all wales integrated care priorities for the last days of ... ldol icp sept 2012 community.pdf ·...
TRANSCRIPT

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p1/17)
All Wales Integrated Care Priorities
for the Last Days of Life (ICP)
This multi-disciplinary document is part of the confidential clinical record. The ICP Document is only a guide to care for the patient and their family in the last days of life. This ICP is based on best accepted practice. Each professional should exercise their professional judgment when using this guidance. Medical & Nursing Assessments should be completed when care is guided by ICP Risk assessments (pressure area, personal care etc.) continue as before Ongoing review (nursing) should be completed 4 hourly or at each visit, using a new sheet daily. Variance occurs if an unexpected event occurs. Any variance should be recorded on the variance
sheet, If a box in italics is ticked, explain action/inaction on variance sheet N.B. A variance is not wrong, but it is important to record it, to help with quality and audit.
Multi-disciplinary progress notes allow scope to record anything not covered by the ICP. These notes should record communication with the patient and family.
This document replaces the medical and nursing notes during this period of care. The ICP should only be used when the following three criteria have ALL been fulfilled: • Reversible causes of deterioration have been excluded • The patient and /or family are aware that the patient is in the last days of life • The clinical team agree that the ICP is appropriate
CONTACT DETAILS
Out of hours GP: 0300 123 50 60

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p2/17)
Medical Assessment DIAGNOSIS
Criteria for ICP Do Not use the ICP for the last days of life unless all three criteria are fulfilled 1 Have reversible causes of deterioration been excluded? Yes ���� No ���� 2 Does the team agree that the patient is dying Yes ���� No ���� 3 The patient or family are aware that the patient is dying Yes ���� No ���� If an in-patient has GP been informed of situation? Yes � No �
Has the patient / family expressed wishes around tissue donation? Yes � No � If yes phone: (for South Wales) 07659 591889
GOAL 1 ���� PRIORITIES OF CARE
The patient’s priorities have been assessed Yes � No � Please document the patient’s priorities: GOAL 2 ���� CURRENT MEDICATION ASSESSED AND NON ESSENTIALS DISCONTINUED Appropriate oral drugs converted to subcutaneous route via syringe driver (if required) Yes � No �
GOAL 3 ���� HYDRATION In some patients or following discussion with relatives it may be appropriate to use s/c fluids Are patient/families and H/C professionals agreed over plan for fluids Yes � No � GOAL 4 ���� PRN WRITTEN UP (AS LIST BELOW) – REFER TO GUIDELINES Pain - e.g. Diamorphine Yes � No � N&V - e.g. Cyclizine Yes � No � Agitation - e.g. Midazolam Yes � No � Respiratory Tract Secretions - e.g. Hyoscine Hydrobromide Yes � No � GOAL 5 ���� DISCONTINUE INAPPROPRIATE INTERVENTIONS Blood Tests Yes � No � Not applicable � Treatments that are failing to achieve therapeutic goal Yes � No � Implantable Cardiac Defibrillator deactivated Yes � No � Not applicable �
GOAL 6 ���� OTHER REQUIREMENTS DNACPR written in Medical notes/form completed Yes � No � DNACPR discussed with relatives Yes � No � Not applicable � If appropriate to involve the Coroner, discussed with relatives Yes � No � Not applicable � Doctor’s Signature __________________________ Date ______________________ Print Name _____________________________________
Name: Date of Birth: Address: NHS Number:
Date………………………
S-1

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p3/17)
Nursing Assessment GOAL 7 ���� COMFORT MEASURES (Consider the environment: comfort, safety, temperature, ventilation). Recording of vital signs discontinued Yes � No � Pressure areas assessed Yes � No � Assessed need for - special mattress Yes � No � - single room Yes � No � Not Applicable � Assessed condition of mouth Yes � No � Assessed elimination difficulties Yes � No �
Action taken on any of above assessments: GOAL 8 ���� COMMUNICATION Preferred language: Barriers to communication: GOAL 9 ���� IDENTIFY AND ADDRESS PATIENT’S FEARS AND ANXIETIES
Patient recognises that they are dying Yes � No � Don’t Know � Fears identified (specify): GOAL 10 ���� MOBILITY/SAFETY Manual Handling Assessment reviewed and appropriate aids obtained Yes � No � GOAL 11 ���� HAZARDS IDENTIFIED Infection/ radiation control referral if appropriate Yes � No � Not Applicable � GOAL 12 ���� SPIRITUAL/RELIGIOUS/CULTURAL REQUIREMENTS
