ami strategy how to achieve door-to-balloon times of 90 minutes and what to do next? aaron...
TRANSCRIPT

AMI StrategyHow to Achieve Door-to-Balloon Times of 90
Minutes and What to Do Next?
Aaron Kugelmass, MDDirector, Cardiac Cath Lab
Associate Division Chief
Henry Ford Hospital
Detroit, Michigan, USA

Overview
• Introduction– The Argument for Primary PCI
• Overview of the Henry Ford Program
• Program Specifics– Process Dictates Outcomes
• Alternative Opportunities

Acute MI: Introduction
• 1.1 million people yearly in the US*
• About 500,000 have STEMI
• 220,000 die from their AMI
• 50% of deaths in the first hour
• Outlook of hospitalized patients better
*AHA: 2001 Heart and stroke statistics

Acute MI: Early ManagementReperfusion
• Pharmacological (Thrombolysis)– Fibrinolytics– Antithrombins– Platelet Inhibitors
• Mechanical (Direct/Primary PCI)• Angioplasty• Stent• Thrombectomy
• Combined– ? Facilitated PCI
Acute MI: Direct PCIAdvantages
• Rapid assessment of anatomy and hemodynamics
• TIMI-3 flow rates 75-95% in infarct artery• Low incidence of hemorrhagic stroke• Can be done in patients with
contraindications for thrombolysis• Results superior to thrombolytics in
randomized trials

PCI vs Lysis Meta Analysis
Keeley E, Lancet 2003; 361: 13–20

Lytics vs Transfer for PCI: DANAMI

Acute MI: Direct PCILimitations
• Only 20% of US hospitals have cath labs and fewer have PTCA facilities
• To achieve results similar to randomized trials the following has to be met:– PTCA within 90 minutes of presentation– Skilled operator (>75 cases/year)– Skilled lab (>200 cases/year)– Surgical back up necessary
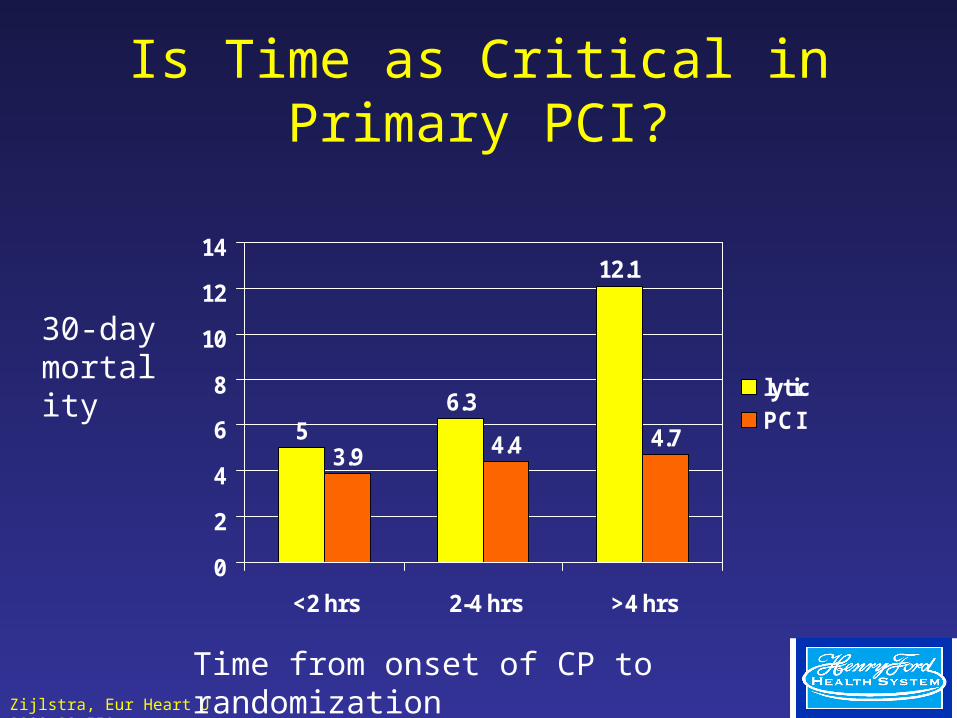
Is Time as Critical in Primary PCI?
56.3
12.1
3.9 4.4 4.7
0
2
4
6
8
10
12
14
<2 hrs 2-4 hrs >4 hrs
lyticPCI
30-day mortality
Time from onset of CP to randomizationZijlstra, Eur Heart J 2002;23:550

