attachment 1 to board report 4 october t2 go-live …
TRANSCRIPT

NHS 24 GREEN
1
ATTACHMENT 1 to BOARD REPORT 4 OCTOBER T2 GO-LIVE DECISION MAKING CRITERIA – STATUS UPDATE
1. INTRODUCTION 1.1. At its August meeting, the NHS 24 Board endorsed a set of decision making
criteria which would be considered prior to any final decision to go-live with T2 of the SAP application. These criteria are shown in Appendix 1 along with the proposed evidence to support these criteria as agreed by a sub-set of the NHS 24 Board on 18 September.
1.2. This paper provides the latest update on the status of the work supporting
each of the criteria, to allow EMT to consider the optimal decision making approach ahead of the target go-live date of 24 October.
2. System Functionality 2.1. There are two tests of system functionality: a) Model Office Team Leader
Feedback and b) Clinical Governance Report. Model Office Team Leader Feedback (Appendix 2) 2.2. Engagement with Team Leaders and staff within the Model Office has been
ongoing since go-live in May 2017. During this time a series of system and operational issues have been identified which have led to a wide range of interventions including system changes (for changes to the functionality of the SAP application), process changes, training enhancements and other developments which will be implemented over time in line with a planned series of enhancements post T2.
2.3. All top priority change requests were implemented for testing at the end of August and testing is ongoing. Meanwhile, the programme team and Model Office teams have focused on resolving priority technical issues, specific concerns raised by Team Leaders relating to system functionality impacting the role of the Team Leader (Appendix 2) and resolving a series of issues identified in an observation session undertaken on Saturday 9 September (also included in Appendix 2).
2.4. The status of these issues is as follows: Total Open Closed Monitor Change Future Key Technical 13 1 12 1 - - TL Concerns 18 0 8 2 0 8 Observation 31 1 21 2 0 7 Clinical Governance Report (Appendix 3)

NHS 24 GREEN
2
2.5. Senior members of NHS 24's Clinical Management Team developed a clinical governance report for consideration by the Clinical Governance Committee which met on 26 September. This is included at Appendix 3.
3. Staff Readiness 3.1. There are three tests of staff readiness: a) Training feedback via survey
responses b) Operational Validation event c) Readiness survey prior to go-live Training Feedback 3.2. Appendix 4 summarises training feedback to date. As will be noted from the
summary, feedback on the training experience has been very positive. Operational Validation Event 3.3. The Operational Validation event on 29 September provided stakeholders with
the opportunity to speak directly with members of staff about the training they have undertaken and their readiness for go-live in October.
Readiness Survey 3.4. Appendix 5 contains the proposed questions for the staff readiness survey to
be issued approximately 1 week prior to go-live. These questions have been developed with input from staff-side colleagues.
4. Training Completion 4.1. The current status of training is shown in the table below. Clyde East Card North Local Total Available Staff 205 288 371 52 55 971 Trained/Scheduled 193 266 362 48 52 921 % 94% 92% 98% 92% 95% 95%
4.2. The remaining balance of available staff (50 staff) are currently being
scheduled for mop-up training which commences on 9 October.
4.3. A total of 84 staff are either on long-term sick leave, short-term sick leave or are on annual leave. These staff can only be scheduled for training on their return to work which will mean training has to be provided post go-live.
5. Contingency Planning
5.1. There are three tests to be met here: a) COPRG approved business continuity plan b) Roll-back criteria c) Evidence that Partner Boards are familiar with relevant aspects of the Plan and roll-back criteria.
Business Continuity Planning

NHS 24 GREEN
3
5.2. The contingency, communication and escalation process is included at
Appendix 6 and the related process 28 (Technical Malfunction) included at Appendix 7.
Roll-back Criteria 5.3. Appendix 8 contains an overview of the technical roll-back criteria which will
apply to any decision to roll-back to the existing PRM system. Partner Board engagement 5.4. Please refer to Appendix 9 for an overview of the Partner Readiness toolkit
and associated questionnaire. It should be noted that the Business Continuity Plan and Roll-back criteria will be shared with Partner Boards only once they have been approved by COPRG and by NHS 24 Board.
6. Service Performance 6.1. An updated service performance forecast, for the eight week period following
cutover, will be provided for consideration by the Board at its meeting of 4 October.
6.2. The latest forecast, produced in early September, is included at Appendix 10.
7. Clinical Supervision 7.1. Service Management are in the process of documenting the proposed clinical
supervision model. 7.2. The proposed model is included at Appendix 13.
8. Cutover Plan inc. Support Model 8.1. There are two aspects to this assessment: a) cutover plan and b) associated
support model. Cutover Plan 8.2. The draft cutover plan is included at Appendix 11 and will be subject to
ongoing review and finalisation in the lead up to go-live. A final version of the cutover run-book will be issued for review and approval by the NHS 24 Board or EMT prior to go-live.
Support Model 8.3. An overview of the proposed support model is included in Appendix 12. This
model is subject to further consultation with service management and staff-side and the final version will be presented to the NHS 24 Board at its meeting

NHS 24 GREEN
4
on 4 October for approval. Rostering staff into this model is a task which will be ongoing in the period beyond the NHS 24 Board meeting.
9. Technical Operating Model 9.1. The proposed model is included at Appendix 14.
10. Partner Board Readiness 10.1. The PAG met on 26 September and its report is at Appendix 15. 10.2. PAG may is seeking further information to support its assurance to NHS 24
and their report will be qualified accordingly.
11. Organisational Readiness
11.1. OAG met on 25 September and its report to the Board is included at Appendix 16.
11.2. OAG is seeking further information to support its assurance to NHS 24, and
their report qualified accordingly. is
12. Technical Readiness 12.1. TAG met on 20 September and agreed to meet again on 18 October in order
to close out its review of the Technical Readiness Checklist. 12.2. TAG's report to the NHS 24 Board is included at Appendix 17 and is qualified
accordingly. 12.3. The Information Security Risk Management and Accreditation Document
(RMAD) was completed in September 2016. The CIO has reviewed this document along with the Head of Information Governance and Security. No changes are proposed to the RMAD at this stage, noting that a review will occur with Capgemini and BT in early 2018 after T2 go-live and winter pressures.
13. Communication and Engagement Plan 13.1. A post go-live Communications and Engagement Plan is included at Appendix
18.
14. Summary

NHS 24 GREEN
5
The following table summarises the status of each decision criteria and forecasts the stage in the go-live governance process at which each criteria will be satisfied. Criteria NHS 24 Board 19 October System Functionality
• Team Leader and Technical Issues - • Clinical Governance Report -
Staff Readiness • Training Survey (complete) • Operational Validation Session - • Readiness Questionnaire
Training Completion Contingency Planning Service Performance Clinical Supervision - Cutover Plan inc. Support Model - Target Operating Model - Partner Board Readiness Organisational/Staff-Side Readiness Technical Readiness Communication and Engagement Plan -
NHS 24 GREEN
6
Appendix 1 – Go-Live Decision Criteria Criteria Evidence System Functionality 1. Model Office Team Leader feedback: Summary report, endorsed by group, describing process for resolution of
basket of issues identified with system functionality and associated work practices during T1. Referencing and appending four key documents:
a. Priority technical issues (12 priority issues) b. Priority 1 and 2 change requests c. Operating risks d. Action tracker from observation day (10 September)
2. Clinical Governance report, endorsed by Director of Nursing and Interim Medical Director, referencing feedback
from observation day (10 September), summarising the extent to which SAP application functionality provides appropriate clinical governance safeguards and describing risk mitigants and escalation processes.
Staff Readiness 1. Feedback from questionnaire issued to all trained, front-line staff prior to go-live, testing degree of readiness for the go-live event.
2. Face to face engagement with front-line staff at the Operational Validation event on 29 September. 3. Training completion feedback from staff surveys issued immediately post-training to assist in validating
responses to readiness questionnaire.
Training Completion 1. All staff must have completed training and had their competency signed-off prior to their first shift.
Contingency Planning 1. Business continuity/disaster recovery plan must be in place and approved by COPRG. 2. The above plan must include a specific T2 roll-back decision making process, again to be endorsed by COPRG. 3. Evidence to be provided that Partner Boards are familiar with relevant aspects of the Plan and roll-back criteria.
Service Performance 1. Board endorsement of go-live performance forecast for minimum eight week period post cut-over.
Clinical Supervision 1. Board endorsement of the operational support model developed by Service Management including assessment of readiness.

