an intro to the world of forensics · (hbo‐ autopsy), dr. henry lee, dead men ... 1. peden m,...
TRANSCRIPT

AnIntrototheWorldofForensics
MayJenAmolat‐Apiado,MD,MFM,MPHForensicPathologist,ForensicScienceAdjunct

FORENSICSDEFINED• Forensic‐fromforensis‐todebate/argue,relatedtothelaw,akaforum
• Forensicscience‐anyscienceappliedtolegalissues
• Forensicmedicine‐medicalknowledgeappliedtolegalissues(appliedtotheliving;forensicnursing;forensicpathology;forensicpsychiatry)
• Differentdisciplineswithintheforensicssciences‐criminalisOcs(hair,fiber,physical/biologicalevidence),quesOoneddocuments,anthropology,pathology,odontology,profiling,digitalmedia,engineering,wildlifeforensics
VALUEOFFORENSICSCIENCE

CRIMESCENERECONSTRUCTION FORENSICSCIENTIST(S)
MEDICALEXAMINER
INVESTIGATOR/POLICE

GENERALEDUCATIONALTRACK
• Bachelors• (Masters• PhD/terminaldegree• Postgradwork/forensicsubspecializaOon)• MembershipsinsocieOes• (Board‐cerOficaOoninparOcularfield• RelevantpublicaOons)• Onthejobexperience

FORENSIC‐RELATEDCAREERS• INSCHOOLSForensiceducators‐K‐12teachers,college/gradschool
• WITHPOLICE:Evidence/crimescenetechnicians,police(policeacademy)
• INCRIMELABS:BS;orMSinForensicScienceorPhDwww.aafs.org,www.criminalists.org
• INCOURT:lawyers:JD,passingthebar

CAREERS2• InMEDICALEXAMINERSOFFICEHAS:MDtrainedinanatomicpathologyandforensicpathology(medicalexaminer)
• PhD‐levelandboard‐cerOfiedforensictoxicologists‐detecOonofchemicalsubstancesinpostmortemorlivingsample
• Morguetechnicians‐anatomy(biology/funeraldirectorbackground)furthertraininginphotography,radiology
• Supportstaff‐secretaries/administrators‐asset;BA/BS/AA/AS
• InvesOgators‐nursing,EMS,Physicianassistant,morgue/funeraldirectorslatertrainedandcerOfiedbyAMERICANBOARDOFMEDICOLEGALDEATHINVESTIGATORS– OPTIONALBUTMOSTWELCOME:Counselors‐PsyD,PhDorMSWforbereaved/PTSD/violent;EPIDEMIOLOGISTS;MS,PHDorMPH
CAREERS3• INHOSPITALS:Forensicnurses;RNwithSANE+forensicmedicine
training(www.iafne.org);forensicphysicians(inUKcalledpolicesurgeons,employedbypolice)
• FORENSICODONTOLOGY‐bitemark,ID,DDSdegree,www.abfo.org
• FORENSICBIOLOGISTS/ENTOMOLOGISTS/DNASCIENTISTS‐BS,MA,PhD
• CRIMINALPROFILING‐FBIbehavioralscienceunit;forensicpsychologists,MA,PhD,alsowww.forensic‐science.org
• WILDLIFEFORENSICS‐USFishandWildlife,criminalistsalsovetswithforensictraining/experiencewww.lab.fws.gov

CAREERS4
• INNGOsvsWARCRIMES:Forensicanthropology(BS(4),MA(2),PhD(4‐6)pluspostgraduatework)www.theabfa.org
• INOWNCOMPANIES:Digital/computerforensics,quesOoneddocuments‐‐AmericanSocietyofQuesOonedExaminerswww.asqde.org,AmericanBoardofForensicDocumentExaminerswww.abfde.org
• INACADEMIAorGovtorNGOsefng,alsoPRIVATEPRACTICE:alloftheabove
BEETHICALASANEXPERTWITNESS;DONOTFALSIFYORCONFOUNDJURYJUSTBECAUSEYOUARE“BELIEVABLE”TOTHEJURY
• MEDIAPERSONALITY:Dr.G(DiscoveryChannel),Dr.Baden(HBO‐Autopsy),Dr.HenryLee,DeadMenTalking,aCBSshow;alsoCSIshowconsultants

