application for inclusion of - who...
TRANSCRIPT

Application for Inclusion of Miltefosine
On WHO Model List of Essential Medicines
Submitted by
Zentaris GmbH Weismüllerstr. 45
60314 Frankfurt/Main Germany
Contact: Dr. Mathias Pietras
Head of Marketing & Communication Zentaris GmbH
Weismüllerstr.45 60314 Frankfurt
Germany Phone: + 49 69 426023423
Fax: + 49 69 426023444 e-mail: [email protected]

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
1. Summary statement of proposal for inclusion, change or deletion Miltefosine is proposed to be included in WHO Model list of essential medicines as single agent for treatment of visceral and cutaneous Leishmaniasis in immunocompetent and immunosuppressed patients including pre-treated patients in section 6.5.2.
2. Name of focal point in WHO submitting the application Dr. Juntra Karbwang Clinical Coordinator Product Research & Development Special Programme for Research and Training in Tropical Diseases (TDR) World Health Organization 20, Avenue Appia 1211 Geneva 26 Switzerland
3. Name of the organisations consulted and/or supporting the application action medeor e.V St. Töniser Str. 21 47918 Tönisvorst Germany
4. International Nonproprietary Name (INN, generic name) of the medicine miltefosine
5. Whether listing is requested as an individual medicine or as an example of a therapeutic group
Listing is requested as individual medicine. Miltefosine is the only phospholipid so far that has been proven to be safe and effective in Leishmaniasis therapy. In addition it is the only compound in its class that can be given orally.
6. Information supporting the public health relevance of the submission Leishmaniasis is ranking third in the WHO neglected diseases list in terms of deaths per year. With annually 60.000 deaths only Malaria and tuberculosis have more victims1. It is estimated that 350 million people are at risk and currently 12 million people are infected. 1-1.5 million new cases are being reported annually. Most cases are found in India, Bangladesh, Brazil and Sudan. The DALY burden has been reported by WHO/TDR to be 860.000 for men and 1.200.000 for women2
The disease, which is transmitted by a species of sandfly (Phlebotomus sp. and Lutzomyia sp.), is found in 88 countries of the new and old world. There are two variations of the disease. The internal or visceral leishmaniasis is the most dangerous and causes death within 6-12 month if untreated. The other form, called cutaneous leishmaniasis, leads to lesions in the skin and if untreated to ulcers. In cases were no spontaneous healing occurs it leads to scars on body and face. The rate of patients with self healing varies between 10-50%, but it can not be predicted if an individual will achieve self-healing. If untreated the danger of secondary infections of ulcer and in the new world development of the mucocutaneous form destroying face and mucosal parts are possible complications.
15 October 2004 Page 2 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
The visceral form is found in the old (L.donovani, L.infantum) and new (L.chagasi) world. It is affecting the Indian subcontinent (India, Bangladesh and Nepal), parts of East Africa (Sudan and Ethiopia) and parts of South America (Brazil and Colombia). The number of new cases per year is 500.000 with a high rate of mortality. Every ten minutes a person is dying on visceral leishmaniasis! Since 1993 there has been recorded an increase in cases and endemic regions. Visceral leishmaniasis is associated with fever, weight loss, enlargement of spleen and liver. If it is left untreated it tends to be fatal. Because visceral leishmaniasis affects the poorest of the world, research and development of new drugs has been neglected. The current standard therapy, introduced 50 years ago, has to be given parenterally in hospitals and has a high toxicity. AIDS and other immunosuppressive conditions such as malnutrition increase the risk, and many of the countries where visceral Leishmaniasis is found they are also hot spots for AIDS and malnutrition. All public health organizations are looking for a new treatment that is effective, easily administered, and well tolerated. Availability of a new treatment option would also increase the chance to set up control programs and to eliminate this disease. The cutaneous form is widespread in both worlds. In the old world L.major and L.tropica are the main forms. L.major is found in rural areas whereas L.tropica is found in urban areas. The main countries are Afghanistan, Pakistan and the whole Middle East especially Iran, Iraq, Syria and Saudi-Arabia. Currently, there is a tendency to leave the patients untreated because scars and painful ulcers are considered as non-life threatening. But also the high risk of side effects from the current treatment may explain the wait-and-see-position. The easy application of a tolerable oral medication may change this attitude and will give the change to treat these people and prevent them from living a disfigured live. Also every untreated patient remains as a reservoir for the Leishmania. In the new world the situation is more dangerous. Patients suffering from cutaneous leishmaniasis may develop the mucocutaneous form which will lead to painful and disfiguring disruption of parts of the face. The disease is found all over Middle and South America with focal points in Venezuela, Peru, Bolivia and Guatemala. Governments are trying to set up programs but the application of parenteral drugs in this, often rural areas, is difficult. In addition, current treatment and the disease Leishmaniasis are building a vicious circle in respect of HIV. The current parenteral applications are causing a danger of infection with HIV because of the sanitary situation in the developing countries. On the other hand patient with HIV-infection are more easily affected with a Leishmania co-infection. Therefore, areas with high HIV rates and Leishmania see a rapidly increasing number of cases (e.g. Ethiopia).
15 October 2004 Page 3 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Fig. 1: Global distribution of leishmaniasis in countries most affected
Because of recent events there is also a re-emerge of the diseases. In countries like Iraq the visceral leishmaniasis was nearly eliminated before the UN sanction from 1990. Meanwhile thousands of cases are found. Also in Afghanistan a new outbreak of cutaneous leishmaniasis has been reported3 and most recently the WHO started a campaign for a control program4. The currently ongoing study in cooperation with HealthNet shows a high demand for a mild treatment. It has been shown that if an oral treatment is available the intramuscular application therapy is not accepted by the patienti. The current treatment options are limited. Since 50 years parenteral antimonials have been the standard therapy for Leishmania. These drugs are listed as essential drug. The side effects are very serious including vomiting, nausea, diarrhoea and anorexia. Creatine values have to be observed and ECG values have to be monitored during the whole course of treatment and a regular ECG monitoring is required.. The alternative and 2nd line treatment amphotericin B has its advantage in the absence of resistance but in addition to the high cost for hospitalisation there is a higher drug price. Side effects are similarly serious with additional drug-induced fevers and it is only approved for visceral leishmaniasis. The alternative to overcome side effects is the use of liposomal amphotericin B but the drug price alone (>1000 U$/per treatment course) will disclose the product from the market of developing countries. All treatments are parenteral. The risk of HIV co-infection caused by this route of application has not found a reflection in the treatment recommendation. A reduction of co-infection with current therapies will not be possible. Even if drug costs are low the cost for hospitalisation and laboratory requirement are high.
i Internal information: The comparission arm with antimony i.m had to be cancelled because of recruitung problems.
