atlas of anatomic thology a p - download.e-bookshelf.de
TRANSCRIPT
Atlas of Bone Pathology
123
Shi WeiGene P. Siegal

Atlas of Anatomic Pathology
Series EditorLiang Cheng
Available VolumesAtlas of Spleen Pathology, Atlas of Genitourinary Pathology
Upcoming VolumesAtlas of Medical Renal Pathology

Shi Wei • Gene P. Siegal
Atlas of Bone Pathology

ISBN 978-1-4614-6326-9 ISBN 978-1-4614-6327-6 (eBook) DOI 10.1007/978-1-4614-6327-6 Springer New York Heidelberg Dordrecht London
Library of Congress Control Number: 2013933857
© Springer Science+Business Media New York 2013 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, speci fi cally the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on micro fi lms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. Exempted from this legal reservation are brief excerpts in connection with reviews or scholarly analysis or material supplied speci fi cally for the purpose of being entered and executed on a computer system, for exclusive use by the purchaser of the work. Duplication of this publication or parts thereof is permitted only under the provisions of the Copyright Law of the Publisher’s location, in its current version, and permission for use must always be obtained from Springer. Permissions for use may be obtained through RightsLink at the Copyright Clearance Center. Violations are liable to prosecution under the respective Copyright Law. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a speci fi c statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. While the advice and information in this book are believed to be true and accurate at the date of publication, neither the authors nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with respect to the material contained herein.
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)
Shi Wei, MD, PhD Assistant Professor of Pathology University of Alabama at Birmingham Medical Director, Immunohistochemistry Laboratory UAB Hospital Birmingham , AL USA
Gene P. Siegal, MD, PhD R.W. Mowry Endowed Professor of Pathology Director, Division of Anatomic Pathology Executive Vice-Chair - Pathology, UAB Health System Department of Pathology University of Alabama at Birmingham Birmingham , ALUSA

This book is dedicated to all those who have taught us and continue to teach us each day: our teachers, our colleagues, and our students—our parents, our children, and our spouses—it’s time to pass the knowledge forward!
Shi Wei Gene Siegal

vii
Series Preface
One Picture Is Worth Ten Thousand Words – Frederick Barnard, 1927
Remarkable progress has been made in anatomic and surgical pathology during the last 10 years. The ability of surgical pathologists to reach a de fi nite diagnosis is now enhanced by immunohistochemical and molecular techniques. Many new clinically important histopatho-logic entities and variants have been described using these techniques. Established diagnostic entities are more fully de fi ned for virtually every organ system. The emergence of personalized medicine has also created a paradigm shift in surgical pathology. Both promptness and preci-sion are required of modern pathologists. Newer diagnostic tests in anatomic pathology, how-ever, cannot bene fi t the patient unless the pathologist recognizes the lesion and requests the necessary special studies. An up-to-date Atlas encompassing the full spectrum of benign and malignant lesions, their variants, and evidence-based diagnostic criteria for each organ system is needed. This Atlas is not intended as a comprehensive source of detailed clinical information concerning the entities shown. Clinical and therapeutic guidelines are served admirably by a large number of excellent textbooks. This Atlas, however, is intended as a “ fi rst knowledge base” in the quest for de fi nitive and ef fi cient diagnosis of both usual and unusual diseases.
The Atlas of Anatomic Pathology is presented to the reader as a quick reference guide for diagnosis and classi fi cation of benign, congenital, in fl ammatory, nonneoplastic, and neoplastic lesions organized by organ systems. Normal and variations of “normal” histology are illus-trated for each organ. The Atlas focuses on visual diagnostic criteria and differential diagnosis. The organization is intended to provide quick access to images and con fi rmatory tests for each speci fi c organ or site. The Atlas adopts the well-known and widely accepted terminology, nomenclature, classi fi cation schemes, and staging algorithms.
This book Series is intended chie fl y for use by pathologists in training and practicing surgi-cal pathologists in their daily practice. It is also a useful resource for medical students, cyto-technologists, pathologist assistants, and other medical professionals with special interest in anatomic pathology. We hope that our trainees, students, and readers at all levels of expertise will learn, understand, and gain insight into the pathophysiology of disease processes through this comprehensive resource. Macroscopic and histological images are aesthetically pleasing in many ways. We hope that the new Series will serve as a virtual pathology museum for the edi fi cation of our readers.
Liang Cheng, MD , Series Editor


ix
Preface
Now that this monograph has been “put to bed,” we thank the series editor, Dr. Liang Cheng, for providing us this opportunity to add to this exciting series of atlases focused on the modern classi fi cation of pathologic conditions by organ type. We had been able to turn aside multiple other competing requests, but his charm and reputation for high-quality publications swayed us to undertake this challenge, and in the end we are glad that we did deliver the product before you. We were also inclined to undertake this project because of the positive experience we had with the publisher, Springer, who graciously published our Bone volume for the Frozen Section Library series in 2011. We now see these two texts as companion works, one for the other.
Attempting to remain true to the spirit of this series, this book does not attempt to be ency-clopedic, as many fi ne such books already exist by us and others, and we try to acknowledge many of them in the Suggested Reading section. Rather, we have sought to highlight, with high-quality images, the histopathologic features of the many conditions of bone, emphasizing the neoplastic ones. Where appropriate, we have supplemented these images with clinical and gross pathology photographs. As radiologic evaluation is critical in virtually every facet of bone pathology diagnosis, we also have included representative conventional radiographs as well as CT and MRI images. For completeness, immunophenotyping of key entities also has been included along with a reference to advances in cytogenetics and molecular genetics in the purposely truncated text.
As a “quick reference guide,” this book is organized along classic lines in some one dozen chapters. Although we have had the opportunity to publish many papers in the peer-reviewed literature, we have made a special effort to provide never-before-seen images that we hope will be aesthetically pleasing but, more importantly, highly informative. In cases in which previ-ously published images were needed, permission was obtained from the publishers, and we thank them collectively. As with the Atlas of Genitourinary Pathology , most of the entities will be familiar to the seasoned pathologist, but we hope that everyone, be they wizened masters or young novices, will see one or more bits of exotica that they can add to their mental libraries for future use to bene fi t their patients.
Birmingham, AL Shi Wei Birmingham, AL Gene P. Siegal


xi
Acknowledgments
As the authors, we greatly acknowledge the contributions of our many colleagues who gave graciously of their intellectual capital to assure the successful completion of this book. We wish to personally acknowledge the following physicians, who provided source material from their personal collections and allowed this material to be published:
Dr. Michael J. Pitt, Emeritus Professor of Radiology, University of Alabama at Birmingham (UAB)
Dr. Philip H. Lander, Professor of Radiology, UAB Dr. Ona Faye-Petersen, Professor of Pathology, UAB Dr. Michael J. Klein, Pathologist in Chief, Hospital for Special Surgery, and Professor of
Pathology, Weill Medical College of Cornell University Dr. Brian Rubin, Cleveland Clinic Dr. Patricia DeVilliers, Assistant Professor of Oral Pathology, UAB Dr. Kristopher McKay, Assistant Professor of Dermatology and Pathology, UAB Dr. Keith Harrison, Children’s Hospital of Alabama We also acknowledge with gratitude the critical support of Mr. Erik (Scott) Young, Ms.
Patricia F. Lott, Dr. Dezhi (Annie) Wang, and Ms. Cassandra (Sandy) B. Cummings.

xiii
Contents
1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.1 Normal Bone Histology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21.2 Callus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 111.3 Chest Wall Hamartoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 161.4 Chondroid Hamartoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
2 Bone-Forming Tumors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 232.1 Osteoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242.2 Osteoid Osteoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262.3 Osteoblastoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292.4 Conventional Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 382.5 Telangietatic Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 672.6 Small Cell Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 712.7 Low-Grade Central Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 782.8 Parosteal Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 812.9 Periosteal Osteosarcoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 892.10 High-Grade Surface Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 932.11 Secondary Osteosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97
3 Cartilage-Forming Tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1013.1 Osteochondroma (Exostosis) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1023.2 Chondroma (Enchondroma) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1093.3 Periosteal Chondroma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1153.4 Enchondromatosis (Including Ollier Disease and Maffucci Syndrome) . . 1173.5 Chondroblastoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1223.6 Chondromyxoid Fibroma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1273.7 Synovial Chondromatosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1323.8 Conventional Chondrosarcoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1343.9 Secondary Chondrosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1443.10 Dedifferentiated Chondrosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1463.11 Clear Cell Chondrosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1503.12 Mesenchymal Chondrosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 152
4 Fibrous and Fibrohistiocytic Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1574.1 Nonossifying Fibroma
(Metaphyseal Fibrous Defect, Fibrous Cortical Defect). . . . . . . . . . . . . . . 1584.2 Benign Fibrous Histiocytoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1634.3 Desmoplastic Fibroma (Desmoid Tumor) . . . . . . . . . . . . . . . . . . . . . . . . . 1674.4 Fibroma of Tendon Sheath . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1694.5 Fibrosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1714.6 Malignant Fibrous Histiocytoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175

xiv Contents
5 Fibro-osseous Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1795.1 Fibrous Dysplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1805.2 Osteo fi brous Dysplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1935.3 Central Ossifying Fibroma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1965.4 Liposclerosing Myxofibrous Tumor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203
6 Giant Cell–Rich Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2076.1 Giant Cell Tumor of Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2086.2 Giant Cell Reparative Granuloma of Gnathic Bones . . . . . . . . . . . . . . . . . 2166.3 Malignant Giant Cell Tumor. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2186.4 Tenosynovial Giant Cell Tumor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2226.5 Hyperparathyroidism (Brown Tumor) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2286.6 Cherubism. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235
7 Small, Round Cell Lesions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2377.1 Benign, Reactive, Inflammatory . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
7.1.1 Osteomyelitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2387.1.2 Langerhans Cell Histiocytosis (Histiocytosis X, Eosinophilic Granuloma). . . . . . . . . . . . . . . . . . . 2467.1.3 Mastocytosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2517.1.4 Sinus Histiocytosis with Massive Lymphadenopathy
(Rosai-Dorfman Disease) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2537.1.5 Sarcoidosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2577.1.6 Xanthoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 258
7.2 Malignant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2597.2.1 Lymphoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2597.2.2 Plasmacytoma/Plasma Cell Myeloma . . . . . . . . . . . . . . . . . . . . . . . 2667.2.3 Ewing Sarcoma/Primitive Neuroectodermal Tumor (PNET) . . . . . 274
8 Cysts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2838.1 Aneurysmal Bone Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2848.2 Unicameral Bone Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2958.3 Ganglion Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 298
9 Vascular Tumors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3019.1 Hemangioma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3029.2 Hemangioendothelioma and Epithelioid Hemangioendothelioma. . . . . . . 3059.3 Hemangiopericytoma/Solitary Fibrous Tumor . . . . . . . . . . . . . . . . . . . . . . 3129.4 Angiosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 314
10 Myogenic, Lipogenic, Neural, and Other Mesenchymal Tumors . . . . . . . . . . . 32110.1 Leiomyoma of Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32210.2 Leiomyosarcoma of Bone. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32310.3 Rhabdomyosarcoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32610.4 Lipoma of Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33110.5 Myxoma of Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33210.6 Paraganglioma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33310.7 Neurilemmoma/Schwannoma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33410.8 Malignant Peripheral Nerve Sheath Tumor . . . . . . . . . . . . . . . . . . . . . . . . 33810.9 Ependymoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34010.10 Adamantinoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34210.11 Ameloblastoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34910.12 Chordoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35310.13 Synovial Sarcoma of Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364
xvContents
11 Tumor-like Conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37311.1 Avascular Necrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37411.2 Bone Infarct . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37911.3 Osteochondral Body . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38111.4 Gout . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38311.5 Calcium Pyrophosphate Dihydrate Disease . . . . . . . . . . . . . . . . . . . . . . . . 38711.6 Bizarre Parosteal Osteochondromatous Proliferation. . . . . . . . . . . . . . . . . 39111.7 Subungual Exostosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39711.8 Myositis Ossificans. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 399
12 Reactive, Metabolic, and Developmental Conditions . . . . . . . . . . . . . . . . . . . . . 40512.1 Osteoarthritis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40612.2 Rheumatoid Arthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41212.3 Detritic Synovitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41512.4 Gaucher Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41812.5 Osteogenesis Imperfecta. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42012.6 Osteomalacia/Rickets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42512.7 Osteopenia/Osteoporosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42612.8 Osteopetrosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42812.9 Paget Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42912.10 Phosphaturic Mesenchymal Tumor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 434
13 Metastases to and from Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44113.1 Metastases to Bone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44213.2 Metastases from Bone. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 463
Suggested Reading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 467
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 469

1S. Wei, G.P. Siegal, Atlas of Bone Pathology, Atlas of Anatomic Pathology,DOI 10.1007/978-1-4614-6327-6_1, © Springer Science+Business Media New York 2013
Human skeletons can be classi fi ed based on their position, shape, and structure (Table 1.1 ). In long bones, the epiphysis is the section between the expanded end of bone and its growth plate (also known as the physis or epiphyseal plate). The physis disappears by 20 years of age. The epiphysis con-sists of a hyaline cartilage joint surface, compact exterior (cortex), and spongy interior (medulla), and it is the region of secondary ossi fi cation. The diaphysis is the central shaft of the long bone with compact bone surrounding marrow cav-ity, and it is the region of primary ossi fi cation. The metaphy-sis is the junctional portion lying between the growth plate and the diaphysis. Cartilage is composed of chondrocytes embedded in a prominent ground substance of extracellular matrix, which is made of proteoglycan aggregates in hyaluronic acid. The varying proportions of collagen types and elastic fi bers embedded within the ground substance give rise to three types of cartilage: hyaline cartilage, fi brocartilage, and elastic cartilage (Table 1.2 ).
Introduction 1
Basis of classi fi cation Type of bone Examples/locations
Region Axial skeleton Skull, vertebral column, sternum, and ribs
Appendicular skeleton Limbs and girdles of limbs
Shape Long bone Limb bones such as humerus
Short bone Wrist and ankle bones such as cuboid
Flat bone Skull, sternum, scapula, and pelvis
Irregular bone Vertebrae, acetabulum, and base of skull
Sesamoid bone (bone embedded in a tendon)
Patella
Structure Compact bone Cortex Cancellous bone/trabecular bone
Medulla
Table 1.1 Classi fi cation of human skeletons
Table 1.2 Classi fi cation of cartilage
Type Examples/locations
Hyaline cartilage Large bone joints (hip, elbow, knee) Fibrocartilage Intervertebral disks, pubic
symphysis, meniscus, and temporomandibular joints
Elastic cartilage External ear, larynx, and epiglottis
2 1 Introduction
1.1 Normal Bone Histology
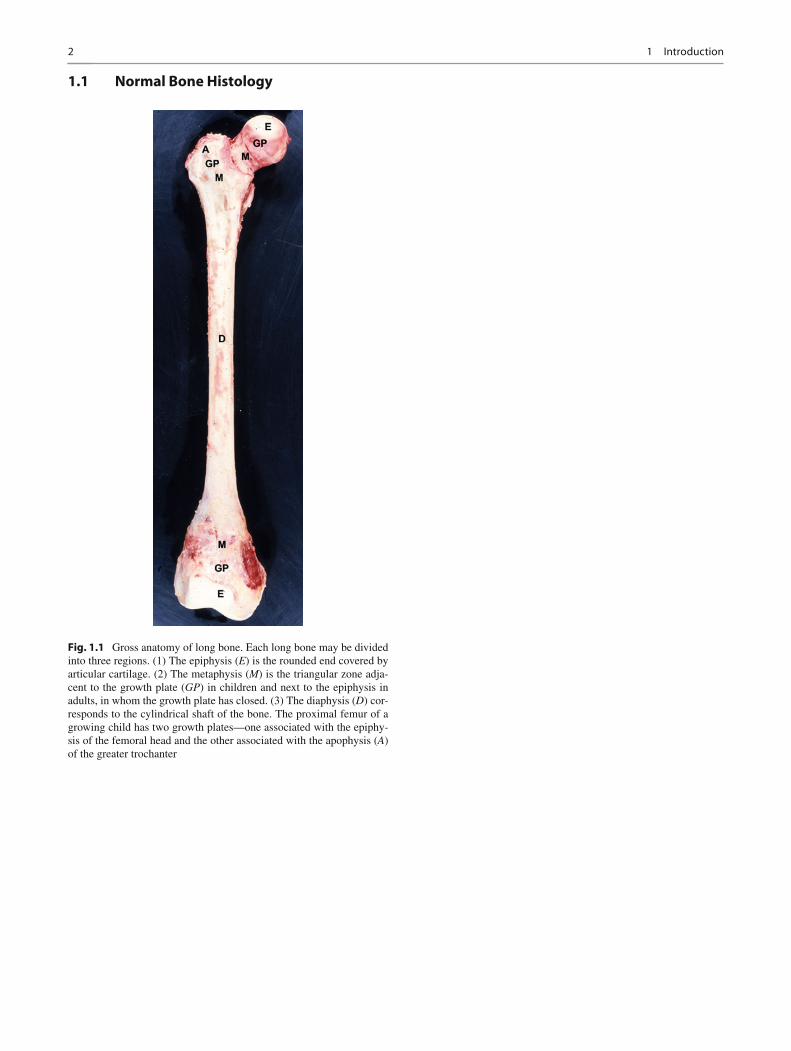
Fig. 1.1 Gross anatomy of long bone. Each long bone may be divided into three regions. (1) The epiphysis ( E ) is the rounded end covered by articular cartilage. (2) The metaphysis ( M ) is the triangular zone adja-cent to the growth plate ( GP ) in children and next to the epiphysis in adults, in whom the growth plate has closed. (3) The diaphysis ( D ) cor-responds to the cylindrical shaft of the bone. The proximal femur of a growing child has two growth plates—one associated with the epiphy-sis of the femoral head and the other associated with the apophysis ( A ) of the greater trochanter

31.1 Normal Bone Histology
Fig. 1.2 Lamellar bone. This type of bone is the dominant form in adults; it is organized in layers (lamellae), either concentrically arranged (e.g., compact bone, as illustrated in this image) or in parallel (cancel-lous bone). The inorganic composition (mineral) of bone is principally derived from crystallized hydroxyapatite (Ca
10 [PO
4 ]
6 [OH]
2 ). The organic
portion of bone (matrix) is composed mainly of type I collagen. The compact bone is of intramembranous origin and constitutes 90 % bone
and 10 % space by volume. The osteocytes situated in the lacunae are terminally differentiated bone cells originating from osteoblasts. They communicate with their neighboring cells and contact them via an intri-cate cell process network called canaliculi. The osteon (also known as the haversian system), the fundamental functional unit of compact bone, consists of concentric layers (lamellae) that surround a central canal (the haversian canal), which contains the nerve and blood supplies
Fig. 1.3 Lamellar bone. Polarized microscopy of the section shown in Fig. 1.2 . The concentric lamellae are more easily recognized in polarized light
4 1 Introduction
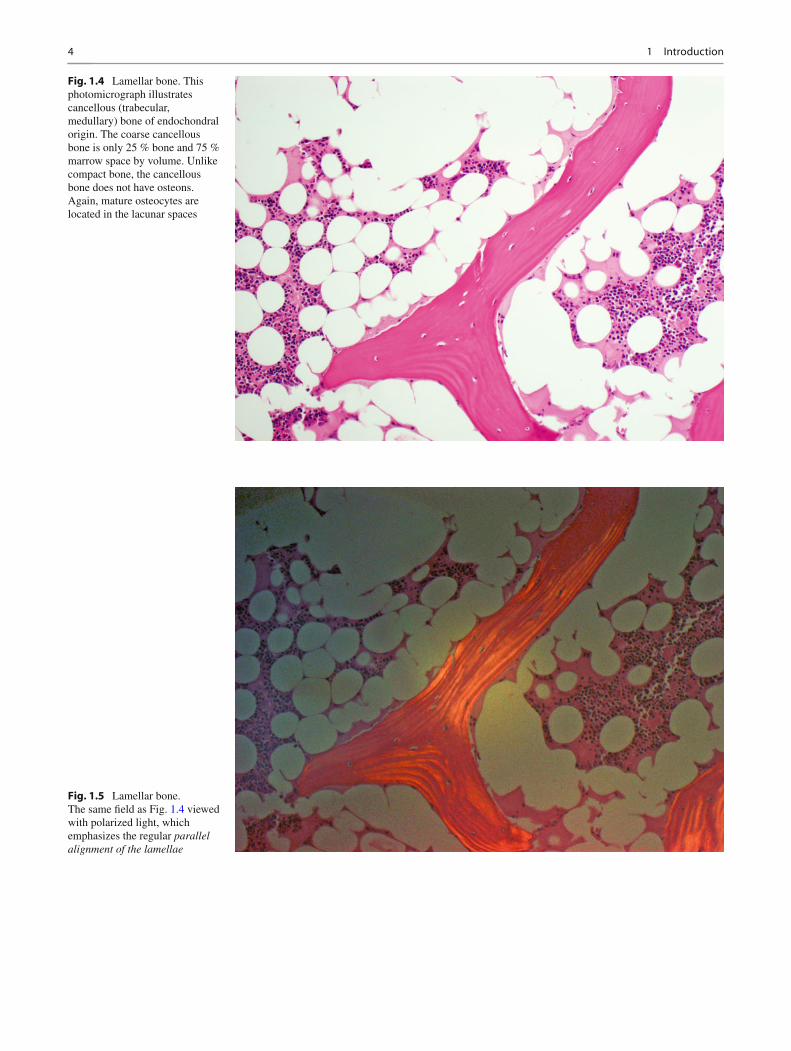
Fig. 1.4 Lamellar bone. This photomicrograph illustrates cancellous (trabecular, medullary) bone of endochondral origin. The coarse cancellous bone is only 25 % bone and 75 % marrow space by volume. Unlike compact bone, the cancellous bone does not have osteons. Again, mature osteocytes are located in the lacunar spaces
Fig. 1.5 Lamellar bone. The same fi eld as Fig. 1.4 viewed with polarized light, which emphasizes the regular parallel alignment of the lamellae
51.1 Normal Bone Histology
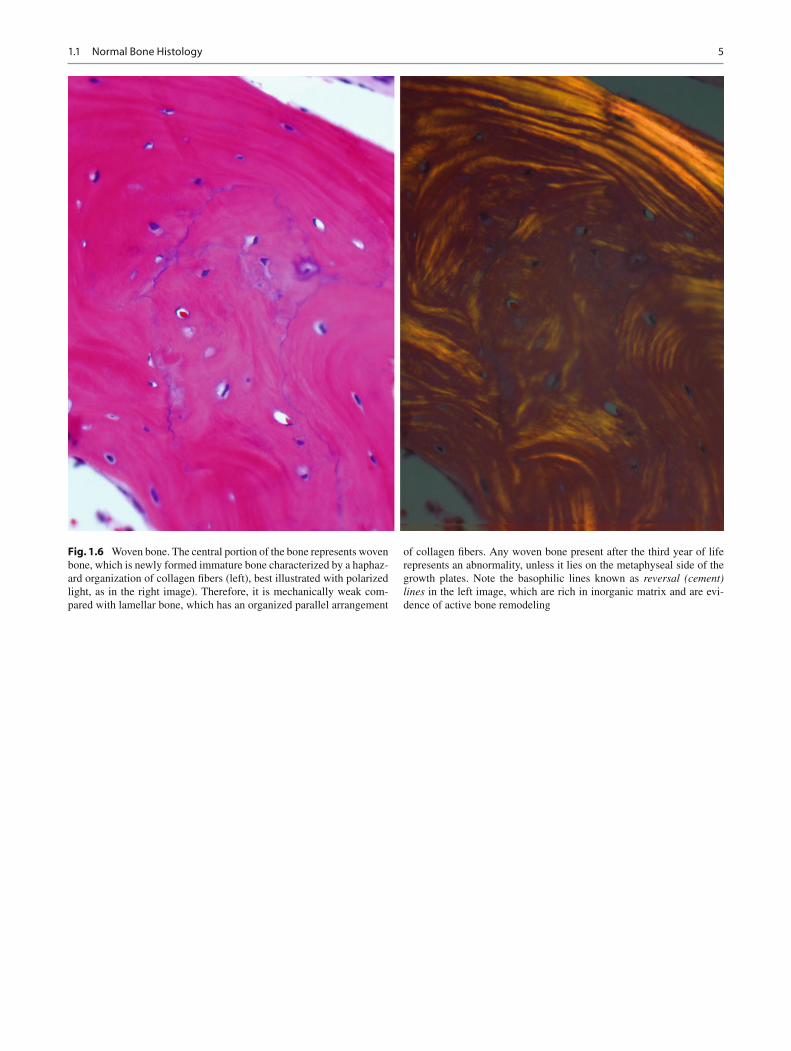
Fig. 1.6 Woven bone. The central portion of the bone represents woven bone, which is newly formed immature bone characterized by a haphaz-ard organization of collagen fi bers (left), best illustrated with polarized light, as in the right image). Therefore, it is mechanically weak com-pared with lamellar bone, which has an organized parallel arrangement
of collagen fi bers. Any woven bone present after the third year of life represents an abnormality, unless it lies on the metaphyseal side of the growth plates. Note the basophilic lines known as reversal (cement) lines in the left image, which are rich in inorganic matrix and are evi-dence of active bone remodeling
6 1 Introduction
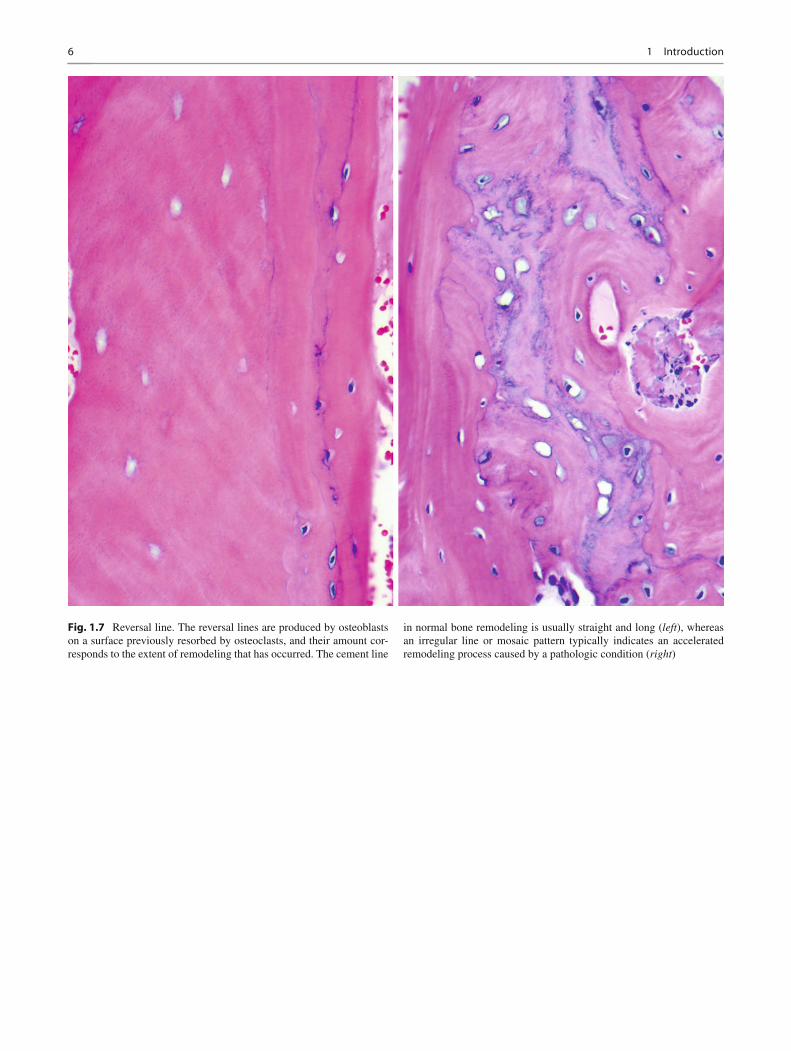
Fig. 1.7 Reversal line. The reversal lines are produced by osteoblasts on a surface previously resorbed by osteoclasts, and their amount cor-responds to the extent of remodeling that has occurred. The cement line
in normal bone remodeling is usually straight and long ( left ), whereas an irregular line or mosaic pattern typically indicates an accelerated remodeling process caused by a pathologic condition ( right )
71.1 Normal Bone Histology
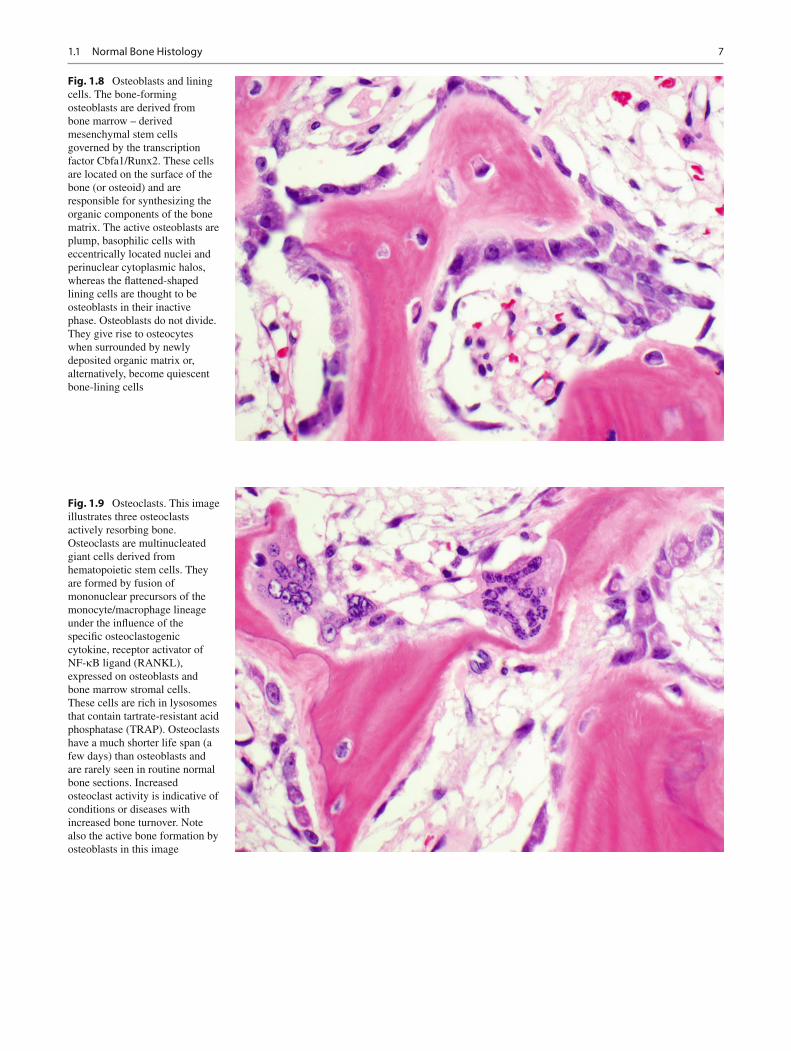
Fig. 1.8 Osteoblasts and lining cells. The bone-forming osteoblasts are derived from bone marrow – derived mesenchymal stem cells governed by the transcription factor Cbfa1/Runx2. These cells are located on the surface of the bone (or osteoid) and are responsible for synthesizing the organic components of the bone matrix. The active osteoblasts are plump, basophilic cells with eccentrically located nuclei and perinuclear cytoplasmic halos, whereas the fl attened-shaped lining cells are thought to be osteoblasts in their inactive phase. Osteoblasts do not divide. They give rise to osteocytes when surrounded by newly deposited organic matrix or, alternatively, become quiescent bone-lining cells
Fig. 1.9 Osteoclasts. This image illustrates three osteoclasts actively resorbing bone. Osteoclasts are multinucleated giant cells derived from hematopoietic stem cells. They are formed by fusion of mononuclear precursors of the monocyte/macrophage lineage under the in fl uence of the speci fi c osteoclastogenic cytokine, receptor activator of NF- k B ligand (RANKL), expressed on osteoblasts and bone marrow stromal cells. These cells are rich in lysosomes that contain tartrate-resistant acid phosphatase (TRAP). Osteoclasts have a much shorter life span (a few days) than osteoblasts and are rarely seen in routine normal bone sections. Increased osteoclast activity is indicative of conditions or diseases with increased bone turnover. Note also the active bone formation by osteoblasts in this image
8 1 Introduction
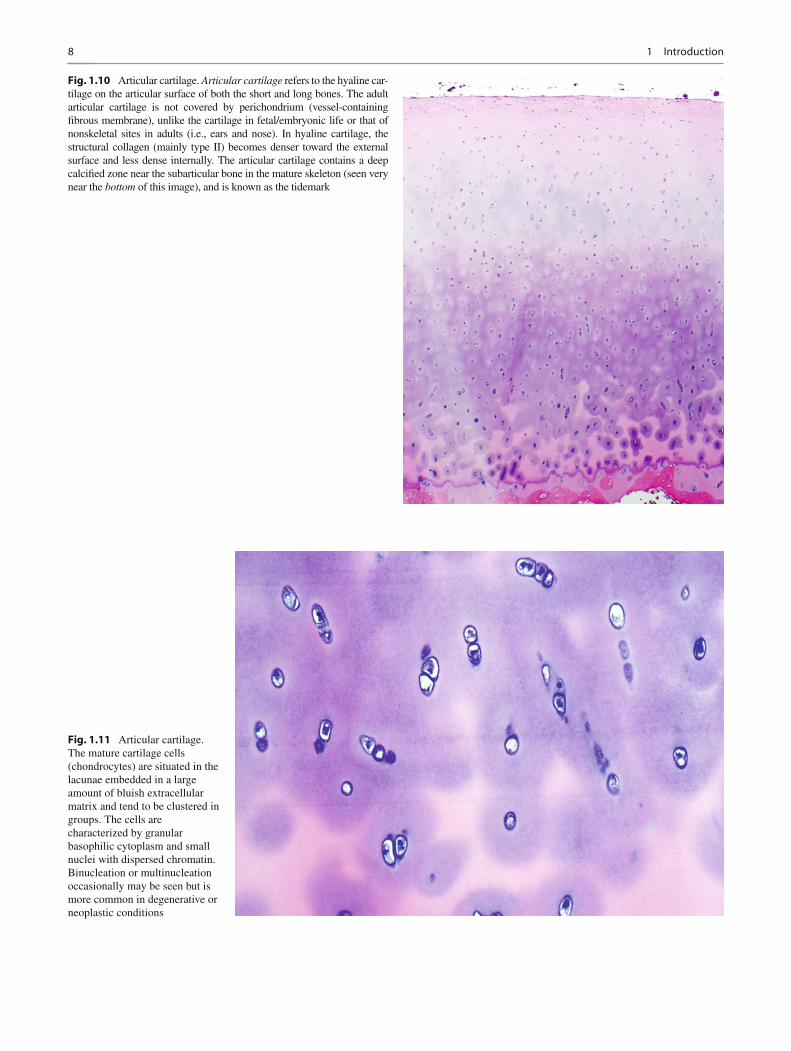
Fig. 1.11 Articular cartilage. The mature cartilage cells (chondrocytes) are situated in the lacunae embedded in a large amount of bluish extracellular matrix and tend to be clustered in groups. The cells are characterized by granular basophilic cytoplasm and small nuclei with dispersed chromatin. Binucleation or multinucleation occasionally may be seen but is more common in degenerative or neoplastic conditions
Fig. 1.10 Articular cartilage. Articular cartilage refers to the hyaline car-tilage on the articular surface of both the short and long bones. The adult articular cartilage is not covered by perichondrium (vessel-containing fi brous membrane), unlike the cartilage in fetal/embryonic life or that of nonskeletal sites in adults (i.e., ears and nose). In hyaline cartilage, the structural collagen (mainly type II) becomes denser toward the external surface and less dense internally. The articular cartilage contains a deep calci fi ed zone near the subarticular bone in the mature skeleton (seen very near the bottom of this image), and is known as the tidemark
91.1 Normal Bone Histology
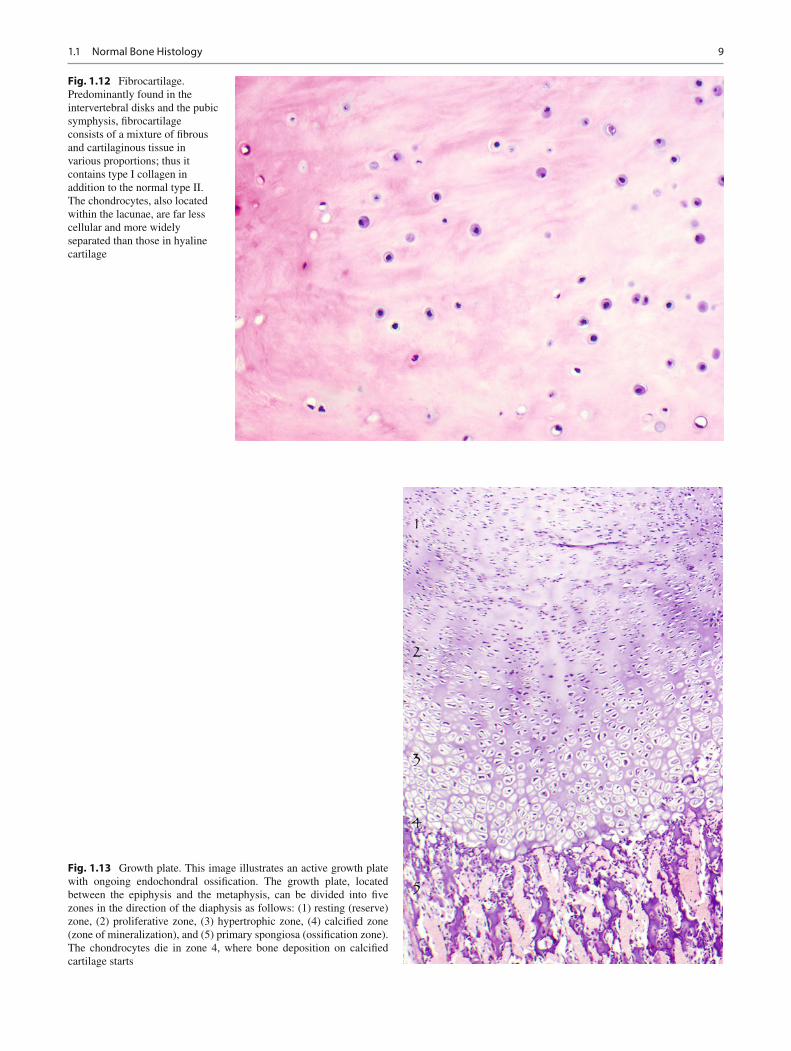
Fig. 1.12 Fibrocartilage. Predominantly found in the intervertebral disks and the pubic symphysis, fi brocartilage consists of a mixture of fi brous and cartilaginous tissue in various proportions; thus it contains type I collagen in addition to the normal type II. The chondrocytes, also located within the lacunae, are far less cellular and more widely separated than those in hyaline cartilage
Fig. 1.13 Growth plate. This image illustrates an active growth plate with ongoing endochondral ossi fi cation. The growth plate, located between the epiphysis and the metaphysis, can be divided into fi ve zones in the direction of the diaphysis as follows: (1) resting (reserve) zone, (2) proliferative zone, (3) hypertrophic zone, (4) calci fi ed zone (zone of mineralization), and (5) primary spongiosa (ossi fi cation zone). The chondrocytes die in zone 4, where bone deposition on calci fi ed cartilage starts
10 1 Introduction
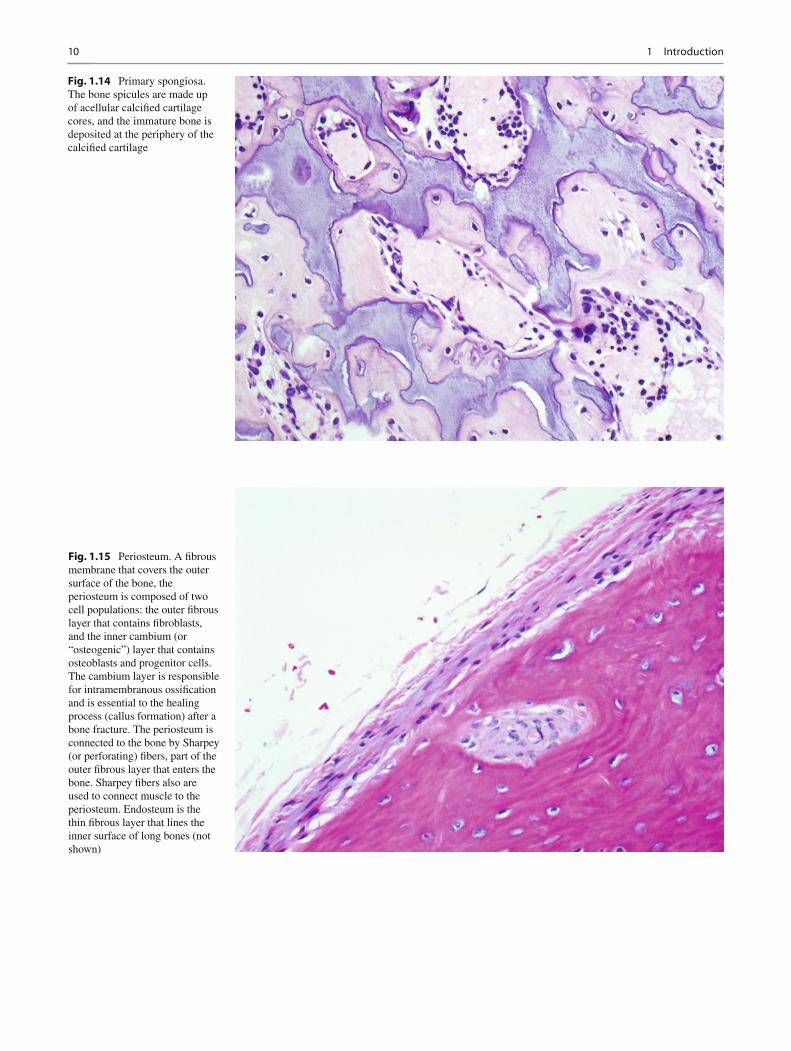
Fig. 1.14 Primary spongiosa. The bone spicules are made up of acellular calci fi ed cartilage cores, and the immature bone is deposited at the periphery of the calci fi ed cartilage
Fig. 1.15 Periosteum. A fi brous membrane that covers the outer surface of the bone, the periosteum is composed of two cell populations: the outer fi brous layer that contains fi broblasts, and the inner cambium (or “osteogenic”) layer that contains osteoblasts and progenitor cells. The cambium layer is responsible for intramembranous ossi fi cation and is essential to the healing process (callus formation) after a bone fracture. The periosteum is connected to the bone by Sharpey (or perforating) fi bers, part of the outer fi brous layer that enters the bone. Sharpey fi bers also are used to connect muscle to the periosteum. Endosteum is the thin fi brous layer that lines the inner surface of long bones (not shown)
111.2 Callus
1.2 Callus
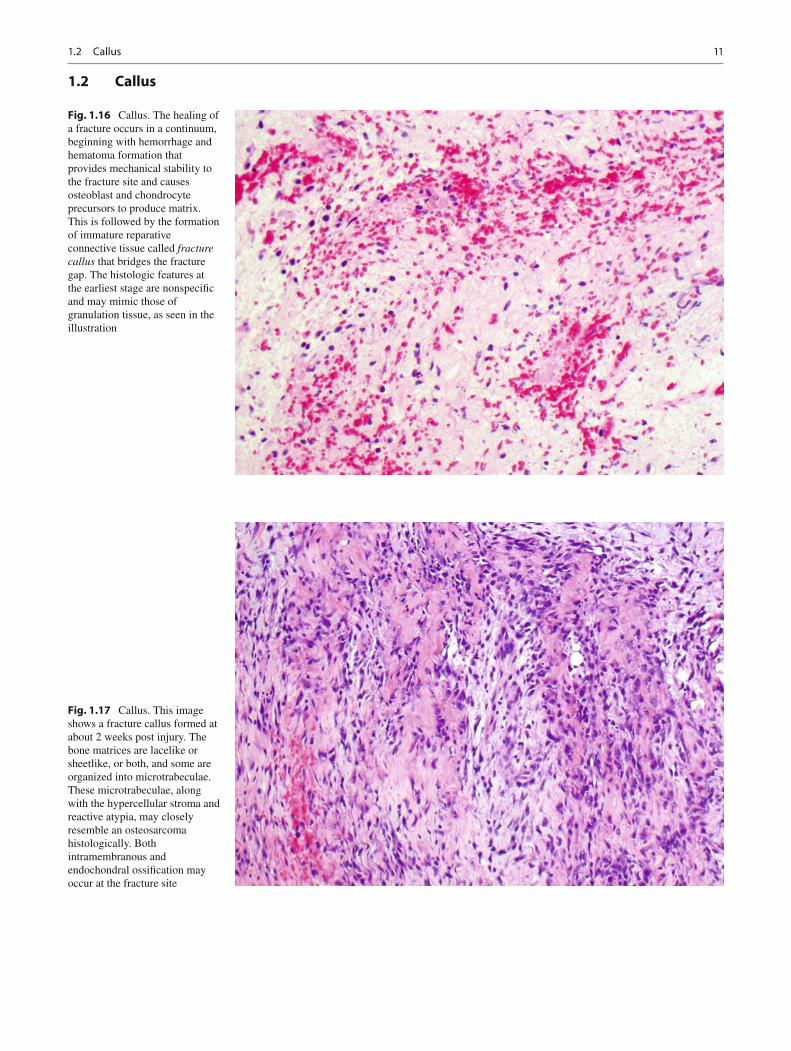
Fig. 1.16 Callus. The healing of a fracture occurs in a continuum, beginning with hemorrhage and hematoma formation that provides mechanical stability to the fracture site and causes osteoblast and chondrocyte precursors to produce matrix. This is followed by the formation of immature reparative connective tissue called fracture callus that bridges the fracture gap. The histologic features at the earliest stage are nonspeci fi c and may mimic those of granulation tissue, as seen in the illustration
Fig. 1.17 Callus. This image shows a fracture callus formed at about 2 weeks post injury. The bone matrices are lacelike or sheetlike, or both, and some are organized into microtrabeculae. These microtrabeculae, along with the hypercellular stroma and reactive atypia, may closely resemble an osteosarcoma histologically. Both intramembranous and endochondral ossi fi cation may occur at the fracture site
12 1 Introduction
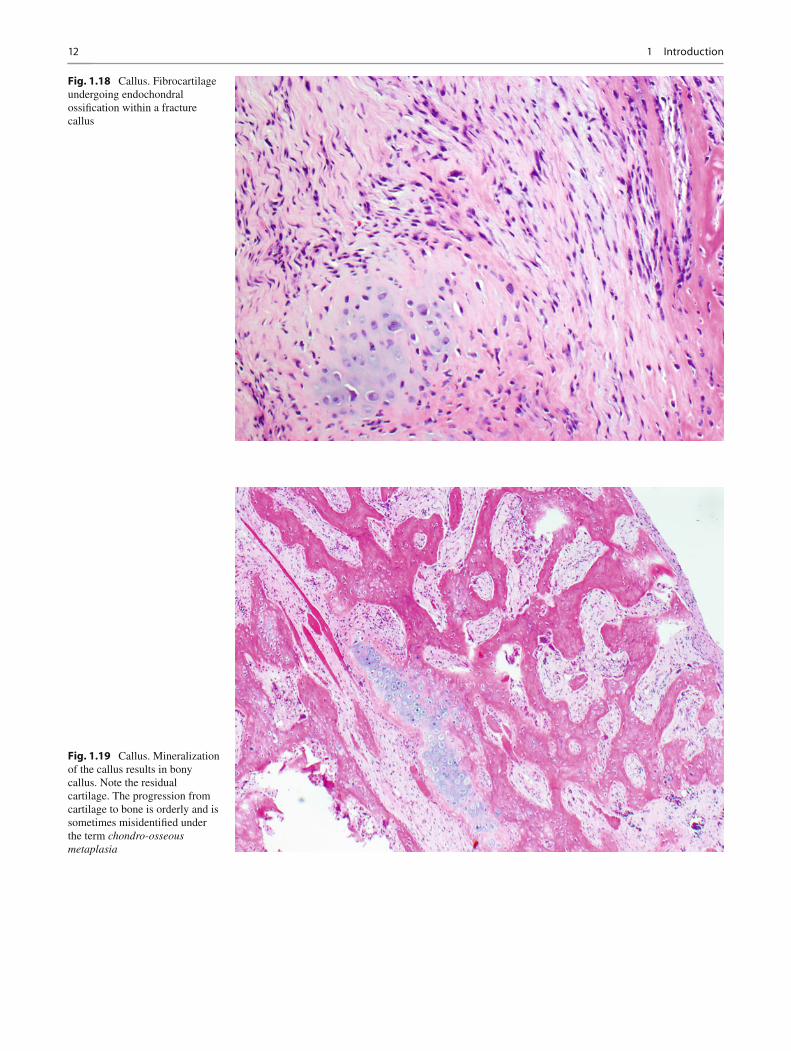
Fig. 1.18 Callus. Fibrocartilage undergoing endochondral ossi fi cation within a fracture callus
Fig. 1.19 Callus. Mineralization of the callus results in bony callus. Note the residual cartilage. The progression from cartilage to bone is orderly and is sometimes misidenti fi ed under the term chondro-osseous metaplasia
131.2 Callus
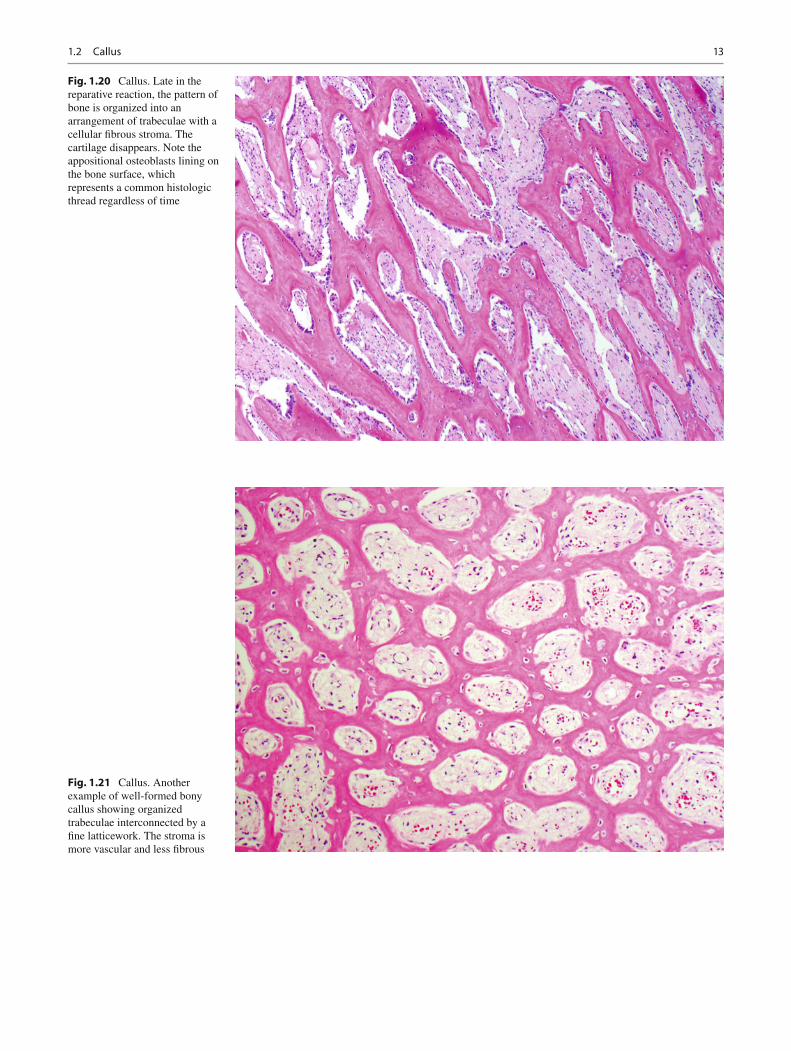
Fig. 1.20 Callus. Late in the reparative reaction, the pattern of bone is organized into an arrangement of trabeculae with a cellular fi brous stroma. The cartilage disappears. Note the appositional osteoblasts lining on the bone surface, which represents a common histologic thread regardless of time
Fig. 1.21 Callus. Another example of well-formed bony callus showing organized trabeculae interconnected by a fi ne latticework. The stroma is more vascular and less fi brous
14 1 Introduction
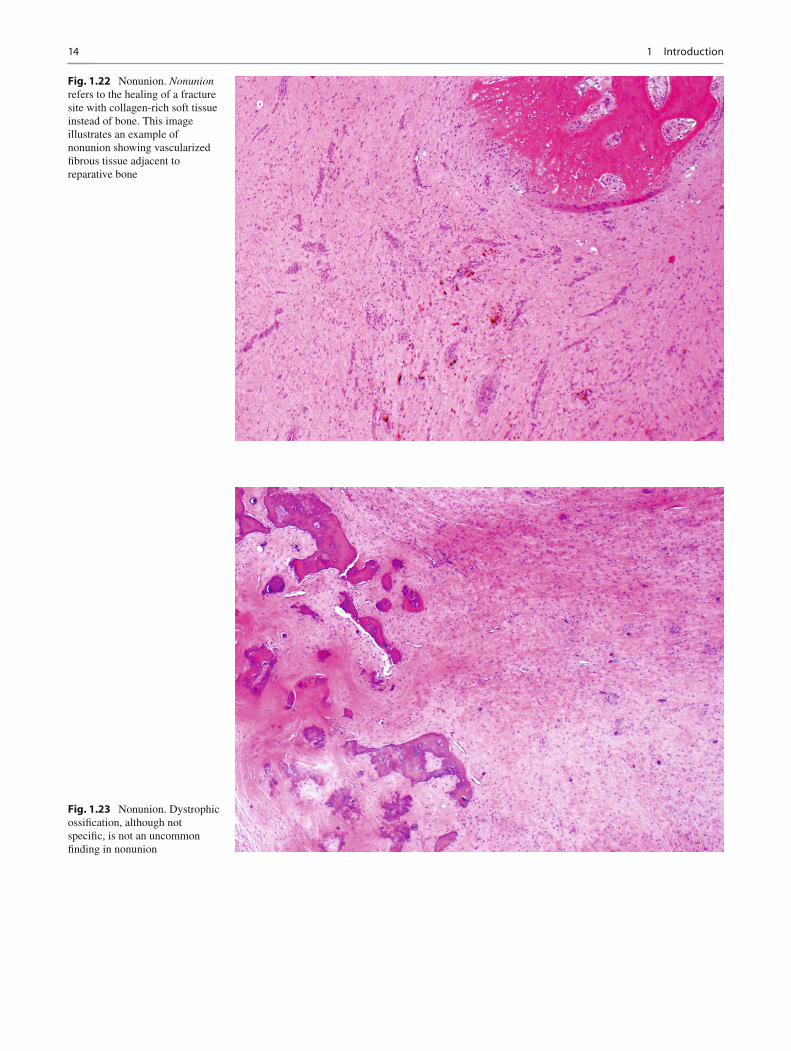
Fig. 1.22 Nonunion. Nonunion refers to the healing of a fracture site with collagen-rich soft tissue instead of bone. This image illustrates an example of nonunion showing vascularized fi brous tissue adjacent to reparative bone
Fig. 1.23 Nonunion. Dystrophic ossi fi cation, although not speci fi c, is not an uncommon fi nding in nonunion