complications of ablation of atrial fibrillation how to prevent and to treat complications of...
TRANSCRIPT

Complications of Ablation Complications of Ablation of Atrial Fibrillationof Atrial Fibrillation
How to Prevent and to TreatHow to Prevent and to Treat
Complications of Ablation Complications of Ablation of Atrial Fibrillationof Atrial Fibrillation
How to Prevent and to TreatHow to Prevent and to Treat
Yong-Mei Cha, MDYong-Mei Cha, MDMayo Clinic, Rochester, MNMayo Clinic, Rochester, MN
GW-ICC 2005, BeijingGW-ICC 2005, Beijing

Incidence of complicationsIncidence of complicationsIncidence of complicationsIncidence of complications
Mayo ClinicMayo Clinic
AF ablation AF ablation
1999-20041999-2004
N=623N=623
Mayo ClinicMayo Clinic
AF ablation AF ablation
1999-20041999-2004
N=623N=623
• Pericardial effusion Pericardial effusion 70 (11%)70 (11%)
Tamponade Tamponade 15 (2.4%) 15 (2.4%)
• Stroke/TIAStroke/TIA 5 (0.8%)5 (0.8%)
• Phrenic nerve injuryPhrenic nerve injury 5 (0.8%)5 (0.8%)
• Pulmonary vein stenosis 20 (3.2%)Pulmonary vein stenosis 20 (3.2%)
• Myocardial infarctionMyocardial infarction 2 (0.3%) 2 (0.3%)
• Valve injuryValve injury 1 (0.2%)1 (0.2%)
• Groin hematomaGroin hematoma 14 (2.2%)14 (2.2%)
• Atrioesophageal fistulaAtrioesophageal fistula ??
• Pericardial effusion Pericardial effusion 70 (11%)70 (11%)
Tamponade Tamponade 15 (2.4%) 15 (2.4%)
• Stroke/TIAStroke/TIA 5 (0.8%)5 (0.8%)
• Phrenic nerve injuryPhrenic nerve injury 5 (0.8%)5 (0.8%)
• Pulmonary vein stenosis 20 (3.2%)Pulmonary vein stenosis 20 (3.2%)
• Myocardial infarctionMyocardial infarction 2 (0.3%) 2 (0.3%)
• Valve injuryValve injury 1 (0.2%)1 (0.2%)
• Groin hematomaGroin hematoma 14 (2.2%)14 (2.2%)
• Atrioesophageal fistulaAtrioesophageal fistula ??

Pericardial effusion and TamponadePericardial effusion and TamponadePericardial effusion and TamponadePericardial effusion and Tamponade
• Small pericardial effusion is common (11%) in wide Small pericardial effusion is common (11%) in wide area circumferential ablation due to extensive area circumferential ablation due to extensive transmural lesions. transmural lesions.
• Pericarditis is not uncommon, pleuritic chest pain.Pericarditis is not uncommon, pleuritic chest pain.
• Myocardial perforation and tamponade Myocardial perforation and tamponade
Mayo 2.4%, Haissaguerre group 2.9%Mayo 2.4%, Haissaguerre group 2.9%
catheter induced catheter induced mechanical perforationmechanical perforation, , 0.5%0.5%
““popping” popping” during energy delivery, 2.4%during energy delivery, 2.4%
•
• Small pericardial effusion is common (11%) in wide Small pericardial effusion is common (11%) in wide area circumferential ablation due to extensive area circumferential ablation due to extensive transmural lesions. transmural lesions.
• Pericarditis is not uncommon, pleuritic chest pain.Pericarditis is not uncommon, pleuritic chest pain.
• Myocardial perforation and tamponade Myocardial perforation and tamponade
Mayo 2.4%, Haissaguerre group 2.9%Mayo 2.4%, Haissaguerre group 2.9%
catheter induced catheter induced mechanical perforationmechanical perforation, , 0.5%0.5%
““popping” popping” during energy delivery, 2.4%during energy delivery, 2.4%
•

