approach to acid-base problems in the critically iii and injured
TRANSCRIPT

cOLLECTIVE REVIEW f
Approach to Acid-Base Problems in the Critically III and Injured
Robert F. Wilson, MD William J. Sibbald, MD
Detroit, Michigan
The use o f the H e n d e r s o n - H a s s e l b a l c h e q u a t i o n and the re la t ionsh ips between b i c a r b o n a t e levels and the pCO2 or c a r b o n i c ac id concentra- ttion in e v a l u a t i n g ac id-base abnormal i t i e s are expla ined . The et io logy, pathophysiology, d iagnos i s and t rea tment of resp ira tory a lka los i s and acidosis and m e t a b o l i c a lka los i s and ac idos i s are d i scussed . The results of laboratory tests shou ld be e x a m i n e d in re la t ion to the pat ient 's condi- tion and c o n s i s t e n c y wi th o ther l abora tory tests. Therapy is d irected at correcting t h e u n d e r l y i n g p r o b l e m s and, secondar i ly , at correc t ing the numbers. Pat i ent s r e s p o n d primari ly to rate o f c h a n g e and n o t abso lute Inumbers. Therefore , p r o b l e m s shou ld be correc ted at a p p r o x i m a t e l y Ithe rate they deve lop . T r e a t m e n t shou ld be gu ided by c o n t i n u e d pat ient observation a n d serial l a b o r a t o r y studies.
~Vilson RF, Sibbald WJ: Approach to acid-base problems in the critically ill and injured. JACEP 5:515-522, July 1976. acid base balance; abnormali- ties; alkalosis, metaboJic . . . respiratory; acidosis, metabol ic . . . respira- tory; Henderson-Hasselbalch equation.
INTRODUCTION Origin of Terms
The word ~acid" is derived from the Lat in acidus mean ing sour tast- ing, and refers to the sour taste of tacid substances such as v inegar . i , 2 Although '~base" was defined in 1774 ~Y Rouelle 3 as a substance tha t re- acts with, or neutral izes, an acid to 'I0rm a salt , i t was not u n t i l 1923 that the first clear definit ion of acids
~rora the Department of Surgery, Wayne
I rate University School of Medicine and he Shock Unit, Detroit General Hospital.
~UPported by the Detroit General Hospi- tal Research Corporation and Michigan ~Ssociation for Regional Medical Pro- ~ra~s. Grant #75-6-25.
I ddress for reprints: Robert F. Wilson, l), Professor of Surgery, Department of rgery, Wayne State University School Medicine, 540 E. Canfield, Detroit,
ichigan 48201.
and bases was supplied by Bronsted. 4 He defined an acid as any substance tha t could accept a hydrogen ion. Be- cause a hydrogen ion is a hydrogen atom without its electron, it can be considered a proton and thus, an acid can also be def ined as a ~'proton- donor" a nd a base as ~pro ton- acceptor."
pH
The c o n c e n t r a t i o n of h y d r o g e n ions, even in an acid solution, is ex- t remely small. In a so-called '~neu- tral" solution, there are as many hy- drogen (H +) ions as hydroxyl ( O H - ) ions. It is inconvenien t to use frac- t ion or logari thmic terms to describe the acidic s t r e n g t h of a so lu t ion . Hasse lba l ch 3 he lped by u s i n g the te rm ~'pH" to refer to the negat ive logari thm of a hydrogen ion concen- tration. A solution with a pH of 1,
therefore, has a hydrogen ion concen- t ra t ion of 1 x 10 -1 and is extremely acid, while a solution with a pH of 14 has hydrogen ion concentrat ion of 1 x 10 -14 and is extremely alkal ine.
Nanomoles of Hydrogen Ions
Some authorsS, s have referred to the hydrogen ion concentrat ion in a s o l u t i o n in t e r m s of n a n o m o l e s , which is 1 x 10 -s moles. A solution with a pH of 7.40 has 40 nanomoles of hydrogen ions per l i ter of solution. As the solut ion becomes more acid, the number of nanomoles of hydro- gen ions rises. For example, at a pH of 7.30, there are about 50 nanomoles of hydrogen ions present; at a pH of 7.50, t h e r e are a p p r o x i m a t e l y 30 nanomoles of hydrogen ions present. The rela t ionship between nanomoles and pH is shown in Table 1.1
A rough es t imate of the number of nanomoles present in a solution can be obtained by us ing the following formula, developed by Kassirer and Bleich. 7
H + (nanograms) = 24 x pCO2 (mm Hg)
HCO3 (mEq/liter)
Thus, if the carbon dioxide par t ia l pressure (pCO2) is 40 mm Hg and the bicarbonate ion (HCO3) is 24 mEq/ liter, there will be 40 nanograms of hyd rogen ions p re sen f a t a pH of 7.40.
Buffers
The pH of blood can be altered by a variety of metabolic and respiratory
J•PJuly 1976 Volume 5 Number 7 Page 515

Table 1 RELATIONSHIP OF
NANOMOLES OF HYDROGEN ION AND pH
(H +) pH (n moles/L)
7.00 100
7.10 79
7.20 63
7.30 50
7.40 40 7.50 32
7.60 25
7.70 20
fac tors . These wou ld cause wide swings in acid-base balance if it were not for the presence of a group of substances , re fer red to as buffers, capab le of n e u t r a l i z i n g , at l eas t partially, acids and bases. The acid buffering capacity of a solution is de- termined by the number of hydrogen ions the so lu t ion can t ake up for each uni t change in pH.
The average adult male has a total "bu f f e r base , " ie, t o t a l b u f f e r i n g capaci ty , of about 1000 mEq. The chief buffers in blood are the red cell hemoglobin and the bicarbonate and protein in the plasma. Most buffering against carbon dioxide is provided by hemoglobin while the bicarbonate/ carbonic acid system is pr imari ly re- sponsible for buffering blood and in- tersti t ial fluid. Inside tissue cells, the mos t i m p o r t a n t buffers are phos- phate and protein.
Most of the body's buffer systems act pr imari ly to neutralize acid. As a consequence, an acid load is generally handled better than a base or bicar- bonate excess.
Carbon Dioxide (Volatile Acid) Production and Transport
About 12,000 to 15,000 m E q of carbon dioxide (CO2), or volatile acid, are produced daily as a result of the cellular metabolism of carbohydrate and fat and excreted by the lungs.
The bicarbonate and carbonic acid (I-I2CO3) in the blood, which are the main determinants of pH in the ex- t r a c e l l u l a r f lu id (ECF), are con- s tant ly equil ibrat ing with CO2. CO2 is t ransported from peripheral tissue
cells to the lungs in t h r ee ways : (1) in red cells; (2) combined with amino groups on p l a sma proteins , and (3) in solution, as CCh, H2COs and b i c a r b o n a t e in p l a sma . Most t ranspor t is provided in the plasma, as bicarbonate, and in the red cells, as CO2 combined with the hemoglo- bin. The c o m b i n a t i o n of CO2 and amino groups on proteins produces v a r y i n g q u a n t i t i e s of c a r b a m i n o compounds, of which the concentra- tion may vary between 0.5 and 2.5 mEq/liter. CO~, present as I-hCOs in the plasma, averages about 1.2 mEq/ liter.