NHS 24 GREEN
7
Criteria Evidence Cutover Plan inc. Support Model
1. Board approval of the Cutover Plan and associated Support Model
Target Operating Model 1. Board approval of proposed operational model for Technology team post-handover of application to BAU.
Partner Board Readiness 1. Partner Assurance Group report
Organisational/Staff-Side Readiness
1. Organisational Assurance Group report
Technical Readiness 1. Technical Assurance Group report 2. Information Risk Management Accreditation Document (RMAD)
Communication and Engagement Plan
1. Board approval of T2 communications strategy
NHS 24 GREEN
8
Appendix 2 – Consolidated Tracker: Model Office Issues
Team Leader_Model Office Issues Tracker

NHS 24 GREEN
9
Appendix 3 – Clinical Governance Report NHS 24 26 SEPTEMBER, 2017 CLINICAL GOVERNANCE COMMITTEE ITEM NO. 1
ORGANISATIONAL IMPROVEMENT PROGRAMME (SAP IMPLEMENTATION TRANCHE 2) – CLINICAL GOVERNANCE AND ASSURANCE
Executive Sponsor: Director of Nursing & Care/Medical Director
Lead Officer/Author: Medical Director with multiple cross directorate
contribution from Senior Leads Action Required The Clinical Governance Committee is asked to note
this paper for assurance. Key Points This paper provides an update to the Clinical
Governance Committee regarding the safety aspects and processes for Tranche 2 (T2) go-live scheduled for 24 October 2017.This paper provides an analysis of service safety through a clinical lens and seeks to provide assurance that the national rollout will provide a safe, effective and person centred service to the people of Scotland.
Financial Implications The OIP Programme budget for 2017/18 has been set at £2.84m with double running costs of £5.171m also included.
Timing Timing of go-live is targeted for 24 October 2017 and is subject to ongoing review and assessment by the NHS 24 Board and its external and internal assurance groups.
Contribution to NHS 24 strategy
Successful delivery of the Organisational Improvement Programme (OIP) is central to NHS 24's strategy.
Contribution to the 2020 Vision and National Health and Social Care Delivery Plan (Dec 2016)
The introduction of the new technology platform enables a Better Health, Better Care, Better Value approach to the delivery of Health & Social Care.
Equality and Diversity An Equality Impact Assessment (EQIA) will be developed and will assess the impact of the new system implementation on Equality & Diversity.
1. RECOMMENDATION 1.1 It is recommended that the Clinical Governance Committee note the update on the clinical governance and assurance processes related to T2 planning and implementation. 2. ORGANISATIONAL IMPROVEMENT PROGRAMME (OIP) OIP Context

NHS 24 GREEN
10
2.1 The implementation of T2 is a priority work-stream within NHS 24's Operational Improvement Programme. Tranche 1 of the SAP application roll-out went live successfully for a single board (NHS Ayrshire and Arran) in May 2017 and followed the successful implementation of SAP telephony services to scheduled care service in late 2016. 2.2 Other service development projects within the OIP include:
• In hours GP Triage; • National Speak to Doctor; • Advanced Nurse Practitioner; • Mental Health; • Modernising Outpatients; and • Digital
2.3 Whilst the majority of the OIP Team's focus is currently on the roll-out of T2, planning and implementation of the remaining Operational Improvement Programmes is ongoing and will ramp up further in November once T2 implementation has occurred. These additional programmes have been subject to a business case which is for consideration by Scottish Government. Roll-back Criteria 2.4 T2 roll back criteria are in place, as they were for T1. The roll back procedures are embedded within existing technology and service management business continuity processes. Several workshops have been held with the Clinical Operations Process Review Group (COPRG) and service delivery to review the existing processes, ensure these adequately reflect the functionality of the new SAP system, and validate the roll-back arrangements. Roll-back and business continuity plans, endorsed by COPRG, are included within the go-live decision making criteria to be considered by the NHS 24 Board. Incident Tracker Update 2.5 The incident tracker is being monitored and reviewed on a weekly basis with both the Model Office team and the wider CSM group. This ensures all operational managers are aware of any issues being flagged through model office and solutions to address. 2.6 Technical input from Cap Gemini and Chief Information Officer has also ensured that any technical issues are validated to confirm whether they are genuine system issues or process issues. A session was held weekend of the 10th September to review with the Model Office team the issues arising through the tracker and identify any potential new issues; no new issues emerged from this session and it was also clear that a number of perceived technical issues were process related. Where this has become apparent, processes have either been amended or reinforced appropriately. Partner Assurance Update

NHS 24 GREEN
11
2.7 The Partner Assurance Group, chaired by the Deputy Chief Medical Officer and with members drawn from the National Out of Hours (OOH) leadership group, is the key external OIP assurance group focusing on clinical and partner board related matters. PAG's remit includes: 2.8 PAG provides assurance to the OIP Programme Board, the NHS 24 Board and the Executive Management Team that the implementation plan for the programme has been appropriately developed to address the broader risks and concerns of NHS Scotland in relation to the implementation of the system.
2.9 Specifically PAG provides review and assurance to the OIP Programme Board, the Executive Management Team and the NHS 24 Board on the following:
• that appropriate systems and processes are in place to monitor progress,
manage risks and to take corrective action in relation to Partner Board engagement in the programme implementation;
• validate the outcomes of "end to end" testing from the perspective of
Partner Boards and provide assurance thereon to OIP Programme Board, the NHS 24 Board and the Executive Management Team; and
• review and validation of the NHS 24 proposal for a phased implementation
and national roll out of the system from a Partner Board perspective. 2.10 PAG provided assurance to support the NHS 24 Board's decision to go-live with T1 in May 2017. 2.11 PAG has also been meeting monthly ahead of T2 go-live in October 2017. 2.12 At its most recent meeting, on 4 September, PAG identified that it needed answers to the following questions to allow it to provide assurance ahead of T2. Will staffing profiles and supervision models sufficiently support staff to deliver a safe service? 2.13 An enhanced level of support will be provided for up to 6 weeks post go-live and longer if needed. The support model mirrors the model used successfully for T1. 2.14 Over 100 support staff, made up of trainers and existing users of the new SAP application (from T1(Ayrshire and Arran) have been identified to support the call handling operations directly with the first line of support. This group will assist with issues relating to the use of the system, help users gain confidence when problems arise and engage technical support where this proves necessary. 2.15 This front-line support team will be supported 24/7 by a technical staff at each key contact centre and by a central control room where specialists from CapGemini, BT and NHS 24's technology and voice teams will be on hand to address technical issues. 2.16 An enhanced clinical supervision model will also be implemented in terms of numbers of staff, but the model itself will function as it does currently. Numbers of

NHS 24 GREEN
12
staff will be tailored to demand forecasts and to allow for need over cutover. This modelling is continuous and on an ongoing basis. Included in the supervision and support model will be some senior staff from Ayrshire and Arran whose expertise and visibility will further enhance the approach to supervising frontline activities and supporting staff post go-live. 2.17 Other important points to consider in terms support offered to staff to deliver services are:
• The extensive three day training package provided to all front-line and support staff and positive feedback from staff regarding this;
• Staff are being provided an opportunity to refresh their knowledge following competency sign-off during a 'keep warm' period prior to go live;
• That staff confidence is a criterion for go live; • Real- time engagement with staff in the model office environment in recent
weeks, to listen to their feedback, make enhancements to the SAP application and to processes as a result of this feedback including following a period of direct observation by senior colleagues.
Can NHS 24 be assured that technology is functioning as required? 2.18 The technology is stable and has been functioning successfully in the Model Office environment (Ayrshire and Arran ) for over four months.
2.19 Prior to and subsequent to T1, there has been extensive testing of the technology, including with Partner Boards, and the Technical Assurance Group (TAG) will assure NHS 24 Board on key aspects of this again prior to T2. 2.20 Assurance on specific areas identified by OOH partners in 2015 and still relevant to PAG is detailed below
• The revised clinical summary format has been successfully running in Ayrshire and Arran since May with positive feedback;
• Safe cross-boundary management of patients - the new method in SAP of connecting a patient to a GP removes the issues of GPs working across boundaries as NHS 24 connect the patient to the correct practice/GP combination as the surgery is selected first then the GP;
• Holding area - there is a clearer understanding of the management of this function and which will be demonstrated to NHS 24's partners on the 29th of September during the proposed Operational Validation event;
• End to end testing is being performed with all Partner Boards; • A Partner Board assurance check-list has been drafted which reflects the
information which must be provided back to NHS 24 in mid October to offer assurance of the readiness of NHS 24's key stakeholders; and
• Clinical content provided to frontline staff - there is no current indication of outlying content behaviour, however there will be continuous monitoring of this over the go-live period, with a specific plan being developed to work with colleagues to ensure the content does not place excess or inappropriate demands on partners.

