als het hart faalt…. - azdiest.be cardiologie/hartfalen... · over aanwezigheid van hartfalen....
TRANSCRIPT

+
Als het hart faalt….
Dr. Sofie Moreels
Cardiologie-Intensieve geneeskunde

+

+
HF bij cardioloog
HF bij huisarts
Ongekend HF met
symptomen
Asymptomatisch HF
Wie behandelt hartfalenpatiënten?
Inadequate behandeling leidt tot (re)hospitalisaties en mortaliteit!

+Hartfalen anno 2017
Hartfalentherapie:
Wat verandert?
Wat blijft belangrijk?
Wat is nieuw?
Enkele stellingen
GEEN exhaustief hartfalenoverzicht!

+Definitieve diagnose van hartfalen is enkel
mogelijk door een cardioloog

+
Ja, want een huisarts beschikt niet over echocardiografie
toestel.
Neen, want NT-pro-BNP bepaling geeft mij altijd zekerheid
over aanwezigheid van hartfalen.
Neen, kliniek van de patiënt en NT-pro-BNP bepaling staan
altijd toe om zelf de diagnose te stellen.
Definitieve diagnose van hartfalen is enkel
mogelijk door cardioloog


+
Ja, want een huisarts beschikt niet over echocardiografie toestel.
Neen, want NT-pro-BNP bepaling geeft mij altijd zekerheid over aanwezigheid van hartfalen. NT Pro BNP geeft zekerheid over afwezigheid van hartfalen zo laag
Neen, kliniek van de patiënt en NT-pro-BNP bepaling staan altijd toe om zelf met zekerheid de diagnose te stellen. niet altijd maar vaak wel!
Definitieve diagnose van hartfalen is enkel
mogelijk door cardioloog

+Wat is er verandert in definitie van hartfalen?


HFrEF HFpEF en HFmrEF
EF< 40% EF 40-49%EF >50%

+HFrEF, HFmrEF, HFpEF: medicamenteuze
basistherapie blijft altijd dezelfde

+
Ja, ACE-I, betablokker en spironolactone verbeteren altijd de outcome in elke groep!
Ja, maar enkel HFrEF heeft nood aan lisdiuretica.
Neen, bij HFpEF en HFmrEF hebben ACE-I, betablokkers en spironolactone weinig effect op de outcome.
HFrEF, HFmrEF, HFpEF: medicamenteuze
basistherapie blijft altijd dezelfde
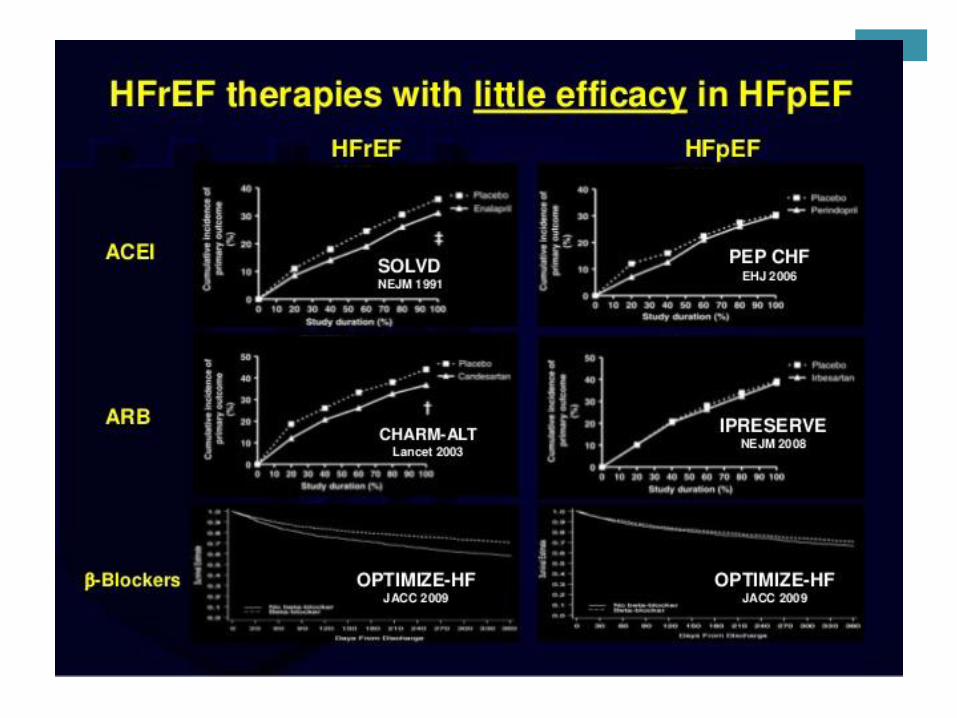



+
Ja, ACE-I, betablokker en spironolactone verbeteren altijd de outcome in elke groep!
Ja, maar enkel HFrEF heeft nood aan lisdiuretica. te gebruiken bij congestie zowel voor HFrEF, HFmrEF als HFpEF!
Neen, bij HFpEF en HFmrEF hebben ACE-I, betablokkers en spironolactone weinig effect op de outcome.
HFrEF, HFmrEF, HFpEF: medicamenteuze
basistherapie blijft altijd dezelfde


Wie is symptomatisch?


