ankylosing spondylitis and related spondyloarthropathies 3
TRANSCRIPT

Ankylosing Spondylitis and Related Spondyloarthropathies3

Spondylarthropathy
• Association with HLA-B27
• Inflammatory back pain
• Sacroiliitis
• Enthesitis
• Common extral -articular manifestation

AS Pathogenesis• Multifactorial: genetic and environmental
• Genetic: B27
• AS develops in 2–5% of HLA–B27-positive individuals.
• First-degree relatives HLA-B27–positive ≈15-20% chance of developing AS,10 times more than B27-positive individuals with no such family history

AS Pathogenesis
• Environmental:• Bacterial triggers: Molecular mimicry

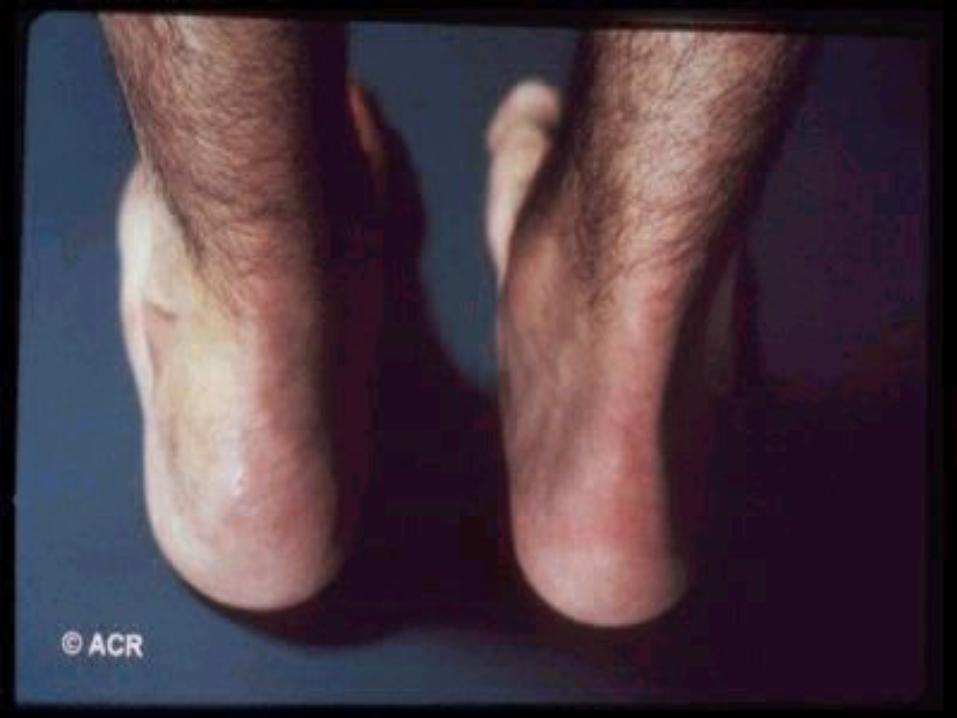
Enthesitis
• Enthesis as the area of insertion of tendon, ligament, joint capsule, or fascia to bone
• Hallmark that characterized SpAs• Enthesis is not a static one.
-high capacity for dynamic tissue turnover in continual response to changes in mechanical factors.
• This would explain why this is a target for inflammation.

Enthesitis
• . There are 2 types: • Fibrous entheses :dense fibrous connective
tissues linking tendon and ligament to bone. located at the metaphyses and diaphyses of long bones
• Fibrocartilage entheses :more common, have an additional transitional zone of fibrocartilage at the bony interface located at sites with a great deal of joint movement, probably because fibrocartilage can dissipate mechanical stress.

58
retrocalcaneal bursa
sesamoid fibrocartilage
Enthesis fibrocartilage
periosteal fibrocartilage
Fibrocartilage enthesis of human Achilles tendon

History
• Vertebral symptoms.• Inflammatory back • first manifestation in 75% of patients.
• Onset insidious occurring over months or years, at least 3 months.
• Alternating buttock pain• Systemic features.
• Morning stiffness characteristic.
• Fatigue is common.
• Fever and weight loss may occur during periods of active disease.

