an advanced diagnostic method in surgical pathology an advanced diagnostic method in surgical...
TRANSCRIPT

An
advanced diagnostic method
in
surgical pathology
An
advanced diagnostic method
in
surgical pathology

Mexico CampecheMexico Campeche“Hemotoxylum campechianum”
Bloody red bark tree
“Hemotoxylum campechianum”
Bloody red bark tree
Rosai : “The H & E technique” Rosai : “The H & E technique”
Old mistress apologueOld mistress apologue
Mainstay of surgical pathology Mainstay of surgical pathology The H & E technique ,1998 pathologicaThe H & E technique ,1998 pathologica

H&E AdvantagesH&E Advantages
Relatively quick
Inexpensive
Suitable for most situations
Easy to master
Allows accurate Dx of the large majority of specimens
Nevertheless, Cannot answer all the questions
Relatively quick
Inexpensive
Suitable for most situations
Easy to master
Allows accurate Dx of the large majority of specimens
Nevertheless, Cannot answer all the questions

SPECIAL TECHNIQUESSPECIAL TECHNIQUES
Special stains
Enzyme histochemistry
Tissue culture
Electron microscopy
Immunohistochemistry vs Immunocytochemistry !
Flow cytometry Cytogenetics
Molecular pathology Histometry
Special stains
Enzyme histochemistry
Tissue culture
Electron microscopy
Immunohistochemistry vs Immunocytochemistry !
Flow cytometry Cytogenetics
Molecular pathology Histometry

Ag
1st Ab
2nd Ab
Ag
Tag
Chromogene
To detect target antigens cytoplasmic
cytokeratin vimentin chromogranin A nuclear estrogen receptor progesterone receptor Ki-67 P-53 memebranous
Her 2-neu E-cadherin EGFR
Basic structure:PolypeptideGlycoproteinLipoprotein

Antigen
• The small site on an antigen to which a complementary antibody may specifically bind is called an epitope.
• This is usually one to six monosaccharides or 5–8 amino acid residues on the surface of the antigen.

Antigen
• Because antigen molecules exist in space, •specific three-dimensional antigenic conformation
(e.g., a unique site formed by the interaction of two native protein loops or subunits), or the epitope may correspond to a simple primary sequence region.
• Such epitopes are described as conformational and linear.
Antigen
•The range of possible binding sites is enormous, with each potential binding site having its own structural properties derived from: covalent bonds,
ionic bonds and hydrophilic and
hydrophobic interactions.
Ag-Ab reactionFor efficient interaction to occur between the antigen and the antibody: the epitope must be readily available for binding.
If the target molecule is denatured, e.g.
through fixation, reduction, osmolalaity changes, pH changes, temperature, chemical agents, the epitope may be altered and this may affect its ability to interact with an antibody.

Characteristics of a Good Antigen Include:
1.Areas of structural stability and chemical complexity within the molecule.
2.Lacking extensive repeating units.
3.A minimal molecular weight of 8,000–10,000 Daltons, although haptens with molecular weights as low as 200 Da have been used in the presence of a carrier protein.
4.The ability to be processed by the immune system.

Characteristics of a Good Antigen Include:
5.Immunogenic regions which are accessible to the antibody-forming mechanism.
6.Structural elements that are sufficiently different from the host.
7.For peptide antigens, regions containing at least 30% of immunogenic amino acids: K, R, E, D, Q, N.
8.For peptide antigens, significant hydrophilic or charged residues.

Class/ Subclass
Heavy Chain
Light Chain Molecular Weight (kDa)
Structure Function
lgA1
lgA2
12
or κ 150 to 600 Monomer to tetramer Most produced lg; protects mucosal surfaces; resistant to digestion; secreted in milk.
lgD or κ 150 Monomer Function unclear; Works with lgM in B-cell development. mostly B cell bound
lgE or κ 190 Monomer Defends against parasites; causes allergic reactions
lgGlgG2a
lgG2b
lgG3
lgG4
12234
or κ 150 Monomer Major lg in serum; good opsonizer; moderate complement fixer (lgG3); can cross placenta
lgM µ or κ 900 Pentamer First response antibody; Strong complement fixer; Good opsonizer

Monoclonal vs. Polyclonal2nd Ab : Mouse / goat / rabbit anti- 1st Ab1st Ab : Mouse / goat / rabbit anti-human

Antigen-Antibody Interaction
The specific association of antigens and antibodies is dependent on hydrogen bonds, hydrophobic interactions, electrostatic
forces, and van der Waals forces .
These are all bonds of a weak, non-covalent nature-Like antibodies.

Antigen-Antibody Interaction
Antigens can be multivalent, either through multiple copies of the same epitope, or through the presence of multiple epitopes that are recognized
by multiple antibodies .
Interactions involving multivalency can produce more stabilized complexes, however multivalency can also result in steric difficulties,
thus reducing the possibility for binding .

Antigen-Antibody Interaction
All antigen-antibody binding is reversible, however, and follows the basic thermodynamic principles of any
reversible bimolecular interaction :
where KA is the affinity constant, Ab and Ag are the molar concentrations of unoccupied binding sites on the antibody or antigen respectively, and Ab–Ag is the molar
concentration of the antibody-antigen complex.
Antigen-Antibody Interaction
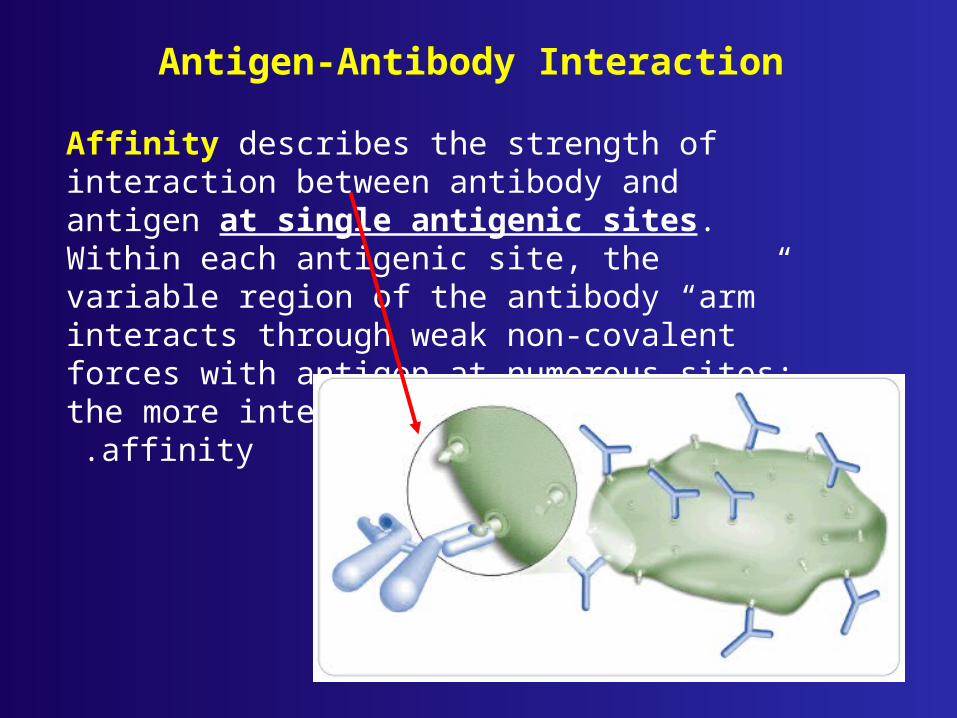
Affinity describes the strength of interaction between antibody and antigen at single antigenic sites. Within each antigenic site, the variable region of the antibody “arm” interacts through weak non-covalent forces with antigen at numerous sites; the more interactions, the
stronger the affinity.

Antigen-Antibody Interaction
Avidity is perhaps a more informative measure of the overall stability or strength of the antibody-antigen complex. It is controlled by three major factors:
1.antibody-epitope affinity;2. the valence of both the antigen and antibody;
3.and the structural arrangement of the interacting parts.

Polyclonal vs monoclonal
1.Polyclonal antibodies often recognize multiple epitopes ,
making them more tolerant of small changes in the nature of the antigen.

Polyclonal vs monoclonal
2.Polyclonal antibodies are often the preferred choice for detection of denatured proteins

Polyclonal vs monoclonal
3.Polyclonal antibodies may be
generated in a variety of species,
including rabbit, goat, sheep,
donkey, chicken and others,
giving the users many options
in experimental design.

Polyclonal vs monoclonal
4.Polyclonal antibodies are sometimes used when the nature of the antigen in an untested species is not known.

Polyclonal vs monoclonal
5.Polyclonal antibodies target multiple epitopes and so they generally provide more robust detection.

Monoclonal vs polyclonal
6.Because of their specificity,monoclonal antibodies are excellent as the primary antibody in an assay, or for detecting antigens in tissue, and will often give significantly less background staining than polyclonal antibodies.

Monoclonal vs polyclonal
7.When compared to that of polyclonal antibodies, homogeneity of monoclonal antibodies is very high. If experimental conditions are kept constant, results from monoclonal antibodies will be highly reproducible between experiments.

Monoclonal vs polyclonal
8.Specificity of monoclonal antibodies makes them extremely efficient for binding of antigen within a mixture of related molecules, such as in the case of affinity purification.


© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 28
Basic conceptsBasic concepts &&
Historical aspectsHistorical aspects

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 29
Basic ConceptBasic Concept
Immunohistochemistry isImmunohistochemistry is
1.The localization of antigens in tissue sections by the 1.The localization of antigens in tissue sections by the use ofuse of
2.labeled antibody as specific reagents through 2.labeled antibody as specific reagents through
3.antigen-antibody interactions3.antigen-antibody interactions
4.that are visualized by a marker such as 4.that are visualized by a marker such as
fluorescent dye, fluorescent dye, enzyme, enzyme,
radioactive element or radioactive element or colloidal gold.colloidal gold.

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 30
There are There are numerounumerous immunohistochemistrys immunohistochemistrymethodsmethods that may be used to localize antigens. that may be used to localize antigens.
The The selection of a suitable methodselection of a suitable method should be should be based on parameters such as :based on parameters such as :
the type of specimen under the type of specimen under investigation and investigation and
the degree of sensitivity required.the degree of sensitivity required.