Religious/cultural needs identified & action taken: Yes � No � Not Applicable � Religion identified (please specify): ……………………………………………………………................... If appropriate – contact made with relevant minister? Yes � No � Not Applicable � Contact name: Tel. no
Name: Date of Birth: Address: NHS Number:
Date………………………
S-2.1

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p4/17)
GOAL 13 ���� BEREAVEMENT PLANNING/FAMILY CARE Family recognise that patient is dying Yes � No � Don’t Know � Care discussed with relative and recorded on MDT sheet Yes � No � Anxieties or Fears identified, please state: GOAL 14 ���� DETAILS OF HOW TO INFORM FAMILY/ OTHERS OF IMPENDING DEATH At anytime � Not at night � Contact name: Relationship to patient: Telephone No: Second contact name and number: GOAL 15 ���� FAMILY GIVEN LOCAL INFORMATION Family shown local facilities Yes � No � Not Applicable � - over-night stay, availability of food and drinks, location of phones, washing facilities, parking arrangements etc. Family needs (please state): ……………………………………………………………
Nurse’s signature ___________________________ Date _______________ Print Name _______________________________________________
Name: Date of Birth: Address: NHS Number:
Date………………………
S-2.2

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p5/17)
Regular Symptom Assessment & Review CODES (to enter in columns) A – goal achieved, V – goal not achieved record on variance sheet, N/A – not applicable
DATE & TIME��
�������������������������������������������
GOAL 16 ����PAIN
GOAL 17 ���� AGITATION
GOAL 18 ���� “RATTLING” SECRETIONS
GOAL 19 ���� NAUSEA / VOMITING
GOAL 20 ���� MOUTH CARE Mouth care carried out & mouth is clean.
GOAL 21 ���� MEDICATION Medications reviewed & delivered safely.
GOAL 22 ���� INTERVENTIONS Inappropriate interventions discontinued.
GOAL 23 ���� COMMUNICATION – PATIENT Patient aware of situation as appropriate.
GOAL 24 ���� COMMUNICATION – FAMILY/ OTHERS Family/others prepared for patient’s death.
GOAL 25 ���� OTHER SYMPTOMS Other distressing symptoms controlled
Symptom Goal � Symptom Goal �
GOAL 26 ���� MEDICAL REVIEW Daily medical review carried out.
Print Name & sign each observation
Name: Date of Birth: Address: NHS Number:
Date………………………
S-3

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p6/17)
CARE AFTER DEATH Death verified within 6 hours Yes � No � (Not relevant for acute sector)R DEATH Death Verification
Date of death ____________________________ Time of death ______________ Signature of verifier _____________________ Date __________ Time ________ Print Name _____________________
Death Certification
Date of death ____________________________ Time of death ______________ Signature of certifier _____________________ Date __________ Time ________ Print Name _____________________
GOAL 27���� FAMILY To prepare, inform and support the patient’s family /others, during final stages and immediately after death
Coroner needs to be informed Yes � No � Not applicable � Post mortem discussed Yes � No � Mortuary viewing explained Yes � No � Not applicable � Collection of belongings / valuables explained Yes � No � Not applicable � Collection of certificate explained Yes � No � Not applicable �
Please tick ���� one option Patient for burial � Patient for cremation � for cremation see below Names of people present at time of death and relationship to the deceased:
GP informed of death by telephone or fax Yes ���� No ���� Date __/__/__ Time ___________ Health Professional Signature _______________________ Date _______________
Print Name ____________________________
Please remember - Copy and forward the variance sheet(s) �
Name: Date of Birth: Address: NHS Number:
Date………………………
S-4

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p7/17)
Multi-disciplinary Progress Notes/Communication Sheet Date � Signature�
Name: Date of Birth: Address: NHS Number:
Date………………………
S-5

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p8/17)
Variance Page
Date Variance and explanation Action Taken Outcome Signature
Please state your locality: Rhondda/Taf Ely � Merthyr / Cynon � GP practice………………………………………………………………
Please indicate setting: Patient’s own home � Nursing Home � Residential Home � Please give name of Home ………………………………………..