Renal Excretion of Acid
N o r m a l l y , the k i d n e y exc re tes about 70 mEq of acid daily. In acido- tic pa t ien ts this may be increased fourfold . Of th i s , a p p r o x i m a t e l y l m E q consists of non-volatile acids - - such as phosphoric acid (I-I3PO4), uric acid, and sulfuric acid (H2SO4) - - which are by-products of protein and phospholipid metabolism. Because these acids cannot be excreted by the lungs, they mus t be excreted by the kidneys.
Renal tubular excretion of acid is accomplished by three mechanisms: (1) direct secret ion of hydrogen - - accounting for only about 0.1 mEq of acid daily; (2) excretion with urine buffers, including sodium phosphate (Na2HPO4) - - accounting for about 20 mEq of ac id per day, and (3) exc re t ion wi th a m m o n i a , pro- duced in the distal tubular cells from g l u t a m i n e and o t h e r p r ecu r so r s , which accounts for about 50 mEq of hydrogen ions per day. Bicarbonate is absorbed in the proximal tubule and H+ is secreted into the tubular lumen in exchange for sodium(Na+). In the distal tubule, I-I~CO~ is dis- sociated into H ÷ (excreted in elec- t roequivalent exchange for Na ÷ and potassium [K-] ) and HCO~, which moves out of the other side of the cell into the blood stream.
Henderson-Hasselbalch Equation
pH = pK' + log base acid
To p r o p e r l y e v a l u a t e ac id-base changes, it is essential to unders tand the Henderson-Hasselbalch equation. This equa t ion re la tes the pH (the negative logar i thm of the hydrogen ion concent ra t ion) to the pK' (the
negative log of the dissociation % stant) and the log of the ratio of t~ f concentrat ion of a base to its relat~ acid. AS ment ioned previously, t~ I most impor tant buffer for ECF is ~ b i ca rbona t e / ca rbon i c acid syste~ The average concentration of bical. bonate is 24 mEq/liter, and the avel, age concentrat ion of carbonic acid i 1.2 mEq/liter. Therefore, the ratio QI bicarbonate to carbonic acid is nor, mal ly 20 to 1. The log of 20 is 1.3 a~t adding this 1.3 to 6.1 (the pK' or~0 i of the dissociation constant for cej bonic acid), results in the normal p~ of 7.4. It is in the maintenance ofths bicarbonate to carbonic acid ratio of to 1 tha t a t t empts to correct acid: base abnormalit ies are grounded.
DEFINITIONS
CO2 Content
The CO2 content is the total of all carbon dioxide present in the blood, a b o u t 24 to 31 mEq / l i t e r . In the plasma, this includes carbonic acid, b i ca rbona t e , and c a r b a m i n o co~ I pounds. I
The amount of carbonic acid pres. ent can be est imated by multiplyin t the pCO2 by 0.03, and averages 1.1 mEq/liter. The bicarbonate concenJ trat ion averages about 24 mEq/lite~ and the c o n c e n t r a t i o n of the car t bamino compounds averages 0.5~ 1.5 mEq/liter. Thus, under ordina~ hi circumstances, the plasma bicarb0n t ate concent ra t ion is approximatell i 1.0 to 2.0 mEq/li ter less than the C(~ content.
Buffer Base and Base Deficit
In p a t i e n t s who h a v e either~ metabolic acidosis combined with 1 respiratory alkalosis or a metab01i t alkalosis combined wi th a respire I tory acidosis, it may be difficult to de*~
/
t e r m i n e if the a l t e r a t i o n in th~ bicarbonate concentrat ion is due an abnormal i ty in cell metabolism 0] renal function or is a compensat0rll change.
Singer and Hast ings in 19488 de' ve loped t he concep t of the whole blood "buffer base" as the sum of the buffer anions. Under most circur~' stances, this averages 45 to 55 ml~ liter. If the buffer base is increased, the pat ient is said to have "base e~" cess," wh ich is a ssoc ia ted with a metabolic alkalosis. In contrast, if the buffer base is decreased, as 0c'
Page 516 Volume 5 Number 7 July 1976 ~
c~rs in me tabo l i c acidosis , the pa- tient is said to h a v e a "base deficit."
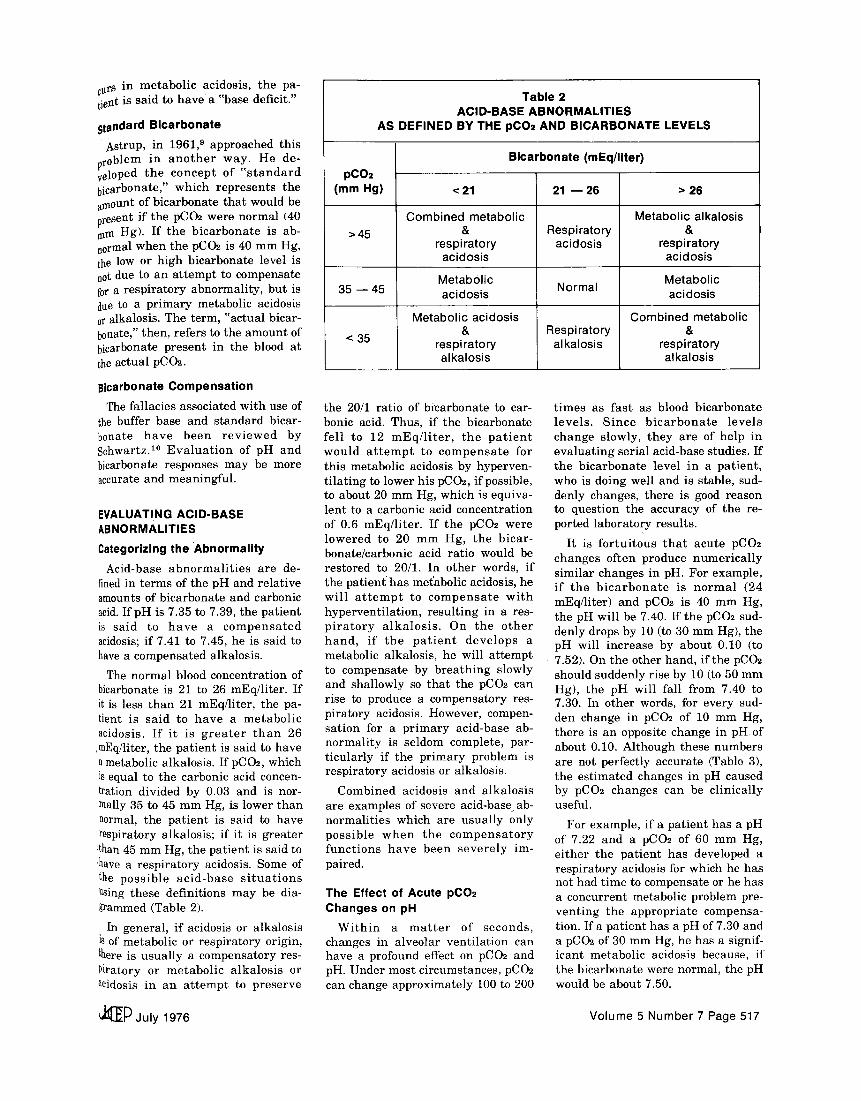
standard Bicarbonate
A s t r u p , in 1961, 9 approached th is problem in a n o t h e r way . He de- veloped t h e c o n c e p t of " s t a n d a r d bicarbonate," which r ep re sen t s the amount of b icarbona te t ha t would be present if the pC(h were normal (40 am Hg). If t h e b i c a r b o n a t e is ab- normal when the pC(h is 40 m m Hg, the low or h igh b icarbonate level is not due to an a t t e m p t to compensate for a r e sp i r a to ry abnormal i ty , bu t is due to a p r i m a r y metabol ic acidosis or alkalosis. The term, "ac tua l bicar- bonate," then, refers to the amoun t of bicarbonate p resen t in the blood at the ac tual pC(h .