History
• Non-vertebral Symptoms.
• Asymmetric peripheral arthritis.Arthritis of the toe IP Joints.Sausage Digits.Achilis Tenosynovitis.Plantar Faciitis.Costochondritis.Iritis.Mucocutaneous Lesions

– Inflammatory back pain.– Most common symptom ,first manifestation in 75% of patients.
– Onset insidious occurring over months or years, at least 3 months.
– Morning stiffness lasting at least 30 minutes, improvement of symptoms with moderate physical activity.
– Diffuse nonspecific radiation of pain into both buttocks.
– Patients often experience stiffness and pain that awakens them in the early morning hours, a distinctive symptom not generally found in patients with mechanical back pain.
– Most patients have mild chronic disease or intermittent flares with periods of remission.
– The spinal disease rarely is active persistently.
– The spinal disease starts in the sacroiliac joints.
–

Diagnosis of SpAs
• Inflammatory back pain and at least two of the following.• Psoriasis.• Family history.• Response to NSIADs• Enthesistis.• Alternating buttock pain.• Peripheral arthritis.• Dactylitis.• Anterior uveitis.• Positive predictive probability >90% for diagnosis of SpA

58
58

58


• insidious onset of chronic low back pain and stiffness
• Sites of inflammation
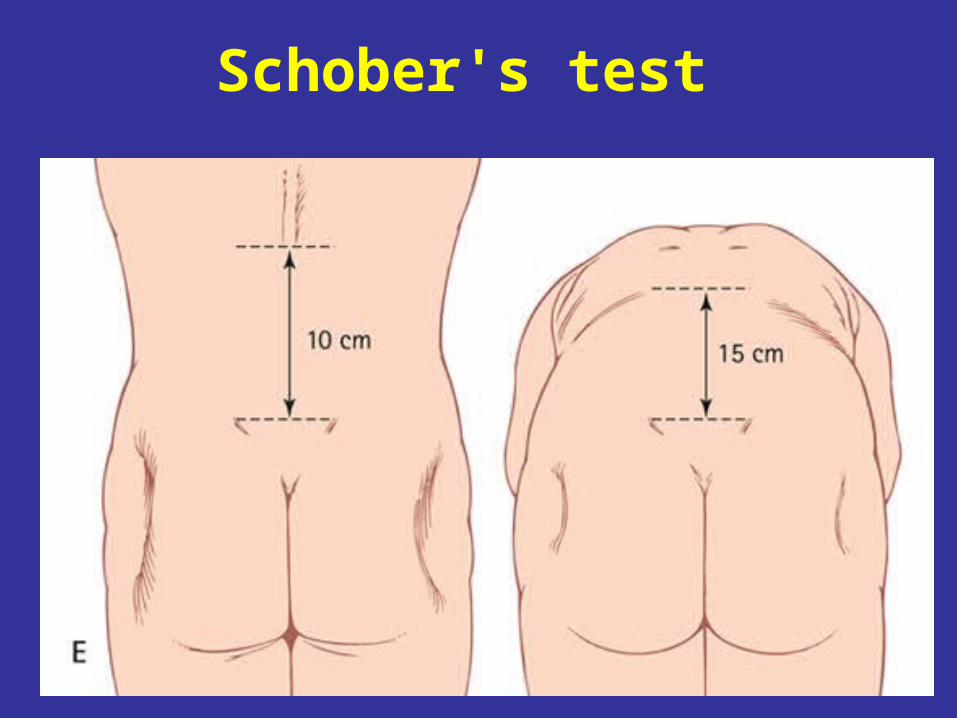
Schober's test




Copyright ©2002 BMJ Publishing Group Ltd.
Sieper, J et al. Ann Rheum Dis 2002;61:8iii-18iii
AS bilateral sacroiliitis grade III.


