army medicine - amops
TRANSCRIPT

ARMY MEDICINE:
Ensuring Health, Performance, and
Trauma Care in the Soldier-Athlete
Prepared from Lessons Learned, Research and Experience
for
AMOPS
MG Philip Volpe United States Army
3 May 2013


Active/Reserve
10 / 16 Combat Spt Hosp (CSH)
16 / 22 FWD Surg Tm (FSTs)
97 / 0 Other Active Units
0 / 54 Other Army NG Units
0 /138 Other Army AR Units
123/54/176 AC/NG/AR
Deployable Units
(353 Total)
9 Medical Centers
15 Army Community Hospitals
7 Army Health Centers
10 Army Health Clinics (supporting an installation)
128 Army Health Clinics
47 Army Troop Medical Clinics
18 Army Occupational Health Clinics
147 Dental Clinics
172 Veterinary Clinics
31 Research and Development Laboratories
32 Prevention Facilities
616 Total
TDA Facilities
FY12 SRC08
EAB TOE Units
Resourcing
$13.7B DHP
26,827 Total AC Military
47,939 Civilians
7,309 Contractors
2,326 Total NG/RC Military
84,401 Total
576K Active Duty (AD)
906K Family Members (FM) (AD)
225K Dependent Survivor
152K Eligible NG/R
228K Family Members of NG/R
754K Retired
868K FM Retired
239K Other
3.95M Total
Beneficiaries AMEDD Personnel
World Wide
4,349 Medical Corps Officers
981 Dental Corps Officers
11,283 Other Officers
36,376 Enlisted
52,989 Total AC
7,309 Contractors
49,241 Civilian
50,002 Total NG/RC
159,541 Total
OTSG/MEDCOM Personnel
Army Medicine Today

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
MEDCOM Commands
EUROPE RMC
TAMC
Japan Korea
PACIFIC RMC
NORTHERN RMC
Ft. Belvoir
FSH BAMC
WBAMC
WESTERN RMC
JBLM
MAMC
Readiness
Division
Readiness
Division
CRDAMC
DDEAMC
WAMC
Readiness
Division
Readiness
Division
SOUTHERN RMC
APG
PUBLIC HEALTH COMMAND (P)
MEDICAL RESEARCH &
MATERIEL COMMAND
Ft. Detrick
WARRIOR TRANSITION COMMAND
Crystal City
AMEDDC&S
DENCOM
FSH
FSH
MEDCOM
FSH
Readiness
Division

Environment
Spiritual Psychological
MIND Behavioral Social & Family
Physical Nutritional
BODY Medical
Environment
Total Force Fitness for the 21st Century

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
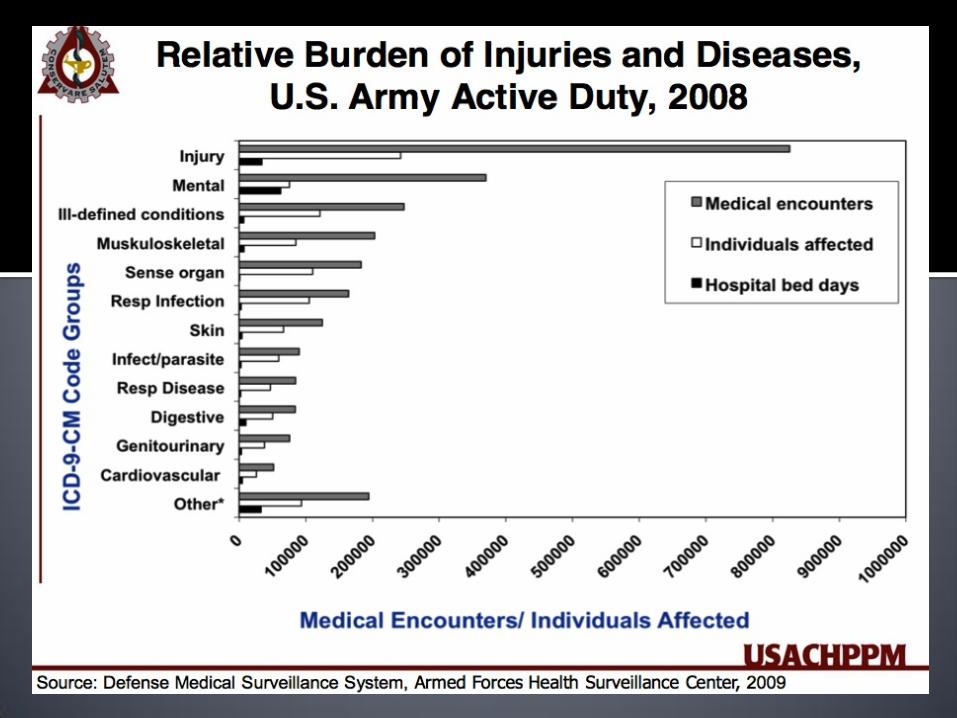
GENERAL OVERVIEW
1. Disease and Non-Battle Injuries (DNBI) are Still #1 Cause for
seeking Healthcare in Garrison and on Deployments --- not
Combat Injuries or Wounds.
2. Musculoskeletal System makes up the Vast Majority on
DNBIs.
3. Focusing Efforts on Injury Prevention, Performance
Optimization (and Resilience), and Early Intervention /
Rehabilitation has Greatest Opportunity to decrease Morbidity
and increase Military Readiness.
4. 91% Combat Survivability is the highest ever and is due to
advances in Protective Gear and Pre-Hospital Trauma Care.


Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
• Injuries from Physical Training are largest cause of morbidity & mortality in peacetime military.
•MSK Injuries cause significant morbidity during deployment.
Musculoskeletal Injuries in the Military
*Sick Call Visits? Injury = Illness
*Lost Duty Time? Injury >> Illness
*Injury with highest number of lost
duty days? *ACL Ligament Tear

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Musculoskeletal Injury and Disability
• Leading Cause of Disability in US Armed Forces:
• 22 – 63% of Disabilities.
• Mental Disabilities are 2nd (10-21%).
• 34% of ALL V.A. Disability Compensation .

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
M/S Injury & Early Discharges
• 22.1% Males
• 24.6% Females
• 81/100 Soldiers/year
• 60% unable to return to full duty
•Primarily during routine physical training
Knapik JJ et al, Discharges during U.S. Army basic training: Injury rates
and risk factors. Military Medicine; 166:641-647.
Risk of Injury in Soldiers
Tomlinson et al. Military Medicine 1987; Vol 152.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Musculoskeletal Injury Study
• 3,195 infantrymen
• 95 injuries /100 /year
• 46% running or marching
• 15.5 days light-duty
compared to only 2.1
days for illness
Smith TA, Cashman TM. The incidence of injury in light infantry soldiers.
Military Medicine 2002 Feb;167(2):104-8.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Musculoskeletal Injuries in 1 Brigade
•Average of 30% of Soldiers have:
– Undiagnosed injuries
– Incompletely evaluated injuries
– Not getting satisfactory care
Source: BCT Pre and Post-Deployment HRA II Data from SWAPP (2010)

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
CHAMP: A USUHS Initiative
CHAMP
USUHS Consortium for Health
and Military Performance
Optimizing Human Performance: the process of applying
knowledge, skills and emerging technologies to improve and
preserve the capabilities of DoD personnel to execute essential tasks.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Vision and Mission Statements
“To be the premier medical
resource in military
unique human
performance
optimization.”
“.. to promote basic, clinical and
translational research, education,
and clinical expertise in optimizing
the functional capacity of the
warfighter, with the objective of
maximizing performance in the
operational environment.”

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Improve Health and Stamina
Sleep Activity Nutrition

Military Power, Performance, & Prevention (MP3)
Mobility
Speed
Agility Power
Strength

• Performance Nutrition
– Nutrient needs
– Ideal body composition
– Supplements
• Mental Toughness
– Ideal Performance State
– Fatigue counter-measures
– Endurance events
• Functional Fitness
– Strength
– Endurance
– Movement skill
• Sports Medicine
– Prevention/early intervention
– Finishing rehab
– Multi-disciplinary team
Ranger Athlete Program

Get Healthy Ranger onto Target
Injury Prehabilitation (Fitness/Nutrition)
Daily Acute and Chronic Health Care
Immunizations/Chemoprophylaxis
Routine physical examinations
Psychological Screening
Pre-Deployment SRP
Preventive Medicine
Bring Healthy Ranger Home from Target
Injury Rehabilitation (Fitness/Nutrition)
Post-Deployment SRP
Psychological Support
Care Coalition Support
Casualty Tracking
Keep Ranger Healthy while on Target
Tactical Combat Casualty Care
Care Under Fire
Tactical Field Care
Casualty Evacuation
Healthy Ranger through Healthy Ranger Family
Liaison Efforts
Direct Care
TARGET
CONCEPT OF MISSION SUPPORT
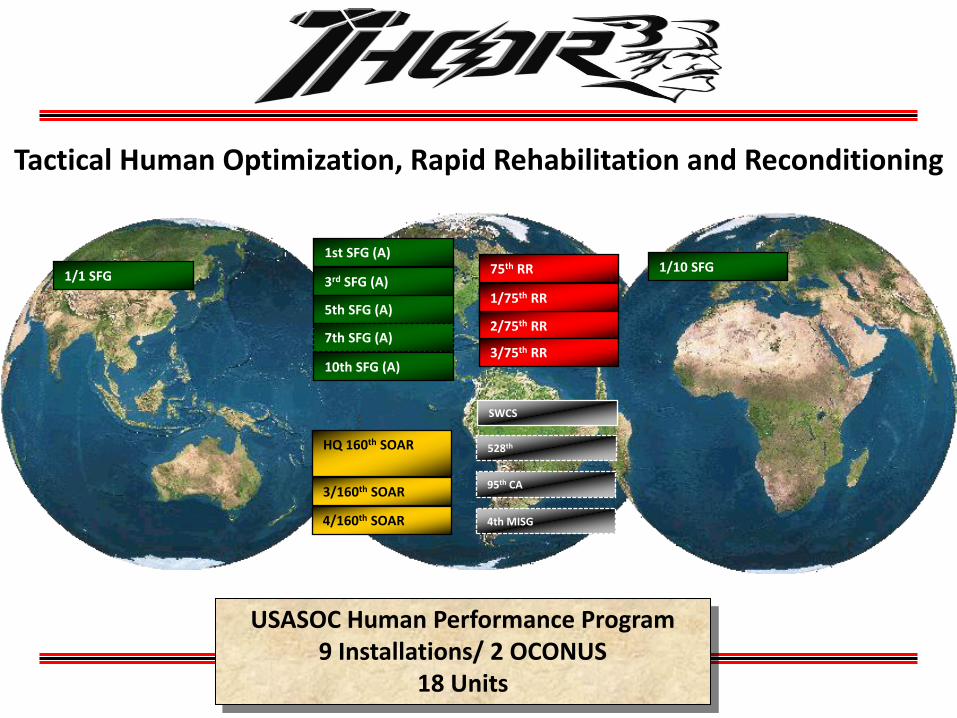
USASOC Human Performance Program 9 Installations/ 2 OCONUS
18 Units
Tactical Human Optimization, Rapid Rehabilitation and Reconditioning
1/10 SFG 1/1 SFG 3rd SFG (A)
5th SFG (A)
7th SFG (A)
10th SFG (A)
1st SFG (A) 75th RR
1/75th RR
2/75th RR
3/75th RR
HQ 160th SOAR
3/160th SOAR
4/160th SOAR
SWCS
528th
95th CA
4th MISG

Tactical Human Optimization, Rapid Rehabilitation and Reconditioning



United States Army Institute of Surgical Research Combat Casualty Care
PR
OTE CT
PR
O
JE C T
- SU S
T
AIN
T
INS
TIT
U
TEOF SURGICAL RE
SE
AR
CH

United States Army Institute of Surgical Research Combat Casualty Care
PR
OTE CT
PR
O
JE C T
- SU S
T
AIN
T
INS
TIT
U
TEOF SURGICAL RE
SE
AR
CH
Battle Injuries by Body Region
Source: JTTR September 2001 – September 2011
Face 7%
Eye 3%
Head/Neck
2%
Head/Neck
27%
Chest 5%
Abdomen 6%
Pelvis/ Urogenital 3%
Trunk/Back/Buttock
1%
Torso
15%
3%
Spine/Back
3%
Shoulder/Upper Arm
6%
Forearm/Elbow 6%
Wrist/Hand/Fingers
7%
Other 3%
Upper
Extremities
22%
Hip/Upper Leg/Thigh
5%
Foot/Toes 5%
Knee/Lower Leg/Ankle
9%
Lower
Extremities
31%
Other 12%
Other 2%
Head/Neck Unspec
3%
Brain Injury (TBI)
12%


United States Army Institute of Surgical Research Combat Casualty Care
PR
OTE CT
PR
O
JE C T
- SU S
T
AIN
T
INS
TIT
U
TEOF SURGICAL RE
SE
AR
CH
Dominant Mechanism of Injury


United States Army Institute of Surgical Research Combat Casualty Care
PR
OTE CT
PR
O
JE C T
- SU S
T
AIN
T
INS
TIT
U
TEOF SURGICAL RE
SE
AR
CH
Cause of Injury
*Includes both battle and non-battle injury


70.7 78.2 76.0
89.8 87.8 90.0
0
10
20
30
40
50
60
70
80
90
100
WW II KOREA VIETNAM OIF OND OEF
Equipment Doctrine Medical Materials Training
% S
urv
ivabili
ty
Improving casualty survivability
20% Increase in past 65 years!

TACTICAL COMBAT CASUALTY CARE, “TCCC”
Three Objectives (1) Treat the patient
(2) Prevent additional casualties
(3) Complete the mission
Three Phases of Care (1) Care under fire
(2) Tactical field care
(3) Casualty evacuation care
Butler FK, Hagmann J, Butler EG. Tactical combat casualty care in special operations. Mil Med 1996;161(Suppl.):3-16.

Hypothermia Infection Pain Documentation Evacuate to surgical capability
TCCC = Prehospital Battlefield
Trauma Care Clinical Practice Guidelines
* In 2001, CoTCCC established to review and update TCCC.

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
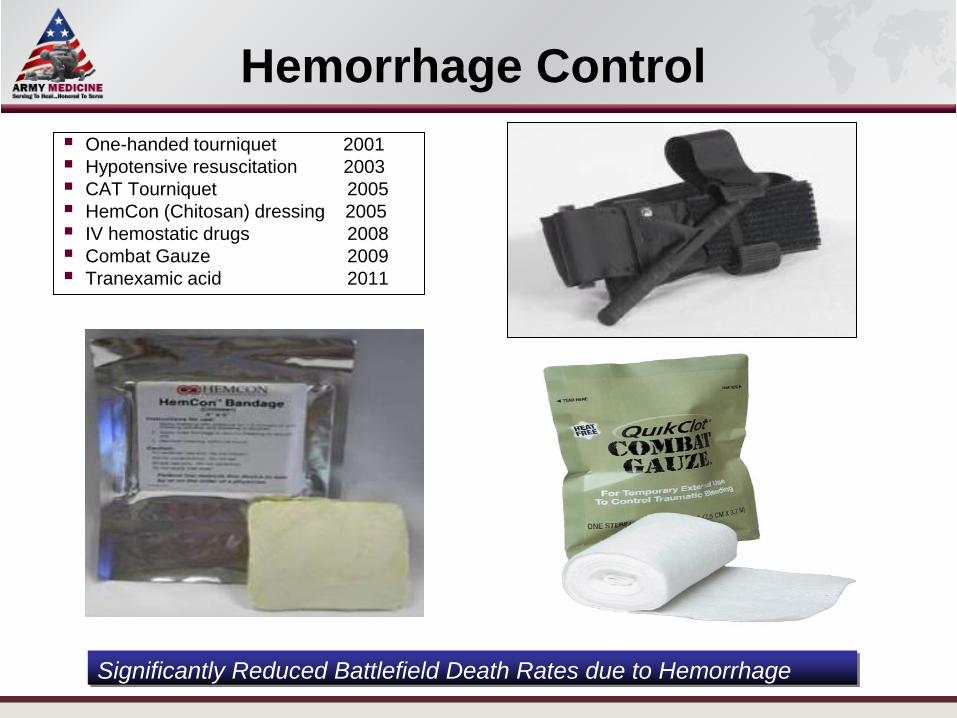
Hemorrhage Control
One-handed tourniquet 2001
Hypotensive resuscitation 2003
CAT Tourniquet 2005
HemCon (Chitosan) dressing 2005
IV hemostatic drugs 2008
Combat Gauze 2009
Tranexamic acid 2011
Significantly Reduced Battlefield Death Rates due to Hemorrhage

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Compressible Hemorrhage –
Tourniquet
•All soldiers must have a suitable tourniquet
readily available at a standard location on their
battle gear and be trained in its use.
•All troops in theater fielded the CAT
Combat Application Tourniquet (CAT) Cravat – Not changed since WWII


Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Tourniquet Studies
COL John Kragh USAISR
•Get tourniquets on BEFORE the onset of shock – Mortality is very high if casualties are already in shock before
tourniquet application
• If bleeding is not controlled and distal pulse is not
eliminated with first tourniquet – use a second one
just proximal to first – Increasing the tourniquet WIDTH with a
second tourniquet controls
bleeding more effectively
and reduces complications

United States Army Institute of Surgical Research Combat Casualty Care
PR
OTE CT
PR
O
JE C T
- SU S
T
AIN
T
INS
TIT
U
TEOF SURGICAL RE
SE
AR
CH
Can We Have An Impact? YES we can!

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
Hypothermia Prevention and
Management Kit
Dimensions: 7.5” x 9.5” x 3”
Weight: 2.5 lbs.
Part Number: 80-0027
NSN: 6515-01-532-8056
Contents:
1 x Heat Reflective Skull Cap
1 x Self Heating, Four Cell Shell Liner
1 x Heat Reflective Shell


STRATEGIC AE
BAS / CCP
ROLE 1
Definitive Care
ROLE 4 / 5
Casualty Care from the Battlefield to Home
or
CASEVAC
MEDEVAC
CSH, EMEDS,
EMF – ROLE 3
C MED / Fwd Surg Tm
ROLE 2
POINT OF INJURY SURV: 91%
RTD 97%
MEDEVAC
INTRATHEATER
MEDEVAC

Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address
“The Future of MEDEVAC is Critical Care,
Intensive Care, and Onboard Hospitalization”
This is what a Critical Care Patient looks like

Select SLIDE MASTER to Insert Briefing Title Here
2-May-13 Name/Office Symbol/(703) XXX-XXX (DSN XXX) / email address