atrial fibrillation ablation indications and results fibrillation ablation.pdf · atrial...
TRANSCRIPT

Atrial Fibrillation Ablation
Indications and Results
Oussama M. Wazni, M.D., FACC
AUB MC

NAAMA’s 24th International Medical Convention
Medicine in the Next Decade: Challenges and Opportunities
Beirut, Lebanon
June 26 – July 2, 2010
I have no actual or potential conflict of interest in relation to this program or presentation. I will inform the audience of any off-label uses discussed.
Name of Presenter:__Oussama Wazni______________________________

Atrial Fibrillation
Affects approximately 2 million people in the United States,
Less than 1% in persons younger than 60 years of age to more than 8% in those older than 80 years
Major Cause of Stroke
Increased mortality riskRelative risk of death increased by 1.5 in men
and 1.9 in women

Rate vs. Rhythm
Medical Approach
Neither approach was superior in terms of mortality at long-term follow-up
32.2 % of the AFFIRM study patients experienced serious events
Only 39% of patients taking AAD including amiodarone and 10% of patients taking AV blocking agent were in NSR at the end of the RACE study

In an analysis of the AFFIRM trial, sinus
rhythm was associated with a 47% reduction
in the risk of death whereas use of
antiarrhythmic drug therapy was associated
with a 49% increase in mortality

Limitations of Antiarrhythmic Therapy
<50% efficacy
Pro-arrhythmia
Toxicity
cost

Treatment
In asymptomatic patients then rate control
and anticoagulation strategy
In symptomatic patients then rhythm control
– Antiarrhythmic meds first
– At this time recurrence of AF after only one AAD
is considered an indication for ablation

AMIODARONE
indirect meta-analysis
dronedarone can prolong survival. But there
was a trend: an increased all-cause
mortality risk with amiodarone, at an OR of
1.61 (95% CI 0.97-2.68), fell short of
significance (p=0.066)
8 studies
Piccini JP, Hasselblad V, Peterson ED, et al. Comparative efficacy of
dronedarone
and amiodarone for the maintenance of sinus rhythm in patients with atrial
fibrillation. J Am Coll Cardiol 2009; 54:1089-1095
Alternative
A therapy that restores and maintains sinus rhythm while avoiding the deleterious effects of AADs would improve survival.
Pulmonary vein isolation may be such a therapy.
In a recent observational study involving a relatively large number of patients, Pappone et al. reported that AF ablation was associated with significantly lower mortality and adverse events compared with drug therapy
AF ablation in heart failure improves EF

The Present

Long Term
PAF cure 80-85%
Persistent/ Chronic 60-75%
Previously ineffective AAD may become
very effective

AF begets AF
ERPs and conduction times of the right atrium (RA), left atrium (LA), and the PVs were determined at baseline.
AF was induced and maintained for a period of 15 min.
Stimulation protocol was repeated.
At baseline, the PVs had significantly longer ERPs than the atria. After exposure to AF, the ERPs of both the atria and the PVs decreased significantly.
AF was more frequently induced after the presence of AF, particularly by pacing in the PVs
J Am Coll Cardiol. 2008 Jun 3;51(22):2161-2.

Sinus Begets Sinus
Artificial maintenance of AF leads to a
marked shortening of AERP, a reversion of
its physiological rate adaptation, and an
increase in rate, inducibility and stability of
AF.
All these changes were completely
reversible within 1 week of sinus rhythm.
Circulation. 1995 Oct 1;92(7):1954-68

70 Patients
PV-LA Junction Disconnection
(ICE+CM guided)
N=33
Randomized
Antiarrhythmic drug therapy
for rhythm control
N=37
RAAFT
Wazni et al JAMA

PVI AAD p
Patients 33 37 ns
Age (years) 538 548 ns
Left atrial size (cm) 4.10.8 4.20.7 ns
Duration of AF (years) 52.0 52.5 ns
Paroxysmal AF 32 35 ns
Persistent AF 1 2 Ns
SHD/HTN 25% (8/33) 28% (10/37) ns
Ejection fraction % 535 546 ns
Use of Beta-blockers 57% 62% ns
RAAFTPatient population
Wazni et al JAMA

PVI AAD p
Symptomatic AF
Recurrence
13%(4/32) 63% (22/35) <0.05
Re-hospitalization 9% (3/32) 54% (19/35) <0.01
Embolic events none none ns
Bleeding 6.3% (2/32) 2.9% (1/35) ns
Bradycardia none 8.6% (3/35) < 0.05
Severe PV stenosis none none ns
Mild PV stenosis 3% (1/32) none < 0.05
Moderate PV stenosis 3% (1/32) none < 0.05
RAAFT
Followup Results
Wazni et al JAMA

PABA CHF


Freedom from
symptomatic atrial
arrhythmia
0
ThermoCool AF
Protocol defined failure was lower with catheter ablation vs.
ADT: HR 0.30
Freedom from symptomatic and any (63% vs. 17%, p < 0.001)
recurrent atrial arrhythmia improved with catheter ablation
Adverse events were similar (4.9% vs. 8.8%, p = NS)
Trial design: Patients with symptomatic paroxysmal AF who had failed one antiarrhythmic
drug were randomized in 2:1 fashion to catheter ablation or ADT & monitored for 9 months.
Results
Wilber DJ, et al. JAMA 2010;303:333-40
Catheter ablation
(n = 106)
• Catheter ablation associated with better
intermediate-term outcomes vs. ADT in
patients with symptomatic paroxysmal AF,
who have failed one antiarrhythmic drug
• Further long-term data are awaited
16.0
66.0
%
(p < 0.001)
Conclusions
ADT
(n = 61)
Protocol-defined failure
(p < 0.001)
70.0
19.0
100
50
0
100
50
%

Thermocool AF


Thermocool Complications
1 pericardial effusion,1 edema, 1
pneumonia, 1 vascular complication,and 1
heart failure) in the
catheter ablation group (5/103 [4.9%])
5 patients (2 with life-threatening
arrhythmias and 3 with disabling drug
intolerance requiring discontinuation)
in the ADT group (5/57 [8.8%]).