58
58

58


58

58

58
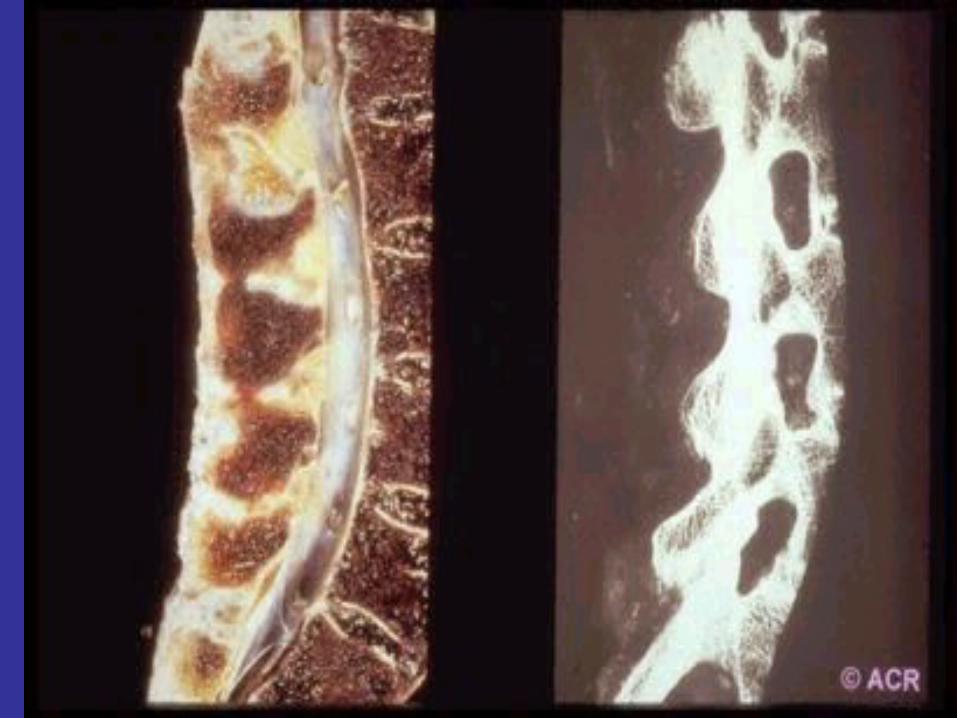
• Metabolic bone disease • Osteopenia:- increased
risk of fracture.• Standard radiographs
may not be revealing.• CT scan ,MRI may be
required to aid in diagnosis.

Enthesitis

Potential Skeletal Sites ofInflammation of AS
Inflammation primarily affects the sacroiliac joints and axial skeleton
Juxta-articular bony tenderness resulting from enthesitis at costosternal junctions,, spinous processes, lateral epicondyle, distal ulna, distal scapula, iliac crests, greater femoral trochanters, tibial tuberosities superior and inferior poles of the patella ischial tuberosity, insertion of the plantar fascia on the calcaneus or the metatarsal heads, the base of the fifth metatarsal head Achilles tendon insertion
11

Eyes(Acute Anterior Uveitis)
Heart(Aortic Insufficiency, Heart Block)
Gut (Inflammatory Bowel Disease,
Microscopic Inflammatory Lesion)
Dactylitis
Potential Other Disease Manifestations in AS
Cauda Equina Syndrome
Osteopenia
Skin(Psoriasis & Nail Changes)
Kidneys(Amyloidosis)
Lungs(Restrictive Lung Disease, Apical Fibrocystic Disease)
12

Ankylosing SpondylitisDifferentiating Inflammatory vs Mechanical
Back Pain
Courtesy of J. Cush, MD

AS in Women
• AS is approximately 3 times less common in women
• The overall pattern of clinical disease is similarin both sexes; axial spinal disease more often may be milder in women than in men
• However, self-ratings of pain and impairment of daily activities by women tend to show a less favorable overall outcome than in male patients
1. Kidd et al. J Rheumatol 1998; 15:1407-92. Carbonne et al. Arthritis Rheum 1992; 35:14793. Zink et al. J Rheumatol 2000; 27:613-224. Boonen et al. J Rheumatol 2001: 28: 1056-62
16

58
Lab Studies.No laboratory tests are specific for AS.
Diagnosis is made by combining clinical criteria of inflammatory back pain and enthesitis or arthritis with radiological findings.
Anemia of chronic disease 15% of patients.
ESR or C-RP elevated in 75%..
Alkaline phosphatase is elevated in 50% patients
Serum IgA level may be elevated.
HLA-B27 positivity is present in 92% of white with AS .
Determining HLA-B27 status is not a necessary part of the clinical evaluation.