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 31
1.Albert H. Coons 1944- 1955; fluorescent dye1.Albert H. Coons 1944- 1955; fluorescent dye
2.Nakane and Pierce 1966 ; enzyme labels / peroxidase; 2.Nakane and Pierce 1966 ; enzyme labels / peroxidase; Mason and Sammons 1978 alkaline phosphataseMason and Sammons 1978 alkaline phosphatase
3.Faulk and Taylor 1971; Colloidal gold by both light and 3.Faulk and Taylor 1971; Colloidal gold by both light and electron microscopy levelelectron microscopy level
4.Radioactive elements, and visualization by autoradiography.4.Radioactive elements, and visualization by autoradiography.
ImmunohistochemistryImmunohistochemistryHistorical aspectHistorical aspect

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 32
With the expansion and development of immunohistochemistry With the expansion and development of immunohistochemistry technique,technique,
enzyme labelsenzyme labels
have been introduced such as have been introduced such as
peroxidaseperoxidase (Nakane and Pierce 1966; Avrameas and Uriel 1966) (Nakane and Pierce 1966; Avrameas and Uriel 1966)
and and
alkaline phosphatasealkaline phosphatase (Mason and Sammons 1978).(Mason and Sammons 1978).

TO APPLY IHC OR ICC FORTO APPLY IHC OR ICC FOR ?…?…
1.Diagnostic purpose.1.Diagnostic purpose.
2.Prognostic purpose2.Prognostic purpose
3.Therapeutic purpose3.Therapeutic purpose
4.Preventive purpose?4.Preventive purpose?

Applications of IHCApplications of IHC Diagnostic purposeDiagnostic purpose::

Applications of IHCApplications of IHC Diagnostic purpose:Diagnostic purpose:
IHC profile for metastatic carcinoma of unknown IHC profile for metastatic carcinoma of unknown originorigin
FemaleFemale MaleMale
ER/PRER/PR PSAPSA
CK 7CK 7 CK 7CK 7
CK 8CK 8 CK 8CK 8
CK 20CK 20 CK 20CK 20
CD X2CD X2 CD X2CD X2
CEACEA CEACEA
TTF 1TTF 1 TTF 1TTF 1

Diagnostic purpose of Diagnostic purpose of IHCIHC
CK CK 77
CK CK 88
CK CK 2020
DxDx
++ ++ -- Follicular Follicular adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Adenocarcinoma ,PancreasAdenocarcinoma ,Pancreas
-- ++ ++ Hepatocellualr carcinomaHepatocellualr carcinoma
-- ++ -- Squamous cell carcinoma Squamous cell carcinoma CK CK 5/65/6
-- -- -- Thymoma Thymoma CK CK 5/65/6
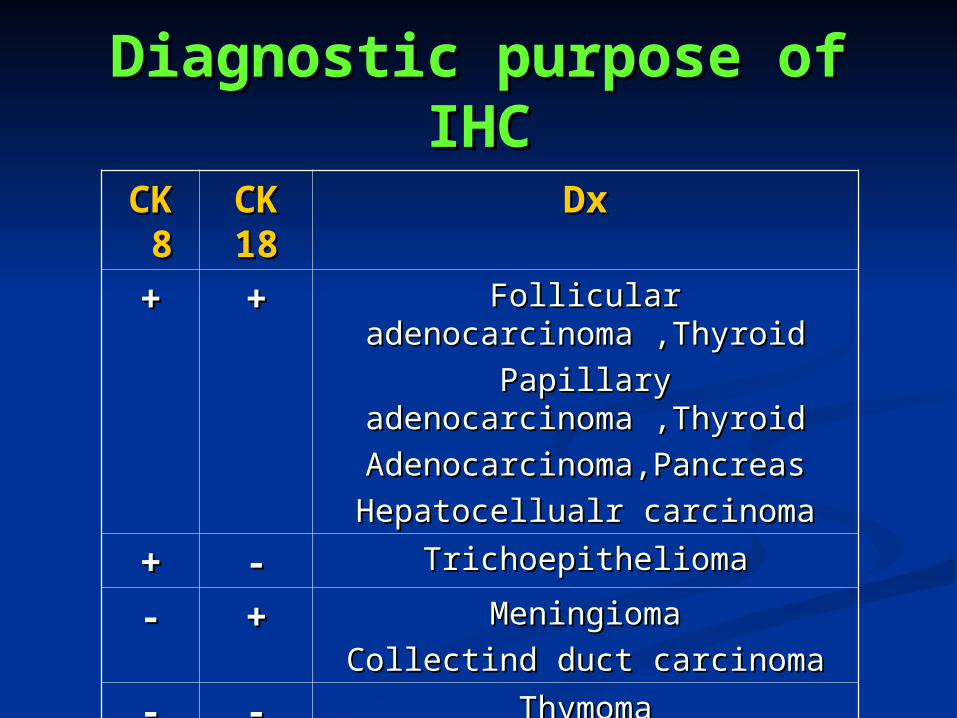
Diagnostic purpose of Diagnostic purpose of IHCIHC
CK CK 88
CK CK 1818
DxDx
++ ++ Follicular Follicular adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Papillary Papillary adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Adenocarcinoma,PancreasAdenocarcinoma,Pancreas
Hepatocellualr carcinomaHepatocellualr carcinoma
++ -- TrichoepitheliomaTrichoepithelioma
-- ++ MeningiomaMeningioma
Collectind duct carcinomaCollectind duct carcinoma
-- -- ThymomaThymoma
Adenocarcinoma , AmpullaryAdenocarcinoma , Ampullary

Applications of IHCApplications of IHC
Diagnostic purpose:Diagnostic purpose:an examplean example
IHC profile for prostatic carcinomaIHC profile for prostatic carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 40
IHC in prostate CancerIHC in prostate Cancer
Indications:Indications:1- Distinction of Benign from Malignant1- Distinction of Benign from Malignant
• High molecular weight cytokeratin (34High molecular weight cytokeratin (34E12, CK5/6)E12, CK5/6)
– Negative cytoplasmic marker (in basal cells)Negative cytoplasmic marker (in basal cells)• P63P63
– Negative nuclear stain (in basal cells)Negative nuclear stain (in basal cells)• AMACR (P504S)AMACR (P504S)
– Positive cytoplasmic marker (in tumor cells)Positive cytoplasmic marker (in tumor cells)– Also positive in HGPIN, 31% of Bladder Ca. & Also positive in HGPIN, 31% of Bladder Ca. &
70% of Colorectal Ca.70% of Colorectal Ca.

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 41
HMW-CK (34HMW-CK (34E12)E12)
Normal Glands
Negative in Carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 42
AMACR AMACR (P504S) stain (P504S) stain in Carcinomain Carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 43
P63 / AMACR P63 / AMACR cocktailcocktail
Increasing IHC resolution:

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 44
3434E12 / P63 / AMACR E12 / P63 / AMACR 2-chromogen cocktail2-chromogen cocktail
Increasing IHC resolution:

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 45
IHC in prostate Cancer IHC in prostate Cancer (Cont.)(Cont.)
Indications:Indications:
2- Differential Dx from urothelial carcinoma:2- Differential Dx from urothelial carcinoma:
PSA PSAP 34PSA PSAP 34E12 Leu7 CK5/6E12 Leu7 CK5/6
Prostate Ca + + – + -Prostate Ca + + – + -
Urothelial CaUrothelial Ca – – – – + + – +– +

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 46
IHC in prostate Cancer IHC in prostate Cancer (Cont.)(Cont.)
Indications:Indications:
3- Differential Dx in metastatic carcinoma:3- Differential Dx in metastatic carcinoma:
Bone Tumor:
PSA stain

Applications of IHCApplications of IHCPrognostic purposePrognostic purpose
in breast carcinomain breast carcinoma Poor prognostic Poor prognostic
markersmarkersGood prognostic Good prognostic
markersmarkers
ERER(-)(-) ERER(+)(+)
PRPR(-)(-) PRPR(+)(+)
pS2pS2(-)(-) pS2pS2(+)(+)
Her-2 (3+)Her-2 (3+) Her-2 (0/1+)Her-2 (0/1+)
Cathepsin DCathepsin D(+)(+) Cathepsin DCathepsin D(-)(-)
P 53 >10%P 53 >10% P 53 <10%P 53 <10%
EFGREFGR(+) (+) EGFREGFR( - )( - )
Ki-67>23%Ki-67>23% Ki-67<11%Ki-67<11%

Prognostic purpose of Prognostic purpose of IHCIHC
ER/PR/ER/PR/pS2pS2:: pS2 :pS2 : Cystein-rich peptide induced by estrogen Cystein-rich peptide induced by estrogen
secreted from breast cells.secreted from breast cells.
pS2 expression has been found to be associated with pS2 expression has been found to be associated with longer overall & disease free survival.longer overall & disease free survival.
ER +/ PR +/ ER +/ PR +/ pS2 +pS2 + : 85% to 97% have good : 85% to 97% have good prognosisprognosis
ER +/ PR +/ ER +/ PR +/ pS2 -pS2 - : only 50% to 54% have good : only 50% to 54% have good prognosis.prognosis.
How to Assess an IHC immunostain?
reproducibility
Inter-observer variation
inconsistency
Clinical data

An example
Assessment of Her2 status in breast cancer

Published guidelines (ASCO)
Her2 over-expression should be evaluated on every primary breast cancer either at the time of diagnosis or at the time of recurrence.
J Clin Oncol 19:1865-1878, 2001

Importance of getting it right• Poorer prognosis if HER2 positive
• Role in the selection of the most appropriate adjuvant therapy
• Herceptin® improves survival if HER2 positive, but not HER2 negative– false negatives
• deny life-extending treatment– false positives
• false hope
• complications & cost of the treatment

HER2 technical approaches• Gene amplification
– Southern or dot (slot) blotting
– quantitative PCR
– FISH/CISH
• mRNA over-expression– Northern blotting
– quantitative RT-PCR
• Protein over-expression– immunohistochemistry
– Western blotting
– Elisa

POINT MUTATIONS
Point Mutation
C-proto -onc C-onc
m-RNA
C-onc protein over production with Increased activity
M-RNA overexpression

IHCvs
FISH
• Fast• Cheap• Easy• False-negative rate• False-positive rate• Subjective interpretation• Difficult to standardise
• Long• Expensive• Difficult• Accurate (#signals)
• Theoretically does not identify pts with overexpression without gene amplific
• Standardised