ACC/AHA Recommendations for Direct PCI in AMI
2004Class I• General:
– Patients presenting within 12 hours; if performed in a timely fashion by individuals skilled in the procedure and supported by experienced personnel in high volume centers
• Specific:– Door To Balloon Time <90 min– < 3hours symptom, PCI if treatment <1 hour, lytics if >1 hour– Symptom >3 hours, PCI preferred <90min– Within 36 hours of MI when patient develops cardiogenic shock,
is <75 years and revascularization can be done within 18 hours of shock onset.
– <12 hours of symptoms and severe CHF or pulmonary edema
(2004) Http://www.acc.org/clinical/guidelines

Primary PCI in the United States
• Minority of US Hospitals Achieve a median Door to Balloon Time of 90 minutes or less
• Majority of MI occur during “Off Hours” (nights and weekends)
• Off Hour Primary PCI is associated with increased door to balloon times and mortality
• Henry Ford 2002– Door to Balloon 218 minutes– Cath Lab to Balloon 60 minutes

Primary PCI PathwayAn Opportunity for Process Improvement
• Patient Presentation to Diagnosis 20 min• Page Fellow, Fellow Responds 10 min• Fellow Proceeds to ER 15 min• Fellow Evaluates Patient 15 min• Fellow Pages CCU Staff, Staff Responds 10 min• + PCI, Fellow Pages Int Staff, Staff Responds 10 min• Fellow goes to Cath Lab, Pages Team 10 min• Patient Stays in ER or Goes to CICU• Cath Team Arrives 60 min• Find Patient and Transport 15 min• Perform PCI 45 min
Total 210 minutes

Process Change
• Centralize Communications
• Focus Clinical Decision Making
• Transfer SEMI Patients Directly to Site of Therapy
• Establish Transport Pathways
• Unite CICU/Cath Lab Nursing Functions
• Improve Door to Balloon Times!
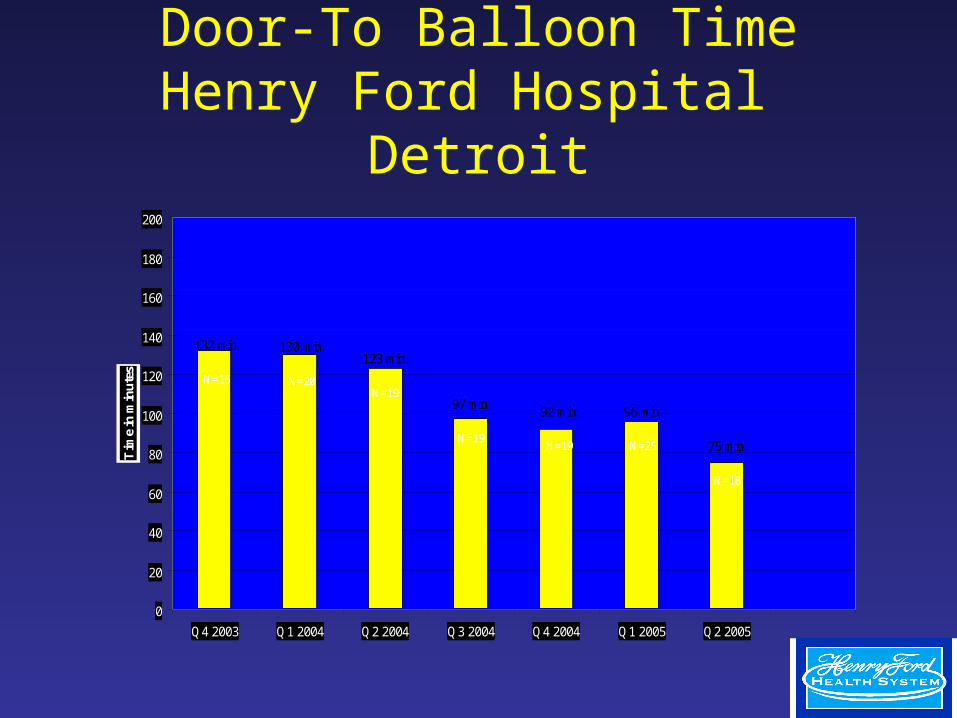
Door-To Balloon TimeHenry Ford Hospital
Detroit
123 min.
N=19
132 min.
N=16
130 min.
N=20
97 min.
N=19
92 min.
N=19
96 min.
N=25 75 min.
N=18
0
20
40
60
80
100
120
140
160
180
200
Q4 2003 Q1 2004 Q2 2004 Q3 2004 Q4 2004 Q1 2005 Q2 2005
Tim
e in
min
ute
s