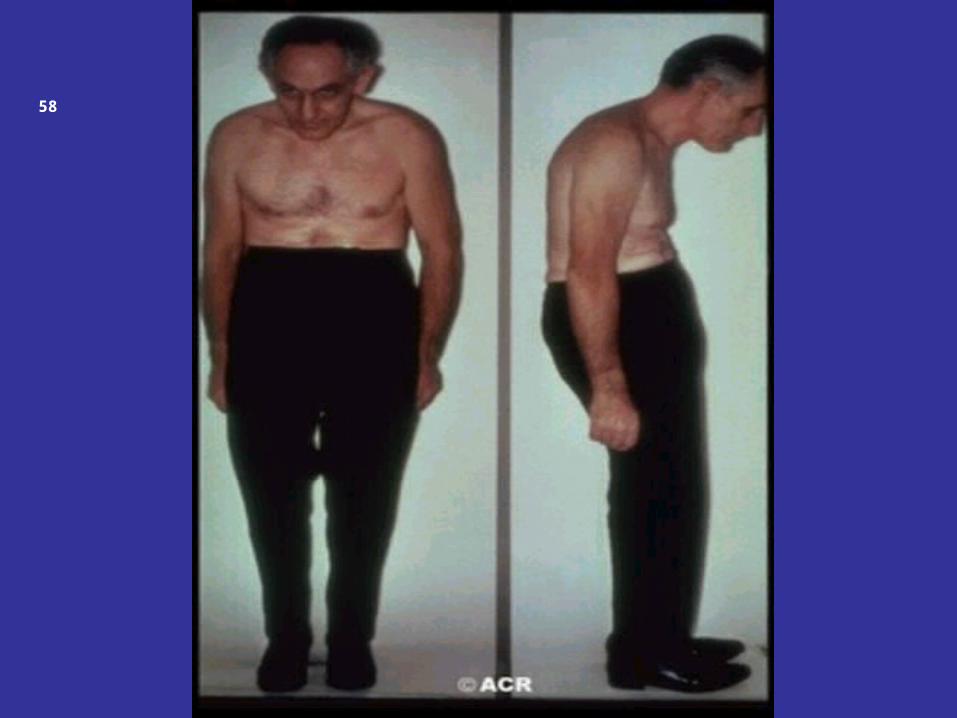
AS Yesterday: Severe Disease Outcome• Obliteration of lumbar lordosis with atrophy of buttocks• Accentuation of thoracic kyphosis• Forward stoop of neck if the cervical spine is involved• Hip involvement can lead to
– Flexion contractures– Compensated for by knee flexion
After hipreplacement
56

• Management of AS• AS:- often misdiagnosed or diagnosed late ,under-treated
– consider when seeing a young patient who has chronic back pain.
• Basic therapy
– Regular exercise .
– Maintain posture.– NSAIDs
• NO smoking (significant negative impact on AS). • Avoid physical trauma :-risk of fracture• Early diagnosis early introduction of biologic therapy is an important therapeutic goal
– Anti-TNF- therapy

58
58

58

58

58

58

58

58

58

• Reactive Arthrits :-
• Sterile joint inflammation triggered by a distant infection
• Weaknesses.
• 1-Bacterial components—may be detectable at the sites of inflammation.
• A more appropriate definition would therefore be a joint inflammation triggered by a distant infection, with no cultivable microbes in the joints.
• 2-The disease is not limited only to the joints but affects the whole individual, • causing a variety of lesions. • Previously healthy persons.• • Triggering infection may pass unnoticed. • • Microbiological and serological investigations are the cornerstones of the
diagnosis • •.

Bacterial Infections that can Trigger HLA-B27-Associated Reactive Arthritis
• Gastointestinal Infection
a. Usual triggers:
• Shigella flexneri
• Salmonella enteritides and S. typhimurium
• Yersinia enterocolitica and Y. pseudotuberculosis
• Campylobacter jejuni
• b. Unusual triggers:
• Shigella sonnei and S. dysenteriae
• Salmonella paratyphi
• Bacillus Calmette-Guerin
• Clostridium dificille
• Urogenital Infection• a. Usual triggers:
• Chlamydia trachomatis
• b. Unusual triggers:
• Ureaplasmaurealyticum.
• Respiratoroy infection• Chlamydia pneumoniae

Psoriatic Arthritis: Clinical Charactrastics
Erosive Arthritis
Arthritis in DIPs
Asymetric ArthritisParavertebral Ossification and Sacroiliitis
Enthesopathy
Sausage DigitsNail Pitting or OnycholysisNo Rheumatoid NodulesRF Negative

Epidemiology
• Approximately 2% of the Caucasian population has psoriasis.
• 5-7% are affected by an inflammatory arthritis.– men and women are affected with equal frequency– The peak incidence 4th through 6th decades.