15 October 2004 Page 4 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
The treatment with antimonials is seeing a rapid decrease of efficacy. There is a growing number of resistant cases reported with up to 80% in the state of Bihar in India5. From Brazil the recent alarming news about low efficacy of Antimonial therapy has been reported.6 Leishmaniasis belongs to one of the most neglected disease. Research and medical breakthroughs are rare7. For more than 50 years no new drugs have been developed. Miltefosine does enable a safe and effective new treatment for Leishmaniasis. The oral application will prevent HIV-coinfection and does also facilitate its use in control programm in rual areas because no hositalisation is needed.
7. Treatment details The daily dosage of miltefosine capsules depends on body weight. Recommended dosage for visceral Leishmaniasis Children from 8 - 20 kg body: 2.5 mg/kg miltefosine. corresponding to 20 - 50 mg miltefosine. Children with a body weight between 20 and 25 kg: 50 mg miltefosine. Children with a body weight above 25 kg, adolescents and adults: 100 mg miltefosine. An increase of the daily dosage to 150 mg could be considered in patients with a bodyweight above 67 kg under monitoring of the tolerability. Recommended dosage for cutaneous Leishmaniasis Children from 8 - 20 kg: 2.5 mg/kg miltefosine. corresponding to 20 - 50 mg miltefosine. Children with a body weight between 20 and 25 kg: 50 mg miltefosine. Children with a body weight above 25 kg, adolescents and adults with a body weight up to 45 kg: 100 mg miltefosine. Adults with a body weight above 45 kg:150 mg miltefosine. Formulations and administration Miltefosine is available in two capsule sizes containing either 10 mg or 50 mg miltefosine. The capsules should be taken with meals. Dosages of 2 - 8 capsules per day should be divided into 2 - 3 individual doses to be taken either in the morning and in the evening or in the morning, at noon and in the evening. Duration The duration of treatment is 28 days. Immunocompromised patients may require prolonged treatment.
8. Summary of comparative effectiveness in a variety of clinical settings
8.1 Identification of clinical evidence The applicant performed 9 clinical trials, as shown in Tab. 1. All studies were conducted according to Good Clinical Practice (GCP) principles; sponsor’s study ID number is
15 October 2004 Page 5 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
indicated in brackets. VL studies (except 033 and 3089) were conducted in collaboration with WHO/TDR. All studies used appropriate criteria for evaluating the safety and efficacy of the product, e.g. recording of adverse events and repeated evaluations of laboratory and 6 month post treatment follow-up to verify definite cure, respectively. While dose finding studies had sequential or parallel dose groups without use of an active comparator drug, the phase III trial in adult VL patients was active controlled (amphotericin B, given by intravenous route), while the confirmatory study in CL patients was placebo-controlled. Tab 1: Studies of Miltefosine in patients with visceral leishmaniasis (VL) or cutaneous leishmaniasis (CL)
Study Principal Investigator(s) Group: Dosages / ranges tested No. of patients Studies in VL patients aged 12 years and older 00338
S Sundar 50 mg q2d x 14
up to 250 mg/day x 28
30
30899
S Sundar 100 mg/day x 28
up to 200 mg/day x 28
46
310910
TK Jha, S Sundar, CP Thakur (WHO)
50 mg/day x 42 up to 100 mg/day x7 + 150 mg/day x 21
120
312711
S Sundar 100 mg/day x 14
up to 100 mg/day x 28
54
315412
TK Jha, S Sundar, CP Thakur (WHO)
Miltefosine: 100 mg/day x28 (below 25 kg: 50 mg/day x28)
Amphotericin B: 1 mg/kg/day x30
400 (300 +100)
Studies in VL patients aged 11 years and younger 309113
S Sundar 1: 1.5 mg/kg/day x 28
2: 2.5 mg/kg/day x 28 39
3206 14
TK Jha, S Sundar, CP Thakur, S Bhattacharya (WHO)
2.5 mg/kg/day x 28 80
Studies in CL patients aged 12 years and older 309215
J Soto, Bolivia 50 mg/day x 20
up to 150 mg/ day x 28
64
309216
J Soto, Bolivia B Arana / M Gilardi, Guatemala
150 mg/day x 28 vs Placebo
133 (89 + 44)
In addition to data from clinical trials in VL and CL patients, data from a compassionate use program in 39 patients with leishmaniasis and HIV co-infection are available (Clin Infect Diseases; MS accepted for publication).
15 October 2004 Page 6 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
8.2 Summary of available data
8.2.1 Visceral Leishmaniasis Rapid improvement in clinical and laboratory parameters
In all studies of Miltefosine for visceral leishmaniasis, the anti-parasitological effect of the treatment was paralleled by a rapid resolution of all clinical signs and symptoms and abnormalities in laboratory parameters which are commonly associated with the disease. These beneficial changes specifically included the disappearance of fever, splenomegaly (spleen enlargement), and hepatomegaly (liver enlargement), as well as the recovery from anemia, leukocytopenia, and thrombocytopenia (reduced counts of red blood cells, white blood cells, and blood platelets, respectively). Eventually, the recovery from the infection and the improvement in the general health status was also documented by patients’ weight gain, starting during and continuing beyond the end of the treatment period.