Door-To Balloon TimeHenry Ford System Wide
2005
218
119
94102
108
7989
0
50
100
150
200
250
PREVIOUS January February March April May June
Syste m wide population consisting of: De troi t, W yandotte , Bi -C ounty, Fairlane , S te rl ing He ights, and W . Bloom fie ld
Tim
e in
min
ute
s

Henry Ford Acute Myocardial Infarction Program
• 6 Emergency Rooms– Henry Ford Hospital 90,000 visits– HF Wyandotte Hospital 72,000– HF Bicounty Hospital 28,000– Fairlane ER 47,000– West Bloomfield ER 22,000– Sterling Heights ER 21,000
• Primary PCI @ Henry Ford Hospital– Large Urban Teaching Hospital in Detroit


Henry Ford ER Locations
Henry Ford Owned (5) Partially Owned (3) HF Medical Center (24)
OAKLANDOAKLANDOAKLANDOAKLANDOAKLANDOAKLANDOAKLANDOAKLANDOAKLAND
WAYNEWAYNEWAYNEWAYNEWAYNEWAYNEWAYNEWAYNEWAYNE
MACOMBMACOMBMACOMBMACOMBMACOMBMACOMBMACOMBMACOMBMACOMB
SJMMSJMMSJMMSJMMSJMMSJMMSJMMSJMMSJMM
CottageCottageCottageCottageCottageCottageCottageCottageCottageBon SecoursBon SecoursBon SecoursBon SecoursBon SecoursBon SecoursBon SecoursBon SecoursBon SecoursNew Center OneNew Center OneNew Center OneNew Center OneNew Center OneNew Center OneNew Center OneNew Center OneNew Center One
HamtramckHamtramckHamtramckHamtramckHamtramckHamtramckHamtramckHamtramckHamtramck
HarbortownHarbortownHarbortownHarbortownHarbortownHarbortownHarbortownHarbortownHarbortownFairlaneFairlaneFairlaneFairlaneFairlaneFairlaneFairlaneFairlaneFairlane
Detroit NWDetroit NWDetroit NWDetroit NWDetroit NWDetroit NWDetroit NWDetroit NWDetroit NW
LakesideLakesideLakesideLakesideLakesideLakesideLakesideLakesideLakeside
Grosse PointeGrosse PointeGrosse PointeGrosse PointeGrosse PointeGrosse PointeGrosse PointeGrosse PointeGrosse Pointe
Detroit EastDetroit EastDetroit EastDetroit EastDetroit EastDetroit EastDetroit EastDetroit EastDetroit East
East JeffersonEast JeffersonEast JeffersonEast JeffersonEast JeffersonEast JeffersonEast JeffersonEast JeffersonEast Jefferson
Ann ArborAnn ArborAnn ArborAnn ArborAnn ArborAnn ArborAnn ArborAnn ArborAnn Arbor
WoodhavenWoodhavenWoodhavenWoodhavenWoodhavenWoodhavenWoodhavenWoodhavenWoodhaven
SouthlandSouthlandSouthlandSouthlandSouthlandSouthlandSouthlandSouthlandSouthland
TaylorTaylorTaylorTaylorTaylorTaylorTaylorTaylorTaylor
CantonCantonCantonCantonCantonCantonCantonCantonCanton
PlymouthPlymouthPlymouthPlymouthPlymouthPlymouthPlymouthPlymouthPlymouth LivoniaLivoniaLivoniaLivoniaLivoniaLivoniaLivoniaLivoniaLivonia
NoviNoviNoviNoviNoviNoviNoviNoviNovi
Royal OakRoyal OakRoyal OakRoyal OakRoyal OakRoyal OakRoyal OakRoyal OakRoyal OakSouthfieldSouthfieldSouthfieldSouthfieldSouthfieldSouthfieldSouthfieldSouthfieldSouthfield
WarrenWarrenWarrenWarrenWarrenWarrenWarrenWarrenWarren
Sterling HeighSterling HeighSterling HeighSterling HeighSterling HeighSterling HeighSterling HeighSterling HeighSterling HeighTroyTroyTroyTroyTroyTroyTroyTroyTroy
HFHHFHHFHHFHHFHHFHHFHHFHHFH
HFBCHHFBCHHFBCHHFBCHHFBCHHFBCHHFBCHHFBCHHFBCH
KingswoodKingswoodKingswoodKingswoodKingswoodKingswoodKingswoodKingswoodKingswood
HFWHHFWHHFWHHFWHHFWHHFWHHFWHHFWHHFWH
HFWBHHFWBHHFWBHHFWBHHFWBHHFWBHHFWBHHFWBHHFWBH
HFHS RegionsHFHS RegionsHFHS RegionsHFHS RegionsHFHS RegionsHFHS RegionsHFHS RegionsHFHS RegionsHFHS Regions
DetroitDownriverMacombPlusOaklandWestern Wayne
20 m, 33 min14 m, 25 min
9 m, 24 min
8 m, 17 min
12 m, 26 min