TRUTV.COMTRUTVLIBRARY

WHATNEXT?CHECKOUT—AAFS.ORG,

FREEONLINEFORENSICINVEST.COURSE
www.physicians
forhumanrights/forensics

NEXTFRONTIER• Morepeople,morestudentsinbekerschools(CSIeffect‐inTVcrimesissolvedsomuchfaster,BUTrealityismorecolorfulormorebizarrethanficOon)
• Improvedscienceandtechnology(fasterDNAthroughputsonobackloginpropertyandpersonalcrimes),moreandbekerresearch
• Bekerstandardsinlawandforensics,sotherewillbenowrongfulconvicOons(ex.Innocenceproject)
• OUTCOMES:LESSCRIME,SAFERCOMMUNITIES,LESSPEOPLEDYINGBEFORETHEIRTIME
MayJenniferAmolat‐Apiado,MD,MFM,MPHAmericanAcademyofForensicSciencesAnnualMeeOng
ACauseforForensicPublicHealth:Preven7onandPublicHealthContentinTwoU.SForensicJournals

GLOBALINJURYBURDEN
• Injuryresultsin9%oftheworld’smortality
– mostlyfromlow‐andmiddle‐incomecountries
– 5Mdieannuallyfrominjury– Thenumberofhomicides(500,000)orthenumberofsuicides(860,000)ishigherthanthenumberofdeathsfromHIV,malariaandtuberculosiscombined(1)
1.PedenM,McGeeK,SharmaGTheInjuryChartbook:AGraphicalOverviewoftheGlobalBurdenofInjuries.Geneva:WorldHealthOrganizaOon;2002.

NUMBEROFPAPERSbyINJURYMECHANISM/FORENSICTOPIC2
Injury mechanism/forensic topic No. of Papers % of total
Criminology/criminalistics 15 9%
Infection 15 9%
Transportation fatalities 15 9%
Abuse (elder, domestic, sexual, interpersonal, child)) 14 9%
Occupational health 13 8%
Environment-related deaths 13 8%
Mental health 11 7%
Custody/Police-related deaths 10 6%
Medical devices/complications 6 4%
Drowning 6 4%
Electrical injuries 5 3%
Natural (aside from infection) 2 1%
Others 2 1%

NO.OFPAPERSbyMANNEROFDEATH
Manner of death Number of Papers
Percentages of total
Accidents 61 37%
Suicide 30 19%
Homicide 29 18%
Natural 24 15%
Therapeutic complication/misadventure
7 4%
Other/not applicable 36 22%

