annual meeting nutrition and social protection second sustainable development goal end hunger,...
TRANSCRIPT

www.food-security.net
32nd ANNUAL MEETING
NutritioN ANd SoCiAl ProtECtioNBACKGROUND DOCUMENT, THEMATIC SESSIONABUJA (NIGERIA), 13 DECEMBER 2016
dec 2016
© SWAC/OECD
One out of three children under the age of five in the Sahel and West Africa (or some 20 million young children) currently suff ers from chronic malnutrition, limiting the development of its full physical and cognitive potential. This weakens the region’s human capital, thereby compromising resilience, causing significant economic losses and impeding development in the region. How can eff ective intervention packages be put in place to improve nutrition and resilience? How can they be implemented on a large scale? How can they be sustainably financed?
the Sahel and West africa region is experiencing major economic and social changes, notably due to rapid population growth. the population has increased fivefold over the past 65 years and is expected to reach 830 million in 2050. demographic growth is also a key factor in urbanisation; urban dwellers now account for close to 50% of the region's population. these changes have a significant impact on food and nutrition security. While these trends may be a source of regional growth, economic diversification and development, they also present new challenges in terms of delivering appropriate food, education, health and social protection services. over the past decade, recurrent food crises have weakened people’s resilience and the social fabric, further destabilising the region. it is therefore essential to build a more equitable society which is focused on human development and responds to young people's aspirations.
food and nutrition crises are caused by a combination of several factors: cyclical (related to climate, the economy and conflict) and structural ones, that play a role in dragging the poorest segments of the population into a state of permanent crisis. the extreme poverty experienced by the most vulnerable exposes them to high food and nutrition vulnerability. tackling malnutrition and building resilience calls for a holistic response to the situation and long-term commitment. recognising the importance of such an approach, the region established the global alliance for resilience (agir) – Sahel and West africa in december 2012. this demonstrates the region's strong political will to break the vicious circle of crises through preventive action and anticipation. the first two pillars of the alliance address social protection and nutrition issues. indeed, social protection is increasingly seen as an indispensable tool for reducing economic barriers to achieving adequate access to food and basic social services.
This background document aims to guide the discussion of the RPCA
thematic session on "Nutrition and Social Protection". It provides an overview of the current nutrition
situation, challenges and links between social protection,
nutrition and resilience. It also raises a number of questions for the
panel debates, focusing on the following key issues :
1. Social protection: a key element in improving resilience & nutrition