Please return a photocopy of variance page/s even if no variances recorded on them to: Clinical Audit & Effectiveness Department (AWCPLDL), Royal Glamorgan Hospital
Name: Date of Birth: Address: NHS Number:
Date started on ICP……………………… Date of Death …………………………….. No of days using ICP ……………………
S-6
Gender … M / F Age …………………………….. Diagnosis ……………………………….…
or Fax to: 01443 443420

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p9/17)
PRN Medication Symptom Medication Dose Frequency Route Doctor’s
Signature
Date
Nausea/ Vomiting
Cyclizine Maximum 150mg/24hrs
50mg 4hrly sc
Agitation Midazolam Usual max 30mg/24hrs If more required, seek advice
5mg 2hrly sc
“Rattle” Hyoscine Hydrobromide Maximum 2.4mg/24hrs
0.4mg 4hrly sc
Pain See Guidelines
Others
PRN MEDICATION GIVEN Date
Time Drug Dose Route Signature
(Given by) Signature (Checked by)
Name: Date of Birth: Address: NHS Number:
Date………………………
S-7

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p10/17)
PRN MEDICATION GIVEN Date
Time Drug Dose Route Signature
(Given by) Signature (Checked by)
Name: Date of Birth: Address: NHS Number:
Date………………………
S-7.2

�
CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p11/17)
�
Regular Prescriptions MORNING (around 0800); MIDDAY (between 1200 & 1400); EVENING (around 1800); BEDTIME (around 2200)
��������� ���� � � � ��� � ������������ ������ ���� ��
��� ������ ��� ����� ����� ����
��� ������ �������
���� � � � � � � � � � � � � �
������ � �
�� ������ � �
����� �� ��
�� �
�������� ����
��� ������������ ��
��
� ��
���������
� ������������������ � � ������� ������� � ��� ��!��" �
��������
������
� � � � � � � � � � � � � � � � � �
� ���#�$� � � � � � � � � � � � � � � � � �
� #���%� � � � � � � � � � � � � � � � � �
����#�$� � � � � � � � � � � � � � � � � �
!��&#� �� � � � � � � � � � � � � � � � � �
� � � � � � � � � � � � � � � � � �
��������� ���� � � � ��� � ������������ ������ ���� ��
��� ������ ��� ����� ����� ����
��� ������ �������
���� � � � � � � � � � � � � �
������ � �
�� ������ � �
����� �� ��
�� �
�������� ����
��� ������������ ��
��
� ��
���������
� ������������������ � � ������� ������� � ��� ��!��" �
��������
������
� � � � � � � � � � � � � � � � � �
� ���#�$� � � � � � � � � � � � � � � � � �
� #���%� � � � � � � � � � � � � � � � � �
����#�$� � � � � � � � � � � � � � � � � �
!��&#� �� � � � � � � � � � � � � � � � � �
� � � � � � � � � � � � � � � � � �
��������� ���� � � � ��� � ������������ ������ ���� ��
��� ������ ��� ����� ����� ����
��� ������ �������
���� � � � � � � � � � � � � �
������ � �
�� ������ � �
����� �� ��
�� �
�������� ����
��� ������������ ��
��
� ��
���������
� ������������������ � � ������� ������� � ��� ��!��" �
��������
������
� � � � � � � � � � � � � � � � � �
� ���#�$� � � � � � � � � � � � � � � � � �
� #���%� � � � � � � � � � � � � � � � � �
����#�$� � � � � � � � � � � � � � � � � �
!��&#� �� � � � � � � � � � � � � � � � � �
� � � � � � � � � � � � � � � � � �
Name: Date of Birth: Hospital No: (Or affix label)
Ward ………………………………… Consultant ………………………….. Date / Time…………………………..
