annual non-communicable diseases (ncd) program report … ministry of health reports... · chronic...
TRANSCRIPT
KINGDOM OF SWAZILAND
MINISTRY OF HEALTH
SIY I N Q A B A
ANNUAL NON-COMMUNICABLEDISEASES (NCD) PROGRAM REPORT
Strategic Information Department
2015Monitoring & Evaluation Unit

This publication was produced with the support of the United States Agency for International Development (USAID) under the terms of MEASURE Evaluation cooperative agreement AID-0AA-L-14-00004. Views expressed are not necessarily those of USAID or the United States government

TABLE OF CONTENTS
LIST OF ACRONYMS......................................................................................................................................vACKNOWLEDGEMENTS...............................................................................................................................viEXECUTIVE SUMMARY................................................................................................................................viiNCD Key Indicators....................................................................................................................................viii
CHAPTER 1: Overview....................................................................................................................11.1. The Burden of NCDs risk factors in Swaziland.............................................................21.2. PURPOSE AND SCOPE of the report.............................................................................41.3. Data Sources...................................................................................................................41.4. Report Writing Process..................................................................................................51.5. Structure of the report...................................................................................................5
CHAPTER 2: NCDs Prevention and Control in Swaziland...........................................................62.1. The NCD Prevention and Control Program.................................................................72.1.1. Program Management..................................................................................................7
CHAPTER 3: Program Results........................................................................................................83.1. NCDs morbidity and mortality......................................................................................93.1.1. Morbidityt due to NCDs.................................................................................................93.1.2. In Patient Morbidity.....................................................................................................103.2. Top 4 NCDs Morbidity and Mortality in Swaziland....................................................113.2.1. Mortality due to NCDs.................................................................................................113.3. Morbidity and Mortality of Cardio-vascular diseases .............................................123.3.1. Cardio-vascular diseases by sex................................................................................133.3.2. Mortality by Cardio-Vascular Disease by sex.............................................................143.4.2 Morbity and Mortality due to Cancer.........................................................................153.5. Morbidity and mortality due to DIABETES mellitus..................................................163.5.1 Diabetes at Out Patient................................................................................................163.5.2. Mortality due Diabetes................................................................................................173.6. Chronic Obstructive Pulmonary Disease...................................................................173.6.1. Morbidity due to Chronic Obstructive Pulmonary Disease.....................................173.7. MENTAL DISORDERS....................................................................................................203.7.1. Morbidity due to Mental disorders............................................................................203.7.2. Mental disorders at In-Patient....................................................................................203.8. Oral Health...................................................................................................................213.8.1. Morbidity due to Oral Health.....................................................................................213.9. EYE AND EAR HEALTH..................................................................................................213.9.2. Morbidity due to Ear related Disease trends.............................................................223.9.3. Eye related cases..........................................................................................................23
CHAPTER 4: PROGRAM ACHIEVEMENT AND BEST PRACTICES.................................................24
CHAPTER 5: CONCLUSIONS AND RECOMMENDATIONS..........................................................275.1. Conclusions...................................................................................................................285.2. Action Points.................................................................................................................28
ANNEXURES..................................................................................................................................29
DEFINITION OF TERMS.................................................................................................................30

List of FiguresFigure 1: Percentage who currently smoke tobacco 2007-2014 STEPS survey..............................................2Figure 2: Status of harmful use of alcohol in Swaziland by sex,2014 STEPS survey....................................2Figure 3: Percentage of people who ate less than 5 combined servings of fruit and or vegetables on average per day by sex 2014 STEPS survey....................................................................................3Figure 4: Percentage of people not engaging in vigorous activity 2014 STEPS survey...............................3Figure 5: Avarage waist circumference(cm) for males and females 2007-2014 STEPS survey.....................4Figure 6: Top ten leading conditions at OPD, 2015..........................................................................................9Figure 7: Non-Communicable Diseases at OPD,2015........................................................................................9Figure 8: Top ten leading causes of admission...............................................................................................10Figure 9: NCDs at In-patient in 2015.................................................................................................................10Figure 10: Morbidity of In-patients due to NCDs, 2015......................................................................................11Figure 11: Number of in- patient deaths due to non-communicable disease by sex, 2015..........................12Figure 12: Top ten leading Cadio Vascular Diseases..........................................................................................13Figure 13: Cardio vascular disease by sex 2015..................................................................................................14Figure 14: Percentage of Cardio-vascular disease by sex 2015.......................................................................14Figure 15: Top ten leading conditions of cancer 2015......................................................................................15Figure 16: Number of deaths due to cancer, by sex, 2012-2015......................................................................15Figure 17: Leading types of cancer that lead to death 2015.............................................................................16Figure 18: Diabetes related deaths by sex.........................................................................................................17Figure 19: Chronic obstructive pulmonary diseases at in-patient 2015..........................................................18Figure 20: Number of Chronic obstructive pulmonary diseases related deaths by sex, 2015......................18Figure 21: Number of Epilespsy cases at OPD 2005-2015.................................................................................19Figure 22: Ear related cases at OPD by age, 2010-2015.....................................................................................22Figure 23: Eye related cases attended in the Out-patient department by age-group, 2010-2015................23
List of TablesTable 1: Diabetes at Out-patient by Age, 2015....................................................................................................17Table 2: Epilepsy cases attended at Outpatient department by sex, 2015......................................................19Table 3: Mental disorders by age and sex at OPD, 2015....................................................................................20Table 4: Mental disorders at In-patient segregated by sex, 2015....................................................................21Table 5: Oral health problems and dental carries at OPD................................................................................21Table 6: Eye and Ear related cases at OPD by sex, 2015.....................................................................................22

LIST OF ACRONYMS
AIDS Acquired Immunodeficiency Syndrome
BMI Body Mass Index
COPD Chronic Obstructive Pulmonary Diseases
CVDs Cardiovascular diseases
HIV Human Immunodeficiency Virus
HMIS Health Management Information System
MoH Ministry of Health
NCDs Non-Communicable Diseases
NGOs Non-Governmental Organizations
OPD Out-Patient Department
RH Reproductive Health
TB Tuberculosis
TWG Technical Working Group
WHO World Health Organization

ACKNOWLEDGEMENT
The National Prevention and Control of Non-Communicable diseases programme annual 2015 would not have been possible without the leadership of the NCD Program,stakeholders and the Strategic Information Department which consists of the HMIS and the M&E unit. The Institute of Health Measurement supported the NCD program in writing this report both technical and financial.
The report writing process involved a wide stake-holder: namely, Diabetes Swaziland, MSH, Hope House, CANASWA, Swaziland Epilepsy Organization, National Pyschatric Hospital and WHO.
Lindiwe Tsabedze-Sibanyoni- NCD ProgramDr. K Makadzange- WHODumsile Mavuso- Diabetes SwazilandXolisile Dlamini- MOH Cancer RegistryMacg-man Mahlalela- Swaziland Epilepsy Organization.Thulani Dlamini- MoH SID M&ETengetile Tsabedze- IHM

EXECUTIVE SUMMARY
NCDs are caused, to a large extent, by four behavioural risk factors that are pervasive aspects of economic transi-tion, rapid urbanization and 21st-century lifestyles such as tobacco use, unhealthy diet,insufficient physical activity and the harmful use of alcohol. The program has made huge achievements in promoting a healthy lifestyle at community level, particularly the work of Diabetes Association of Swaziland and other stakeholders.
The data shows that in 2015, more females died due to NCDs when compared to males, however males were more likely to die of communicable diseases. The effect of NCDs on women is in line with WHO surveys and estimates, which point to NCDs affecting more females than males. Of the top 10 leading causes of admission in 2015, NCDs account for 15% of all top ten inpatient admissions.Of the 15% of in-patients admitted to health facilities in 2015, 9 % were as a result of Diabetes Mellitus whilst essential hypertension accounted for 6% of all admissions.Cancer presents one of the top NCDs leading causes of mortality amongst the admissions attended in 2012 to 2015. There is an increase in the number of recorded deaths due to cancer for both males and females. Data from 2015 indicates that 3 major cancers that account for 60 percent of all deaths due to cancer in the country which are cervical cancer , cancer of the liver and bile duct and prostate cancer.
The Ministry of Health needs a strong interest to start a vigorous program which will encourage lifestyles that will help in preventing these illnesses through a multi-sectorial involvement which can be intergrated into the existing health system. The program needs to continue to improve in diabetes management due to the fact that the number of patients seen for diabetes mellitus is increasing; however the deaths are declining.
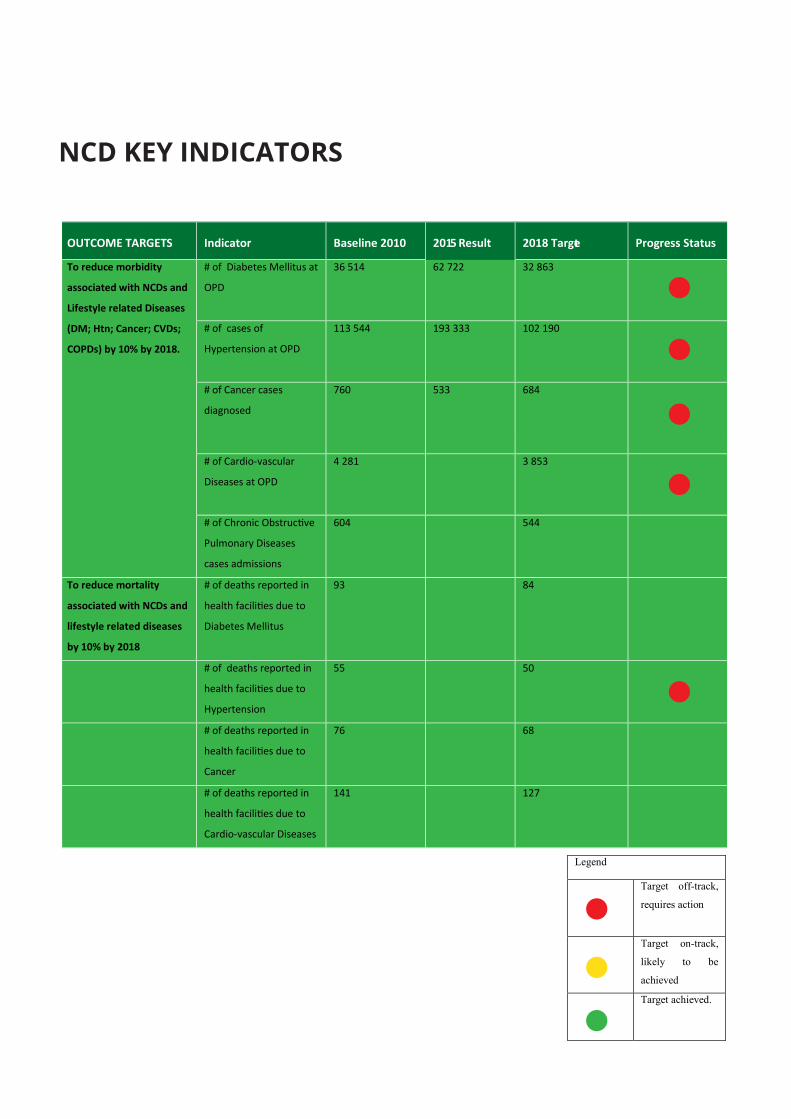
NCD KEY INDICATORS
OUTCOME TARGETS
Indicator
Baseline 2010
2015 Result
2018 Target
Progress Status
To reduce morbidity
associated with NCDs and
Lifestyle related Diseases
(DM; Htn; Cancer; CVDs;
COPDs) by 10% by 2018.
# of Diabetes Mellitus at
OPD
36 514 62 722 32 863 # of cases of
Hypertension at OPD
113 544 193 333 102 190 # of Cancer cases
diagnosed
760 533
684 # of Cardio-vascular
Diseases at OPD
4 281 3 853 # of Chronic Obstructive
Pulmonary Diseases
cases admissions
604 544
To reduce mortality
associated with NCDs and
lifestyle related diseases
by 10% by 2018
# of deaths reported in
health facilities due to
Diabetes Mellitus
93 84
# of deaths reported in
health facilities due to
Hypertension
55 50 # of deaths reported in
health facilities due to
Cancer
76 68
# of deaths reported in
health facilities due to
Cardio-vascular Diseases
141 127
Legend
Target off-track,
requires action
Target on-track,
likely to be
achieved
Target achieved.
CHAPTER 4:CHAPTER 1:OVERVIEW

Figure 1: Percentage who currently smoke tobacco 2007-2014 STEPS survey
Figure 2: Status of harmful use of alcohol in Swaziland by sex,2014 STEPS survey
Noncommunicable diseases (NCDs) are the leading causes of death globally, killing more people each year than all other causes combined. Contrary to popular opinion, available data demonstrate that nearly 80% of NCD deaths occur in low- and middle-income countries. Despite their rapid growth and inequitable distribution, much of the human and social impact caused each year by NCD-related deaths could be averted through well-understood, cost-effective and feasible interventions. A major reduction in the burden of NCDs will come from population-wide interventions, which are cost effective and may even be revenue-generating, for instance as is the case with tobacco and alcohol tax increases. However effective interventions, such as tobacco control measures and salt reduction, are not implemented on a wide scale because of inadequate political commitment,insufficient engagement of non-health sectors, lack of resources, vested interests of critical constituencies, and limited engagement of key stakeholders. For example, less than 10% of the world’s population is fully protected by any of the tobacco demand-reduction measures contained in the WHO Framework Convention on Tobacco Control.
Non-communicable diseases (NCDs) present an urgent and growing health emergency in countries around the world with evidence showing an ever growing increase in number of deaths due to NCDs coming from middle-income coun-tries. Chronic, non-communicable diseases are responsible for about two thirds of all deaths globally. The main chronic diseases that share the most common risk factors are heart disease; stroke; cancer; chronic respiratory diseases including asthma. The major risk factors for non-communicable diseases are classified into behavioural (modifiable) and biological risk factors. The major behavioural risk factors are: tobacco use; harmful alcohol consump-tion, unhealthy diet (low fruit and vegetable consumption)and physical inactivity. The major biological risk factors are overweight and obesity, raised blood pressure, raised blood glucose andabnormal blood lipids. The major risk factors together account for approximately 80% of deaths from heart disease and stroke.
1.1. THE BURDEN OF NCDS RISK FACTORS IN SWAZILAND The STEPs survey which is a stepwise approach to chronic non-communicable disease risk factor surveillance was carried out from November to December 2014. The target population included both males and females aged 15-69 years and a total of 3 281 people participated in the survey.
11.7%
PERCENTAGE WHO CURRENTLY SMOKE TOBACCO
in 2014
12.9%in 2007
1.2%in 2014
2%in 2007
Source: STEPS survey 2015
Tobacco use
The prevalence of smoking among the adult population in Swaziland stands at 6%. The smoking is higher in males at 12% and only 1.2% in females. Those who smoke daily are at higher risk of developing chronic non-communicable diseases. About 5% of the adult population in Swaziland smoke on daily basis and the average number of cigarettes smoked a day is 5. The majority (93%) of those who use tobacco smoke manu-factured cigarettes. Also of note is the fact that the average age of starting smoking is 19 years.
Harmful use of alcohol
Harmful consumption of alcohol is also a major risk factor for non-communicable diseases. The findings revealed that about three quarters of the adult popu-lation in Swaziland do not drink alcohol. About 60% of adult males compared to 84% of the females do not drink alcohol. The prevalence of alcohol use in Swazi-land therefore stands at 13%. One in every five men drinks alcohol compared to one in every 20 women. About one in every ten adults drinks 6 or more drinks on any occasion with one in every six men compared to one in every thirty women being heavy drinkers.
STATUS OF HARMFUL USE OF ALCOHOL IN SWAZILAND BY SEX, 2014
Source: STEPS survey 2014
22%
3%
5%
15%
5%
1%
2%
3%
5% 10% 15% 20% 25%
Percentage of current drinkers(who drank alcohol in the past 30
days)
Percentage who drank alcohol on 4or more days in the last week
Percentage who drank alcohol daily
Percentage who binge drink (menwho had 5 or more / women whohad 4 or more drinks on any day in
the last week)
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 2

