autoinflammatoire aandoeningen - internisten...hyper-igd syndroom (hids) oftwel mevalonaat kinase...
TRANSCRIPT

Autoinflammatoire aandoeningen
Anna Simon
Radboudumc Expertiscentrum Immuundeficientie en Autoinflammatie Afd Interne Geneeskunde Radboudumc Nijmegen

Casus: 45-jarige Nederlandse vrouw
• Sinds leeftijd <1 jr, 3-4x per jaar, duur: 5-7 dgn
• Koorts, stijve gewrichten, aften, lymfadenopathie
• Uitlokkende factor: vaccinaties, stress
• VG: oa 41 jr vasculitis benen
• Familie: gb
• CRP tijdens aanval: 230 mg/L
• IgD 1200 U/ml (nl <100)
• IgA 6.46 g/L
• DNA diagnostiek: V377I + I268T mutaties in mevalonaat kinase gen
• mevalonaat kinase deficientie, ook bekend als hyper-IgD
syndroom
• Goede response op anakinra ‘on demand’, later goede respons op
canakinumab
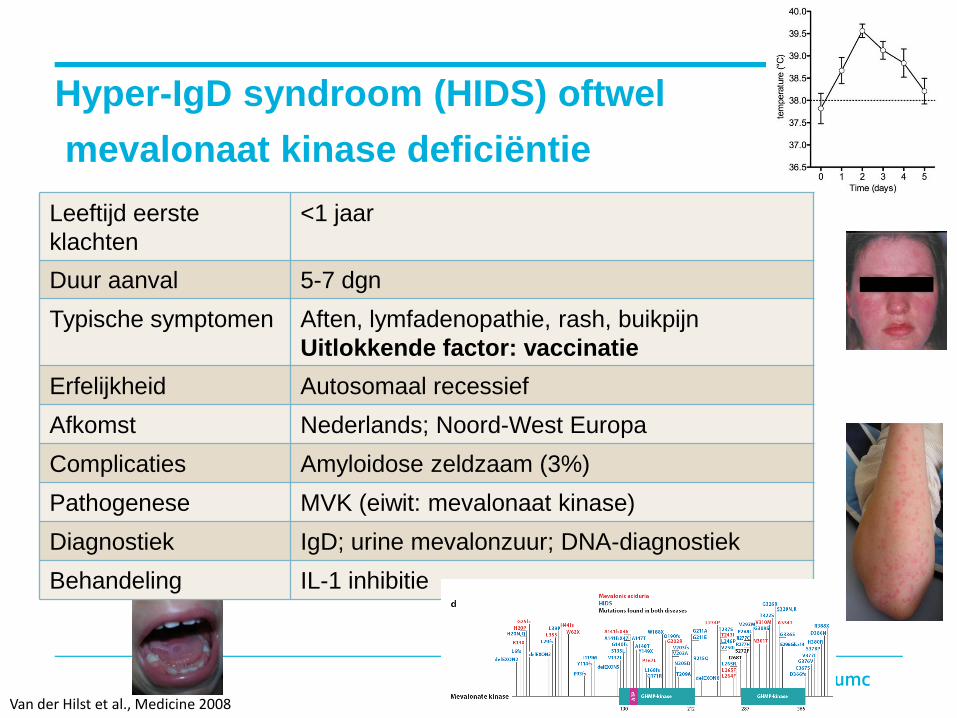
Hyper-IgD syndroom (HIDS) oftwel
mevalonaat kinase deficiëntie
Van der Hilst et al., Medicine 2008
Leeftijd eerste
klachten
<1 jaar
Duur aanval 5-7 dgn
Typische symptomen Aften, lymfadenopathie, rash, buikpijn
Uitlokkende factor: vaccinatie
Erfelijkheid Autosomaal recessief
Afkomst Nederlands; Noord-West Europa
Complicaties Amyloidose zeldzaam (3%)
Pathogenese MVK (eiwit: mevalonaat kinase)
Diagnostiek IgD; urine mevalonzuur; DNA-diagnostiek
Behandeling IL-1 inhibitie

Pathofysiologie mevalonaat kinase deficientie
Acetyl-CoA + Acetoacetyl-CoA
Cholesterol
Isopentenyl Adenine (tRNA)
Dolichol
Haem A
Ubiquinone
Isoprenylation of proteins
(e.g. RAS, lamin B)
HMG-CoA
Isopentenyl-PP
Geranyl-PP
Farnesyl-PP
Mevalonate-PP
Mevalonate
Mevalonate-P
HO S-CoA
O OHO
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
HO OP
OOH
HO S-CoA
O OHO
HO S-CoA
O OHO
OPPOPP
OPPOPP
OPPOPP
HO OPP
OOH
HO OPP
OOH
HO OH
OOH
HO OH
OOH
HO OP
OOH
HO OP
OOH
Steroid Hormones
Vitamin D
Bile Acids
Lipoproteins
Steroid Hormones
Vitamin D
Bile Acids
Lipoproteins
HMG-CoA reductaseHMG-CoA reductase
mevalonate kinasemevalonate kinase Deficientin HIDS
Acetyl-CoA + Acetoacetyl-CoA
Cholesterol
Isopentenyl Adenine (tRNA)
Dolichol
Haem A
Ubiquinone
Isoprenylation of proteins
(e.g. RAS, lamin B)
HMG-CoA
Isopentenyl-PP
Geranyl-PP
Farnesyl-PP
Mevalonate-PP
Mevalonate
Mevalonate-P
HO S-CoA
O OHO
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
Acetyl-CoA + Acetoacetyl-CoA
Cholesterol
Isopentenyl Adenine (tRNA)
Dolichol
Haem A
Ubiquinone
Isoprenylation of proteins
(e.g. RAS, lamin B)
HMG-CoA
Isopentenyl-PP
Geranyl-PP
Farnesyl-PP
Mevalonate-PP
Mevalonate
Mevalonate-P
HO S-CoA
O OHO
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
HO OP
OOH
HO S-CoA
O OHO
HO S-CoA
O OHO
OPPOPP
OPP
OPP
OPP
OPP
HO OPP
OOH
HO OH
OOH
HO OP
OOH
HO S-CoA
O OHO
HO S-CoA
O OHO
OPPOPP
OPPOPP
OPPOPP
HO OPP
OOH
HO OPP
OOH
HO OH
OOH
HO OH
OOH
HO OP
OOH
HO OP
OOH
OPP
OPPOPP
HO OPP
OOH
HO OPP
OOH
HO OH
OOH
HO OH
OOH
HO OP
OOH
HO OP
OOH
Steroid Hormones
Vitamin D
Bile Acids
Lipoproteins
Steroid Hormones
Vitamin D
Bile Acids
Lipoproteins
HMG-CoA reductaseHMG-CoA reductase
mevalonate kinasemevalonate kinase Deficientin HIDS
Simon, A et al. Clin Pharmacol Ther 2004; 75: 476-83.
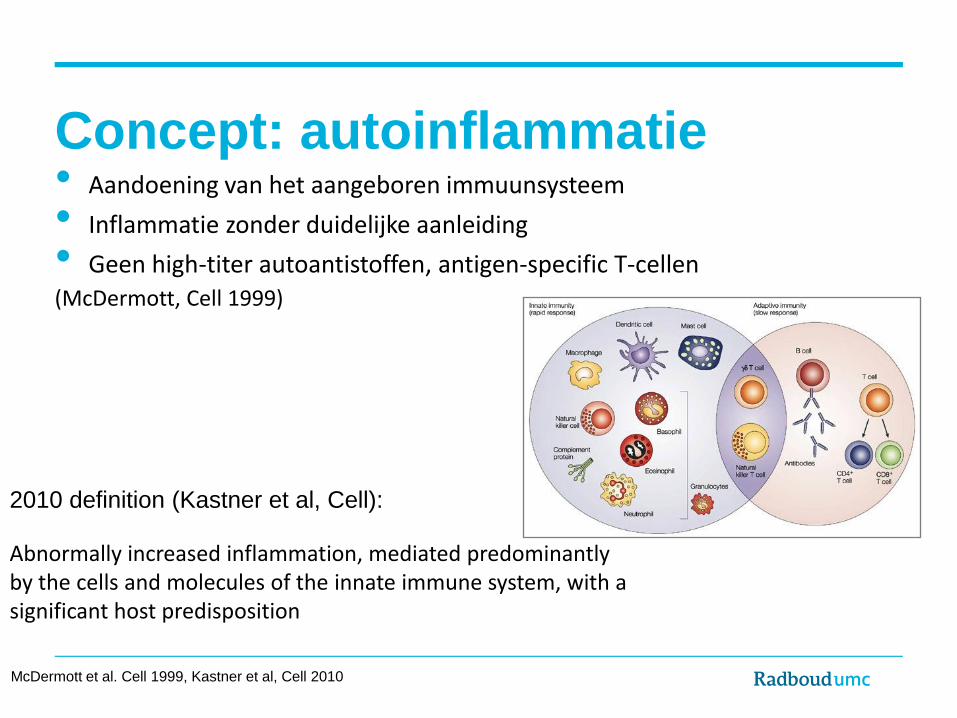
Concept: autoinflammatie • Aandoening van het aangeboren immuunsysteem
• Inflammatie zonder duidelijke aanleiding
• Geen high-titer autoantistoffen, antigen-specific T-cellen (McDermott, Cell 1999)
McDermott et al. Cell 1999, Kastner et al, Cell 2010
2010 definition (Kastner et al, Cell):
Abnormally increased inflammation, mediated predominantly by the cells and molecules of the innate immune system, with a significant host predisposition

