australian menopause centre - ebook
DESCRIPTION
Find out exactly what Menopause is and how you can stop suffering from the symptoms and feel fabulous again!TRANSCRIPT
The MENOPAUSE Booklet 1
MenopauseBooklet
The
eBook
The MENOPAUSE Booklet 2
This booklet briefly explains how your treatment program works. It answers many commonly asked questions about
how soon your menopausal symptoms should subside, how and when you need to fine tune your treatment, as well as
when you can expect to stop treatment.

The MENOPAUSE Booklet 3
Welcome to the Australian Menopause Centre (AMC)
Introduction
Phases of Menopause
Getting Started
What to Expect in the First Four Months
How Long Will You Remain On The Program?
Your Medical Checklist
Compounding Of Hormones
Fresh Is Best
How to Take Your Medication
Prescription Delivery
Important Points Regarding Medication
Understanding Your Menopause
Understanding Your Hormones
Bio-identical Natural Hormones - A More Natural Approach
The Health Risks of Hormone Replacement Therapy
Meet the Bio-Identical Hormones
Menopause Lifestyle Eating and Exercise Plan
Contributors to Menopausal Symptoms - Lifestyle Tips
Exercising Through Menopause
Check for Osteoporosis
What The Man In Your Life Can Do To Help!
We Are Here To Help
Private Health Fund Rebate
Privacy
Our Treatment Program Overview
4
5
6
7
8
10
11
12
12
13
14
15
16
24
29
32
34
36
38
40
44
45
46
47
47
48
Table of Contents

The MENOPAUSE Booklet 4
Welcome to theaustralian Menopause Centre (aMC)
Our aim is to provide you with a treatment program of Bio-identical Hormone Replacement Therapy(BHRT) designed to help your menopausal symptoms sub-side as quickly as possible. Every woman is physiologically different and will also be at a different stage of menopause. This is why we individualise our approach on a person by person basis.
We will recommend a starting point for your treatment based on your medical history as well as your current symptoms. We may use pathology testing of your hormones as a helpful diagnostic tool. We encourage your regular feedback so that we can understand how best to address your symptoms over time.
When you start your treatment program, we will stay in regular contact through-out your time with us. Based on your feedback, relevant medical history and any investigation results, we will counsel you and if necessary, adjust your medication dosage to ensure that you gain the best symptom relief with the lowest required treatment dose.
Our skilled staff are delighted to have the opportunity to assist you and we assure you that we will endeavour to provide you with our prompt, personal and profes-sional attention.
Kind Regards,
Dr Gary Aaron
MEDICAL DIRECTOR
Australian Menopause Centre
The MENOPAUSE Booklet 5
Introduction
Menopause is a natural change that occurs in a woman, marking the end of her monthly menstrual periods, sometimes referred to as “cessation of the menses”, “the climacteric” or “change of life”. Menopause is the last stage of a gradual bio-logical process in which the ovaries reduce their production of sex hormones. Most of the symptoms of menopause come from decreased production of the hormone oestrogen. This process progresses gradually over a period of time. It is rare for a woman to be menstruating after the age of 55.
The average age of menopause is 51 however some women can experience symp-toms from age 35 or earlier. It is most common for menopausal symptoms to occur between the mid forties and early fifties. Sometimes a woman will follow the same course as her mother.
Menopause can be induced by surgically removing the ovaries. Early onset of menopause may also occur from cancer therapy, certain illnesses or diseases and smoking.
Menopause is an individual experience, therefore symptoms and intensity of symp-toms will vary from person to person. Typical symptoms are night sweats, hot flushes, mood swings, anxiety, depression, insomnia, vaginal dryness (painful inter-course) and loss of libido (low sex drive).
What Is Menopause?
When Will It Occur?
What Are The Symptoms?

The MENOPAUSE Booklet 6
can occur from age 35 onwards and women may have regular periods but be experiencing menopausal symptoms.
can occur in the middle to late 40s and women may experience irregular men-strual periods and symptoms such as hot flushes, night sweats, mood swings or depression. Peri-menopause, is perhaps the most difficult to treat and can require multiple changes in hormonal supplementation. Many women simply do not cope well with this erratic time in their life.
is marked by the end of monthly bleeding and signals a major decline in oes-trogen production. It could be said to have commenced when a woman in her 40s or 50s has not had a period for six months or more. If it has been 12 months since her last period, then menopause is almost certain.
represents the first five or so years after menopause. The lack of oestrogen released from the ovaries leads to several changes. These may include de-crease in bone density, rising levels of cholesterol and other lipids in the blood, and other physical changes. Hot flushes, night sweats and mood swings may occur during this phase, although these generally decrease within one to two years.
Pre Menopause
Peri Menopause
Menopause
Post Menopause
1 |
2 |
3 |
4 |
phases of Menopause
The phases of menopause can be characterised as follows:
Despite a commonly held belief, menopause is not an end ~ it is a beginning. Most women will live at least one-third of their lives after menopause. Menopause can be described as the beginning of a new
phase in a woman’s life that will bring different expectations, opportunities and experiences.
The MENOPAUSE Booklet 7
Getting started
This section outlines the steps involved as well as what to expect when you first commence the treatment program. Also included is some general information and some useful health and lifestyle tips that may help you minimise your symptoms and improve your quality of life
Our goal is to provide you with a BHRT treatment program designed to adequate-ly control your menopausal symptoms, and to provide a low dose treatment to accommodate your body’s requirements. We will assist you in reaching that goal by us first arriving at a starting point for your treatment and then monitoring your situation until such time as you are ready to be weaned off the treatment.
In order for us to arrive at that starting point we will require:
A detailed medical history, where we will ask you relevant questions pertaining to your health. A description of your current menopausal symptoms Results from pathology and or other investigations
Our staff will assist you organising this in advance of your first consultation with one of our doctors.
An initial consultation will then be booked for you with one of our doctors. Based on the information and the outcome of your first consultation, our doctors will suggest an appropriate course of action.
Frequent follow up with you by our patient care team during the initial phase of your treatment.
Continuing regular follow up, providing you with our counsel and assistance along the way.
Finally assisting you to wean off the treatment.
Our Goal
STePS In BrIef
1
2
3
4
5

