alkylnitriles viruses formaldehydes bacterias hydrogen cyanides...
TRANSCRIPT

An information for medical staff and patients
Smoke by-products in laser and electrosurgical procedures
● alkylnitriles● viruses● formaldehydes● bacterias● hydrogen cyanides● priones
MedizinTechnik
2
Hepatitis B
Hepatitis C
HPV
HIV
Introduction
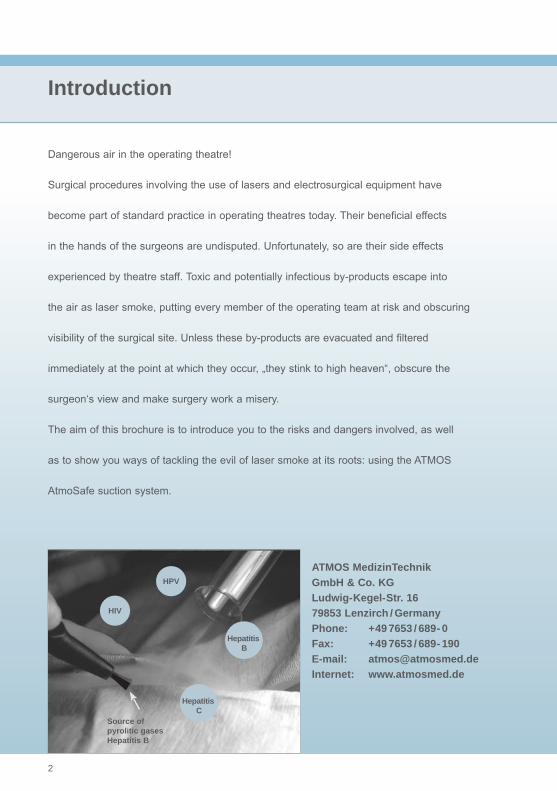
Dangerous air in the operating theatre!
Surgical procedures involving the use of lasers and electrosurgical equipment have
become part of standard practice in operating theatres today. Their beneficial effects
in the hands of the surgeons are undisputed. Unfortunately, so are their side effects
experienced by theatre staff. Toxic and potentially infectious by-products escape into
the air as laser smoke, putting every member of the operating team at risk and obscuring
visibility of the surgical site. Unless these by-products are evacuated and filtered
immediately at the point at which they occur, „they stink to high heaven“, obscure the
surgeon‘s view and make surgery work a misery.
The aim of this brochure is to introduce you to the risks and dangers involved, as well
as to show you ways of tackling the evil of laser smoke at its roots: using the ATMOS
AtmoSafe suction system.
ATMOS MedizinTechnik GmbH & Co. KG
Ludwig-Kegel-Str. 16 79853 Lenzirch / Germany
Phone: +49 7653 / 689- 0 Fax: +49 7653 / 689- 190
E-mail: [email protected] Internet: www.atmosmed.de
Source ofpyrolitic gases Hepatitis B

MedizinTechnik
3
List of contents
Chapter Page
Introduction 3 Frequently asked questions (FAQs) 5- 6 Guidelines 7 How are laser aerosols generated? 8 The process of generation 9 The tissue explodes 9-10 Size of particles 10 Chemical compounds in laser plumes 11 Danger of laser plumes 11-12 Risks of infection 12 Bad odour 12 Protective measures I 13- 18 AtmosSafe for smoke evacuation in medicine 19- 20 Appendix I 22-26 Appendix II 27-29 Glossary 30-34
4
Frequently asked questions:
1. Is normal operating theatre ventilation adequate for evacuating smoke? No, the rate of air circulation in the room - up to 24 x volume / hour - is not sufficient to evacuate locally generated aerosols and gases; the user is still exposed to dangerous laser smoke.
2. So a normal room suction system (a central vacuum) is not good enough? No, the rate of room suction in an operating theatre is too low, at 30-40 l / min. Research has shown that a minimum of 400-600 l / min. is required in the operating field. 3. How great is the risk of becoming infected from biological substances during an operation? Research is currently being undertaken to ascertain the degree of danger that exists from using different lasers and electrosurgical instruments. It has been proven that infectious particles can reach theatre staff and thereby create an acute risk of infection via the mucous membranes and respiratory tracts.
4. So are the particles generated during an operation really dangerous? Airborne viruses such as papilloma viruses, proteins such as prions (BSE pathogens) and other airborne bacteria and funghi are dangerous substances that can lead to direct infection.
5. Do surgical face masks help protect the operating staff? No, surgical face masks offer theatre staff no protection against airborne particles. These masks were designed to protect patients from droplet infections emanating from the operating team. Up to 25 % of air breathed in gets past the mask.
6. Are there other reasons for carrying out localised smoke evacuation, apart from the risk of infection? The use of local smoke evacuation, when carried out during endoscopies, minimally invasive surgery and partially open and closed body cavities, gives optimum visibility.