+
Levin et al. N Engl J Med 1998;339:321–8.
Nathisuwan & Talbert. Pharmacotherapy
2002;22:27–42 . Kemp & Conte.
Cardiovascular Pathology 2012;365–71 .
Schrier & Abraham. N Engl J Med
1999;341:577–85
HF SYMPTOMS &
PROGRESSION
Sympathetic
nervous system
Epinephrine
Norepinephrineα1, β1, β2
receptors
VasoconstrictionRAAS activity
VasopressinHeart rate
Contractility
Renin-angiotensin-
aldosterone system
VasoconstrictionBlood pressure
Sympathetic toneAldosterone
HypertrophyFibrosis
Ang II AT1R
VasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
NPRs NPs
Natriuretic peptide
system
ANP, BNP and CNP
Afname in systolische functie geeft activatie van 3 neuro-humorale
assen = BASIS van hartfalen behandeling bij HFrEF

+Basistherapie HFrEF
Betablokkade
ACE- inhibitor, bij intolerantie: ARB
Mineralocortoid receptor antagonist: spironolactone!
Trage optitratie tot maximale dosis is ABSOLUUT
aangewezen!

+
1. McMurray et al. Eur J Heart Fail. 2013;15:1062–73; Figure references: Levin et al. N Engl J Med 1998;339:321–8; Nathisuwan and Talbert. Pharmacotherapy 2002;22:27–42; Kemp and Conte. Cardiovasc Pathol2012;365–71; Schrier and Abraham N Engl J Med 2009;341:577–85.
SNS
RAAS
VasoconstrictionBlood pressure
Sympathetic toneAldosterone
HypertrophyFibrosis
Ang II AT1R
HF SYMPTOMS &
PROGRESSION
NP system
VasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
NPRs NPs
Epinephrine
Norepinephrineα1, β1, β2
receptors
VasoconstrictionRAAS activity
VasopressinHeart rate
Contractility
RAAS inhibitors
(ACEI, ARB, MRA)
β-blockers
ANP, BNP and CNP
Aanknopingspunt basistherapie

+
Relative risk reduction of all-cause mortality (%)
17%
48%
ARB
ACEI
ACEI + BB + ARB
ACEI + BB + MRA 56%
ACEI + MRA 43%
12%
43%
BUT: mortality remains high ~50% of patients die within 5 years of diagnosis1-3
Improved HFrEF therapies lead to increased survival
vs. placebo
ACEI + BB


+ARNI = angiotensine receptor
neprilysin inhibitor
Sacubitril/Valsartan is a salt complex that
comprises
the two active moieties:1,2
– sacubitril (AHU377) – a pro-drug; further
metabolized to the neprilysin inhibitor
sacubitrilat (LBQ657), and
– valsartan – an AT1 receptor blocker
in a 1:1 molar ratio
1. Gu et al. J Clin Pharmacol 2010;50:401–14;
2. Langenickel & Dole. Drug Discov Today: Ther Strateg 2012;9:e131–9
Sacubitril/valsartan = LCZ696 = Entresto®

+
1. McMurray et al. Eur J Heart Fail. 2013;15:1062–73; Figure references: Levin et al. N Engl J Med 1998;339:321–8; Nathisuwan and Talbert. Pharmacotherapy 2002;22:27–42; Kemp and Conte. Cardiovasc Pathol2012;365–71; Schrier and Abraham N Engl J Med 2009;341:577–85.
SNS
RAAS
VasoconstrictionBlood pressure
Sympathetic toneAldosterone
HypertrophyFibrosis
Ang II AT1R
HF SYMPTOMS &
PROGRESSION
INACTIVE
FRAGMENTS
NP system
VasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
NPRs NPs
Epinephrine
Norepinephrineα1, β1, β2
receptors
VasoconstrictionRAAS activity
VasopressinHeart rate
Contractility
Neprilysin
inhibitors
RAAS inhibitors
(ACEI, ARB, MRA)
β-blockers
ANP, BNP and CNP
Sacubitril
Valsartan
Neprilysin inhibition combined with RAAS blockade

+
McMurray et al. Eur Heart J 2012;33:1787–847
STANDARD
HFrEF CAREMRA ACEI
/
ARB
BB
ARNI as breakthrough treatment for HFrEF
+ ARNI
At 3.5 years of follow-up
ARNIMRA
BB
Relative risk reduction of all-cause mortality (%)
+ 16%PARADIGM-HF*
Sacubitril/valsartan (ARNI) led to a 16% reduction in all-cause mortality
on top of standard HFrEF care

+Welke patiënt?
Standard patient profile
• Symptomatic chronic HFrEF
• NYHA Class II/III/IV
• SBP ≥ 100 mmHg
• GFR ≥ 30 ml/min/1.73m2
• K < 5.4 mmol/L
• No co-administration ACEi/ARB
Reimbursement (1 Nov 2016)
• Symptomatic chronic HFrEF
(LVEF ≤ 35%)
• NYHA Class II/III/IV
• Optimal pretreatment with
ACEI/ARB
• Initiation by cardiologist or internist
TITRATION BY GP AND
CARDIOLOGIST
Nevenwerkingen en contra-indicatie gelijkaardig aan ACE-I en ARB!

