addiction is a brain disease: meanings for the anesthesia community art zwerling, dnp, crna, daapm...
TRANSCRIPT

Addiction is a brain disease: Meanings for the anesthesia
community
Art Zwerling, DNP, CRNA, DAAPM
AANA PAAC
April 2013

Grateful Acknowledgements
• Diana Quinlan, CRNA, MA• Heather Hamza, CRNA, MS• Greg Ramplemann, CRNA• Linda Stone, CRNA, MSN• Tony Chipas, CRNA, PhD• Gary Clark, CRNA, EdD• Saundra Dockins, CRNA • Terry Wicks, CRNA, MSHS• Michael Lords, SRNA• Julie Rice, AANA• Don Bell, CRNA, DNSc • Steven D. LaRowe, Ph.D.• AANA BOD

Learning Objectives
– Inform communities of interest regarding the antecedents, risks and consequences of chemical dependency
– Promote awareness of the impact of CD on the anesthesia community
– Review the basic neurobiology of chemical dependency as a chronic brain disease.
– Reduce the incidence of chemical dependency and the impact of CD on the nurse anesthesia profession
History/Background
• Diana Morgan, Minnesota President • 1983 Annual Business Meeting
Resolved: That the American Association of Nurse Anesthetists form a task force to study the impact of chemical dependency upon our profession and to be a source of positive public relations concerning chemical dependency information as it affects our members.

Pioneers in the AANA’s Peer Assistance and Recovering Community
Rusty Ratliff, Diana Quinlan and many other worked to support and find acceptance for the recovering CRNA community

A Rude Awakening…
• Death of Jan Stewart in 2002• Jan Stewart Memorial Lecture
Series 2004• Virginia Trotter Betts 2004• AANA Blue Ribbon Wellness
Panel and establishment of the Wellness Program 2005
• Presidential Wellness TF 2010AANA President
1999-2000
Chemical Dependency
• Substance related disorders characterized by chronicity and progression that threaten wellness..
• Propensity for relapse• Transition to a chronic disease, chronic care model• Subversion of primitive reward and anti-reward
systems• Neuroplasticity

CRNA Statistics
• Approximately 1 in 10 CRNAs becomes addicted during their career (Clark & Stone, 1999)
• 15.8% of CRNAs found to be dependent on alcohol, drugs or both (Berry, 2000)
• Male CRNAs with 6 to 10 years of clinical experience are most at risk for addiction (Bell, 1999)
• 66.7% of SRNAs with substance abuse problems were ranked in the upper third of their graduating class (Clark & Stone, 1999)

Drugs of Choice
• Opioids such as fentanyl and sufentanil are the most commonly cited abused substances by anesthesia providers (Booth, 2002)
• CRNA studies have shown midazolam is the most misused controlled drug among providers (Bell, 1999)

Drug Misuseby PreferenceInside the OR
1. OPIOIDS Fentanyl & Sufenta (Nasal)
2. BENZODIAZEPINES Midazolam (Nasal)
3. N2O4. PROPOFOL5. DISSOCIATIVE DRUGS6. AGONIST/ANTAGONISTS7. BARBITURATES
Bell 2007

Triad of Contributing Factors©
Drug Misuse by CRNAs
Genetics
AVAILABILITY
ACCESSIBILITY
ACCOUNTABILITY
Stress
Fatigue
Invulnerability
Burnout
Prior Experimentation
Adapted from Bell 2007

Warning Signs
• At work during off hours
• Isolation• Frequent breaks• Tardy or Absent• Signing out more
drugs than peers• Inappropriate
dosages, drug choices
• Problematic alcohol use at social functions
Difficulty with authority Forgetful, confused Freq. Illness, physical
complaints Dishonesty (trivial
matters) Elaborate excuses Tremors Long sleeves, alcohol
on breath
Source: AANA Website