The MENOPAUSE Booklet 8
Insufficient response to the medication ~ your symptoms haven’t completely subsided
Break-through bleeding
Breast tenderness
Bloating
Headaches
What to expect in the First Four Months
It’s important to understand that it may have taken years for your body to become hormonally imbalanced - it’s not possible to correct this instantly.
Every woman will respond differently. Response will also be dependent on the par-ticular stage of the menopause a woman is at. Your response will be in accordance with your body’s natural sensitivity and absorption rate of the various hormones. You may experience rapid symptom relief or, as is more usually the case, this may take a number of weeks.
Some women, especially in the first 14 days after starting BHRT, may experience an increase in hot flushes and night sweats. These may actually increase in intensity and frequency before they start to reduce. This may be due to what we refer to as an “oestrogen dip” - this is when your body reduces production of its own oestro-gen in response to the BHRT supplementation.
When you begin your treatment program, you may experience symptoms that re-flect insufficient supplementation or over-sensitivity to the hormones. These symp-toms may include uncomfortable reactions such as:
Your response to the medication should stabilise over a period of time.
The MENOPAUSE Booklet 9
If you are experiencing any unwanted symptoms including any of those set out above, it is important that you contact the AMC help line on 1300 883 405 and book an appointment as soon as possible.
One of our goals is to provide you symptom relief using the lowest required dose of BHRT for as short a duration as is required.
In order to fine tune your treatment and reach this goal, your treatment dosage will from time to time require a review.
If after your initial consultation with one of our doctors, you decide to join our pro-gram, we will contact you as follows:After the date your first medication is dispensed, you will receive a Welcome Call from us where we will go over the details of your treatment program and establish that you have received what is needed to start your treatment program. We will also then schedule follow up clinical reviews with our clinical team. We will then contact you regularly during this time.
You will also be able to contact us for advice.
Adjusting Your Initial Dosage
regular follow Up
At all times it is vital that you take the medication according to the instructions supplied with the medication and the advice given
by our medical team.
The MENOPAUSE Booklet 10
How Long Will You Remain on The program?
It is normal for women to remain on the program from anywhere between two and five years (some women may require treatment beyond five years.)
Treatment duration is determined by your body’s adjustment to the menopause and its ability to eventually cope without supplementation. With ongoing regular testing and assessment of your symptoms we will be able to guide you through your program.
The rebalancing process involves two different but equally important hormones.
Oestrogen can be effective for hot flushes, night sweats, low energy, skin dryness and vaginal dryness but in excess can cause fluid retention.
Progesterone can be effective in reducing anxiety, mood swings and stress. It also helps release excess fluid from the body and helps with hot flushes and improves sleep.
While both of those hormones offer positive benefits, the benefit of one hormone can be offset by the other if dosage levels are not carefully monitored. For exam-ple, oestrogen causes fluid retention while progesterone acts like a diuretic and helps with fluid release. It is important to ensure that while we are weaning you off your treatment, the correct balance is maintained.
The duration of the complete process of weaning off BHRT may vary but may be as short as just a few months. Each month during the weaning off process we will determine from you, based on your feedback, how you are progressing and wheth-er or not any of your symptoms have returned. Together with you, we will consider each month whether or not to reduce your medication any further. Of course, if any symptoms return during this process, you should contact the Australian Meno-pause Centre immediately.
reducing Your Dependency

The MENOPAUSE Booklet 11
Your Medical Checklist
As part of your treatment program, we may recommend that you undertake spe-cific medical tests. These will be advised by our doctor during your consultation. In addition, we suggest that you consult with your general practitioner and have the following tests:
As a patient of the Australian Menopause Centre we encourage you to maintain these regular medical checks and also strongly advise that you inform us of your results. We do recommend a yearly blood test and clinical reviews with our clinical staff. If you find that you have not had a review or scheduled 12 monthly blood test, please remind us when you speak with your care consultant.
(unless you have had a hysterectomy or if you are being followed for previous abnormal smears).
Especially if over the age of 50. Some women, with a family history of breast cancer, may require a mammogram yearly and from an earlier age. Regular self examination of your breasts is also recommended.
(more regularly if on blood pressure medication).
Consider an initial assessment of your cholesterol and other blood lipids, espe-cially if you are overweight or you have other risks of having elevated cholester-ol, e.g. a family history of heart disease. Further testing will depend on this initial result.
An initial assessment of your blood sugar is advisable. Further testing will de-pend on this initial result.
An initial bone scan is advisable. Further bone scans will depend on this outcome.
Pap Smear - every 2 years
Mammogram - every 2 years
Blood Pressure - At least every 12 months
Cholesterol Levels
Blood Sugar Levels
Bone Scan
The MENOPAUSE Booklet 12
Compounding of Hormones
The Hormones used in BHRT have chemical structures identical to those the hu-man body produces naturally and are commonly referred to as being “bio iden-tical”. Bio identical hormones with the appropriate strength to assist in relieving your symptoms cannot be dispensed over the counter of a retail pharmacy. They can only be dispensed by prescription.
Your BHRT medication will be individually compounded as prescribed by our doc-tors according to the specific dose and combination you require. Because these hormones are compounded specifically, our doctors can tailor a formulation to suit. Furthermore, the medication can be finetuned over time to increase or de-crease the strength. The pharmacy that compounds the medication is a dedicat-ed compounding pharmacy and uses only British Pharmacopoeia (BP) or United States Pharmacopoeia (USP) grade products. Good manufacturing practices and principles, along with using the highest grades of raw ingredients ensure the quali-ty of the medication dispensed.
Prescribed By Doctors and Compounded To Order
Fresh Is Best
It is very important that to get the best results from any medication, is to ensure that it is used before its expiry date. Compounded medication has an expiry date of 3 months from the date of dispense. We encourage patients to use their medi-cation as prescribed by the doctor and to ensure that they do not use out of date medication.
This usually means that you will well and truly use your prescribed does well within the expiry date. Your health is too important to take unwise and unnecessary risks by using medication that is past its expiry date. You will find us committed to en-suring that you use your medication properly. It is part of our duty of care to con-tinually monitor your progress and to ensure you get the best result from fresh and effective bio-identical hormones.
The MENOPAUSE Booklet 13
How to Take Your Medication
Our initial aim with your treatment program is to balance your levels of oestrogen and progesterone - the two hormones responsible for the majority of your symp-toms. To facilitate this goal most patients will initially receive two separate packs of medication as troches, (most patients are prescribed troches):
For patients who are prescribed creams or other forms of BHRT, please refer to the instructions accompanying your medication.
Keeping your dosage of the medication low will be the most desirable outcome for you. Therefore some dosage adjustments may be required to ensure you get the most effective result.
The purpose of these separate packages is to allow your doctor or nurse to make dosage changes as and when required. If you are taking this medication for the first time, you should have received enough medication to last you approximately 4, 8 or 12 weeks depending on your particular program.
If you experience over-sensitivity to your BHRT, please contact the AMC Helpline immediately.
It is important to understand that you may have been in a state of hormonal imbal-ance for many years and correcting these levels may take a few months.
Through the course of the program your doctor may prescribe a change of medi-cation dosage for you.
It is very important that you follow instructions from our medical team in relation to any changes to your medication and dose.
one pink pack containing oestrogen (translucent colour)one blue pack containing progesterone (white colour)
Your Starting Dose
The MENOPAUSE Booklet 14
prescription Delivery
Medication will automatically be dispatched regularly, either monthly, bi-monthly or quarterly to patients on a automatic dispense and payment plan (if you are not on a direct debit payment plan please call the Australian Menopause Centre to ar-range one). This is to ensure you never run out of medication. It is vital to maintain regular daily doses and to ensure you always have a fresh effective supply.
If you are not home at the time of delivery the courier will try to leave the medica-tion at an agreed delivery point (near the front or rear door / veranda and out of the sun or your local post office for pick up).
It is important to notify AMC immediately if you have changed your address.
A courier delivers your medication to you, but occasionally a batch does get lost.
It is important to contact us immediately if you have only seven days or less med-ication left and have not received the next month’s supply. Please do not leave notifying us to the last minute as it does take 2-3 days to arrange replacement dispenses.
Each prescription is individually compounded to order at a specialised pharmacy. It can therefore take approximately five working days from the time you contact us until your medication actually arrives at your requested delivery location. It may take slightly longer for remote areas.
Automatic Monthly repeats
What to Do if Your Medication Has not Arrived
The MENOPAUSE Booklet 15
Important points Regarding Medication
If you have been late in starting your medication, please call us so that we can resynchronise the delivery of your next batch.
If you have not received your expected delivery of medication, and you have only 7 days medication left, please urgently call us on
1300 883 405. We will need to follow up to ensure that you do not run out.
Whilst you are on our program we strongly suggest that you do noT take any other forms of hormone therapy unless
specifically advised by our Clinical team.
The MENOPAUSE Booklet 16
understanding Your MenopauseMenopause is literally the cessation of your menses, and the end of your menstrual cycles.

