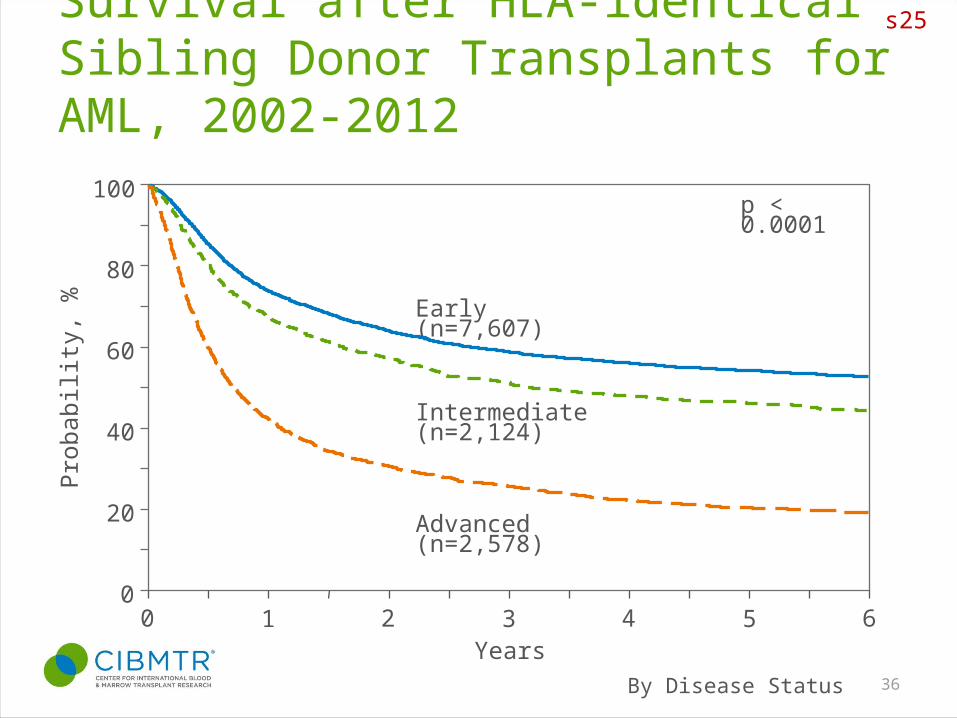
Survival after HLA-identical Sibling Donor Transplants for AML, 2002-2012
By Disease Status 36
100
0
20
40
60
80
Pro
babi
lity,
%
Years
p < 0.0001
Early (n=7,607)
Intermediate (n=2,124)
Advanced (n=2,578)
10 2 64 53
s25
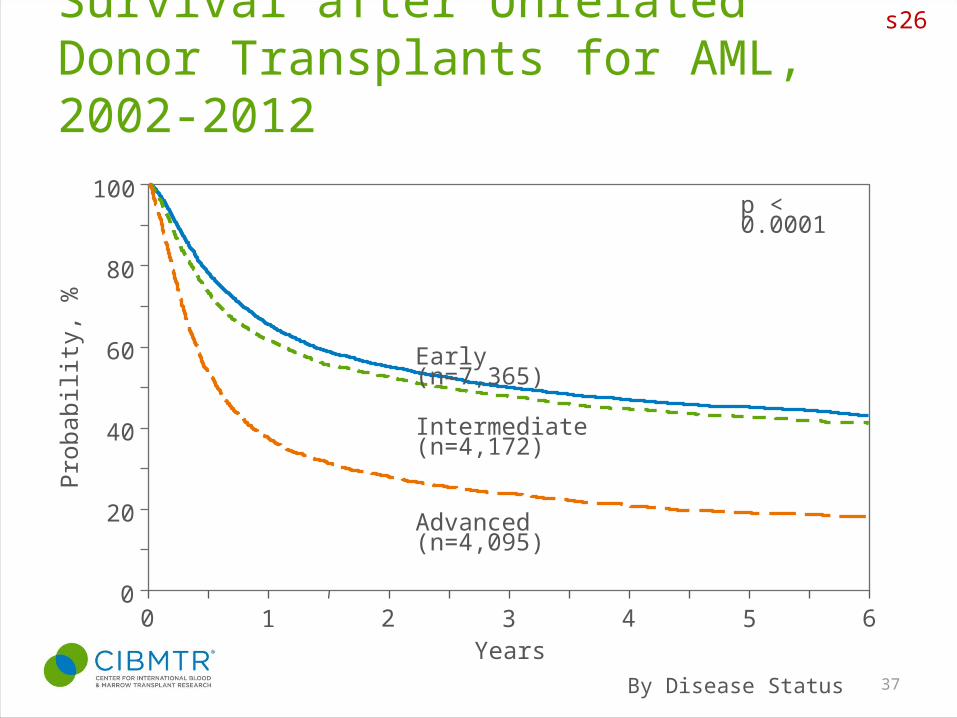
Survival after Unrelated Donor Transplants for AML, 2002-2012
By Disease Status 37
s26
100
0
20
40
60
80
Pro
babi
lity,
%
Years10 2 64 53
Early (n=7,365)
Intermediate (n=4,172)
Advanced (n=4,095)
p < 0.0001
Conclusions
• AML is a heterogeneous disease• Understanding prognosis helps in planning
therapy• Understanding better the biology is helping
the development of new treatments. • Transplants for AML are less toxic and able to
help a greater number of patients.