Causes of Addiction:Disease Model
• Alcoholism and other addictions represent diseases for which a certain proportion of the population is genetically predisposed– Developed by Dr. Benjamin Rush, late 1700’s– Scientific credence in 1960
• Jellinek’s “Disease Concept of Alcoholism”
– Originally rejected by AMA, but now accepted– Framework for AA and other 12 step groups– Burgeoning support from bench research in the
neurobiology of addictions
Why Do People Take Drugs in The First Place?
To feel good
To have novel:feelings
sensationsexperiences
ANDto share them
To feel betterTo lessen:anxietyworriesfearsdepressionhopelessness
0
50
100
150
200
0 60 120 180
Time (min)
% o
f B
asal
DA
Ou
tpu
t
NAc shell
Empty
Box Feeding
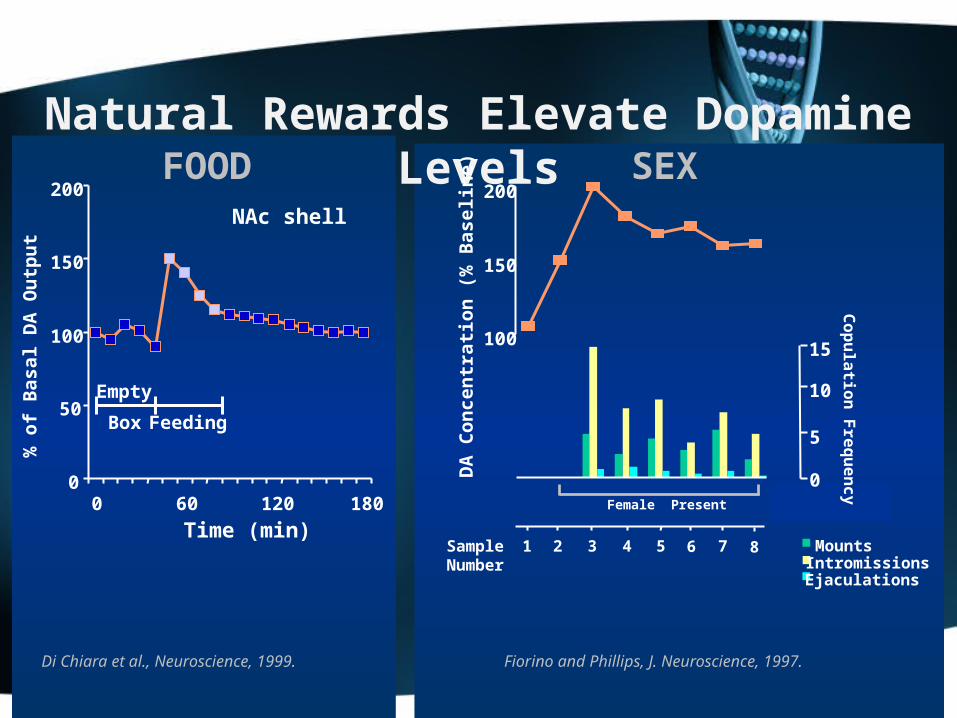
Di Chiara et al., Neuroscience, 1999.
FOOD
MountsIntromissionsEjaculations
Fiorino and Phillips, J. Neuroscience, 1997.
Natural Rewards Elevate Dopamine Levels
100
150
200
DA
Co
nce
ntr
ati
on
(%
Bas
elin
e)
15
0
5
10
Co
pu
latio
n F
req
ue
nc
y
SampleNumber
1 2 3 4 5 6 7 8
SEX
Female Present

0100200300400500600700800900
10001100
0 1 2 3 4 5 hr
Time After Amphetamine
% o
f B
as
al
Re
lea
se
DADOPACHVA
Accumbens AMPHETAMINE
0
100
200
300
400
0 1 2 3 4 5 hrTime After Cocaine
% o
f B
as
al
Re
lea
se
DADOPACHVA
AccumbensCOCAINE
0
100
150
200
250
0 1 2 3 4 5hrTime After Morphine
% o
f B
as
al
Re
lea
se
Accumbens
0.51.02.510
Dose (mg/kg)
MORPHINE
0
100
150
200
250
0 1 2 3 hrTime After Nicotine
% o
f B
as
al
Re
lea
se
AccumbensCaudate
NICOTINE
Di Chiara and Imperato, PNAS, 1988
Effects of Drugs on Dopamine Release