NHS 24 GREEN
13
Communication with partners at the go live date and cutover period 2.21 NHS 24 has undertaken a significant stakeholder engagement with its OOH partners and across social care as well as third sector and voluntary agencies. The readiness of partners is integral to the successful delivery of this aspect of the OIP. Our Partner Board information-toolkit will detail what the partners can expect from NHS 24 through the cutover period. Communications have commenced with stakeholders and will continue in the lead up to go-live and for the period of enhanced cover post go-live. Escalation processes and criteria for roll-back 2.22 It is important to emphasise that the current technology is in the last stages of its life span and that moving to the new technology platform will place us in a more resilient and safer space. To switch on the new technology and then revert back to the PRM system would be an exceptionally high risk strategy. This has been acknowledged by the TAG and key risks and mitigations will be reviewed as part of TAG's final assurance review. 2.23 NHS 24 had a Board approved business continuity plan, escalation processes and roll-back criteria for T1. These have recently been reviewed by the Medical, Nursing and Care Directorate (including Interim Medical Director, Head of Clinical Governance and Quality Improvement, Associate Director of Nursing and Operations, Risk and Resilience Lead and Chief Information Officer) and have been deemed by that group as being fit for purpose for T2. 2.24 The patient safety matrix elements of the plan, which were agreed with the OOH National Operations Group and reported to PAG prior to T1, are now part of the service management and business continuity processes and will be used in T2. 2.25 Service management processes have been refreshed in the past two years and have been demonstrated to the NHS 24 Board and Non Executive Directors in the past year. This an agile set of processes which maintain the safety of patients who are trying to access the service and those who are already captured within NHS 24's processes. Real-time data monitoring allows staff to be moved responsively to manage demand and maintain key performance indicators. 2.26 NHS 24 is undertaking very significant regular planning sessions and workshops to match forecast demand to resource placement. 2.27 As a result of careful planning and service management processes, we currently have no patient safety incidents, the Priority 3 call response times have improved and there has been a reduction in complaints received. 2.28 To monitor NHS 24 outputs we have the enhanced capability in the new application to look at screen recordings to see how users are navigating the system. We can refine the application accordingly if there is an observed need i.e. NHS 24's monitoring and measurement of safety is now enhanced and is even more auditable. How are we working with Scottish Ambulance Service (SAS) in planning for go-live of T2?

NHS 24 GREEN
14
2.29 Regular meetings are occurring with NHS 24 and SAS and are informed by detailed forecasting and planning meetings. Operational Improvement Programme Clinical Risks 2.30 The 111 risk register was reviewed on 19 September by operational, resilience and risk leads. There are currently no clinical risks on the register felt to be a risk to T2 go live.
2.31 The OIP risk register has been reviewed and the outstanding risks are at an amber status and reducing in score progressively. None of these risks are felt to represent a clinical risk at this time to T2 as they are on track to be achieved within timelines and will be continuously monitored. Resource Escalation Action Plan (REAP) and potential use at T2 2.32 Resource Escalation Action Planning is a model of escalation and assessment of risk, it uses a joint decision model to assess level of risk and actions to be taken. Work continues to explore the development of a REAP model in conjunction with existing tools, e.g. the Service Management Process and Patient Safety Matrix, to support NHS 24 in defining and understanding service management pressure points, mitigation and escalation as well as understanding associated roles and responsibilities. 2.33 Senior organisational leaders have agreed that this is not a model that is ready to be applied to or inform the T2 go-live process. Adding a new layer into the go-live process at this point may not be helpful and potentially could disrupt current planning. It is proposed that a further work stream will be implemented to ensure that that REAP is adopted within NHS 24, it is suggested this work commence post T2.

NHS 24 GREEN
15
3. Appendix 4 – Staff Training: Survey Feedback at Week 5
Did you find the training session effective, useful and informative (i.e. did it meet your objectives)?
Total Yes No % Yes % No 282 258 24 91% 9%
In terms of delivering the content, the quality of how it was delivered, how it was communicated and the support that was offered throughout the programme, how would you rate the performance of the trainers?
Total Highly
Effective Effective Not Effective Not Effective at all
269 104 156 8 1
39% 58% 3% 0% How confident do you feel in navigating the integrated applications in line with your role?
Highly Confident Confident Not Confident Not Confident at all
Total 268 18 189 57 4
% 7% 71% 21% 1%
0
10
20
30
40
50
60
70
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7
Who has attended training?
Team Leader Call Handler Nurse Practitioner CSM SCH

NHS 24 GREEN
16
0
5
10
15
20
25
30
35
40
45 M
ore
Tim
e
Less
Tim
e
elea
rnin
g in
tera
ctiv
e sim
ulat
ion
Grou
p di
scus
sion
Nar
rate
d Sy
stem
Ove
rvie
w
Proc
esse
s
Reco
rded
Cal
ls
Trai
ning
syst
em s
cena
rio p
ract
ice
Sim
ulat
ed W
orkp
lace
Env
ironm
ent
Wou
ldn'
t Cha
nge
Anyt
hing
Would you change anything about the training to enhance the learning experience, please give details?
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7

NHS 24 GREEN
17
Appendix 5 – Staff Readiness Survey Questions 1. Job Role
o Call Handler o Nurse o Team Leader o Senior Call Handler o Clinical Services Manager o Service Delivery Analyst o Dental o Clinical Governance o Health Information Services o Other, please specify
2. I feel able to handle a patient call using the new system in a supported
environment
o Definitely Agree o Tend to Agree o Tend to Disagree o Definitely Disagree
3. I have awareness and understanding of where I can access the Phase 2 processes utilised during my training to support my practice.
o Definitely Agree o Tend to Agree o Tend to Disagree o Definitely Disagree
4. I am able to use the SCC/CDT telephone as a standalone application in the event of an IT malfunction.
o Definitely Agree o Tend to Agree o Tend to Disagree o Definitely Disagree

NHS 24 GREEN
18
5. I have sufficient knowledge at this stage in my ability to troubleshoot common system issues.
o Definitely Agree o Tend to Agree o Tend to Disagree o Definitely Disagree
6. I feel that the organisation has provided me with sufficient time/opportunity to build my confidence to operate the new system within a supported environment
o Definitely Agree o Tend to Agree o Tend to Disagree o Definitely Disagree
7. If you have disagreed with any of the statements above please detail why? 8. Any additional comments?
Comments
Comments

NHS 24 GREEN
19
Appendix 6 – Contingency, communication and escalation plan [Awaiting finalisation following COPRG 29 Sept]

NHS 24 GREEN
20
Appendix 7 – Process 28 (Technical Malfunction) [Awaiting finalisation following COPRG 29 Sept]
NHS 24 GREEN
21
Appendix 8 – Roll-back criteria
15. INTRODUCTION 15.1. The technical solution will be assessed for final readiness to deploy across all
health boards by the Technical Assurance Group (TAG) at the next scheduled session on 18th October 2017.
15.2. As part of the system readiness assessment, a document was produced detailing the expected timings for key system transactions. These expected timings give an objective reference for expected and acceptable system performance measurement. See Attachment 1 to this paper for this benchmarking document.
15.3. In situations where technical malfunction creates unacceptable performance
impacts over a prolonged period, a decision may be taken to revert (or "roll-back") to using the legacy PRM system.
15.4. This paper provides the criteria and guidance for roll-back decision making.
16. PERFORMANCE 16.1. The system performance metrics (Attachment 1) provide the benchmark to
determine if the SAP solution falls below an acceptable level. These metrics will be used as part of expected performance monitoring and to inform any roll-back consideration.
16.2. Service performance may be affected by a number of other non-technical
factors and this performance will be monitored and assessed through other measurement tools [reference]. If the service performance falls below expected levels due to non-system issues then current business continuity processes would be followed.
16.3. For the avoidance of doubt, poor service performance due to non-technical
issues alone will not invoke the roll-back protocol.
17. ROLLBACK DECISION CRITERIA 17.1. In the event of unexpected issues that require the system to be taken offline,
there is a maximum amount of time that the service can be managed by the business continuity process.
17.2. Service delivery can be maintained through the business continuity process for
up to 48 hours at weekends and for up to 72 hours on weekdays.
17.3. There is an escalation process in place which will use the rollback decision criteria as guidance for decision making. Whilst the system downtime duration

NHS 24 GREEN
22
has been quantified, the decision making process will take into account other factors especially the ‘expected time to fix’ where there may be some tolerance of boundaries. The escalation process will be walked through as part of a ‘desk top’ exercise to ensure that all key stakeholders and participants are clear on the process and expectations. This exercise will also confirm the practical components required for go live.
17.4. The table below outlines the decision making process should there be
technical issues that affects the SAP system performance. Downtime constitutes either the system being completely unavailable or the impact of technical failure rendering performance unacceptable.
Cause Solution Time to Fix
System Down < agreed downtime
System Down >= agreed downtime
1 Unknown Unknown Unknown Continue diagnostics with review points within agreed downtime window
Invoke rollback protocol
2 Known Unknown Unknown Continue diagnostics with review points within agreed downtime window
Invoke rollback protocol
3 Known Known Unknown Implement fix if completion time due within agreed downtime window
Invoke rollback protocol
4 Known Known Known Implement fix if completion time due within agreed downtime window
Seek extension to continue Invoke roll-back protocol if rejected
18. CONSIDERATIONS 18.1. Moving the service to the business continuity process is very disruptive and
time consuming. Should the decision be taken to move the service from the new SAP technical system and on to the manual process whilst a technical issue is being resolved, great consideration should be given to when the service is moved back onto the SAP system following the technical resolution. It is better for service delivery to wait until the resolution is clearly proven which will reduce the risk of having to return to the manual process in the event of the issue not being fully resolved.

