advanced wound closure - cdn.ymaws.com · closure types • primary closure (primary intention) –...
TRANSCRIPT

7/16/18
1
Advanced Wound Closure
• M ic h a e l H a z e l , D N P, R N , F N P - B C
• S t e v e B r a n h a m , P h D , R N , F N P, A C N P
• T a r a L . R o b e r t s M S N , R N , A N P - B C
What to expect today..• D iscuss different types of w ound healing techniques and assessm ents
• Identify different suture types and uses in the clinical setting
• D iscuss several w ound considerations and/or com plications that can arise during
healing process
• Practice, practice, practice
Types of Sutures• A b s o r b a b le o r n o n - a b s o r b a b le ( n a t u r a l o r s y n t h e t i c )
• M o n o f i la m e n t o r m u l t i f i l a m e n t ( b r a id e d )
• D y e d o r u n d y e d
• S iz e s 3 t o 1 2 - 0 ( n u m b e r s a lo n e in d ic a t e p r o g r e s s iv e ly
la r g e r s u t u r e s , w h e r e a s n u m b e r s f o l lo w e d b y 0 in d ic a t e p r o g r e s s iv e ly s m a l le r )
• N e w a n t ib a c t e r ia l s u t u r e s

7/16/18
2
Suture
Natural Suture• Biological• Cause inflammatory reaction
–Catgut (connective from cow or sheep)
–Silk (from silkworm fibers)–Chromic catgut
Synthetic• Synthetic polymers• Do not cause inflammatory response
–Nylon–Vicryl–Monocryl–PDS–Prolene
Suture
Monofilament• Single strand of suture m aterial
• M inim al tissue traum a
• Sm ooth tying but m ore knots needed
• H arder to handle due to m em ory
• Exam ples: nylon, m onocryl, prolene, PD S
Multifilament (braided)• Fibers are braided or tw isted
together
• M ore tissue resistance
• Easier to handle
• Few er knots needed
• Exam ples: vicryl, silk, chrom ic
SutureA b s o r b a b le
• N ot biodegradable and perm anent