Bicarbonate Compensation
The fa l lacies associa ted wi th use of the buffer base and s t anda rd bicar- bonate h a v e b e e n r e v i e w e d by Schwartz. 1° E v a l u a t i o n of pH and bicarbonate responses may be more accurate and meaningful .
EVALUATING ACID-BASE ABNORMALITIES
Categorizing the Abnormality
Acid-base a b n o r m a l i t i e s a re de- fined in t e rms of the pH and re la t ive amounts of b icarbonate and carbonic acid. I f p H is 7.35 to 7.39, the pa t i en t is s a id to h a v e a c o m p e n s a t e d acidosis; if 7.41 to 7.45, he is said to have a compensa ted alkalosis .
The no rma l blood concentra t ion of bicarbonate is 21 to 26 mEq/l i ter . If it is less t han 21 mEq/ l i ter , the pa- tient is s a id to h a v e a m e t a b o l i c acidosis. I f i t is g r e a t e r t h a n 26 ,mEq/liter, the pa t i en t is said to have a metabolic a lkalosis . If pC(h , which is equal to the carbonic acid concen- tration d iv ided by 0.03 and is nor- raally 35 to 45 m m Hg, is lower t h a n normal, the pa t i en t is said to have respiratory alkalosis ; if i t is g rea te r :than 45 mm Hg, the pa t i en t is said to have a r e sp i r a to ry acidosis. Some of the p o s s i b l e a c i d - b a s e s i t u a t i o n s Using these def ini t ions may be dia- grammed (Table 2).
In genera l , i f acidosis or a lka los is is of metabol ic or r e sp i r a to ry origin, there is u sua l ly a compensa tory res- Piratory or m e t a b o l i c a l k a l o s i s or acidosis in an a t t e m p t to p re se rve
Table 2 ACID-BASE ABNORMALIT IES
AS DEFINED BY THE pCO2 AND BICARBONATE LEVELS
Bicarbonate (mEq/liter) pCO2
(mm Hg) < 21 21 - - 26 > 26
Combined metabolic Metabolic alkalosis > 45 & Respiratory &
respiratory acidosis respiratory acidosis acidosis
Metabolic Metabolic 35 - - 45 acidosis Normal acidosis
Metabolic acidosis Combined metabolic & Respiratory &
< 35 respiratory alkalosis respiratory alkalosis alkalosis
the 20/1 ra t io of b icarbonate to car- bonic acid. Thus, if the b icarbonate fe l l to 12 m E q / l i t e r , t h e p a t i e n t w o u l d a t t e m p t to c o m p e n s a t e for th is metabol ic acidosis by hyperven- t i l a t ing to lower his pCO2, if possible, to about 20 m m Hg, which is equiva- len t to a carbonic acid concentra t ion of 0.6 mEq/ l i t e r . I f t he pCO2 were l o w e r e d to 20 m m Hg, t he b i ca r - bonate /carbonic acid ra t io would be res tored to 20/1. In o ther words, i f the pat ient ' has metabol ic acidosis, he w i l l a t t e m p t to c o m p e n s a t e w i t h hyperven t i l a t ion , r e su l t i ng in a res- p i r a t o r y a l k a l o s i s . On t h e o t h e r h a n d , i f t h e p a t i e n t d e v e l o p s a metabolic a lkalosis , he will a t t e mp t to compensa te by b r e a t h i n g s lowly and shal lowly so tha t the pC(h can rise to produce a compensa tory res- p i ra tory acidosis. However, compen- sa t ion for a p r i m a r y ac id -base ab- n o r m a l i t y is se ldom complete, par- t i cu la r ly i f the p r i m a r y problem is r e sp i ra to ry acidosis or alkalosis .
Combined acidosis and a l k a l o s i s a re examples of severe acid-base r ab- no rma l i t i e s which are u sua l ly only p o s s i b l e w h e n t h e c o m p e n s a t o r y f u n c t i o n s h a v e been s e v e r e l y im- paired.
The Effect of Acute pC02 Changes on pH
W i t h i n a m a t t e r of s econds , changes in a lveolar ven t i l a t ion can have a profound effect on pC(h and pH. Under most c i rcumstances , pC(h can change approx ima te ly 100 to 200
t imes as f a s t as blood b i ca rbona te l e ve l s . S i n c e b i c a r b o n a t e l e v e l s change s lowly, t hey a r e of he lp in e va lua t i ng ser ia l acid-base studies. I f the b i ca rbona t e level in a pa t i en t , who is doing well and is s table, sud- denly changes, there is good reason to ques t ion the accuracy of the re- ported l abora to ry resul ts .
I t is f o r t u i t o u s t h a t acu te pCO2 changes of ten produce n u m e r i c a l l y s imi la r changes in pH. For example , i f t h e b i c a r b o n a t e is n o r m a l (24 mEq/l i ter) and pC(h is 40 m m Hg, the pH wil l be 7.40. If the pC(h sud- denly drops by 10 (to 30 mm Hg), the pH wil l inc rease by about 0.10 (to 7.52). On the other hand, if the pC(h should suddenly r ise by 10 (to 50 m m Hg), the pH wil l fal l from 7.40 to 7.30. In o ther words, for every sud- den change in pC(h of 10 m m Hg, there is an opposite change in p H of about 0.10. Al though these numbers are not perfect ly accura te (Table 3), the e s t ima ted changes in pH caused by pC(h changes can be c l in i ca l ly useful.
For example , i f a pa t i en t has a pH of 7.22 and a pCO2 of 60 m m Hg, e i the r the p a t i e n t has developed a r e sp i r a to ry acidosis for which he has not had t ime to compensate or he has a concurrent metabol ic problem pre- ve n t i ng the a p p r o p r i a t e compensa- tion. If a pa t i en t has a pH of 7.30 and a pC(h of 30 mm Hg, he has a signif- icant metabol ic acidosis because, if the b icarbonate were normal , the pH would be about 7.50.
J : • P July 1976 Volume 5 Number 7 Page 517

Table 3 ACUTE pH CHANGES
OCCURRING WITH SUDDEN CHANGES IN THE ARTERIAL pCO2
HCO~ H2CO~ pCO2 (mEq/liter) (mEq/liter) (ram Hg) pH
24 1.8 60 7.22
24 1.5 50 7.30
24 1.2 40 7.40
24 0.9 30 7.52
Checking the Consistency of Laboratory Reports
It is not unusua l , p a r t i c u l a r l y at n igh t and on weekends, for acid-base r e p o r t s to be d i f f e r e n t f rom w h a t would be expected based on the pa- t ien t ' s c l in ical condit ion and the re- sul ts of previous l abora to ry studies. As a consequence , w h e n we d r a w blood gas studies, we will f requent ly do electrolyte de t e rmina t ions at the same t ime.
The b icarbonate can be es t ima ted in two ways - - from the blood gases and from the C(h content. A var ie ty of g raphs , n o m o g r a m s or o ther de- vices have been const ructed to corre- la te pH, pC(h and bicarbonate . 11 The b icarbonate ob ta ined in th i s manner can then be compared wi th tha t es- t ima t ed from the C(h content . Usu- ally, the b icarbonate e s t ima ted from the pH and pC(h is app rox ima te ly 1.0 to 2.0 mEq/ l i te r less t h a n the C(h content.