S-8

CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p12/17)
OUT OF HOURS COMMUNICATION SHEET Integrated Care Priorities for The Last Days Of Life
URGENT FOR IMMEDIATE ATTENTION OF DOCTOR
When ICP commenced, please complete and fax this sheet to relevant Out of Hours Service FROM: SIGNATURE:
DESIGNATION: DATE AND TIME:
Please Fax to OOH service: 01443 425770
PATIENT DETAILS Name:
D.O.B
Address: Telephone No:
Next of Kin/Main Carer: Address: Telephone No:
PATIENT’S OWN GP DETAILS Name: Practice Name: Telephone No:
Date of Notification to Out of Hours Service: Do you wish to be contacted concerning care? Yes No
OTHER SERVICES INVOLVED: - Please indicate District Nurses: Marie Curie Nursing Service: Macmillan Specialist Palliative Care Team: DIAGNOSIS AND RELEVANT HISTORY Patient aware of Diagnosis Yes No Relatives aware of Diagnosis Yes No DRUGS PRESCRIBED FOR THIS PATIENT - Please Indicate
Diamorphine YES/NO
Hyoscine YES/NO
Midazolam YES/NO
Cyclizine YES/NO
Water for injection YES/NO
MANAGEMENT PLAN
�
S-9
������
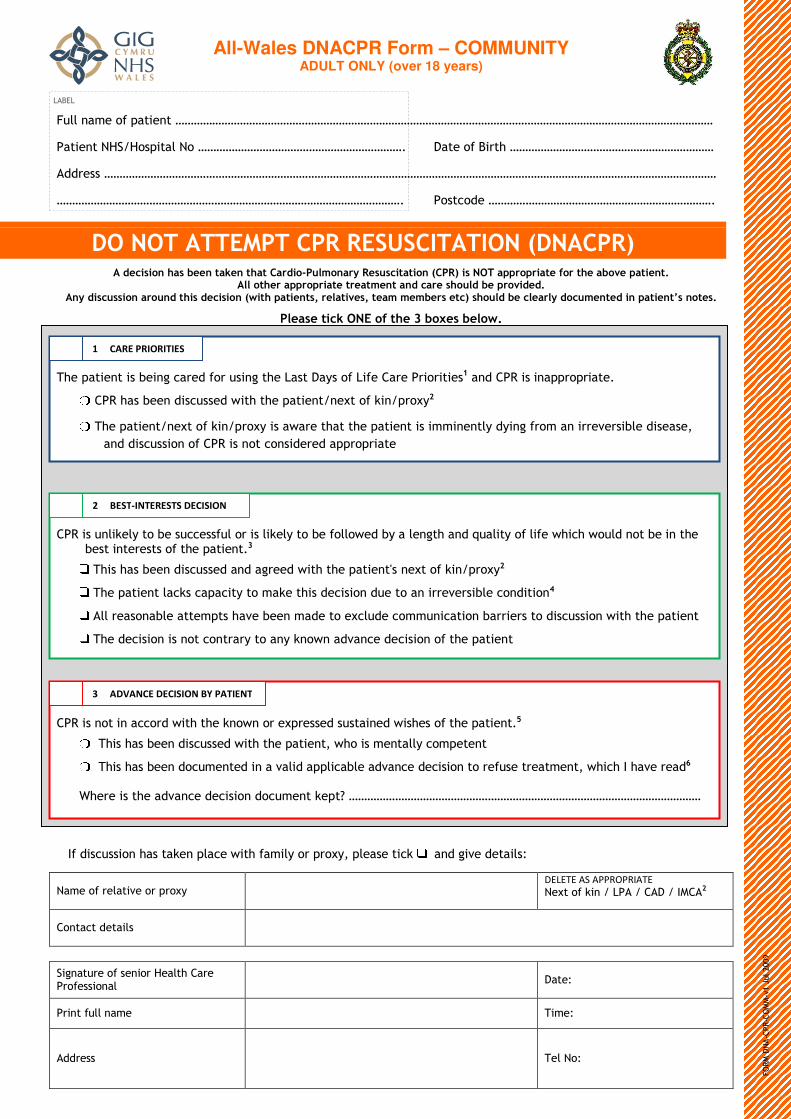
All-Wales DNACPR Form – COMMUNITY ADULT ONLY (over 18 years)
������� ��� ��������������
��
�������� ������������� �
���������!"#! �$��������� %� ���������&�'� �
�((&�$$� �
%� ��$�)�(�� %�
����������������� ���� � ������������ ������������ � ������������� � ����������� ������ ���������� �� ������� ������������ �� ��� � � �������������������������� ��
������������������� ������������! � ��� �� �"����� ����"� ��� �� �� ������ ������������������������� � ������� �� #��� �� �
������� ����� � $���� ��%���&�������! ����*'�����������$�+���,�)�&�(���&��$��,��'����$���-$��������� �&���&��&����$
'���(� ����$������&��&����%�
�� ���'�$�+����(�$)�$$�(�. ��'��'���������#��/�����0��#�&�/-(��
��*'���������#��/�����0��#�&�/-��$��. �&���'����'�����������$��� � ������-�(-��,��&�� �����&&���&$�+���(�$��$�1�
��(�(�$)�$$������� ����$�����)��$�(�&�(����&��&�����
�
�
�
����$�����0��-����+��$�))�$$�����&��$���0��-����+�������. �(�+-������,�'���(�2�����-���������. '�)'�. ���(�����+������'��+�$������&�$�$�����'���������%%�
��*'�$�'�$�+����(�$)�$$�(���(��,&��(�. ��'��'���������3$���/�����0��#�&�/-(�
��*'������������)0$�)���)��-����� �0���'�$�(�)�$����(����������&&���&$�+���)��(�����)�
������&��$���+�������� ��$�'����+����� �(������/)��(��)�� � ���)������+�&&��&$����(�$)�$$����. ��'��'����������
��*'��(�)�$�����$�����)���&�&-������-�0��. ���(���)��(�)�$��������'����������
����
����$���������))�&(�. ��'��'��0��. ���&��/�&�$$�(�$�$�����(�. �$'�$�����'���������%*�����*'�$�'�$�+����(�$)�$$�(�. ��'��'���������1�. '���$�� ������-�)�� �������
���*'�$�'�$�+����(�)�� ����(����������(������)�+����(���)��(�)�$�������&���$���&���� ���1�. '�)'�4�'����&��(+�
5 '�&���$��'���(���)��(�)�$����(�)�� ����0���6� ���
4��(�$)�$$����'�$���0������)��. ��'���� ��-��&��&�/-1�����$����)0������(�,����(�����$7�
��� �����&���������&��&�/-� �������� ��������������/�����0���#�����#� ��#�4 �(�
�
����)��(�����$� �
�
"�,����&�����$����&�! ����'� �&���&���$$������
� ���7�
�&������������ �� � *�� �7�
�((&�$$� � *�����7�
�
,� �� � �����$- ��������$./ .�0���0� � ��,�������
�������������� ���������
������ ����� ������������ � �
����������� ��������� � � ��������

�
Review of DNACPR Status �� ���$����$�$'���(�+��&����. �(�. '����'�&���$���-�$�,����)����)'��,������'���������3$�)�&)�� $���)�$%��
0�� ��,�������������������������"�������1�
• � ����� ���2��� ���������� ������� �
• ����� ������� ��� ���� �� 3����� ��������
• ����� �� ������������������
��
Notes '�*'����$���-$��������� �&���&��&����$�. �$���$��0��. ���$��'������5 ���$�4���,&���(� �&�����'. �-���&��'��-��,1���(���'�&�
$�� ���&���� �$%��$)�$$����. ��'��'���������#��/�����0��#���# �#4 ���$�����)�� ���$�&-�����'�$�$��������1�+�����������'��������$�� �$��+����)0�(%�
(��&�/-�� ���$���������'�������. ��,7�����8���$���,���. �&��������&��-9�4 ��8�4�(����(�����(�)��� ���)��-��(��)���9� ��8� ��&����������(�����-%��������$����&��&����%�
%���+�$������&�$��(�)�$����� �(�����+�'������������������ �$��� ���������'��)��(�����$�����'�������� ���)��-��)�����:%�4����;+�$������&�$�<�(�)�$���1�����=�����'��+�/�$�� �$��+����)0�(%�>���$'���(���$��&�)�&(�(�����$����(�$)�$$���$�����'���������<$�����$%�
)�����$��&���&�����'�������� ���)��-��)�����:���&�)��(�����$�. '���(���&� ����,���3+�$������&�$�3�(�)�$������&�����������. '����)0$�)���)��-%�
*��$)�$$����. ��'��'����/�����0����$�����)�� ���$�&-�����'�$�$��������1�+����$�$�&��,�-��(��$�(�?. ��'��'���������<$���&� �$$���@%���������'����������$�� �$��+����)0�(%�
+�����$��&���&�����'�������� ���)��-��)�����:���&�(�����$����. '���)��$������$���A����(������)�+����(���)��(�)�$���A%�
�
CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p15/17)
Summary of Guidelines for Symptom Management Syringe Drivers Syringe drivers are not always necessary, but are extremely useful if the patient is: • nauseous or vomiting, or has poor oral absorption • unable to swallow or too weak for oral drugs • unconscious All the drugs in the guidelines are compatible in mixtures in a syringe driver. • Precipitation may occur with higher concentrations of cyclizine. • Water for injection can be used to dilute all of these drugs