The MENOPAUSE Booklet 17
The MENOPAUSE Booklet 18
understanding Your Menopause
Prior to this occurring many women experience “menopause like” symptoms well before the actual “last period” as the body undergoes various hormonal changes and fluctuations. This is often referred to as the “climacteric” or “change of life”.
We are born with approximately 2 million egg follicles. By the time we reach pu-berty there are about 750,000 and by the age of around 45, only 10,000 may be left. The rest may have disintegrated over the years. Menopause occurs when your store of eggs run dry.
During the transition to menopause most women will experience at least one of the following phases.
Read on to identify where you may be at this very moment?
Pre-Menopause
Peri-Menopause
Menopause
Post Menopause
Early Menopause
Surgical Menopause
The pre-menopause can be characterised when a woman begins to experience menopausal symptoms whilst still having a regular monthly cycle. This indicates the hormones are beginning to change.
Pre-menopausal symptoms can occur for a woman as early as the age of 30 but tend to occur more commonly around the mid to late 40’s. They may include hot flushes, sweats, emotional swing.
Pre-MenOPAUSe

The MENOPAUSE Booklet 19
The peri-menopause is the next stage following the pre-menopause. During peri-menopause the ovaries begin to decline in the production of hormones and the menstrual period become irregular. The changes in the cycle may be subtle or very dramatic. Women may notice a slightly lighter flow, or slightly heavier flow. The duration of the cycle may differ too, going from a 28 day cycle to a 33 day cycle, followed by a 31 day cycle.
Alternatively, the changes may be more dramatic. It is not uncommon to skip a period completely, or cease having periods for a few months at a time then re-commence two weekly or monthly. Women often say they experience the heaviest periods of their entire reproductive life or alternately their menstrual flow may be significantly lighter. Regardless, this is a time when changes are noticed within the cycle whether they be subtle or dramatic.
Most women experience what is termed a “natural” menopause, which occurs gradually. Many women begin noticing changes in their menstrual cycle and/or mood, years before they actually have their final period. It is not uncommon for a woman to experience irregular cycles with associated symptoms sometimes up to 5-10 years prior to complete cessation of the menses. For other women their peri-ods suddenly stops one month and they never menstruate again.
Progesterone is generally the primary female hormone to decline during the pre/peri-menopausal stage whilst oestrogen can remain stable or even increase. This ultimately creates an ‘imbalance’ between the two hormones. This state of low progesterone to oestrogen ratio is commonly referred to as “oestrogen domi-nance”. Testosterone levels may also start to decline well before the last menstrual cycle.
PerI-MenOPAUSe
Generally speaking, the symptoms during the Peri-menopause will be more severe than those experienced during the pre-menopause and
normally occur around the mid 40’s but can occur as early as the late 30’s early 40’s and for other women as late as the early 50’s.
The MENOPAUSE Booklet 20
Oestrogen production during the peri-menopausal stage may become erratic with surges of inappropriately high levels alternating with irregular low levels. This helps to explain periods of hot flushes and night sweats coupled with oestrogen dominant symptoms (high ratio of oestrogen to progesterone) such as breast tenderness, headaches, fluid retention and cravings. In many cases, women can successfully manage these symptoms effectively with the support and balancing effects of natural progesterone alone. Ideally both hormones work best when they are in balance and harmony with each other.
As progesterone is an important hormone involved with building bone, bone loss is accelerated during the first 5 years after a woman enters her menopause.
Therefore, it is important to adopt healthy lifestyle factors to further prevent the risk osteoporosis. These include regular weight-bearing exercise such as walking or jogging, enjoying a healthy diet with an adequate supply of calcium, avoiding foods and substances that compromise bond health, such as smoking or drinking soft drink that contain substances known to strip calcium from the bones.
Symptoms of Peri-menopause will generally be the result of low levels of pro-gesterone, potentially coupled with oestrogen dominant symptoms and symp-toms associated with low levels of testosterone. Oestrogen levels during this stage can be quite erratic hence your symptoms may reflect this.
Mood swings, depression, anxiety, feeling emotional or more vulnerable, sore breasts, bloating, hot flushes/sweats, tiredness, insomnia, weight gain, forget-fulness, lack of concentration, reduced capacity to deal with stress, aching in the muscles and joints, irritability, reduced sex drive, lack of energy, fibrocystic breast, period problems and fibroids, endometriosis, low metabolism, cravings (particularly for sweet things), sluggishness in the mornings.
Headaches/migraines, recurrent vaginal yeast infections, breast swelling and tenderness, depression, nausea, vomiting, bloating, leg cramps, yellow tinged skin, excessive vaginal bleeding, possible weight gain irritability, cravings par-ticularly for sweet things, fatigue.
Symptoms of Peri-menopause
Symptoms of a lack of progesterone
Oestrogen Dominant Symptoms
The MENOPAUSE Booklet 21
Loss of sex drive, decreased sexual response, decreased sensitivity in your erogenous zones, decreased sense of well-being, energy and ambition, depres-sion, loss of or thinning of pubic hair.
Symptoms of menopause include many of the symptoms associated with peri-menopause, coupled with the symptoms of a lack of oestrogen.
Increase in hot flushes, night sweats, vaginal dryness, vaginal wall thinning, decreased sexual response, dry skin, crawling or itching sensations under the skin, dry hair and possible hair loss, ageing skin, mental fuzziness, urinary fre-quency, vaginal and/or bladder infections, infection, incontinence, recurrent urinary tract infections, difficulty sleeping, lack of esteem, osteoporosis
Low Testosterone Symptoms
Symptoms of Menopause
Lack of Oestrogen Symptoms
Menopause is your very last period and officially classified as such once your peri-ods have completely ceased for a full 12 months. The average age of menopause is 51 years, give or take 5 years.
For some women the full symptoms of menopause do not kick in until after this 12 month period, indicating a dramatic drop in circulating oestrogen leading to the more common symptoms associated with menopause such as hot flushes, night sweats, dryness of the skin and dry vaginal tissue.
Symptoms of menopause can last on average between 4-6 years. In saying this, some women breeze through menopause with few or no symptoms at all, where as others, when you include the pre and peri-menopausal stages, may experience symptoms for up to 20 years.
MenOPAUSe
The MENOPAUSE Booklet 22
The post menopause follows on from the menopause. Oestrogen and progester-one levels are still low but the body has learned to cope with these lower levels and most of the symptoms disappear. There is still an ongoing concern about os-teoporosis so weight bearing exercises and good dietary habits need to be main-tained. Vaginal dryness and low libido are symptoms that often require ongoing attention.
Menopause affects each woman differently and every woman may be experienc-ing different symptoms at different stages of menopause. We are all unique and while the symptoms of menopause, maybe similar to that of other women, every-one will travel their own journey.
Other considerations that may affect the severity of your symptoms include life-style factors such as diet, nutrition, exercise, other prescription medications, other health concerns, stress levels and relationship issues.
Menopause before the age of 40 is called an early or premature menopause. It may occur naturally when the ovaries have stopped working, surgically when a woman has her ovaries removed or chemically from chemotherapy/radiotherapy for cancer.
Smokers tend to have an earlier menopause by about 2 years on average because smoking diminishes the secretion of oestrogen in the ovaries.
A hysterectomy, even without the removal of the ovaries can lead to the earlier onset of menopause by about five years. It is believed this happens due to the change in blood supply to the ovaries after surgery. A tubal ligation may also bring on an earlier menopause for some women.
POST MenOPAUSe
eArLY MenOPAUSe