Pericardial EffusionPericardial EffusionPericardial EffusionPericardial Effusion

How to prevent myocardial perforationHow to prevent myocardial perforationHow to prevent myocardial perforationHow to prevent myocardial perforation
♥♥ Understand atrial anatomy Understand atrial anatomy
♥♥ Gentle catheter manipulationGentle catheter manipulation
♥♥ use 4 or 5mm catheter tip if possibleuse 4 or 5mm catheter tip if possible
♥♥ Monitor arterial blood pressure continuouslyMonitor arterial blood pressure continuously
♥♥ Monitor pericardial space by intracardiac echoMonitor pericardial space by intracardiac echo
♥♥ Understand atrial anatomy Understand atrial anatomy
♥♥ Gentle catheter manipulationGentle catheter manipulation
♥♥ use 4 or 5mm catheter tip if possibleuse 4 or 5mm catheter tip if possible
♥♥ Monitor arterial blood pressure continuouslyMonitor arterial blood pressure continuously
♥♥ Monitor pericardial space by intracardiac echoMonitor pericardial space by intracardiac echo

How to manage pericardial effusion How to manage pericardial effusion How to manage pericardial effusion How to manage pericardial effusion
♥♥ Small pericardial effusion: usually asymptomatic Small pericardial effusion: usually asymptomatic and do not require treatmentand do not require treatment
♥♥ Pericarditis: anti-inflammatory agent for a week Pericarditis: anti-inflammatory agent for a week to relieve chest painto relieve chest pain
♥♥ Tamponade: requires emergency Tamponade: requires emergency pericardiocentisis to drain hemapericardium pericardiocentisis to drain hemapericardium Surgical myocardial repair is rarely requiredSurgical myocardial repair is rarely required
♥♥ Small pericardial effusion: usually asymptomatic Small pericardial effusion: usually asymptomatic and do not require treatmentand do not require treatment
♥♥ Pericarditis: anti-inflammatory agent for a week Pericarditis: anti-inflammatory agent for a week to relieve chest painto relieve chest pain
♥♥ Tamponade: requires emergency Tamponade: requires emergency pericardiocentisis to drain hemapericardium pericardiocentisis to drain hemapericardium Surgical myocardial repair is rarely requiredSurgical myocardial repair is rarely required

Thromboembolic strokeThromboembolic strokeThromboembolic strokeThromboembolic stroke
• Mayo Clinic, 5 patients, 0.8%Mayo Clinic, 5 patients, 0.8%
• Causes: Causes: ♥ ♥ preexisting left atrial clotpreexisting left atrial clot♥♥ new clot is formed during the new clot is formed during the
ablationablation often on the sheath, lasso and often on the sheath, lasso and ablationablation
cathetercatheter♥ ♥ ablation lesion thrombosisablation lesion thrombosis
• 21/270 (8%) patients had thrombi, attached to: 21/270 (8%) patients had thrombi, attached to: EP catheter/sheath 17/21EP catheter/sheath 17/21Endocardial surface 5/21Endocardial surface 5/21
• Mayo Clinic, 5 patients, 0.8%Mayo Clinic, 5 patients, 0.8%
• Causes: Causes: ♥ ♥ preexisting left atrial clotpreexisting left atrial clot♥♥ new clot is formed during the new clot is formed during the
ablationablation often on the sheath, lasso and often on the sheath, lasso and ablationablation
cathetercatheter♥ ♥ ablation lesion thrombosisablation lesion thrombosis
• 21/270 (8%) patients had thrombi, attached to: 21/270 (8%) patients had thrombi, attached to: EP catheter/sheath 17/21EP catheter/sheath 17/21Endocardial surface 5/21Endocardial surface 5/21


Suction from the sheathSuction from the sheathSuction from the sheathSuction from the sheath
How to prevent strokeHow to prevent strokeHow to prevent strokeHow to prevent stroke
• Pre-ablation:Pre-ablation: transesophageal echocardiogram to transesophageal echocardiogram to
rule-out atrial thrombusrule-out atrial thrombus
• During ablation:During ablation:
intracardiac echocardiogram intracardiac echocardiogram systemic and sheath systemic and sheath
heparinizationheparinization
• Post-ablation:Post-ablation: coumadincoumadin
• Pre-ablation:Pre-ablation: transesophageal echocardiogram to transesophageal echocardiogram to
rule-out atrial thrombusrule-out atrial thrombus
• During ablation:During ablation:
intracardiac echocardiogram intracardiac echocardiogram systemic and sheath systemic and sheath
heparinizationheparinization
• Post-ablation:Post-ablation: coumadincoumadin
During ablation:During ablation:
intracardiac echocardiogramintracardiac echocardiogram♦♦ facilitate transseptal facilitate transseptal
puncturepuncture♦♦ monitor clot and bubblesmonitor clot and bubbles♦♦ identify venoatrial junctionidentify venoatrial junction♦♦ monitor pericaridial monitor pericaridial
effusioneffusion
During ablation:During ablation:
intracardiac echocardiogramintracardiac echocardiogram♦♦ facilitate transseptal facilitate transseptal
puncturepuncture♦♦ monitor clot and bubblesmonitor clot and bubbles♦♦ identify venoatrial junctionidentify venoatrial junction♦♦ monitor pericaridial monitor pericaridial
effusioneffusion
How to prevent strokeHow to prevent strokeHow to prevent strokeHow to prevent stroke