Why do some people become addicted while others do not?
Vulnerability

We Know There’s aBig Genetic Contribution to
Drug Abuse and Addiction…
….Overlapping with Environmental Influences that Help Make
Addiction a Complex Disease.
Biology/genes
Environment
Biology/EnvironmentInteractions

Biology/genes
Environment
Biology/EnvironmentInteractions
Anesthesia
Applicant genome
Stress AccessibilityAccountability Potency

high
low
High DA receptor
Low DA receptor
DA Receptors and the Response to Methylphenidate (MP)
As a group, subjects with low receptor levels found MP pleasant while those with high levels found MP unpleasant
Adapted from Volkow et al., Am. J. Psychiatry, 1999.
Do
pam
ine
rece
pto
r le
vel

Adaptations to reward & anti-reward systems lead to chronic disease
Dancing with the white rabbit: A break from the neuroscience

EMERGING THREAT: PROPOFOL

Another must read
The Misuse and Abuse of Propofol *
Todd Monroe, Heather Hamza, Greg Stocks, Paula Davies Scimeca and Ronald Cowan
*Substance Use & Misuse, Early Online:1–7, 2011 ISSN: 1082-6084 print / 1532-2491 online

Seminal Review Article: Concise, Clear & Comprehensive*
• Critical review of the current state identification, intervention and monitoring.
• There are areas with an incredible paucity of data such as CRNA specific outcomes
• Must read for every anesthesia educator
*The Drug Seeking Anesthesia Care ProviderEthan O. Bryson, MD, Heather Hamza, MS, CRNAInt Anesthesiol Clin. 2011 Winter;49(1):157-71
Evolution of the concept of the high-jacked cortex
• For millennia we have grappled with the perverse polymorphic nature of addictive processes and the behaviors exhibited.
• Addictive behavior appears to defy logical analysis at many levels.
• By exposing how primitive (midbrain) reward & anti-reward system dynamics supersede higher cognitive processes (orbitofrontal) allows us a different perspective on the powerful, cunning, & baffling nature of addiction.

The high jacked cortex
• It certainly can look like demonic possession• The behavior is puzzling, baffling, perplexing and frightening.• Once complete abstinence is achieved an effective denialectomy is possible.

Addictive Thinking Revisited
• Normal Logic: All trees have leaves, this has leaves, this may be a tree.
• Neurotic Logic: All trees have leaves, this has leaves, this may be a tree and when fall comes I’m going to pick up each leaf.
• Psychotic Logic: All trees have leaves, this has leaves therefore I am a tree.
• Addictive Logic: All trees have leaves, this has leaves therefore I need a drink/drug.

The Neurobiology of Addiction
Steven D. LaRowe, Ph.D.
Center for Drug and Alcohol ProgramsMedical University of South Carolina
Substance Abuse Treatment CenterRalph H. Johnson VAMC

Addictive Behavior = Survival Behavior Gone Awry
• Over the course of evolution, we have developed circuitry in our brains that have promoted our survival
• Drugs of addiction activate this “survival circuitry” and with chronic use, essentially take it over
• In the late stages of addiction, an individual is basically a “survivalist” doing whatever it takes to acquire and use drugs regardless of the costs

Addiction: Hijacking the Basic Survival Circuitry

Basic Neurobiology
• Acquisition• Progression• Neuroplasticity• Chronicity & relapse

Healthy Heart Diseased Heart
Decreased Heart Metabolism in Heart Disease PatientDecreased Heart Metabolism in Heart Disease Patient
ADDICTION IS A DISEASE OF THE BRAINas other diseases it affects the tissue function
Control Cocaine Abuser
Decreased Brain Metabolism in Drug Abuse Patient
Sources: From the laboratories of Drs. N. Volkow and H. SchelbertSources: From the laboratories of Drs. N. Volkow and H. Schelbert
High
Low