Door-To Balloon TimeHenry Ford System Wide
2005
218
119
94102
108
7989
0
50
100
150
200
250
PREVIOUS January February March April May June
Syste m wide population consisting of: De troi t, W yandotte , Bi -C ounty, Fairlane , S te rl ing He ights, and W . Bloom fie ld
Tim
e in
min
ute
s
Improving Door to Balloon Time
How Do You Change The Process?

Create A Multi Disciplinary TeamIdentify Advocates
• Cath Lab– Doctors, Nurses, Managers
• CCU– Doctors, Nurses, Managers
• Emergency Room– Doctors, Nurses
• Cardiologists– Staff and Trainees
• Hospital Administration• Ambulance Transport
Changing the Process
• Improve the Process to Meet the Science
• Dissect Complex Activities into Quantifiable Steps– Team members help to redesign the
processes in their areas
• Establish Parallel (not serial) Processes
• Avoid Duplication– Example: IV Compatibility

Changing the Process
• Activation– Simple
• 1 Phone Call- 24 hours a day– Staffed by Decision Maker (MD who accepts patient and
activates team)– Team Activation is Invisible to the Outside
» Coordinator then activates staff members, arranges admission, etc…
Changing the Process
• Transport– Activate transport (ambulance) as early as
possible, usually before activating central team.
– Establish well known dispatch pathway– Minimize emergency room time– Communicate during transport

Changing the Process
• Minimize Steps– Patients Transported Directly to Cath Lab
• Business Hours- Easy• Off Hours
– In House Nurses and MD’s » Staff Cath Lab while Cath Lab Staff Travel to
Hospital» Prep Room and Patient

Changing the Process
• Cath Lab– Focused Pathway to Reperfusion
• 7 F Sheath• Diagnostic Angiography of non-IRV• Guide Catheter for suspected IRV• “Standard” initial PTCA Equipment
– Floppy Wire
– 2.0/2.5 mm Balloon
• Establish Reperfusion First, Optimize Result Later
• Remember the Team!– Call the ER and let them know the results