–Nylon–Prolene–Stainless steel–Silk (natural, can
break down over years)
N o n - A b s o r b a b le
• D egraded via inflam m atory response
–Vicryl–Monocryl–PDS–Chromic–Cat gut (natural)
7/16/18
3
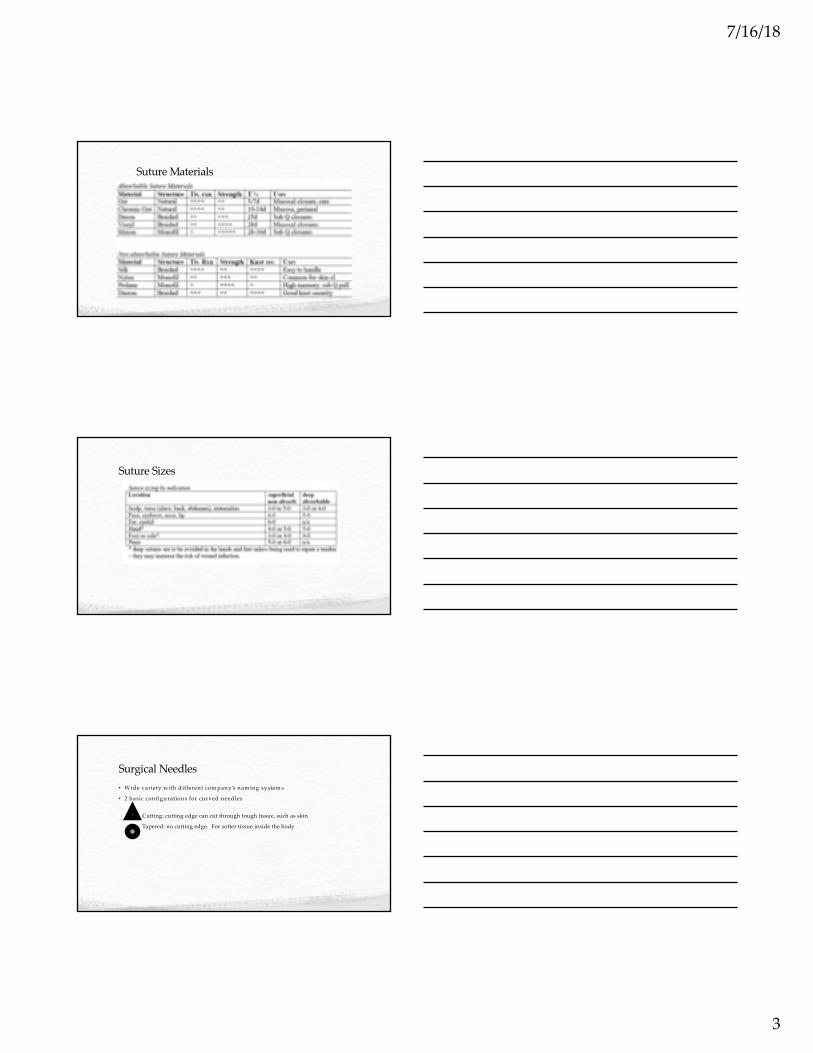
Suture Materials
Suture Sizes
Surgical Needles• W ide variety w ith different com pany’s nam ing system s
• 2 basic configurations for curved needles
Cutting: cutting edge can cut through tough tissue, such as skin
Tapered: no cutting edge. For softer tissue inside the body
7/16/18
4
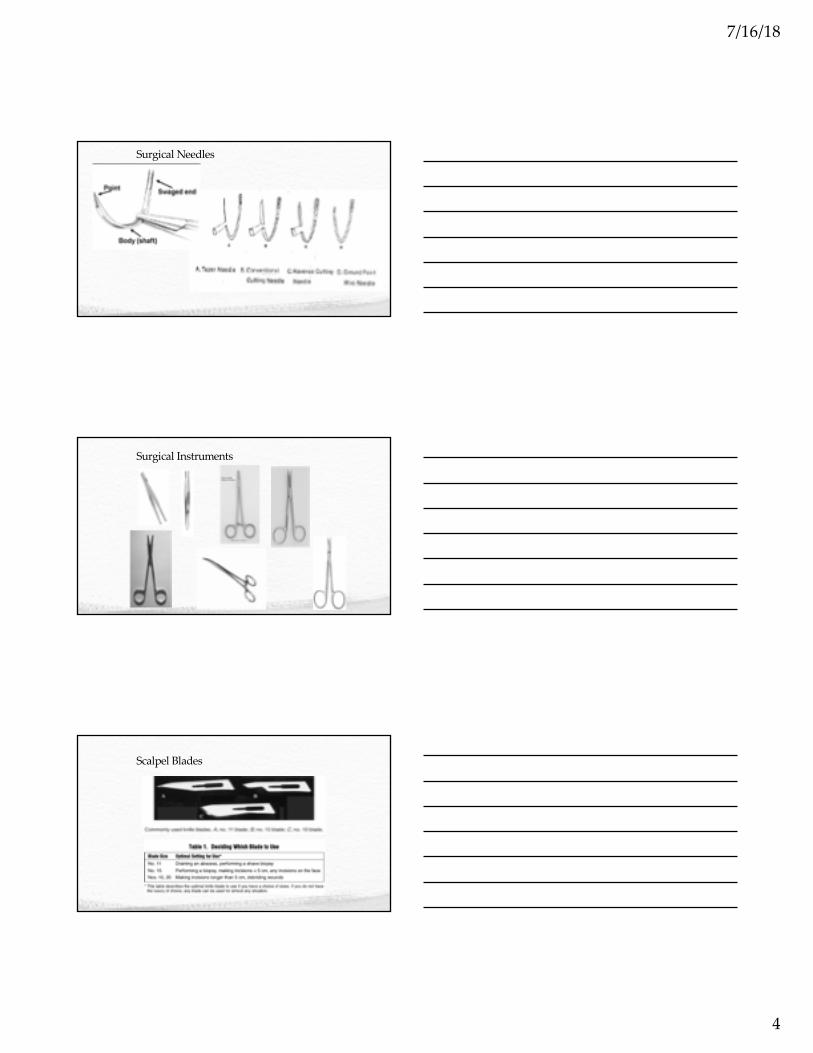
Surgical Needles
Surgical Instruments
Scalpel Blades
7/16/18
5
Wound Evaluation• Tim e of incident
• Size of w ound
• D epth of w ound
• Tendon / nerve involvem ent
• Bleeding at site
When to Refer•Deep wounds of hands or feet, or unknown depth of penetration• Full thickness lacerations of eyelids, lips or ears• Injuries involving nerves, larger arteries, bones,
joints or tendons•Crush injuries•Markedly contaminated wounds requiring
drainage•Concern about cosmesis
Contraindications to Suturing• R e d n e s s
• E d e m a o f t h e w o u n d m a r g in s
• I n f e c t io n
• F e v e r
• P u n c t u r e w o u n d s
• A n im a l b i t e s
• T e n d o n , n e r v e , o r v e s s e l in v o lv e m e n t
• W o u n d m o r e t h a n 1 2 h o u r s o ld ( b o d y ) a n d 2 4 h r s( f a c e )
7/16/18
6
Wound Cleaning• Consider…– Hand washing
– Personnel precautions
– Hair removal– Anesthesia
– Foreign material– Wound soaking
Wound Cleaning• H and washing (after patient contact before proceeding to the next)
– Nurses 58.2%– Residents 18.6%
– Faculty 17%
Wound Preparation• M o s t im p o r t a n t s t e p f o r r e d u c in g t h e r i s k o f w o u n d in f e c t io n .