For example, in the randomized controlled study # 315412, comparing oral use of Miltefosine with intravenously administered amphotericin B, miltefosine treated patients were free of fever within less than 1 week from start of treatment and remained so until the end of treatment, while in amphotericin B treated patients each drug application was associated a recurrent fever reaction. While the loss of fever and the body weight gain, as well as the disappearance of the sometimes massive enlargement in the size of spleen and liver are signs of improvement which the patient experiences immediately him-/herself, the improvements in the mentioned blood parameters are important for the reduction in the risk of bleeding or infection with other parasites or bacteria. Parasitological cure rates in different studies: Table 2 shows for the ITT populations of all studies the final cure rates irrespective of dosage used. Except for the dose-finding pilot study (0033), all subsequent studies resulted in high global rates of final cure rates, underlining the therapeutic potential of miltefosine in this indication. Tab 2: Cure rates of VL patients after treatment with Miltefosine, irrespective of administered dosage; ITT analyses
Final parasitological cure, ITT population missing/ not assessable no Yes All
Study N % n % n % N 0033 0 0 8 26.7 22 73.3 30 3089 1 2.2 0 0 44 97.8 45 3109 0 0 6 5.0 114 95.0 120 3127 0 0 2 3.7 52 96.3 54 3154 8 3.0 9 3.0 282 96.6 299 3091 1 2.6 4 10.3 34 87.2 39 3206
all patients treated with miltefosine, irrespective of daily dose, age, and treatment duration
2 2.5 3 3.7 75 93.4 80 all patients treated with miltefosine aged > 12 years *) 9 1.6 25 4.6 514 93.8 548 all patients treated with miltefosine (any age) 12 1.8 32 4.8 623 93.4 667 3154 patients allocated to treat-
ment with amphotericin B 3 3.0 0 0 96 97.0 99 all patients (any treatment) 15 2.0 32 4.2 719 93.9 766
*) i.e. excluding studies 3091 and 3206
15 October 2004 Page 7 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Cure rates by dosage: As the clinical studies included dose groups with higher and with lower dose intensities compared with the approved dosage scheme, Table 3 shows the cure rates according to the administered daily. Tab. 3: Cure rates of VL patients after treatment with Miltefosine, by administered daily dose; ITT analyses.
Final parasitological cure, ITT population *) missing/not assessable No Yes all
Dose group *) n % n % n % n ≤ 50 mg 1 0.9 12 11.2 94 87.9 107 100 mg 9 2.2 14 3.4 384 94.3 407 150 mg 0 0 2 3.8 51 96.2 53 200-250 mg 0 0 1 5.0 19 95.0 20 AMP 3 3.0 0 0 96 97.0 99 all *) 13 1.9 29 4.2 644 93.9 686
*) excluding data from study 3206 in which all patients received the same target dosage of 2.5 mg/kg/day and variability in dosage was caused by rounding to 10 mg increments .
It is evident that all dose groups with a daily dosage of 100 mg and higher showed final cure rates around 95%. The cure rate for the dose group ≤ 50 mg/day is lower as it includes data from pediatric patients of study 3091 as well as the patients treated at the first dose levels in the dose finding studies 0033 and 3109.
It should be noted that the dose group of 100 mg/day includes data from those patients of study 3127 who received the treatment for only 2 and 3 weeks. Failure to achieve cure was noticed for the short treatment duration. Cure rates by patients’ age
Tab 4. shows the cure rate of VL patients by age group. The lower global response rate in the group of patients aged 15 years and above results from the inclusion of early dose-finding studies. These studies with higher failure rates due to under-dosing, had a lower age limit of 14 years. Thus, the higher cure rate in the age group 12-14 years is due to the fact that this age group comprised patients from studies excluding sub-optimal dosage schemes. Cure rates in the patients aged 2-11 years draw upon data from both the dose-finding study (study 3091) and the confirmatory study in this age group (study 3206). Tab. 4: Cure rates of VL patients after treatment with Miltefosine, by patient age; ITT analyses.
Final parasitological cure, ITT populationmissing/ not assessable No yes all
Age [years] n % N % n % n 2-11 3 2.6 7 10.3 109 91.6 119 12-14 2 1.4 1 0.7 139 97.9 142 >= 15 10 2.0 24 4.8 471 93.3 505 All 15 2.0 32 4.2 719 93.9 766
15 October 2004 Page 8 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Cure rates in relation to pre-treatment
In patients of all ages, miltefosine was effective both in pre-treated and non-pretreated patients. All studies consistently showed for study treatment with miltefosine similar high global cure rates in pre-treated patients and in patients with newly diagnosed visceral leishmaniasis. Pre-treatment, in most cases with pentavalent antimonial drugs, apparently did not adversely affect the chance to respond to treatment with miltefosine. Response rates, both in pre-treated and in non-pre-treated patients did not show a remarkable differences between oral treatment using miltefosine and intravenous treatment using amphotericin B. Tab. 5: Cure rates of VL patients after treatment with Miltefosine, by patient age; ITT analyses.
Final parasitological cure, ITT population missing/ not assessable no yes all
Treatment / status of leishmaniasis n % n % n % n newly diagnosed 9 2.1 24 5.5 407 92.7 439 previously treated 3 1.3 8 3.5 218 95.6 228 All patients 12 1.8 32 4.8 623 93.4 667
8.2.2 Cutaneous Leishmaniasis (CL) The following table shows the dose ranging and confirmatory studies that evaluated the safety and efficacy of oral miltefosine in the treatment of South American cutaneous leishmaniasis (CL).
Study Principal Investigator(s) Group: Dosage ranges tested No. of patients 3092 J Soto, Bolivia 1: 50 mg qd x 20
2: 50 mg qd x 7; 100 mg qd x 13 3: 100 mg qd x 7; 150 mg qd x 13 4: 150 mg qd x 28
16 19 17 20
3168 J Soto, Bolivia B Arana / M Gilardi, Guatemala
1: 150 mg/day x 28 2: Placebo
89 44
Dose finding study study 3092, a rising dose, open-label phase I/II trial (study #3092) evaluated oral miltefosine versus Colombian cutaneous leishmaniasis. The study was conducted in 72 male Colombian soldiers, mean 67 kg and the cure rate in the per protocol evaluable patients was as follows.