MedizinTechnik
5
Frequently asked questions
7. How do doctors react to smoke evacuation devices? Smoke evacuation enjoys a high level of acceptance among medics, as they no longer have to contend with an obscured view of the surgical site. 8. What effects do particles and gases have on the patient? During laparoscopies in particular, toxic gases diffuse into the patient‘s bloodstream. Small airborne particles in this smoke (measuring from 0.1 to 0.5 μm) cause ocular and upper respiratory tract irritation.
9. Is there a risk to the patient? Medical staff should be aware of the risks to the patient from laser use and diathermic smoke generation during an operation. Some of the smoke inside a closed abdominal cavity can lead to an increase in methaemoglobin content, which reduces the capacity of body tissue to absorb oxygen.
10. Does the suction device have to be operated separately? No, the suction device runs in the background; assistant theatre staff do not need to devote any resources to operating it. The smoke evacuation unit is activated automatically when needed.
11. How high are the running costs of local smoke evacuation? The operating costs of the filter system are less than 1 Euro per surgical procedure and the filter unit has a life of up to 52 hours, depending on flow.
12. Do lasers deactivate dangerous airborne viruses? No, research on retroviruses has shown that infectious viruses and constituents of virus DNA are carried in laser smoke. So it is possible to be infected, for example, by papilloma viruses in the laser smoke.
Local smoke evacuation - making things easier for theatre staff and patient alike!
6
Guidelines
American National Standard Institute (ANSI)
National Institute for Occupational Safety and Health (NIOSH)
National Safety and Health Act (OSHA)
American Society for Laser Medicine and Surgery (ASLMS)
US-Department of Health and Human Services (DHHS)
Centers for Disease Control and Prevention (CDC)
National Association of Theatre Nurses
Canadian Centre for Occupational Health and Safety
Medical Devices Agency
CEN/ DIN (European commission for standardization,
German institute for standardization)
BGW (professional association for health and welfare care)
Biostoffverordnung (TRBA, technical rules für biologic working materials)
MedizinTechnik
7
3)
2)1)
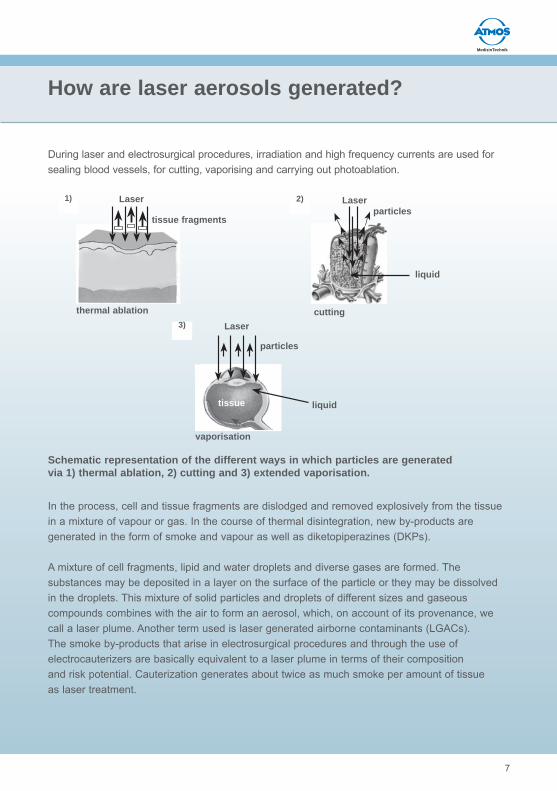
During laser and electrosurgical procedures, irradiation and high frequency currents are used for sealing blood vessels, for cutting, vaporising and carrying out photoablation.
In the process, cell and tissue fragments are dislodged and removed explosively from the tissue in a mixture of vapour or gas. In the course of thermal disintegration, new by-products are generated in the form of smoke and vapour as well as diketopiperazines (DKPs).
A mixture of cell fragments, lipid and water droplets and diverse gases are formed. The substances may be deposited in a layer on the surface of the particle or they may be dissolved in the droplets. This mixture of solid particles and droplets of different sizes and gaseous compounds combines with the air to form an aerosol, which, on account of its provenance, we call a laser plume. Another term used is laser generated airborne contaminants (LGACs).The smoke by-products that arise in electrosurgical procedures and through the use ofelectrocauterizers are basically equivalent to a laser plume in terms of their compositionand risk potential. Cauterization generates about twice as much smoke per amount of tissue as laser treatment.
How are laser aerosols generated?
Schematic representation of the different ways in which particles are generatedvia 1) thermal ablation, 2) cutting and 3) extended vaporisation.
Laser
tissue fragments
thermal ablation
Laserparticles
liquid
cutting
particles
liquid
Laser
vaporisation
tissue

8
The process of generation
The way laser light works is that its energy beam is absorbed by chromophores (porphyrins, melanins) and water in body tissue. Factors that determine the depth of penetration and the degree of energy absorption include not only the wavelength of the laser light, which may range from UV through to deep infrared (100-10600 nm), but also the energy per area (or fluence), the type of irradiation (pulse or continuous wave) and the duration of laser impact. As the temperature rises, the following processes occur:
Coagulation
Coagulation is the formation of new networks of macromolecular tissue structures. The irradiated tissue matrix remains in place, so there are hardly any emissions of coagulation products.
Vaporisation
Vaporisation of tissue fluid and volatile parts of tissue structures occurs at temperatures of more than 100° C. The structures of the tissue matrix are released by the stream of vapour in both solid and liquid form.
Denaturisation of protein structures
Melanisation (browning)
1. Formation of solid Maillard products2. Fat oxidation 3. Carbonisation
At the centre of the laser‘s target area, temperatures rise as high as 700 to 800 degrees C.
The tissue explodes (plasma formation)
Velocities of several hundred metres per second have been recorded; evidence fromacoustic phenomena even suggests that particles move at the speed of sound. Twoquotations on this from the literature:
“By evaluating recoil momentum and mass loss data, the average initial velocity of theplume was calculated to be 230 to 280 m/s. The kinetic energy is approximately 1 % ofthe input energy. The measurements lend support to the hypothesis of a thermallyinduced explosive process”. (Lasers Surg Med 1992; 12 (2): 125 - 30)
MedizinTechnik
9
The tissue explodes / Size of particles
“…the velocity for the first 500 ns following the excimer pulse averages 400 m / s at193 nm. Plume size and velocity increase with increasing fluence”.(Arch Ophthalmol 1987 Sep; 105(9): 1255 - 9)
Particle sizes of 0.1 μm upwards
Particles that have been flung out have a diameter of 0.1 to 10 μm. Larger particlesare less common but can be carriers of infectious material. Generally speaking, thehigher the fluence is, the smaller the particles are. Particles of up to 1.2 μm are highlyviscous and transparent; if they are more than 1.2 μm they appear brownish to blackand solid like dust. Only particles below 10 μm are considered as “airborne”.
Particles in the region of 0.1 - 1 μm are generated through condensation of vaporisedcell constituents. Particles of 1 - 10 μm are dried cell fragments that are flung outexplosively during vaporisation of the tissue fluid. If the tissue is fatty, as in liver parenchyma,the proportion of lipid droplets present is noticeably higher.
Up to 350 volatile chemical compounds in laser plumes
With regard to electrosurgical plumes there is a distinction drawn between biologicaland chemical components.Cell tissue consists of macromolecules (proteins, peptides, oligosaccharides, polysaccharidesand nucleotides) and compounds such as lipids, carbohydrates and aminoacids. During pyrolysis, that is, incomplete thermic disintegration of human tissue, newchemical substances are generated. These pyrolytic products split under the impact ofthe laser and form new compounds.So far 350 volatile chemical compounds have been identified in laser plumes as wellas up to 43 DKPs (diketopiperazines). Many of these are regarded as harmless or arecontained in everyday foodstuffs. Smoke generated from a laser releases about50 -150 mg of a complex mixture of substances per gramme of vaporised tissue.