NHS 24 GREEN
23
18.2. Transferring the service to a manual process has an impact on partners. This would mean that partners would have to manage additional workload and backlog. This is currently the case for business continuity.
19. ESCALATION PROCESS 19.1. The criteria and proposed outcomes within this paper will support the decision
making as part of the approved contingency, communication and escalation process.
Attachment 1 (to Appendix 8) – System Performance Benchmarks
Test Completion Report.pdf

NHS 24 GREEN
24
Appendix 9 – Partner Board Readiness Toolkit Refer Embedded PDF File
Partner Readiness Toolkit.pdf

NHS 24 GREEN
25
Appendix 10 – Potential Impact on Calls Answered within 30 Seconds The table below sets out the predicted weekly service level performance range for the 8 weeks inclusive of go live. For each week an upper, mid, and lower-range projection has been included based on the following factors: Lower:
• Demand 5% over forecast; • AHT consistently above Model Office to reflect the scale of implementation
nationally. Upper:
• Demand as forecast; • AHT in line with Model Office experience.
Mid:
• Demand 2.5% over forecast; • AHT in line with Model Office experience.
W/C Date Upper Mid Lower 23/10/17 48.7% 46.1% 36.7% 30/10/17 60.9% 57.0% 38.4% 06/11/17 57.6% 54.3% 42.9% 13/11/17 45.9% 44.3% 35.3% 20/11/17 91.9% 89.1% 67.5% 27/11/17 79.7% 79.7% 73.4% 04/12/17 78.0% 78.0% 69.0% 11/12/17 78.3% 78.3% 68.7%
Factors affecting service levels:
• Throughout the training period, demand has consistently outstripped forecast. This is a pattern that was not evident prior to the training and one we would not expect to see continue once training has been completed. This is reflective of the reduced capacity on the floor throughout the training period, which has caused some increase in abandonment rates and redial behaviour. So, whilst we have factored this into both the lower and mid-range forecasts, we would expect to see demand levels in line with forecast assumptions as we cutover.
• In all scenarios, 10% shrinkage has been factored in to accommodate dynamic service management, for example, for additional rapid triage capacity above normal modelling assumptions. Again, this is additional flexibility within the capacity planning, that helps maintain clinical performance for call back.
• The table below shows the P1, P2 and P3 call back performance throughout the training to illustrate the continued focus on maintaining clinical performance despite the predicted impact on access service levels as a result of reduced capacity throughout training.

NHS 24 GREEN
26
Week ending % P1 % P2 % P3
Calls answered within 30 seconds
27-08-17 100.0% 97.3% 87.4% 51.2% 03-09-17 100.0% 100.0% 94.1% 54.4% 10-09-17 100.0% 100.0% 80.1% 49.3% 17-09-17 100.0% 100.0% 93.9% 67.8% 24-09-17 100.0% 100.0% 84.5% 49.1% 01-10-17 100.0% 99.9% 88.7% 57.4%
• Final scheduling of the clinical supervision and support models will allow CRT
to specify the individual names, and associated shifts, into the projections. At this stage, the requisite number of heads has been removed from the modelling but this may be disproportionately affecting certain shifts more than others; our experience is that once the actual staff shifts are modelled there is a positive impact on service levels but this work is still to be completed.
• Whilst the service levels above are modelled weekly, it is acknowledged that there is variation across the weeks, not least in terms of variation between week days an weekend. To mitigate against this, additional hours will be offered, with a targeted focus on weekends, notably in the first 4 weeks of cutover. This will be a rolling process where additional hours are sought 4 weeks in advance. As such, the daily performance projections will be subject to change, however, this would be a projected increase in performance as a result of additional capacity on shift where available.
• Consideration is also being given to the IVR messaging that could be available to service delivery in the event of continued significant variation in demand forecasts in order to manage public expectations on call back times and minimise redial behaviour and consequent demand inflation.
• A detailed communication and engagement plan has been developed to ensure routine and continuous engagement with NHS Boards throughout cutover. This will include a daily discussion with SAS to review the level and appropriateness of 999 calls and quickly identify and address any potential issues.
The detailed modelling across a number of scenarios is being reviewed weekly by a sub-set of NHS 24 Board non-executive directors. This group will review the final set of projections once the support model is finalised ahead of the final go live decision by the Board.
NHS 24 GREEN
27
Appendix 11 – Cutover Plan See embedded PDF File
Cutover Plan.pdf