Cessation of Coagulation
3,355 patients: 2,692 discontinued OAT 3 to 6 months after ablation (Off-OAT group) and 663 remained on OAT after this period (On-OAT group).
CHADS2 1 ≥2 Off-OAT 723 (27%) 347 (13%) On-OAT 261 (39%) 247 (37%)
Follow-up
28 ± 13 months Ischemic Stroke Hemorrhage
Off-OAT 2 (0.07%) 1 (0.04%) p = 0.06 On-OAT 3 (0.45%) 13 (2%) p < 0.0001
No other thromboembolic events occurred.
No Off-OAT group patient with a CHADS2 risk score of ≥2 had an ischemic stroke.
the risk–benefit ratio favored the suspension of OAT after successful AF ablation even in patients at moderate-high risk of TE.
Themistoclakis,JACC February 2010, 735-743

PV Isolation & Substrate ModificationNademanee et al (JACC 2004;43:2044-53)
Pappone et al (Circulation 2004;109:327-334)
Nakagawa et al (HR 2005;2(Suppl):S10-S11)Natale et al.2003
Oral H., Circulation 2003;108:2355
Pappone C., Circulation 2001;104:2539. Paschon, et al..

AF Catheter Ablation Strategies
Targets
1. Pulmonary Vein Isolation
Antral, focal, segmental, ostial
2. Substrate Modification
CFAE’s, lines, circles, tachycardias
3. Autonomic Modulation
“Ganglionic Plexi”

PV Antrum Isolation: Catheter Ablation

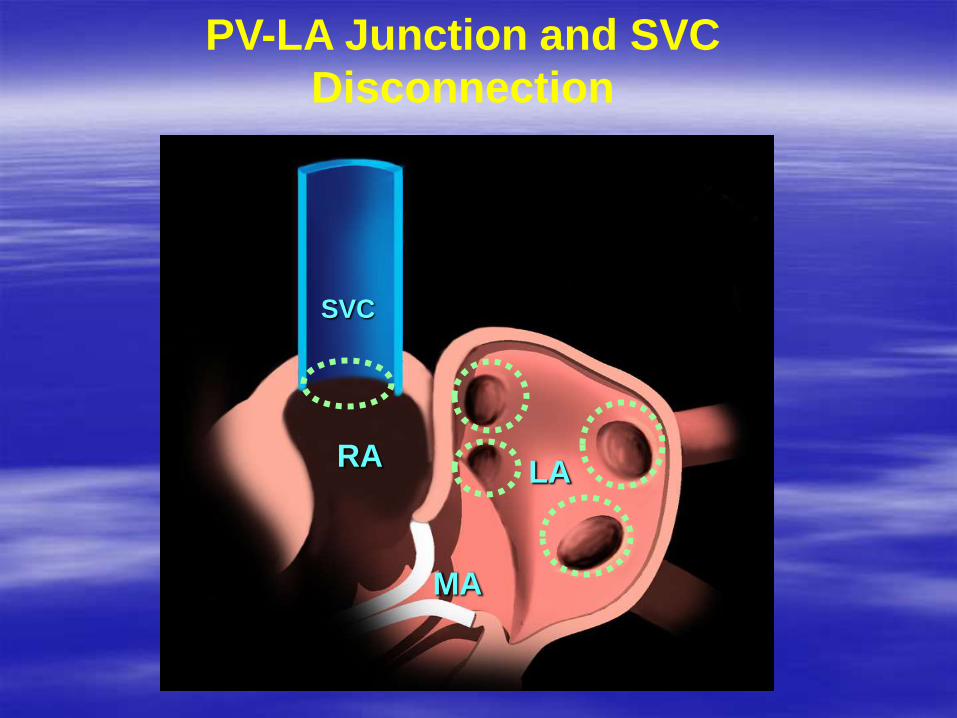
PV-LA Junction and SVC
Disconnection
RALA
MA
SVC


PV Antrum Isolation

Post RFA: Voltage Map



ICE Imaging - Transseptal

ICE guided PV-LA junction disconnection
Lasso-Catheter
RLPV
RUPV
PA

SVC Isolation
Pulmonary artery
SVC
Right superior PV
Lasso catheter

SVC Isolation

Importance of ICE
January 2005 and December 2008, PVI was performed in 3,052 patients with therapeutic INR (≥1.8) at the time of ablation.
Mean INR was 2.53 ± 0.62.
Only 3 (0.098%) patients had ischemic strokes.
One patient had a hemorrhagic stroke on the third day postablation but recovered completely by 1-week follow-up.
Bleeding complications occurred in 34 (1.11%) patients; most were minor (0.79%).
Major hemorrhagic complications occurred in 10 (0.33%) patients (tamponade in 5,(0.16%)
hematomas requiring intervention in 2, transfusion necessary in 3).
Wazni et al, Heart Rhythm Journal, 2010

Circular Mapping Approach to PVAI
Major Complications
0.6% 0.0% 0.3%
0.7% 0.0%

Future ?