anaesthesia in animals for intracranial surgery - ecvn.org · (icp) in presence of space occupying...
TRANSCRIPT

Dick White Referrals
Anaesthesia in animals for intracranial surgery
Federico Corletto PhD CertVA Dipl.ECVAA MRCVS European Veterinary Specialist in Anaesthesia and Analgesia
1

Dick White Referrals
Does one size fit all?
Dick White Referrals
One does not fit all!
• Variety of conditions • Neoplasia • Traumatic brain injury • Experimental procedures in laboratory animals
• Management of clinical cases derived from publications related to clinical anaesthesia and research in humans
• Physiology and pharmacology characterised in laboratory animals
Dick White Referrals
Topics of this presentation
• Basic principles and physiological goals • Total intravenous anaesthesia (TIVA) vs balanced
inhalational anaesthesia • Mannitol or hypertonic saline? • Dexmedetomidine use in neuroanaethesia • Ketamine and intracranial procedures • Managing early anaesthetic recovery
Dick White Referrals
Physiological goals and problems
• Problems relevant for the anaesthetist • rigid skull does resulting in increased intracranial pressure
(ICP) in presence of space occupying lesions (SOL) • high vascularisation of the brain and risk of intra and
postoperative bleeding • great susceptibility of the brain to both hypoxic and
ischaemic damage
Dick White Referrals
• Review MRI, plan the procedure with the neurologist
Dick White Referrals
Physiological goals and problems
• Main goals • maintain adequate perfusion and oxygenation of the brain • decrease metabolic requirements • provide optimal conditions for surgery • preserve cerebrovascular reactivity in responses to
changes in arterial blood pressure and partial pressure of CO2