NUMBEROFPAPERSBYPRIMARYAUTHOR’SSPECIFICAFFILIATION1
Specific affiliation of 1st author No.of Papers % of total Medical examiners’ offices 34 21%
Academic forensic medicine department 18 11%
Hospital department, pathology 18 11%
Other government public health agencies 16 10%
Hospital departments, psychiatry 14 9%
Medical school/med center/hospitals 12 7%
University department/university 11 7%
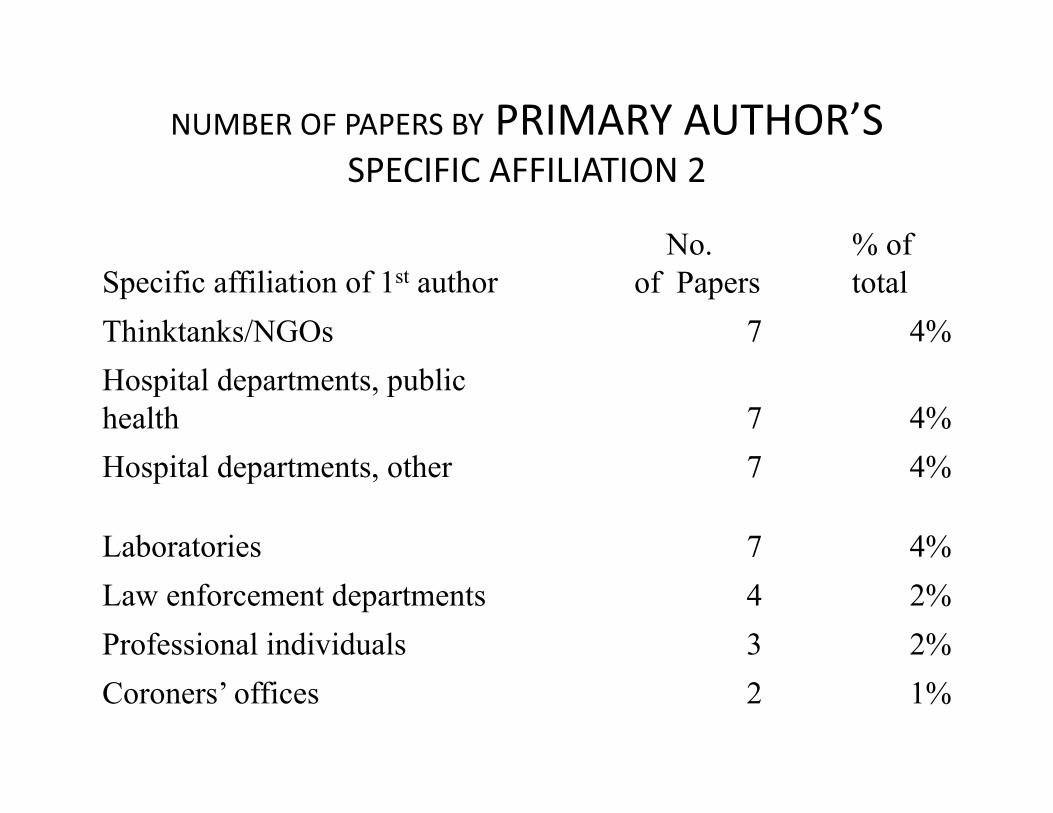
NUMBEROFPAPERSBYPRIMARYAUTHOR’SSPECIFICAFFILIATION2
Specific affiliation of 1st author No.
of Papers % of total
Thinktanks/NGOs 7 4%
Hospital departments, public health 7 4%
Hospital departments, other 7 4%
Laboratories 7 4%
Law enforcement departments 4 2%
Professional individuals 3 2%
Coroners’ offices 2 1%
AREWEDOINGENOUGH?
PublichealthpracOcecanbenefitfromincreasedparOcipaOonofmedicalexaminersandotherforensicdisciplinesastheyareinherentlyinvolvedincasesofinjuryandviolence
THEBESTFORENSICSISNOTENOUGH!WENEED
SOCIALWORK/MENTALHEALTHREFERRALS,PARTICIPATIONINCOMMUNITY,IMPROVESCHOOLS,PARENTINGPRACTICES/PEERQUALITY,ANTI‐CRIMELAWS(ex.firearms),JOBSANDBETTERSURROUNDINGS(environmentalpolicing)

ECOLOGICALMODELFrameworkfordeterminingrisksandintervenOons
age,educaOon,income,substanceandalcoholabuse,psychiatricorpersonalitydisordersandhistoryofviolentbehaviororabuse
poorparenOngpracOces,conflictinthehome(marriageorfamily)andassociaOonwithdelinquentorviolentfriends
drugtrade,highratesoftransients(residenOalmobility),poverty,unemployment,socialisolaOonandweakorineffecOveinsOtuOons.
normsthatsupporttheuseofviolence,availabilityofweapons,weakcriminaljusOcesystems,policiesthatperpetuateorincreasesocioeconomicinequaliOes

YES,YOUCAN!
WECANALLCONTRIBUTEINHELPINGSAVELIVES.
ADDRESSINDIVIDUAL,FAMILY,COMMUNITYANDSOCIETALRISKFACTORSTHROUGHABROAD‐BASEDFORUMOR(PUBLICHEALTH)GROUP.
USEINTERVENTIONSTHATAREPROVENTOWORK!(SEEHANDOUTorblog)

VIOLENCEINTERVENTIONSECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE INFANT AND TODDLER (AGED 0–3) CHILDHOOD (AGED 3–11)
Individual • Reduce unintended pregnancies • Increase access to prenatal/postnatal services • Treatment programmes for victims of maltreatment to reduce consequences • Services for children who witness violence
• Social-development training • Pre-school enrichment
• School-based child maltreatment prevention programmes
• Drug-resistance education • Gun-safety training
Relationship (for example, family, peers)
• Home-visitation services • Parenting training • Therapeutic foster care
• Mentoring • Home-school partnership programmes to promote parental involvement
Community • Lead monitoring and toxin removal • Screening by health-care providers for maltreatment
• Safe havens for children on high-risk routes to and from school • After-school programmes to extend adult supervision • Recreational programmes
• Community policing • Improving emergency response and trauma care • Training for health-care providers in the detection and reporting of child maltreatment • Promotion of safe storage of firearms and other lethal weapons • Prevention and educational campaigns to increase awareness of child maltreatment • Child-protection service programmes • Services for incarcerated perpetrators
• Gun buy backs
Societal • Reduce media violence • Public information campaigns to promote pro-social norms
• Strengthen police and judicial systems • De-concentrate poverty • Reduce income inequality

ECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE
ADOLESCENCE (AGED 12–19) ADULTHOOD (AGED 20 AND OVER)
Individual • Social-development training • Educational incentives for at-risk, disadvantaged high-school students • School-based dating violence prevention programmes • Academic enrichment programmes
• Individual counselling • Shock probation or parole • Residential programmes in psychiatric or correctional institutions • Gun-safety training • Boot camps • Trying young offenders in adult court • Drug-resistance education • Programmes modelled on basic military training
Relationship (for example, family, peers)
• Mentoring • Family therapy
• Temporary foster-care programmes for serious and chronic delinquents
• Peer mediation, counselling
AdaptedfromRosenbergMLetal.Violence.ChaptersubmikedtoJamisonDTetal.(Eds)DiseasecontrolprioriBesindevelopngcountries,secondediOon.NewYork,OxfordUniversityPress.InButchartA,PhinneyA,CheckP,VillavecesA.PrevenBngviolence:aguidetoimplemenBngtherecommendaBonsoftheWorldreportonviolenceandhealth.DepartmentofInjuriesandViolencePrevenOon,WorldHealthOrganizaOon,Geneva,2004.(BOLD‐WORKS,GRAY‐SHOWSPROMISE;ITALICS;NOTHELPFUL)

Community
• Recreational programmes • Reduce alcohol availability • Train health-care professionals in identification and referral of high-risk youth and victims of sexual violence • Metal detectors in schools
• Reduce alcohol availability • Establish adult recreational programmes • Shelters and crisis centres for battered women and victims of elder abuse • Criminal justice reforms to criminalize child maltreatment, intimate-partner violence, and elder abuse • Mandatory arrest policies for intimate-partner violence • Public shaming of intimate partner violence offenders • Services for identifying and treating elder abuse • Train health-care professionals in identification and referral of battered women, victims of elder abuse, and victims of sexual violence
• Multi-component gang-prevention programmes
• Laws permitting gun carrying in public
• Community policing • Improve emergency response and trauma care • Disrupt illegal gun markets • Forbid firearm sales to high-risk purchasers • Mandatory sentences for gun use in crimes • Coordinated community interventions for violence prevention • Prevention and educational campaigns to increase awareness of youth violence, intimate-partner violence and elder abuse
• Gun buy backs
Societal • Reduce media violence • Enforce laws prohibiting illegal transfers of guns to youth
• Establish job-creation programmes for the chronically unemployed
• Strengthen police and judicial systems • Promotion of safe storage of firearms • De-concentrate poverty • Reduce income inequality • Change cultural norms that support violence and abuse of children and adults
ECOLOGICAL CONTEXT
DEVELOPMENTAL STAGE ADOLESCENCE (AGED 12–19) ADULTHOOD (AGED 20 AND OVER)

WHO‐VIPwebsite
hkp://www.who.int/violence_injury_prevenOon/violence/en/

CDC

THANKYOU!
• Dr.AMOLAT‐APIADO’sCONTACTANDHANDOUTS:
Blog:
theautographer.wordpress.com
Email: