arthroscopic management of heterotopic ossification of the subscapularis tendon in a patient with...
TRANSCRIPT

No ethical or re
*Reprint req
Department of M
Medicine, Univ
Ancona, Italy.
E-mail addre
J Shoulder Elbow Surg (2012) 21, e1-e5
1058-2746/$ - s
doi:10.1016/j.jse
www.elsevier.com/locate/ymse
CASE REPORTS
Arthroscopic management of heterotopic ossificationof the subscapularis tendon in a patient withtuberculosis: a case report
Alberto Busilacchi, MD, Carlo Bottegoni, MD, Antonio Gigante, MD*
Orthopaedic Clinic and Department of Molecular Pathology and Innovative Therapies, School of Medicine, Universit�aPolitecnica delle Marche, Ancona, Italy
Ossification of rotator cuff tendons, involving metapl-asia of soft tissue into bone, is uncommon compared withcalcifying tendonitis.1 Ossification is due to mechanicalcompression and intracellular signaling phenomena thatcontribute to a change in phenotype, giving rise to a lamellarbone structure endowed even with Haversian canals.8 Wedescribe the en bloc removal of a subscapularis tendon ossi-fication by arthroscopy in a patient with tuberculosis (TB).
Patient history
The patient, a 32-year-old Bangladeshi man who hadworkedin Italy for many years, first came to the Orthopaedic ClinicShoulderUnit inMarch 2009 for deep, anterior, sporadic painin his left shoulder. He could recall no high- or low-energytraumas involving the shoulder or swelling of its anterioraspect. The pain was not related to his occupation. It pre-vented him from sleeping pronewith his arm under the pillow(flexion and adduction of the glenohumeral joint).
The patient was being treated at the Infectious DiseasesDepartment of our university hospital for TB, contracted inhis homeland. When he came to our attention, he wasreceiving maintenance therapy.
view board approval was obtained for this case study.
uests: Antonio Gigante, MD, Orthopaedic Clinic and
olecular Pathology and Innovative Therapies, School of
ersit�a Politecnica delle Marche Via Tronto 10/A 60020,
ss: [email protected] (A. Gigante).
ee front matter � 2012 Journal of Shoulder and Elbow Surgery
.2011.05.007
Clinical preoperative examination
The subacromial impingement tests and the Patte andexternal rotation lag sign (ERLS) tests were negative;adduction and internal rotation were painful (85 on a visualanalog scale [VAS] ranging from 0 to 100) and reduced(liftoff test, þþþ; Napoleon test, þþ; O’Brien test, þþ).The patient had full abduction and flexion range of motion.
The most painful maneuver involved flexion, adduction,and maximal elevation of the fully extended arm. Motion ofthe scapulothoracic joint was normal. Pressure on the cora-coid and surrounding area elicited acute pain thatwas relievedby subcoracoid injection of bupivacaine. The calculatedConstant-Murley score3 was 68 of 100.
Imaging and differential diagnosis
Plain radiographs with anteroposterior (Fig. 1), lateral, andoutlet views and ultrasound scanning showed a pear-shapedcalcific/bony formation with a longitudinal diameter ofabout 2 cm, just under the coracoid process. On ultrasound(US), the lesion was seen to be inside the subscapularistendon. A magnetic resonance scan was performed to gaugethe lesion’s volume more accurately; its signal intensity onT1- and T2-weighted sequences, very similar to bone(Fig. 2), ruled out hypotheses of either a calcification or anunusual caseating granuloma containing active mycobacte-rium inside calcified tissue.
Review of previous chest and shoulder radiographs andcomputed tomography follow-up scans did depict the
Board of Trustees.