NHS 24 GREEN
28
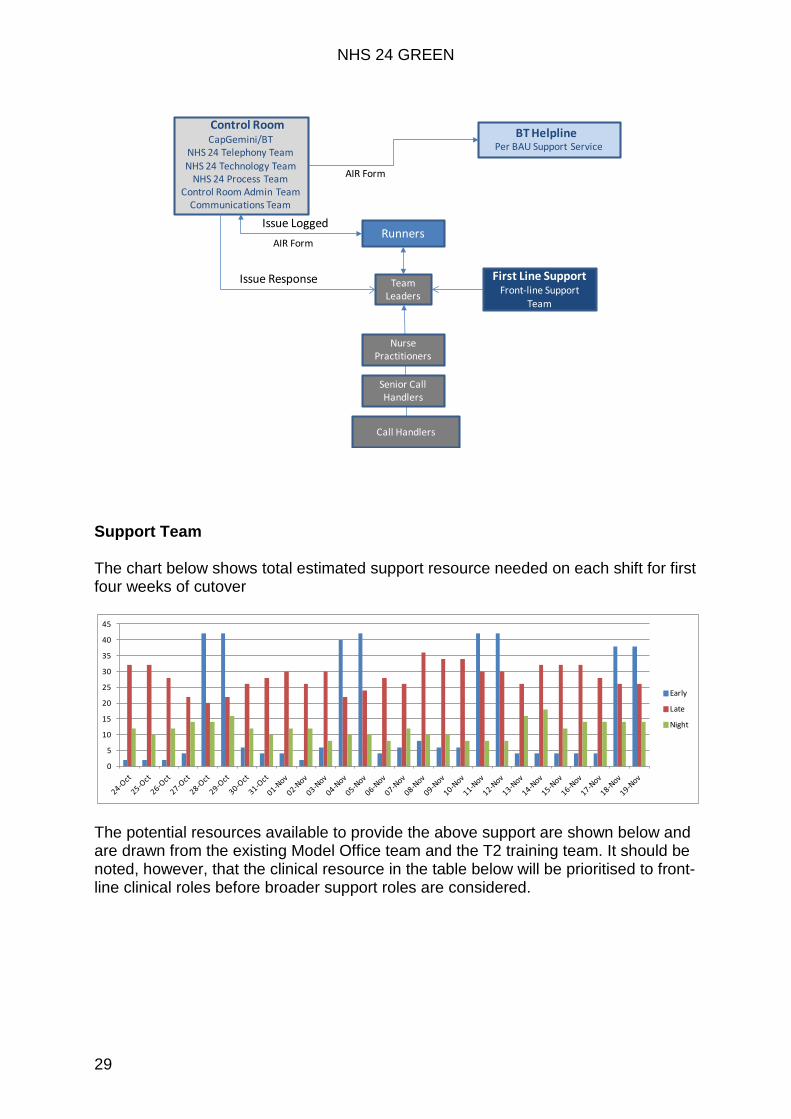
Appendix 12 – Support Model Overview Key Principles
• Front-line staff must be able to focus their efforts on helping patients without distraction
• Support services will be enhanced but no material change to BAU processes for front-line staff
• Enhanced support levels will persist for up to six weeks with a minimum of four weeks
• A central technical support control room will be located in Clyde • Runners will pass messages to and from the front-line contact centres and the
central control room • A dedicated support email address and mobile phone number will also be
provided to all Team Leaders and Partner Boards Model Summary The proposed support model replicates successful support model for T1 but at scale
The model uses a three-line support approach as shown in the diagram below, with the emphasis on triage of issues on the call handling floor, with escalation to the control room where technical support is needed. In order to ensure appropriate triaging of technical issues, there will be a technical lead at each centre to support the CHC support team. Staffing of the control room will be identical to staffing during T1, however in the early stages of cutover CapGemini will be providing specialist technical resource to the control room, with this resource typically based at CapGemini's HQ, supporting the incident management team in the control room.
NorthCHC Support Team
Technical Lead
ClydeCHC Support Team
Control Room
CardonaldCHC Support Team
Technical Lead
EastCHC Support Team
Technical Lead
Partner Boards
•One West centre for nightshift•Central resource for Variation
Tracker/Holding Area•Two CHC support personnel per
Pod
CHC= Call Handler & Clinical
Local CentresCHC Support Team
BAU
NHS 24 GREEN
29
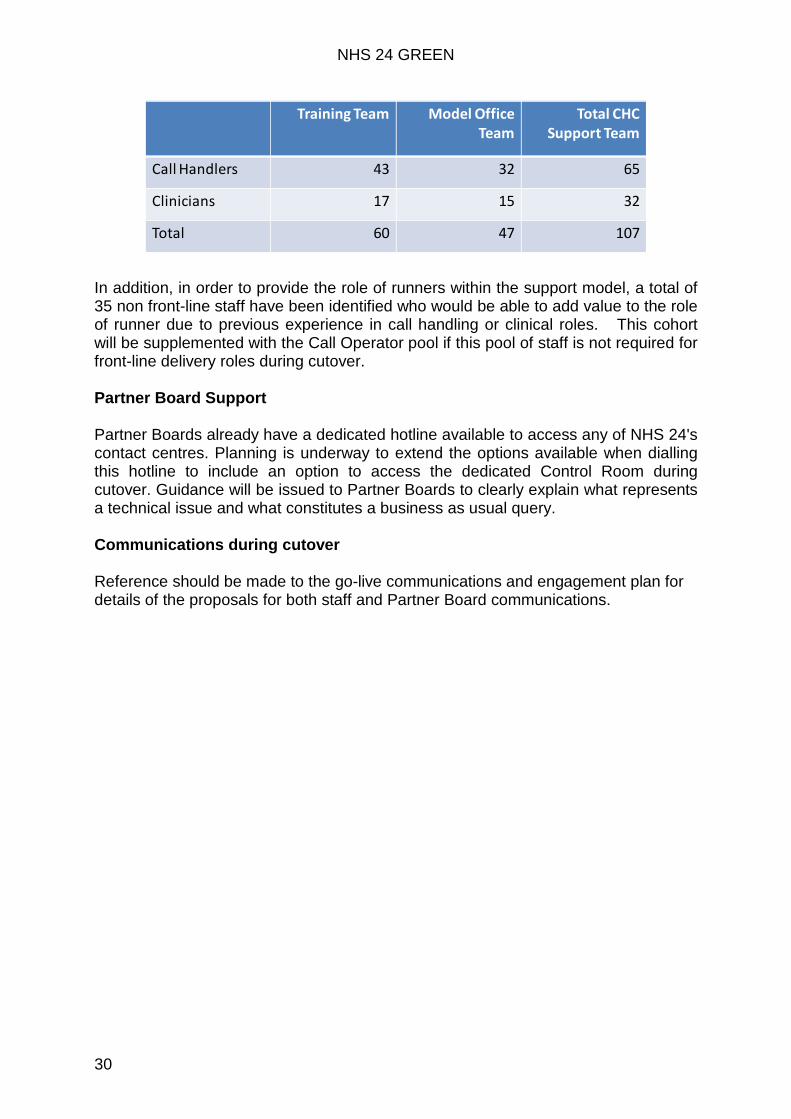
Support Team The chart below shows total estimated support resource needed on each shift for first four weeks of cutover
The potential resources available to provide the above support are shown below and are drawn from the existing Model Office team and the T2 training team. It should be noted, however, that the clinical resource in the table below will be prioritised to front-line clinical roles before broader support roles are considered.
AIR Form
Call Handlers
Senior Call Handlers
Nurse Practitioners
Team Leaders
First Line SupportFront-line Support
Team
Runners
Per BAU Support ServiceCapGemini/BT
NHS 24 Telephony TeamNHS 24 Technology Team
NHS 24 Process TeamControl Room Admin Team
Communications Team
Control RoomBT Helpline
AIR Form
Issue Logged
Issue Response
0
5
10
15
20
25
30
35
40
45
Early
Late
Night
NHS 24 GREEN
30
In addition, in order to provide the role of runners within the support model, a total of 35 non front-line staff have been identified who would be able to add value to the role of runner due to previous experience in call handling or clinical roles. This cohort will be supplemented with the Call Operator pool if this pool of staff is not required for front-line delivery roles during cutover. Partner Board Support Partner Boards already have a dedicated hotline available to access any of NHS 24's contact centres. Planning is underway to extend the options available when dialling this hotline to include an option to access the dedicated Control Room during cutover. Guidance will be issued to Partner Boards to clearly explain what represents a technical issue and what constitutes a business as usual query. Communications during cutover Reference should be made to the go-live communications and engagement plan for details of the proposals for both staff and Partner Board communications.
Training Team Model Office Team
Total CHC Support Team
Call Handlers 43 32 65
Clinicians 17 15 32
Total 60 47 107

NHS 24 GREEN
31
Appendix 13 – Clinical Supervision Model The key principles supporting the enhanced clinical supervision model during the cutover period are outlined below:
• Enhanced T2 service management plan for six week cutover period;
• Duty Clinical Service Manager (CSM) and Deputy CSM cover for six weeks including midweek nightshifts for first two weeks (typically only one Duty CSM per shift);
• Senior Service Delivery (SD) on call rota and location of SD senior team
optimised across the first two weeks, [with emphasis on enhanced cover for busy backshift, night shift and weekends.
• Consolidate supervision and enhance control by closing Clyde and merging
operations with Cardonald for all night shifts during six week cutover period – noting 2/3rd of staff are based in Cardonald.
• Clear plan and lines of communication for Local and Remote Centres in terms
of support and supervision with a CHC support team member in the centre if there’s not a nurse on shift with enhanced SAP knowledge.
• If single nurses are rostered on shift at local or remote centres they will they
be asked to attend Regional centre for supervision (unless they are a member of the train the trainer pool and are happy to stay).
• Holding Area – will be managed centrally, from Norseman, which is the
optimal location due to the fact that the clinical queue is normally based there and the expertise in prioritisation lies with that team leader group.
• This approach mirrors business as usual arrangements where particular roles are centralised as the service is managed on a National basis. In the main the hub function also runs from Norseman so the SDAS have a clear picture of the call flow and what is in the clinical queue to enable them to load balance to meet our clinical KPIs.
• Holding Area management resource required for each shift has been identified including subject matter experts from Model Office, who will support Team Leaders in the East. All team leaders have been trained in the Holding Area and have been regularly prioritizing from the East throughout our live period in Model Office.
• Variation Tracker will be managed centrally. Currently the queue coordination
role runs centrally from Cardonald and because the roles within the variation tracker are similar and some the same as queue co ordination, the expertise and experience including the skillsets required are based in Cardonald
• Variation Tracker management resource will include one Team Leader, one Senior Call Handler and three call operators per shift.

NHS 24 GREEN
32
• Rapid Triage will be managed centrally. Rapid triage in BAU is usually based
in the West with other centres complementing them when resource allows. Due to automation of outbound calling in the new application it is important that Rapid triage is run from only one site as the process involves the removal of automation thus it is critical that the selection of calls is monitored closely to ensure NHS 24 meets its clinical KPIs.
• Rapid Triage team will be based in Clydebank, resource required is 15 Call Handlers, two CHC support personnel, three Nurse Supervisors.
• Seasonal Initiative (SI) runs from Cardonald in BAU and all CHs are trained in this process with specific clinicians trained to supervise. Currently the protocol is on paper whereas in the new application it is embedded in PCM. Staff have been moved from Cardonald to the model office at Clydebank to ensure the calls flow in the way expected. Resource identified per shift to supervise SI is two CHC support, 15 Call Handlers and three Nurse Supervisors.
• Supervision plan for on floor/support lines by centre requires a ratio of 2:15
consisting of 1 x CHC Support and 1 x Clinical Supervisor.
• NHS 24 always has clinical team leaders on all operational floors where there are call handlers. The team leader provides face to face supervision as well as physically taking over calls where required.
• Clinical team leaders also provide clinical support for child protection, vulnerable adults etc. The clinicians on support lines will ask three questions of the call handlers then either take the call over, give advice or advise the CH to queue the call.
• SCH s on duty do not give any clinical advice or supervision. Their role is to manage and support the staff ,answer sick phones and general partner queries, ensure adherence to process, adherence to breaks etc and generally people management.
• During cutover, we are enhancing in particular our face to face support as in times of high stress this model of supervision is preferable, however, we recognise that due to our national staffing model and local management model we will require the support lines to be operational.
• Operational partner engagement at cutover will be the role of Senior Call
Handler. A SCH will be assigned within each centre to take calls via the new Partner Board contact number, with an IVR message to direct partners straight to the control room if the matter is of a technical non patient facing nature.