Dick White Referrals
Arterial Blood Pressure cardiac output heart rate vascular resistance
Local factors local vascular resistance myogenic control neurogenic control (sympathetic system) local metabolic control adenosine, H+, K+, Ca2+, TX, PG metabolic derangement (TBI/stroke)
Blood O2 content Haemoglobin PaO2 Local diffusion (oedema)
Intracranial pressure soft tissue (CNS) blood (arterial and venous) CSF pathology
Oedema, neoplasia, bleeding
Blood viscosity
PaCO2, PaO2
CNS metabolic activity
Cerebral oxygenation and perfusionAutoregulation
Cerebral perfusion pressure
Dick White Referrals
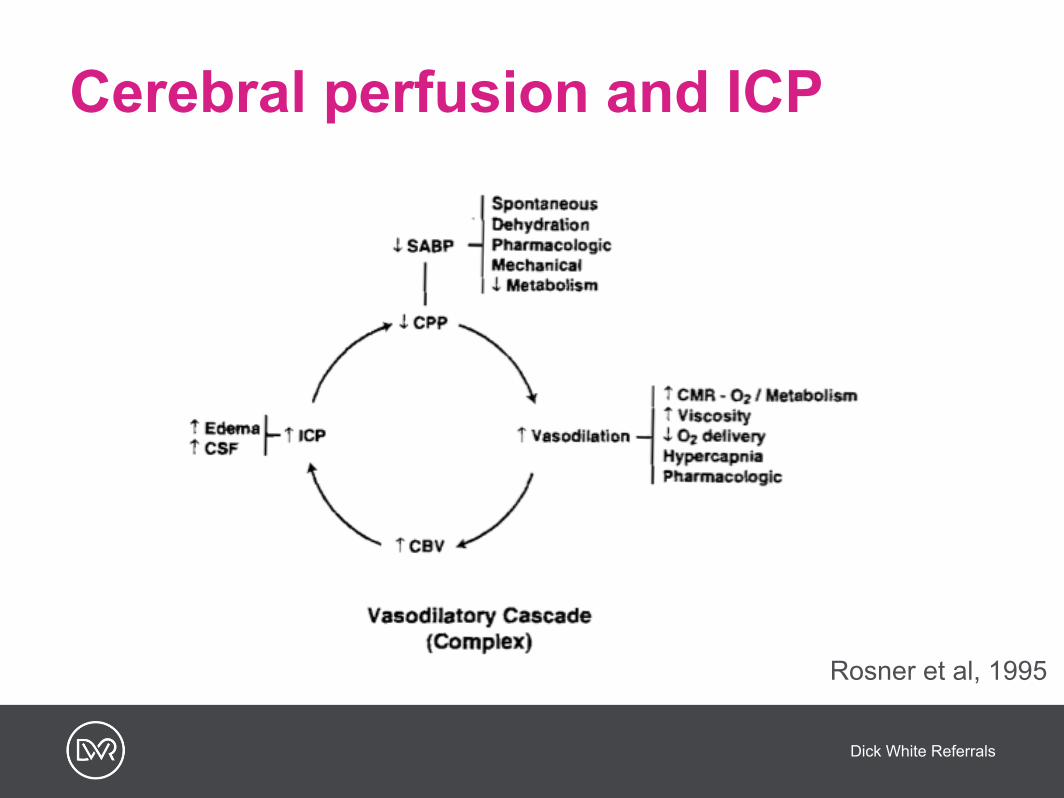
Cerebral perfusion and ICP
Rosner et al, 1995
Dick White Referrals
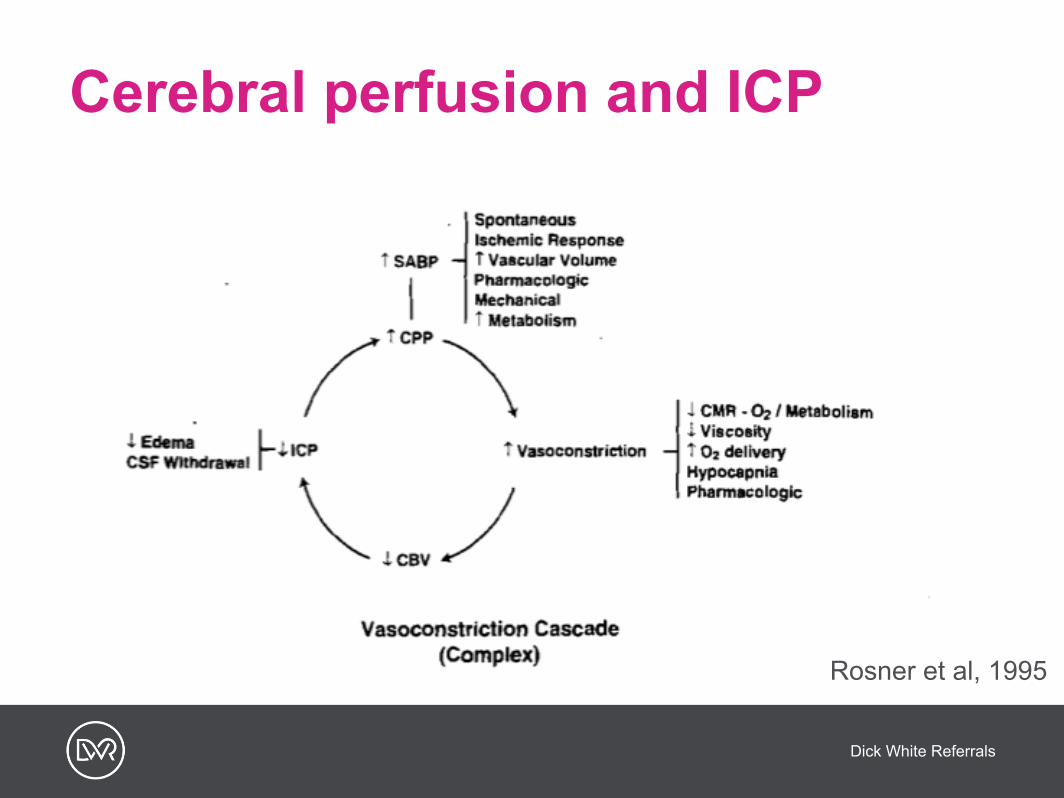
Cerebral perfusion and ICP
Rosner et al, 1995
Dick White Referrals
Controlling ICP
• Reduction of intracranial volume • promoting venous drainage (head elevation) • hypocapnic vasoconstriction • reflex vasoconstriction • control of oedema • CSF drainage in absence of risk of herniation
• Sedation and anaesthesia to reduce the effects of poor perfusion • Decompressive craniectomy
Dick White Referrals
TIVA or inhalational?
• Propofol-based TIVA is considered the gold standard in neuroanaesthesia
• Inhalational anaesthetics may affect ICP • Direct increase in cerebral volume (vasodilation) • Effect on cerebrovascular reactivity
• Sevoflurane vs isoflurane • Normal vs pathological brain
Dick White Referrals
Sevoflurane or Isoflurane ?