2. West African experiences in the field of social protection for nutrition & resilience
3. Sustainable funding for social protection & nutrition
The paper was prepared with the support of the teams of the
European Commission Nutrition Advisory Service (EC-NAS, Claire
Chastre et Hélène Berton) and the Advisory Service in Social Transfers
(ASiST Cécile Cherrier).
UEMOA
ClubSAHEL ANDWEST AFRICA
Secretariat
nutrition: a major challenge for the Sahel and WeSt africa
A. Scope of the problem and recent trends
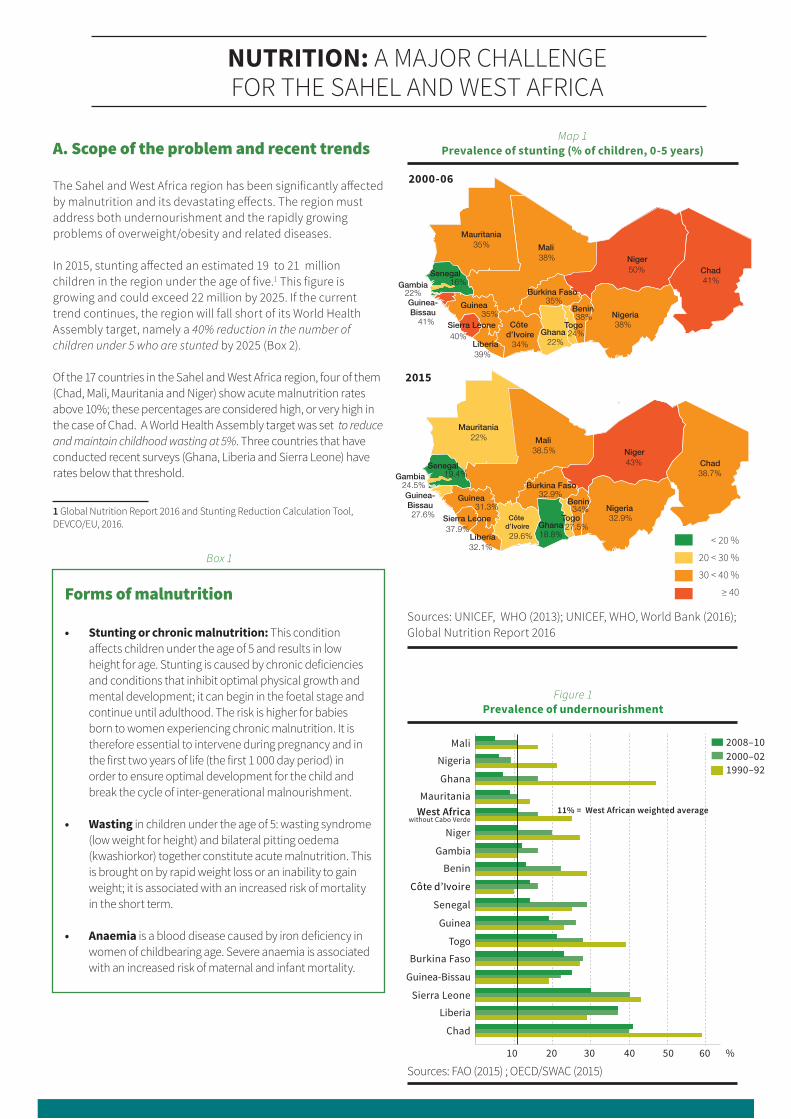
the Sahel and West africa region has been significantly affected by malnutrition and its devastating effects. the region must address both undernourishment and the rapidly growing problems of overweight/obesity and related diseases.
in 2015, stunting affected an estimated 19 to 21 million children in the region under the age of five.1 this figure is growing and could exceed 22 million by 2025. if the current trend continues, the region will fall short of its World health assembly target, namely a 40% reduction in the number of children under 5 who are stunted by 2025 (Box 2). of the 17 countries in the Sahel and West africa region, four of them (chad, mali, mauritania and niger) show acute malnutrition rates above 10%; these percentages are considered high, or very high in the case of chad. a World health assembly target was set to reduce and maintain childhood wasting at 5%. three countries that have conducted recent surveys (ghana, liberia and Sierra leone) have rates below that threshold.
1 global nutrition report 2016 and Stunting reduction calculation tool, deVco/eU, 2016.
10
Mali
Nigeria
Ghana
MauritaniaWest Africa
Niger
Gambia
Benin
Côte d’Ivoire
Senegal
Guinea
Togo
Burkina Faso
Guinea-Bissau
Sierra Leone
Liberia
Chad
20 30 40 50 60 %
11% = West African weighted average
2008–102000–021990–92
without Cabo Verde
MaliNiger
NigeriaBenin
TogoGhana
Burkina Faso
SenegalGambia
Côte d’Ivoire
Guinea
Liberia
Sierra Leone
Guinea-Bissau
Chad41%
Mauritania
50%
38%38%
24%22%34%
38%
35%
39%
40%
35%41%
22%16%
35%
MaliNiger
NigeriaBenin
TogoGhana
Burkina Faso
SenegalGambia
Côte d’Ivoire
Guinea
Liberia
Sierra Leone
Guinea-Bissau
Chad38.7%
Mauritania
43%
32.9%34%
27.5%18.8%29.6%
38.5%
32.9%
32.1%
37.9%
31.3%27.6%
24.5%19.4%
22%
< 20 %
20 < 30 %
30 < 40 %
≥ 40
Map 1 Prevalence of stunting (% of children, 0-5 years)
Sources: Unicef, Who (2013); Unicef, Who, World Bank (2016); global nutrition report 2016
Figure 1 Prevalence of undernourishment
Sources: fao (2015) ; oecd/SWac (2015)
2015
Forms of malnutrition
• Stunting or chronic malnutrition: this condition affects children under the age of 5 and results in low height for age. Stunting is caused by chronic deficiencies and conditions that inhibit optimal physical growth and mental development; it can begin in the foetal stage and continue until adulthood. the risk is higher for babies born to women experiencing chronic malnutrition. it is therefore essential to intervene during pregnancy and in the first two years of life (the first 1 000 day period) in order to ensure optimal development for the child and break the cycle of inter-generational malnourishment.