O the r e l ec t ro ly t e v a l u e s m a y be he lpfu l in e s t i m a t i n g the p a t i e n t ' s acid-base s ta tus . Those wi th acidosis tend to have h igher po tass ium levels t h a n those wi th a lka los is because, as t he i n c r e a s e d E C F h y d r o g e n ions en te r the cells, po tass ium ions will t e n d to l e a v e ce l l s and e n t e r t he ECF. TM In genera l , a r ise or fall in pH of 0.10 is a s soc i a t ed w i th a corre- sponding rise or fall of 0.5 mEq/ l i te r in se rum po tass ium levels. Thus, a p a t i e n t w i t h a pH of 7.30 a n d a s e r u m p o t a s s i u m of 4.8 m E q / l i t e r would tend to have a s e rum potas- s i u m l e v e l of 3.8 i f h i s pH were ra ised to 7.50.
In a d d i t i o n , c h l o r i d e a n d b ica r - bonate move in opposi te direct ions. Thus, pa t i en t s wi th a metabol ic al-
k a l o s i s t e n d to have low ch lo r ide levels while those wi th acidosis tend to have normal , or e levated, levels.
CLINICAL ACID-BASE PROBLEMS
Respiratory Alkalosis
E t i o l o g y . In most s t ressful s i tua- t i o n s , eg, e a r l y s e ps i s , shock or t r auma , there is a tendency for the p a t i e n t to h y p e r v e n t i l a t e a n d de- velop r e s p i r a t o r y a lka los i s , w i th a pC(h of about 25 to 35 m m Hg.3~, 14 Ma in t enance of no rma l ven t i l a t ion , w i th a pCO2 of 40 m m Hg, u n d e r such c i r c u m s t a n c e s , s h o u l d be a cause for concern. Pa t i en t s who are not h y p e r v e n t i l a t i n g when suffering from shock, sepsis or t r a u m a appear to have an i n c r e a s e d r i s k of sub- sequen t ly deve loping acute respi ra- tory fai lure.
In a smal l n u m b e r of pa t i en t s wi th severe sepsis, a metabol ic a lka los is of u n k n o w n e t i o logy wil l develop, in spite of the r e sp i r a to ry alkalosis . 15 In most, however, as the i r cl inical si tu- a t i o n d e t e r i o r a t e s , a m e t a b o l i c acidosis develops, the pa t i en t hyper- ven t i l a tes even more and the pC(h falls fur ther . Eventua l ly , i f shock or severe sepsis pers is ts for an extended period, the lung 's ab i l i ty to e l imina te C(h becomes impaired . Then, even if b i ca rbona te levels cont inue to fall, pC(h may beg in to r e tu rn to normal . This rise in pC(h , even though st i l l lower t han normal , is an impor t an t sign of pu lmona ry de te r iora t ion and is an excel len t example of the princi- ple t h a t t r e n d s or c h a n g e s a r e of much g r e a t e r cli~nical s i gn i f i cance t h a n absolute levels. Termina l ly , the lungs may become so damaged that , in spite of an increased minu te venti- lat ion, the pC(h may r ise above 45
m m Hg, c a u s i n g a combia~( metabol ic and r e sp i r a to ry acidosis tt develop. Very few pa t i en t s survive i al lowed to develop a pers i s ten t , c0~ b i n e d m e t a b o l i c a n d r e sp i r a to r i acidosis.
O the r condi t ions a s soc ia t ed witt an acu te h y p e r v e n t i l a t i o n includt s a l i c y l a t e i n t o x i c a t i o n , hyper. t h y r o i d i s m and r e s t r i c t i v e pulra0 na ry diseases. An infrequent , but el. t r eme ly in te res t ing , phenomenon ii the uncontrol lable progress ive acu~ r e s p i r a t o r y a l k a l o s i s t h a t m a y de., velop in o therwise h e a l t h y individu. als, pa r t i cu l a r ly those wi th hysteri~ cal hyperven t i l a t ion . This phenon~e~ non is expla ined by changes in cerel bra l blood flow and pH as the pC(~ falls. One of the m a i n determinan~ of c e r e b r a l b lood f low is arterial pC(h . A sudden, severe respiratory a lka los is can cause enough cerebral vasoconstr ic t ion to produce cerebra] i s c h e m i a a n d loca l metabolic acidosis. '~ This i n t r a c e r e b r a l met.~ abolic acidosis will cause the respi.i r a to ry center to s t imu la t e ventilati0nl even more, producing a progressively severe r e sp i r a to ry a lkalos is .
P a t h o p h y s i o l o g y . W i t h a very ~ rap id deve lopment of resp i ra to ry alJ k a l o s i s , a 10 m m H g d e c r e a s e in pCO2 wi l l c ause a p p r o x i m a t e l y a 0.10 increase in pH. Thus, if a pc. t i en t wi th pH, 7.40 and pC(h , 40 m~ Hg, sudden ly began to hyperventi. la te and his pC(h fell to 30 m m Hg, h i s pH w o u l d r i s e to a b o u t 7.50. Wi th in an hour or two, t i ssue buffers and, to a lesser extent , hemoglobin wil l p a r t i a l l y compensa te for these changes so t ha t the pH wil l fall back s l ight ly , to about 7.48. Wi th chronic h y p o c a p n i a , r e n a l compensatory, mechan i sms become impor tan t . 17
D i a g n o s i s , D i a g n o s i s of a re. sp i ra tory a lka los i s is based on clini. cal evidence of hype rven t i l a t i on and labora tory f indings of a h igh pH as. soc ia ted w i t h low pCO2. Occasion" a l ly , i t m a y be d i f f i cu l t to differ. en t ia te be tween hyperven t i l a t ion 0i hys t e r i ca l or ig in and hyperventila" t ion as a response to sepsis or pul. monary emboli . Under such circur~" stances, careful , cont inued, observa" t i on of t h e p a t i e n t a n d h is blood gases (especia l ly the pO2) is esseX'! t ial .
T r e a t m e n t . I f t h e pCO2 falls
Page 518 Volume 5 Number 7 July 1976 , , , ~ P

below 20 to 25 m m Hg, hypocarb ia SaY s e r i o u s l y i n t e r f e r e w i t h car - diovascular and cerebra l function. TM
~reatment of r e s p i r a t o r y a l k a l o s i s dae to hys te r i ca l hype rven t i l a t ion is often bes t accompl i shed by h a v i n g pthe pa t i en t r eb rea the his expi red air , ~hich has a r e l a t i v e l y h igh pCO=, antil h is a r t e r i a l p C ( h r e t u r n s 'to normal. The m o s t c o n v e n i e n t re- breathing device is a paper bag. Once che pCO= beg ins to r e t u r n t o w a r d normal, the cerebra l blood flow ap- Iparently i m p r o v e s e n o u g h so t h a t in t racerebra l ac idos i s is co r r ec t ed and the ven t i l a to ry pa t t e rn can re- turn to n o r m a l . S e d a t i o n m u s t be given c a r e f u l l y because t h e s e pa- tients o f t e n b e c o m e e x c e s s i v e l y llethargic af ter the cycle of hyperven- tilation and r e sp i r a to ry a lka los is has been broken.