PP population Group 1 Group 2 Group 3 Group 4Rate of definite cure 9/14
(64.3%) 12/18
(66.7%) 14/14
(100.0%) 16/18
(88.9%) 95% (90%) lower
confidence bound 39.0%
(43.7%) 44.6%
(48.8%) 80.7%
(84.8%) 69.0%
(73.1%)
15 October 2004 Page 9 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
There was a trend (p = 0.05) between cure rate and dosage group. In addition, there was a significant difference (p = 0.01, Fisher exact test) between the cure rate for the lower dosage groups (groups 1-plus-2 combined: 21 of 32 = 66%) and the cure rate for the groups who essentially received 150 mg/day (groups 3-plus-4 combined: 30 of 32 = 94%). Confirmatory study 3168 was performed as a doubleblind placebo-controlled study of miltefosine (2.5 mg/kg/day orally for 28 days) in Colombia and Guatemala in 133 patients. In Lv panamensis regions in Colombia, the per-protocol cure rates for miltefosine and placebo were 91% (40/44) and 38% (9/24). These values are similar to historic values for the standard of care, meglumine parenterally for 20 days, and for placebo. In combined Lv braziliensis and Lm mexicana regions of Guatemala, the per protocol cure rates were 53% (20/38) for miltefosine and 21% (4/19) for placebo. The miltefosine rate was lower than historic antimony cure rates of >90% in Guatemala for Lv brasiliensis but is similar to recently reported cure rate of this strain in Brazil6,17.
Colombian Site Miltefosine pts Placebo pts Number of patients 49 24 Number cured 40 9 Number failed 4 15 ITT cure rate 82% 38% PP cure rate 91% 38% Age (years) 24±10 25±13 Weight (kg) 60±13 57±14 No. Of lesions 1(1-8) 1(1-5) Ulcer size (mm2) 171(72-1775) 238(6-2110) Previous Rx failure (# [%]) 3[6%] 2[8%] Time since first diagnosis (days)
8(5-47) 8(3-39)
Guatemalan Site Miltefosine pts Placebo pts Number of patients 40 20 Number cured 20 4 Number failed 18 15 ITT cure rate 50% 20% PP cure rate 53% 21% Age (years) 26±10 28±12 Weight (kg) 59±8 60±8 No. Of lesions 1(1-10) 1(1-3) Ulcer size (mm2) 165(6-1650) 154(6-3300) Previous Rx failure (# [%]) 10[25%] 8[40%] Time since first diagnosis (days)
9(7-21) 9(7-21)
15 October 2004 Page 10 of 21
Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
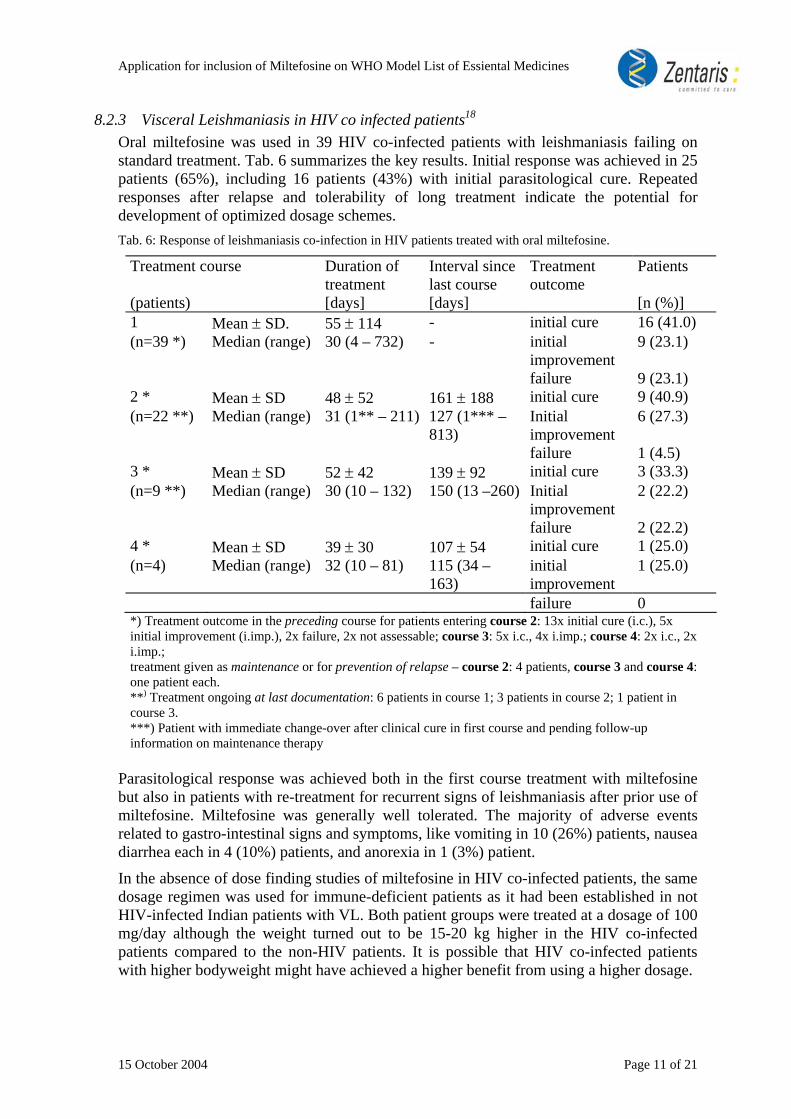
8.2.3 Visceral Leishmaniasis in HIV co infected patients18
Oral miltefosine was used in 39 HIV co-infected patients with leishmaniasis failing on standard treatment. Tab. 6 summarizes the key results. Initial response was achieved in 25 patients (65%), including 16 patients (43%) with initial parasitological cure. Repeated responses after relapse and tolerability of long treatment indicate the potential for development of optimized dosage schemes. Tab. 6: Response of leishmaniasis co-infection in HIV patients treated with oral miltefosine.
Treatment course Duration of treatment
Interval since last course
Treatment outcome
Patients
(patients) [days] [days] [n (%)] 1 Mean ± SD. 55 ± 114 - initial cure 16 (41.0) (n=39 *) Median (range) 30 (4 – 732) - initial
improvement 9 (23.1)
failure 9 (23.1) 2 * Mean ± SD 48 ± 52 161 ± 188 initial cure 9 (40.9) (n=22 **) Median (range) 31 (1** – 211) 127 (1*** –
813) Initial improvement
6 (27.3)
failure 1 (4.5) 3 * Mean ± SD 52 ± 42 139 ± 92 initial cure 3 (33.3) (n=9 **) Median (range) 30 (10 – 132) 150 (13 –260) Initial
improvement 2 (22.2)
failure 2 (22.2) 4 * Mean ± SD 39 ± 30 107 ± 54 initial cure 1 (25.0) (n=4) Median (range) 32 (10 – 81) 115 (34 –
163) initial improvement
1 (25.0)
failure 0 *) Treatment outcome in the preceding course for patients entering course 2: 13x initial cure (i.c.), 5x initial improvement (i.imp.), 2x failure, 2x not assessable; course 3: 5x i.c., 4x i.imp.; course 4: 2x i.c., 2x i.imp.; treatment given as maintenance or for prevention of relapse – course 2: 4 patients, course 3 and course 4: one patient each. **) Treatment ongoing at last documentation: 6 patients in course 1; 3 patients in course 2; 1 patient in course 3. ***) Patient with immediate change-over after clinical cure in first course and pending follow-up information on maintenance therapy
Parasitological response was achieved both in the first course treatment with miltefosine but also in patients with re-treatment for recurrent signs of leishmaniasis after prior use of miltefosine. Miltefosine was generally well tolerated. The majority of adverse events related to gastro-intestinal signs and symptoms, like vomiting in 10 (26%) patients, nausea diarrhea each in 4 (10%) patients, and anorexia in 1 (3%) patient.
In the absence of dose finding studies of miltefosine in HIV co-infected patients, the same dosage regimen was used for immune-deficient patients as it had been established in not HIV-infected Indian patients with VL. Both patient groups were treated at a dosage of 100 mg/day although the weight turned out to be 15-20 kg higher in the HIV co-infected patients compared to the non-HIV patients. It is possible that HIV co-infected patients with higher bodyweight might have achieved a higher benefit from using a higher dosage.
15 October 2004 Page 11 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
8.3 Summary of available estimates of comparative effectiveness Miltefosine has shown that it is an effective and safe drug for treatment in Leishmaniasis and an alternative to currently available standard treatment. The cure rate for visceral Leishmaniasis has been shown to be equal to the current second line treatment even in already pretreated and antimony resistant cases. It has also shown to have 2,2 fold higher cure rates than placebo for cutaneous leishmaniasis in South America. Finally, in HIV co-infected patients it has indicated to be an alternative to the current treatments. Side effects have been mild compared to the standards. In the currently ongoing studies performed by Zentari,s with a total of 2000 patients involved, no new safety issue has been detected.
9. Summary of comparative evidence on safety The most commonly reported adverse events related to the use of Miltefosine are transient gastrointestinal discomfort, vomiting, diarrhea, elevation of liver enzymes and serum creatinine. These effects are usually mild to moderate and transient or reversible at the end of treatment and therefore do not require discontinuation of treatment or dosage reduction. In clinical trials (Phase I-III) the following undesirable effects were observed in 564 VL patients treated at the recommended dosages: Organ systems Very common side
effects 10% of patients
Common side effects 1 – 10% of patients
Unommon side effects 0.1 – 1% of patients
Gastrointestinal disorders
Vomitting Diarrhea
Anorexia Nausea
Abdominal pain
Hepato biliary disorders
Increase in liver enzymes (SGOT, SGPT, AP)
Renal and urinary disorders
Increase of BUN, Creatinine
In addition one patient each was observed with Steven Johnson Syndrome. Estimate on patient exposure to date: About 2000 patients were included in Phase I – IV clinical studies with miltefosine. Miltefosine was recently launched in India, the only country were a Marketing Authorisation has been granted up to now. Zentaris estimates that up to date an additional number of 2000 patient have been treated; however, these do not provide information to the safety data base of miltefosine. Comparative safety evidence of safety in VL patients – based on amphotericin B controlled study 3154 This randomized controlled study compared oral miltefosine (100 mg/kg/day for 28 days) and intravenous amphotericin B (1 mg/kg every other day for 30 days) in a total of 398 patients with VL (randomization ratio: 3:1). Adverse events related to miltefosine primarily comprised gastrointestinal side effects, like nausea, vomiting and diarrhea, and increases in serum transaminases (mostly transient) and creatinine. In few patients only (1.3%) adverse drug reactions required premature discontinuation of treatment with miltefosine. In 92% of patients global rating for tolerability of miltefosine was very good or good, compared with 37% for amphotericin B, most prominent adverse reactions being
15 October 2004 Page 12 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
recurrent fever after each drug administration, nephrotoxicity, and gastrointestinal symptoms. Treatment emergent adverse events (TEAE) were reported in 106 patients (35.5%) after use of miltefosine and in 39 patients (39.4%) after use of AMP, respectively. The following table shows those TEAE that were reported more than once in either treatment group, those with number of observations classified likely related to treatment and all TEAE, irrespective of investigator’s classification.
Incidence of Most Frequent TEAE Treatment (patients) Miltefosine (N = 299) Amphotericin B (N = 99)
Causality Likely any Likely any WHO preferred term n % n % n % n %Anorexia 33 11.0 49 16.4 13 13.1 18 18.2 Fever * 0 0.0 28 9.4 0 0.0 11 11.1 Diarrhea * 1 0.3 8 2.7 0 0.0 2 2.0 Rash 1 0.3 2 0.7 0 0.0 0 0.0 Vomiting * 0 0.0 3 1.0 0 0.0 7 7.1 Thrombocytopenia 0 0.0 2 0.7 1 1.0 2 2.0 Headache 0 0.0 3 1.0 1 1.0 2 2.0
* These symptoms (and rigors) were recorded separately at each treatment day (see table below). The frequencies reported here do not reflect the true incidences
Specifically monitored reactions: The following table summarizes data on reactions that were recorded at each treatment day. Gastro-intestinal reactions were more important after miltefosine, rigors were characteristic for AMP.