The MENOPAUSE Booklet 23
Surgical menopause is when the ovaries are removed prior to a natural meno-pause (known as an oophorectomy). This causes a sudden and permanent drop of the ovarian hormones, oestrogen, progesterone and testosterone.
The surgical procedure may include the removal of the uterus - when both are removed, this is termed a total hysterectomy.
An oophorectomy or total hysterectomy will lead to an instant menopause and often the symptoms are intense unless treatment is initiated immediately.
SUrGICAL MenOPAUSe
We are more than just our hormones hence this is why an integrated and individualised approach to managing your symptoms will offer
the best possible outcomes.

The MENOPAUSE Booklet 24
understanding Your HormonesIn order to fully understand the hormonal changes that the body may be experiencing as it enters menopause we must first understand the monthly cycle.
The MENOPAUSE Booklet 25
The MENOPAUSE Booklet 26
understanding Your Hormones
During the reproductive years women produce a number of hormones. These include oestrogen, progesterone, follicle-stimulating hormone (FSH) and luteinis-ing hormone (LH). Each of these hormones has a specific role to play during the various stages of your monthly menstrual cycle.
On the first day of the menstrual period, FSH is released from the pituitary gland. FSH stimulates the growth of a group of follicles on the surface of the ovary. These follicles will eventually produce eggs. Over the next two weeks (the follicu-lar phase) the eggs will develop and mature. At the same time, your levels of oes-trogen (the primary female hormone) will increase.
As your oestrogen level increase, the pituitary gland decreases its production of FSH. At this stage another hormone comes into play, known as luteinising hor-mone, LH surges at mid cycle and triggers the release of an egg (ovulation). The egg enters the fallopian tube and is carried into the uterus.
The empty follicle (corpus luteum) begins to produce progesterone, as the second half of the cycle commences - this is termed the luteal phase. If fertilization does not occur the lining of the uterus (endometrium) is shed, resulting in a menstrual period. At the same time there is a dramatic fall in both oestrogen and progester-one levels, which in turn triggers FSH and the cycle starts all over again.
A sign that menopause is approaching is a surge of FSH. In the lead up to meno-pause, the number of cycles in which eggs are NOT released increase. Oestrogen rather than increasing begins to decline during the first two weeks and ovulation is less likely to occur, although women can still experience a period. The chance of falling pregnant diminishes, though it is still possible.
Without the rising levels of oestrogen to send back a message to the pituitary to produce smaller amounts of FSH, the levels of FSH in the blood stream keep rising as the body registers that ovulation is not happening.

The MENOPAUSE Booklet 27
Increases in FSH can be measured via a blood test to help detect the onset of menopause. Women begin to notice a “difference” internally; signs and the symptoms normally experienced with ovulation may now be absent. This may be replaced by the onset of experiencing menopausal symptoms, such as mood swings, hot flushes, night sweats, bloating, fluid retention, to name a few.
Your adrenal glands and other hormone producing sites such as the fatty tissues now take on a more significant role to minimise symptoms and support a woman throughout the transition of menopause.
Hormone replacement took hold in the 1960’s with the introduction of unopposed oestrogen in the form of pregnant horse’s urine (Premarin) to manage the “disease” of menopause.
It soon became “fashionable” to take as women were sold and marketed the prom-ise of remaining young forever. With the release of the book “Feminine Forever” by Dr Robert Wilson, Premarin soon became the standard treatment for women going through “The Menopause” and quickly became the number one selling drug in the United States.
By the 1970’s it was discovered that oestrogen alone increased the risk of uterine endometrial cancer, so a synthetic progestin was added to stop this danger. How-ever, in avoiding HRT induced uterine cancer, we then induced even more dangers namely an increased risk of breast cancer, cardiovascular disease and blood clots were induced.
Well before the WHI study confirmed the above risks, a number of short term clini-cal studies indicated the carcinogenic (cancer causing) properties and risk of blood clots of these synthetic hormones.
Conventional HrT (Hormone replacement Therapy) and the Women’s Health Initiative (WHI)

The MENOPAUSE Booklet 28
The most comprehensive evidence about the risks and benefits of taking hormones after menopause to prevent disease comes from the Women’s Health Initiative re-search program. This research program examined the benefits of menopausal hor-mones on women’s health.
The WHI research program involved two studies - the use of conjugated oestro-gens plus progestin for women with a uterus and the use of conjugated oestrogens alone for women without a uterus. In both hormone therapy studies, women were randomly assigned to receive either the hormone medication being studied or the placebo.
The WHI conjugated oestrogens plus progestin study was stopped in July 2002, when investigators reported that the overall risks of conjugated oestrogens plus progestin outweighed the benefits. The news made headlines around the world. Ul-timately, the study showed an increased risk of breast cancer, heart disease, stroke and blood clots. However, the risk of colorectal cancer and hip fractures was lower on HRT than those on placebo.
A subgroup of women in the WHI research program participated in the WHI Mem-ory study. This showed that conjugated oestrogens plus progestin doubled the risk for developing dementia in postmenopausal women age 65 and older. The risk increased for all types of dementia, including Alzheimer’s disease.
The WHI conjugated oestrogens alone study, was stopped in February 2004, when the researchers concluded that conjugated oestrogens alone increase the risk of stroke and blood clots.
The risk of breast cancer on oestrogen decreased in comparison to women on pla-cebo. Similar to the results of oestrogen plus progestin, oestrogen alone decreased the risk of urinary incontinence and showed a decreased risk of hip fractures.
Potential risks of Taking Conventional HrT as revealed by the WHI Study
The MENOPAUSE Booklet 29
Bio-identical natural HormonesA More Natural Approach

The MENOPAUSE Booklet 30
Bio-identical natural Hormones - a More natural approach
Bio-identical hormones have been in use for over 30 years and are used extensive-ly throughout Europe, the US, Canada, the UK and Australia. They are fast becom-ing the “preferred” choice for many women as they seek more “natural” alterna-tives to managing their symptoms of menopause.
The term bio-identical means “bio-logically the same as”. From a medical perspec-tive, bio-identical hormones share a similar bio-chemical and molecular structure to that of a hormone the human body naturally produces.
We call a human hormone a “natural” hormone and hence the reason why bio-identical hormones are also commonly referred to as “natural hormones” in that they match that which the body naturally produces.
Bio-identical hormones offer a more natural approach in that the hormones are plant derived. They are extracted predominantly from the wild yam plant and a smaller percentage from soy. Research has shown that bio-chemically the hor-mones produced by these plants share a similar bio-chemical structure to that of a human hormone.
The molecular structure is then slightly modified, in specialised labs, to match that of a human hormone.
In Dr Sandra Cabot’s book “Hormones the Real Truth” she states: “natural hor-mones are chemically identical to the hormones produced by your own glands, which means that your body cannot tell the difference between your own hor-mones and a natural hormone... These natural hormones are called bio-identical hormones”
What Are Bio-Identical natural Hormones?
The MENOPAUSE Booklet 31
Dr Christianne Northrup in “Wisdom of Menopause” states: “In contrast to pre-marin, Provera and Prempro, the hormones that I recommend are exactly the same as those found in the female body. Though they are synthesized in the lab from hormone precursors found in soy beans or yams, their molecular structure us de-signed to be an exact match of the hormones found in the human body. Hence we call them Bio-indentical....”
“Because Bio-identical hormones are just like the hormones that our bodies were designed to recognize and utilize, their effects are more physiologic-consistent with our normal biochemistry - with less chance for unpredictable side effects at low replacement doses than with synthetic, non bio-identical hormones”
Natural or bio-identical hormones are commonly used for peri-menopausal and menopausal women and include progesterone and the natural oestrogens (oestra-diol, oestrone and oestriol), DHEA and testosterone.
The beauty of natural hormones is that they can be “created” and tailored to each individual woman in unique doses and combinations, in a variety of applications to meet the needs of each woman. This allows for an individualised approach and considers such factors as: body weight, emotional and sexual needs, personal history, medical conditions and risk factors, unique metabolic and hormonal char-acteristics whilst evaluating the results of blood and salivary tests.
Over the past decade, millions of women have used bio-identical hormones with great success and improvement in health. Research studies done in the US and Europe on bio-identical hormones have confirmed this. Since 2003, the Australian Menopause Centre has had over 50,000 women complete our treatment program.
We now have a hormone that is plant derived, bio-chemically and molecularly similar to a human hormone. The idea being that the body
recognises the hormone as though it is one of it’s very own thus converts it into a hormone to work similar to it’s own hormones.
The MENOPAUSE Booklet 32
The Health Risks of Hormone Replacement Therapy
Studies including the Women’s Health Initiative, a large pharmaceutical trial, have indicated that conventional Hormone Replacement Therapy (HRT) is linked to a small but significant increase in breast cancer, such that taking the therapy for 5 years or more can result in approximately 4 extra cases of breast cancer per 1000 women. At the time there were no equivalent research studies done specifically on BHRT (bio-identical hormone replacement therapy) so the risks associated with BHRT had not been proven.
However, more recent studies1;2 which included bio-identical hormone treatment and in particular the use of micronized bio-identical progesterone have document-ed that there appears to be no increased concern regarding breast cancer risk.
If you have at least one first degree relative (i.e. mother or sister) who has devel-oped breast cancer, then you are at a slightly increased risk of developing breast cancer relative to the average population.
The effect of hormone replacement therapy on breast cancer risk for women who have a history of breast cancer (mother or sister) appears to be the same as for women who have no family history of breast cancer
BreAST CAnCer
Unequal risks for breast cancer associated with different hormone replace-ment therapies: results from the E3N cohort study, Agnès Fournier, Franco-Berrino and Françoise Clavel-Chapelon Postgrad Med. 2009 Jan;121(1):73-85. doi: 10.3810/pgm.2009.01.1949.
The bioidentical hormone debate: are bioidentical hormones (estradiol, estriol, and progesterone) safer or more efficacious than commonly used synthetic versions in hormone replacement therapy? Holtorf K
1 |
2 |

The MENOPAUSE Booklet 33
It is important to be vigilant with breast monitoring throughout your life, as at no stage of your life are you ever free from the risk of breast cancer. You should have regular mammograms (at least every 2 years) and regular self examination of your breasts. This should be done regardless of whether or not you are at an increased risk of breast cancer.
Women who have had breast cancer in the past are at a greater risk of devel-oping a recurrence of breast cancer.
Women who have had a blood clot in the past are at a greater risk of a recur-rence of a blood clot. If you have had a blood clot in the past, you will need blood tests to assess this risk.
Women who have had a stroke in the past are at a greater risk of a further stroke in the future. If any of these groups apply to you, your situation will be considered after specific blood testing and may require discussion with your specialists.
In keeping with good medical practice, we also recommend that you have your blood pressure checked by your GP at least once a year (more frequently if you have high blood pressure) and if you have not had a hysterectomy, you should have a pap smear test every 2 years. (Refer to“Your Medical Checklist”).
How to deal with the risk of breast cancer:
Breast Cancer
Blood Clot
Stroke
There is an increased risk of venous thrombosis (blood clots in the veins) in wom-en using hormone therapy, however the incidence is very low and more likely in the first year of therapy. The Women’s Health Initiative also concluded that women receiving HRT have a risk of suffering side effects such as fluid retention, head-aches, irregular bleeding, weight gain and breast pain. BHRT or HRT may there-fore not be advisable in particular if the following affects you:
OTHer rISkS

The MENOPAUSE Booklet 34
Meet the Bio-Identical Hormones
Bi-oestrogen (Bi-Est), a combination of oestriol and oestradiol. 80% of Bi-Est is oestriol, which has been shown to protect against breast cancer in animal studies. Oestriol causes little or no stimula-tion to the uterine lining and is clinically effective for the treatment of symptoms caused by oestrogen deficiency, such as vaginal dry-ness and atrophy, painful intercourse, and urinary tract disorders (incontinence, frequent urinary tract infections). Oestradiol relieves symptoms such vaginal thinning dryness. It decreases hot flush-es and night sweats; improves mood, energy level, sleep patterns, memory, cognitive function; and reduces bone loss. It may also help to lower blood pressure. Tri-oestrogen (Tri-Est), a combination of 80% oestriol, and 10% oestradiol, and 10% oestrone. Oestrone is the primary oestrogen produced after menopause. It is produced from hormone precursors in peripheral fat tissue.
Progesterone is a hormone commonly prescribed for women with too much oestrogen relative to the level of progesterone produced by the body. Pro-gesterone minimises the stimulating effects of oestrogen on coronary arter-ies, and when given alone or combined with oestrogen, it may improve bone mineral density. Progesterone improves sleep, may increase libido, act as a diuretic, lowers blood pressure and improves the insulin-glucose balance to facilitate blood glucose control.
Special Note: “Progestins” are sometimes erroneously referred to as “pro-gesterone.” A Progestin is very different and is not a bio-identical hormone. It is a synthetic hormone made to mimic the effects of progesterone. Some practitioners do not make the distinction between progestin and progester-one, which has caused much confusion. For example progestins are given to women to prevent pregnancy, whereas progesterone is used to assist fertility. The two could not be more different. Since progestins are foreign to a wom-an’s body, sometimes they create adverse effects on a woman’s body and sometimes they create adverse effects on a woman’s brain, blood vessels, skin, heart and breast.
OeSTrOGenS
PrOGeSTerOne
The MENOPAUSE Booklet 35
DHEA is prescribed for women whose hormone profile as determined by blood testing, indicates a low level of DHEA. DHEA enhances libido, helps to build bone mass, lowers the levels of cholesterol and triglycerides, improves the sense of well-being and increases alertness. Please note in Australia, DHEA is not registered with the TGA. Overseas DHEA is ap-proved and is commonly purchased as an “over the counter” nutritional supplement.
Testosterone is present in women too, not just males. Testos-terone is prescribed for women whose pathology suggests a deficiency in the hormone. It can help to improve libido, help to build bone mass, improve mood and the sense of well-be-ing, increase muscle mass and strength, lower levels of cho-lesterol and triglycerides, normalize blood glucose levels, and decrease body fat.
Melatonin is a naturally occurring compound found in hu-mans, animals, plants and microbes. In humans, circulating levels of melatonin vary in a daily cycle, thereby regulating the circadian rhythms of several biological functions. It also has a role as a pervasive and powerful antioxidant with a particular role in the protection of nuclear and mitochondri-al DNA. Melatonin signals the part of the body system that regulates the sleep wake cycle by chemically causing drows-iness. It is used to help improve sleep and get back into a reg-ular routine of sleep.
Pregnenolone is a pre hormone involved in the production of progesterone, mineralocorticoids, androgens and oestrogens. Pregnenolone may be considered a good brain enhancer in those who are deficient. In some people pregnenolone im-proves energy, memory, clarity of thinking, wellbeing, and often sexual enjoyment or libido.
DHeA
TeSTOSTerOne
MeLATOnIn
PreGnenOLOne
The MENOPAUSE Booklet 36
Menopause Lifestyle eating and exercise plan
One of the many ways you can take charge of your own health and wellbeing throughout menopause is to adopt a healthy eating approach used in conjunction with undertaking a regular (daily) exercise regime. The benefits of nutrition and exercise are numerous and studies have indicated by purely changing your eating habits for the better you can significantly reduce your risk of breast cancer, heart disease, osteoporosis and many other ageing ailments whilst promoting energy, wellbeing and further supporting the reduction of menopausal symptoms.
Menopause is a time of change women will need to embrace with an open mind and educated brain. Certain dietary and lifestyle habits will need to be adjusted to suit their hormonal changes. Left unchanged, menopause can often lead to weight gain.
Refined sugars – Treat ‘treats’ as a treat, and not a regular thing
Refined carbohydrates and many packaged items, including soft drinks and refined fruit juices
Protein (meat, tofu, eggs etc.) with each meal. A portion would be considered
100g of meat or 200g of tofu.
Good fats regularly. Cook with olive oil or coconut oil.
A rainbow of vegetables, and lots of them.
A maximum of 2 pieces of fruit daily.
Snack on fresh fruit, unsalted nuts, a tin of tuna etc.
Conscious of your daily calcium intake; food or supplement.
Wary of your carbohydrate intake; this commonly encourages weight gain during menopause.
Lose Weight And feel Great
General Dietary Tips:
avoID
eaT
Be
The MENOPAUSE Booklet 37
To ensure that you are getting the most from your food, proper digestion and absorption must be addressed.
Eat in a relaxed environment
Chew you food slowly
Eat in moderation
Avoid multi-tasking at meal times
Try fresh lemon juice in warm water before meals to aid digestion
Foods to aid hormone production and communication Food can be a medicine for your hormones. Specific foods can affect chemical processes within the body, by reducing excessive production of oes-trogens, stimulating hormone detoxifica-tion and clearance and/or competitively and beneficially binding to oestrogen re-ceptors. The foods listed below have been shown to benefit women through their menopausal journey.
Ginger, rosemary, turmeric, coriander, dill,
fennel, parsley
Blueberries, strawber-ries, oranges, grapes, avocado, banana, figs,
blackberries Broccoli, cauliflower, Brussel sprouts, kale,
spinach, cabbage, mushrooms, celery,
onion, alfalfa sprouts
Milk, cheese and yoghurt (calcium-rich
alternative may be substituted), deep-sea
fish
Water, green tea, dan-delion tea, chamomile
tea, spearmint tea
Pumpkin seeds, sesame seeds, sunflower seeds,
almonds, cashews, Brazil nuts
Soy, chickpeas, quinoa, millet, bulgur,
buckwheat, brown rice
Tips To Promote Optimal Digestion Specific Dietary Strategies for Healthy Hormones
enjOY AT LeAST 1 frOM eACH GrOUP DAILY
Herbs and Spices
fruits and Vegetables Meat, poultry, fish and dairy
Beverages
nuts and Seeds Grains and Legumes
The MENOPAUSE Booklet 38
Contributors to Menopausal symptoms - Lifestyle Tips
The amount of stress within your life, and the way that you react to that stress can play a large role in how you experience menopause. Tips to reduce your stress include:
Regular aerobic and weight bearing exercise
Time out for yourself
Relaxation techniques
Play a musical instrument
Learn to draw, paint, knit or crochet
Clinical observation has showed us that alcohol intake can exacerbate hot flushes/night sweats.
Studies have shown moderate to high levels of alcohol consumptions to result in an increased risk of breast cancer. Increased risk was also noted at lower levels of consumption, equivalent to 1-2 drinks/day.
Stress Can Significantly Impact Your Menopause Symptoms
Alcohol Intake
If you cannot change the stress, change the way you view the stress.