In c r i t i c a l l y - i l l p a t i e n t s w i t h a mild-moderate r e sp i r a to ry a lkalos is , ibut not on a resp i ra tor , sedat ion may be used bu t very caut ious ly because hypoventi lat ion or hypox ia or both nlay rap id ly develop in such individ- uals. If the pa t i en t is on a respi ra tor , sedation a l o n g w i t h t h e g r a d u a l addition of 50 to 100 ml of dead space !at a t ime , (be tween the r e s p i r a t o r band the p a t i e n t ) m a y r e s t o r e t he pC(h to about 35 m m Hg, which we consider op t imal for these pat ients . Up to 300 ml of dead space can often Ibe added in such c i rcumstances bu t the p a t i e n t m a y t o l e r a t e f a r t h e r additions poorly.
Respiratory Acidosis
Et io logy . Resp i ra to ry acidosis re- sults from any process t ha t e levates pCO=. An impor tan t , and f requent , cause is hypoven t i l a t ion subsequent to c e n t r a l n e r v o u s s y s t e m (CNS) !damage or disease, drug overdose, or d amage to the chest wall , d i a p h r a g m or lungs. Ano the r f requent cause is aa increase in pulmonary dead space, ie, areas of the lung which are venti- lated bu t not perfused, as may occur ~'~ith e m p h y s e m a or pu lmona ry em- ~01i.
Severe r e sp i r a to ry acidosis is un- COmmon in the c r i t i c a l l y i l l or in- JUred, u n l e s s t h e p a t i e n t has pre- existing chronic obs t ruc t ive pulmo- l~ary disease (COPD) . :Pa t i en t s wi th '~evere COPD m a y have a chronica l ly lelevated pC02. In a pa t i en t wi th pre- Viously no rma l lungs, however, if the
pCO2 exceeds 40 to 45 m m Hg, ear ly in tuba t ion to provide ven t i l a to ry as- s is tance should be considered. Such pa t ien t s are expected to hypervent i - la te and i f they don't , someth ing is often wrong w i th the CNS (drugs, d i s e a se or t r a u m a ) , a i r w a y , ches t wall , d i a p h r a g m or lungs.
In g e n e r a l , a r i s e in t h e pCO2 s t imula te s the r e sp i r a to ry center to cause i n c r e a s e d v e n t i l a t i o n . How- ever, when the a r t e r i a l pCO2 begins to approach, or exceed, 70 m m Hg, it ac t s to d e p r e s s t h e r e s p i r a t o r y center . U n d e r such c i r cums tances , the s t imulus for ven t i l a t ion is pro- vided p r i m a r i l y by a decreased pO2 ac t i ng on chemorecep to r s , such as the carot id or aort ic bodies. In such pat ients , the admin i s t r a t i on of oxy- gen may severe ly depress, or arres t , v e n t i l a t i o n and cause a dange rous hypercarb ia .
P a t h o p h y s i o l o g y Wi th the acute d e v e l o p m e n t of a r e s p i r a t o r y aci- dosis, a 10 m m Hg increase in pC(h produces a p p r o x i m a t e l y a 0.10 de- crease in the pH. Thus, if a pa t i en t wi th a pH of 7.40 and pCO2 of 40 mm Hg suddenly began to hypovent i l a te and his pCOe rose to 50 m m Hg, his pH would fall to about 7.30. Wi th in an hour or two, however, some buf- f e r i n g occurs , p r i m a r i l y by t i s s u e bu f f e r s a n d to a l e s s e r e x t e n t by hemoglobin so t ha t the pH will rise to about 7.32. Dur ing the next two to four days , t h e r e is i nc reased prox- ima l t u b u l a r exchange of N a ÷ for H+. 19 As a consequence, b icarbonate is p rese rved , i nc reased a moun t s of chloride and hydrogen ion appear in the ur ine and, thus, a pa r t i a l l y com- p e n s a t i n g m e t a b o l i c a l k a l o s i s de- velops. 2°
D i a g n o s i s . Pa t i en t s wi th respi ra- to ry ac idosis have a pH less t h a n 7.40 and a pCO2 g rea te r t han 45 mm Hg. Most pa t i en t s wi th COPD are el- d e r l y a n d h a v e an i n c r e a s e d an- te r ioposter ior chest d iameter . Occa- s ional ly , however , younger , appar - en t ly he a l t hy ind iv idua ls may have s ignif icant emphysema tous changes, drug overdose or damage to the CNS, a i r w a y , c h e s t wa l l , d i a p h r a g m or lungs. Repea t blood gas de te rmina- t ions and e v a l u a t i o n of the t i m e d v i t a l capac i ty a re p a r t i c u l a r l y im- por t an t in eva lua t i ng pa t ien t s wi th COPD or neurogenic problems.
T r e a t m e n t . T r e a t m e n t of res - p i ra tory acidosis is designed to im- prove a lveo la r ven t i l a t ion 21 and may i n c l u d e b r o n c h o d i l a t o r s , such as a m i n o p h y l l i n e , or v a r i o u s sym- pa thomimet i c agents , such as isopro- t e r e n o l or a d r e n a l i n . In t r e a t i n g these p a t i e n t s , chronic r e s p i r a t o r y acidosis should be corrected slowly. 22 S ince b i c a r b o n a t e l e v e l s c h a n g e slowly, r ap id correct ion of a respira- t o r y a c i d o s i s , a f t e r c o m p e n s a t o r y me tabo l i c a l k a l o s i s has developed, can cause the sudden development of a s eve re c o m b i n e d m e t a b o l i c and r e s p i r a t o r y a lka los is . This m a y re- s u l t in c a r d i a c a r r h y t h m i a s , or d e a t h , b e c a u s e t h e c o m b i n e d al - kalosis can cause an abrup t fall in the concentra t ion of ionized calc ium in the p lasma. To p reven t this , the pC(h in pa t ien t s wi th chronic respi- r a to ry acidosis should genera l ly not be co r r ec t ed a t a r a t e more r a p i d t h a n 5 m m Hg per hour.
Rapid correct ion or p revent ion of an acu te r e s p i r a t o r y ac idosis is of p a r t i c u l a r i m p o r t a n c e in p a t i e n t s wi th recent t r a u m a or hypoxic b ra in damage. Hype rca rb i a can aggrava te g rea t ly the cerebra l edema in such pa t ien ts by producing excessive cere- bra l vasodi la t ion and increased cere- b r a l b lood flow. In such p a t i e n t s , ma in t enance of a mi ld-modera te res- p i ra to ry a lka los i s wi th a vent i la tor may cause cerebra l vasoconstr ic t ion to d r a m a t i c a l l y r e d u c e c e r e b r a l edema, a t l eas t t emporar i ly .
Metabolic Acidosis
E t i o l o g y . The causes of metabolic ac idos i s m a y be d i v i d e d in to two m a i n grot lps : (1) those a s s o c i a t e d wi th increased product ion of organic acids, and (2) those associated wi th a loss of b ica rbona te . 23 These can be d i f ferent ia ted by ca lcu la t ing the '~an- ion gap," which represen t s the sums of the "unmeasured" se rum anions, inc lud ing sulfates , phosphates , pro- te ins and organic acids such as lactic acid. Normal ly , the Na ÷ concentra- t ion is 138 to 142 mEq/ l i te r and the sum of the CO2 content and chloride anions is 124 to 131 mEq/l i ter . Thus, the d i f fe rence b e t w e e n the sum of two a n i o n s (CO2 c o n t e n t a n d chloride) and the sodium n o r m a l l y averages 10 to 15 mEq/ l i ter . In pa- t i e n t s w i t h m e t a b o l i c ac idos i s re- su l t ing from excessive acid produc-
• [ ] •P July 1976 Volume 5 Number 7 Page 519

t ion, the anion gap tends to be in- creased. On the other hand, in those wi th me tabo l i c acidosis due to the loss of b i c a r b o n a t e , (such as wi th d i a r r h e a , l a r g e p a n c r e a t i c f i s tu l i , d is ta l r ena l t u b u l a r acidosis, adrena l insufficiency, or use of Diamox) the anion gap tends to r ema in re la t ive ly normal .