How to prevent strokeHow to prevent strokeHow to prevent strokeHow to prevent stroke
During AblationDuring AblationAA ssystemic ystemic
heparinization to heparinization to maintain maintain ACT 300-350 when catheters are ACT 300-350 when catheters are in in the left atrium after the left atrium after transseptaltransseptal
BB continuous continuous heparinized saline heparinized saline infusion infusion through transseptal through transseptal sheathssheaths
CC if clot is formed on the if clot is formed on the catheter, catheter, remove the catheter remove the catheter and suck the and suck the sheathsheath
During AblationDuring AblationAA ssystemic ystemic
heparinization to heparinization to maintain maintain ACT 300-350 when catheters are ACT 300-350 when catheters are in in the left atrium after the left atrium after transseptaltransseptal
BB continuous continuous heparinized saline heparinized saline infusion infusion through transseptal through transseptal sheathssheaths
CC if clot is formed on the if clot is formed on the catheter, catheter, remove the catheter remove the catheter and suck the and suck the sheathsheath

How to prevent strokeHow to prevent strokeHow to prevent strokeHow to prevent stroke
Post-ablationPost-ablation
AA low molecular weight heparin low molecular weight heparin injection starting the next morning injection starting the next morning until INR ≥ 2.0until INR ≥ 2.0
BB coumadincoumadin starting the evening of starting the evening of ablation and for at least 3 months ablation and for at least 3 months to prevent lesion thrombusto prevent lesion thrombus
Post-ablationPost-ablation
AA low molecular weight heparin low molecular weight heparin injection starting the next morning injection starting the next morning until INR ≥ 2.0until INR ≥ 2.0
BB coumadincoumadin starting the evening of starting the evening of ablation and for at least 3 months ablation and for at least 3 months to prevent lesion thrombusto prevent lesion thrombus

Phrenic nerve injuryPhrenic nerve injuryPhrenic nerve injuryPhrenic nerve injury
• Uncommon, <1%Uncommon, <1%
• the right phrenic nerve has close proximity the right phrenic nerve has close proximity
to the superior caval vein 0.3 mm to the superior caval vein 0.3 mm to the right superior pulmonary vein 2.1 to the right superior pulmonary vein 2.1 mmmm
• Uncommon, <1%Uncommon, <1%
• the right phrenic nerve has close proximity the right phrenic nerve has close proximity
to the superior caval vein 0.3 mm to the superior caval vein 0.3 mm to the right superior pulmonary vein 2.1 to the right superior pulmonary vein 2.1 mmmm


Phrenic Stimulation SiteRSPV

Post-ablationPre-ablation
Right hemidiaphragm paralysis

How to prevent phrenic nerve injuryHow to prevent phrenic nerve injuryHow to prevent phrenic nerve injuryHow to prevent phrenic nerve injury
♥♥ Be cautious when ablate right superiorBe cautious when ablate right superiorpulmonary veinpulmonary vein
♥♥ High output pacing from ablation catheter High output pacing from ablation catheter before delivering the energy.before delivering the energy.
♥♥ Be cautious when ablate right superiorBe cautious when ablate right superiorpulmonary veinpulmonary vein
♥♥ High output pacing from ablation catheter High output pacing from ablation catheter before delivering the energy.before delivering the energy.

Pulmonary vein stenosisPulmonary vein stenosis
• The lesion is characterized by intimal thickening, The lesion is characterized by intimal thickening, thrombus formation, endocardial contraction, thrombus formation, endocardial contraction, and proliferation of elastic laminae and proliferation of elastic laminae

Diagnosis of PV stenosisDiagnosis of PV stenosisDiagnosis of PV stenosisDiagnosis of PV stenosis
• The mean onset of symptoms is two to five The mean onset of symptoms is two to five months after the procedure months after the procedure
• Progressive dyspnea on exertion, orthopnea, Progressive dyspnea on exertion, orthopnea, Intermittent cough, hemoptysisIntermittent cough, hemoptysis
• Chest CT: pulmonary vein narrowingChest CT: pulmonary vein narrowing
• Echo Doppler: increased PV flow velocityEcho Doppler: increased PV flow velocity
• VQ Scan: Markedly reduced lung perfusionVQ Scan: Markedly reduced lung perfusion



Pre ablation
Pre ablation
Post ablation
Post ablation
LIPV stenosis

How to prevent PV stenosisHow to prevent PV stenosisHow to prevent PV stenosisHow to prevent PV stenosis
♥♥ PV venogram may help to identify venoatrial PV venogram may help to identify venoatrial junctionjunction
♥♥ Intracardiac echocardiography monitor PV flow Intracardiac echocardiography monitor PV flow velocityvelocity
♥♥ Ablate outside of PV orificeAblate outside of PV orifice
♥♥ RF power RF power ≤ 30W, Temperature ≤ 50 ºC≤ 30W, Temperature ≤ 50 ºC
♥♥ Fewer burns in small pulmonary veinsFewer burns in small pulmonary veins
♥♥ PV venogram may help to identify venoatrial PV venogram may help to identify venoatrial junctionjunction
♥♥ Intracardiac echocardiography monitor PV flow Intracardiac echocardiography monitor PV flow velocityvelocity
♥♥ Ablate outside of PV orificeAblate outside of PV orifice
♥♥ RF power RF power ≤ 30W, Temperature ≤ 50 ºC≤ 30W, Temperature ≤ 50 ºC
♥♥ Fewer burns in small pulmonary veinsFewer burns in small pulmonary veins

RSPVRSPV

ICE guidanceICE guidanceICE guidanceICE guidance

How to manage pulmonary vein stenosisHow to manage pulmonary vein stenosisHow to manage pulmonary vein stenosisHow to manage pulmonary vein stenosis
• Mild to moderate pulmonary narrowing Mild to moderate pulmonary narrowing ≤50%:≤50%: observationobservation
• Moderate to severe PV stenosis: close follow-up, Moderate to severe PV stenosis: close follow-up, chest CT in 3 monthschest CT in 3 months
• Severe PV stenosis Severe PV stenosis ≥90%: PV dilation and ≥90%: PV dilation and stenting. stenting.
• Mild to moderate pulmonary narrowing Mild to moderate pulmonary narrowing ≤50%:≤50%: observationobservation
• Moderate to severe PV stenosis: close follow-up, Moderate to severe PV stenosis: close follow-up, chest CT in 3 monthschest CT in 3 months
• Severe PV stenosis Severe PV stenosis ≥90%: PV dilation and ≥90%: PV dilation and stenting. stenting.
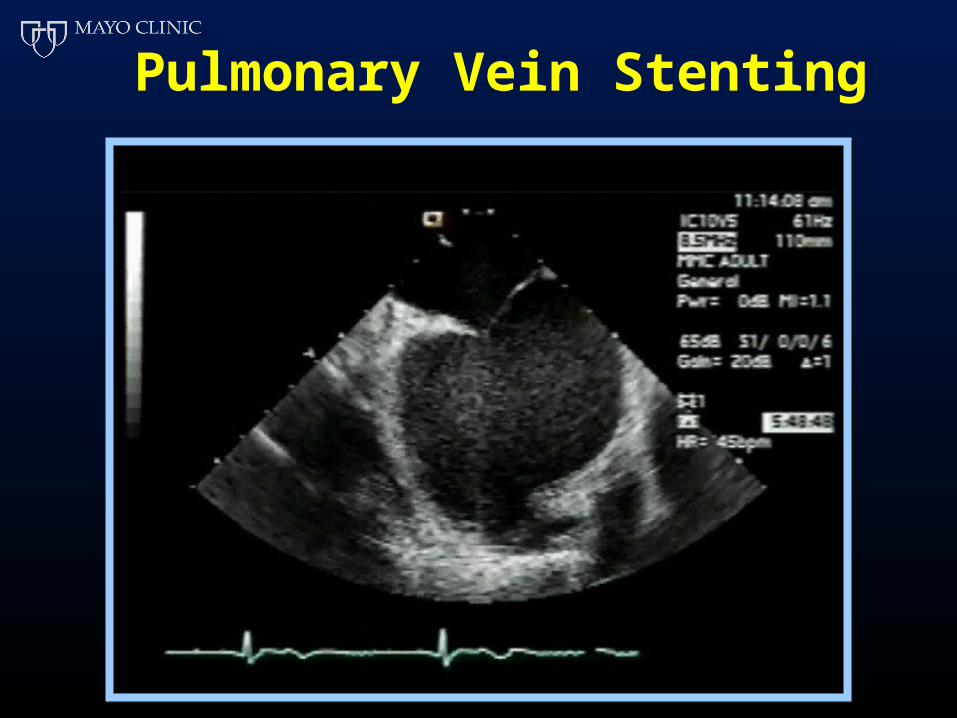
Pulmonary Vein Stenting