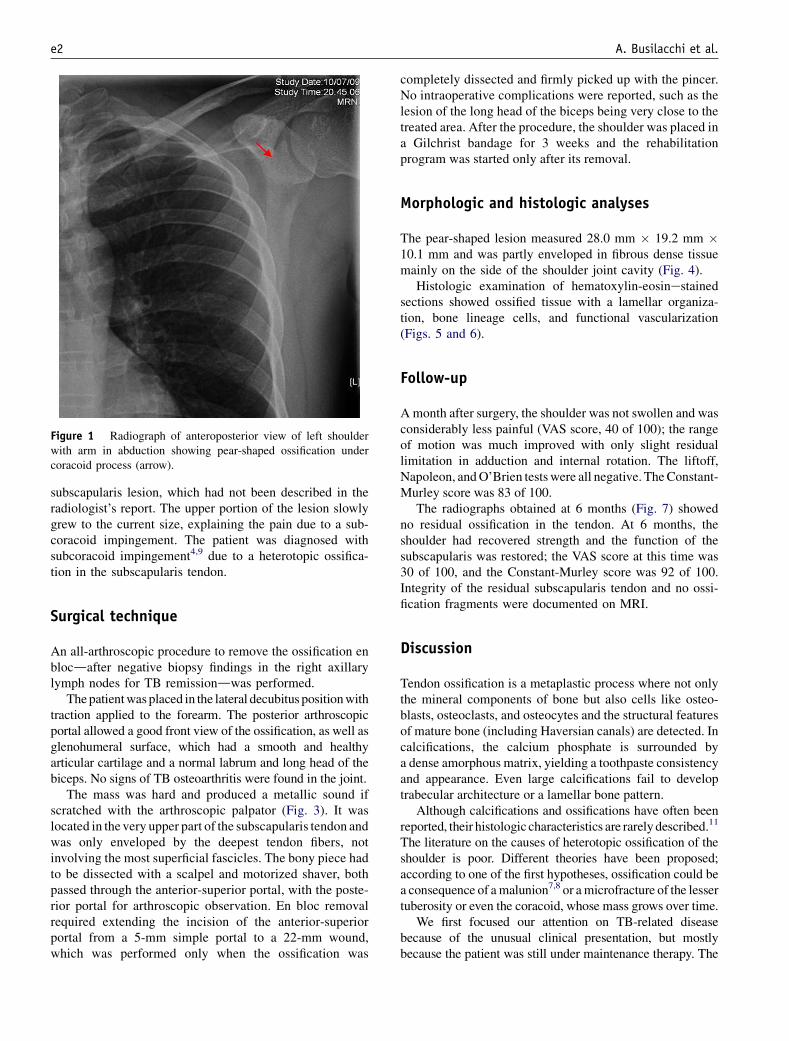
Figure 1 Radiograph of anteroposterior view of left shoulderwith arm in abduction showing pear-shaped ossification undercoracoid process (arrow).
e2 A. Busilacchi et al.
subscapularis lesion, which had not been described in theradiologist’s report. The upper portion of the lesion slowlygrew to the current size, explaining the pain due to a sub-coracoid impingement. The patient was diagnosed withsubcoracoid impingement4,9 due to a heterotopic ossifica-tion in the subscapularis tendon.
Surgical technique
An all-arthroscopic procedure to remove the ossification enblocdafter negative biopsy findings in the right axillarylymph nodes for TB remissiondwas performed.
Thepatientwas placed in the lateral decubitus positionwithtraction applied to the forearm. The posterior arthroscopicportal allowed a good front view of the ossification, as well asglenohumeral surface, which had a smooth and healthyarticular cartilage and a normal labrum and long head of thebiceps. No signs of TB osteoarthritis were found in the joint.
The mass was hard and produced a metallic sound ifscratched with the arthroscopic palpator (Fig. 3). It waslocated in the very upper part of the subscapularis tendon andwas only enveloped by the deepest tendon fibers, notinvolving the most superficial fascicles. The bony piece hadto be dissected with a scalpel and motorized shaver, bothpassed through the anterior-superior portal, with the poste-rior portal for arthroscopic observation. En bloc removalrequired extending the incision of the anterior-superiorportal from a 5-mm simple portal to a 22-mm wound,which was performed only when the ossification was
completely dissected and firmly picked up with the pincer.No intraoperative complications were reported, such as thelesion of the long head of the biceps being very close to thetreated area. After the procedure, the shoulder was placed ina Gilchrist bandage for 3 weeks and the rehabilitationprogram was started only after its removal.
Morphologic and histologic analyses
The pear-shaped lesion measured 28.0 mm � 19.2 mm �10.1 mm and was partly enveloped in fibrous dense tissuemainly on the side of the shoulder joint cavity (Fig. 4).
Histologic examination of hematoxylin-eosinestainedsections showed ossified tissue with a lamellar organiza-tion, bone lineage cells, and functional vascularization(Figs. 5 and 6).
Follow-up
Amonth after surgery, the shoulder was not swollen and wasconsiderably less painful (VAS score, 40 of 100); the rangeof motion was much improved with only slight residuallimitation in adduction and internal rotation. The liftoff,Napoleon, andO’Brien testswere all negative. TheConstant-Murley score was 83 of 100.
The radiographs obtained at 6 months (Fig. 7) showedno residual ossification in the tendon. At 6 months, theshoulder had recovered strength and the function of thesubscapularis was restored; the VAS score at this time was30 of 100, and the Constant-Murley score was 92 of 100.Integrity of the residual subscapularis tendon and no ossi-fication fragments were documented on MRI.
Discussion
Tendon ossification is a metaplastic process where not onlythe mineral components of bone but also cells like osteo-blasts, osteoclasts, and osteocytes and the structural featuresof mature bone (including Haversian canals) are detected. Incalcifications, the calcium phosphate is surrounded bya dense amorphous matrix, yielding a toothpaste consistencyand appearance. Even large calcifications fail to developtrabecular architecture or a lamellar bone pattern.
Although calcifications and ossifications have often beenreported, their histologic characteristics are rarely described.11
The literature on the causes of heterotopic ossification of theshoulder is poor. Different theories have been proposed;according to one of the first hypotheses, ossification could bea consequence of amalunion7,8 or amicrofracture of the lessertuberosity or even the coracoid, whose mass grows over time.
We first focused our attention on TB-related diseasebecause of the unusual clinical presentation, but mostlybecause the patient was still under maintenance therapy. The

Figure 2 T1- and T2-weighted MRI scans showing shape of ossification and its inclusion (arrows) in subscapularis tendon.
Figure 3 Arthroscopic image showing dissection of ossification(arrow) from fibers of subscapularis tendon.
Figure 4 Gross evaluation showing that the lesion had a bonystructure partially enveloped in fibrous tissue.
Arthroscopic management of subscapularis ossification e3
arthroscopic removal, which seems to be a simple procedure,was delayed to complete the diagnostic process and mostly toconfirm the noninfectious/noncontagious origin of the mass.An infectious origin of the lesion was excluded also bya review of the literature, which highlighted that TB mayinduce no more than modest calcifications in the subdeltoid
bursa.6,11 The hypothesis of a side effect of the antibiotictherapy was not supported by the literature.

Figure 5 Section on light microscopy showing lamellar bonystructure, bone cells, and Haversian systems. (hematoxylin-eosinstain, original magnification �40).
Figure 6 Detail at light microscopy showing the tidemarkbetween the haversian bone and the envelope of the lesion. (ie,interface between bone and fibrous tissue) (hematoxylin-eosinstain, original magnification X10).
Figure 7 Six months after surgery, a radiograph of the treatedshoulder shows no residual ossification or relapses.
e4 A. Busilacchi et al.
Some authors support that the long-term evolution ofosteochondritis can form a separate bone, like the ossic-ulum in Osgood-Schlatter disease. Uhthoff et al13 believedthat the ossification may be an evolution of a previouscalcification that had developed a blood supply. Later,Uhthoff and Loehr12 reported that decreased tissue hypoxiamay lead to metaplasia from tendon to fibrocartilage andfrom fibrocartilage to a bony structure. The last hypothesisis that an ossification may simply be an accessory bone.
A similar lesion but with multiple ossifications of thesubscapularis tendon, causing a form of subcoracoidimpingement, was first described by Peidro et al,10 who alsoreported its histologic characteristics. The lesion in this case
was close to the bone-tendon junction and was removed byopen surgery through a deltopectoral approach.
Given the absence of chondral areas in the subscapularisossification, which are usually related to chronic compr-ession and friction, as in rotator cuff pathology, we areinclined to view this ossification as a sort of accessory bonewith a different growth rhythm compared with the otherstructures of the shoulder. Two articles describing sub-coracoid impingement due to calcifications arthroscopi-cally treated by previous authors prompted us to opt for anall-arthroscopic technique.2,5 To our knowledge, this is thefirst report of an en bloc arthroscopic removal, whichshowed the benefits of a minimally invasive technique andavoided the possible complications of open surgery.
Conclusion
Ossification of the subscapularis tendon is a rare cause ofsubcoracoid impingement that should be considered duringphysical examination. A careful arthroscopic excisionallows, as well as the open technique, its complete removaland provides durable pain relief. Given its unclear origin,histologic examination after removal would provide usefulinformation to differentiate its bony structure froma simplecalcification and to understand its prevalence.
Disclaimer
The authors, their immediate families, and any researchfoundations with which they are affiliated have not

Arthroscopic management of subscapularis ossification e5
received any financial payments or other benefits fromany commercial entity related to the subject of thisarticle.
References
1. Archer RS, Bayley JI, Archer CW, Ali SY. Cell and matrix changes
associated with pathological calcification of the human rotator cuff
tendons. J Anat 1993;182(Pt 1):1-11.
2. Arrigoni P, Brady PC, Burkhart SS. Calcific tendonitis of the sub-
scapularis tendon causing subcoracoid stenosis and coracoid impin-
gement. Arthroscopy 2006;22:1139.e1-3. doi:10.1016/j.arthro.2005.
06.028
3. Constant CR, Murley AH. A clinical method of functional assessment
of the shoulder. Clin Orthop Relat Res 1987:160-4.
4. Dines DM, Warren RF, Inglis AE, Pavlov H. The coracoid impinge-
ment syndrome. J Bone Joint Surg Br 1990;72:314-6.
5. Franceschi F, Longo UG, Ruzzini L, Rizzello G, Denaro V. Arthro-
scopic management of calcific tendinitis of the subscapularis tendon.
Knee Surg Sports Traumatol Arthrosc 2007;15:1482-5. doi:10.1007/
s00167-007-0340-x
6. Kenin A. Tuberculosis of the subdeltoid bursa. Bull Hosp Joint Dis
1950;11:128-33.
7. Kowalsky MS, Bell JE, Ahmad CS. Arthroscopic treatment of
subcoracoid impingement caused by lesser tuberosity malunion: a case
report and review of the literature. J Shoulder Elbow Surg 2007;16:
e10-4. doi:10.1016/j.jse.2006.09.018
8. Ozaki J, Kugai A, Tomita Y, Tamai S. Tear of an ossified rotator cuff
of the shoulder. A case report. Acta Orthop Scand 1992;63:339-40.
9. PatteD. The subcoracoid impingement. ClinOrthopRelat Res 1990:55-9.
10. Peidro L, Serra A, Suso S. Subcoracoid impingement after ossification
of the subscapularis tendon. J Shoulder Elbow Surg 1999;8:170-1.
11. Sharma SV, Varma BP, Khanna S. Dystrophic calcification in tuber-
cular lesions of bursae. Acta Orthop Scand 1978;49:445-7.
12. Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff:
pathogenesis, diagnosis, and management. J Am Acad Orthop Surg
1997;5:183-91.
13. Uhthoff HK, Sarkar K, Maynard JA. Calcifying tendinitis: a new
concept of its pathogenesis. Clin Orthop Relat Res 1976:164-8.