- 0.9% sodium chloride is a suitable alternative for most mixtures - Cyclizine is always incompatible with sodium chloride
Renal Impairment /Renal Failure and End of Life Care Many of the drugs used for symptom control in end of life care are eliminated by the kidney to a greater or lesser degree. Morphine and diamorphine (or their active metabolites) accumulate in even modest degrees of renal impairment, and great care is needed to avoid toxicity.
Renal Impairment: Oxycodone is often used as an alternative to morphine/diamorphine in mild to moderate renal impairment. NSAIDs can worsen renal impairment. Most other drugs (used for symptom control in end of life care) can be used in renal impairment as long as the patient is regularly reviewed; consider starting with smaller doses and /or longer intervals between doses (e.g. 50% normal recommended dose).
Renal Failure: Prescribing for end of life care in patients with end stage renal failure (e.g.”dialysis” levels) is complex and advice should usually be sought from the renal/palliative care specialists. If a strong opioid analgesic is required urgently, give stat. fentanyl 25 microgram SC or alfentanil 100 microgrammes. (If fentanyl/alfentanil is not immediately available consider oxycodone 1-2mg SC). Seek advice if starting syringe driver and/or pain remains a problem. If treatment needs to be started for excess respiratory secretions or ‘rattle’ glycopyronium 0.2mg stat SC is recommended. (If glycopyronium is not available, consider hyoscine hydrobromide 0.2-0.4mg SC.) For midazolam, haloperidol and levomepromazine, administer half of the usual dose subcutaneously stat. Repeat doses on a PRN basis to allow for negligible elimination of the drug.
Pain Is the patient able to swallow medication? If yes � continue oral morphine SR + 1/6th dose for breakthrough pain If no � convert to a syringe driver • Calculate 24h intake of morphine. • Divide total by 3 to get the equivalent dose of diamorphine CSCI over 24h.
- e.g. Patient on 60mg MST b.d. and had 3 doses of 20mg Oramorph - Total (60 x 2) + (3 x 20) =180mg morphine total in 24h - Equivalent dose of diamorphine = 180/3 = 60mg/24h
• Also needs breakthrough dose prescribing of 1/6th of syringe driver i.e. 10mg diamorphine 4-hourly SC PRN in this example.
If not previously on a strong opioid: • Bolus diamorphine 2.5-5mg SC • Syringe driver up to 20mg diamorphine CSCI over 24h • PRN medication - 2.5-5mg SC diamorphine 4-hourly
�
CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p16/17)
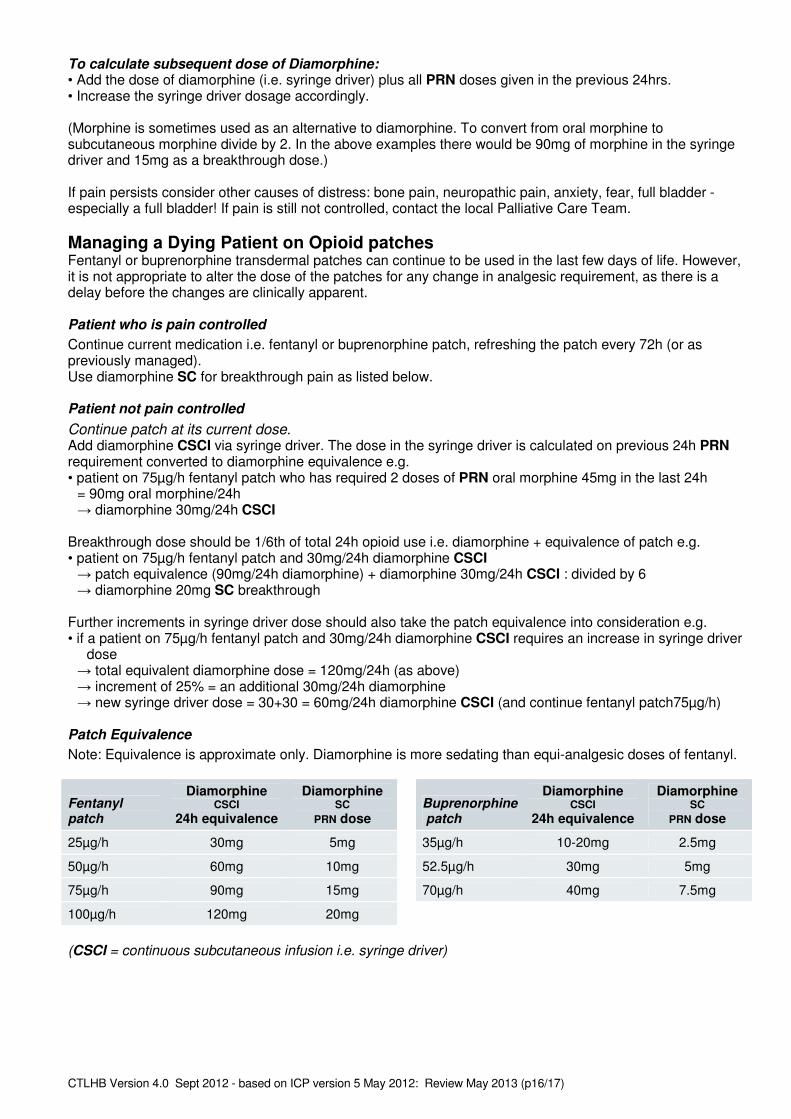
To calculate subsequent dose of Diamorphine: • Add the dose of diamorphine (i.e. syringe driver) plus all PRN doses given in the previous 24hrs. • Increase the syringe driver dosage accordingly. (Morphine is sometimes used as an alternative to diamorphine. To convert from oral morphine to subcutaneous morphine divide by 2. In the above examples there would be 90mg of morphine in the syringe driver and 15mg as a breakthrough dose.) If pain persists consider other causes of distress: bone pain, neuropathic pain, anxiety, fear, full bladder - especially a full bladder! If pain is still not controlled, contact the local Palliative Care Team. Managing a Dying Patient on Opioid patches Fentanyl or buprenorphine transdermal patches can continue to be used in the last few days of life. However, it is not appropriate to alter the dose of the patches for any change in analgesic requirement, as there is a delay before the changes are clinically apparent.
Patient who is pain controlled Continue current medication i.e. fentanyl or buprenorphine patch, refreshing the patch every 72h (or as previously managed). Use diamorphine SC for breakthrough pain as listed below.