LSPV 45/25 (mean=24) LSPV 23/12 (mean=17)
Mean LA = 8 Mean LA = 9
P = 16 P = 8


Atrioesophageal fistulaAtrioesophageal fistulaAtrioesophageal fistulaAtrioesophageal fistula
• Incidence? FatalIncidence? Fatal
• Esophagitis: Heartburn, midsternal painEsophagitis: Heartburn, midsternal pain
• Bacteremia: fever, chills, Bacteremia: fever, chills,
• Thromboembolism or air embolism: neurological Thromboembolism or air embolism: neurological deficitdeficit
• Massive gastrointestinal bleedingMassive gastrointestinal bleeding
• Incidence? FatalIncidence? Fatal
• Esophagitis: Heartburn, midsternal painEsophagitis: Heartburn, midsternal pain
• Bacteremia: fever, chills, Bacteremia: fever, chills,
• Thromboembolism or air embolism: neurological Thromboembolism or air embolism: neurological deficitdeficit
• Massive gastrointestinal bleedingMassive gastrointestinal bleeding

Lemola et al, Circ 2004

Lemola et al, Circ 2004

40%
20%
Lemola et al, Circ 2004
40%
Relationship of esophagus to posterior LA wall: 3D CT images

How to prevent atrioesophageal fistulaHow to prevent atrioesophageal fistulaHow to prevent atrioesophageal fistulaHow to prevent atrioesophageal fistula
♥♥ Placing esophageal probe and knowing the Placing esophageal probe and knowing the anatomic course of the esophagus under anatomic course of the esophagus under fluoroscopyfluoroscopy
♥♥ Tagging the anatomical relationship of Tagging the anatomical relationship of esophagus and left atrium on CARTO mapesophagus and left atrium on CARTO map
♥♥ measuring esophageal temperature during measuring esophageal temperature during ablationablation
♥♥ Monitoring microbubbles to adjust RF powerMonitoring microbubbles to adjust RF power
♥♥ Placing esophageal probe and knowing the Placing esophageal probe and knowing the anatomic course of the esophagus under anatomic course of the esophagus under fluoroscopyfluoroscopy
♥♥ Tagging the anatomical relationship of Tagging the anatomical relationship of esophagus and left atrium on CARTO mapesophagus and left atrium on CARTO map
♥♥ measuring esophageal temperature during measuring esophageal temperature during ablationablation
♥♥ Monitoring microbubbles to adjust RF powerMonitoring microbubbles to adjust RF power

AF ablationAF ablation
CP1121662-7
Elimination of AFElimination of AF70-80%70-80%
Elimination of AFElimination of AF70-80%70-80%
ComplicationsComplications6-8%6-8%
ComplicationsComplications6-8%6-8%
Weigh benefit and adverse effectsWeigh benefit and adverse effectsWeigh benefit and adverse effectsWeigh benefit and adverse effects

Ablation paradigm in CHF patients
Circumferential PV isolationn=19
Wide area LA ablationn=9

Wide area LA ablation (PA view)
RSPVLSPV
RIPV
LSPV




• PV ostia located with aid of ICE and accessed PV ostia located with aid of ICE and accessed using Multipurpose catheter advanced via using Multipurpose catheter advanced via Mullins sheath into LA Mullins sheath into LA
• Pressure gradient measured using catheters Pressure gradient measured using catheters and Doppler velocity signalsand Doppler velocity signals
• Pulmonary venographyPulmonary venography
Pulmonary Vein StentingPulmonary Vein Stenting