• R e m o v e a l l c o n t a m in a n t s a n d d e v i t a l iz e d t i s s u e b e f o r e w o u n d c lo s u r e .
– I R R I G A T E w / N S o r T A P W A T E R ( A V O I D H 2 O 2 , P O V I D O N E -I O D I N E )
– C U T O U T D E A D , F R A G M E N T E D T I S S U E
• I f n o t , t h e r i s k o f in f e c t io n a n d o f a c o s m e t i c a l ly p o o r s c a r a r e g r e a t ly in c r e a s e d
• P e r s o n a l P r e c a u t io n s
7/16/18
7
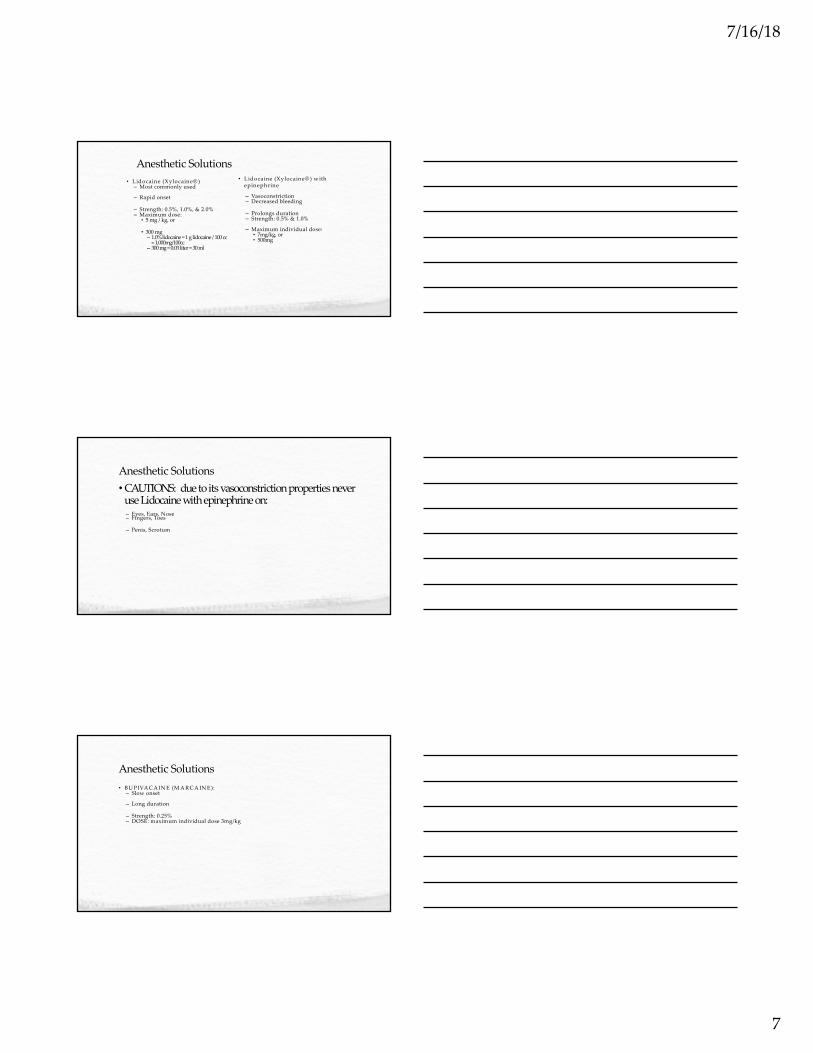
Anesthetic Solutions
• Lidocaine (Xylocaine® ) – Most commonly used
– Rapid onset
– Strength: 0.5%, 1.0%, & 2.0% – Maximum dose:• 5 mg / kg, or
• 300 mg – 1.0% lidocaine = 1 g lidocaine / 100 cc
= 1,000mg/100cc– 300 mg = 0.03 liter = 30 ml
• Lidocaine (Xylocaine® ) w ith epinephrine
– Vasoconstriction– Decreased bleeding
– Prolongs duration – Strength: 0.5% & 1.0%
– Maximum individual dose:• 7mg/kg, or• 500mg
Anesthetic Solutions•CAUTIONS: due to its vasoconstriction properties never
use Lidocaine with epinephrine on: – Eyes, Ears, Nose – Fingers, Toes
– Penis, Scrotum
Anesthetic Solutions
• BU PIVA CA IN E (M A RCA IN E):– Slow onset
– Long duration
– Strength: 0.25%– DOSE: maximum individual dose 3mg/kg
7/16/18
8
Local Anesthetics
Injection Techniques• 25, 27, or 30-gauge needle
• 6 or 10 cc syringe
• Check for allergies
• Insert the needle at the inner w ound edge
• A spirate
• In ject agent into tissue SLO W LY
• Wait…
• A fter anesthesia has taken effect, suturing m ay begin
Closure Types
• Primary closure (primary intention)– Wound edges are brought together so that they are adjacent to each
other (re-approximated) – Examples: well-repaired lacerations, well reduced bone fractures,
healing after flap surgery
• Secondary closure (secondary intention)
– Wound is left open and closes naturally (granulation)– Examples: gingivectomy, gingivoplasty,tooth extraction sockets,