Daily recording of treatment-associated side effects No. of days Miltefosine
(N=299) Amphotericin B
(N=99) Vomiting n % n % 1 or more 113 37.8 20 20.2 1-2 / 3-4 82 / 23 27.4 / 7.7 15 / 3 15.2 / 3.0 > 4 8 2.7 2 2.0
Diarrhea 1 or more 61 20.4 6 6.1 1-2 / 3-4 46 / 14 15.4 / 4.7 4 / 1 4.0 / 1.0 > 4 1 0.3 1 1.0
Rigors 1 or more 1 0.3 90 90.9 1-2 / 3-4 1 / - 0.3 / - 13 / 14 13.1 / 14.1
5-16 - - 63 63.6
Fever: Fever dropped rapidly in both treatment groups, however, in the AMP group the recovery from disease-related fever was superimposed by drug-induced fever following each application. Safety laboratory variables: Both treatments were associated with signs of reversible liver and renal toxicity. Increases in liver-specific enzymes increased more frequently during use of miltefosine than during AMP while an increase in substrates indicative of renal function impairment was 4-fold more frequent in patient treated with AMP than with miltefosine.
15 October 2004 Page 13 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Patients with increases of CTC grades compared to baseline (or re-increases after initial decrease for enzymes)
and resulting maximum CTC grades Parameter \ Group Miltefosine
(N=299) Amphotericin B
(N=99) SGOT 177
CTC 1 / 2 / 3: 91 / 70 / 16 46
CTC 1 / 2 / 3: 28 / 16 / 2 SGPT 155
CTC 1 / 2 / 3: 133 / 21 / 1 29
CTC 1 / 2 / 3: 26 / 2 / 1 AP 108
CTC 1 / 2 / 3: 88 / 19 / 1 29
CTC 1 / 2 / 3: 27 / 2 / - Creatinine 28
CTC 1 / 2 / 3: 20 / 6 / 2 42
CTC 1 / 2 / 3: 33 / 9 / - BUN 30
CTC 1 / 2 / 3: 20 / 6 / 4 43
CTC 1 / 2 / 3: 30 / 10 / 3
Serious adverse events were reported in 7 patients, 6 in miltefosine and 1 in AMP group. Of these, one case of a Stevens-Johnson syndrome (pat. no. 2/71; miltefosine) and one case of renal function impairment (pat no. 3/104; AMP) were assessed as adverse drug reactions. Premature discontinuations due to lack of tolerability: Overall, 4 and 2 patients did not complete their treatment of miltefosine and AMP because of intolerability. Miltefosine: arthritis and rash (pat 1/116), diarrhea (2/43), jaundice (2/69), and Stevens-Johnson syndrome (2/71); AMP: thrombocytopenia (2/21), and renal function impairment (3/104). Global assessment: In 92% of patients treated with miltefosine tolerability was globally assessed as very good or good, and in 5% as satisfactory. This compares favorably with amphotericin B with corresponding ratings in 37% and 59% of the patients, respectively. In only 2% of patients in both groups tolerability of treatment was classified as insufficient. Comparative safety evidence of safety in CL patients – based on placebo controlled study 3168 Miltefosine was generally well tolerated. One patient discontinued miltefosine treatment on day 27 due to motion sickness and headache. Daily monitoring of patients for vomiting and diarrhea revealed incidence rates for miltefosine of 31.5% and 5.6%, and for placebo 4.5% and 2.3%, respectively. For both types of reactions episodes were commonly mild and limited to 1 or 2 days. Treatment emergent adverse events (TEAE) were reported in 23/44 placebo patients (52.3%) and in 65/89 miltefosine (73.0%) patients. The table shows the incidences of TESS which were observed in more than one miltefosine patient; only nausea occurred with a considerably higher frequency after application of miltefosine than after application of placebo (p-value χ2- test 0.001).
15 October 2004 Page 14 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Placebo (N=44)
Miltefosine (N=89)
TEAE n % n % Nausea 4 9.1 32 36.0 motion sickness 10 22.7 26 29.2 Headache 9 20.5 24 27.0 abdominal pain 3 6.8 6 6.7 Diarrhea 2 4.5 5 5.6 Fever 2 4.5 5 5.6 Pharyngitis 1 2.3 4 4.5 Dizziness 0 0.0 4 4.5 Pruritus 0 0.0 4 4.5 Vomiting 0 0.0 4 4.5 Somnolence 0 0.0 3 3.4 Dyspepsia 1 2.3 2 2.2 Infection 0 0.0 2 2.2 Malaise 0 0.0 2 2.2 Pain 0 0.0 2 2.2
Laboratory investigations and other parameters showed for miltefosine the following mild changes, none of which resulted in dosing modifications or required other measures: Increase in serum creatinine, reaching CTC grade 1 in 31.5% (1 patient with CTC grade 1 at baseline and CTC grade 2 after use of antibiotic due to second infection). Increase in SGPT, reaching CTC grade 1 in 10.1% of patients (same rate for placebo). Decrease in mean body weight (-1%), compared with 1.5% increase for placebo Both ophthalmological examinations and spermiograms did not reveal adverse changes. Overall, tolerability of treatment was globally classified as follows.
Assessment Placebo (N=44)
Miltefosine (N=89)
Very good/good 36 (81.8%) 55 (61.8%) Satisfactory 4 ( 9.1%) 23 (25.8%) Insufficient 2 ( 4.5%) 6 ( 6.7%) Not assessable 2 ( 4.5%) 5 ( 5.6%)
10. Summary of available data on comparative cost and cost effectivness within the pharmacological class of therapeutic group
The treatment cost of Miltefosine will vary with dosage and treatment scheme as described in Section 7. It is estimated that the total treatment cost in developing countries will range between 80 and 300 Euro. Zentaris has agreed to supply miltefosine at a special low price for public use and control programmes, if patients are treated free of charge in developing countries (dual pricing). The higher total cost of 300 Euro will reflect the price for patients on the private market of developing countries whereas the lower total cost of 80 Euro will reflect the public use price in large control programmes. In the industrial countries the price will be adjusted to the price of current standard therapies.