Figure 3: Percentage of people who ate less than 5 combined servings of fruit and or vegetables on average per day by sex 2014 STEPS survey
Figure 4: Percentage of people not engaging in vigorous activity 2014 STEPS survey
Unhealthy diet
Consumption of sufficient amount of fruits and vegetables is key to the prevention and control of chronic non-communicable diseases. On average the adult population consumes one serving of fruits per day for half of the week. People eat about one and half servings of vegetables per day on about 5 days of the week. The majority (92%) of the adult population in Swaziland eat less than five servings of fruits and/or vegetables on average day per day. A fifth of the popu-lation always add salt to food as well as consume processed food high in salt.
PERCENTAGE WHO ATE LESS THAN 5 COMBINED SERVINGS OF FRUIT AND/OR VEGETABLES ON AVERAGE PER DAY BY SEX
92.5%in 2014
89.6%in 2007
91.7%in 2014
85.6%in 2007
Source: STEPS survey 2015
Physical Inactivity
Sufficient physical activity defined as more than two and half hours of moderate-intensity activity per week is needed to reduce the risk of developing chronic non communicable diseases. However one in every six adults in Swaziland has sufficient physical activity. One in every ten men compared to one in every five women lacks sufficient physical activity. About half of the adult Swazi population is not engaging in vigorous activity. This is higher in women whereby about two thirds of women do not engage in vigorous physical activity compared to one third of men.
29%in 2014
39%in 2007
62%in 2014
58%in 2007
Source: STEPS survey 2015
Cervical cancer screening
Access to cervical cancer screening is necessary for the prevention and control of one of the leading cancers in Swaziland. To date about one in every five women aged 30-49 years has ever had a screening test for cervical cancer.
Physical measurements
Physical measurements reveal the biological risk factors for chronic non-communicable diseases which include overweight and obesity as well as raised blood pressure. The average body mass index among the adult population stands at 25.7 kg/m2 being 23.5 kg/m2 in men and 27.5 kg/m2 in women. About half of the adult population is overweight. One quarter of adult males compared to two thirds of women are over-weight. About one fifth of the population is obese, one tenth of men and one third of women. The average waist circumference is 79cm in men and 86.6cm in women.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 3
PERCENTAGE OF PEOPLE NOT ENGAGING IN VIGOROUS PHYSICAL ACTIVITY, 2007-2014, STEPS SURVEY

Figure 5: Avarage waist circumference(cm) for males and females 2007-2014 STEPS survey
Cervical cancer screening
Access to cervical cancer screening is necessary for the prevention and control of one of the leading cancers in Swaziland. To date about one in every five women aged 30-49 years has ever had a screening test for cervical cancer.
Physical measurements
Physical measurements reveal the biological risk factors for chronic non-communicable diseases which include overweight and obesity as well as raised blood pressure. The average body mass index among the adult population stands at 25.7 kg/m2 being 23.5 kg/m2 in men and 27.5 kg/m2 in women. About half of the adult population is overweight. One quarter of adult males compared to two thirds of women are over-weight. About one fifth of the population is obese, one tenth of men and one third of women. The average waist circumference is 79cm in men and 86.6cm in women.
Biochemical measurements
The prevalence of raised blood pressure among the adult population is 25% .Of the people with raised blood pres-sure about 80% of them are not on medication which is 87% in male and 72% in female. Raised blood sugar and cholesterol contribute towards the development of non-communicable diseases. The average blood sugar level among the population is 5.1 mmol/l. The prevalence of raised blood sugar in 10% which is the same as the preva-lence of raised cholesterol.
1.2. PURPOSE AND SCOPE OF THE REPORT
This report focuses on the prevention and control of NCDs in Swaziland with a focus on the interventions targeting the major risk factors.The purpose of this report is to present the performance of the NCD Program that will be useful to policy makers, program managers, and other stakeholders. The major aim of this report is to present a trend of the mortality and morbidity caused by NCDs in Swaziland. The report is in line with international perfor-mance targets as set by WHO, and also as stipulated in National Health Sector Strategic Plan(NHSSP II).
While this report is not designed to provide complex analysis due to various constraints, it indicates areas where more detailed, complex analysis would be fruitful. The data are presented in terms of national level statistics and for population subgroups such as those defined by age, and sex. Where necessary and appropriate, further data analysis and disaggregation will be shown. It is intended that this report will continue to be produced annually in order to identify trends and changes over time. Some elements of the report will include trend analysis for the period 2010-2015 where data is available.
1.3. DATA SOURCES
The Health Management Information System (HMIS) database was used as the main source of the service delivery results. The results are based on data collected routinely from 2010 to 2015. NCD data is collected routinely through HMIS which involves the use of facility based registers for out-patient and in-patient. out-patient data is case based where in-patient is client or individual based. In-patient data is captured at both facility and regional level by health information officers, while out-patient data is submitted monthly as a summary to the regional SID offices for capturing into an electronic system.
79.4cm
AVERAGE WAIST CIRCUMFERENCE (CM) FOR MALES AND FEMALES
in 2014
81.2cmin 2007
86.6cmin 2014
82.4cmin 2007
Source: STEPS survey 2014
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 4

1.4. REPORT WRITING PROCESS
The report writing process began with the programme stating the need for the annual report. The program along-side SID reviewed the required data sources, including key performance indicators. Relevant data was extracted from the HMIS and cleaned by the Data Management Committee.
A data analysis and report writing workshop was conducted in April 2016. The team included NCD program, Strate-gic Information Department (SID), Institute for Health Measurement (IHM), and other stakeholders.
1.5. STRUCTURE OF THE REPORT
The report is structured by disease mortality and morbidity of NCDs. The first part of the report focuses on review-ing the trends on mortality and morbidity caused by NCDs. The report then focuses on service interventions, and finally ends with conclusions and recommendations.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 5

CHAPTER 4:CHAPTER 2:NCDS PREVENTION AND CONTROL IN SWAZILAND

2.1. THE NCD PREVENTION AND CONTROL PROGRAM
2.1.1. PROGRAM MANAGEMENT
The National diabetes prevention and control unit was established in 1999, but due to other emerging non-communicable diseases, this unit gave birth to a National Prevention and Control of Non Communicable Diseases Programme. Currently the NCD programme receives the majority of its funding from the Government of Swaziland. Currently the NCDs programme offices are situated in Manzini. There is a national NCD programme manager who is supported by 6 technical staff members and other support staff. The programme works in collaboration with international partners,Non governmental organization, community based organizations and other government sectors.
The operations of the programme are guided by the National NCDs prevention policy, strategic plan and technical working group. Currently surveillance data for NCDs is managed through the Health Management Information System (HMIS), which covers largely the data from health facilities. Population level data is collected through surveys. However, limitations still exist in NCD data availability and management.
Non Communicable Diseases programme mainly focuses on the following conditions;
• Cardiovascular diseases CVDs, • Diabetes mellitus,• Cancer, • Chronic obstructive pulmonary diseases and • Epilepsy.
Other service delivery interventions include the following conditions; • Mental health, • Ear and eye health and, • Oral health.
Vison, Goal and Objectives
The NCD programme is founded on the following mission and vision;
Vision: An empowered population where NCDs are no longer a major public health problem
Mission: To improve the health of the Swaziland population by reducing the burden of NCDs through prevention and control targeted interventions.
The Goal of the NCD programme is to reduce NCD related morbidity, disability and mortality and to achieve this goal the programme has in their strategic plan come up with the following objectives.
1. To sustain government commitment to NCDs at all levels.2. To reduce modifiable risk factors for NCDs and create a safe and health promoting environment3. To strengthen and orient health systems to address the prevention and control of non-communicable
diseases and the underlying social determinants through people-cantered primary health care and univer-sal health coverage.
4. To establish mechanisms for multi-sectorial coordination and partnership for prevention, treatment, care and rehabilitation of NCDs.
5. To promote and support national capacity for high-quality research and development for the prevention and control of Non Communicable Diseases.
6. To monitor the trends and determinants of Non Communicable Diseases and evaluate progress in their prevention and control.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 7