• 1. Asymmetrical mono- and oligoarticular arthritis (30-50% of cases)
• 2. Symmetrical polyarticular arthritis (30-50% of cases).
• 3. Distal interphalangeal (DIP) joint involvement (25% of cases) is nearly always associated with nail manifestations).
• 4. Arthritis mutilans (5% of cases) is characterized by resorption of the phalangeal bones.
• 5. Axial arthritis (30-35% of cases) may be different in character from ankylosing spondylitis,. It may present as sacro-iliitis, which may be asymmetrical and asymptomatic, or spondylitis, which may occur without sacro-iliitis and may affect any level of the spine in “skip” fashion.
Clinical Manifestation

Distinguishing PsA and RA
• Enthesopathic features
–dactylitis
–enthesitis
• Signs of psoriatic skin disease or nail disease
• Spinal involvement or sacroiliitis

Distal interphalangeal (DIP) joint involvement (25% of cases) is nearly always
associated with nail manifestations

Symmetrical polyarticular arthritis (30-50%).

Dactylitis presents as the so-called “sausage digit”, diffuse swelling of the entire digit likely due to a combination of both arthritis and tenosynovitis


58


58

Nail involvement may be manifested as pitting, ridging, separation from the nail bed (onycholysis

58

Extra-cutaneous manifestations
•Conjunctivitis.•Uveitis.•Aortic insufficiency.•Pulmonary fibrosis.
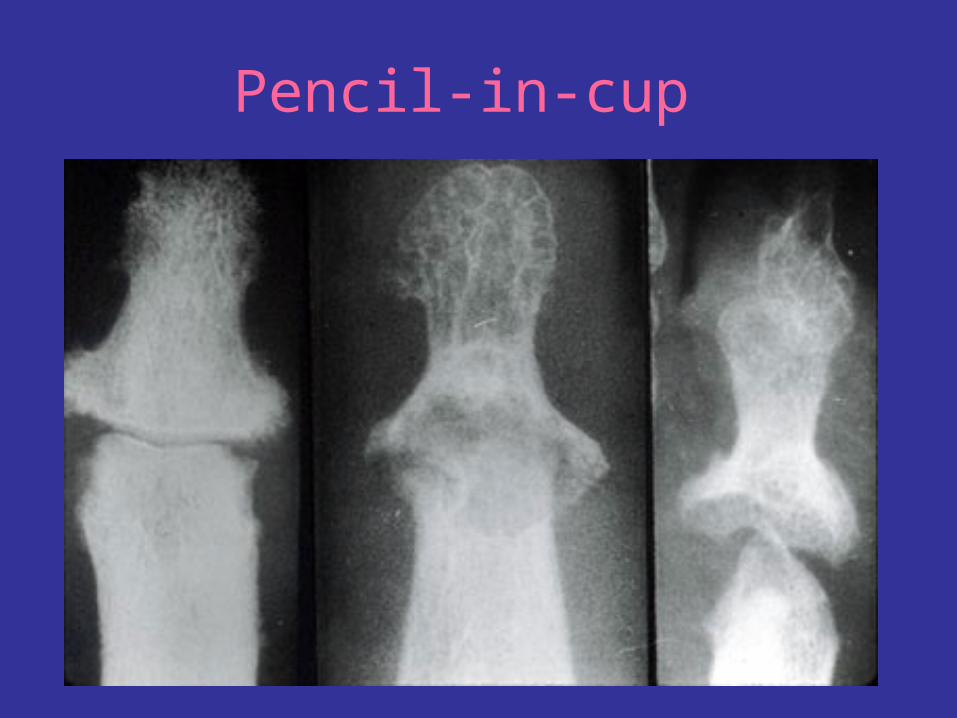
Pencil-in-cup

58

Sacroiliitis

Spondylitis,enthesitis and periostitis

Axial arthritis (30-35% of cases) may be different in character from ankylosing spondylitis,. It may present as sacro-iliitis, which may be asymmetrical and asymptomatic, or spondylitis, which may occur without sacro-iliitis and may affect any level of the spine in “skip” fashion.

Arthritis mutilans (5% of cases) characterized
by resorption of the phalangeal bones.

Treatment• Treatment for psoriasis remains suppressive, rather
than curative.
• Articular disease .
• Non-steroidal anti-inflammatory agents (NSAIDs).
• patients with aggressive and potentially destructive disease, disease-modifying anti-rheumatic drugs (DMARDs) should be added early on in the course.
• Methotrexate.is effective for both the cutaneous and peripheral articular manifestations of psoriasis. It is generally the first choice of DMARD, given its efficacy and tolerability.