approach to ct chest 578
DESCRIPTION
TRANSCRIPT

CT CHESTCT CHESTGiselle Revah
University of Toronto Class of 0T7
Dr. N. Jaffer Staff Radiologist MSH and University of Toronto

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
THE BASICSTHE BASICS
1. The different options for CT imaging of the lung
2. An approach to looking at chest CT’s
3. A few disease patterns that will help you impress

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
CT TYPESCT TYPES1. Standard2. High Resolution3. Low Dose4. CT Angio

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
1. STANDARD CT1. STANDARD CT• Slice thickness: 3-10 mm • scans a large volume, very quickly • Covers the full lung• +/- contrast
Indications• CXR abnormality • Pleural and mediastinal abnormalities• Lung cancer staging• F/U metastases• Empyema vs abscess

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO • narrow x-ray beam collimation: 1-1.3mm vs. conventional 3-10mm
• cross sections are further apart: 10 mm• high definition images of lung
parenchyma: vessels, airspaces, airway and interstitium
• No contrast
2. HIGH RESOLUTION 2. HIGH RESOLUTION (HRCT)(HRCT)
STANDARD CT HRCT

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
2. HIGH RESOLUTION 2. HIGH RESOLUTION (HRCT)(HRCT)Indications• Hemoptysis • Diffusely abnormal CXR• Normal CXR with abnormal PFT’s • Baseline for pts with diffuse lung disease• Solitary pulmonary nodules• Reversible (active) vs. non-reversible
(fibrotic) lung disease • Lung biopsy guide• F/U known lung disease • Assess Rx response

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO• Premise: lower dose radiation will not
reduce the diagnostic functionality of the scan (eg. 250 mAs 50 mAs)
• Detail is decreasedUses• Screening
– ongoing trials • F/U
– infections– post lung transplant– metastases
3. LOW DOSE3. LOW DOSE

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO• contrast injected into peripheral vein • injection timing/rate controlled automatically • dye is where you want it during scan• replaced conventional catheter angiogram
Indications• Pulmonary embolism• Aortic aneurysms• Aortic dissection
Risks• Iodinated contrast:
– Allergic/ nephrotoxic
4. ANGIOGRAPHY 4. ANGIOGRAPHY (CTA)(CTA)

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO Three Windows1. Soft Tissue
APPROACHING THE APPROACHING THE ANATOMYANATOMY
2. Bone
3. Lung

DISEASE PATTERNS
CT TYPE
ANATOMY
INTROLook at these structures• Thyroid• Chest wall• Pleura
Heart• Chambers• CA calcifications• Pericardium
Vessels• Aorta• PA• Smaller vasculature
Nodes • mediastinal • axillary
1. SOFT TISSUE 1. SOFT TISSUE WINDOWWINDOW

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
Ascending aorta
Descending aorta
Main pulmonary artery
L pulmonary artery
R pulmonary artery
SVC
Azygous vein
Esophagus
What is this duct?
DISEASE PATTERNS
CT TYPE
ANATOMY
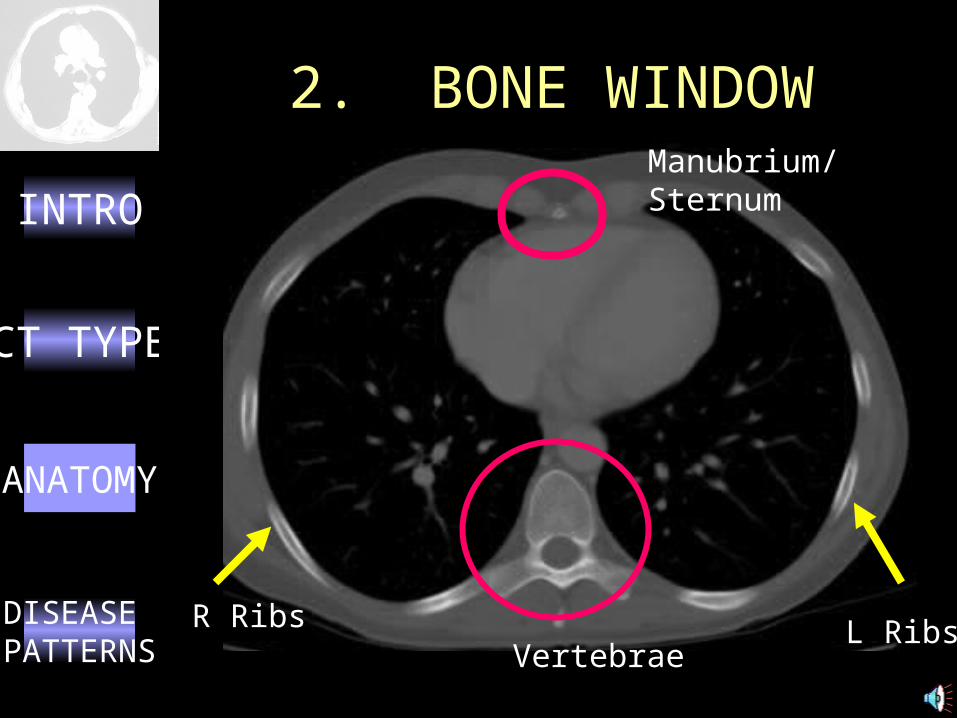
INTROManubrium/ Sternum
VertebraeR Ribs L Ribs
2. BONE WINDOW2. BONE WINDOW

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
3. LUNG WINDOW3. LUNG WINDOWAIRWAYS Bronchial Tree
Central
LLL
LUL
Fissure
RUL
RLL
PARENCHYMA
Fissure

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO 1. Air Bronchograms2. Bronchiectasis3. Septal Thickening4. Ground Glass Opacity5. Emphysema6. Nodules7. Filling Defect
COMMON COMMON PATHOLOGIC PATHOLOGIC FEATURESFEATURES

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRODescription• Bronchi become visible due to increased
attenuation of surrounding lung
• Implies proximal bronchi patency
• Excludes pleural or mediastinal lesion
DDx• Non-obstructive atelectasis
• Pneumonia
• Pulmonary edema
• Hemorrhage
• Bronchioloalveolar carcinoma
• Lymphoma
1. AIR 1. AIR BRONCHOGRAMSBRONCHOGRAMS

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRODilatation of medium-sized bronchi (>2 mm) impaired clearance recurrent infection bronchial
damage
Types1. Cylindrical2. Cystic3. Varicose
HRCT is diagnostic tool of choice
DDx• Infection• Bronchial obstruction• Cystic fibrosis • Primary ciliary
dyskinesia
2. BRONCHIECTASIS2. BRONCHIECTASIS
What type is this?
• Immunodeficiency states • alpha 1-Antitrypsin deficiency • RA and Sjögren• Pulmonary fibrosis
DISEASE PATTERNS
CT TYPE
ANATOMY
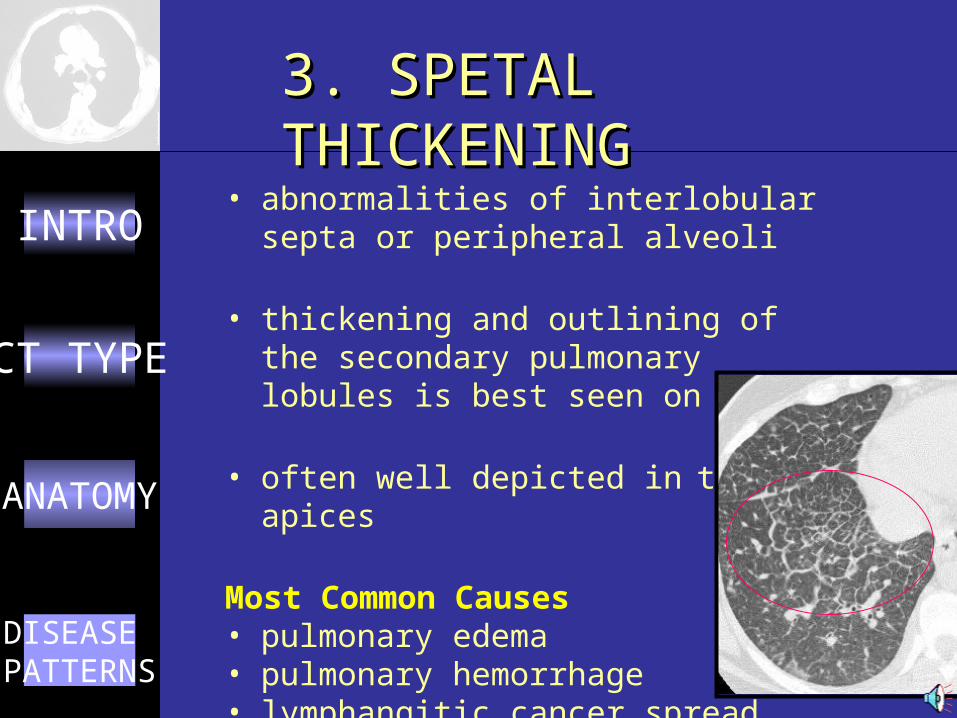
INTRO • abnormalities of interlobular septa or peripheral alveoli
• thickening and outlining of the secondary pulmonary lobules is best seen on HRCT
• often well depicted in the apices
Most Common Causes • pulmonary edema • pulmonary hemorrhage • lymphangitic cancer spread
3. SPETAL 3. SPETAL THICKENINGTHICKENING

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO• common nonspecific finding
• decreased air content without totally obliterating the alveoli
• increased lung opacity not sufficient to obscure pulmonary vessels
4. GROUND GLASS 4. GROUND GLASS OPACITIESOPACITIES
DDx• Alveolitis or interstitial
pneumonitis– Hypersensitivity pneumonitis– IPF– Sarcoidosis
• Pulmonary edema• Resolving pneumonia/
hemorrhage
Early
Dense

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO• permanent enlargement of air
spaces distal to the terminal bronchioles
• destruction of the walls without obvious fibrosis
Young pt with bullous emphysema at the lung bases.
What’s the diagnosis?
DDx• smoking • alpha 1-Antitrypsin deficiency• IV drugs• Immundeficiency• Vasculitis • Connective tissue disorders
5. EMPHYSEMA5. EMPHYSEMA

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO3 Types1. Centriacinar/lobular • respiratory bronchioles periphery• upper half of lungs • smoking
2. Panacinar• destroys entire alveolus uniformly • lower half of lungs• homozygous alpha1-antitrypsin
deficiency
3. Distal acinar/paraseptal• distal airway, alveolar ducts, and alveolar sacs• around the lung septae or pleura• apical bullae may spontaneously
pneumothorax
5. EMPHYSEMA5. EMPHYSEMA
What 2 types are found here?
DISEASE PATTERNS
CT TYPE
ANATOMY
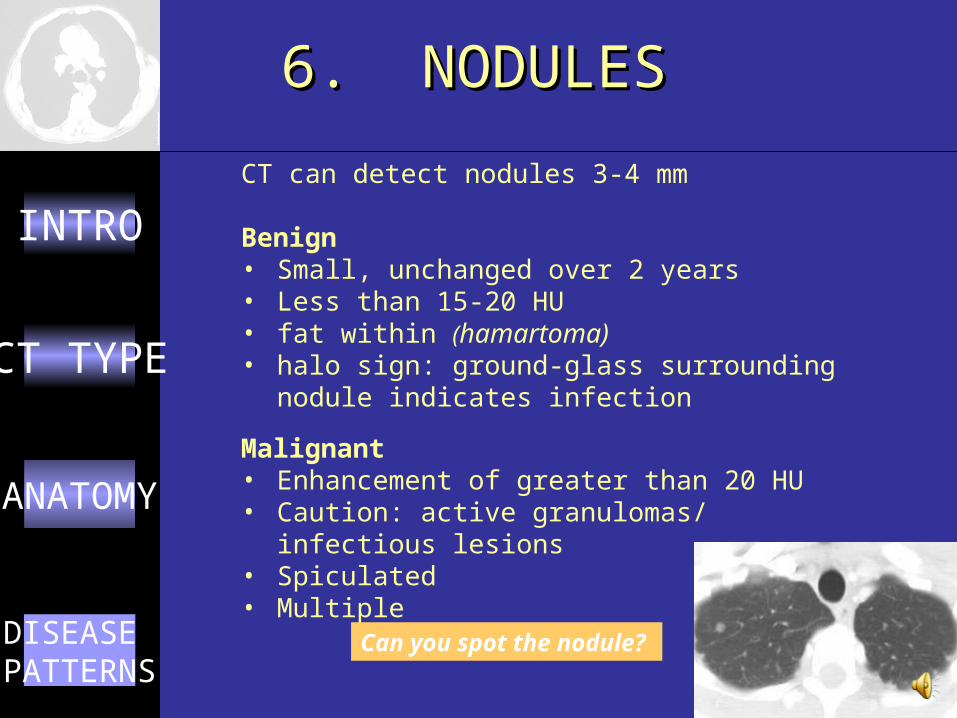
INTROCT can detect nodules 3-4 mm
Benign• Small, unchanged over 2 years• Less than 15-20 HU • fat within (hamartoma) • halo sign: ground-glass surrounding nodule
indicates infection
Malignant• Enhancement of greater than 20 HU• Caution: active granulomas/ infectious lesions• Spiculated• Multiple
6. NODULES6. NODULES
Can you spot the nodule?

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO
Circumscribed nodules suspect metastatic disease
Septated nodules, suspect primary lung malignancy
Neoplastic Infectious InflammatoryBenign (hamartoma)Bronchogenic CaMetsLymphoma
GranulomaAbscess
Rheumatoid arthritisWegener’s Sarcoidosis
6. NODULES6. NODULES

DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO• Pulmonary Embolism is a well defined hypodensity in the
pulmonary artery • CTA sensitive for PE (90%) • can’t evaluate arteries below 4th segmental level
DDx: • Anatomical landmarks and variants eg intersegmental
nodes• Vascular tumor invasion • Technical psuedo filling defects (eg flow artifact)
7. FILLING DEFECTS7. FILLING DEFECTS
DISEASE PATTERNS
CT TYPE
ANATOMY
INTRO1. Engeler CE, Tashjian JH, Trenkner SW, and Walsh JW.
Ground Glass Opacity of the Lung Parenchyma: A Guide to analysis with High Resolution CT. AJR 1993; 160: 249-251.
2. Collins, J. CT signs and patterns of lung disease. Radiol Clin North Am. 2001 Nov;39(6):1115-35.
3. Lee JKT, Sagel SS, Stanley RJ, Heiken JP. Computed Body Tomography with MRI correlation. 3rd ed. Raven Press NYC, 1998.
REFERENCESREFERENCES