Cath Lab TimesArrival to Balloon Inflation
60
35
26 25
29
2627
0
10
20
30
40
50
60
70
PREVIOUS January February March April May June
System wide population consisting of: Detroit, Wyandotte, Bi-County, Fairlane, Sterling Heights, and W. Bloomfield
Tim
e in
min
ute
s
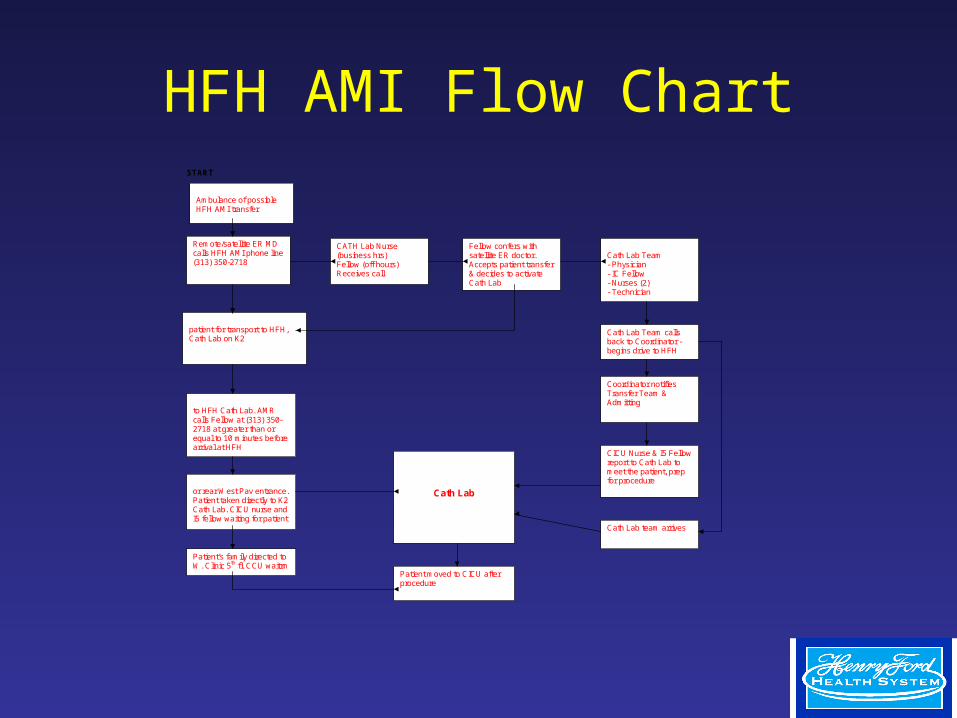
HFH AMI Flow ChartSTART
Remote/satellite ER MD calls HFH AMI phone line (313) 350-2718
CATH Lab Nurse Lab (business hrs) Fellow (off hours) Receives call
Fellow confers with satellite ER doctor. Accepts patient transfer & decides to activate Cath Lab
Coordinator pages the Cath Lab Team - Physician - IC Fellow - Nurses (2) - Technician
Remote ER site prepares patient for transport to HFH, Cath Lab on K2
Patient being transported to HFH Cath Lab. AMR calls Fellow at (313) 350-2718 at greater than or equal to 10 minutes before arrival at HFH
Cath Lab Team calls back to Coordinator - begins drive to HFH
Coordinator notifies Transfer Team & Admitting
CICU Nurse & I5 Fellow report to Cath Lab to meet the patient, prep for procedure Patient arrives through ER
or rear West Pav entrance. Patient taken directly to K2 Cath Lab. CICU nurse and I5 fellow waiting for patient
Cath Lab
Patient’s family directed to W. Clinic 5th fl. CCU waitrm
Cath Lab team arrives
Patient moved to CICU after procedure
Remote ER notifies Ambulance of possible HFH AMI transfer

Action start f inish duration
Remote or satellite ER/EKG assessment 0 5 5
Remote ER calls AMI phone line 5 7 2
CICU Nurse answers the call and takes report 5 7 2
CICU Nurse finds I5 Fellow, I5 Fellow accepts AMI patient transfer from satellite MD and Cath Lab is activated 7 10 3
CICU Nurse pages Cath Lab team 10 12 2
Cath Lab team calls back 12 17 5
Patient being prepared for transfer 10 20 10
CICU Nurse notifies Transfer Team & Admitting 12 25 13
AMI patient transported to HFH Cath Lab 20 65 45
CICU Nurse & I5 Fellow report to Cath Lab to stabilize, assess, prep prior to patient arrival 25 30 5
Cath Lab team transit/arrival 12 57 45
AMI patient arrives at HFH - family directed to CICU wait area 45 65 15
60+ minutes - Cath procedure performed on AMI patient 60 +
0 5 45 50 55 60+25 30 35 40Time (Minutes) 10 15 20
AMI Gann Chart
Changing the Process
• Metrics– Measure Your Lean Processes
• Door to EKG• EKG to Activation
– Transport
– Cath Lab
• Activation to Ambulance Arrival• “Pick Up Time” Ambulance arrival to departure• Transport Time ER departure to cath lab arrival• Cath Prep Time Cath arrival to arterial access• Procedure TimeArterial access to balloon or
reperfusion

Changing the Process
• Feedback– Share Outcomes and Pertinent Metrics with
Participants– Constructive Criticism is the Only Way to
Improve the Process– Success Begets Success
• Foster Participant Pride and Enthusiasm

Alternative Strategies and Next Steps
• Remote 12 lead EKG– EKG in Ambulance
• Transmit EKG from field• Activate Cath Lab field
• Disseminate Primary PTCA Centers– Offsite Surgical Back Up
• Centralize MI Centers– Practice Makes Perfect– Staff Lab 24/7

HFHS Initiatives
• Improve Door to EKG Time• Improve Transport Times
– New ambulance Structure• Activation to Arrival• “PickUp” Times
• Improve Cath Lab Response Times• Remote EKG
– In Field 12 lead EKG with telephonic transmission

Conclusions
• Careful Process Engineering Can Dramatically Reduce Door To Balloon Times– This Requires:
• A Multi-Disciplinary Team and Institutional Commitment
• Careful Metrics to Guide Improvement• Ongoing Feedback to Team Members• Continuous Evaluation to Drive Process
Improvement