Source: Adapted from Volkow et al., Neuropharmacology, 2004.
DriveSaliency
Memory
Control
Non-Addicted Brain
NOT GO
Addicted Brain
Drive
Memory
Control
GOSaliency
Addiction Changes Brain CircuitsStop & Go Systems Awry

Dopamine and Glutamate Revisited

Addictive Thinking Revisited
• Normal Logic: All trees have leaves, this has leaves, this may be a tree.
• Neurotic Logic: All trees have leaves, this has leaves, this may be a tree and when fall comes I’m going to pick up each leaf.
• Psychotic Logic: All trees have leaves, this has leaves therefore I am a tree.
• Addictive Logic: All trees have leaves, this has leaves therefore I need a drink/drug.
Neurobiological Basis • Addiction: a condition in which behavior that can function both to produce pleasure and to reduce painful effects is employed in a pattern that is characterized by two key features: (1) recurrent failure to control behavior and (2) continuation of the behavior despite significant harmful consequences (Goodman,2007).
• Dependence: Emergence of a negative emotional state produced by negative reinforcement mechanisms (e.g. dysphoria, anxiety, irritability) when access to the drug is prevented (Koob, 2009).
• Salience: Prioritization of a stimulus in the environment based on its relative importance to the organism’s overall well being or survival. Readily influenced by long-term memory stores or anticipatory mechanisms. *important concept
• Hedonism: Intrinsic value of pleasure. The only value is how much good is produced and how little pain is experienced (Encyclopedia Britannica, 11th ed., 1911).

Allostasis • A state of chronic deviation of the regulatory system from its normal operating level (homeostasis) (Koob et al. 2008).
• A continuous readjustment of all parameters toward a new set point illustrates the construct of this mechanism as “stability through change” (Koob et al. 2008).
• Repeated challenges, such as the case with drugs of abuse, lead to attempts of the brain via molecular, cellular and neurocirciutry changes to maintain stability (Koob et al. 2008).
• The residual deviation from normal brain reward systems threshold is termed the allostatic state (Koob et al. 2008).
Opponent Processes
• Reward system (s) involved in the acquisition of addictions
• Anti-reward system (s) involved in the maintenance of addictions
• Neuroplasticity appears to underpin the chronicity of addictions and propensity for relapse
Neurocircuitry of Addiction
George F. Koob,
& Nora D. Volkow
Neuropsychopharmacology REVIEWS (2010) 35, 217–238 & 2010 Nature Publishing Group

Neuroplasticity Progression
• Figure 5. Neurocircuitry schematic illustrating the combination of neuroadaptations in the brain circuitry for • the three stages of the addiction cycle that promote drug-seeking behavior in the addicted state. Note the activation of the • ventral striatum/dorsal striatum/extended amygdala driven by cues• through the hippocampus and basolateral amygdala and stress through the insula. The frontal cortex system is compromised, • producing deficits in executive function and contributing to the incentive salience of drugs compared to natural reinforcers. • Dopamine systems are compromised, and brainstress systems such as CRF are activated to reset further the salience of drugs and• drug-related stimuli in the context of an aversive dysphoric state
Green= Go Preoccupation CompulsivityBlue= Binge IntoxicationRed= Withdrawal Stress Dysphoria

Dark Side of Addiction
• The transition to a progressive, chronic and relapsing begins with the euphoric effects of these potent intoxicants on primitive reward systems that underpin basic biological survival drives.
• Ultimately maintenance of the addiction cycle is mediated by persistent Neuroplasticity in the reward and anti-reward systems.
• Avoidance of dysphoric states/withdrawal symptoms become the most powerful drivers of persistent addictive behavior.