The MENOPAUSE Booklet 39
The use of toxic plastics can interrupt, aggravate and mimic hormone communica-tion within the body. Exposing your body to these toxic chemicals should be ac-tively avoided. While no plastic can be considered 100% safe, we have provided a guide for which plastics to strictly avoid and which plastics have no known health effects (green). Avoiding plastics as much as possible and using glass alternatives is the best option.
recognise Bad Plastics
The MENOPAUSE Booklet 40
exercising Through MenopauseAlthough the research doesn’t directly show that exercise reduces menopausal symptoms, it has been shown to reduce stress, increase energy and reduce your waist line.
The benefits obtained from regular exercise can indirectly support and ease your transition through menopause. In addition to this, certain types of exercise can reduce your risk of osteoporosis and heart disease.
Starting an exercise program can be difficult, especially when you are facing hormonal symptoms, but the key is to remember that your main goal is to boost your health on multiple levels, whilst supporting your transition through menopause.
The MENOPAUSE Booklet 41
Often the trick is to pick a sport/exercise that you actually like.
The MENOPAUSE Booklet 42
australia’s physical activity and sedentary Behaviour Guidelines For adults (18-64years)
australia’s physical activity Recommendations For older australians (65years and older)
Doing any physical activity is better than doing none. If you currently do no physical activity, start by doing some, and gradually build up to the recom-mended amount.Be active on most, preferably all, days every week.Accumulate 150 to 300 minutes (2 to 5 hours) of moderate intensity physical activity or 75 to 150 minutes (1 to 2 hours) of vigorous intensity physical activi-ty, or an equivalent combination of both moderate and vigorous activities, each week.
Do muscle strengthening activities on at least 2 days each week
Minimise the amount of time spent in prolonged sitting.Break up long periods of sitting as often as possible
Physical Activity Guidelines
Sedentary Behaviour Guidelines
Being physically active and staying fit and healthy will help you to get the most out of life, whatever your age. These recommendations are designed to help older Australians achieve sufficient physical activity for good health as they age.
Physical Activity recommendations
Older people should do some form of physical activity, no matter what their age, weight, health problems or abilities.
1 |

The MENOPAUSE Booklet 43
Good exercises for Peri- And Post- Menopausal Women
Moderate to brisk walking. Experts agree that walking is the best form of ex-ercise for post-menopausal women as it can be done anywhere, anytime and promotes social interaction.
Light to moderate weight training. This will help to build muscle mass and keep muscle tone. This can also help to support metabolism, improve body composi-tion and increase overall health.
Moderate to low impact aerobics. This is great for increasing heart and respira-tory rates, which helps to keep the vital organs healthy.
Light to moderate resistance training. Particularly for women worried about their bone health. An improvement to bone strength is site-specific; those bones attached to the exercised muscles are affected. Choose exercises to strengthen the small and large muscle groups of the spine and hip, the most common sites of osteoporotic fractures.
Relaxation based exercise (e.g. yoga), especially for those with hot flushes. Re-laxation based exercises with paced respiration may significantly reduce objec-tively measured hot flush occurrence.
For both cardiovascular and strength training exercises, remember to increase the amount of exercise gradually, starting with realistic amounts and moving towards achieving the guidelines stated above. Exceeding the minimum recommendations further reduces the risk of inactivity-related chronic disease and may be helpful in improving symptoms of menopause.
Older people should be active every day in as many ways as possible, doing a range of physical activities that incorporate fitness, strength, balance and flexibility.
Older people should accumulate at least 30 minutes of moderate intensity physical activity on most, preferably all, days.
Older people who have stopped physical activity, or who are starting a new physical activity, should start at a level that is easily manageable and gradually build up the recommended amount, type and frequency of activity.
Older people who continue to enjoy a lifetime of vigorous physical activity should carry on doing so in a manner suited to their capability into later life, provided recommended safety procedures and guidelines are adhered to.
2 |
3 |
4 |
5 |