IHC/FISH concordance
0 1+ 2+ 3+
FISH - 207 28 67 21
FISH + 7 2 21 176
3% 7% 24% 89%
Overall concordance: 82%
Mass R et al.: Proc ASCO 2000

Her2 testing algorithm
Patient tumour sample
IHC FISH
2+ 3+ + –
Retest withFISH
Herceptin®
therapyHerceptin®
therapy
– +
Herceptin®
therapy

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 58
How to interpret?How to interpret?
1.Intimacy with pattern of staining:1.Intimacy with pattern of staining:
NuclearNuclear ERER PRPR P 53P 53 Ki 67Ki 67
MembranousMembranous Her 2Her 2 EGFREGFR CD CD 2020
CD CD 4545
CytoplasmicCytoplasmic CKCK VimeVimentinntin
DesmDesminin
NSENSE SMASMA HMB-HMB-4545
CytonuclearCytonuclear S100S100 CalretCalretinininin

How to interpret? 2.Intimacy with scoring methods
Score Pattern Assessment
0 Staining of 0-10% cells Negative
1+ Faint and partial membrane staining
Negative
2+ Weak to moderate complete membrane
staining
Positive/ Negative
3+ Moderate to strong complete membrane
staining
Positive

Proficiency surveys of HER2 testing
2001 College of American Pathology IHC survey
• A breast tumor sample unreactive by IHC and FISH was distributed to 415 laboratories– 72% reported negative results
– 28% reported immunoreactivity
– 9% reported 2+ or 3+ scoresConclusion
Any HER2 assay performed at a non-reference laboratory (<100 cases/month) will require validation
at a reference laboratory

Potential for misdiagnosis (IHC)
• Antibodies (>28 commercially available)
• Technical performance
• Interpretation– scoring– artifacts
Common problems in HER2 IHC
• Underestimation of expression:– (over)fixation in NBF– poor antigen retrieval (unmasking)– choice of antibodies
• Overestimation– alcoholic (post)fixation (check normal
cells!)• Cytoplasmic staining

Who can interpret an IHC?

Normal lobule
3+ breast carcinoma

Lobular cancerization


2+ breast carcinoma

2+ breast carcinoma?
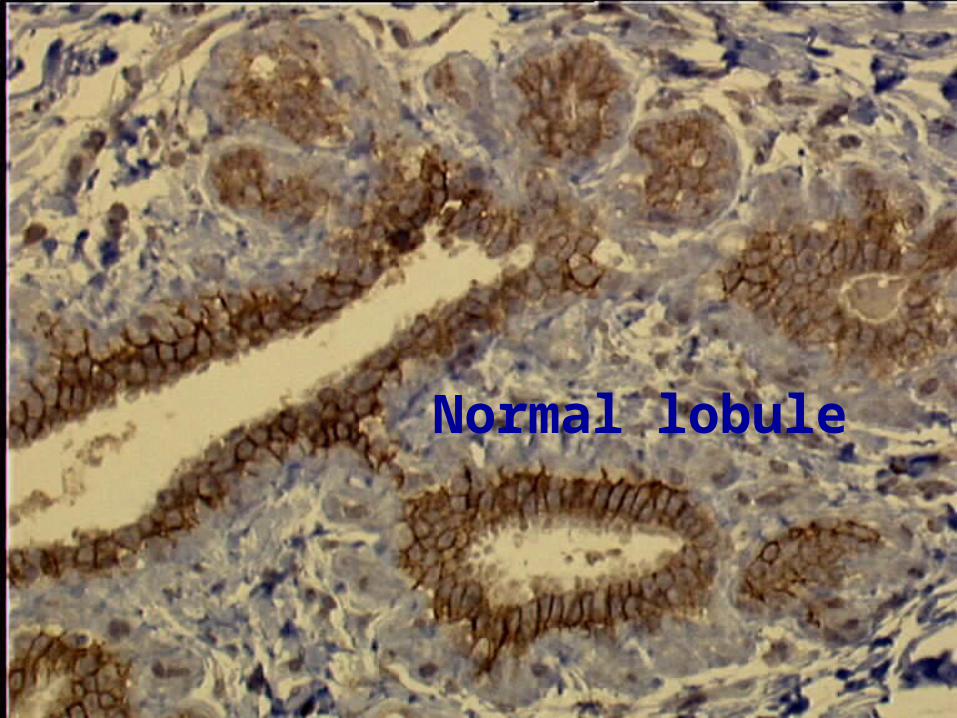
Normal lobule

Cytoplasmic staining

What to do?• Central Reference or large local laboratories
– high number of cases (>250 cases/year* or >100 cases/months [NSABP])
– quality assurance controls (internal and external)– automated IHC – high level of training (technique/interpretation)
• Small laboratories (<250 cases/yr or <100 cases/mos) – do not do it– send to larger laboratories
*Ellis I, et al: J Clin Pathol 2004
… but• There are labs capable of performing
quality testing with lower volumes• A high test volume does not ensure
an accurate test result• If an individual lab can properly
validate an assay and perform acceptably in an external validation, then it should be permitted to offer the test
Hsi ED & Tubbs RR: JCP 2004

Applications of IHCApplications of IHC therapeutic purposetherapeutic purpose Chemotherapy in breast Chemotherapy in breast
carcinomacarcinomaERER(+) (+) PRPR(+) (+) Tamoxifen / FemaraTamoxifen / Femara
ERER(-) (-) PRPR(+) (+) Tamoxifen / FemaraTamoxifen / Femara
ERER(+) (+) PRPR(-) (-) Tamoxifen / FemaraTamoxifen / Femara
Her-2 Her-2 psoitivpsoitiv
ee
TrastazumabTrastazumab
))HerceptinHerceptin((
Cost :300 000 000 Cost :300 000 000 RialsRials
Her-2 Her-2 negatinegati
veve
-- --

Applications Of IHCApplications Of IHC Therapeutic purpose: PharmaDx AbsTherapeutic purpose: PharmaDx Abs Chemotherapy in breast carcinomaChemotherapy in breast carcinoma ER - / PR - / Her-2 -ER - / PR - / Her-2 -
Triple negative breast Triple negative breast carcinomacarcinoma
Treatment is completely different:Treatment is completely different:
CisplatinCisplatin


Technical pointsTechnical points

Handling of AntibodiesHandling of Antibodies RTURTU Abs have a Abs have a shorter shelf lifeshorter shelf life
Upon receipt reagents should be Upon receipt reagents should be stored promptlystored promptly according to according to manufacturer’s recommendation.manufacturer’s recommendation.
Record: lot No, expiration date, date of receipt, invoice Record: lot No, expiration date, date of receipt, invoice number.number.

Storage ContainersStorage Containers Containers:Containers:
Negligible protein absorptivityNegligible protein absorptivity Polypropylene, polycarbonate, borosilicate glassPolypropylene, polycarbonate, borosilicate glass Clear & colorless containersClear & colorless containers Labels should allow access for inspectionLabels should allow access for inspection Solutions containing very low concentrations of Solutions containing very low concentrations of
protein (<10-100 microg/mL) should receive inert protein (<10-100 microg/mL) should receive inert protein such as 0.1 % to 1.0 % albumin to reduce protein such as 0.1 % to 1.0 % albumin to reduce polymerization & adsorption onto the container.polymerization & adsorption onto the container.

Storage TemperatureStorage Temperature Accurate and consistent temperatureAccurate and consistent temperature Temperature alarm & emergency backup systemTemperature alarm & emergency backup system Store RTU Abs & kits at 2-8 CStore RTU Abs & kits at 2-8 C Store concentrated Abs at -20 C in aliquotsStore concentrated Abs at -20 C in aliquots Prevent from contamination, heat, excessive light exposure.Prevent from contamination, heat, excessive light exposure. Sterile , clean pipette tipsSterile , clean pipette tips Prompt return to storage temperature.Prompt return to storage temperature.

Antibody TiterAntibody Titer

Antibody DilutionAntibody Dilution
How to determine optimal dilution?How to determine optimal dilution? TitrationTitration
First select a fixed incubation time.First select a fixed incubation time. Make small volumes of experimental dilutions.Make small volumes of experimental dilutions. 100 to 400 microL per section100 to 400 microL per section
What is the optimal dilution?What is the optimal dilution? Peak in intensityPeak in intensity Minimal background Minimal background Maximal signal to noise ratioMaximal signal to noise ratio

Effecte of pH & ion strength on Ab Effecte of pH & ion strength on Ab dilutiondilution
All monoclonal Abs could be diluted All monoclonal Abs could be diluted higher & stained more intensly at higher & stained more intensly at pH 6.0 .pH 6.0 .
IgG3 is an exception at pH 9.0 IgG3 is an exception at pH 9.0

PBS suppress the reactivity of all PBS suppress the reactivity of all monoclonal Absmonoclonal Abs
Commercial Ab diluents are Commercial Ab diluents are preferred.preferred.
PBS is usually used for dilution PBS is usually used for dilution nevertheless it leads to less reaction nevertheless it leads to less reaction and decrease in affinity, thus not and decrease in affinity, thus not recommended.recommended.

Antibody Dilution Antibody Dilution BuffersBuffers
Antibody dilution buffer is used for diluting primary and Antibody dilution buffer is used for diluting primary and secondary antibodies as well as some detecting reagentssecondary antibodies as well as some detecting reagents..
Primary Antibody Dilution BufferPrimary Antibody Dilution Buffer
1%1% BSA (stabilizer and blocking)BSA (stabilizer and blocking)
0.1%0.1% cold fish skin gelatin (blocking)cold fish skin gelatin (blocking)
0.05%0.05% sodium azide (preservative)sodium azide (preservative)
0.01M PBS, pH 7.20.01M PBS, pH 7.2

Antibody Dilution Antibody Dilution BuffersBuffers
TBS as Ab diluentTBS as Ab diluent11((TBS pH 7.6 used in primary antibody dilution buffer produces TBS pH 7.6 used in primary antibody dilution buffer produces
weaker stainingweaker staining ; ;
22((Antibodies diluted using this buffer can be stored at 4 ºC for 6 Antibodies diluted using this buffer can be stored at 4 ºC for 6 months without reducing binding activitymonths without reducing binding activity ; ;
33 ( (This buffer can not be used for diluting HRP conjugated This buffer can not be used for diluting HRP conjugated antibodies since sodium azide is an inhibitor of HRPantibodies since sodium azide is an inhibitor of HRP..