The Dark Side of Addiction • Development of an aversive emotional state that drives negative reinforcement of addiction (Koob et al. 2008).
• Consists of key motivational elements: chronic irritability, emotional pain, difficulty identifying feelings (alexithymia), malaise, dysphoria, loss of motivation for natural rewards (Koob et al. 2008).
• Two processes involved:–Loss of reward systems–Recruitment of brain stress or anti-reward
systems (Koob et al. 2008)

Neurobiological Basis • There are two key areas of brain arousal and stress mechanisms in the development of dependence:
–Neuropharmacological actions of corticotropin-releasing factor (CRF)
–Norepinephrine in the extrahypothalamic systems in the extended amygdala
• Central nucleus of the amygdala
• Bed nucleus of the stria terminalis
• Transition area in the shell of the nucleus accumbens
(Koob, 2009)

Common pathway

Addiction is Similar to Other Chronic Illnesses Because:
• Recovery from it--protracted abstinence and restored functioning--is often a long-term process requiring repeated treatments
• Relapses to drug abuse can occur during or after successful treatment episodes
• Participation in self-help support programs during and following treatment can be helpful in sustaining long-term recovery
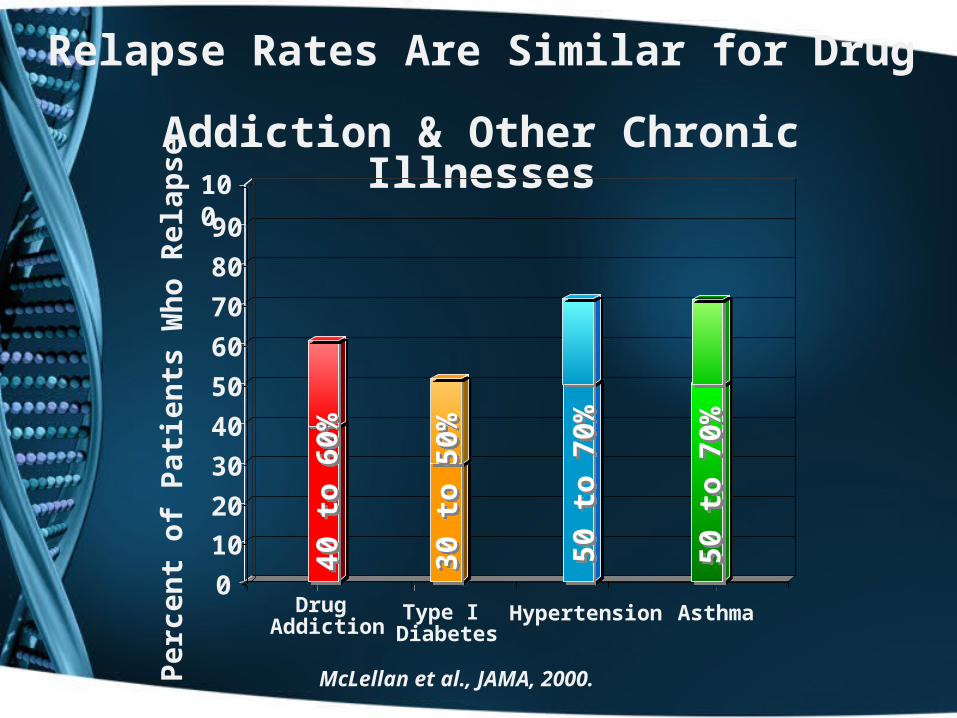
Relapse Rates Are Similar for Drug Addiction & Other Chronic Illnesses
Drug Addiction
Type I Diabetes
0
10
20
30
40
50
60
70
80
90
100
Hypertension Asthma
40 t
o 6
0%40
to
60%
30 t
o 5
0%30
to
50%
50 t
o 7
0%50
to
70%
50 t
o 7
0%50
to
70%
Per
cen
t o
f P
atie
nts
Wh
o R
elap
se
McLellan et al., JAMA, 2000.