CHAPTER 4:CHAPTER 3:PROGRAM RESULTS

Figure 6: Top ten leading conditions at OPD, 2015
Figure 7: Non-Communicable Diseases at OPD,2015
3.1. NON-COMMUNICABLE DISEASES MORBIDITY AND MORTALITY
Non-communicable diseases (NCDs) present an urgent and growing health emergency in countries around the world with evidence showing an ever growing increase in number of deaths due to NCDs coming from middle-income countries. In Swaziland, NCDs account for 28 percent of total annual deaths (WHO NCD country profile 2014). According to WHO estimates, Swazis suffer mainly from diseases of lifestyle such as cardiovascular diseases, type 2 diabetes, cancer and chronic respiratory diseases..
3.1.1. MORBIDITYT DUE TO NCDS
The bar chart shows the top ten leading conditions reported atOut-Patient Department (OPD) in 2015 with Upper respiratory infections having the highest cases. Hypertension presents as the second leading condition at OPD with diabetes mellitus presenting as the ninth leading condition. The other NCD condition that are in the top ten leading conditions include ear problems which is the seventh primary cause of OPD visits in 2015. Skin disorder accounted
Figure 7 reveals that there was 70% other NCD and hypertension accounted for 30% accounted for the other NCDs like epilepsy,diabetes mellitus and hyper-tension. The other NCDs is made up of cancer,cardio vascular diseases and chronic obstructive pulmonary diseases.
Source: HMIS 2015
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 9
421932
193333
168429
140860
135405
110630
110397
101651
62722
58382
Upper Respiratory Infection
Hypertension
Skin Disorder
Acute Watery Diarrhoea
Muskulo Skeletal Conditions
Lower Respiratory Infection (Mild)
Ear Problems
Digestive Disorders
Diabetes Mellitus
Dehydration
TOP TEN CONDITIONS IN OPD 2015
Figure 6 above shows NCDs reported at OPD in 2015 and hypertension had the highest percentange(40%) followed by ear problems (23%) and diabetes mellitus(13%).Other main NCDs like epilepsy,cardiac disease account for 3% and 2% disease burden at OPD respectively. Mental disorders,oral health and dental carries contributes about 19% of cases at OPD combined.
4%
2%
40%
13% 3%
23%
8% 7%
NCD AT OPD, 2015
Mental disorder Cardaic disease HypertensionDiabetes Mellitus Epilepsy Ear ProblemsDental Caries Oral Health Problems

Figure 8: Top ten leading causes of admission
Figure 9: NCDs at in-patient in 2015
3.1.2. IN-PATIENT MORBIDITY
Among the top ten leading conditions at in-patient in 2015, diabetes mellitus ranked as the fifth cause of admis-sion and essential hypertension ranked as the eighth cause of admission at in-patient.
Figure8 above shows that Diabetes Mellitus(1242) and essential hypertension had the highest number of admis-sions at in-patient in 2015 followed by cancers with a total of 510 whilst asthma and epilepsy accounted for 430 and 4286 of in patient admissions respectively.
Source: HMIS 2015
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 10
2503
2119
1571
1319
1242
1235
1111
838
834
776
623
Other Nonifective Gastroenteritis and Colitis
Other Indications For Care or Intervention…
Acquired Immune Deficiency Syndrome
Early or Threatened Labour
Diabetes Mellitus
Spontaneous Abortion
Pulmonary Tuberculosis
Pneumomia, Organism Unspecified
Essential Hypertension
Other Complications Of Labour and Delivery ,…
Cataract
TOP TEN LEADING CAUSES OF IN-PATIENT ADMISSIONS 2015
1242 834
510 430 428
220 107 100
39 36 32 31 22
0 200 400 600 800 1000 1200 1400
Diabetes MellitusEssential Hypertension
CancersAsthma
EpilepsyAffective Psychoses
CardiomyopathySenile and Presenile Organic Psychotic Conditions
HypotensionDrug Dependence
Secondary HypertensionChronic Airways Obstruction, Not Elsewhere Classified
Drug psychoses
No. of admissions
NCD
s at
in-p
atien
t
NCD ADMISSIONS AT IN-PATIENT 2015

NCD'S AT IN- PATIENT 2015
Figure 10: Morbidity of in-patients due to NCDs, 2015
510
1242
613
247
0
200
400
600
800
1000
1200
1400
Cancer Diabetes Mellitus Chronic Pulmnarydisease
Cardio-vasculardisease
Total
3.2. TOP FOUR NCDS MORBIDITY AND MORTALITY IN SWAZILAND
According to the NCD strategic plan there are four major NCDs which are cancers,diabetic mellitus, cardio vascular disease and chronic obstructive pulmonary related diseases which.
are mostly seen at out-patient and they are attributed to the NCDs risk factors which includes tobacco use,harmful use of alcohol, insufficient physical inactivity,obesity, etc. Therefore this section focuses on the four major NCDs.
Diabetes Mellitus had the highest number of in patient admissions in 2015 with a total of 1242 admissions followed by chronic obstructive pulmonary disease (613). Cancers had 510 admissions and the least was cardio-vascular disease(247).This could be attributed to the four behavioural risk factors according to the STEPS survey 2014.
3.2.1. MORTALITY DUE TO NCDS
Measuring the outcomes of admissions in health facilities each year is one of the most important means for assess-ing the effectiveness of a country’s health system.This section seeks to establish mortality due to NCDs .
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 11

Figure 11: Number of in- patient deaths due to non-communicable disease by sex, 2015
The data shows that in 2015 more females died due to the four major NCDs as compared to males, however other studies have shown that males were more likely to die of communicable diseases. The effect of NCDs on females is in line with WHO surveys and estimates, which point to NCDs affecting more females than males. The number of people dying due to diabetes mellitus and cancers is increasing over the years, followed by chronic obstructive pulmonary diseases. The first leading cause of death among the NCDs in 2015 was cardio vascular diseases with a total 123 deaths, cancer(85) and 88 deaths were recorded due to diabetes mellitus.
3.3. MORBIDITY AND MORTALITY OF CARDIO-VASCULAR DISEASES
By definition Cardio- Vascular diseases are conditions that involves narrowed or blocked blood vessels that can lead to heart attack,chest pain or stroke. Globally, Cardio-Vascular Diseases (CVD) is the leading NCD, contributing to 17 million deaths (48% of NCD deaths) annually and 10% of the disease burden (1). Cardio vascular diseases include coronary heart disease, cerebrovascular disease, rheumatic heart disease and are attributed to the major risk factors include tobacco use, physical inactivity, unhealthy diet, obesity, hypertension, diabetes.
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 12
53
10
72
47
32
13
51
41
Cancer COPD Cardio-vascular Diabetes Mellitus
NCD DEATHS AT IN PATIENT BY SEX, 2015
Female Male
TOP TEN LEADING CARDIO VASCULAR DISEASES, 2015
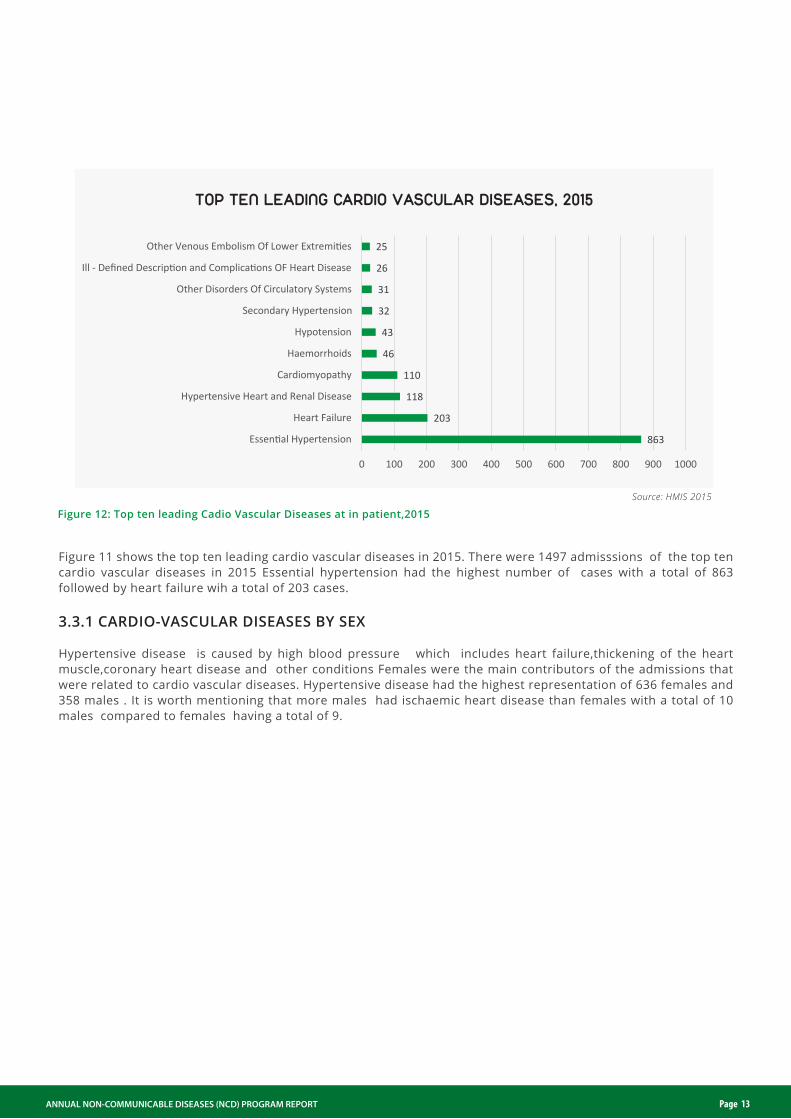
Figure 12: Top ten leading Cadio Vascular Diseases at in patient,2015
863
203
118
110
46
43
32
31
26
25
0 100 200 300 400 500 600 700 800 900 1000
Essential Hypertension
Heart Failure
Hypertensive Heart and Renal Disease
Cardiomyopathy
Haemorrhoids
Hypotension
Secondary Hypertension
Other Disorders Of Circulatory Systems
Ill - Defined Description and Complications OF Heart Disease
Other Venous Embolism Of Lower Extremities
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 13
Figure 11 shows the top ten leading cardio vascular diseases in 2015. There were 1497 admisssions of the top ten cardio vascular diseases in 2015 Essential hypertension had the highest number of cases with a total of 863 followed by heart failure wih a total of 203 cases.
3.3.1 CARDIO-VASCULAR DISEASES BY SEX
Hypertensive disease is caused by high blood pressure which includes heart failure,thickening of the heart muscle,coronary heart disease and other conditions Females were the main contributors of the admissions that were related to cardio vascular diseases. Hypertensive disease had the highest representation of 636 females and 358 males . It is worth mentioning that more males had ischaemic heart disease than females with a total of 10 males compared to females having a total of 9.