10
Chemical compounds in laser plumes
How dangerous are laser plumes?
The extent to which people working in the operating theatre will be affected by these chemicals depends partly on the general rate of air ventilation in the room. In operating theatres in clinics air circulation is generally better than in outpatient practices, at up to 24 x room volume / hour. Some chemical components have the potential to cause irritation of the mucous membranes, to possess cell and gene toxicity, to be mutagenic, carcinogenic and to provoke allergic reactions. It is a matter of dispute and is indeed unclear whether the amounts contained in a laser plume are sufficient to actually generate these effects in people exposed them, especially as the exact composition of the plume depends on the tissue type being treated as well as on fluence, the temporal parameters and the wavelength of the laser being used. The chemical spectrum rangesfrom carbon monoxide and slightly volatile alkanes (VOC) through polycyclical aromatichydrocarbons (PAH), mutagenic, heterocyclical amines, formaldehyde, acroleinand benzene to hydrogen cyanide and alkylnitriles.It is even suspected that another possible source of risk is anaesthetic gases containing CFCs: they supposedly split off their halogen substituents under laser impact. These radicals can react with organic material in the living cell and form hydrohalogenic acids.
Schematic overview of pyrolytic products during medical use of lasers

MedizinTechnik
11
Danger of laser plumes
The biological risks from dispersion of intact pathogenic material are considered to bemore critical in the literature. Risks emanate from microorganisms (bacteria, viruses,funghi); bioaerosols serve as a medium of transportation for intact infectious material.The literature describes a potential viral risk especially through hepatitis B and humanpapilloma viruses and also, of course, through retroviruses such as HIV and hepatitis C.Retroviruses retain their infectivity for a long time when they come into contact withmucous membranes and sores. Their prevalence in the population is constantly on theincrease due to the spread of AIDS and hepatitis C. Bacterial pathogens include in particularStaph. aureus, resistant strains of Mycobact. tuberculosis and Escherichia coli.
Patients are particularly at risk during minimally invasive laser and electrosurgery. Individual gas components can get into the patient‘s bloodstream unless they are evacuated immediately. If unfiltered laparoscopy gases escape into the room, they too pose a risk to the operating team.
The stench is appalling
Surgical practice is dominated by a pungent, nauseating odour that can generatetears, sickness, stomach cramps, vomiting and irritation of the respiratory tract.It is mainly caused by heterocyclical amines.Although the existence of active viral DNA in laser plumes has been proven, the literaturecontains only very isolated references to proven infections (aetiologically uncertain laryngeal papillomatosis of a surgeon, Hallmo and Naess, 1991, and Gloster and Roenigk 1995).
What is definitely a problem is the proportion of the laser plume that is able to penetrateinto the alveoli: 80- 90 % of all particles are smaller than 2 μm, that is, they are completelyinhalable and capable of alveolar penetration. They are deposited in the alveoli and bronchioles in the lungs (70 - 90 m² surface area), where no mucociliary cleaning takes place. Certain fine dust particles are also a concern as potential allergens.
Surgery using electrosurgical equipment

12
Protective measures
The legal situation is clear !
There is no justification for exposing medical staff or patients to laser plumes containinghuman tissue - all the experts agree on that. It is imperative for employers toimplement protective measures and to be subject to legal challenge if they fail to doso, following the various national and international legal regulations (see Appendix I).I).
In the interests of both patient and clinic…
Economic and practical factors also speak in favour of the implementation of protectivemeasures to counteract laser plumes. Smoke and stench limit the effectiveness of theoperating team and cause additional absences on account of sickness. In addition, thesmoke obscures the surgeon‘s view of the surgical site, something that can in no waybe justified towards the patient!
However, in medical circles the rule of thumb is that successful treatment is consideredmore important than the avoidance or minimisation of toxic emissions, although thisdoes not apply to the risk of infection!
Local smoke evacuation is indispensable
The primary measure is to ensure that laser use generates a minimum of toxic emissions.However, in medical circles successful treatment is the top priority, so that measuressuch as a recommended increase in oxygen supply during laser use or sprayingwith water can only be implemented to a limited extent.The most important secondary measure, by some way, is the evacuation of the laserplume directly at source. General room suction is secondary to this. Since conditionsfor regulating air circulation in doctors‘ practices are not the same as those in an operatingtheatre, smoke evacuation here must be carried out with special care.Airborne substances with a high initial velocity, such as those that occur during the treatmentof hard tissue (bones) with laser pulses, are particularly hard to capture.For local suction (or local exhaust ventilation - LEV) there are principally two possibilities:either centrally installed or portable suction systems. If central exhaust ventilationsystems are not available, portable systems, available commercially in a variety ofdesigns, must be used.