NHS 24 GREEN
33
Appendix 14 – Technical Operating Model
INTRODUCTION Following the successful implementation of the SAP system in T2, an operational support capability must be in place to provide support on going. Initially, when the programme was first established, a ‘SAP Competency Centre’ was proposed however, following contract negotiations detailing NHS 24 responsibilities and those of BT and Cap Gemini, this specific function is no longer required. This paper provides the details for the roles and functions that will support the user community and technology for the SAP system post go live.
CURRENT MODEL
Ayrshire and Arran Board (A&A) have been live with SAP since 16th May and being supported by NHS 24, BT and Cap Gemini. This support covers system issue management, software support as well as change management for both the telephony and the application. SAP account administration is the responsibility of NHS 24 Technology. There are currently two administrators in place supporting A&A as well as T2 activities.
Telephony support and change management is performed for both the current Avaya system and the SAP system.
Avaya is supported by NHS 24 for change and support Avaya is supported out of hours by NHS 24 Technology The telephony element of SAP system by Cap Gemini.
The User Reference Group is currently in place to feedback issues, concerns and proposals regarding the SAP system into the OIP Programme.
PROPOSED MODEL Expansion of the A&A support model, in which A&A have been successfully supported with since 16th May 2017, will be implemented as part of the cutover and will become the support model post go live. This will be a single support and change process for all boards using the SAP system. This support covers system issue management, software support as well as change management for both the telephony and the application. Post go live, the cessation of the T2 SAP admin activities will provide the capacity required for the remaining boards.
The Avaya telephony system, currently supported by NHS 24, will be decommissioned.
Telephony support and change management will be provided by Cap Gemini. This will include all out of hours support.

NHS 24 GREEN
34
The User Reference Group will continue with an agreed new terms of reference and will provide the two way feedback for SAP system issues, changes and performance reviews.
SUMMARY The table below shows the current and proposed operating model responsibilities.
Post T1
Post T2
Comment
SAP Administration NHS 24 A&A only
NHS 24 Two SAP administrators recruited within Technology
SAP Issue Resolution
Cap Gemini Cap Gemini All SAP system issues will be logged via BT and resolved by Cap Gemini
SAP Telephony Cap Gemini Cap Gemini Minor changes not affecting any configurations will be undertaken by NHS 24 Technology
SAP Changes Cap Gemini
NHS 24
Cap Gemini
NHS 24
The change management process will be owned by NHS 24 Technology. Clinical content changes will be provided by CDT The actual changes to content and function will be performed by Cap Gemini
AVAYA Administration
NHS 24
BT
NHS 24
BT
Within the decommissioning plan, AVAYA is scheduled to be decommissioned by the end of December 2017 BT to provide support until decommissioning is complete
AVAYA Issue Resolution
NHS 24
BT
NHS 24
BT
Within the decommissioning plan, AVAYA is scheduled to be decommissioned by the end of December 2017 BT to provide support until decommissioning is complete
AVAYA Changes NHS 24
BT
NHS 24
BT
Within the decommissioning plan, AVAYA is scheduled to be decommissioned by the end of December 2017 BT to provide support until decommissioning is complete

NHS 24 GREEN
35
Appendix 15 – PAG Report [Awaited from PAG Chair]

NHS 24 GREEN
36
Appendix 16 – OAG Report
INTRODUCTION This paper presents a summary of the assurance obtained by OAG in the lead up to the proposed go-live date for Tranche 2 (T2) of the SAP application in October 2017.
TERMS OF REFERENCE OAG's Terms of Reference were agreed on 18 January 2017. Key aspects of OAG's remit can be summarised as follows:
• Assurance over the development and resourcing of the plans supporting the overall delivery of the OIP including appropriate monitoring of programme status and risks;
• Expert advice and assurance in relation to the execution of the OIP and specifically the staff readiness aspects of the programme;
• Challenge and support to the cultural change and capability elements of OIP;
• Engagement with partnership representatives as appropriate.
MEETING DATES The OAG met on the following dates in 2017:
• 18 January • 26 July • 13 April1 • 28 August • 22 May • 25 September • 26 June
APPROACH In carrying out its remit as identified in section 2, OAG has considered the following six issues as of primary importance to supporting its conclusions.
• Quality and quantum of training provided to staff; • Ability to keep staff "warm" prior to go-live and post training; • Staff Communication and Engagement; • Learnings from Tranche 1; • Partnership working – with specific focus on involvement of staff-side in
planning and decision making; and • Programme reporting and management.
1 Briefing session with Chair of OAG prior to Tranche 1 go-live

NHS 24 GREEN
37
This summary report highlights our assessment of each matter and our overall conclusions. We believe this assessment and our conclusions provide NHS 24 at this stage of the implementation process with the assurance it seeks in line with our remit and are happy to discuss any aspect of this with NHS 24 colleagues as necessary. Quality and quantity of training OAG noted that a three-day training session was developed for T2 and that this created some concern among staff given the training for T2 was spread over four days. OAG has been given assurance that the three-day training model has been appropriate and delivered the necessary level and quality of training to staff. Our confidence in the training delivered is based on the following understanding:
• The three day training course is almost identical to the four day course but uses external and volunteer "patient callers" to provide practice calls into the training environment, thus avoiding the need for trainees to call each other during training, saving significant time;
• Staff-side colleagues were involved at an early stage in planning the new model;
• Feedback from staff, obtained through formal surveys, the highlight results were presented to OAG, were very positive regarding the quality of the training and, while there was feedback from a number of staff stating they would have liked "more time" to train we believe this is not related to the change in course duration as the content is almost identical. Rather we think this reflects previous staff experiences of difficulties with failed go-live attempts and the associated nervousness as a result regarding the launch of the OIP ;
• Feedback from trainers themselves, again sought through formal surveys and presented to OAG, have been very positive.
Ability to keep staff "warm" pre go-live and post training Survey feedback clearly shows a desire from many staff to have the opportunity to maintain the knowledge gained from training in the period before go-live. This need is likely to be most acute in staff trained early in the training programme (Clyde, East, North based staff). OAG has been given assurance that actions have already been taken and plans are being put in place to support keep warm activities based on its understanding of the following:
• As of 22 September, all staff who have requested access to the ‘keep-warm’ had been rostered into two-hours of off-line time in order to undertake e-learning via specially designed e-learning modules which support and build on the training received; and
• In addition NHS 24 Executive Management Team (EMT) has endorsed a proposal to offer all staff two hours of paid additional time to undertake "live" practice sessions out of their normal hours in the two week period immediately prior to go-live.
NHS 24 GREEN
38
OAG will seek further information from NHS 24 regarding the feedback from staff and staff-side colleagues on the success of these initiatives prior to finalising its assurance to NHS 24. Staff Communication and Engagement OAG is briefed on the approach to communications and engagement by the OIP Programme Director at its monthly meetings, and also attended the validation session for T1 with some OAG members attending the same session for T2 (29 September). OAG also notes the feedback obtained from recent roadshow events across all key regional and local contact centres and notes that a second series of roadshows commenced on 21 September to brief staff on the keep warm activities and proposed go-live support model. Ultimately, staff communications and engagement activities are intended to provide staff with information to build confidence ahead of go-live. The ultimate test of the success of the approach taken will be in responses to the staff readiness questionnaire to be issued in the fortnight prior to go-live. OAG will be interested in the responses to this questionnaire ahead of finalising our assurance report.
Learnings from Tranche 1 The approach to training and readiness activities has been built on the success of the T1 go-live event in mid-May 2017. OAG representatives attended the pre go-live validation event on 20 April and spoke with staff regarding the approach to training, communication and readiness planning. OAG been given assurance that the planning for T2, specifically in relation to training and support logistics (including planning of trainer numbers, staff attrition rates, on the floor support at go-live and support logistics) has been evidence based using the learnings from T1. The T2 validation session on 29 September provided further assurance that lessons had been learned from the experience of T1 and that the training had been well received by staff. . The success of T1 allowed the Model Office concept to be tested more fully prior to T2 go-live. OAG acknowledges feedback from the Programme Team and staff-side representatives that the development of Model Office test and learn activities to the desired extent has been compromised by the intensive planning and delivery of T2.
However, OAG is assured, having reviewed the Model Office issues tracker at its meeting on 25 September, that significant steps have been taken to engage with Model Office training staff and that the results of this engagement are being used to benefit and de-risk T2 go-live. OAG also notes feedback from an individual Team Leader in Model Office (21 September) in email communication to the programme team that "we have all worked towards a common goal and the feedback of every member of the team has been valued". We take this as a positive indication of the