poorly reduced fractures
• Tertiary closure (delayed primary closure)– Wound is left open for a number of days and then closed if it is
found to be clean
– Examples: healing of wounds by use of tissue grafts.

7/16/18
9
Vertical Mattress
Good for everting wound edges (neck, forehead creases, concave surfaces)
http://www.youtube.com/watch?v=824FhFUJ6wc

7/16/18
10
Vertical Mattress Suture
Horizontal Mattress
Good for closing wound edges under high tension,and for hemostasis.
Horizontal Mattress
http://www.youtube.com/watch?v=9DdaooEXshk
7/16/18
11
Subcuticular Suture
http://www.youtube.com/watch?v=I7C7nsl5Tuk
The trick to an instrument tie
•Always place the suture holder parallel to the wound’s direction.
•Hold the longer side of the suture (with the needle) and wrap OVER the suture holder.
•With each tie, move your suture-holding hand to the OTHER side.•By always wrapping OVER and moving the hand to the
OTHER side = square knots!!
7/16/18
12
Suturing - finishing
• A fter sutures placed, clean the site w ith norm al saline.
• A pply a sm all am ount of Bacitracin or w hite petroleum and cover w ith a sterile
non-adherent com pression dressing (Tefla).
Suturing - before you go…
• N eed for tetanus globulin and/or vaccine?– D irty (playground nail) vs clean (kitchen knife)– Im m unization history (>10 yrs need booster or >5 yrs if
contam inated)
• Tell pt to return in one day for recheck, for signs of infection (redness, heat, pain, puss, etc), inadequate analgesia, or suture com plications (suture strangulation or knot failure w ith possible w ound dehiscence)
• It should be em phasized to patients that they return at the appropriate tim e for suture rem oval or com plications m ay arise leading to further scarring or subsequent surgical rem oval of buried sutures.
Patient instructions and follow up care• W o u n d c a r e
– A f t e r t h e f i r s t 2 4 - 4 8 h o u r s , p a t ie n t s s h o u ld g e n t ly w a s h t h e w o u n d w i t h s o a p a n d w a t e r , d r y i t
c a r e f u l ly, a p p ly t o p ic a l a n t ib io t i c o in t m e n t , a n d r e p la c e t h e d r e s s in g / b a n d a g e s .
– F a c ia l w o u n d s g e n e r a l ly o n ly n e e d t o p ic a l a n t ib io t i c
o in t m e n t w i t h o u t b a n d a g in g .– E s c h a r o r s c a b f o r m a t io n s h o u ld b e a v o id e d .
– S u n s c r e e n s p f 3 0 s h o u ld b e a p p l ie d t o t h e w o u n d t o
p r e v e n t s u b s e q u e n t h y p e r p ig m e n t a t io n .
7/16/18
13
Suture Removal
• Average time frame is 7 – 10 days– FA C E : 3 – 5 d
– N E C K : 5 – 7 d
– S C A L P : 7 – 1 2 d a y s– U P P E R E X T R E M IT Y, T R U N K : 1 0 – 1 4 d a y s
– L O W E R E X T R E M IT Y : 1 4 – 2 8 d a y s– S O L E S , PA L M S , B A C K O R O V E R JO IN T S : 1 0 d a y s
•Any suture with pus or signs of infections should be removed immediately.
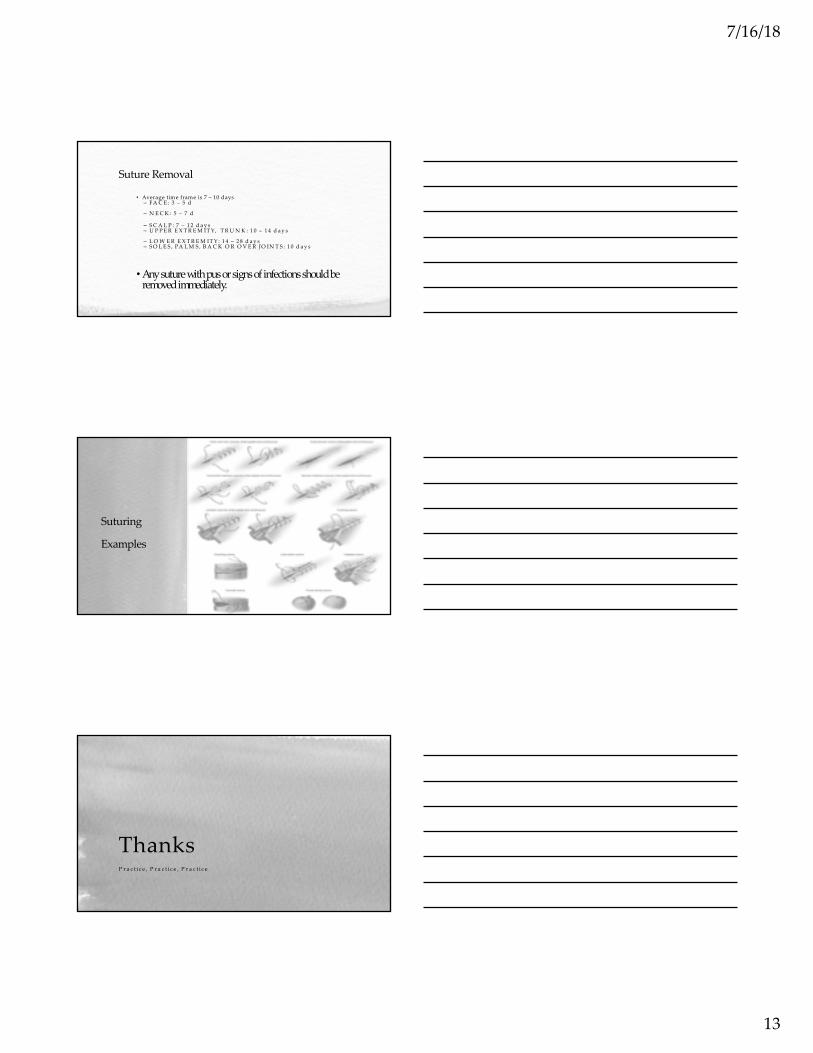
Suturing
Examples
ThanksP r a c t i c e , P r a c t i c e , P r a c t i c e