• Cerebrovascular reactivity in response to changes of blood pressure • at 1.5 MAC VMCA after an hypotensive challenge recovers
quickly with sevoflurane (Summors, 1999) • preservation of cerebrovascular reactivity with sevo 0.5
and 1.5 MAC after hypertensive challenge (Gupta, 1997) • Cerebral vasodilation
• greater with iso at the same MAC equivalent (Matta, 1999) • greater with iso with similar AEP suppression (Holmstrom,
2004)
Dick White Referrals
Inhalational anaesthetics
• The effect on ICP and CBF depends on the agent used AND the MAC equivalent (Gunduz, 2009) • metabolic suppressions prevalent at low concentrations,
causing reflex vasoconstriction • direct vasodilation prevalent at high concentrations,
causing an increase of CBV and ICP
Dick White Referrals
Propofol TIVA
• Propofol consistently reduces CBV and metabolism • Dose dependent • Direct vasoconstriction?
• At same level of BIS (35), flow-metabolism uncoupling was observed with sevoflurane-remifentanil, but not with propofol-remifentanil anaesthesia (Conti, 2006) • sevoflurane 4% was used to achieve the desired BIS
• Recently propofol vs isoflurane in dogs undergoing MRI • Reduced dopamine use
Dick White Referrals
What is the clinical relevance?
• Propofol based protocol was compared with sevoflurane based protocol in patients undergoing elective intracranial surgery (Sneyd, 2005) • 50 patients • hypotensive episodes more frequent with sevoflurane • hypertension during recovery more frequent with sevoflurane • both protocols deemed suitable