How to diluteHow to dilute??
1:10 dilution = one part of stock 1:10 dilution = one part of stock solution + nine parts of diluents.solution + nine parts of diluents.
Then , two-fold serial dilutionsThen , two-fold serial dilutions

How to diluteHow to dilute
To prepare 1.0 mL of a 1:1000 To prepare 1.0 mL of a 1:1000 dilution:dilution:
Step 1:Step 1: 10 micro + 90 micro ------- > 10 micro + 90 micro ------- > 1:101:10
Step 2:Step 2: 10 micro + 990 micro ----- > 10 micro + 990 micro ----- > 1:1001:100
Final dilution is 1:1000Final dilution is 1:1000

Checkerboard titrationCheckerboard titration
Checkerboard titrations are used to determine the Checkerboard titrations are used to determine the optimal dilution of more than one reagent optimal dilution of more than one reagent
simultaneously.simultaneously.
1.The optimal dilutions of the primary Ab & the streptavidin-HRP reagent are found.
2.While the dilution of the biotinylated link Ab is held constant.
3.Nine tissue sections are required for testing three dilutions.
4.If results achieved by use of several dilutions are identical or similar, reagent costs may become an additional factor in selecting optimal dilutions.

Incubation TimeIncubation Time
Inverse relationship between incubation time Inverse relationship between incubation time & antibody titer.& antibody titer.
The higher the Ab titer , the shorter the incubation The higher the Ab titer , the shorter the incubation time required for optimal result.time required for optimal result.
In practice:In practice:
First set a suitable incubation time then determine First set a suitable incubation time then determine the optimal dilution.the optimal dilution.
Incubation TimeIncubation Time
The most widely used incubation time:10-30 minThe most widely used incubation time:10-30 min
High concentration , high affinity , optimal pH,High concentration , high affinity , optimal pH,
Optimal ion strength ------ > shorter incubationOptimal ion strength ------ > shorter incubation
24 hr incubation for economy purpose ----- > allow higher 24 hr incubation for economy purpose ----- > allow higher
dilutionsdilutions

Incubation TimeIncubation Time
Low titer / low affinity Abs must be Low titer / low affinity Abs must be incubated for long periods in order incubated for long periods in order
to reach to reach equilibrium.equilibrium.
But nothing can be gained by prolonging primary Ab incubation But nothing can be gained by prolonging primary Ab incubation beyond the time at which the tissue is saturated with antibody.beyond the time at which the tissue is saturated with antibody.

Incubation TimeIncubation Time
Equilibrium is usually not reached Equilibrium is usually not reached before 20 min.before 20 min.
Consistent timing is important.Consistent timing is important.
Inconsistent timing leads to variations Inconsistent timing leads to variations in overall stain quality & intensity.in overall stain quality & intensity.

Incubation temperatureIncubation temperature
Equilibrium may achieved more quickly Equilibrium may achieved more quickly at 37C compare to RT.at 37C compare to RT.
Incubation at 37C allows higher dilution Incubation at 37C allows higher dilution + shorter incubation time ------ > + shorter incubation time ------ > consistency in incubation time becomes consistency in incubation time becomes even becomes more crucial.even becomes more crucial.
Incubation at 37C ----- > increase Incubation at 37C ----- > increase backgroundbackground

Incubation temperatureIncubation temperature
4C is used in combination with overnight or longer incubations.4C is used in combination with overnight or longer incubations.
Slides incubated for extended periods , or at 37C should be Slides incubated for extended periods , or at 37C should be placed in humidity chamber to prevent evaporation and drying placed in humidity chamber to prevent evaporation and drying of tissue sections.of tissue sections.
Tissue incubated at RT in a very dry or drafty environment will Tissue incubated at RT in a very dry or drafty environment will require the use of a humidity chamber.require the use of a humidity chamber.
Specimen requirementsSpecimen requirements Paraffin-embedded blocks vs. fresh Paraffin-embedded blocks vs. fresh
frozen vs. cytospin prep. cytological frozen vs. cytospin prep. cytological slides.slides.
Comprising the representative lesion. Not too small.Comprising the representative lesion. Not too small. Devoid of necrosis.Devoid of necrosis. Devoid of extensive hemorrhage.Devoid of extensive hemorrhage. Not too old Paraffin blocks < 3 years old.Not too old Paraffin blocks < 3 years old. Free from over fixation.Free from over fixation. Don’t treat with overheated paraffin during Don’t treat with overheated paraffin during
embedding & embedding &
processing.processing. Proper labeling. Proper labeling. Clear and precise IHC request.Clear and precise IHC request. Corresponding conventional pathology report.Corresponding conventional pathology report.

FixationFixation

FixationFixation
Each tissue has finite amount of AgEach tissue has finite amount of Ag
Most steps in IHC process destroy some of the AgsMost steps in IHC process destroy some of the Ags particularly : fixationparticularly : fixation

FixationFixation The purpose of fixation:The purpose of fixation:
1. To change protein structure in order to preserve them from 1. To change protein structure in order to preserve them from elution, elution, degradation,degradation,and other modificationsand other modifications
2.To preserve the position of the Ag ; 2.To preserve the position of the Ag ; Nuclear Nuclear CytoplasmicCytoplasmic Membrane-boundedMembrane-bounded
3.Preserve secondary and tertiary structue3.Preserve secondary and tertiary structue
4.To provide a target for Abs4.To provide a target for Abs

FixationFixation
Elution of ER protein from nucleus Elution of ER protein from nucleus to cytoplasmto cytoplasm
Elution of Cerb-b2 from membrane Elution of Cerb-b2 from membrane to cytoplasmto cytoplasm
Therefore diagnostically the stain is Therefore diagnostically the stain is useless.useless.
Poor or inadequate fixation
Incorrect interpretation

FixationFixationTissue :A Tissue :A
Neutral buffered formalin Neutral buffered formalin
ER as target Ag ER as target Ag
Monoclonal Ab clone E15 Monoclonal Ab clone E45RT
Result: negative Result: positive
Fixation may destroy specific epitopes thus may lead to improve two different reactions with two different monoclonal Abs

What is the solutionWhat is the solution??
Standardization of the fixative and Standardization of the fixative and fixation protocols would be an start.fixation protocols would be an start.

Fixation & Ag retrievalFixation & Ag retrieval
Aldehyde cross link after formalinfixation
AB Ag

There is no one universal fixativeThere is no one universal fixative that is ideal for that is ideal for the demonstration of all antigens. the demonstration of all antigens.
However, in general, However, in general, many antigens can be many antigens can be successfully demonstrated in formalin-fixedsuccessfully demonstrated in formalin-fixed paraffin-embedded tissue sections. paraffin-embedded tissue sections.
The discover and development of antigen The discover and development of antigen retrieval retrieval techniquestechniques further enhanced the use of formalin further enhanced the use of formalin as routine fixative for immunohistochemistry in as routine fixative for immunohistochemistry in many research laboratories. many research laboratories.

Some antigens will not survive even moderateSome antigens will not survive even moderate
amounts of amounts of aldehyde fixationaldehyde fixation..
Under this condition, tissues should be rapidly Under this condition, tissues should be rapidly fresh frozenfresh frozen in liquid nitrogen and cut with a in liquid nitrogen and cut with a cryostat without infiltrating with sucrose. cryostat without infiltrating with sucrose.
The sections should be kept frozen at -20 C or The sections should be kept frozen at -20 C or lower until lower until fixation with cold acetonefixation with cold acetone or alcohol. or alcohol.
After fixation, the sections can be processed After fixation, the sections can be processed using standard immunohistochemical staining using standard immunohistochemical staining protocolsprotocols

Ten percent neutral buffered formalin , Ten percent neutral buffered formalin , pH 7 pH 7
(10% NBF)(10% NBF) FreshFresh && Buffered to pH of 7.0-7.6Buffered to pH of 7.0-7.6
Formalin 40%Formalin 40% 100100 mLmL
Dibasic sodium Dibasic sodium phosphate, anhydrous, phosphate, anhydrous, Na2HPo4Na2HPo4
6.56.5 gg
Monobasic sodium Monobasic sodium phosphate, monohydrate, phosphate, monohydrate, KH2Po4KH2Po4
4.04.0 gg
DWDW 900900 mLmL

Most common fixativesMost common fixatives
a)a) 4% paraformaldehyde in 0.1M phosphate buffer 4% paraformaldehyde in 0.1M phosphate buffer
b)b) 2% paraformaldehyde with 0.2% picric acid in 0.1M 2% paraformaldehyde with 0.2% picric acid in 0.1M phosphate bufferphosphate buffer
c)c) PLP fixative: 4% paraformaldehyde, 0.2% periodate and 1.2% PLP fixative: 4% paraformaldehyde, 0.2% periodate and 1.2% lysine in 0.1M phosphate bufferlysine in 0.1M phosphate buffer
d)d) 4% paraformaldehyde with 0.05% glutaraldehyde (TEM 4% paraformaldehyde with 0.05% glutaraldehyde (TEM immunohistochemistry)immunohistochemistry)

Other aldehyde-based Other aldehyde-based fixativefixative
Glutaraldehyde 2%Glutaraldehyde 2%
Act similarly to 10% NBF and are used Act similarly to 10% NBF and are used much less frequentlymuch less frequently

Mercuric chloride fixativesMercuric chloride fixatives
Used in the pastUsed in the past
Mechanism: react with amino acid residues such as thiols, Mechanism: react with amino acid residues such as thiols, amino groups, imidazole, phosphate, and hydroxyl groups.amino groups, imidazole, phosphate, and hydroxyl groups.
Fixation time : is short , as a positive pointFixation time : is short , as a positive point
Highly toxic with special disposal procedures, as a negative Highly toxic with special disposal procedures, as a negative point point
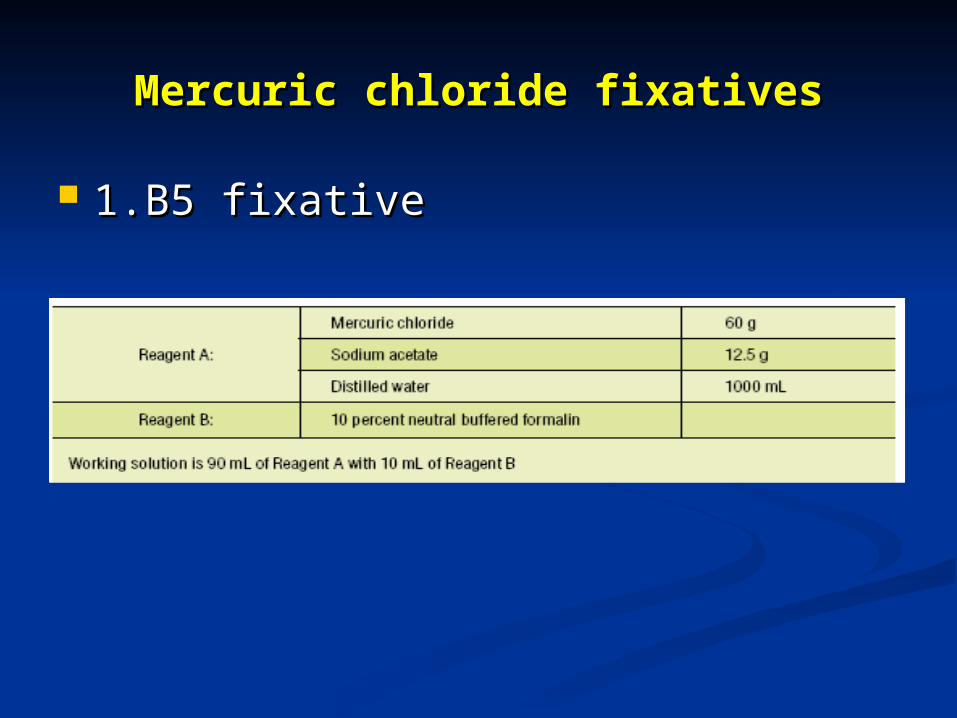
Mercuric chloride fixativesMercuric chloride fixatives
1.B5 fixative1.B5 fixative

Mercuric chloride fixativesMercuric chloride fixatives
2.Zenker’s fixative2.Zenker’s fixative

Alcoholic FixativesAlcoholic Fixatives
Carnoy’sCarnoy’s
In looking at lymphocytes using CD-In looking at lymphocytes using CD-specific markersspecific markers
In looking for immunoglubins such as In looking for immunoglubins such as IgG, IgA, IgMIgG, IgA, IgM

1. Tissue not dry out : onto moist absorbent paper ,in a covered 1. Tissue not dry out : onto moist absorbent paper ,in a covered containercontainer
2. Rapid delivery to the path. Lab.2. Rapid delivery to the path. Lab.
3. Trimming and cut for fixation3. Trimming and cut for fixation
4. Into blocks no more than 2 cm square by four mm thick4. Into blocks no more than 2 cm square by four mm thick
Tissue pretreatment
5. Thickness is important:5. Thickness is important:
1. Penetration: ideally fast1. Penetration: ideally fast2. Fixation : usually slow2. Fixation : usually slow
6. Optimum fixation time: 6-12 hr6. Optimum fixation time: 6-12 hr
7. Over fixation can pose problems: increased cross linking7. Over fixation can pose problems: increased cross linking
8. How to repair this damage?8. How to repair this damage?
Heating the fixed tissue in boiling water to 95 degrees for 15-20 minHeating the fixed tissue in boiling water to 95 degrees for 15-20 min
Tissue pretreatmentTissue pretreatment

Tissue & slide processingTissue & slide processing
Once the tissue is well-fixed, subsequent steps seem to have Once the tissue is well-fixed, subsequent steps seem to have little effect on antigen detection.little effect on antigen detection.
Variation in xylol processing, alcohol rehydration, wax Variation in xylol processing, alcohol rehydration, wax temperature, time or formulation, instrumentation used etc , temperature, time or formulation, instrumentation used etc , provide satisfactory results.provide satisfactory results.

Tissue & slide processingTissue & slide processing
No process should raise temperature No process should raise temperature to higher than 60C,to higher than 60C,
as this will cause severe loss of as this will cause severe loss of antigenicity that may not be antigenicity that may not be recoverable.recoverable.

Tissue & slide processingTissue & slide processing
Tissue fixation medium must be replaced by wax, Tissue fixation medium must be replaced by wax, generally done through a series of incubations in generally done through a series of incubations in increasing alcohol concentrations to 100 percent, increasing alcohol concentrations to 100 percent, followed by xylene and then hot wax.followed by xylene and then hot wax.
This is to provide stability of the tissue (wax) in order This is to provide stability of the tissue (wax) in order
to make cutting the sections easier.to make cutting the sections easier.

Tissue & slide processingTissue & slide processing
Appropriate thickness: 3-4 micronsAppropriate thickness: 3-4 microns No more than 5 micronsNo more than 5 microns

Tissue & slide processingTissue & slide processing
Commercially available slides with Commercially available slides with positive charge.positive charge.
Albumin coated slidesAlbumin coated slides Silane coated slidesSilane coated slides Poly-L-Lysine coated slidesPoly-L-Lysine coated slides Sections that are not flat and that Sections that are not flat and that
have non-adherent ridges likely will have non-adherent ridges likely will be digested or torn off the slide be digested or torn off the slide during immunostain.during immunostain.

Tissue & slide processing :Tissue & slide processing :De-waxing protocolDe-waxing protocol
A. Circle & label the specimen with a diamond pencilB. Place in 60C oven for 30 minutesC. Transfer immediately to a fresh xylene bath for three minutes.D. Repeat step C above with a second xylene bath.E. Place in a fresh bath of absolute alcohol for three minutes.F. Repeat step E above with a second bath of absolute alcohol.G. Place in a bath with 95 percent ethanol for three minutes.H. Repeat step G with the second 95 percent ethanol bath.I. Rinse under gently running water.J. Do not let dry, store in buffer; begin required Ag treatment or immunostaining
Note: 50 slides per 250 mL of xylene is the limit before the xyleneIs no longer effective and residual wax begins causing artifacts in the final stained tissue.

ProcedureProcedure
1.3 micron slide sections1.3 micron slide sections 37c37c 48hr48hr2.Xylol2.Xylol RTRT 15min15min3.Xylol3.Xylol RTRT 15min15min4.Absolute alcohol4.Absolute alcohol RTRT 15min15min5.96 alcohol5.96 alcohol RTRT 15min15min6.70 alcohol6.70 alcohol RTRT 15min15min7.DW7.DW RT RT rinse/*2/5minrinse/*2/5min8.3%H2O2/methanol v/v8.3%H2O2/methanol v/v RTRT 30min30min9.DW9.DW RT RT rinse/*2/5minrinse/*2/5min10.Citrate buffer pH=610.Citrate buffer pH=6 microwavemicrowave 14min14min11.Cooling11.Cooling RTRT graduallygradually

ProcedureProcedure
12.PBS12.PBS RTRT rinse/*2/5 minrinse/*2/5 min13.Protein block13.Protein block RTRT 10min10min14.114.1stst Ab Ab RTRT 10-60min10-60min15.PBS15.PBS RTRT rinse/*2/5 minrinse/*2/5 min16.216.2ndnd Ab Ab RTRT 30min30min17.PBS17.PBS RTRT rinse/*2/5 minrinse/*2/5 min18.Detection system18.Detection system RTRT 30min30min19.PBS19.PBS RTRT rinse/*2/5 minrinse/*2/5 min20.Chromogen DAB20.Chromogen DAB RTRT 10min10min21.DW21.DW RTRT rinserinse22.Hematoxyline22.Hematoxyline RTRT 3 dips (10 sec)3 dips (10 sec)

Citrate Buffer pH=6.0Citrate Buffer pH=6.0
2.1 gr2.1 gr acid citric monohydarteacid citric monohydarte
900mL900mL DWDW
13mL13mL NaOH 2 normalNaOH 2 normal
Up to 1000mLUp to 1000mL

PBS 10xPBS 10x
Na2HPo4Na2HPo4 11.5 gr11.5 gr
NaClNaCl 80 gr80 gr
KCLKCL 2 gr2 gr
KH2Po4KH2Po4 3.4 gr3.4 gr
Up to Up to 1000mL1000mL

Antigen Retrieval ProtocolsAntigen Retrieval Protocols
Break the protein cross-links formed by Break the protein cross-links formed by formalin fixation and thereby uncover formalin fixation and thereby uncover hidden antigenic siteshidden antigenic sites..
Heat Induced Epitope Retrieval (HIER)Heat Induced Epitope Retrieval (HIER)Hydrochloric Acid Method (pH 1)Hydrochloric Acid Method (pH 1)Formic Acid Method (pH 2)Formic Acid Method (pH 2)Citrate Buffer Method (pH 6)Citrate Buffer Method (pH 6)Citrate-EDTA Buffer Method (pH 6.2)Citrate-EDTA Buffer Method (pH 6.2)EDTA Method (pH 8)EDTA Method (pH 8)TrisTris-EDTA Method (pH 9)-EDTA Method (pH 9)TBS Method (pH 9)TBS Method (pH 9)TrisTris Buffer Method (pH 10) Buffer Method (pH 10)

Heat Induced Epitope Retrieval (HIER)Heat Induced Epitope Retrieval (HIER)
Pressure cookerPressure cooker AutoclaveAutoclave MicrowaveMicrowave Ag retrieval solutions:Ag retrieval solutions:
0.01 M citrate pH=60.01 M citrate pH=6 10x10x 1 mM EDTA1 mM EDTA 10x10x 20 mM Tris/0.65 mM EDTA/0.0005% 20 mM Tris/0.65 mM EDTA/0.0005%
Tween 20 pH=9Tween 20 pH=9 10x10x

Proteolytic Induced Epitope Retrieval Proteolytic Induced Epitope Retrieval (PIER)(PIER)
ProteinaseProteinase K Method K Method
TrypsinTrypsin Method Method
Pepsin MethodPepsin Method
PronasePronase Method Method
Protease MethodProtease MethodFrozen Section Epitope RetrievalFrozen Section Epitope Retrieval
SDS MethodSDS Method
Heating En Bloc MethodHeating En Bloc Method

BlockingBlocking::
The main cause of The main cause of non-specific non-specific backgroundbackground staining is non- staining is non-immunological binding of the specific immunological binding of the specific immune sera by immune sera by hydrophobic and hydrophobic and electrostaticelectrostatic forces to certain sites within forces to certain sites within tissue sections. tissue sections.
This form of background staining is This form of background staining is usually usually uniformuniform and can be reduced by and can be reduced by blockingblocking those sites with those sites with normal serumnormal serum..

BlockingBlocking::
Background staining may be specific or non-Background staining may be specific or non-specific. specific.
Inadequate or delayed fixationInadequate or delayed fixation may give rise to may give rise to false positive results due to the passive uptake of false positive results due to the passive uptake of serum protein and diffusion of the antigen. serum protein and diffusion of the antigen.
Such false positives are common Such false positives are common in the center of in the center of large tissue blockslarge tissue blocks or throughout tissues in or throughout tissues in which fixation was delayed. which fixation was delayed.

Non-immunological bindingNon-immunological bindingInadequate or delayed fixation Inadequate or delayed fixation
common in the center of large tissue blockscommon in the center of large tissue blocks
binding of the specific immune sera by binding of the specific immune sera by hydrophobic and electrostatichydrophobic and electrostatic
non-specific backgroundnon-specific background staining is staining is non-immunological bindingnon-immunological binding
usually usually uniformuniform and can be reduced by and can be reduced by
blocking those sites with blocking those sites with normal serumnormal serum..

BlockingBlocking::
Antibodies, specially Antibodies, specially polycolonal polycolonal antibodiesantibodies, are sometimes , are sometimes contaminated with other antibodies contaminated with other antibodies due to impure antigen used to due to impure antigen used to immunize the host animalimmunize the host animal . .

Immunological bindingImmunological binding
impure antigen used to immunize the host animalimpure antigen used to immunize the host animal
contaminated contaminated polyclonal antibodiespolyclonal antibodies with other antibodieswith other antibodies
Non-specific Immunological bindingNon-specific Immunological binding

Non-immunological Non-immunological backgroundbackground
Peroxidase BlockPeroxidase BlockEndogenous peroxidaseEndogenous peroxidase activity is found in many tissues and can activity is found in many tissues and can be detected by reacting fixed tissue sections with DAB be detected by reacting fixed tissue sections with DAB substratesubstrate . .
The solution for eliminating endogenous peroxidase activity is by The solution for eliminating endogenous peroxidase activity is by the pretreatment of the tissue section with the pretreatment of the tissue section with hydrogen peroxidehydrogen peroxide prior to incubation of primary antibodyprior to incubation of primary antibody..

30% H2O2 ------------------------- 2 ml 30% H2O2 ------------------------- 2 ml Methanol --------------------------- 18 mlMethanol --------------------------- 18 ml Mix well and store at 4 ºC.Mix well and store at 4 ºC. Block sections for 20-30 minutes after primary Block sections for 20-30 minutes after primary antibody incubation.antibody incubation. Note: The solution must be fresh.Note: The solution must be fresh.
Peroxidase Blocking Solution (3% H2O2 in Methanol)Peroxidase Blocking Solution (3% H2O2 in Methanol)

Endogenous alkaline phosphatase (AP) Endogenous alkaline phosphatase (AP) activityactivity
Many tissues also contain Many tissues also contain endogenous endogenous alkaline phosphatase (AP) activityalkaline phosphatase (AP) activity and should be blocked by the and should be blocked by the pretreatment of the tissue section pretreatment of the tissue section with with levamisolelevamisole if using AP as a if using AP as a labellabel..

BlockingBlocking::
Some tissues such as liver and Some tissues such as liver and kidney have kidney have endogenous biotinendogenous biotin..
To avoid unwanted avidin binding to To avoid unwanted avidin binding to endogenous biotin if using biotin-endogenous biotin if using biotin-avidin detection system, a step is avidin detection system, a step is necessary for these tissues by the necessary for these tissues by the pretreatment of pretreatment of unconjugated avidin unconjugated avidin which is then saturated with biotin.which is then saturated with biotin.

Avidin 0.001% in PBSAvidin 0.001% in PBSBiotin 0.001% in PBSBiotin 0.001% in PBSStore these blocking solution at 4 ºC. Store these blocking solution at 4 ºC. Incubate sections for 10-15 min each and rinse with Incubate sections for 10-15 min each and rinse with PBS between steps. Recommended to block before PBS between steps. Recommended to block before primary antibody incubation.primary antibody incubation.
Avidin/Biotin BlockAvidin/Biotin Block

ControlsControls::
Positive controlPositive control
To use the tissue of known positive as a controlTo use the tissue of known positive as a control . .
If the positive control tissue showed negative staining, the If the positive control tissue showed negative staining, the protocol or procedure needs to be checked until a good protocol or procedure needs to be checked until a good positive staining is obtainedpositive staining is obtained..
ControlsControls::
Negative controlNegative control is to test for the specificity of an antibody is to test for the specificity of an antibody involvedinvolved . .
FirstFirst, no staining must be shown , no staining must be shown when omitting primary antibodywhen omitting primary antibody or replacing an specific primary antibody with normal serum or replacing an specific primary antibody with normal serum (must be the same species as primary antibody)(must be the same species as primary antibody) . .
This control is easy to achieve and can be used routinely in This control is easy to achieve and can be used routinely in immunohistochemical stainingimmunohistochemical staining..

ControlsControls::
SecondSecond, the staining must be inhibited by adsorption of a primary , the staining must be inhibited by adsorption of a primary antibody with the purified antigen prior to its use, but not by antibody with the purified antigen prior to its use, but not by adsorption with other related or unrelated antigensadsorption with other related or unrelated antigens . .
This type of negative control is ideal and necessary in the This type of negative control is ideal and necessary in the characterization and evaluation of new antibodies but it is characterization and evaluation of new antibodies but it is sometimes difficult to obtain the purified antigen, therefore it sometimes difficult to obtain the purified antigen, therefore it is rarely used routinely in immunohistochemical stainingis rarely used routinely in immunohistochemical staining..

Direct MethodDirect Method::
Direct method is one step staining method, and involves a labeled Direct method is one step staining method, and involves a labeled antibody (i.e. FITC conjugated antiserum) reacting directly antibody (i.e. FITC conjugated antiserum) reacting directly with the antigen in tissue sections:DFAwith the antigen in tissue sections:DFA
This technique utilizes only one antibody and the procedure is This technique utilizes only one antibody and the procedure is short and quick. However, it is insensitive due to little signal short and quick. However, it is insensitive due to little signal amplification and rarely used since the introduction of indirect amplification and rarely used since the introduction of indirect methodmethod..

Indirect MethodIndirect Method::
Indirect method involves an unlabeled primary antibody (first Indirect method involves an unlabeled primary antibody (first layer) which react with tissue antigenlayer) which react with tissue antigen,,
and a labeled secondary antibody (second layer) react with and a labeled secondary antibody (second layer) react with primary antibody (Note: The secondary antibody must be primary antibody (Note: The secondary antibody must be against the IgG of the animal species in which the primary against the IgG of the animal species in which the primary antibody has been raised)antibody has been raised)..

Indirect MethodIndirect Method::
This method is more sensitive due to signal amplification through This method is more sensitive due to signal amplification through several secondary antibody reactions with different antigenic several secondary antibody reactions with different antigenic sites on the primary antibodysites on the primary antibody . .
In addition, it is also economy since one labeled second layer In addition, it is also economy since one labeled second layer antibody can be used with many first layer antibodies (raised antibody can be used with many first layer antibodies (raised from the same animal species) to different antigensfrom the same animal species) to different antigens . .

PAP Method (peroxidase anti-PAP Method (peroxidase anti-peroxidase method)peroxidase method)Three layer methodThree layer method
Rabbit antibody to peroxidase, coupled with peroxidase
Unconjugated goat anti-rabbit Unconjugated goat anti-rabbit gaba-globulingaba-globulin

PAP Method (peroxidase anti-PAP Method (peroxidase anti-peroxidase method)peroxidase method)
The sensitivity is about 100 to 1000 times higherThe sensitivity is about 100 to 1000 times higher since the since the peroxidase molecule is not chemically conjugated to the anti peroxidase molecule is not chemically conjugated to the anti IgG but immunologically bound, and loses none of its enzyme IgG but immunologically bound, and loses none of its enzyme activityactivity . .
It also allows for much higher dilutionIt also allows for much higher dilution of the primary antibody,of the primary antibody, thus eliminating many of the unwanted antibodies and thus eliminating many of the unwanted antibodies and reducing non-specific background stainingreducing non-specific background staining..

Avidin-Biotin Complex (ABC) Avidin-Biotin Complex (ABC) MethodMethod
Is standard IHC methodIs standard IHC method..
AvidinAvidin, a large glycoprotein, can be labeled with peroxidase or , a large glycoprotein, can be labeled with peroxidase or fluorescein and has a very high affinity for biotinfluorescein and has a very high affinity for biotin . .
BiotinBiotin, a low molecular weight vitamin, can be conjugated to a , a low molecular weight vitamin, can be conjugated to a variety of biological molecules such as antibodiesvariety of biological molecules such as antibodies . .

Avidin-Biotin Complex (ABC) Avidin-Biotin Complex (ABC) MethodMethod
Three layers method.Three layers method.
1.The first layer is unlabeled primary antibody. 1.The first layer is unlabeled primary antibody.
2.The second layer is biotinylated secondary antibody. 2.The second layer is biotinylated secondary antibody.
3.The third layer is a complex of avidin-biotin peroxidase. 3.The third layer is a complex of avidin-biotin peroxidase.
4.The peroxidase is then developed by the DAB or other 4.The peroxidase is then developed by the DAB or other substrate to produce different colorimetric end products.substrate to produce different colorimetric end products.

Labeled StreptAvidin Biotin (LSAB) Labeled StreptAvidin Biotin (LSAB) MethodMethod
StreptavidinStreptavidin, derived from streptococcus avidini, is a recent , derived from streptococcus avidini, is a recent innovation for substitution of avidininnovation for substitution of avidin..
The streptavidin molecule is uncharged relative to animal The streptavidin molecule is uncharged relative to animal tissue, unlike avidin which has an isoelectric point of 10, tissue, unlike avidin which has an isoelectric point of 10, and therefore electrostatic binding to tissue is eliminatedand therefore electrostatic binding to tissue is eliminated . .
In addition, streptavidin does not contain carbohydrate In addition, streptavidin does not contain carbohydrate groups which might bind to tissue lectins, resulting in groups which might bind to tissue lectins, resulting in some background stainingsome background staining . .

Labeled StreptAvidin Biotin Labeled StreptAvidin Biotin (LSAB) Method(LSAB) Method
11..The first layer is unlabeled primary antibodyThe first layer is unlabeled primary antibody . .22..The second layer is biotinylated secondary antibodyThe second layer is biotinylated secondary antibody . .
33..The third layer is Enzyme-Streptavidin conjugates (HRP-Streptavidin The third layer is Enzyme-Streptavidin conjugates (HRP-Streptavidin or AP-Streptavidin)or AP-Streptavidin)
A recent report suggests that LSAB method is about 5 to A recent report suggests that LSAB method is about 5 to 10 times more sensitive than standard ABC method10 times more sensitive than standard ABC method..

Polymeric MethodsPolymeric Methods::

Polymeric MethodsPolymeric Methods::
Dextran polymer technologyDextran polymer technology . .
Binding of a large number of enzyme molecules (horseradish Binding of a large number of enzyme molecules (horseradish peroxidase or alkaline phosphatase) to a secondary antibody peroxidase or alkaline phosphatase) to a secondary antibody via the dextran backbonevia the dextran backbone . .
The benefits are many, includingThe benefits are many, including increased sensitivity, increased sensitivity, minimized non-specific background staining minimized non-specific background staining reduction in the total number of assay steps reduction in the total number of assay steps

Polymeric MethodsPolymeric Methods::
ProcedureProcedure::
i) Application of primary antibody; i) Application of primary antibody; ii) Application of enzyme labeled polymer; ii) Application of enzyme labeled polymer; iii) Application of the substrate chromogen. iii) Application of the substrate chromogen.
EnVision+ was developed after EnVision to provide increased EnVision+ was developed after EnVision to provide increased sensitivity.sensitivity.
Chromogen Substrate Chromogen Substrate SolutionsSolutions
DAB-DAB-PeroxidasePeroxidase Substrate Solution (Brown) Substrate Solution (Brown)DAB-Peroxidase Substrate Soluiton (Gray)DAB-Peroxidase Substrate Soluiton (Gray)DAB-DAB-PeroxidasePeroxidase Substrate Solution (Black) Substrate Solution (Black)DAB-DAB-PeroxidasePeroxidase Substrate Solution (Blue) Substrate Solution (Blue)AEC-AEC-PeroxidasePeroxidase Substrate Solution (Red) Substrate Solution (Red)BDHC-BDHC-PeroxidasePeroxidase Substrate Solution (Blue) Substrate Solution (Blue)TMB-TMB-PeroxidasePeroxidase Substrate Solution (Blue) Substrate Solution (Blue)New New FuchsinFuchsin Alkaline Alkaline PhosphatasePhosphatase Substrate Substrate SulutionSulution (Red) (Red)BCIP/NBT Alkaline BCIP/NBT Alkaline PhosphatasePhosphatase Substrate Solution (Blue) Substrate Solution (Blue)

Protocol for DAB Peroxidase Substrate Protocol for DAB Peroxidase Substrate SolutionSolution
DAB Peroxidase Substrate Solution – BrownDAB Peroxidase Substrate Solution – BrownFinal DilutionFinal Dilution::
0.05%0.05% DAB - 0.015% H2O2 in 0.01M PBS, pH 7.2DAB - 0.015% H2O2 in 0.01M PBS, pH 7.2 Stock SolutionsStock Solutions::
1%1% DAB (20x) in Distilled WaterDAB (20x) in Distilled Water::
Add 0.1g of DAB (3,3’-diaminobenzidine Add 0.1g of DAB (3,3’-diaminobenzidine tetrahydrochloride, Sigma) in 10 ml distilled water. Add tetrahydrochloride, Sigma) in 10 ml distilled water. Add 10N HCl 3-5 drops and solution turns light brown color. 10N HCl 3-5 drops and solution turns light brown color. Shake for 10 minutes and DAB should dissolve completely. Shake for 10 minutes and DAB should dissolve completely. Aliquot and store at –20 Aliquot and store at –20 CC . .
0.3%0.3% H2O2 (20x) in distilled waterH2O2 (20x) in distilled water::
Add 100ul of 30% H2O2 in 10 ml distilled water and mix Add 100ul of 30% H2O2 in 10 ml distilled water and mix well. Store at 4 well. Store at 4 C or aliquot and store at –20 C or aliquot and store at –20 CC . .

Counterstain SolutionsCounterstain Solutions
Gill's Gill's HematoxylinHematoxylin Solution (Blue) Solution (Blue)
Mayer's Mayer's HematoxylinHematoxylin Solution (Blue) Solution (Blue)
Nuclear Fast Red Solution (Red)Nuclear Fast Red Solution (Red)
Methyl Green Solution (Green)Methyl Green Solution (Green)
PI PI CounterstainCounterstain Solution (Fluorescent Red) Solution (Fluorescent Red)
DAPI DAPI CounterstainCounterstain Solution (Fluorescent Blue) Solution (Fluorescent Blue)

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 155

TO APPLY IHC OR ICC FORTO APPLY IHC OR ICC FOR ?…?…
1.Diagnostic purpose.1.Diagnostic purpose.
2.Prognostic purpose2.Prognostic purpose
3.Therapeutic purpose3.Therapeutic purpose
4.Preventive purpose?4.Preventive purpose?

Applications of IHCApplications of IHC Diagnostic purposeDiagnostic purpose::

Applications of IHCApplications of IHC Diagnostic purpose:Diagnostic purpose:
IHC profile for metastatic carcinoma of unknown IHC profile for metastatic carcinoma of unknown originorigin
FemaleFemale MaleMale
ER/PRER/PR PSAPSA
CK 7CK 7 CK 7CK 7
CK 8CK 8 CK 8CK 8
CK 20CK 20 CK 20CK 20
CD X2CD X2 CD X2CD X2
CEACEA CEACEA
TTF 1TTF 1 TTF 1TTF 1

Diagnostic purpose of Diagnostic purpose of IHCIHC
CK CK 77
CK CK 88
CK CK 2020
DxDx
++ ++ -- Follicular Follicular adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Adenocarcinoma ,PancreasAdenocarcinoma ,Pancreas
-- ++ ++ Hepatocellualr carcinomaHepatocellualr carcinoma
-- ++ -- Squamous cell carcinoma Squamous cell carcinoma CK CK 5/65/6
-- -- -- Thymoma Thymoma CK CK 5/65/6

Diagnostic purpose of Diagnostic purpose of IHCIHC
CK CK 88
CK CK 1818
DxDx
++ ++ Follicular Follicular adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Papillary Papillary adenocarcinoma ,Thyroidadenocarcinoma ,Thyroid
Adenocarcinoma,PancreasAdenocarcinoma,Pancreas
Hepatocellualr carcinomaHepatocellualr carcinoma
++ -- TrichoepitheliomaTrichoepithelioma
-- ++ MeningiomaMeningioma
Collectind duct carcinomaCollectind duct carcinoma
-- -- ThymomaThymoma
Adenocarcinoma , AmpullaryAdenocarcinoma , Ampullary

Applications of IHCApplications of IHC
Diagnostic purpose:Diagnostic purpose:an examplean example
IHC profile for prostatic carcinomaIHC profile for prostatic carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 162
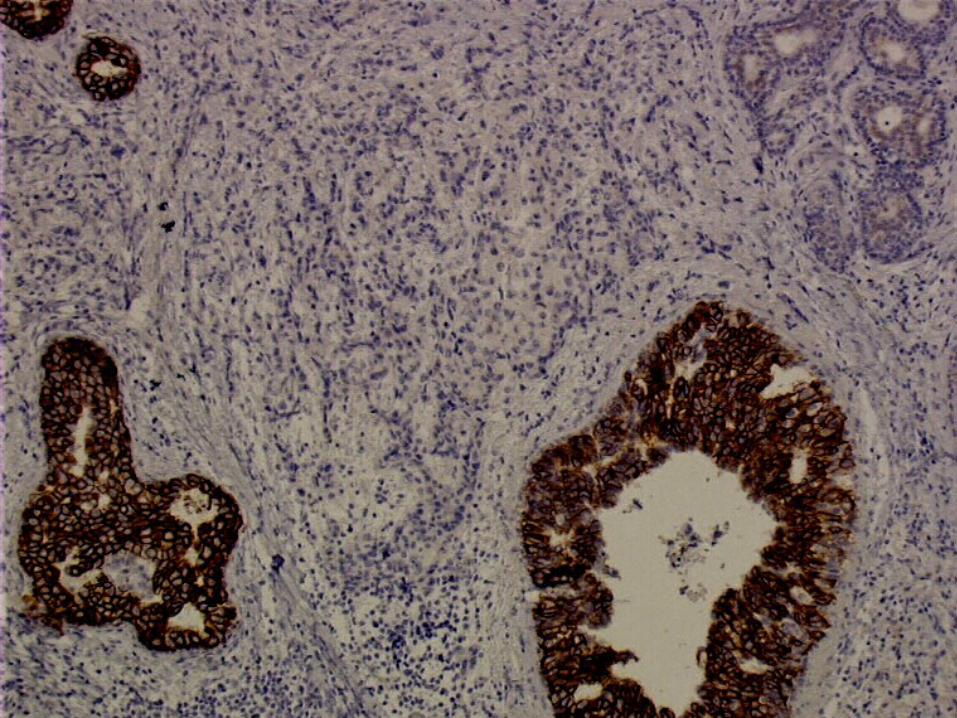
IHC in prostate CancerIHC in prostate Cancer
Indications:Indications:1- Distinction of Benign from Malignant1- Distinction of Benign from Malignant
• High molecular weight cytokeratin (34High molecular weight cytokeratin (34E12, CK5/6)E12, CK5/6)
– Negative cytoplasmic marker (in basal cells)Negative cytoplasmic marker (in basal cells)• P63P63
– Negative nuclear stain (in basal cells)Negative nuclear stain (in basal cells)• AMACR (P504S)AMACR (P504S)
– Positive cytoplasmic marker (in tumor cells)Positive cytoplasmic marker (in tumor cells)– Also positive in HGPIN, 31% of Bladder Ca. & Also positive in HGPIN, 31% of Bladder Ca. &
70% of Colorectal Ca.70% of Colorectal Ca.