PROPORTION OF CVD DEATH BY SEX, 2015
CARDIO VASCULAR DISEASES BY SEX,2015
Figure 13: Cardio vascular disease by sex 2015
Figure 14:Percentage of Cardio-vascular Deaths by sex 2015
Female Male
FemaleMale
636
187
89
11 9 8
358
163
72
9 10 60
100
200
300
400
500
600
700
HYPERTENSIVEDISEASE
OTHER FORMS OFHEART DISEASE
DISEASES OF VEINS& LYMPHATICS &
OTHER DISEASES OFCIRCULATORY
SYSTEM
CHRONICRHEUMATIC HEART
DISEASE
ISCHAEMIC HEARTDISEASE
DISEASES OFARTERIES,
ARTERIOLES ANDCAPILLARIES
57.93%
42.07%
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 14
3.3.2.MORTALITY BY CARDIO-VASCULAR DISEASE BY SEX
The figure on the right shows the proportion of people that died from CVD in 2015.More females died of cardio-vascular disease as compared to males with a percentage of 58% females and 42% males.

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 15
FIGURE 16: NUMBER OF DEATHS DUE TO CANCER, BY SEX, 2012-2015
FIGURE 15: TOP TEN LEADING CONDITIONS OF CANCER AT IN PATIENT, 2015
FemaleMale
134
112
78
38
30
23
13
11
11
9
0 20 40 60 80 100 120 140 160
Malignant Neoplasm Of Cervix Oteri
Malignant Neoplasm Of Prostate
Malignant Neoplasm Of Liver and Intrahepatic Bile Ducts
Malignant Neoplasm Of Oesophagus
Malignant Neoplasm Of Female Breast
Malignant Melanoma of Skin
Malignant Neoplasm Of Rectum, Rectosigmoid Junction and Anus
Malignant neoplasm of lip
Malignant Neoplasm Of Stomach
Malignant neoplasm of bladder
4246
4246
49
56
34
43
2319 20
30
0
10
20
30
40
50
60
2010 2011 2012 2013 2014 2015
Source: HMIS 2015
Source: HMIS database
The major known risk factors of cancer include tobacco use, dietary factors, obesity, physical inactivity,harmful use of alcohol,hormonal and reproductive factors. The malignant neoplasm of the cervix oteri and malignant neoplasm of the prostrate represent the highest among the top ten cancer conditions with 134 and 112 cases repectively.
3.4.2 MORTALITY DUE TO CANCER
Cancer presents one of the top NCDs leads to mortality amongst the admissions attended from 2010 to 2015. There was a slight increase in the number of deaths due to cancer for both males and females.Deaths due to cancer was high in all the years from 2010 as shown in bar chart below and this can be attributed to malignant neoplasm of the cervix oteri. The figure below shows that in 2015 there was an increase in the number of cancer deaths as compared to the previous years (figure16). Deaths due to cancer presents a total 85 deaths and this shows a sharp increase from the previous years(2010-2014)

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 16
Figure 17: Leading types of cancer that lead to death 2015
Cervical
25%
Liver and Intrahepatic bile
19%
Other cancers
14%Prostate
cancer
10%
Skin 6%Oesophagus 5%
5%5%Pancrease
Breast Cancer
Trachea Brochures & Lung
StomachBladder
3%3%
Source: HMIS 2015
The figure above shows that in 2015 there was an increase in the number of cancer deaths as compared to the previous years (figure16). Deaths due to cancer presents a total 85 deaths and this shows a sharp increase from the previous years(2010-2014)
During 2015 a total of number 85 cancer related deaths were recorded, the leading cause of deaths caused by cancer were mainly due to cervical cancer, accounting for 25% of all those reported cancer death, this is followed by liver and intrahepatic bile, which accounts for 19% percent. Prostate cancer which affects mainly males accounts for 19% of the deaths.
3.5. MORBIDITY AND MORTALITY DUE TO DIABETES MELLITUS
The burden of diabetes is increasing globally, particularly in developing countries such as Swaziland. WHO projects that diabetes deaths will double between 2005 and 2030. The causes are complex, but the increase can be attrib-uted to rapid increases in overweight, that can lead to obesity due to physical inactivity. Over time, diabetes can damage the heart, blood vessels, eyes, kidneys and nerves causing chronic illness and early death. Although there is evidence that a large proportion of cases due to diabetes and its complications can be prevented by a healthy diet, regular physical activity, maintaining a normal body weight and avoiding tobacco, however this evidence is not widely implemented.
3.5.1.MORBITY DUE TO DIABETES
MORBIDITY DUE TO DIABETES AT OUT-PATIENT
Throughout the world incidences of diabetes are increasing and consequently so is diabetes among children. Most children are affected by type 1 diabetes. Genetics is a prominent factor as to whether a child will develop diabetes with the risks heightened if the new borns parents or siblings have diabetes. The figure below shows that a total of 62722 cases were atteneded at OPD in 2015 and 119 of the cases were the under 5 population. The above 5 population presented at total of 62603 cases of diabetes.