+
Washout
Moderate dose
Low dose *
Low dose *
24/26 mg
49/51 mg
2-4
weeks
ACEi
ARB
or
Day 1 Day 2/3
Day 1
97/103 mg
Start
EntrestoACEi
Start
EntrestoARB
36 h
49/51 mg
97/103 mg
24/26 mg
49/51 mg
97/103 mg
49/51 mg
97/103 mg
2-4
weeks
2-4
weeks
2-4
weeks
2-4
weeks
2-4
weeks
Twice daily intake
Day 1
* Renal or hepatic impairment, hypotension (SBP < 100-110
mmHg)
Moderate dose


+Cardiale resynchronisatie therapie


+Ivabradine

+


+Ijzertekort wordt best behandeld bij HFrEF

+Ijzertekort wordt best behandeld bij HFrEF
Ja, een ijzerbepaling zit dus best in een standaard
bloedname bij follow-up van chronisch hartfalen.
Neen, want meestal is er eerder ijzerstapeling bij
hartfalen.
Ja, maar enkel intraveneuze ijzertoediening heeft bewezen
effect op hartfalensymptomen, inspanningscapaciteit en
levenskwaliteit.



+Ijzertekort wordt best behandeld bij HFrEF
Ja, een ijzerbepaling zit dus best in een standaard bloedname bij
follow-up van chronisch hartfalen. nood aan ferritine en TSAT
bepaling!
Neen, want meestal is er eerder ijzerstapeling bij hartfalen.
haemochromatose is een zeldzame oorzaak van hartfalen
Ja, maar enkel intraveneuze ijzertoediening heeft bewezen effect
op hartfalensymptomen, inspanningscapaciteit en
levenskwaliteit.


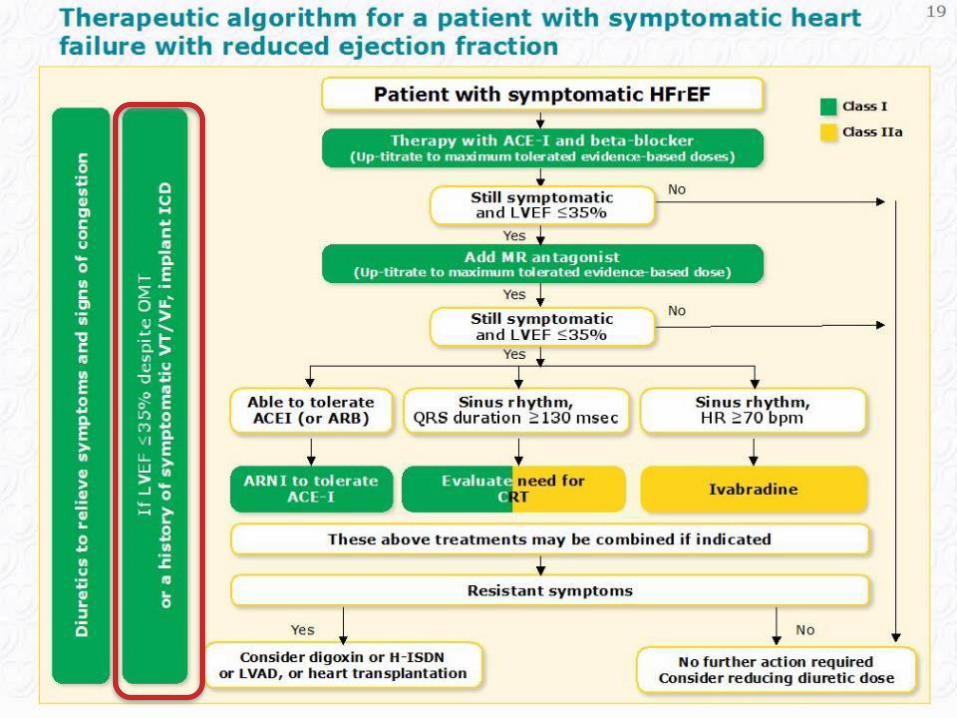
+Take home messages
Herken uw hartfalenpatiënt en stuur door, ook in geval van twijfel: nood aan echocardiografie!
Bij HFmrEF en HFpEF:
Behandel cardiale co-morbiditeit: hypertensie, VKF, coronair lijden, ….
Opvolgen congestietekens, tijdig diuretica om hospitalisatie te voorkomen!
Bij HFrEF:
titreer actief en kritisch de ingestelde basistherapie op!
herken nieuwere zinvolle therapieën: ARNI, CRT-D, ivabradine.
Bepaal ferritine en TSAT bij chronische follow-up van uw hartfalenpatiënt

+Vragen?

+ Van harte…