Dick White Referrals
So...which one is better?• In absence of raised ICP, both propofol based TIVA and
sevoflurane based anaesthesia are comparable • When a reduction of ICP is desired, propofol based TIVA may
be superior • In veterinary medicine, only propofol based TIVA has been
reported for elective intracranial surgery (Raisis, 2007) • Alfaxalone/alfadolone decreases CBF in ventilated cats (Baldi/
Moulinier, 1975) • Alfaxalone/alfadolone decreases CBF and metabolism in man
(Renou, 1976)
Dick White Referrals
• Pharmacokinetics of mannitol in dogs is similar to humans (Cloyd, 1986) • distribution half-life of a couple of minutes • elimination half-life of approximately 80 minutes • peak effect at end of infusion
• Furosemide used to potentiate the effect of mannitol • Experimental evidence in dogs suggests that administration
15 minutes after mannitol is more effective (Roberts, 1987)
Mannitol or hypertonic saline?

Dick White Referrals
Mannitol or hypertonic saline?
• Mannitol is commonly used, although hypertonic saline (HS) seems promising • In a rodent model of TBI, HS was more effective in reducing
ICP compared to mannitol (54% vs 35% and for longer (500 min vs 120 min) (Mirski, 1999)
• In a canine model of ICH, HS 3% was more effective and for longer (120 min) than HS 7.2% and mannitol 1 g/kg in reducing ICP (Qureshi, 2000)
Dick White Referrals
Mannitol or hypertonic saline?
• HS/HES was more effective in reducing ICP than mannitol in a randomised clinical trial in humans undergoing intracranial surgery (Harutjunyan, 2005)
• HS reduces ICP in elective supratentorial surgery (Gemma, 1996)
• HS was effective in treating refractory post-traumatic elevated ICP (Vialet, 2002)

Dick White Referrals
Mechanism of action of HS
• Vascular expansion leading to increased brain perfusion and reflex vasoconstriction
• Improved blood rheology • Reduction of CSF production • Reduction of cerebral volume • Immunomoduating effect • Hypernatremia is the most common side effect after
administration of multiple doses • neurological sequaelae
Dick White Referrals
Dexmedetomidine
• Attractive features for neuroanaesthesia • haemodynamic stability • analgesic effect • minimal ventilatory depression
• Other interesting features • cerebral vasoconstriction
- consequent reduction of CBF and CBV • minimal effect on cerebral autoregulation
Dick White Referrals
Dexmedetomidine and CBF
• Dexmedetomidine 10 µg/kg decreases CBF, but not CMRO2 in dogs anaesthetised with isoflurane (0.5-2.2. MAC) • 57% decrease of cardiac output • 40 mmHg increase of MAP • despite not decreasing CMRO2, dexmedetomidine depressed
EEG activity • no evidence of ischaemia • dexmedetomidine sedative effect caused by action on specific
sites, not global depression (Zornow, 1990)
Dick White Referrals
Dexmedet. and inhal. agents
• Dexmedetomidine 0.5-2 µg/kg attenuates cerebral vasodilation induced by isoflurane and sevoflurane (0.5-1.5 MAC) in dogs, and oxygen extraction is not increased (Ohata, 1999)
• Dexmedetomidine effect on CBF is preserved during hypercapnia (90 mmHg) in dogs anaesthetised with isoflurane (Fale, 1994)
• A detrimental role of cerebral oxygenation was not found in patients with neurovascular injuries (Drummond, 2010) • sevoflurane and sufentanil or dexmedetomidine
Dick White Referrals
What about ketamine?
• Attractive option • neuroprotective in laboratory animals (NMDA antagonist)
- Effective if administered prior to ischaemic (Lin, 1996) and traumatic insults (Shapira, 1994)
• inconclusive evidence in clinical trials • Ketamine decreases ICP in patients with TBI sedated with
propofol (Albanese, 1997) • 8 patients
Dick White Referrals
Early postanaesthetic recovery
• Hypertension common in humans (Muzzi, 1990) • exact cause not yet clear • not unequivocally linked to postoperative bleeding
(Warner, 2002) • Disorientation in animals if recovered quickly and after
cranial fossa surgery • may contribute to hypertension
Dick White Referrals
Early postanaesthetic recovery
• Hypertension and disorientation are usually transient • related to the procedure OR • indicating complications (bleeding, raised ICP)
• Frequent neurological evaluation and team work allow to rule in/out effect of anaesthesia and procedure vs complications • Consider diagnostic imaging if in doubt
• Preoperative and regular postoperative neurological assessment
Dick White Referrals
Early postanaesthetic recovery
• Management of emergence from anaesthesia • ensure adequate analgesia (esp. if using remifentanil)
- balance opioids administration with delaying return of spontaneous ventilation
• consider sedation - dexmedetomidine prior to beginning the recovery process,
infusion in the postoperative period • perioperative antiepileptic administration • administration of esmolol/labetalol to control hypertension

Dick White Referrals
• Difficult translating significant basic science findings into clinically relevant interventions • Neuroprotective drugs and interventions
- Clinically relevant outcome measures - Confounding factors not controllable in a clinical setting
• Lack of large scale clinical trials in veterinary medicine • ... if in doubt...
Are our interventions evidence-based?
Dick White Referrals
Dick White Referrals