Table 1: Diabetes at Out-patient by Age, 2015
Source: HMIS 2015
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 17
NUMBER OF DIABETES BY SEX,2011-2015
Figure 18: Diabetes related Deaths by sex 2011-2015
33
25
36
26
4749
58
49
29
41
0
10
20
30
40
50
60
70
,2011 ,2011 ,2013 ,2014 ,2015
Num
ber o
f dea
ths
Female
Male
Source: HMIS 2015
Condition
Age Group Grand Total <5 >5
Diabetes Mellitus 119 62603 62722
3.5.2.MORTALITY DUE DIABETES
Generally, deaths due to diabetes from 2012-2015 have been fluctuating. A sharp increase was observed whereby 45 deaths were reported in 2014 to 88 deaths reported in 2015 with more females dying as compared to males. Females presented a total of 47 deaths and males presented with a total of 41.
3.6. CHRONIC OBSTRUCTIVE PULMONARY DISEASE
Chronic Obstructive Pulmonary Disease (COPD) is a name for a collection of lung diseases which makes it difficult to breathe. Generally, COPD includes diseases such as chronic bronchitis and emphysema. Globally, it is estimated that 4 million people died prematurely from COPD in 2005, and it is projected that the global death rate and burden due to COPD will rank as the third leading cause of death in 2030.
3.6.1. MORBIDITY DUE TO CHRONIC OBSTRUCTIVE PULMONARY DISEASE
The major cause of COPD is tobacco smoke (including passive exposure) and the major risk factors include indoor air pollution, outdoor air pollution as well as occupational dusts and chemicals.
The figure below that most males are affected by COPD in 2015 however most females were affected by asthma.

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 18
COPD IN-PATIENT ADMISSIONS SEX, 2015
PROPORTION OF COPD DEATHS DISAGGREGATED BY SEX,IN-PATIENT 2015
Figure 19: Chronic obstructive pulmonary diseases at in-patient 2015
Figure 20: Number of Chronic obstructive pulmonary diseases related deaths by sex, 2015
Female Male
249
21
75
12
1
2
184
56
80
19
8
2
2
Asthma
Bronchiectasis
Bronchitis Not Specified as Acute or Chronic
Chronic Airways Obstruction, Not Elsewhere Classified
Chronic Bronchitis
Emphysema
Extrinsic Allergic Alveolitis
2.81%
0.00%
2.67%
8.33%
0.00%
0.00%
0.00%
2.78%
1.63%
1.79%
3.75%
26.32%
12.50%
0.00%
0.00%
3.70%
0.00% 5.00% 10.00% 15.00% 20.00% 25.00% 30.00%
Asthma
Bronchiectasis
Bronchitis Not Specified as Acute or Chronic
Chronic Airways Obstruction, Not Elsewhere Classified
Chronic Bronchitis
Emphysema
Extrinsic Allergic Alveolitis
Grand Total
Percentage
Source: HMIS 2015
Source: HMIS 2015
3.6.2 MORTALTY DUE TO CHRONIC OBSTRUCTIVE PULMONARY DISEASE
The figure shows that in health facilities, a total of twenty three (23)deaths were recorded as related to COPD in 2015 (Figure 19). In 2015, there were more female deaths, Chronic Airways obstruction not elsewhere classified had the highest percentage among males compared to females.

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 19
NO. OF EPILEPSY AT OPD CASES 2010-2015
TABLE 2: EPILEPSY CASES ATTENDED AT OUTPATIENT DEPARTMENT BY SEX, 2015
Figure 21: Number of Epilespsy cases at OPD 2005-2015
4132
6741
5539
68416672
1176512659
13748
15759
13053
15291
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Epile
psy
case
s
Source: HMIS 2015
3.6. EPILEPSY
3.6.1 MORBIDITY DUE TO EPILEPSY
Epilepsy is a chronic non-communicable disorder of the brain that can affects people of all ages. Whilst epilepsy can occur at any time in life, 50% of cases begin before the age of 25 years and many in early childhood. It is character-ised by recurrent seizures which are brief episodes of involuntary movements that may involve a part of the body or the entire body accompanied by loss of consciousness and control of the bowel or bladder.
Age -groups Under 5 years Above 5 years
Sex Female Male Female Male
No. Of cases 379 523 6804 7585
Approximately 50 million people worldwide have epilepsy and nearly 80% of the people with epilepsy are found in developing countries. In 2015 more males were attended at OPD with epilepsy than females. The table above also shows that the under 5 males presented with 523 and above 5 population presenting with 7585 cases.
3.6.2 TRENDS OF EPILEPSY SINCE 2005
The figure below shows epilspsy trends over the years and since 2005 there has been a constant increase in the number of epilepsy cases attended at outpatient department..A total of 15291 cases of epilepsy were attended at OPD in the year 2015 showing a slight increase from last year.

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 20
Table 3: Mental disorders by age and sex at OPD, 2015
Diagonisis
> 5 years <5 years
Female Male Female Male
Alcohol Abuse 1 0 0 0
Bipolar Affective Disorder-Mania 213 225 4 10
Cannabis Abuse 91 29 0 0
Cannabis Induced Psychotic Disorder 2431 3409
Mental Disorders 6262 6267 139 186
Schizophrenia 59 40 4 6
Substance Abuse (Heroin,Cocaine,Glue
e.t.c) 10 23 3 4
Grand Total 9067 9993 218 278
Source: HMIS 2015
Since 2005 there has been a constant increase in the number of epilepsy cases attended at outpatient department..A total of 15291 cases of epilepsy were attended at OPD in the year 2015 showing a slight increase from last year.
3.7. MENTAL DISORDERS
3.7.1.MORBIDITY DUE TO MENTAL DISORDERS
The most common mental disorders are schizophrenia, anxiety disorders,dimmentia,alcohol/ drug abuse,psych-social problems leading to depression,suicide and bipolar mood disorder.Mental health according to WHO defini-tion is related to a wide range of symptoms which can characterised by some abnormal thoughts,emotions,behaviour and relationships and all this mental disorders can be successfully treated with time.
3.7.2 MENTAL DISORDERS AT OUT-PATIENT
The table above presents mental conditions seen at OPD. According HMIS there is a variable with mental disor-ders which excludes the other mental conditions as shown in the table and this variable has the highest number of cases seen when compared with the others mental conditions.
3.7.3 MENTAL DISORDERS AT IN-PATIENT
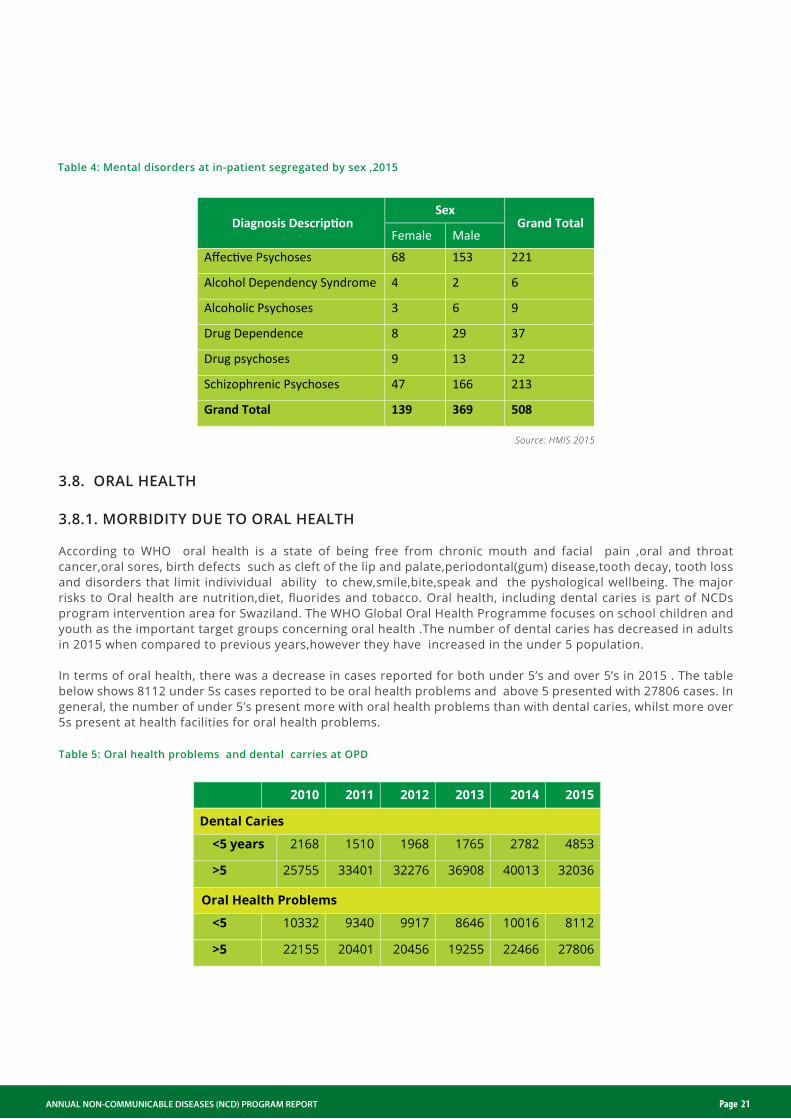
Mental disorders at in-patient included affective psychosis, alcohol dependency syndrome, alcoholic psychosis, drug dependence, drug psychoses and schizophrenic psychosis. In 2015, 508 cases of mental disorders were attended at in-patient with males presenting 166 cases with schizophrenia. Mental disorders at in-patient presented a high number of schizophrenic psychoses in 2015 with a total of 213, males presenting the highest number. The symptoms are losing interest in life, lack concerntration.unlikely to start conversation and feeling suspicious of everyone around.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 21
Table 4: Mental disorders at in-patient segregated by sex ,2015
Table 5: Oral health problems and dental carries at OPD
Diagnosis Description Sex
Grand Total Female Male
Affective Psychoses 68 153 221
Alcohol Dependency Syndrome 4 2 6
Alcoholic Psychoses 3 6 9
Drug Dependence 8 29 37
Drug psychoses 9 13 22
Schizophrenic Psychoses 47 166 213
Grand Total 139 369 508
2010 2011 2012 2013 2014 2015
Dental Caries
<5 years 2168 1510 1968 1765 2782 4853
>5 25755 33401 32276 36908 40013 32036
Oral Health Problems
<5 10332 9340 9917 8646 10016 8112
>5 22155 20401 20456 19255 22466 27806
Source: HMIS 2015
3.8. ORAL HEALTH
3.8.1. MORBIDITY DUE TO ORAL HEALTH
According to WHO oral health is a state of being free from chronic mouth and facial pain ,oral and throat cancer,oral sores, birth defects such as cleft of the lip and palate,periodontal(gum) disease,tooth decay, tooth loss and disorders that limit indivividual ability to chew,smile,bite,speak and the pyshological wellbeing. The major risks to Oral health are nutrition,diet, fluorides and tobacco. Oral health, including dental caries is part of NCDs program intervention area for Swaziland. The WHO Global Oral Health Programme focuses on school children and youth as the important target groups concerning oral health .The number of dental caries has decreased in adults in 2015 when compared to previous years,however they have increased in the under 5 population.
In terms of oral health, there was a decrease in cases reported for both under 5’s and over 5’s in 2015 . The table below shows 8112 under 5s cases reported to be oral health problems and above 5 presented with 27806 cases. In general, the number of under 5’s present more with oral health problems than with dental caries, whilst more over 5s present at health facilities for oral health problems.