MedizinTechnik
13
Protective measures
Evacuate as close to the source as possible!
The most important factor for successful smoke evacuation, by unanimous agreement,is the way in which the suction nozzle is positioned and directed and how close thesuction tip is placed to the smoke source: a maximum of 6 cm. When a mobile laserbeam is being used, the suction funnel must be moved with it.
Successful smoke evacuation depends not only on the velocity of local air flows in theroom, but on the flow volume of the suction system in particular. It has to be strongenough to redirect the laser plume. Since other parameters such as the length of thesuction hose and the filtering have an impact on suction pressure, it is sensible to haveelectronic regulation.
Surgery using a smoke evacuation device
distance 6 cm
14
Protective measures
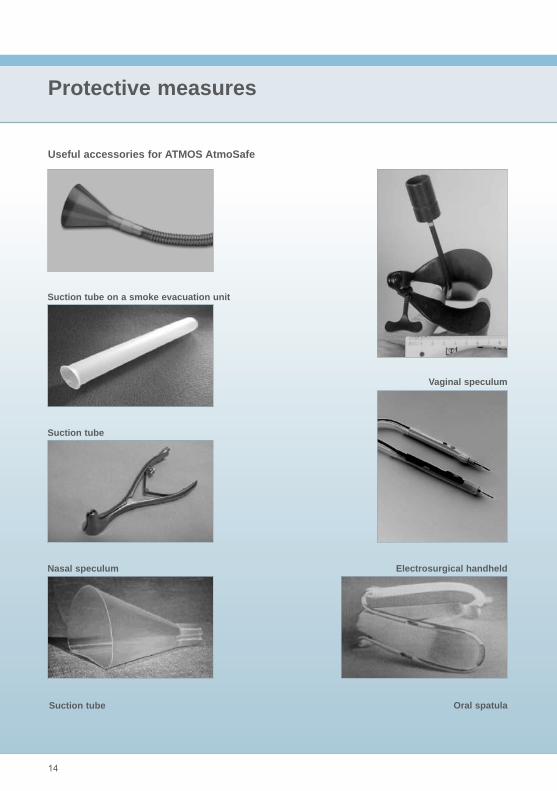
Useful accessories for ATMOS AtmoSafe
Suction tube on a smoke evacuation unit
Electrosurgical handheld
Suction tube
Vaginal speculum
Nasal speculum
Oral spatulaSuction tube
MedizinTechnik
15
Protective measures
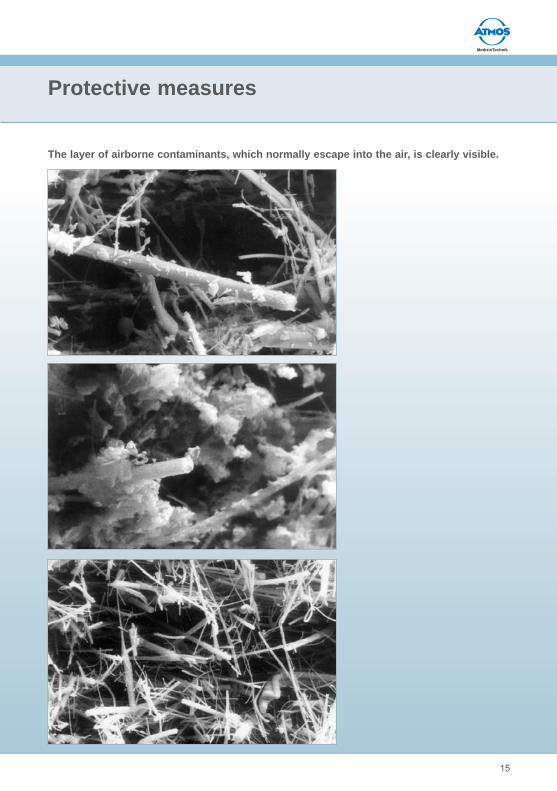
The layer of airborne contaminants, which normally escape into the air, is clearly visible.
16
Protective measures
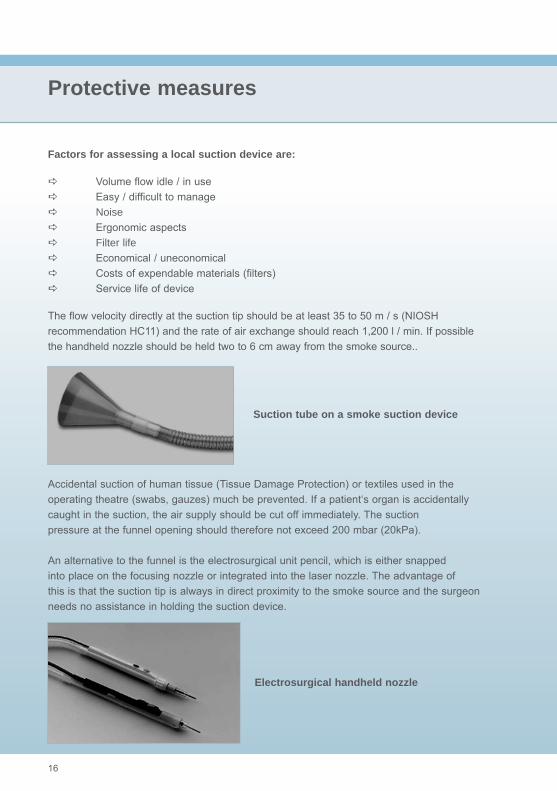
Factors for assessing a local suction device are:
Volume flow idle / in use Easy / difficult to manage Noise Ergonomic aspects Filter life Economical / uneconomical Costs of expendable materials (filters) Service life of device
The flow velocity directly at the suction tip should be at least 35 to 50 m / s (NIOSHrecommendation HC11) and the rate of air exchange should reach 1,200 l / min. If possiblethe handheld nozzle should be held two to 6 cm away from the smoke source..
Accidental suction of human tissue (Tissue Damage Protection) or textiles used in theoperating theatre (swabs, gauzes) much be prevented. If a patient‘s organ is accidentallycaught in the suction, the air supply should be cut off immediately. The suctionpressure at the funnel opening should therefore not exceed 200 mbar (20kPa).
An alternative to the funnel is the electrosurgical unit pencil, which is either snappedinto place on the focusing nozzle or integrated into the laser nozzle. The advantage ofthis is that the suction tip is always in direct proximity to the smoke source and the surgeonneeds no assistance in holding the suction device.
Suction tube on a smoke suction device
Electrosurgical handheld nozzle
MedizinTechnik
17
Protective measures
The surgeon always needs a clear view of the operating field!
The shape of the suction funnel should be optimised in terms of not obscuring visibility and of carrying out effective suction. The material from which the funnel is made must not reflect the laser beam and must be inflammable. The suction hose should have the largest possible lumen leading to the handheld nozzle, otherwise suction will be greatly reduced or the turbine will be unnecessarily noisy unless well soundproofed. Electronic regulation of the suction pressure is recommended. Indeed during endoscopic suction it is indispensable in order not to endangerthe patient by having too much or too little pressure in the body cavity. When cleaning the suction hoses and changing the filters, skin contact must be completely avoided: inside there is a multi-constituent mixture of extremely volatile polyaromatic and heterocyclical hydrocarbons.
Noise from the motor and the suction tip should not exceed 60 dB (A) at full load. The device must always fulfil the increased EMC criteria regarding high frequency emissions in the operating theatre.
Clear view during surgery
18
Assessment criteria for suction devices
Used filters count as infectious waste
Filtering occurs in cascades: each stage removes particular components. The prefiltercatches larger particles and droplets. It consists mostly of microfibres, whose chaoticarrangement creates an effective pore size of over 0.5 μm.
The high performance multi-level fine filter has three qualities, defined by the AmericanIES (Institute for Environmental Services) as:
HEPA-filters (High Efficiency Particulate Air), which, when tested have an efficiency level of 99.97 % at 0.3 μm particles of DOP (dioctylphthalate).
ULPA-filters (Ultra Low Penetration Air) reach 99.999 % at 0.12 μm DOP.
VLSI-grade ULPA-filters (often abbreviated to VLSI filters) reach 99.9999 % at 0.12 μm latex particles.
The final level usually consists of an active carbon filter, which binds the odour and other gas components in the laser plume. The degree of efficiency of an active carbon filter depends not only on its binding capacity, measured by the adsorption of tetrachlorohydrocarbon per unit of weight, but above all on the tissue dwell time. A high through flow speed reduces the effec-tiveness of the filter. This is why the suction performance should not be set higher than is neces-sary. On the other hand the top priority is the maximum capture of the laser plume, as the discar-ded air is already being distributed diffusely.
Filter unit of a local suction device
MedizinTechnik
19
Assessment criteria for suction devices
The odour test is key
Since the build - up of odour is a sensitive indicator of filter failure through wear, excessive suction or insufficient smoke capture, nothing should be introduced into the operating theatre to improve the air. A pressure monitor on the filters should keep a check on their protective function.
Used filters must be treated as infected waste and disposed of. The lifetime of a set of filters should be at least one shift: along with the costs of replacement filters they are a crucial factor in the assessment whether or not a suction system is economical.
The simplest device for testing whether or not suction has been successful is the nose of a person who has just entered the operating theatre and has therefore not had a chance to get used to the odour! However, only foul-smelling pyrazines can be recognised that way, not toxic gas constituents.
Face masks do not offer respiratory protection!
Alongside the obligatory gloves, a protective pair of glasses that fit the face as required in VBG 93 also provide adequate eye protection from tissue splatter. Most important is a respiratory mask, as the surgical face mask is not a breathing filter!
The conventional surgical face mask, introduced in 1897 by Mikulicz to protect wounds from germs carried on the breath, protects staff from particles larger than 50 μm, which are unable to fly around corners for aerodynamic reasons. Since the infection situation in operating theatres is always uncertain, a smoke evacuation system must be standard. If there is a risk of infection, staff standing directly at the operating table must wear a fitted half face filtration mask or a full face mask. However, it does not provide the same filter quality as a suction system.
Surgical face mask

20
Breathable contaminants are generated not only during laser and electrosurgical procedures,but also in pathology departments where bones are sawed or in orthopaedicswhen glues and cements are mixed.
These solid, liquid and gas contaminants are flung out into the air at very high speeds.A suction system must be strong enough to redirect and capture this stream of vapourand particles as comprehensively as possible. The turbine rolls at up to 1250 l / min μm.
This occurs according to the vacuum cleaner principle: a strong, but quiet turbinegenerates a negative pressure. This negative pressure sucks in air at the end of thehose via a filter-hose system. The airflow of AtmoSafe is 1250 l / min in turbo mode and650 l / min in smooth regular operation. In spite of this high airflow the noise level generatedby AtmoSafe is less than 52 dB and is thus quieter than a normal conversation(55dB). The lifetime of the turbine, which is completely maintenance-free, is more than20,000 running hours.
The turbine‘s internal synchronised activation (ISA) starts it up at the same time as thelaser or electrosurgical system. The follow-up control ensures that smoke continues tobe evacuated even after cutting has ceased. There is permanent background suctionto keep the AtmoSafe filters dry at all times. An automatic cut-off switch interrupts thesuction action if a blockage occurs.s
Assessment criteria for suction devices
Construction of the AtmoSafe
Filter contact boardelectrical boardglass filterscarbon packet
particle filters (ULPA)
air hose
prefilters (HEPA)
suction tube
display and operation
electronics
turbine
outlet

MedizinTechnik
21
Filter lifetime: more than 35 hours
The filter system is the centrepiece of AtmoSafe. It consists of two parts: a prefilter on the suction nozzle and a main filter inside the AtmoSafe.
The prefilter is a so-called HEPA filter (High Efficiency Particulate Air), which catches the large solid and liquid constituents. ATMOS uses an HEPA filter that holds back particles from 0.3 μ with an efficiency rate of 99.97 %.
The main filter consists of several levels (cascades): the ULPA filter, three active carbon filter layers and a gas filter, which are housed together in an easily replaceable plastic casing. An electronic diagnostic unit in this filter cartridge measures the air flow of the filter and determines its lifetime, which is generally more than 35 hours. The ULPA filter (Ultra Low Penetration Air) filters small and tiny particles up to the size of viruses. An antibacterial coating on this filter prevents micro-organisms from getting through. The ULPA filter has a 99.9999 % efficiency rate in relation to particles from 10 nm.
The triple-layered active carbon filter behind this binds the odour substances. Finally, AtmoSafe‘s special gas filter retains ammonia and hydrocyanic acid specifically.
AtmoSafe is very economical
The filter cartridge can be changed very easily - no tools are needed - and currently costs 123.- Euro. An analysis of the total cost of AtmoSafe over its lifetime - about10,225.- Euro over 10 years - yields a cost per use of only 0.89 Euro.This includes four new suction hoses, six filter cartridges and 1,300 uses per year.Surely this is not too high a price to pay for fresh air and unencumbered working in theoperating theatre!
Assessment criteria for suction devices
AtmoSafe from ATMOS

22
Appendix I
Regulations and ordinances
The German legal limits for contaminants in breathing air are MAK (maximum occupationalconcentration, as defined by the senate commission of the German ResearchSociety for dangerous occupational substances), TRK (technical recommended concentrationin accordance with the technical rules for dangerous substances (TRGS)900) and BAT (biological occupational tolerance levels in accordance with TRGS 903).For many substances, these limits do not exist or else they are only applicable in limitedcases or for combinations of substances that are only occasionally present in breathingair and are insignificant in terms of a temporal mean.
In so far as the literature reveals cases in which these limits have clearly been exceeded,these are related to the floating dust element, designated internationally as ULPA(ultra low penetration air).
However, an adequate legal basis for ensuring worker protection and an employer‘sduty to inform workers of the dangers of any given procedure emerges from the followingregulations:
Ordinance on dangerous substances of 15th November 1999 (BGBI. I S. 2233)
§ 19 Order of importance of protective measures
(1) Working procedures should be organised in such a way to prevent release of dangerous gases, vapours or suspended particles, as far as current technology allows. Further, working procedures should be organised in such a way that employees do not come into skin contact with dangerous substances or preparations, solid or liquid, as far as current technology allows.
(2) If the measures stipulated in section 1 above are unable to prevent the release of dangerous gases, vapours or suspended particles, these must be contained completely at source and disposed of subsequently so that they pose no risk to humans or the environment, as far as current technology allows.
(3) If complete containment as stipulated in section 2 is not possible, then appropriate ventilation measures should be implemented in accordance with the current state of technology.
MedizinTechnik
23
Appendix I
Accident prevention regulation VBG 1:
§ 2 General requirements(1) The employer should put in place facilities, arrangements and measures that meet the regulations of this accident prevention regulation and other relevant accident prevention regulations as well as generally recognised safety and medical rules.
Accident prevention regulation VBG 93:
§ 10 Section 2
(2) The employer should ensure that safety measures are put in place wherever the use of laser beams may lead to endangerment of health through gases, vapours, dust, fog, explosive mixtures or secondary irradiation.
Technical Regeln für Biologische Arbeitsstoffe (Technical rules for biologicalsubstances at work) TRBA 500 of 01.05.1999, BArbBI No. 6/99 p. 81
A laser plume consisting of human tissue is a bioaerosol in accordance with TRBA 500.
Protective measures II: General remarks
(1) To counteract potential risk, the employer should implement all necessary technical and organisational measures. In addition, the use of personal protective equipment may be necessary.
(2) The employer should also make certain that all necessary general hygiene measures can be implemented. The employer is under obligation to instruct employees, regularly and in a manner and language comprehensible to them, about potential risks to health, adherence to protective measures and the wearing of personal protective equipment.

24
Appendix I
Ordinance on bio-substances of January 1999
All employees are to be informed of potential risks and protective measures.Laser plumes containing human tissue are to be allocated to Risk group 2.
EU bio-substance guideline 2000 / 54 / EG
Concerning protection of employees against risks from occupational biologicalsubstances. Laser plumes containing human tissue are to be allocated to Risk group 2.
US ANSI standard Z 136.3, 1996
ANSI:American National Standards InstituteThe standard provides guidance for safe use of lasers and laser systems for diagnosticand therapeutic uses in health care facilities. The standard takes into consideration theunique problems relation to operating rooms, outpatient clinics, and private medical offices.
US OSHA
(Occupational Safety and Health Act)
NIOSH: National Institute for Occupational Safety and Health(www.osha-slc.gov/SLTC/laserelectrosurgeryplume)
General Duty Clause: 29 U.S.C.A. Section 654:
„Each employere shall furnish to each of his employees employment and a place ofemployment which are free from recognized hazards that are causing or are likely tocause death or serious physical harm to his employees.“
American Society for Laser Medicine and Surgery (ASLMS)
Report of the Laser Safety Committee on Hazards of Vaporized Tissue Plume(www.aslms.org/general-smokeguns1.htm):
Smoking Guns, Part II: Recommendations
The Laser Safety Committee has reported on the hazards of vaporized tissue plume.The recommendations are as follows:
I. All medical personnel should consider the vaporized tissue plume to be potentiallyhazardous both in terms of the particulate matter and infectivity.
MedizinTechnik
25
Appendix I
II. Evacuator suction systems should be used at all times to collect the plume. a) The suction should have a high flow volume with frequent filter changes being made to optimize suction and filter capabilities. b) Filters should be chosen which allow for maximum filtering efficiency. c) The suction tip must be placed as close to laser impact as possible. d) Evacuator suction tips should be cleaned (preferably sterilized) after each procedure.
III. Eye protection, masks, gloves, and appropriate clothing should always be worn during laser use by all laser personnel when vaporized tissue plume is generated. a) Eye protection should be of a nature which would protect from splatter. b) Masks should have good effective filtration. c) Gloves should be preferably latex (or an effective substitute in the case of latex sensitivity).
DHHS/CDC/ NIOSH Recommendation HC 11
US Department of Health and Human Services
Centers for Disease Control and Prevention
National Institute for Occupational Safety and Health
DHHS (NIOSH) Publication 96-128 (www.cdc.gov/niosh/hc11.html)
Control of Smoke from Laser / Electric Surgical Procedures
“During surgical procedures using a laser or electrosurgical unit, the thermal destructionof tissue creates a smoke byproduct. Research studies have confirmed that thissmoke plume can contain toxic gases and vapors such as benzene, hydrogen cyanide,and formaldehyde, bioaerosols, dead and live cellular material (including blood fragments),and viruses. At high concentrations the smoke causes ocular and respiratorytract irritation in health care personnel, and creates visual problems for the surgeon.The smoke has unpleasant odors and has been shown to have mutagenic potential”.
NIOSH research has shown airborne contaminants generated by these surgical devicescan be effectively controlled. Two methods of control are recommended:

26
Appendix I
VENTILATION:
Recommended ventilation techniques include a combination of general room and localexhaust ventilation (LEV). General room ventilation is not by itself sufficient to capturecontaminants generated at the source. The two major LEV approaches used to reducesurgical smoke levels for health care personnel are portable smoke evacuators androom suction systems.
Smoke evacuators contain a suction unit (vacuum pump), filter, hose, and an inletnozzle. The smoke evacuator should have high efficiency in airborne particle reductionand should be used in accordance with the manufacturer‘s recommendations to achievemaximum efficiency. A capture velocity of about 100 to 150 feet per minute at the inlet nozzle is generally recommended. It is also important to choose a filter that is effective in collecting the contaminants. A High Efficiency Particulate Air (HEPA) filter or equivalent is recommended for trapping particulates. Various filtering and cleaning processes also exist which remove or inactivate airborne gases and vapors. The various filters and absorbers used in smoke evacuators require monitoring and replacement on a regular basis and are considered a possible biohazard requiring proper disposal.
Room suction systems can pull at a much lower rate and were designed primarily tocapture liquids rather than particulates or gases. If these systems are used to capturegenerated smoke, users must install appropriate filters in the line, insure that the line iscleared, and that filters are disposed properly. Generally speaking, the use of smokeevacuators are [sic] more effective than room suction systems to control the generatedsmoke from nonendoscopic laser / electrical surgical procedures.
WORK PRACTICES
The smoke evacuator or room suction hose nozzle inlet must be kept within 2 inchesof the surgical site to effectively capture airborne contaminants generated by these surgicaldevices. The smoke evacuator should be ON (activated) at all times when airborneparticles are produced during all surgical or other procedures. At the completion ofthe procedure all tubing, filters and absorbers must be considered infectious waste andbe disposed appropriately. New filters and tubing should be installed on the smokeevacuator for each procedure. While there are many commercially available smokeevacuator systems to select from, all of these LEV systems must be regularly inspectedas “universal precautions”, as required by the OSHA Blood-Borne Pathogen standard.“
MedizinTechnik
27
Appendix II
References
Probably the most comprehensive European study on the risks posed by laser plumesis the STILMED study (Safety Technology in Laser Medicine) produced by the Eurekacollaborative project EU - 642 (conducted 1991-1995), whose results are available inbook form: “Bewertung von Abbrandprodukten bei der medizinischen Laseranwendung” (Analysis of smoke byproducts generated by medical use of lasers), published by the VDI-Technologiezentrum für Physikalische Technologien (VDI Technology Centre for Physical Technologies) Berlin, 1997, ISBN 3-00-002352-6.
Collaborative partners in the STILMED project were:
Dr. H Albrecht; Laser- und Medizin-Technologie GmbH Berlin (LMTB)
Dr. T. Meier, Institut für Lasertechnologien in der Medizin und Messtechnik (ILM)(Institute for Laser Technologies in Medicine and Metrology)
Dr. L. Weber, Institut f. Arbeits- und Sozialmedizin der Universität Ulm (Institute forOccupational and Social Medicine at the University of Ulm)
Dr. W. Wöllmer, University Hamburg, UK Eppendorf, Universitäts-HNO-Klinik(University ENT Clinic)
PD Dr. J. Lademann, Dr. H-J. Weigmann, Humboldt University at Berlin,Universitätsklinikum Charité (Charité University Clinic), Dermatologische Klinik(Dermatalogy Clinic)
The aim of this study was to analyse both pyrolytic gaseous products as well as particles.Different chemical and biochemical analytic systems were used for chemical characterisation.Before the analysis could be carried out it was necessary to develop standardised sampling systems for study in vitro or in vivo. The project made use of both animal and human tissue, but also different cell cultures.In addition the basic components of laser pyrolysis (lipids, proteins, DNA) were broken down for purposes of orientation. Using guide components, that is, selected organic compounds, the aim was to make quantitative statements regarding the generation of gaseous pyrolytic components.

28
Anlagen II
The impact of factors such as tissue type, laser type and laser parameters, parameters of the application technology and experience of the therapist on the generated contaminants was recorded in a series of exhaustive experiments. For example, it was possible to reduce the amount of toxic gaseous compounds generated by choosing appropriate laser parameters. The study of physical characteristics of aerosol particles in terms of particle size, particle velocity and spread behaviour in the room, but also particle morphology, for example, in relation to tissue and the development of relevant modelling systems served amongst other things as a basis for intro-ducing protective measures. Alongside the chemical characterisation of bioaerosols, polymerase chain reaction (PCT) was used in the context of different biological and toxicological assaysto achieve clarification regarding the infectivity of the particulate phase. The data concerning generated contaminant mixtures and particle spectrums form the basis of an occupational medical analysis of risk potential for the laser user (doctor, operating staff) and the patient. The results have been used in the context of recommendations to the laser user, therapeutic guidelines, initial standards for lasers and suction devices and as specifications for optimum suction and filter technology.
Other finds from the specialist literature of the last 15 years include:
Hallmo and Naess (1991) report a laser surgeon who had laryngeal papillomatosis of the same virus strain found in anogenital condylomas previously extirpated from him.(Eur Arch Otorhinolaryngol 1991; 248 (7): 425 - 7)HPV was also found in a CO2 laser plume, but no transferral was observed.(J Reprod Med 1990 Dec; 35 (12): 1117 - 23)
By contrast a study using an erbium-YAG laser for wart ablation yielded no observable HPV in precipitation from the suction nozzle.(J Am Acad Dermatol 1998 Mar: 38 (3): 426 - 8)
Modelling experiments using bacteriophages revealed condensates of active materialin the direct proximity of the laser site. (Lasers Surg Med 1989; 9 (3): 296 - 9)
Rats that inhaled the laser plume developed interstitial pneumonias, bronchitis andemphysemas. (Am J Obstes Gynecol 1987 May;156 (5): 1260 - 5)
Fibroblasts infected with the polio virus were ablated using an excimer pulse laser.Active virus material was found in the rinsing matter from the suction tube.(Opthalmology 1999 Aug;106 (8): 1498 - 9)
MedizinTechnik
29
Anlagen II
In cultures consisting of matter rinsed out of the HEPA filter of a CO2 laser suctiondevice, no viral material was found, but instead coagulase-negative staphylococci,corynebacterium and neisseria. (Lasers Surg Med 1998: 23 (3): 172 - 4)
An attempt to transfer pseudorabies from tissue ablated with an excimer laser to apetrie dish right next to it was unsuccessful.(Am J Ophthalmol 1997 Aug: 124 (2): 206 -11)
Laryngeal papilloma viruses could not be transferred to cell cultures from smoke duringremoval with a CO2 continuous wave laser.(J Laryngol Otol 1996 Nov; 110 (11): 1031 - 3)
The smoke from electrocauterizers is considered twice as harmful as that from lasers.(Todays Surg Nurse 1999 Mar-Apr;21 (2): 15 - 21; quiz 38 - 9)
Attenuated varicella-zoster virus does not seem to survive excimer ablation.(Arch Ophthalmol 1997 Aug; 115 (8): 1028 - 30)
SIV does not survive CO2 ablation. (J Dermatol Surg Oncol 1992 Apr; 18 (4): 297-300)HPV-DNA was observed in the smoke from CO2 lasers.Otolaryngol Head Neck Surg 1991 Feb; 104 (2): 191 - 5)
A group study of normal and CO 2 laser surgeons revealed that there was no higherincidence of warts among the latter. However, reference is made to the risk of HPVinfection of the upper respiratory tract.(J Am Acad Dermatol 1995 Mar;32 (3): 436 -41)
30
Glossary
μm micrometre, 1/1000mmabsorption a gas dissolving (being evenly distributed) in a liquid or solid bodyacrolein carcinogenic organic compoundaerosol disperse system consisting of a liquid and a solid phase, which is suspended in a gaseous mediumAIDS immune deficiency syndrome triggered by the retrovirus HIVactive carbon filter activated filter made of medicinal carbonalkanes chain-shaped hydrocarbons (methane, ethane, propane…)alkyl nitriles carcinogenic organic compoundsalkyl radicals carcinogenic organic compoundsallergenic triggering an allergic immune reactionalveoluses tiny air sacs in the lungs, 100-300 μm diameteralveoli small enough to run to the alveolusesamines derivatives of ammonia; biogenic amines are formed from amino acidsamino acids simplest building blocks of proteinsanaesthesia gases gases which are used at narcosisaromatic having a ring-shaped chemical structureaetiologically originallybenzene carcinogenic organic compoundbio-aerosol aerosol that is biological in origin or effectbronchioles very small bronchial tubeschaotic not arrangedchromophore colouranthydrogen cyanide highly toxic gas, HCN, „cyclone B“continuous wave laser laser with continuous wave emissiondB(A) measurement of sound levelsdenaturation l oss of original structuredispersion a system in which one substance is finely dispersed in another substance, namely the dispersantDKP diketopiperazinesDNA deoxyribonucleic acid, hereditary materialelectro-cauterizer device used in thermic coagulation of tissueEMV electromagnetic compatibility; describes the disruptive Influence of and by (an) other device(s) by radio beamsergonomics denotes the degree of ease of the human-machine interfaceEscherichia. coli bacteria found in the gut