The most f requent cause of acute metabol ic acidosis in the cr i t ica l ly ill or i n j u r e d is i m p a i r e d ce l l me t - abo l i sm r e s u l t i n g from i n a d e q u a t e t issue perfusion. If there is reduced t i s sue blood supp ly , e n e r g y in the fo rm of a d e n o s i n e t r i p h o s p h a t e (ATP) is produced by anaerobic proc- e s se s w h i c h a r e i n e f f i c i e n t . Fo r example , one mole of glucose can be broken down anaeorb ica l ly into two moles of pyruva te wi th the re lease of only two moles of ATP. However, if a d e q u a t e oxygen is a v a i l a b l e , the pyruva te can en te r the Kreb ' s cycle, where i t is b r o k e n down into CO2 and wa te r wi th the even tua l re lease of 38 moles of ATP. When adequate oxygen is not ava i lab le , the pyruva te cannot en te r the Kreb ' s t r icarboxyl ic acid cycle, and the pyruva te is con- ve r t ed into l a c t a t e and lac t ic acid tha t , as they accumula te , cause an i n c r e a s i n g l y severe m e t a b o l i c aci- dosis.
A rare , bu t in t e res t ing , cause of metabol ic (lactic) acidosis is adminis- t r a t ion of phenformin hydrochlor ide (DBI), to d iabet ic pa t ien ts , par t icu- l a r l y those wi th r e n a l d i sease and azo temia or ca rd iovascu la r col lapse of any type. 24 In such pa t ien ts it may be cl inical ly difficult to d i f ferent ia te be tween the metabol ic acidosis due to diabet ic ketoacidosis and tha t due to lactic acidosis produced by DBI.
P a t h o p h y s i o l o g y . An increase in the h y d r o g e n ion concen t r a t i on in blood a lmost immed ia t e ly resu l t s in an increase in a lveo la r ven t i l a t ion , med ia ted th rough the medu l l a ry res- p i ra to ry center , which is s t imula ted p r imar i l y by a fal l in the pH of the m e d u l l a r y i n t e r s t i t i a l f lu id . In a s tudy of normal subjects and pa t ien t s w i th chronic r e n a l d isease , i t was found 5 that , in a pure compensated s ta te , each mEq / l i t e r fal l in b icar- bonate resul t s in a 1.1 mm Hg fall in the pCO2. If the fal l in pCO2 is less t han 1.0 mm Hg/mEq fall in bicar- bonate, the r e sp i ra to ry compensat ion
is abnormal . Thus, if the b icarbonate fa l l s from 24 to 12 m E q / l i t e r , the pCO2 would be expec ted to fal l a t leas t 12 x 1.1 or 13.2 mm Hg. Later , r ena l excret ion of acid may become an impor t an t pa r t of the a t t empt to compensate for metabol ic acidosis.
D i a g n o s i s . The ac id-base abnor- mal i t i e s charac te r i s t i c of metabol ic acidosis include a p l a sma bicarbon- ate less t h a n 21 mEq/ l i te r and a base deficit. These pa t ien ts charac ter i s t i - cal ly appear qui te ill, and genera l ly will hypervent i l a te , marked ly , in an a t t e mp t to produce a compensa tory resp i ra to ry alkalosis .
Many inves t iga tors25 , 26 have at- t empted to corre la te lac ta te concen- t ra t ions wi th prognosis. In general , the h igher the lac ta te levels, the less l ike ly the pa t i en t is to survive. How- ever, we have found tha t i t genera l ly t akes longer to perform lac ta te de- t e rmina t ions t han i t does to es t imate the b icarbonate levels from pH and pCO2 and these b i ca rbona te levels usua l ly provide essen t ia l ly the same informat ion. If pyruva te levels were also avai lab le , the '~excess lacta te , ''27 probably a more accurate indicator of i n a d e q u a t e c e l l u l a r m e t a b o l i s m , could be calculated.
T r e a t m e n t . T r e a t m e n t is a imed, in i t i a l ly , a t cor rec t ing the p r i m a r y problem. For shock, t h i s p r i m a r i l y involves the improvemen t of t i ssue perfusion; for d iabetes mel l i tus , this includes the admin i s t r a t i on of insu- l in . I f m e t a b o l i c ac idos i s p e r s i s t s af ter such efforts, pa r t i cu la r ly if the pH is less t h a n 7.20, we find t h a t sod ium b i c a r b o n a t e shou ld be ad- minis tered. Bicarbonate deficits are ca lcula ted us ing 30% to 50% of the • body weight as the size of the bicar- bonate space. In pa t ien t s wi th acute m i l d - m o d e r a t e b i c a r b o n a t e def i - cits (less t h a n 10 mEq/l i ter) , a 30% b i c a r b o n a t e space o f t en p r o v i d e s adequa te correction. For b icarbonate deficits of 10 to 15 mEq/l i ter , 40% of the body we igh t can be used. How- ever, in pa t i en t s wi th severe acidosis ( w i t h b a s e d e f i c i t s e x c e e d i n g 15 m E q / l i t e r ) , t h e b i c a r b o n a t e space should be considered equal to 50% of the body weight.2 s :
For example , in an acute ly ill 80 kg man, wi th a b icarbonate concen- t r a t i on of 15 mEq/ l i t e r and a base deficit of 9 mEq/ l i ter , we would as-
sume a b icarbona te space of 30% ~ 24 l i ters. As a consequence, he wouli h a v e a t o t a l b i c a r b o n a t e deficit ~i 216 mEq. I n i t i a l l y , approximately! ha l f th is deficit would be correctt~ u s ing 108 mEq of b i c a r b o n a t e ad, min i s t e red in t ravenous ly over 40 t~ 60 minutes . The pa t i en t would the~ be re-evalua ted . On the other han~, if the same pa t i en t had a base deficit of 16 mEq/l i ter , the toal bicarbonate deficit would be ca lcu la ted as (80 kg x 50%) x 16 mEq/ l i te r = 640 mt~q. Only halt ' the total defici t is corrected a t a t ime. Then, the p a t i e n t is re. e x a m i n e d a n d f u r t h e r laboratory tests drawn. Each 50 ml ampule of 71/2% NaHCO3 contains 44.6 mEq 0f b icarbonate .