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 163
HMW-CK (34HMW-CK (34E12)E12)
Normal Glands
Negative in Carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 164
AMACR AMACR (P504S) stain (P504S) stain in Carcinomain Carcinoma

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 165
P63 / AMACR P63 / AMACR cocktailcocktail
Increasing IHC resolution:

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 166
3434E12 / P63 / AMACR E12 / P63 / AMACR 2-chromogen cocktail2-chromogen cocktail
Increasing IHC resolution:

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 167
IHC in prostate Cancer IHC in prostate Cancer (Cont.)(Cont.)
Indications:Indications:
2- Differential Dx from urothelial carcinoma:2- Differential Dx from urothelial carcinoma:
PSA PSAP 34PSA PSAP 34E12 Leu7 CK5/6E12 Leu7 CK5/6
Prostate Ca + + – + -Prostate Ca + + – + -
Urothelial CaUrothelial Ca – – – – + + – +– +

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 168
IHC in prostate Cancer IHC in prostate Cancer (Cont.)(Cont.)
Indications:Indications:
3- Differential Dx in metastatic carcinoma:3- Differential Dx in metastatic carcinoma:
Bone Tumor:
PSA stain

Applications of IHCApplications of IHCPrognostic purposePrognostic purpose
in breast carcinomain breast carcinoma Poor prognostic Poor prognostic
markersmarkersGood prognostic Good prognostic
markersmarkers
ERER(-)(-) ERER(+)(+)
PRPR(-)(-) PRPR(+)(+)
pS2pS2(-)(-) pS2pS2(+)(+)
Her-2 (3+)Her-2 (3+) Her-2 (0/1+)Her-2 (0/1+)
Cathepsin DCathepsin D(+)(+) Cathepsin DCathepsin D(-)(-)
P 53 >10%P 53 >10% P 53 <10%P 53 <10%
EFGREFGR(+) (+) EGFREGFR( - )( - )
Ki-67>23%Ki-67>23% Ki-67<11%Ki-67<11%

Prognostic purpose of Prognostic purpose of IHCIHC
ER/PR/ER/PR/pS2pS2:: pS2 :pS2 : Cystein-rich peptide induced by estrogen Cystein-rich peptide induced by estrogen
secreted from breast cells.secreted from breast cells.
pS2 expression has been found to be associated with pS2 expression has been found to be associated with longer overall & disease free survival.longer overall & disease free survival.
ER +/ PR +/ ER +/ PR +/ pS2 +pS2 + : 85% to 97% have good : 85% to 97% have good prognosisprognosis
ER +/ PR +/ ER +/ PR +/ pS2 -pS2 - : only 50% to 54% have good : only 50% to 54% have good prognosis.prognosis.

How to Assess an IHC immunostain?
reproducibility
Inter-observer variation
inconsistency
Clinical data

An example
Assessment of Her2 status in breast cancer

Published guidelines (ASCO)
Her2 over-expression should be evaluated on every primary breast cancer either at the time of diagnosis or at the time of recurrence.
J Clin Oncol 19:1865-1878, 2001

Importance of getting it right• Poorer prognosis if HER2 positive
• Role in the selection of the most appropriate adjuvant therapy
• Herceptin® improves survival if HER2 positive, but not HER2 negative– false negatives
• deny life-extending treatment– false positives
• false hope
• complications & cost of the treatment

HER2 technical approaches• Gene amplification
– Southern or dot (slot) blotting
– quantitative PCR
– FISH/CISH
• mRNA over-expression– Northern blotting
– quantitative RT-PCR
• Protein over-expression– immunohistochemistry
– Western blotting
– Elisa

POINT MUTATIONS
Point Mutation
C-proto -onc C-onc
m-RNA
C-onc protein over production with Increased activity
M-RNA overexpression

IHCvs
FISH
• Fast• Cheap• Easy• False-negative rate• False-positive rate• Subjective interpretation• Difficult to standardise
• Long• Expensive• Difficult• Accurate (#signals)
• Theoretically does not identify pts with overexpression without gene amplific
• Standardised

IHC/FISH concordance
0 1+ 2+ 3+
FISH - 207 28 67 21
FISH + 7 2 21 176
3% 7% 24% 89%
Overall concordance: 82%
Mass R et al.: Proc ASCO 2000

Her2 testing algorithm
Patient tumour sample
IHC FISH
2+ 3+ + –
Retest withFISH
Herceptin®
therapyHerceptin®
therapy
– +
Herceptin®
therapy

© 2003 By Default!
A Free sample background from www.powerpointbackgrounds.com
Slide 180
How to interpret?How to interpret?
1.Intimacy with pattern of staining:1.Intimacy with pattern of staining:
NuclearNuclear ERER PRPR P 53P 53 Ki 67Ki 67
MembranousMembranous Her 2Her 2 EGFREGFR CD CD 2020
CD CD 4545
CytoplasmicCytoplasmic CKCK VimeVimentinntin
DesmDesminin
NSENSE SMASMA HMB-HMB-4545
CytonuclearCytonuclear S100S100 CalretCalretinininin
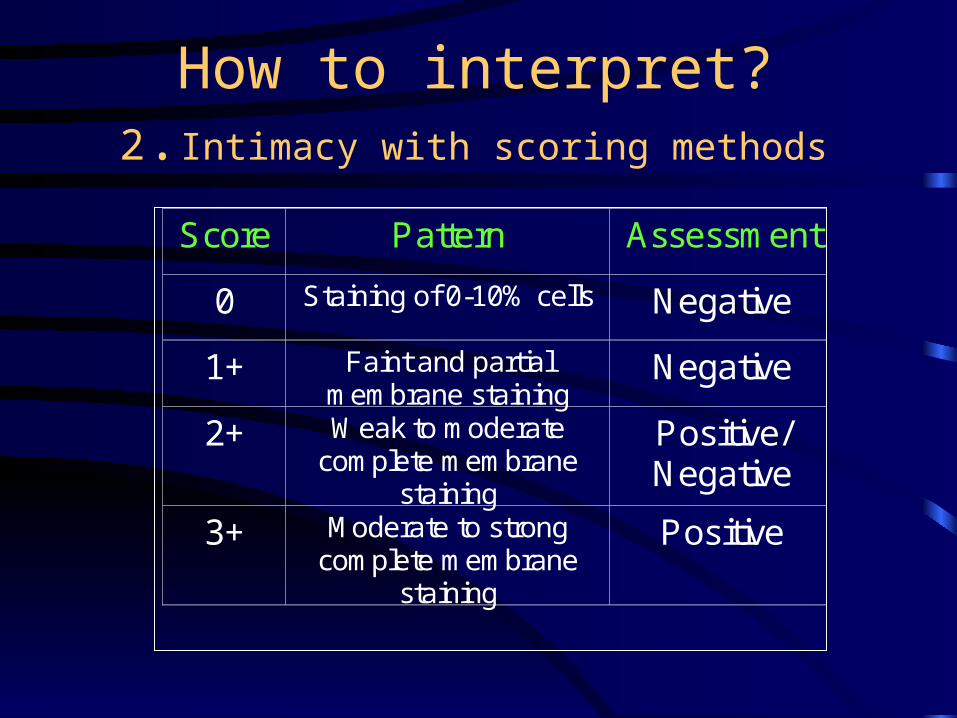
How to interpret? 2.Intimacy with scoring methods
Score Pattern Assessment
0 Staining of 0-10% cells Negative
1+ Faint and partial membrane staining
Negative
2+ Weak to moderate complete membrane
staining
Positive/ Negative
3+ Moderate to strong complete membrane
staining
Positive

Proficiency surveys of HER2 testing
2001 College of American Pathology IHC survey
• A breast tumor sample unreactive by IHC and FISH was distributed to 415 laboratories– 72% reported negative results
– 28% reported immunoreactivity
– 9% reported 2+ or 3+ scoresConclusion
Any HER2 assay performed at a non-reference laboratory (<100 cases/month) will require validation
at a reference laboratory

Potential for misdiagnosis (IHC)
• Antibodies (>28 commercially available)
• Technical performance
• Interpretation– scoring– artifacts

Common problems in HER2 IHC
• Underestimation of expression:– (over)fixation in NBF– poor antigen retrieval (unmasking)– choice of antibodies
• Overestimation– alcoholic (post)fixation (check normal
cells!)• Cytoplasmic staining

Who can interpret an IHC?

Normal lobule
3+ breast carcinoma

Lobular cancerization

2+ breast carcinoma

2+ breast carcinoma?

Normal lobule

Cytoplasmic staining

What to do?• Central Reference or large local laboratories
– high number of cases (>250 cases/year* or >100 cases/months [NSABP])
– quality assurance controls (internal and external)– automated IHC – high level of training (technique/interpretation)
• Small laboratories (<250 cases/yr or <100 cases/mos) – do not do it– send to larger laboratories
*Ellis I, et al: J Clin Pathol 2004
… but• There are labs capable of performing
quality testing with lower volumes• A high test volume does not ensure
an accurate test result• If an individual lab can properly
validate an assay and perform acceptably in an external validation, then it should be permitted to offer the test
Hsi ED & Tubbs RR: JCP 2004

Applications of IHCApplications of IHC therapeutic purposetherapeutic purpose Chemotherapy in breast Chemotherapy in breast
carcinomacarcinomaERER(+) (+) PRPR(+) (+) Tamoxifen / FemaraTamoxifen / Femara
ERER(-) (-) PRPR(+) (+) Tamoxifen / FemaraTamoxifen / Femara
ERER(+) (+) PRPR(-) (-) Tamoxifen / FemaraTamoxifen / Femara
Her-2 Her-2 psoitivpsoitiv
ee
TrastazumabTrastazumab
))HerceptinHerceptin((
Cost :300 000 000 Cost :300 000 000 RialsRials
Her-2 Her-2 negatinegati
veve
-- --

Applications Of IHCApplications Of IHC Therapeutic purpose: PharmaDx AbsTherapeutic purpose: PharmaDx Abs Chemotherapy in breast carcinomaChemotherapy in breast carcinoma ER - / PR - / Her-2 -ER - / PR - / Her-2 -
Triple negative breast Triple negative breast carcinomacarcinoma
Treatment is completely different:Treatment is completely different:
CisplatinCisplatin