NHS 24 GREEN
39
learning approach deployed while acknowledging that it comes from a single team leader. There was recognition at the T2 validation day on 29 September that staff acknowledged that there was a need now to go live with the new system and that there had been a significant shift in the mind-set of staff that this was a reality. Management acknowledged that this was creating some anxiety for a proportion of staff and that positive communications and engagement over the period up to go-live and beyond would be very important. The level of both clinical and technical support in place to support the 6 week switch-over period at go-live will be crucial to reassure staff that they will be supported if any concerns and issues arise. The OAG is keen to be assured that the levels of support will be in place over that period.
Partnership working OAG has been given assurance that staff-side representatives have been involved in the planning and delivery of the programme for T2. Specifically, OAG notes that staff side representatives were invited onto the work-stream project teams for each of Technology, Training and Logistics and Communications and Engagement. Consultation has also occurred with the Area Partnership Forum (APF) on a monthly basis and the User Reference Groups which met in July and September 2017 reported in to the APF for further assurance. OAG is also aware from staff-side representatives that the Programme Director and/or senior representatives of the Programme Team have been represented at almost every Regional Partnership Forum in the period April to September. OAG's core assurance comes from the report from NHS 24 staff-side representatives which is appended to this final report prior to the NHS 24 Board making its final go-live decision.
Programme Management and Reporting OAG has noted that the approach to programme delivery has been centred around the fact that the success of the programme will depend on the approach to people and engagement just as much as it will to technology implementation methodologies. The work-streams that support the programme (Technology, Training and Logistics, Communications and Engagement) clearly show a significant balance of resource and effort goes into the "softer" elements of the technology implementation programme. In addition, the use of staff surveys, roadshows, video and social media and more traditional forms of communication such as the Team Talk newsletter and email

NHS 24 GREEN
40
communication provides further reassurance that the appropriate effort continues to be placed on people and culture as well as technology readiness. OAG also acknowledges that reporting to OAG has been based on the same information supplied to NHS 24's EMT and the NHS 24 Board and meetings have been characterised by open, honest and frank discussions regarding the very significant challenges that this programme has faced and continues to address.
Interim Conclusions Overall OAG has been assured by the development and resourcing of the plans supporting the overall delivery of the OIP including appropriate monitoring of programme status and risks and specifically staff readiness ahead of implementation. We further acknowledge the level and openness of the engagement between OAG and the programme team throughout the assurance process. Whilst providing reassurance of the adequate level of clinical and technical support will further minimise the risks associated with the full implementation of the OIP, we are of the view that there remains the possibility that implementation does not go as smoothly as planned. However, we believe that taking this next step at this stage in the process is merited. We are of the view that a bigger risk to both the success of the programme and ultimately patient safety lies in implementation being delayed until the next feasible period which would be spring 2018. As such we are assured that full implementation should proceed on the 24 October go live target date. A major theme in the development of the implementation plan has been how to help bring about organisational cultural change, in particular in relation to staff and management engagement. The post implementation period will be crucial to achieving such longer term change. We hope the level of engagement evident in the development and implementation of the OIP will mark a turning point in the process and its successes can help build the wider change sought by NHS 24.
Outstanding Matters The following outstanding matters will be assessed by OAG prior to finalising this report to support NHS 24's final decision on go-live in the lead up to the 24 October go-live target date.
• Feedback on keep-warm activities; • Staff readiness survey results from mid October; • Confirmation of the clinical and technical support model and staffing for go-
live and the 6 weeks thereafter; and • Staff-side report.
Matters to be taken forward post implementation During the course of this assurance process, the OAG has been made aware of issues which, due to the pressure of the preparations for the go-live date, have not been resolved/taken forward.

NHS 24 GREEN
41
The OAG believe that benefit would be accrued if the following issues were progressed and resolved:
• Lessons from model office – team based working etc • Review of shift patterns
NHS 24 GREEN
42
Attachment 1 to OAG Report – Staff-side Report
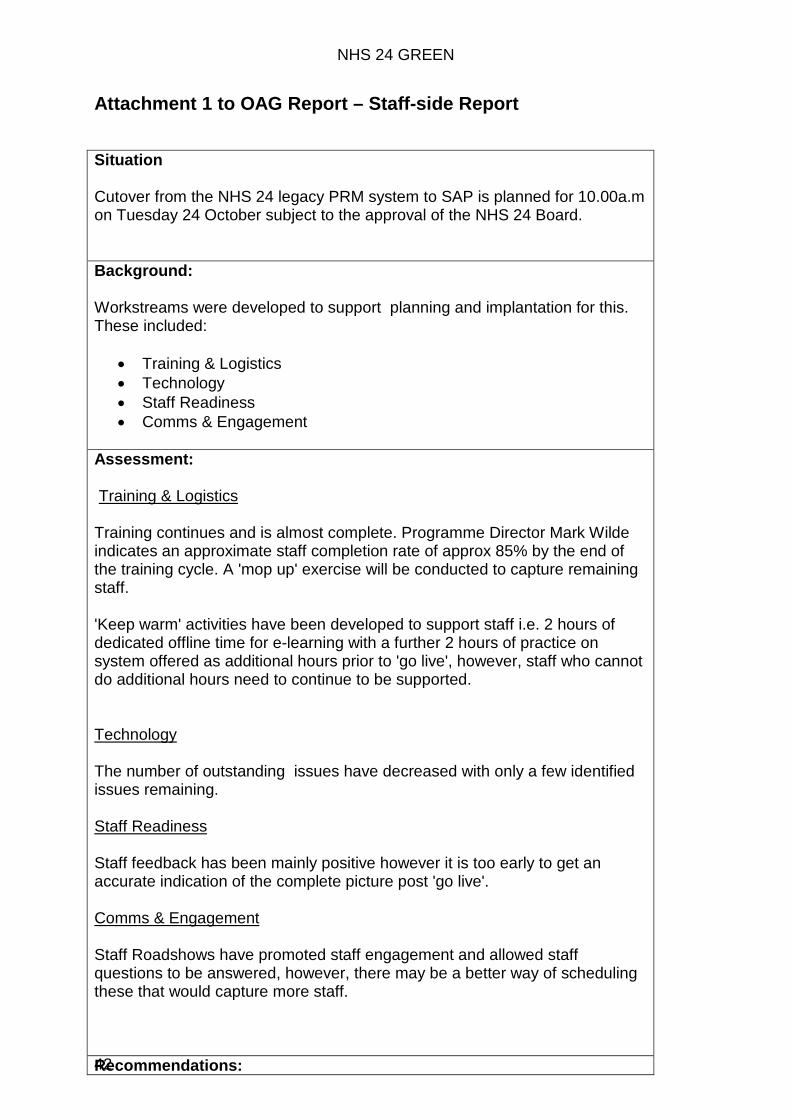
Situation Cutover from the NHS 24 legacy PRM system to SAP is planned for 10.00a.m on Tuesday 24 October subject to the approval of the NHS 24 Board. Background: Workstreams were developed to support planning and implantation for this. These included:
• Training & Logistics • Technology • Staff Readiness • Comms & Engagement
Assessment: Training & Logistics Training continues and is almost complete. Programme Director Mark Wilde indicates an approximate staff completion rate of approx 85% by the end of the training cycle. A 'mop up' exercise will be conducted to capture remaining staff. 'Keep warm' activities have been developed to support staff i.e. 2 hours of dedicated offline time for e-learning with a further 2 hours of practice on system offered as additional hours prior to 'go live', however, staff who cannot do additional hours need to continue to be supported. Technology The number of outstanding issues have decreased with only a few identified issues remaining. Staff Readiness Staff feedback has been mainly positive however it is too early to get an accurate indication of the complete picture post 'go live'. Comms & Engagement Staff Roadshows have promoted staff engagement and allowed staff questions to be answered, however, there may be a better way of scheduling these that would capture more staff.
Recommendations:

NHS 24 GREEN
43
Staff Engagement/Readiness
• MO TL feedback – all issues will have been addressed that have a direct impact on the T2 launch and any issues for future implementation have been jointly agreed.
• All staff will be trained and fully signed off prior to the start of their first operational shift.
• All staff sign off material will be reviewed and where staff have not signed themselves off there is clarification and understanding of how that position can be rectified.
• Outcomes from the staff survey will reflect a position of competence & confidence in NHS 24s ability to support staff during the cutover period.
• A complete 'mop up' plan needs to be confirmed to ensure that staff returning from sick leave are also captured. This plan should be shared with all key stakeholders including Staff Side.
Cutover Plan
• All activities during the cutover will be underpinned by behaviours that demonstrate clearly the NHS 24 values.
• Each shift over the 6 week cutover period will have sufficient trained staff and management support to deliver care for the anticipated call demand.
• A positive learning environment will be created where individual staff performance will be supported to allow them to transition onto the new system with an anticipation that average call handling times will be extended beyond current parameters. For a period of 3 months we would request that individual performance management in relation to call handling time be suspended.
• Command & control will be robust and consistent to support staff confidence.
• All staff will understand what the support model looks like from a technical and clinical point of view and managers and staff will have a common understanding of the support ratios which will be provided with the various aspects of frontline services i.e Seasonal Initiative, Rapid Triage, and real time floor support.
• There will be a clear understanding of the support model which will be in place for staff who identify themselves or are identified by the organisation as needing further offline training
• Staff and staff side will understand how 'experienced users' will be distributed to provide Technical Support.
• Local/Remote Centres – There will be a detailed plan re how these centres will be supported.