Metabolic Alkalosis
Etiology. Soine of the more corn. mon causes of metabol ic a lkalosis in. clude exCessive r emova l of acid (as wi th n a s o g a s t r i c a s p i r a t i o n of the stomach), hypochloremia , hypokale. mia (due to d i u r e s i s or diarrhea), s t e r o i d a d m i n i s t r a t i o n , massive t ransfus ions , and admin i s t r a t ion of large quan t i t i e s of Ringer ' s lactate or antacids:
S ince u r i n a r y potas .~ium loss is a lmost d i rec t ly prupor t ional to urine volume, la rge quan t i t i e s of diuretics can produce a severe hypokalemia w i t h an e x c e s s i v e c h l o r i d e loss. Dia r rhea , because of the high potas- s ium c o n c e n t r a t i o n p r e s e n t in the fluid excreted, may cause a sign:ft. c a n t h y p o k a l e m i a . Minera locor . t i co ids t e n d to cause a l k a l o s i s by f a v o r i n g p o t a s s i u m e x c r e t i o n and b ica rbona te reabsorpt ion . 29 Massive blood t ransfus ions resul t in increased quant i t i es of c i t ra te in the body. As this c i t ra te is metabol ized over the nex t 24 t o 48 hours , the resulting rise in b icarbonate levels causes a~ increas ing alkalosis .
In eva lua t i ng the po tass ium needs of a p a t i e n t w i t h a m e t a b o l i c al. kalosis, i t is impor t an t to recal l that the se rum po tass ium concentrations t end to change opposi te to the pt~. For every 0.10 increase in pH, the se rum po ta s s ium levels u sua l ly de. crease by about 0.5 mEq/l i ter . With acute po tass ium deficiences, approx" ima te ly 40 to 100 mEq of potassiur~ chloride a re needed to ra ise seru~ levels by 1 mEq/l i ter . Less is needed, however, i f the defici t has j u s t oc"
Page 520 Volume 5 Number 7 July 1976 ~ P

c~rred over the pas t few hours, if the patient is smal l or has a r e l a t ive ly small muscle mass.
p a t h o p h y s i o l o g y . Some authors s° have divided the s ta tes of metabol ic alkalosis in to " ch lo r ide - r e spons ive ~lkalosis" (in w h i c h t h e u r i n e chloride concent ra t ion is less than 10 to 20 m E q / l i t e r ) a n d " c h l o r i d e - resistant a l k a l o s i s " (in w h i c h the urine c h l o r i d e c o n c e n t r a t i o n is greater t han 10 to 20 mEq/l i ter) .
' Chloride responsive a lkalos is , such as that caused by vomit ing or exces- sive n a s o g a s t r i c suc t ion , causes a chloride def ic i t t h a t r e s u l t s in de- creased sodium reabsorp t ion in the proximal tubule . Inc reased sodium i0ncentration in the d is ta l tubule re- sults in inc reased exchange of H + and K + for Na + (coincident wi th the increased excret ion of H + and K +, there is increased "absorpt ion," or re- tention of HCO~, p e r p e t u a t i n g the ,alkalosis). If the re is K + deficiency, ~here is an even g rea te r excret ion of }I + and r e t e n t i o n of HCO5 which ~ay resul t in paradoxica l aciduria . If adequate chloride is admin i s t e red to these pat ients , increased chloride in ithe g l o m e r u l a r f i l t r a t e a l lows in- tcreased s o d i u m a b s o r p t i o n in t he proximal tubule. Less sodium is pre- sented to the d i s ta l tubule, less H + is excreted, less HCO~ is absorbed iand the metabol ic a lka los is begins to resolve.
C h l o r i d e - r e s i s t a n t a l k a l o s i s m a y tresult from minera locor t icoid excess p(such as in p r i m a r y h y p e r a l d o - steronism in which the d is ta l tubule is s t imula ted to reabsorb Na + in ex- change for H + a n d K + ) , s e v e r e chronic hypoka l emia and excess ad- ministration of b icarbonate , c i t ra te , and lac ta te - - al l of which .an form ~bicarbonate as they are metabolized. Since t h e s e p a t i e n t s a r e no t ~ypovolemic, la rge quan t i t i e s of Na + and C1- are f i l tered by the g lomerul i and increased H + and K + are ex- Icreted as Na + and HCO~ are reab- ~0rbed in the d i s ta l tubule.
The a m o u n t of r e s p ! r a t o r y com- Pensation t ha t can b e accomplished by hypovent i la t ion in these pa t ien t s is very l imi ted , appa ren t l y because ithey w i l l on ly t o l e r a t e a m i l d - moderate amoun t of hypoxia. In gen- eral, the pCO2 will not exceed 55 to 60 mm Hg unless the a lka los is is se-
vere wi th the b icarbonate exceeding 45 m E q / l i t e r and/or the p a t i e n t is given oxygen.
D i a g n o s i s . The d i a g n o s i s of metabol ic a lka los is is based on labo- ra to ry s tudies t ha t show a base ex- cess, or a b icarbonate level, exceed- ing 26 mEq/ l i ter . In mos t instances, the re is an associa ted hypoka l emia and hypochloremia. Cl inical ly , these pa t i en t s a re cha rac t e r i zed by slow, shallow, resp i ra t ions (in cont ras t to the hype rven t i l a t ion gene ra l ly seen wi th metabol ic acidosis). The reduced pO2 and e leva ted pCO2 due to com- p e n s a t o r y h y p o v e n t i l a t i o n in such pa t i en t s may occasional ly resu l t in an erroneous diagnosis of pu lmonary insufficiency.
T r e a t m e n t . In t r e a t i n g metabol ic alkalosis , in i t i a l efforts are to correct the chloride deficit 3° t h a t is a lmost a lways p resen t . In most ins tances , the chloride deficit is approx imate ly double the b i c a r b o n a t e excess. For example, a chlor ide t ha t is 4 0 mEq less than norma l is often associated with a b icarbona te which is about 20 mEq more t han normal .
The chlor ide defici t is ca lcu la ted on t h e b a s i s of 20% of t h e body weight , or the ECF space, if the pa- t i en t is adequa te ly hydra ted . If the pa t i en t is severe ly dehydra ted , 60% of the body weight should be used to c a l c u l a t e t h e de f i c i t . H a l f t he chloride deficit is corrected at a t ime and, of the chloride given, approxi- ma te ly one four th is g iven as potas- s ium chloride and th ree four ths as sodium chloride.
If a hypoka l emia pers is ts after cor- rect ion of the chloride deficit, enough po tass ium is given to ra ise the se rum concentra t ion to 4.5 to 4.8 mEq/ l i te r to reduce the r ena l t u b u l a r reabsorp- t ion of b icarbonate . 31
If the a lka los i s is very severe (ie, CO2 content is 45 mEq/ l i t e r or more or i f t he p a t i e n t h a s t e t a n y ) , one fourth of the chloride deficit is given as p o t a s s i u m chlor ide , one ha l f as sodium chloride, and one fourth as 1% NH, C1 or HC1. 32 Recen t ly , we have begun to use 0.15 normal hy- d roch lo r ic acid, i n f u s i n g i t s lowly into a large ve in at approx imate ly 25 to 50 ml/hr, pa r t i cu l a r ly if a severe metabolic a lka los i s pers i s t s in spite of c o r r e c t i o n of t he c h l o r i d e a n d po t a s s iumde f i c i t s . In our in i t ia l ex-
pe r i ence , 0.1 n o r m a l h y d r o c h l o r i c acid has provided very good control of the metabol ic a lka los i s but i t mus t be m a n a g e d very careful ly. Argin ine hydrochlor ide was very effective and safe in t r e a t i n g these problems, 13 but i t h a s b e e n w i t h d r a w n f rom the marke t . In some instances , Diamox (acetazolamide) ~3 m a y be used to cor- rect a m i ld -mode ra t e metabol ic al- kalosis bu t these pa t i en t s are usua l ly too sick to t ake any medica t ions by mouth.