The MENOPAUSE Booklet 44
Check for osteoporosis
The majority of women are at risk for osteoporosis during and after the meno-pause. You may have a higher risk of suffering the effects of osteoporosis if you:
we recommend that you have a baseline bone scan early on in your menopause, especially if there is a family history of osteoporotic fractures.
The bone scan is called a DEXA scan (Dual Energy Xray Absorptiometry scan) and is similar to having a normal X-ray (with no pain). Thereafter, and in consulta-tion with your general practitioner, a scan every two to three years should be suffi-cient to monitor your progress.
have a family history of osteoporosis
do little or no physical activity
are a current cigarette smoker
have a high alcohol intake
have a low body weight
if you are Caucasian or Asian
had delayed puberty
had early onset of menopause
had a previous osteoporotic fracture
over 60 years of age
have chronic liver disease, rheumatoid arthritis or kidney failure
have a history of over-active thyroid or parathyroid glands or past treatment
with thyroid hormones
have had long term treatment with corticosteroids
Because it is better to prevent a serious fracture than to treat one
The MENOPAUSE Booklet 45
What The Man In Your Life Can Do To Help!
Menopause is a defining moment in a woman’s life. Sure, it has its ups and downs but with a positive outlook it can be a time of empowerment. But most women cannot do it alone. They need the support of their family and friends ~ and in par-ticular the men in their lives. For those men, we have come up with the following list of useful tips:
Imagine what it would be like to go through times of sleepless nights, hot flushes, and the like. I suspect your mood would not be great all the time.
For a time it may seem your wife is no longer the woman you married. Not true! Appreciate that this roller coaster will pass and that you will both come out the other side much closer.
While her sex drive may dip a little, it does not have to be dormant. Now there are many ways to deal with it. Be resourceful, be creative, keep it fun, and do not be judgmental or rush to conclusions.
Imagine how impressed your partner would be if you knew that the reason she was having hot flushes is most likely because her oestrogen levels are low. Find some literature and read it. Remember, education is empowerment!
This is the perfect time in your life together, to encourage her to seek outwomen’s groups, new friendships and old friends going through the same ex-perience.
It may not be politically correct but menopause can be funny. Try and make her laugh and see the lighter side of things. After all, laughter is the best medi-cine.
Put yourself in her position
Your marriage is not falling apart
Sex? It still exists. just don’t panic
educate yourself
Duck and swerve
keep your sense of humour
The MENOPAUSE Booklet 46
We are Here To Help
At AMC we view ourselves as your resource for advice and counsel at this im-portant stage of your life. Moreover, we understand that every woman is different which is why we place high importance on ongoing patient communication, evalu-ation and support.
We have a full-time clinical team. They are trained and familiar with the program and are available for phone appointments. You can make an appointment them to discuss your medication dosages or treatment program.
Following is a summary of the support we offer Australian Menopause Centre patients:
We will be in regular contact with you. This will be your opportunity to provide us with valuable feedback on the progress of your treatment program. If required, your AMC consultant will book a time for a medical review.
Call this number if you have any questions about your medication, side-effects that you may be experiencing or any other question about your treatment program.
Our AMC hotline is staffed by trained patient care representatives. They can refer you to our clinical staff who have extensive experience in women’s health issues. You can call this number Monday to Friday between the hours of 8.30am and 5.30pm (EST time) to schedule an appointment (a medical advisor will then call you back at a mutually convenient time).
You can email any time and expect a response sometimes beyond these hours. We provide clinical appointments from 8.00am EST until 6.30pm EST as well as Saturdays from 9.00am – 1.00pm.
Patient Care Call
AMC Help Line - 1300 883 405

The MENOPAUSE Booklet 47
We collect personal information (including health information) about you in various ways to enable us to provide you with our services, and need you to consent to us disclosing it. For example, we collect information when you request an appoint-ment with one of our doctors; this will allow them to provide you with medical advice. We only collect the information we need to fulfill the purpose of collection, and if we do not receive it we will not be able to provide you with our services. You have the right to access the information we hold about you at any time.
There is no fee for access, but we may charge reasonable expenses of supplying information depending on the request. If you would like access please call our help line on 1300 883 405. We take all reasonable steps to ensure your health and other personal information is kept secure from unauthorised access or disclosure, up-to-date and accurate.
We will not sell your personal information to anyone, but in providing you our services we may disclose it as required to others (including transmitting electroni-cally). When we do so they are we required to handle the information in the same way we do. For example we may disclose your personal information:
We may write or email you about additional services we or other organisations offer if we think they might benefit you. If you do not want us to communicate in that way please let us know by calling our help line on 1300 883 405.
Your Privacy Is Important To Us
private Health Fund Rebate
privacy
If you belong to a private health fund you may be eligible for a rebate on the med-ical component of your treatment program. Please contact your health fund to receive the most up to date listing of claimable medications.
To enable the pharmacy to prepare and dispense your medication;
When another organisation helps us process transactions, store or access data or provide services to you so they can perform their role;
Where laws require or allow us to provide information to a government agency or organisation.
The MENOPAUSE Booklet 48
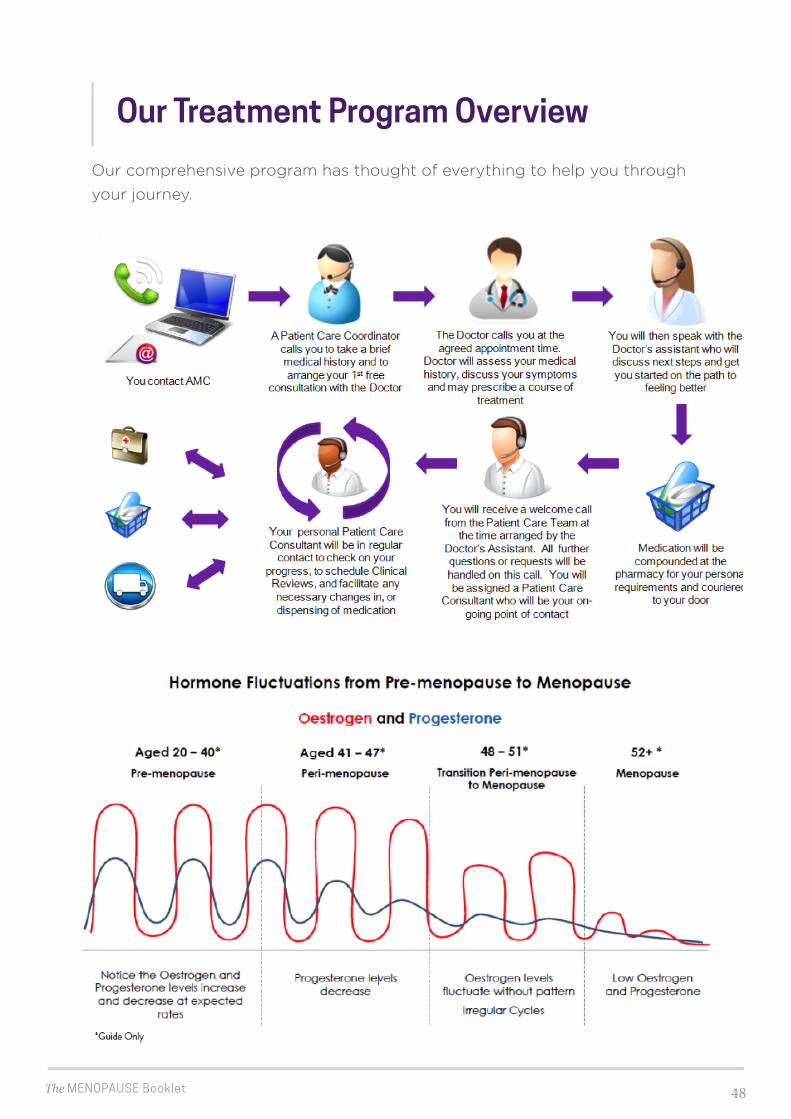
our Treatment program overview
Our comprehensive program has thought of everything to help you through your journey.

The MENOPAUSE Booklet 49