15 October 2004 Page 15 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Treatment with miltefosine will decrease total therapy cost dramatically. The therapy can be compared with published total cost estimations for parenteral treatment of visceral leishmaniasis19. Zentaris market research shows the following situation after the introduction of miltefosine. Drug price per unit:
Exchange rate: 1U$=1€
drug Duration Dosage active ingridient unit unit price SSG 28 days 20mg per day
and kg body weight
100mg/ml Vial 30ml 4,52 €1
Amphotericin B 30 days 1mg per kg body weight every 2nd day
50 mg vial 5,30 €1
miltefosine 28 days 1.5 - 2.5 mg per day and kg body weight
50 mg 56 capsules 90 €3
Liposomal Amphotericin B
5 days 1 mg per day and kg body weight
50 mg vial 181,13 €2
1) International drug price indicator guide 2) Latest wholesaler/tender prices from India 3) 60kg adult. Price list of action medeor e.V. Drug price per treatment:
51€SSG
90 €Impavido®
Amphotericin B 95 €
Liposomal 1087 €Amphotericin
Drug price of miltefosine is equal to the current second line treatment. Cost per treatment: Current treatment costs are high due to high hospital and social economical cost. Patient treated with current parenteral drugs require hospitalisation and suffer from loss of earnings. Miltefosine overcomes this problem. Because of the mild side effects under treatment with miltefosine patient are able to work within a few days.
15 October 2004 Page 16 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
SSG Amphotericin B Impavido® Liposomal Amphotericin B
Drug cost 51 € 95 € 90 € 1087 € Loss of earnings 75 € 75 € 25 € 12,5 € Physician, hospitalisation and infusion/injection material
194 € 250 € 15 € 70 €
Total cost of treatment 320 € 420 € 130 € 1170 € Assumption: 60kg patient, loss of earnings 2,50 Euro per day, laboratory cost for all at the beginning and in addition weekly if parenteral 10 Euro each, Material: total 19 Euro for SAG, 5 Euro for each injection of Amphotericin B, cost of hospital 2 Euro and 2 Euro for food per day, For miltefosine only 10 day of inability of work is assumed Miltefosine reduces cost of treatment compared to the current first line therapy. The cost of treatment under miltefosine is only 40% of the current standard treatment.20.
11. Summary of regulatory status of the medicine Worldwide Marketing Authorisation Status – Impavido
Territory Approval date Trade Name
India 15.03.2002 1) Impavido® India Pending3) Impavido®
Germany Pending 1) Impavido® Pakistan Pending 2) Impavido®
Colombia Pending 2) Impavido® 1) visceral leishmaniasis 2) visceral leishmaniasis and cutaneous leishmaniasis 3) additional application for cutaneous leishmaniasis
12. Availability of pharmacopoieal standards A pharmacopoieal standard is not available for miltefosine. Miltefosine has just been registered as new drug. Therefore up to now it was not regarded as appropriate to request the entry of a drug substance specification into an official pharmacopoeia.
13. Proposed text for the WHO Model Formulary Description: Miltefosine has a marked direct antileishmanial activity in vitro and in animal models. The mode of action of miltefosine in leishmaniasis is unknown. Among others, miltefosine can inhibit metabolism of phospholipids How supplied: Capsules, 10 and 50 mg miltefosine. Use: Treatment of visceral and cutaneous Leishmaniasis. Up to now only limited experience is available from therapeutic use in immunocompromised patients. Therefore miltefosine should be used in these patients only after failure of standard therapy.
15 October 2004 Page 17 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Contraindications: Hypersensitivity to the active substance or any of the excipients. Pre-existing severe damage of liver or kidney function. Pregnancy. Warnings: Pregnancy There are no adequate data from the use of miltefosine in pregnant women. Studies in animals have shown reproductive toxicity. Miltefosine is contraindicated in pregnancy. Women of childbearing potential have to use effective contraception during and up to 3 months after treatment. Lactation It is not known whether miltefosine is excreted in the milk. Miltefosine should not be used by breast feeding women. Precautions: Male patients Toxicological studies have shown an impairment of reproductive function in male rats. Data on reproductive performance of 267 male patients who were treated with miltefosine in clinical studies did not indicate an effect on fertility. Patients with impaired renal function Treatment with miltefosine may lead to an increase in creatinine levels. The kidney function should be monitored in patients requiring concomitant use of miltefosine and other drugs with nephrotoxic potential. Drug interactions In vitro investigations have shown that interactions are unlikely with medications that are metabolised by cytochrome P450 or glucuronised or conjugated otherwise. However, the possibility of interactions with commonly used medicinal products cannot entirely be excluded. Dosage and Administration Miltefosine capsules are for oral use. The daily dosage of miltefosine capsules depends on body weight. Visceral Leishmaniasis Children from 8 - 20 kg body: 2.5 mg/kg miltefosine. corresponding to 20 - 50 mg miltefosine. Children with a body weight between 20 and 25 kg: 50 mg miltefosine.