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 22
Table 6: Eye and Ear related cases at OPD by sex, 2015
Condition < 5 years > 5 years
Total Female Male Female Male
Ear Problems 9762 9962 56156 34517 110397
Eye Diseases 5621 5566 22544 18514 52245
Grand Total 15383 15528 78700 53031 162642
EAR RELATED CASES BY AGE 2010-2015
Figure 22: Ear related cases at OPD by age, 2010-2015
11120 9632 9579 9916 109041972422878 22530 23764 22264 22351
90673
2010 2011 2012 2013 2014 2015
< 5 years > 5 years
Source: HMIS 2015
3.9. EYE AND EAR HEALTH
3.9.1 MORBIDITY DUE TO EYE AND EAR HEALTH
Eye and ear health are part of NCDs program, largely due to the diseases that can be traced back to environmental and biological risk factors. In Swaziland, the HMIS data shows that even though female cases were always more than male cases, the differences were consistently minor for both inpatient and outpatient as shown in Figure 25. The data by age group indicates that there is an increase in the number of cases seen for people over the age of 5 from 42 348 in 2014 to 162,642 cases in 2015. This increase amounts to over six thousand cases. The number of cases for those under 5 increased slightly from 11 802 to 12 856 in 2014.
3.9.2 MORBIDITY DUE TO EAR RELATED DISEASE TRENDS
The trend for ear related cases by sex shown in Figure 22 also indicates that the number of females presenting at OPD is stabilizing overtime, however the number of males seen at OPD is increasing slightly.
The data from HMIS shows that the number of ear related cases in OPD has remained stable in the 5 year period for both age-groups. There was a slight increase in the number of ear related cases seen at OPD under 5 age-group; from 2013 there were 9916 cases reported, in 2014 a total of 10 904 cases were reported. In 2015 the under 5 presented with a 19724 ear related cases and there was a increase from the previous years and the above 5 years had a total of 90673 ear related cases at OPD.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 23
EYE RELATED CASES ATTENDED IN THE OPD 2010-2015
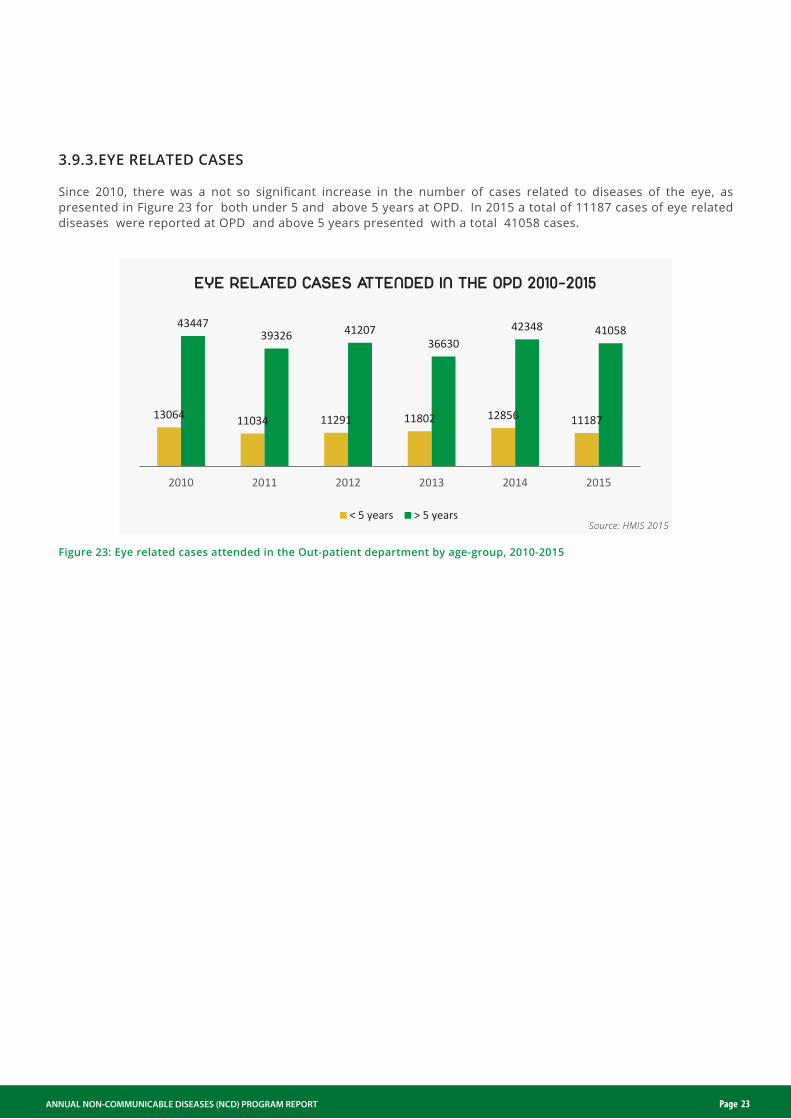
Figure 23: Eye related cases attended in the Out-patient department by age-group, 2010-2015
< 5 years > 5 years
13064 11034 11291 11802 12856 11187
4344739326 41207
3663042348 41058
2010 2011 2012 2013 2014 2015
Source: HMIS 2015
3.9.3.EYE RELATED CASES Since 2010, there was a not so significant increase in the number of cases related to diseases of the eye, as presented in Figure 23 for both under 5 and above 5 years at OPD. In 2015 a total of 11187 cases of eye related diseases were reported at OPD and above 5 years presented with a total 41058 cases.