• Wasting in children under the age of 5: wasting syndrome (low weight for height) and bilateral pitting oedema (kwashiorkor) together constitute acute malnutrition. this is brought on by rapid weight loss or an inability to gain weight; it is associated with an increased risk of mortality in the short term.
• Anaemia is a blood disease caused by iron deficiency in women of childbearing age. Severe anaemia is associated with an increased risk of maternal and infant mortality.
Box 1
2000-06

SGd2: Second Sustainable development GoalEnd hunger, achieve food security and improved nutrition and promote sustainable agriculture
140% REDUCTION IN THE NUMBER OF CHILDREN UNDER-5 WHO ARE STUNTED
50% REDUCTION OF ANAEMIA IN WOMEN OF REPRODUCTIVE AGE
2
30% REDUCTION IN LOW BIRTH WEIGHT 3
To improve maternal, infant and young child nutrition
5INCREASE THE RATE OF EXCLUSIVE BREASTFEEDING IN THE FIRST 6 MONTHS UP TO AT LEAST 50%
REDUCE AND MAINTAIN CHILDHOOD WASTING TO LESS THAN 5%
6
NO INCREASE IN CHILDHOOD OVERWEIGHT4
B. Consequences & costs of undernourishment
140% REDUCTION IN THE NUMBER OF CHILDREN UNDER-5 WHO ARE STUNTED
50% REDUCTION OF ANAEMIA IN WOMEN OF REPRODUCTIVE AGE
2
30% REDUCTION IN LOW BIRTH WEIGHT 3
To improve maternal, infant and young child nutrition
5INCREASE THE RATE OF EXCLUSIVE BREASTFEEDING IN THE FIRST 6 MONTHS UP TO AT LEAST 50%
REDUCE AND MAINTAIN CHILDHOOD WASTING TO LESS THAN 5%
6
NO INCREASE IN CHILDHOOD OVERWEIGHT4
Undernourishment has many devastating consequences in the short and long term. it is involved in 45% of the deaths among children under the age of 5 and 35% of the diseases among the same group. twenty percent of maternal mortality is tied to anaemia, which is brought on by iron deficiency. anaemia is at record high levels in the region (figure 2). according to the global nutrition report 2015, of the 17 countries in the region, 15 are among the 25 countries with the highest prevalence rates in the world.
Country USD million
Benin 1 571
Chad 3 718
Mali 2 814
Niger 5 553
Nigeria 29 274
Senegal 1 723
Togo 842
Table 1estimated total additional gdP associated with stepping up
investment in achieving the global target for stunting, 2035-60
Source: hod hoddinott, j. (2016), global panel on agriculture and food Systems for nutrition, Working paper, the economics of reducing malnutrition in Sub-Saharan africa.
Box 2international commitments
Source: estimates (2011), adapted from a presentation by prével, gnr 2015
Figure 2Anaemia in women of childbearing age (%)
20
60
40
0
%Insu�icient or no progress
Côte d’Ivoire
GuineaNigeria
GhanaNiger
Liberia
Senegal
Burkina Faso
Sierra LeoneMali
ChadTogo
Cabo Verde
Mauritania
GambiaBenin
Guinea-Bissau
585656
535050494949484747
454545
3938
Stunting impairs the physical and cognitive development of children and is largely irreversible aft er the age of two years. it therefore reduces the capacity of individuals and plays a role in keeping entire societies in poverty.
led by the african Union (aU), the Un economic commission for africa (Uneca) and the World food programme (Wfp), the studies on the Cost of Hunger in Africa (coha) in Burkina faso, chad and ghana showed that in 2012, the cost associated with infant malnutrition was equivalent to 6.4%, 9.6% and 7.7% of gdp, or a total amount of eUr 3.9 billion for the three countries. good nutrition plays a role in the economic development of a country and off ers opportunities for generating additional revenues (table 1). according to prof. hoddinott, interventions that prevent malnutrition are excellent investments: "For a typical African country, each uS dollar invested in reducing the chronic undernourishment of children generates uSd 16 in return".

1. SociAl Protection: a KeY element in improVing reSilience & nUtrition
Social protection"a set of non-contributory transfers and services (support for the most vulnerable) as well as other contribution-based social benefits (pensions, unemployment insurance, etc.). its purpose is to promote livelihoods, risk prevention, protection for the most vulnerable in addition to the structural transformation of vulnerability factors."
Regional Agency for Agriculture and Food (RAAF/ECOWAS)
non-contributory social transfers (also known as social safety nets) have produced good results in terms of nutrition and household resilience. they can have an impact on the three levels of causes presented in the conceptual framework for malnutrition (figure 3).
in terms of the underlying and root causes, targeted (non-contributory) social transfers to vulnerable populations can make up for a lack of resources, help reduce poverty and food insecurity and improve purchasing power. this can translate into better access to health services, improved capacity to care for young children, an enhanced food regime for individuals and better overall nutrition.
as regards the immediate causes, social transfers can have a more direct impact on food intake for individuals by providing suitable food supplements, for example. Some social transfers have more potential to reduce undernourishment than others. Subsidised food sales aimed at improving access to food (by increasing the purchasing power of households) do not oft en produce good results in terms of food and nutrition and rarely benefit the poorest households. in a case study conducted in West africa, their cost eff ectiveness was shown to be lower than that of targeted cash transfers.1
generally speaking, cash transfers produce better results when they include or are combined with specific nutrition measures such as food supplements, behaviour change communication, or mandatory visits to eff ective health care facilities.2
in the case of nutrition-focused social transfers, eligibility must reflect the most aff ected populations or areas and the most vulnerable groups. Such groups may include pregnant women, children under the age of two, or more generally young children and women of childbearing age; it may also target a region with especially high numbers or prevalence rates of malnutrition.3
1 alderman, h. (2015), Leveraging social protection programs for improved nutrition, Summary of evidence prepared for the global forum on nutrition-sensitive social protection programmes, World Bank; jayasinghe, d., crosby, l. & hypher, n. (2012), A chance to grow – How social protection can tackle child malnutrition and promote economic opportunities, Save the children UK; gentilini, U. (2016), The revival of the ‘cash versus food’ debate: new evidence for an old quandary?, World Bank.2 alderman, h. (2015), idem; jayasinghe, d., idem; Bailey, S. & K. hedlund (2012), The impact of cash transfers on nutrition in emergency and transitional contexts - A review of evidence, odi et premand, p. & al (2016), Transferts monétaires, valeur ajoutée de mesures d’accompagnement comportemental et développement de la petite enfance. rapport descriptif de l’évaluation d’impact à court terme du projet filets sociaux au niger, World Bank.3 alderman, h. (2015), idem ; freeland, n. & c. cherrier (2015), Social protection and nutrition – Guidance note, dfat.
Figure 3 conceptual framework for malnutrition
PANEl 1: liNKS BEtWEEN SoCiAl ProtECtioN ANd NutritioN
• Which social protection levers can play a role in improving nutrition?• Which social protection measures are more promising in terms of improving nutrition and resilience?• Which instruments are common to social protection and nutrition actors? • What synergies exist between these two sectors that seem important to develop in order to improve nutrition?
Box 3
MALNUTRITION & CONSEQUENCES
Inadequate food intake Diseases
Food insecurity at the household level
Inadequate care Inadequate hygiene and
health care services
POVERTY
IMMEDIATE CAUSES
Lack of natural, financial, human and institutional
resources
Social, economic and political context
UNDERLYING CAUSES
ROOT CAUSES
Beyond targeting, the size of transfers, frequency and programme coverage are key factors that determine the impact of social transfer programmes on nutrition objectives. providing significant transfers that are suff iciently frequent, regular and predictable; placing them under the control of women; and combining them with nutrition support measures are the key factors for success.4
4 jayasinghe, d., crosby, l. & hypher, n. (2012), A chance to grow – How social protection can tackle child malnutrition and promote economic opportunities, Save the children UK ; freeland, n. & cherrier, c. (2015), idem.
?

2. WeSt AfricAn exPerienceS in the field of Social protection for nUtrition & reSilience
A. Expanding non-contributory social protection
over the past decade, most countries in the region have developed a social protection policy or national strategy. at the regional level, ecoWaS has expressed an interest in developing a regional social protection strategy. in december 2012, ecoWaS adopted a general convention on Social Security aimed at ensuring effective co-ordination of the social security systems of its member States (to enable migrants who have worked in one of the member States to exercise their right to social security in their country of origin). through its regional agency for agriculture and food (raaf) and its directorate for Social and humanitarian affairs, ecoWaS also supports the development of a regional mechanism for enhancing social transfer expertise.
existing protection measures include free health care for children under the age of 5 in Burkina faso, chad, niger, and Senegal. a number of countries in the region are working toward universal health coverage (Benin, Burkina faso, côte d’ivoire, ghana, niger and Senegal).
national social cash transfer programmes have also been developed (for example, in Burkina faso, mali, niger and Senegal), sometimes in the form of public works programmes (ghana and Sierra leone). despite this rapid development, programme coverage is still limited. for example, in Senegal in 2016, 180 000 households (or roughly 7.5% of the total population) were covered by the national family Security allowance programme (pnSBf). Based on selective criteria such as income levels, school enrollment and attendance, the programme aims to "combat social injustices and inequalities for a better distribution of national wealth". however, these national programmes still heavily rely on external funding sources. Gradually increasing the percentage contributed by the State is a major challenge to ensuring the sustainability of these promising initiatives.
in addition to financial constraints, the development of these systems involves technical challenges, in particular as regards targeting, which is a key issue in the context of limited resources. however, the relevance of narrow targeting can be called into question, given the tremenduous nutrition and resilience challenges in the region.
to improve targeting, unique national registers of vulnerable persons have been put in place in Benin and Senegal, and a number of other countries intend to advance in this area (Burkina faso, chad, niger, mali and mauritania).
Benin National social protection strategy (2014)
Burkina Faso National social protection strategy (2012)
Chad National social protection strategy (2015)
Côte d'Ivoire National social protection strategy (2013)
Ghana National social protection strategy (2007)
Guinea National social protection strategy (2016)
Liberia National social protection strategy/programme (2013)
Mali National social protection strategy (2002); National action plan to expand social protection (2011-15)
Mauritania National social protection strategy (2014)
Niger National social protection strategy (2011)
Nigeria National social protection strategy (2016 - draft)
Senegal National social protection strategy (2013-17)
Sierra Leone National social protection strategy (2015)
Togo National social protection strategy (2015)
Table 2national social protection policies or programmes
B. National systems for preventing and managing social transfer crises
Since 2012, most Sahelian countries have developed an annual national crisis response plan (or a response plan for food and nutrition security) based on the results of the Cadre harmonisé, in an effort to address food and nutrition crises in the region. these plans include an emergency social transfer component. crisis response tools (traditionally based on more or less targeted food distribution and the sale of subsidised food) are increasingly diversified and targeted. the use of cash transfers becomes more and more popular. these new practices, as well as new long-term social transfer programmes and insurance schemes such as africa risk capacity (arc), are quite promising in terms of strengthening resilience and food and nutrition security in the region. their very existence calls for changes to the national and regional response mechanisms. Some countries have started reforming or revitalising their crisis response system (notably mali, niger and Senegal) in order to improve targeting of the most vulnerable and strengthen the links between emergency and long-term responses.
according to estimates, about 6 million people per year require emergency food aid in the Sahel area (Burkina faso, chad, niger, mali, mauritania and Senegal). as needs can be partially forecasted and are tied to root causes, regular national social transfer programmes would be more appropriate and effective in terms of strengthening resilience and nutrition.
Whether long-term social transfer programmes are a component of crisis response systems or whether crisis response mechanisms are part of the structure responsible for social protection (as is the case in Senegal), it is vital to ensure consistency between emergency responses and long-term social assistance programmes.

C. Social protection initiatives for strengthening resilience and improving nutrition
in addition to emergency response systems, national frameworks now exist that link social protection, nutrition and resilience. these include national resilience priorities (nrp-agir), multi-Sector Strategic plans for nutrition, and social protection strategies/policies that include a specific food and nutrition security component.
the social transfer programmes resulting from these different frameworks are beginning to produce results. evidence from the field shows that transfers have a bigger impact on nutrition and resilience in the region if they are part of an integrated approach that addresses the different causes of malnutrition and food insecurity. in niger, cash transfers include behavioural support measures (nutrition, health, psychosocial stimulation) that are improving exclusive breastfeeding and supplementary feeding practices. they are also playing a role in improving food security for children. Behavioural changes have also been observed in terms of preventive health care, but are more
subtle. Supplementary measures are needed to achieve greater impact in terms of the quality of basic social services, home visits, increased level and frequency of activities, etc .1
the evaluation of the cash transfer programmes in niger suggests that these programmes can have a lasting impact on productive investment in the most disadvantaged. indeed, sustained increases in the levels of livestock ownership and participation in tontines were seen 18 months after the benefits programme was launched.2
despite the magnitude of the need and encouraging results, the setting-up of social transfers that target nutrition and resilience is advancing only slowly, largely due to financial constraints.