Relapse and Relapse Triggers
• Cue based- People Places Things• Exposure- Iatrogenic Mediated• Stress- Alterations in CRF Responsiveness• Defining the dysphoric experience

Stress Susceptibility Model of Addictions
Certain people, due to a variety of biologically-based factors:
• genetics, neurocognitive functioning, stress response
• may be predisposed to developing an addiction to something, be it alcohol, heroin, gambling, sex or other process addictions
• if the right stressor, or combination of stressors, affects the person at a critical time, the person may be more inclined to develop an addiction.
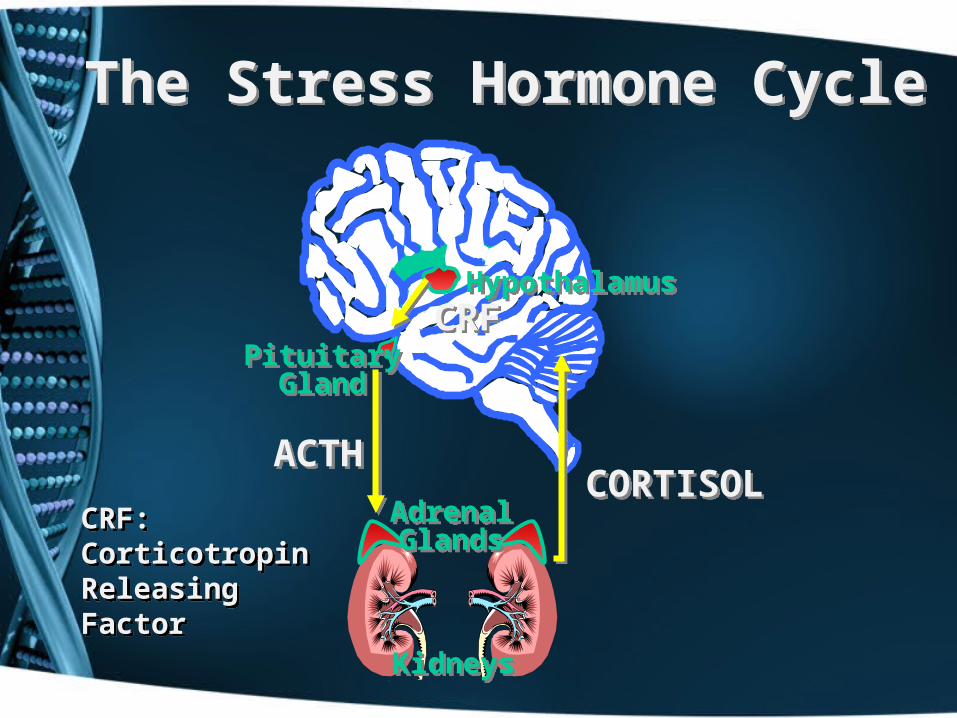
The Stress Hormone CycleThe Stress Hormone Cycle
HypothalamusHypothalamus
PituitaryGland
PituitaryGland
AdrenalGlandsAdrenalGlands
KidneysKidneys
CRFCRF
ACTHACTHCORTISOLCORTISOL
CRF:Corticotropin ReleasingFactor
CRF:Corticotropin ReleasingFactor