Patient not pain controlled Continue patch at its current dose. Add diamorphine CSCI via syringe driver. The dose in the syringe driver is calculated on previous 24h PRN requirement converted to diamorphine equivalence e.g. • patient on 75µg/h fentanyl patch who has required 2 doses of PRN oral morphine 45mg in the last 24h = 90mg oral morphine/24h � diamorphine 30mg/24h CSCI Breakthrough dose should be 1/6th of total 24h opioid use i.e. diamorphine + equivalence of patch e.g. • patient on 75µg/h fentanyl patch and 30mg/24h diamorphine CSCI � patch equivalence (90mg/24h diamorphine) + diamorphine 30mg/24h CSCI : divided by 6 � diamorphine 20mg SC breakthrough Further increments in syringe driver dose should also take the patch equivalence into consideration e.g. • if a patient on 75µg/h fentanyl patch and 30mg/24h diamorphine CSCI requires an increase in syringe driver
dose � total equivalent diamorphine dose = 120mg/24h (as above) � increment of 25% = an additional 30mg/24h diamorphine � new syringe driver dose = 30+30 = 60mg/24h diamorphine CSCI (and continue fentanyl patch75µg/h)
Patch Equivalence Note: Equivalence is approximate only. Diamorphine is more sedating than equi-analgesic doses of fentanyl. �
Fentanyl patch
Diamorphine CSCI
24h equivalence
Diamorphine SC
PRN dose
25µg/h 30mg 5mg
50µg/h 60mg 10mg
75µg/h 90mg 15mg
100µg/h 120mg 20mg ��
�
Buprenorphine patch
Diamorphine CSCI
24h equivalence
Diamorphine SC
PRN dose
35µg/h 10-20mg 2.5mg
52.5µg/h 30mg 5mg
70µg/h 40mg 7.5mg �
(CSCI = continuous subcutaneous infusion i.e. syringe driver)

�
CTLHB Version 4.0 Sept 2012 - based on ICP version 5 May 2012: Review May 2013 (p17/17)
Nausea and Vomiting • PRN medication on all treatment sheets: cyclizine 50mg SC bolus 4hrly • If patient is already on cyclizine: levomepromazine (methotrimeprazine) 6.25mg SC bolus 4hrly PRN • If nauseous or vomiting:
- Cyclizine 150mg SC via syringe driver over 24h If patient has congestive heart failure use haloperidol rather than cyclizine. • If problem persists:
- Add haloperidol up to 5mg to syringe driver over 24h, or - Replace above drugs with levomepromazine (methotrimeprazine) 12.5mg over 24h - Contact Palliative Care Team
• If bowel obstruction present: contact the Palliative Care Team.
Restlessness, Agitation, Anxiety There is wide inter-individual variation in the sedative effect of midazolam. Please prescribe the doses of
midazolam on a patient-by-patient basis. • All treatment sheets to have PRN midazolam (average dose 5mg) SC. The option of a higher dose (e.g.
10mg) may be appropriate for some patients e.g. at risk of a seizure or major haemorrhage. • If patient is restless: - Add 10-20mg midazolam to syringe driver over 24h. - Give midazolam 2-hourly PRN • The dosage in the syringe driver should be increased as needed, either by a fixed increment e.g. 50%, or by
adding in the previous 24h PRN requirement. If patient remains restless, or more than 30mg is required in 24h, review for reversible causes e.g. urinary retention, and consider contacting Palliative Care Team.
Noisy Breathing due to Respiratory Tract Secretions • All treatment sheets to have hyoscine hydrobromide 0.4mg SC 4-hourly written up. • If symptoms present give:
- Hyoscine hydrobromide 0.4mg SC bolus - Add hyoscine hydrobromide 1.2mg SC to syringe driver over 24h.
• If symptoms persist increase hyoscine hydrobromide to 2.4mg (in 24h).
Out of Hours Specialist Telephone Help Line (South East Wales): 02920 426000
Guidelines: http://book.pallcare.info