1 premand, p. & al (2016), Transferts monétaires, Valeur ajoutée de mesures d’accompagnement comportemental, et développement de la petite enfance. rapport descriptif de l’évaluation d’impact à court terme du projet filets sociaux au niger, World Bank.2 Stoeffler, Q., mills, B. & premand, p. (2016), Poor Households’ Productive Investments of Cash Transfers: Quasi-experimental Evidence from Niger, World Bank.
PANEl 2: SuCCESS StoriES ANd iNNovAtivE ExPEriENCES
• What social protection issues are linked to nutrition, crisis management and resilience building?• Which innovative social protection experiences targeting nutrition and resilience have strong potential? • What lessons can be drawn from experiences in the Sahel and West africa in terms of: → cash transfer support measures for strengthening nutrition security? → ways to improve inter-sectoral co-ordination and develop synergy between emergency & development actors? • are there any social protection and nutrition measures that have been shown to work in the region?• how and to what degree could they be implemented on a large scale?
?

3. SuStAinAble funding for Social protection & nUtrition
the level of public funding for social protection is particularly low in Sub-Saharan africa. in chad (1.2%), côte d’ivoire (1.9%), nigeria (2.8%) and niger (2.7%), for example, it falls far below the global average of 8.7% of gdp and below the Sub-Saharan average of 4.1%.1 Similarly, overall investment in nutrition is not sufficient to put an end to this scourge. in Burkina faso, a recent study showed that investment in nutrition represented a mere
1 drouin a., Bit (2014), Un financement des socles nationaux de protection sociale réalisable à moyen terme, conférence du conseil économique et social pour l’afrique francophone portant sur les socles nationaux de protection sociale.
0.6% of gdp in 2014 and 20152, well below the 3% recommended by the federation of african nutrition Societies (fanUS). at the same time, national governments and their partners mobilise significant funds each year for emergency responses, funds that could otherwise be better invested in more predictable, sustainable and long-term responses.
2 reSonUt (2016), Analyse des allocations budgétaires et des dépenses annuelles du gouvernement pour les interventions spécifiques et sensibles à la nutrition.
investing in social protection and nutrition is a challenge for low-income countries. the magnitude of this challenge becomes clear when the cost of inaction is evaluated in social, human and economic terms, which is much higher.
in addition to the consequences for nutrition, social protection is both an investment in people and in the economy. it generates productivity gains and gives rise to new markets and increased domestic demand, which stimulates economic growth. a study of seven cash transfer programmes in Sub- Saharan africa has shown that all seven generated significant spin offs in the local economy; each dollar transferred to a poor household brought in between USd 1.27 and USd 2.52 in total revenue for the local economy.1 Small-scale farmers and small businesses tend to benefit because poor households buy most of their goods from them.2 Social protection also reduces inequality, which leads to better economic results and greater national stability.
during the 2008-09 global economic crisis, studies showed the need to invest in social protection, and in non-contributory social transfers in particular, to support the resilience of the most vulnerable households confronted with food price increases in West africa.3 these households are hit harder and, without aid, the negative consequences persist in the long term (erosion of productive and human capital and therefore resilience).
1 thome, K., taylor, e., filipski, m., davis B. and handa, S., fao (2016), The Local Economy Impacts of Social Cash Transfers: A Comparative Analysis of Seven Sub-Saharan Countries.2 davies, S.and davey, j. (2008), A regional multiplier approach to estimating the impact of cash transfers on the market: The case of cash transfers in rural Malawi. development policy review, Vol. 26, no. 1, pp. 91-111.3 oxfam & al. Save the children (2008), Rising food prices in the Sahel, the urgency of long-term action.
A. the cost of inaction B. Securing new resources and allocating existing resources differently
Social transfers that target the most vulnerable are more cost effective.