SUMMARY
Correct i n t e rp re t a t ion of acid-base a b n o r m a l i t i e s r e q u i r e s an un- d e r s t a n d i n g of t h e H e n d e r s o n - Hasse lba lch equat ion and the appro- p r i a t e r e l a t i onsh ip s be tween bicar- bonate levels and the pCO2 or car- bonic acid concentra t ion. All labora- tory tes t s m u s t be e x a m i n e d cri t i - cal ly in r e l a t ion to the pa t ien t ' s con- d i t i o n a n d t h e i r c o n s i s t e n c y w i t h other l abora to ry tests. Once a prob- l e m is i d e n t i f i e d a n d a c c u r a t e l y c a t e g o r i z e d , t h e r a p y is d i r e c t e d p r imar i ly at correct ing the under ly- ing problem and, only secondari ly, a t c o r r e c t i n g t h e n u m b e r s . T h e r a p y should be guided by con t inued pa- t i en t observa t ion and ser ia l labora- t o r y s t u d i e s , c o r r e c t i n g p r o b l e m s rapid ly only i f they develop rapid ly and ser iously t h r e a t e n the pa t ien t ' s life.
REFERENCES 1. Davenport HW: The ABCs of Acid- Base Chemistry, Chicago, University of Chicago Press, 1969, p 16. 2. Weisberg HF: A better understanding of anion-cation Cacid-base") balance. Surg Clin North Am 39:93, 1959.
3. Clark WM: Topics in Physical Chemis- try: A Supplementary Text for Students of Medicine, ed 2. Baltimore, Williams & Wilkins Co, 1952.
4. Bronsted JN: Einige Bemerkungen uber den Begriff der Sauren und Basen. Recueil des Trauaux Chimiques des Pays-Bas, 42:718, 1923.
5. Lennon EJ, Lemann J: Defense of hy- drogen ion concentrat ion in chronic metabolic acidosis. Ann Intern Med 65:265-274, 1966.
6. Huckabee WE: Henderson vs Hassel- balch. Clinical Research 9:116-119, 1961. 7. Kassirer JP, Bleich HI~: Rapid estima- tion of plasma carbon dioxide tension from pH and total carbon dioxide content. N Engl J Med 792:1067-1068, 1965.
8. Singer RB, Hastings AB: An improved clinical method for the estimation of dis-
~]~P July 1976 Volume 5 Number 7 Page 521

t u r b a n c e s of the ac id-base ba l ance of h u m a n blood. Medicine 27:223, 1948.
9. Astrup P: A new approach to acid-base metabolism. Clin Chem 7i1-15, 1961.
10. Schwartz WB, Relman AS: A critique of the parameters used in the evaluation of acid-base disorders. "Whole-blood buf- fer base" and " s t a n d a r d b i c a r b o n a t e " c o m p a r e d w i t h blood pH and p l a s m a bicarbonate concentration. N Engl J Med 268:1382-1388, 1963.
11. W e i s b e r g HF: C a l c u l a t o r far the Henderson-Hasselbalch equation, in Sun- derman FW (ed): Manual for Procedures for the Appl ied Seminar on Clinical Pathology of Respiratory Diseases, Phi ladelphia , Ins t i tu te for Clinical Sci- ence Inc, 1972, pp 239-245.
12. Brown EB, Goot t B: I n t r a c e l l u l a r h y d r o g e n ion c h a n g e s and p o t a s s i u m movement . A m J Physiol 204:765-770, 1963.
13. Wilson RF, Gibson DB, Percinel AK, et al: Severe alkalosis in critically-ill pa- tients. Arch Surg 105:197-203, 1972.
14. Wilson RF, McCarthy B, LeBlanc LP, et al: R e s p i r a t o r y and c o a g u l a t i o n changes af ter uncompl ica ted fractures. Arch Surg 106:395-399, 1973.
15. Wilson RF, Gibson DB, Percinel AK, et al: Severe alkalosis in critically-ill pa- tients. Arch Surg 105:197-203, 1972.
16. Lassen NA: Control of cerebral circu- l a t ion in h e a l t h and disease. Circ Res 34:749-760, 1974.
17. Gennar i FJ, Goldstein MB, Schwartz WB: The na tu re of the renal adaptat ion to ch ron ic h y p o c a p n i a . J Clin Invest 51:1722-1730, 1972.
18. Trimble C, Smith DE, Rosenthal MH, et al: Pathophysiologic role of hypocarbia in p o s t - t r a u m a t i c p u l m o n a r y insuf f i - ciency. A m J Surg 122:633-638, 1971.
19. S h e p a r d RS: H u m a n Physiology. Phi l ade lph ia , JB Lippincot t Company, 1972, pp 399-400.
20. Bracket t NS, Wingo CF, Muren O, et al: Acid-base response to chronic hyper- capnia in man. N Engl J Med 280:124, 1969.
21. Sen io r RM, F i s h m a n AP: Dis tu r - bances of alveolar venti lat ion. Med Clin North A m 51:403-425, 1967.
22. Chr is tensen MS, Brodersen P, Olesen. J, e t al: C e r e b r a l apoplexy ( s t roke) t reated with or wi thout prolonged artifi- cial hypervent i la t ion: II. Cerebrospinal fluid acid-base balance and in t racrania l pressure. Stroke 4:620-631, 1973.
23. Bear RA, Gribik M: Assessing acid- base i m b a l a n c e s t h r o u g h l a b o r a t o r y parameters . Hospital Practice 9:157, 1974.
24. Assan R, Heuclin C, Girard JR, et al: P h e n f o r m i n - i n d u c e d lac t ic acidosis in diabetic patients . Journal of the American Diabetes Association 24:791, 1975.
25. Weil MH, Afifi AA: E x p e r i m e n t a l and clinical studies on lactate and pyru- vate as indicators of the severi ty of acute
c i rcu la tory fa i lure (shock). Circulatio~ 41:989-1001, 1970.
26. Peretz DI, McGregor M, Dossetor j~ Lacticacidosis: a clinically significant a~ pect of shock. Canadian Medical Associ~ tion 90:673-675, 1964.
27. H u c k a b e e WE: M e t a b o l i c co~s~. quences of chronic hypoxia. Ann N Y Ac~ Sci 121:723-730, 1965.
28. Kassi rer JP: Serious acid-base dis0r, ders. N Engl J Med 291:773-776, 1974.
29. Giebish G, MacLeod MB, Pi t ts R~: Effect of adrenal steroids on renal tubulat reabsorption of bicarbonate. A m J Physiol 183:377~-386, 1955.
30. Kassi rer J, Be rkman P, Lawrenz~i et al: The critical role of chloride in th~ correct ion of hypoka lemic alkalosis i~ man. A m J Med 38:172-189, 1965.
31. Ful ler F, MacLeod MB, Pit ts RF: I~ I f luence of a d m i n i s t r a t i o n of potassiu~ salts on the renal tubu la r reabsorption bicarbonate. A m J Physiol 182:111-11~, 1955.
32. Abouna GM, Veazey PR, Terry D~: In t ravenous infusion of hydrochloric acid for t r e a t m e n t of m e t a b o l i c alkalosis. Surgery 75:194-202, 1974.
33. Mudge GH: D i u r e t i c s and other agents employed in the mobilization of edema fluid. Goodman LS, Gi lman A, (eds): Pharmacological Basis of Therapeu. tics. New York, M a c m i l l a n Company 1965, chapter 4, p 840.
Page 522 Volume 5 Number 7 July 1976 ~]~P