DRUG USE(Self-Medication)DRUG USE
(Self-Medication)
STRESSSTRESS
CRFCRF
AnxietyAnxiety
CRFCRF
AnxietyAnxiety
What Role Does Stress Play In Relapse to Drug Use
What Role Does Stress Play In Relapse to Drug Use
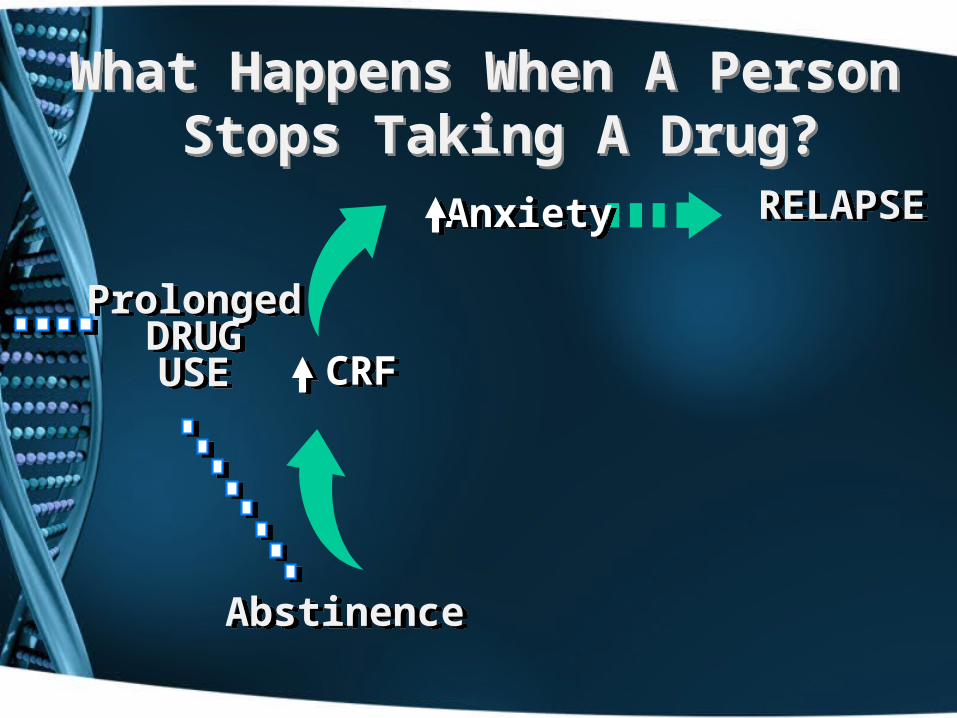
ProlongedDRUGUSE
ProlongedDRUGUSE
AbstinenceAbstinence
RELAPSERELAPSE
CRFCRF
AnxietyAnxiety
What Happens When A Person Stops Taking A Drug?
What Happens When A Person Stops Taking A Drug?

Relapse Triggers: Distinctions
• Stress appears to mediate reinstatement of drug seeking via CRF1 receptor activity in the BNST.
• Contextual relapse appears to be mediated via prefrontal and extended amygdala Glutaminergic afferents to NAC shell.
• Priming (drug exposure) induced relapse appears to be mediated via direct increases in Dopaminergic tone via the VTA to the NAC core.
Sinha R et al Psychological stress, drug-related cues, and cocaine craving. Psychopharmacology 2000; 152:140-148

Relapse Triggers: Limbic Kindling of Craving
• Glutaminergic prefrontal afferents from the prefrontal cortex appear to mediate the experience of craving induced by contextual exposure as evidenced by fMRI.
• Susceptibility to exaggerated responsiveness on exposure to drug related cues appears to persist.

Relapse Triggers: Stress
• Stress appears to mediate reinstatement of drug seeking via CRF1 receptor activity in the BNST
• The mediation of cue associated reinstatement appears to be via Glutaminergic prefrontal inputs into the NAC
• Drug (priming) induced reinstatement appears to induce direct Dopaminergic release between the VTA and NAC.
Sinha R et al Psychological stress, drug-related cues, and cocaine craving. Psychopharmacology 2000; 152:140-148

Relapse Cycle and Recommendations
Chronic Disease Models
• DM as a model
a. We know medication or diet non compliance can lead to relapse.
b. We know that physiologic stressors such as a infective process can lead to an exacerbation.
c. We know that compliance with treatment regimen is the key to disease management!

Case Study: Martin
• Expert cardiothoracic CRNA• Voted favorite preceptor• Played viola in a string
quartet• Adored husband and father• Drug of choice: Fentanyl

Failed Re-entry
• Often it is a unfortunate confluence of circumstances combining stress, failed recognition of place preference and or exposure to kindling cues that leads to relapse.
• Recognition of potential relapse triggers and scenarios are critical to successful re-entry.
• Timing and assessing for readiness for reentry in addition to relapse prevention strategies and resources is also critical to success.
• Emphasis should be on getting it right the first time!