Simulated change in poverty gap resulting from the global crisis and alternative social protection measures costing 1% of gdp, 2009. a study simulated the impact of the 2008 global food crisis on children and the cost effectiveness of two kinds of measures: food subsidies and cash transfers targeting households living below the national poverty line. the study suggests that in all three countries targeted cash transfers would be much more cost effective than food subsidies. Sources: cockburn & al., 2010); dfid (2013)
Box 4
1.5
2
-1.5
-1
-0.5
No social protection measures
Food subsidies
0
11
0.5
Burkina Faso Cameroon Ghana
Cash transfers targeted to vulnerable populations
2.2
1.6
-0.3
1.0 0.9
-1.5
1.0
-0.3
1.0
the notion that investing in basic social protection is not affordable is a preconceived idea. in some countries, public budgets are able to provide their poorest residents with support.
according to Unocha, donors mobilise more than USd 1 billion per year for the emergency response in the Sahel (USd 1.16 billion in 2012, USd 1.04 billion in 2013 and USd 1.24 billion in 2014 - these figures do not include the contributions made by national governments, which is not negligible, although not documented at the regional level). these amounts are mobilised to address humanitarian challenges of increasing complexity due to recent conflicts, and to meet the food and nutrition needs of people who experience structural vulnerability. needs are tied to seasonal food and nutrition insecurity that is severe, but in reality, chronic, and are not covered by development programmes. despite colossal budgets, it is important to note that each year, the humanitarian needs identified are never fully covered. nearly three million people per year who require food assistance do not receive it.
C. Comparative advantage of social protection for nutrition versus emergency responses
Most food and nutrition insecure people in the region regularily find themselves in that situation due to structural factors. in such a context, setting up planned social transfer programmes has a number of advantages as compared with humanitarian aid, as the resources available for the latter are ad hoc and unpredictable. Scheduled social transfers make it possible to avoid implementing adverse coping mechanisms and guarantee access to food and minimum basic services at the height of the lean season. regular transfers also provide the most vulnerable households with the security that enables them to more easily invest in the future.
lastly, in the medium term, the percentage of budgetary allocations for administrative costs of social transfer programmes decrease as programmes are scaled-up. over time, they therefore become less costly than humanitarian food aid programmes, which oft en involve very high operating costs.
PANEl 3: SuStAiNABlE FuNdiNG For SoCiAl ProtECtioN PoliCiES
• are there any estimates comparing the costs of implementing and scaling up social protection systems that target nutrition and resilience-building versus the social, human and economic costs of failing to implement such systems?
• how are social protection measures for the most vulnerable currently funded? What measures are in place (or planned) to secure sustainable and sovereign funding in the medium or long tem?
• What innovative experiences with sustainable and sovereign funding (insurance mechanisms, innovative tax regimes) have been successful in the region and how could they be scaled up?
?
� for example, mauritania used its own resources to fund 84% of the cost of its social assistance programmes (including general subsidies for energy products).1 fuel subsidies are also available in cameroon and Sierra leone. But general subsidies (for food and energy products) are costly and oft en inadequate in terms of reaching the poor.2 rationalising programmes and subsidies may help increase the budgetary resources available for more eff ective social transfer programmes that target the most vulnerable.
in low-income countries with high rates of poverty it is still essential in the short and medium-term to attract financial resources from partners to ensure basic social protection programmes are put in place, with a view to stepping up public funding in the future. according to the World Bank, development partners currently provide 80% of the funding for social safety
1 dickinson, t. (2013), République Islamique de Mauritanie, programmes de filets sociaux, World Bank.2 monchuk, V. (2014), Réduire la pauvreté et investir dans le capital humain : le nouveau rôle des filets sociaux en Afrique, case studies in 22 countries, World Bank.
nets in Burkina faso, 60% in mali and close to 70% in niger.3 aid from donors is still essential in these countries, particularly in the start up phase of national social transfer programmes which is quite costly.
lastly, there are existing sources of funding in all countries that could be mobilised at the national level to fund social protection and nutrition in a specific and sustainable manner. in conjunction with reallocating food and energy subsidies, a number of other sources could be put to use, such as increasing the tax revenue from new sectors (telephony or mineral resources). for example, the value of niger's only export products, namely uranium and oil, has increased by eUr 400 million since 2006.4 combating fraud or restructuring public debt are other possible options to explore in terms of making available additional funds.
3 Stührenberg, l. & pelon, V. (2014), Les obstacles à la protection sociale contre la faim : vrais défis et faux problèmes, inter-réseaux.4 idem
UEMOA
ClubSAHEL ANDWEST AFRICA
Secretariat