approaches to pulmonary ibrosis - rcp london
TRANSCRIPT
NOVEL APPROACHES TO PULMONARY FIBROSIS
Gisli Jenkins FRCP PhD Professor of Experimental Medicine
University of Nottingham

OVERVIEW
Review of ILDs What is pulmonary
fibrosis? How should IPF be
diagnosed? How should IPF be
treated? Is personalised therapy
for IPF possible?

ILD OLYMPICS
IPF Sarcoidosis
Asbestosis CTD
HSP Drugs
NSIP
The rest

ILD OLYMPICS
NSIP
IPF
Sarcoidosis
Asbestosis HSP
CTD
Drugs The rest
RA

ILD OLYMPICS
Fibrotic
Granulomatous
Inflammatory

CHRONIC PROGRESSIVE FIBROTIC LUNG DISEASE OR INFLAMMATORY INTERSTITIAL LUNG DISEASE
Fibrotic IPF Fibrotic HSP Rheumatoid -UIP Asbestosis IPPFE
Inflammatory Sarcoid CTD-ILD HSP NSIP DIP RBILD LIP

DEFINITELY NOT IPF Hypersensitivity Pneumonitis
Metzger F et al. Chest 2010;138:724-726 ©2010 by American College of Chest Physicians
Sarcoid

NOT IPF AT THE MOMENT
NSIP
Marten al Eur Radiol 2009;19:1679-1685
ANA α-dsDNA Ribonucleoproteins
α-Ro and α-La (Sjogrens) α-Smith (SLE) α-Ro52 (none-specific)
α-Topoisomerase/Scl70 (SSc) α-PM/Scl (SSc/PM overlap) α-tRNA synthetases (PDM)
Jo-1 PL-7 PL-12
α-MDA5 (CADM) α-IgG4 (IG4RD) RA and α−CCP (RA) -UIP MPO (Vasculitis) -UIP

MYCOPHENOLATE MOFETIL VERSUS ORAL CYCLOPHOSPHAMIDE IN SCLERODERMA-RELATED INTERSTITIAL LUNG DISEASE (SLS II):A RANDOMISED CONTROLLED, DOUBLE-BLIND, PARALLEL GROUP TRIAL
Donald P Tashkin, Michael D Roth, Philip J Clements, Daniel E Furst, Dinesh Khanna, Eric C Kleerup, Jonathan Goldin, Edgar Arriola, Elizabeth R Volkmann, Suzanne Kafaja, Richard Silver, Virginia Steen, Charlie Strange, Robert Wise, Fredrick Wigley, Maureen Mayes, David J Riley, Sabiha Hussain, Shervin Assassi, Vivien M Hsu, Bela Patel, Kristine Phillips, Fernando Martinez, Jeff rey Golden, M Kari Connolly, John Varga, Jane Dematte, Monique E Hinchcliff , Aryeh Fischer, Jeff rey Swigris, Richard Meehan, Arthur Theodore, Robert Simms, Suncica Volkov, Dean E Schraufnagel, Mary Beth Scholand, Tracy Frech, Jerry A Molitor, Kristin Highland, Charles A Read, Marvin J Fritzler, Grace Hyun J Kim, Chi-Hong Tseng, Robert M Elashoff , for the Sclerodema Lung Study II Investigators*
www.thelancet.com/respiratory Published online July 25, 2016 http://dx.doi.org/10.1016/S2213-2600(16)30152-7
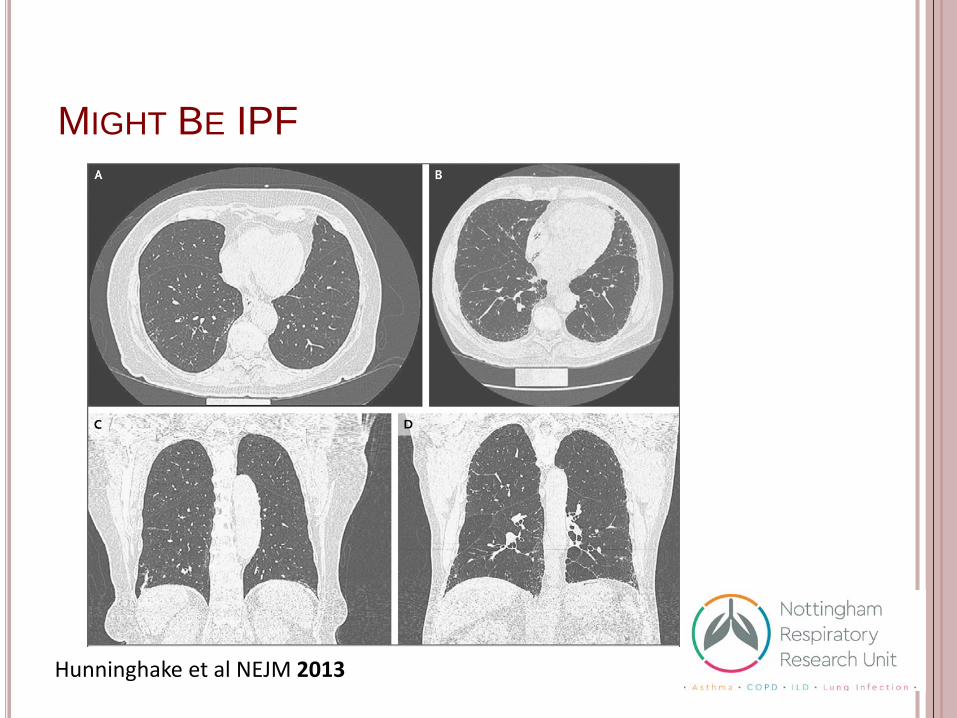
MIGHT BE IPF
Hunninghake et al NEJM 2013

DO INTERSTITIAL LUNG ABNORMALITIES REPRESENT EARLY PULMONARY FIBROSIS?
Putman et al JAMA 2016

IDIOPATHIC PULMONARY FIBROSIS
Elderly male ex-smokers Usually 2 year history of:
Progressive shortness of breath on exertion
Dry non productive cough On examination
Bilateral Basal Crepitations Clubbed
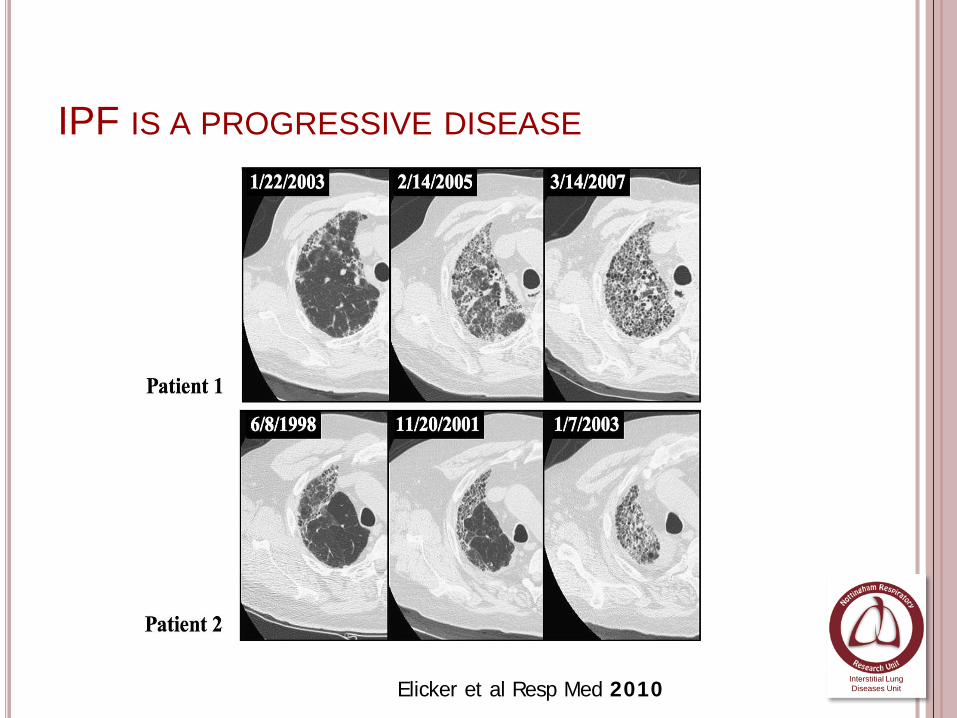
IPF IS A PROGRESSIVE DISEASE
Elicker et al Resp Med 2010 Interstitial Lung Diseases Unit

MORTALITY FROM IPF IN THE UK HAS INCREASED IN THE LAST 40 YEARS
0
500
1000
1500
2000
2500
3000
3500
1968
19
69
1970
19
71
1972
19
73
1974
19
75
1976
19
77
1978
19
79
1980
19
81
1982
19
83
1984
19
85
1986
19
87
1988
19
89
1990
19
91
1992
19
93
1994
19
95
1996
19
97
1998
19
99
2000
20
01
2002
20
03
2004
20
05
2006
20
07
2008
ICD-9 (1979)
ICD-10 (2000)
Navaratnam Thorax. 2011;66(6):462-7.

Vancheri ERJ 2010 35(3):496-504
.
5 year survival rates from IPF compared with various cancers.

CAUSES OF IPF
Idiopathic (and cryptogenic) means “we don’t know”
Genetics responsible for about 30%
Other hypotheses include: Viral infection Gastro-Oesophageal
Reflux Disease Inhaled dust/smoke

A POLYMORPHISM IN THE COMMON VARIANT OF MUC5B PROMOTES SUSCEPTIBILITY TO IPF
Fingerlin et al Nat Genet 2013

RARE VARIANTS ARE ASSOCIATED WITH FAMILIAL PULMONARY FIBROSIS
Telomerase TERT, TERC DKC1, PARN, NAF1 RTEL1, TINF2
Epithelial Cell Function SFTPA1 SFPTA2 SFPTC ABC3
6% patients in UK with IPF have 1° relative Currently we do not recommend genetic
screening These patients are eligible for 100k Genome
Project

DIAGNOSING IPF
HRCT Reticulation Honeycombing Traction
Basal Peripheral Subpleural
(ATS/ERS Criteria AJRCCM 2011)

LUNG FUNCTION

SHOULD VATS BIOPSIES BE PERFORMED? Leads to acute excarbations Mortality rate between 1.7-
2.4% Hutchinson et al Am J Respir Crit Care Med 2016, Hutchinson Eur Respir J 2016
Ventilation promotes TGFβ activation in the lung. Jenkins et al JCI 2006, John et al Science Signalling 2016
Mechanical stretch of IPF tissue has enhanced TGFβ activation. Froese et al Am J Respir Crit Care Med 2016

IPF MANAGEMENT
NICE IPF Guidelines (CG163) Put the MDT at the heart of management
NICE IPF Quality Standard (QS79) Patients should be diagnosed with IPF by MDT All patients should have access to a Specialist Nurse Should have ambulatory Oxygen assessments Should have access to Pulmonary Rehabilitation Should have access to Palliative Care
2 NICE approved drugs for IPF Pirfenidone (TA282) Nintedanib (TA379)

THE PANTHER STUDY
Triple therapy with Pred/AZA/NAC for IPF had significantly worse outcome compared with placebo. Death 8 vs 1 p < 0.01 Hospitalisation 23 vs 7 p < 0.001
Single agent NAC no benefit compared with placebo
Raghu et al N Eng J Med 2012 Martinez et al N Eng J Med 2014

DISEASE MODIFYING ANTIFIBROTIC DRUGS
Richeldi et al NEJM 2014 King et al NEJM 2014
Pirfenidone Nintedanib

BEST SUPPORTIVE CARE
Co-morbidities Withdraw ineffective or harmful
therapies Symptom relief
Dyspnoea Oxygen
Cough PPI Prednisolone Thalidomide Opiates

THERE IS STILL CONSIDERABLE PROGRESS NEEDED
Strict prescribing criteria for anti-fibrotic therapy IPF only FVC 80-50% Responders only
Large number of adverse effects Mechanism of action unclear

SAME DISEASE DIFFERENT COURSE
Adapted from Ley B et al, Am J Respir Crit Care Med 2011
Time
Dise
ase
Prog
ress
ion
1 yr 2 yr 3 yr 4 yr 5 yr 6 yr
Onset of Disease
Onset of Symptoms
Diagnosis
Death
Sub-clinical Period
Pre-diagnosis Period
Post-diagnosis Period
A B C D
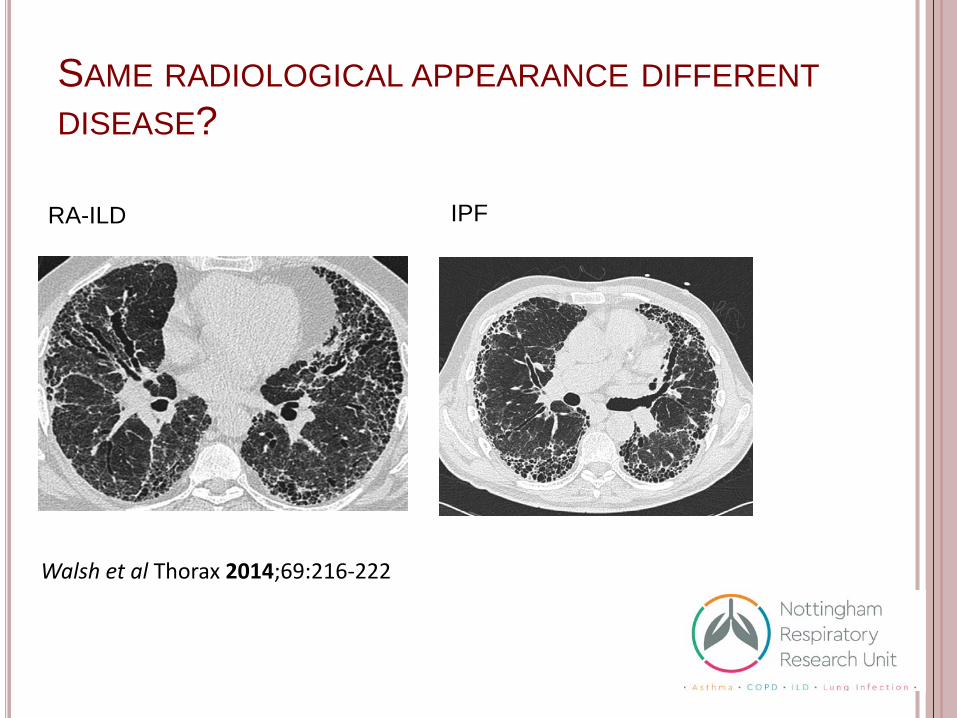
SAME RADIOLOGICAL APPEARANCE DIFFERENT DISEASE?
Walsh et al Thorax 2014;69:216-222
RA-ILD IPF

ARE CURRENT CLINICAL STRATA OF FIBROTIC LUNG DISEASE FIT FOR PURPOSE?
Ryerson et al ERJ 2013 Kim et al. Chest. 2009

Protein MMP7/ SpD Matrix Neoepitopes
Lung Tissue Integrins
Transcript
Genome muc5B Cla
ssic
al IP
F
Atyp
ical
IPF
IPF
+ Em
phys
ema
IPF
+ as
best
os e
xpos
ure
IPF
+ R
A
Acce
lera
ted
IPF
MicroRNA mir29
IPF
+ Pu
lmon
ary
Hyp
erte
nsio
n
IPF
+ Lu
ng C
ance
r
Can Pulmonary Fibrosis be stratified?
Therapy In
ters
titia
l Lun
g Ab
norm
aliti
es

Noth et al Lancet Resp Med 2013
Peljto et al JAMA 2013
MUC5B AND TOLLIP POLYMORPHISMS ARE ASSOCIATED WITH SLOWER PROGRESSION OF IPF

SERUM BIOMARKERS MAY BE USEFUL IN SCREENING EARLY DISEASE
Kropski et al Am J Respir Crit Care Med 2015
MMP7 SpD

CAN IPF BE STRATIFIED BY RESPONSE TO THERAPY?
Responders vs Non-responder The challenge in IPF is defining ‘treatment response’ We currently use >10% absolute drop in FVC We need more dynamic markers of disease which better
reflect disease biology

THE PROFILE STUDY

MATRIX NEOEPITOPES
Karsdal MA et al Assay Drug Dev Technol 2013
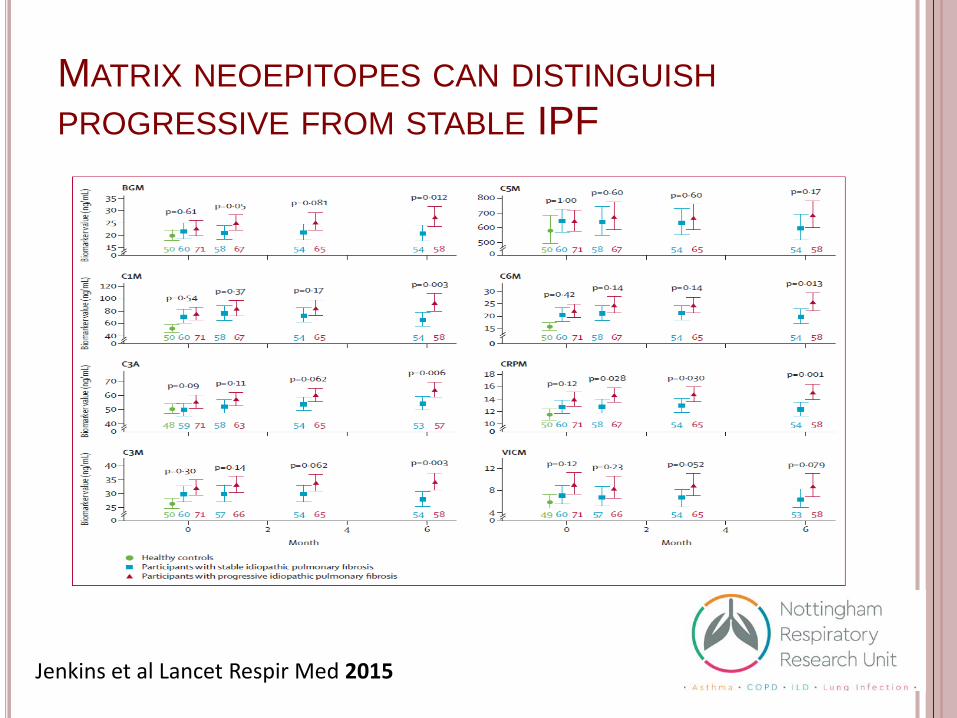
MATRIX NEOEPITOPES CAN DISTINGUISH PROGRESSIVE FROM STABLE IPF
Jenkins et al Lancet Respir Med 2015

PATIENTS WITH RISING MATRIX NEOEPITOPES HAVE INCREASED RISK OF MORTALITY
Jenkins et al Lancet Respir Med 2015
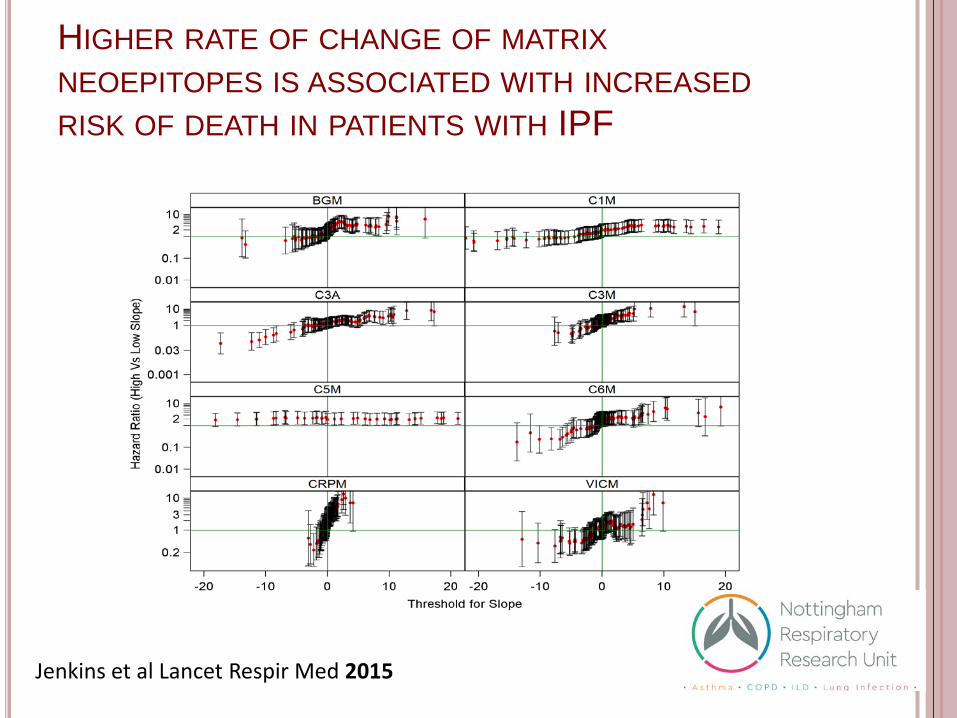
HIGHER RATE OF CHANGE OF MATRIX NEOEPITOPES IS ASSOCIATED WITH INCREASED RISK OF DEATH IN PATIENTS WITH IPF
Jenkins et al Lancet Respir Med 2015

CAN WE IDENTIFY MOLECULAR ENDOTYPES OF PULMONARY FIBROSIS
Identify a subset of pulmonary fibrosis with a specific behaviour
Conserved across clinical phenotypes Targetable by specific therapies Identified by specific biomarkers
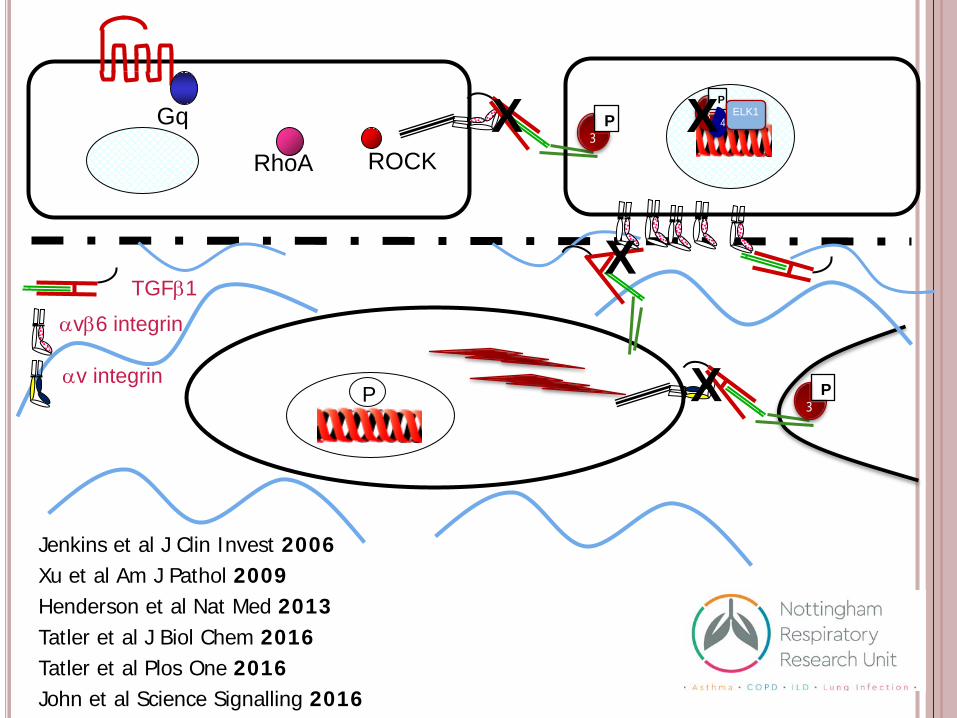
TGFβ1 αvβ6 integrin
P
Gq
RhoA ROCK
P 3
P 3
αv integrin
X
X
P
4 3 ELK1 X
X
Jenkins et al J Clin Invest 2006 Xu et al Am J Pathol 2009 Henderson et al Nat Med 2013 Tatler et al J Biol Chem 2016 Tatler et al Plos One 2016 John et al Science Signalling 2016

THE αVβ6 INTEGRIN IS UPREGULATED IN REGIONS OF FIBROSIS IN PATIENTS WITH UIP
Xu et al Am J Pathol 2009
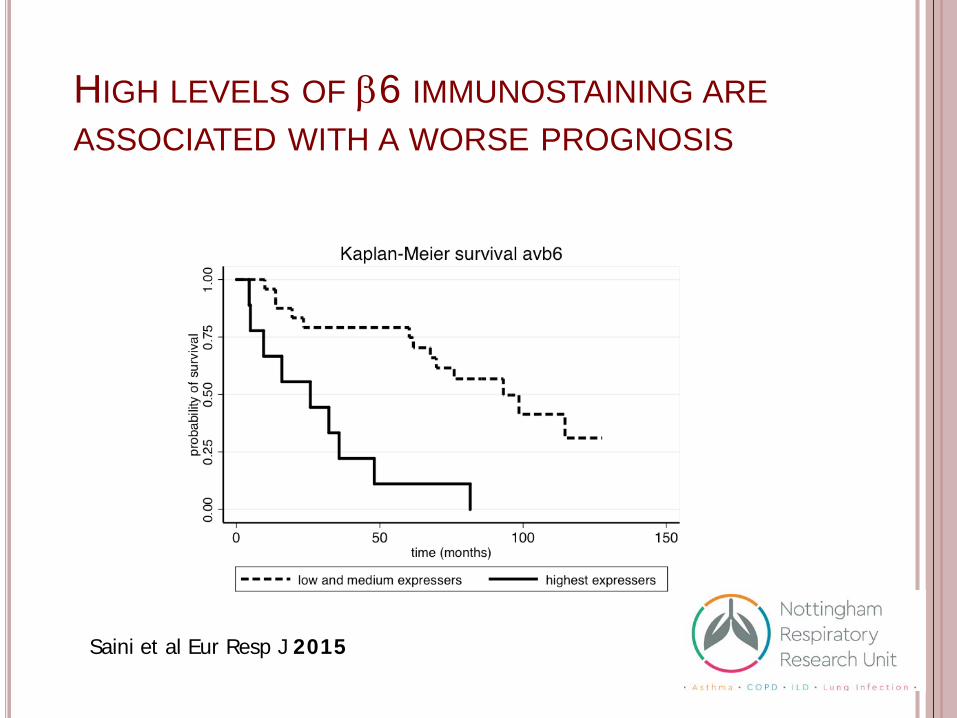
HIGH LEVELS OF β6 IMMUNOSTAINING ARE ASSOCIATED WITH A WORSE PROGNOSIS
Saini et al Eur Resp J 2015

Bleomycin + anti-αvβ6
bleomycin saline
Binding of 111In-DTPA-A20FMDV2 (β6 specific peptide)
αvβ6 Specific peptide
Control peptide
saline bleo
John et al J Nuc Med 2013
THE αvβ6 INTEGRIN IS UPREGULATED FOLLOWING BLEOMYCIN INDUCED LUNG INJURY

A β6 TARGETING PEPTIDE CO-LOCALISES WITH AREAS OF FIBROSIS FOLLOWING BLEOMYCIN INSTILLATION
John et al J Nuc Med 2013

CONCLUSIONS 1
ILDs should be considered inflammatory or fibrotic
Inflammatory ILDs can be treated with steroids and immunosuppression
Fibrotic ILD should NOT be treated with steroids and immunosuppression

CONCLUSIONS 2 Genetics plays a key role in IPF and patients with
affected 1° relatives are eligible for 100k genome project
The Disease Modifying Anti-fibrotic Drugs pirfenidone and nintedanib slow disease progression but do not cure IPF
Serum biomarkers may play a role in monitoring disease progression or therapeutic response
Understanding specific endotypes of disease and developing appropriate therapeutics and companion biomarkers will help the majority of patients who are ineligible, intolerant or unresponsive to current therapy

THE PULMONARY FIBROSIS GROUP

Acknowledgements Nottingham Richard Hubbard Simon Johnson Alan Knox Ian Hall Ian Sayers Imperial Toby Maher Leicester Martin Tobin Louise Wain Richard Allen Queen Mary John Marshall
Edinburgh Nick Hirani Moira Whyte
William Wallace
Bristol Ann Millar Cambridge Helen Parfrey UCL Robin McAnulty Hull Simon Hart Biogen Idec Paul Wienreb
Shelia Violette GSK Richard Marshall Andy Blanchard Pauline Lukey