NHS 24 GREEN
44
Appendix 17 – TAG Report 2 October 2017 FOR NOTING TECHNICAL ASSURANCE GROUP – HIGHLIGHT REPORT
Purpose: To provide an update on progress being made in the area of assurance of the “technical” aspects of the Programme. Author: Eddie Turnbull, Head of Information Services, SG ARE Andy Robertson Director of IT, NSS 1. Situation 1.1 The TAG met on 20th September. The purpose of the meeting was to review
plans and actions taken in readiness for Tranche 2 Full Board Go Live. 2. Background 2.1 The work of the TAG is focussed on a risk based approach to the ‘technical’
elements of the Programme over its incremental “go-live” phases and is focussing on four key elements: a) The Systems’ performance; b) The Systems’ functionality; c) The ‘Target Operating Model’, including ensuring that NHS 24 is
capable of fulfilling its responsibilities as defined in the contract; and d) The integrity of the overall delivery plan, including the re-profiled
timescales and the sustainability of legacy applications in that timeframe.
2.2 The rest of this report provides assurance on each of these aspects and concludes with an overall assessment of go-live readiness as reflected in the TAG Assurance Plan.
3. Actions and Status Assessment Element Risk Status Comment The Systems’ performance
GREEN TAG have noted that the full functionality of system has now been live since May 2017. NHS24 have worked with their staff in the Model Office to ensure the system performs as expected, and this has been further verified throughout the training sessions. TAG is satisfied that no substantial changes to infrastructure or functionality have taken place for T2 Full Board Go Live. TAG has endorsed NHS24’s decision that a full performance test (as was carried out in 2016) is not necessary given that performance is now being monitored as an on-going activity. BT are

NHS 24 GREEN
45
checking the network on a daily basis and optimising as required. A final focused check is scheduled for 9 October, which will be after CapGemini final changes are applied and before the technology change freeze goes into effect. TAG has been assured that enhanced active/anticipatory monitoring of performance will be in place for the “go live” day and for support arrangements in the days that follow. This will cover both network and application performance.
The Systems’ functionality
GREEN Since the T1 May 2017 Go Live a number of changes/enhancements as well as defect fixes have been identified. These changes/enhancements were developed in the summer of 2017, have been tested in Sept 2017 and will be deployed at the start of Oct 2017, ahead of T2 Full Board Go Live. TAG has been assured that a plan is in place to ensure that all endpoint devices are configured correctly with IE11 and ready for use on “go live” day. TAG is satisfied that, pending satisfactory completion of the remaining testing and the delivery of the Test Completion Report, that testing has been appropriate and has been completed satisfactorily to support the T2 Full Board go-live.
The ‘Target Operating Model’, including ensuring that NHS 24 is capable of fulfilling its responsibilities as defined in the contract
GREEN TAG is satisfied that NHS 24 has adequate arrangements in place to manage the “Tranche 2” Full Board Go Live. However TAG notes that the conclusion of contractual negotiations may not be completed ahead of T2.
The integrity of the overall delivery plan, including the re-profiled timescales and the sustainability of legacy applications in that timeframe.
GREEN The go-live project plan and supporting day-book from T1 Single Board Go Live in May 2017 has been be renewed and updated for the T2 Full Board Go Live in Oct 2017. TAG will have a final review of this at its meeting scheduled for 18th October. TAG has been informed of support plans for the “go live” day and for enhanced support arrangements in the days that follow and agree that these are comprehensive.

NHS 24 GREEN
46
Overall readiness – Technical Assurance Plan
Green TAG is satisfied that the information provided in the Technical Assurance Plan (Appendix 1) – which highlights those activities carried over once T1 was live - supports the decision of TAG to recommend a go-live decision for T2 Go Live in Oct 2017.
Appendix 1 to TAG Report – Technical Assurance Plan (Final)
Microsoft Office Excel 97-2003 Worksh

NHS 24 GREEN
47
Appendix 18 – T2 Go-Live Communications and Engagement Plan Communications and Engagement Plan at go-live and during cutover This plan outlines the arrangements for communications and engagement activities with staff and partner boards during the enhanced support period (up to 6 weeks) following cutover from the legacy PRM system to SAP. It will be appended to the approved Communications and Engagement Plan for the Organisational Improvement Programme. Cutover from PRM to SAP will occur at 10.00a.m on Tuesday 24 October subject to the approval of the NHS 24 Board. A detailed cutover plan governs the hour by hour activities supporting cutover. This paper is concerned only with how executive management, staff and partner boards will receive communications during the enhanced support period following cutover. First 24 Hours post cutover Timing/Update method
Reporting themes Audience Provided by
12 noon: Email • Call demand • Service Levels • Technical Incidents
NHS 24 Board, EMT
Control Room
3pm: Conference Call with Handover Report
• Technical Incidents • Emerging Themes • Wrap up of previous shift
(inc staff experience)
CSM/Team Leaders
Control Room/Service Management
4pm: Email • Call demand • Service Levels • Technical Incidents
NHS 24 Board, EMT (email to all staff)
Control Room
4pm: Conference Call
• Call demand • Service Levels • Technical Incidents • Staff experience (inc Staff
Side view)
All Partner Boards,SAS
Control Room/Medical Director
9pm: Conference Call with Handover Report
• Technical Incidents • Emerging Themes • Wrap up of prev. Shift (inc
staff experience inc Staff Side view)
CSM/Team Leaders
Control Room/Service Management
10pm: Email and Call
• Call demand • Service Levels • Technical Incidents • Wrap up of day's activity (inc
staff experience & staff side view)
NHS 24 Board, EMT (email to all staff)
Control Room
10.30pm: Email and Call
• Call demand • Service Levels
All Partner Boards,
Control Room/Medical

NHS 24 GREEN
48
Timing/Update method
Reporting themes Audience Provided by
• Technical Incidents • Wrap up of day's activity (inc
staff experience & staff side view)
SAS Director
7.30 a.m. Conference Call with Handover Report
• Technical Incidents • Emerging Themes • Wrap up of prev shift (inc
staff experience & staff side view)
• Partner experience
CSM/Team Leaders
Control Room/Service Management
8.00a.m: Email • Call demand • Service Levels • Technical Incidents • Wrap up of prev 24hrs
activity • Staff experience & staff side
view • Partner experience
NHS 24 Board, EMT and Partner Boards, SAS, SG (email to all staff)
Control Room
Consideration should be given to the best approach to engaging with SG in the first 24 hour period. First week of cutover (ex first 24 hours) – Daily Routine Effective from Wednesday 25th October Timing/Update method
Reporting themes Audience Provided by
7.30 a.m. Conference Call with Handover Report
• Technical Incidents • Emerging Themes • Wrap up of prev shift • Partner experience • Staff experience & staff side
view
CSM/Team Leaders
Control Room/Service Management
8.00a.m: Email • Call demand • Service Levels • Technical Incidents • Wrap up of prev 24hrs
activity • Partner experience • Staff experience & staff side
view
NHS 24 Board, EMT and Partner Boards, SAS, SG (email to all staff)
Control Room
3pm: Conference Call with Handover Report
• Technical Incidents • Emerging Themes • Wrap up of previous shift
CSM/Team Leaders
Control Room/Service Management

NHS 24 GREEN
49
Timing/Update method
Reporting themes Audience Provided by
9pm: Conference Call with Handover Report
• Technical Incidents • Emerging Themes
• Wrap up of previous shift
CSM/Team Leaders
Control Room/Service Management
10.00p.m: Email • Call demand • Service Levels • Technical Incidents • Partner Feedback • Staff experience & staff side
view
NHS 24 Board and Partner Boards, SAS, SG
Control Room
In addition to the above daily routine, it is proposed that each Partner Board will receive an individual call on the Thursday morning and Monday morning from clinical leadership* within NHS 24, to undertake a "temperature test" of each Partner Board and SAS and ensure communication channels are operating effectively Reporting information will be available for discussion as part of these engagements. *These meetings will be led by the Interim Medical Director or Associate Medical Director and will have support from relevant clinical expertise. Week 2 onwards After the first week, and on each Tuesday thereafter, the week 1 communications plan will be reviewed by EMT and agreement reached as to whether a) the week 1 communications plan is rolled forward into week 2 unchanged b) the plan is scaled back to an appropriate level c) additional tasks are agreed to enhance communications