MedizinTechnik
31
Glossary
ESU electrosurgical unit (high frequency surgical device)excimer pulse particular type of laserCFCs chlorofluorohydrocarbons, „ozone depleters“fat oxidation fat burningformaldehyde disinfectant, emits harmful vapourshalogen umbrella term for fluorine, chlorine, bromine, and iodinehydro-halogenic acids highly aggressive halogen acidsHEPA filter High Efficiency Particulate Air filter; highly effective air filter, actually developed by the military to filter tiny radioactive suspended particles. The ULPA filter is even more effective.Hepatitis B highly infectious viral inflammation of the liver, immunisableHepatitis C highly infectious retroviral inflammation of the liver, nonimmunisableheterocyclical consisting of different circular structureshigh frequency device electro surgery using high frequency surgical instruments, which have surgerya cutting and coagulation mode, giving the instrument a styptic effectHIV the retrovirus that gives rise to AIDSinfectious contageousinfectivity denotes the degree of contagiousness of a pathogencarbonisation generation of a black, soot-like layer of carbon, e.g. on organic tissue through turning all volatile constituents into carbon and degasifying them. The non-volatile carbon sub stance remains behind and is visible as a black coating.carcinogenic cancer-causingcascades groups placed one behind anothercoagulation denaturation of proteins through irreversibly dissolving their molecular formation (tertiary structure) on account of heat (>56ºC), a change in pH value or other solubilising influencescarbohydrate compounds consisting of C, O and Hlaparoscopy abdominal investigationlaryngeal affecting the larynxlaser intensification of light by stimulating emissions; extremely coherent beam of light with extremely high energy laser plume due to the composition of the volatile smoke by-products from laser surgery (water vapour, gases, liquid and solid constituents) the term ‚smoke‘ or ‚vapour‘ is not quite correct. Hence the use of ‚plume‘.laser surgery use of a laser as a surgical instrumentliver parenchyma sponge-like liver tissueLEV local exhaust ventilation
32
Glossary
LGAC laser generated airborne contaminantslipids fatsmacromolecules large organic groups of moleculesmbar old measurement of pressure, nowadays given in Pascalsmelanin brown colourant (pigment)melanisation the process of turning brownmicroorganisms bacteria, viruses, funghi etc.Mikulicz inventor of surgical face masksminimally through invasive operating procedure: endoscopic penetration into the body small openingsmucociliary cleaning self-cleaning of the lungsmutagenic capable of altering hereditary materialMycobact. tuberculosis tuberculosis pathogenNIOSH National Institute for Occupational Safety and Healtholigo-saccharide collective name for certain carbohydratesorganic belonging to the realm of carbon compoundsPAH polycyclical aromatic hydrocarbonspapilloma viruses viruses that cause condylomasPascal unit of measurement of pressureparticle smallest particle in the solid or liquid dispersal phasepathogen disease-causingpeptides compounds consisting of amino acidsphotoablation explosive removal of tissue matter by using very low heat on the surrounding tissue. Thermic damage can be kept very minimal, sometimes as low as the thickness of a cell layer (< 10 mm). Often excimer pulse lasers with a high fluence are used as ablation lasers. (Ablation lasers: excimer lasers for microsurgery; Er:YAG lasers for dermatology). Emissions from this procedure are particularly high, especially in dermatology.polysaccharides high molecular carbohydratespolycyclical containing several circular structuresporphyrine biologically important colourantpulse laser laser with (lightning-like) pulsed laser; opposite: continuous wave laserpyrazine gases that have a strong smellpyrolysis incomplete oxidative thermic disintegration (sometimes burning) of organic substances such as body tissue. The chemical transformation of the heated tissue generally occurs by breaking up chemical bonds.radical chemical group that reacts easilyretroviruses viruses with RNA instead of DNA

MedizinTechnik
33
Glossary
Staph. aureus pathogenic domestic germtetrachlorocarbon toxic solution, part of the CFC grouptoxic poisonousULPA filter Ultra Low Particulate Air filter = currently the most effective filter in the world (has a retention rate of 99.9999 %@ 0.12μm); better quality than a HEPA filter.vaporisation causing tissue (>100ºC) to change a gaseous state by adsorbing high thermic values produced by ESU, lasers etc.viral caused by virusesVLSI-grade v ery strongly characterised, especially effectiveVOC volatile organic compounds; e.g. strong smelling gases such as pyrazines and butanes
ATMOS –worldwide your reliable and competent partnerfor medical engineering!
In more than 100 years ATMOS MedizinTechnik
has grown to a company which combines long
time experience and future-orientated technology
in four business ranges.
We are represented in over 70 countries
worldwide 12 subsidiaries) having more than 250
employees.
Our Headquarter Lenzkirch / Black Forest!
ATMOS MedizinTechnik GmbH & Co. KG Ludwig-Kegel-Str. 16 | 79853 Lenzkirch | Tel: +49 7653 689-0 | [email protected] | www.atmosmed.com
ENT GynaecologySurgery Care
2010-05 Index: 01