15 October 2004 Page 18 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Children with a body weight above 25 kg, adolescents and adults:100 mg miltefosine. An increase of the daily dosage to 150 mg could be considered in patients with a bodyweight above 67 kg under monitoring of the tolerability. Cutaneous Leishmaniasis Children from 8 - 20 kg: 2.5 mg/kg miltefosine. corresponding to 20 - 50 mg miltefosine. Children with a body weight between 20 and 25 kg: 50 mg miltefosine. Children with a body weight above 25 kg, adolescents and adults with a body weight up to 45 kg: 100 mg miltefosine. Adults with a body weight above 45 kg:150 mg miltefosine. The duration of treatment is 28 days. Immunocompromised patients may require prolonged treatment. Overdose A specific antidote against miltefosine is not known. Gastrointestinal symptoms (nausea, vomiting, loss of appetite) are to be expected in case of acute overdose. Adverse effects on liver, kidney, and retinal function cannot be excluded in case of substantial overdose. Adverse effects The most commonly reported adverse drug reactions are transient gastrointestinal discomfort, vomiting, diarrhea, elevation of liver enzymes and serum creatinine.These effects are usually mild to moderate and transient or reversible at the end of treatment and therefore do not require discontinuation of treatment or dosage reduction. In clinical trials the following undesirable effects were observed in 564 patients treated at the recommended dosages: Organ systems Very common side
effects 10% of patients
Common side effects 1 - 10% of patients
Unommon side effects 0.1 - 1% of patients
Gastrointestinal disorders
Vomiting Diarrhea
Anorexia Nausea
Abdominal pain
Hepato biliary disorders
Increase in liver enzymes (SGOT, SGPT, AP)
Renal and urinary disorders
Increase of BUN, Creatinine
In addition one patient was observed with Steven Johnson Syndrome.
15 October 2004 Page 19 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Patient advice: The capsules should be taken with meals. Dosages of 2 - 8 capsules per day should be divided into 2 - 3 individual doses to be taken either in the morning and in the evening or in the morning, at noon and in the evening.
1. References
1 World Health report 2004 2 TDR strategic direction: Leishmaniasis Februar 2002
3 Leishmaniasis in Afghanistan, CSR Report 2002 4 WHO action in Afghniastan aims to control debilitating leishmaniasis
Press release 10.August 2004 5 Sundar S.
Drug resistance in Indian visceral leishmaniasis Tropical Medicine and international Health 6(11) 2001 849-54
6 Sierra Romeo, G.A., Farias Guerra, M.V., Paes Gomes M., Oliveira MacedoV. Comparison of cutaneous leishmaniasis due to Leishmania (Viannia) braziliensis and L. (v.) guyanensis in Brazil: Therapeutic response to meglumine antimoniate Am. J. Trop. Med. Hyg. 65(5) 2001 456-65
7 Morel C.M. Neglected diseases: under-funded research and inadequate health interventions EMBO report 2003 4 37-38
8 Sundar S, Rosenkaimer F, Makharia MK, Goyal AK, Mandal AK, Voss A, Hilgard P, Murray HW. Trial of oral miltefosine for visceral leishmaniasis. [Study # 033] Lancet. 1998 Dec 5;352(9143):1821-3.
9 Sundar S, Gupta LB, Makharia MK, Singh MK, Voss A, Rosenkaimer F, Engel J, Murray HW. Oral treatment of visceral leishmaniasis with miltefosine. [Study # 3089] Ann Trop Med Parasitol. 1999 Sep;93(6):589-97.
10 Jha TK, Sundar S, Thakur CP, Bachmann P, Karbwang J, Fischer C, Voss A, Berman J. Miltefosine, an oral agent, for the treatment of Indian visceral leishmaniasis. [Study # 3109] N Engl J Med. 1999 Dec 9;341(24):1795-800.
11 Sundar S, Makharia A, More DK, Agrawal G, Voss A, Fischer C, Bachmann P, Murray HW. Short-course of oral miltefosine for treatment of visceral leishmaniasis. [Study # 3127] Clin Infect Dis. 2000 Oct;31(4):1110-3.
12 Sundar S, Jha TK, Sindermann H, Junge K, Bachmann P, Berman J. Oral miltefosine treatment in children with mild to moderate Indian visceral leishmaniasis. [Study # 3091] Pediatr Infect Dis J. 2003 May;22(5):434-8.
13 Sundar S, Jha TK, Thakur CP, Engel J, Sindermann H, Fischer C, Junge K, Bryceson A, Berman J. Oral miltefosine for Indian visceral leishmaniasis. [Study # 3154] N Engl J Med. 2002 Nov 28;347(22):1739-46.
14 Bhattacharya SK, Jha TK, Sundar S, Thakur CP, Engel J, Sindermann H, Junge K, Karbwang J, Bryceson AD, Berman JD.
15 October 2004 Page 20 of 21

Application for inclusion of Miltefosine on WHO Model List of Essiental Medicines
Efficacy and tolerability of miltefosine for childhood visceral leishmaniasis in India. [Study # 3206] Clin Infect Dis. 2004 Jan 15;38(2):217-21. Epub 2003 Dec 18.
15 Soto J, Toledo J, Gutierrez P, Nicholls RS, Padilla J, Engel J, Fischer C, Voss A, Berman J. Treatment of American cutaneous leishmaniasis with miltefosine, an oral agent. [Study # 3092] Clin Infect Dis. 2001 Oct 1;33(7):E57-61. Epub 2001 Sep 05.
16 Soto J, Arana BA, Toledo J, Rizzo N, Vega JC, Diaz A, Luz M, Gutierrez P, Arboleda M, Berman JD, Junge K, Engel J, Sindermann H. Miltefosine for new world cutaneous leishmaniasis. [Study # 3168] Clin Infect Dis. 2004 May 1;38(9):1266-72. Epub 2004 Apr 09.
17 Arana B.A., Berman J.D., Navin T.R., Arana F.E., Chajón J.F. Placebo-controlled clinical trial of sodium stibogluconate (Pentostam) versus Ketoconazole for treating cutaneous leishmaniasis in Guatemala Journal of Infectious Diseases 165 1992 528-534
18 Sindermann H, Engel KR, Fischer C, Bommer W. Oral miltefosine for leishmaniasis in immuno-compromised patients: compassionate use in 39 patients with HIV co-infection. Clin Infect Dis. 2004, accepted for publication
19 Murray H.W. Treatment of Visceral Leishmaniasis (Kala-Azar): A Decade of Progress and Future Approches Int.J.Infect.Dis. 4(3) 2000 158-77
20 Murray H.W. Progress in treatment of a neglected infectious disease: visceral leishmaniasis Expers. Anti-infect. Ther. 2(2) 2004 279-92
15 October 2004 Page 21 of 21