CHAPTER 4:CHAPTER 3:PROGRAM ACHIEVEMENT
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 25
4.1 Policy
The national NCD program has developed the NCD policy and NCD Strategic plan, which are at the endorsement stage. The NCD Technical Working Group has been established. There is also a draft mental health policy and guidelines. Diabetes has the following documents developed; Constitution, Board charter, Finance policy, Human resource policy, Strategic Plan 2014-2019, Organizational profile and the Diabetes Charter. 4.2 Service delivery
• With the assistance of an occupational therapist for group counselling in substance abusers and drug adher-ence was established which is still in its infacy stage.
• The Psychiatric hospital has been able to integrate HIV services such as ART into Mental Health services, the country is now able to handle defaulters of both HIV and mentally challenged patients at the same time thus improving service delivery.
• Interaction of mental health service into general hospital and clinics as part of health package concept.
• Drugs for hypertension,diabetes mellitus, asthma, CVD; and epilepsy revised for easy access by the clinics at PHC; now available at CMS.
• Integration of T.B and HIV into NCD screening and service provision a step in progress.
• Child Obesity project intiated.
• Diabetes Swaziland has increased the number diabetes support groups from 13 support groups in 2010, (which were only limited to health facility settings) to 63 in 2014 which now includes faith based organiza-tions, Chiefdoms and workplace. There are 2 categories of Diabetes Educators comprising 50 out-of-school youth, 120 carers in all the four regions of Swaziland. The out-of- school youth were able to conduct health diabetes talks as outlined in the table below.
• In collaboration with Sports Council – established shukuma Swaziland in 2012 and was able to reach approximately 500 elderlies through sessions at Ludzeludze and Ngudzeni Tinkhundla in 2013 and 2014, respectively. Healthy Lifestyle – promoting eight principles drinking of water, enough resting time, physical activity, healthy foods and proper preparation of nutritious food. Discouraging use of tobacco and alcohol. Drugs for hypertension,diabetes mellitus, asthma, CVD; and epilepsy revised for easy access by the clinics at PHC; now available at CMS
• CANASWA, a fully registered non-Governmental Organization formed by Cancer Survivors and Caregivers aims to create awareness on cancer early dictation, mentoring, promoting positive living to people living with cancer, prevention. This organization conducted the following community activities: The public has been empowered with knowledge of early signs and symptoms of cancer through the activities conducted by CANASWA. In addition, these activities were achieved in collaboration with the NCD Stakeholders Alliance (i.e. Diabetes Swaziland, Epilepsy, COSAD, Vine Branch International). The progam established a population based cancer registry to look atall cancer data in the country.
4.3. Capacity Building
• In-service trainings and workshops were conducted to train nurses and all staff with current knowledge and skills thus increasing competence in the practice area. Capacity building on Cancer Cervix conducted.
• The Availability of a vehicle for community services for mental health outreach clinics has improved services of social health and welfare in re-integration of patients back to the community. Improved independent drug procurement system through medical stores though shortages and challenges are still there. The national hospital has an internal laboratory.
4.4. Data/Monitoring & Evaluation
• The NCD program with support from WHO undertook the second national survey called STEPS; Non-communicable diseases step wise approach for risk factors. The report was finalized and disseminated in 2015.
• HIMS for NCDs needs to be intergrated – work in progress.• The Swaziland Population Based Cancer Registry was established.• NCD STEPS SURVEY 11 report was finalised and to be disemminated in 2016
4.5. Constraints
• Non-availability of transport• No Office space• Lack of funding• Lack of human resource• Staff work on voluntary basis• Non-availability of comprehensive services from Government (e.g. laboratory, oncology units, medication)• Palliative care is not decentralized• LACK OF ANTI-EPILEPTIC DRUGS (AEDS)• Lack of Diagnosis equipment (MRI Scan and EEG) for epilepsy• Lack of Therapeutic Drug Monitor (TDM) for epilepsy
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 26

CHAPTER 4:CHAPTER 5:CONCLUSIONS AND RECOMMENDATIONS
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 28
5.1. CONCLUSIONS
The NCDs that contribute more to the death in these health facilities are CVD, Chronic obstructive pulmonary disease, cancer, and diabetes.This might suggest that more NCD patients seek health care when the condition is at an advanced stage and require admission as compared to preventative measures.
The trend analysis of NCDs indicates that hypertensive disease and cancer has been increasing over the last three years in terms number of deaths. Deaths due to diabetes is however on a decline.
NCDs in Swaziland disproportionality affect more females than males. In cardio-vascular disease affect more females (57%) than males (43%). Deaths due to cancer are more prominent among females than males, and the leading cause of death due to cancer is cervical cancer.
5.2. ACTION POINTS
Since most of NCDs are preventable and treatable if diagnosed early, MOH needs to increase efforts on health education around the causes and risk factors for NCDs to encourage health seeking behavior amongst the Swazi population. There is a need to focus on patient care for hypertensive disease and cancer since the number of deaths due to these conditions are increasing.
The Ministry of Health needs a strong interest to start a vigorous program which will encourage lifestyles that will help in preventing these illnesses through a multi-sectorial involvement which can be intergrated into the existing health system. The program needs to continue to improve in diabetes management due to the fact that the number of patients seen for diabetes mellitus is increasing; however the deaths are declining.
NCD present an increasing burden on the national health care system, both in terms of mortality and morbidity. The NCD diseases are preventable through management of the risk factors. It is critical the health care workers be further trained on how to integrate NCD in the routine patient care, and ensure that the data is captured accurately. The program also needs to further strengthen its governance by developing guidelines and Standard Operation Procedures (SOPs) and ensure a comprehensive representation of all NCD stakeholders.
There is an inconsistent reporting in the diseases related to mental health recorded in OPD and the mental hospi-tal. Although the mental hospital is a specialist center, there is a need to strengthen the international statistical classification of diseases coding of disease. Health care workers and the data collectors need to be trained on proper ICD coding to improve data.
• There is a great need to conduct a surveillance on cancer. We have no evidence based data• The Swazi population still lacks knowledge on cancer risks factors• They is a need to consistently educate communities on healthy lifestyle• Most people still have myths concerning cancer

ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 29
Annexures

DEFINITION OF TERMS
Chronic obstructive pulmonary disease (COPD) - is a lung disease characterized by chronic obstruction of lung airflow that interferes with normal breathing and is not fully reversible. The more familiar terms 'chronic bronchitis' and 'emphysema' are no longer used, but are now included within the COPD diagnosis. COPD is not simply a "smoker's cough" but an under-diagnosed, life-threatening lung disease.
Communicable disease- An illness due to a specific infectious agent or its toxic products that arises through transmission of that agent or its products from an infected person, animal or inanimate reservoir to a susceptible host; either directly or indirectly through an intermediate plant or animal host, vector or the inanimate environ-ment. (Synonym: infectious disease).
Diabetes mellitus- is a chronic disease caused by inherited and/or acquired deficiency in production of insulin by the pancreas, or by the ineffectiveness of the insulin produced. Such a deficiency results in increased concentra-tions of glucose in the blood, which in turn damage many of the body's systems, in particular the blood vessels and nerves.
Disability- is a term which covers impairment, activity limitation and participation restriction. It may be physical, cognitive like hearing loss, mental, sensory or a combination of these.
Endemic- the constant presence of a disease or infectious agent within a given geographic area; it may also refer to the usual prevalence of a given disease within such area.
In-patient- a patient who comes to a hospital or other health care facility for diagnosis or treatment that requires an overnight stay.
Risk factor- is any attribute, characteristic or exposure of an individual that increases the likelihood of develop-ing a disease or injury. Some examples of the more important risk factors are underweight, unsafe sex, high blood pressure, tobacco and alcohol consumption, and unsafe water, sanitation and hygiene.
Morbidity- refers to the disease state of an individual, or the incidence of illness in a population.
Mortality- refers to the state of being mortal, or the incidence of death (number of deaths) in a population.Non-communicable disease- non-communicable diseases (NCDs), also known as chronic diseases, are not passed from person to person. They are of long duration and generally slow progression. The 4 main types of non-communicable diseases are cardiovascular diseases (like heart attacks and stroke), cancers, chronic respiratory diseases (such as chronic obstructed pulmonary disease and asthma) and diabetes.
Out-patient- a patient who is not hospitalized overnight but who visits a hospital, clinic, or associated facility.
ANNUAL NON-COMMUNICABLE DISEASES (NCD) PROGRAM REPORT Page 30