People, Places, Things

Effectiveness of Treatment & Relapse Prevention
Recovery
• According to the Betty Ford Institute, recovery is defined as a voluntary maintained lifestyle characterized by sobriety, personal health, and living with respect for yourself and those around you.
• Recovery is an ongoing process…
…NOT a cure.
Over-riding principles
• Our primary focus needs to be on prevention:
a. screening of applicants and identifying and educating those at high risk
b. toxicology screening
c. increased accountability/decreasing ease of access
• Once we have identified the SRNA/CRNA with a CD the focus is:
First we save lives and then downstream when and where appropriate we may cautiously help resurrect careers.

Take Homes
• CD is a chronic disease with similar compliance and relapse issues to other chronic diseases such as DM and HTN.
• Chronicity and relapse potential can be explained by persistent neuroplastic alterations in the CNS.
• New pharmacotherapy strategies may assist as a part of a multimodality approach to increase long term recovery in some cases.
• We need to take the long view and focus on relapse prevention!

References
• Auer JA: Learning mechanisms in addiction: synaptic plasticity in the ventral tegmental area as a result of exposure to drugs of abuse. Annu Rev Physiol 2004, 66:447-475.
• Gardner E - What we have learned about addiction from animal models of drug self-administration Am J Addict 2000;9:285-313

References
• Faleiro LJ, Jones S, Kauer JA: Rapid synaptic plasticity of glutamatergic synapses on dopamine neurons in the ventral tegmental area in response to acute amphetamine injection. Neuropsychopharmacology, 2004, 29, 2115-2125
• Fattore,L., Spano, S., Deiana,S., Melis, V. Cossu, G., Fadda,P. & Fratta, W. An endocannabinoid mechanism in relapse to drug seeking: A review of animal studies and clinical perspectives Brain Research Reviews, In Press, Corrected Proof, Available online 12 July 2006
References
• Kauer, J. A.: Learning Mechanisms in Addiction:Synaptic Plasticity in the Ventral TegmentalArea as a Result of Exposure to Drugs of AbuseAnnu. Rev. Physiol. 2004. 66:447–75
• Kim JA, Pollak KA, Hjelmstad GO, Fields HL: A single cocaine exposure enhances both opioid reward and aversion througha ventral tegmental area-dependent mechanism. Proc Natl Acad Sci USA 2004, 101:5664-5669.

References
• Nestler, E J: Molecular basis of long-term plasticity underlying addiction. Nat Rev Neurosci 2001; 2:119–128;
• Nestler, E J: Molecular Biology of Addiction. Am J of Addictions 10:201-217, 2001
• Nestler, E J, Malenka, R C: Biotechnology:
The Addicted Brain, Scientific American, April 2004, retrieved online on the WWW at:
http://www.sciam.com/article.cfm?articleID=0001E632-978A-1019-978A83414B7F0101&sc=I100322 on 7-20-06.

References
• Sinha R et al Psychological stress, drug-related cues, and cocaine craving.
• Psychopharmacology 2000; 152:140-148• Volkow ND, Wang G-J, Ma Y, Fowler JS,
Zhu W, Maynard L, Telang R, Vaska P, Ding Y-S, Wong C, Swanson JM: Expectation enhances the regional brain metabolic and the reinforcing effects of stimulants in cocaine abusers. J Neurosci 2003; 23:11461–11468

References
• Volkow ND, Fowler JS, Wang GJ, Swanson JM: Dopamine in drug abuse and addiction: results from imaging studies and treatment implications. Mol Psychiatry, 2004, 9:557–569.
• Volkow ND, Wang GJ, Telang F, Fowler JS, Logan J, Childress AR, Jayne M, Ma Y, Wong C: Cocaine cues and dopamine in dorsal striatum: mechanism of craving in cocaine addiction. The Journal of Neuroscience, June 14, 2006, 26(24):6583-6588
Resources
• AANA PEER ASSISTANCE:
http://www.aana.com/peerassist.aspx• AIR (Anesthetists in Recovery):
[email protected] or 215-635-0183• AANA Wellness:
http://tinyurl.com/6du96lj