Autoinflammatie vs autoimmuniteit
Schade ten gevolge van inflammatie gericht tegen het eigen lichaam, door:
• Autoimmuniteit: afwijkende respons van T- en B-cellen (en dendritische cellen) defect in tolerantie immuunreactie tegen eigen antigenen (fout in self/non-self herkenning)
• Autoinflammatie: lokaal, intrinsiek defect waardoor cellen van het
aangeboren immuunsysteem te sterk geactiveerd worden (bv ontregeld
inflammasoom)
NB dus ook onderscheid van inflammatie
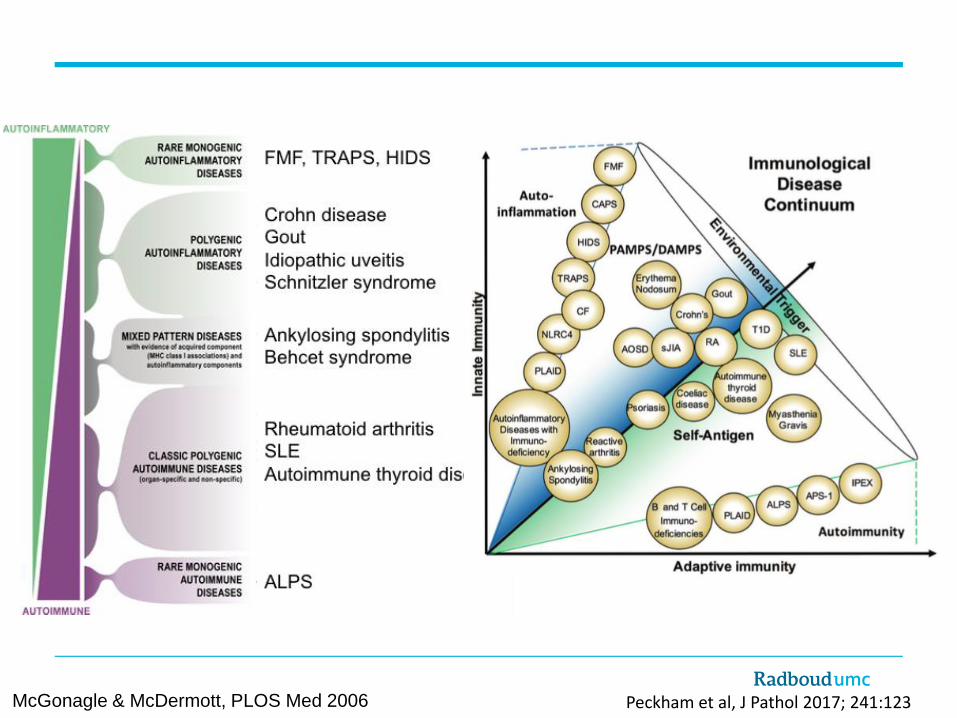
McGonagle & McDermott, PLOS Med 2006 Peckham et al, J Pathol 2017; 241:123

Monogenetische erfelijke autoinflammatoire syndromen
(aka ‘periodieke koorts syndromen’)
Syndrome Inherited Mutated protein
Cryopyrin-associated periodic syndrome includes: - Muckle-Wells syndrome (MWS) - Familial Cold Autoinflammatory syndrome (FCAS) - CINCA/NOMID
CAPS Dominant NLRP3 (= cryopyrin)
Familial Mediterranean Fever FMF Recessive Pyrin
TNF-receptor associated periodic syndrome
TRAPS Dominant TNF-receptor 1
Hyper-IgD syndrome/ mevalonate kinase deficiency
HIDS/MKD
Recessive Mevalonate kinase

Gemeenschappelijk fenotype recidiverende koortssyndromen • Levenslang terugkerende episoden met ontsteking
• Koorts
• Buikpijn, diarrhee
• Huiduitslag
• Arthralgie, myalgie
• Lymphadenopathie
• Acute fase respons
• Vaak geen duidelijke oorzaak
• Autosomaal overerving
• Gevreesde complicatie: amyloidosis

Overeenkomsten achtergrond
Ozen & Bilginer, Nat Rev Rheum 2014, 10:135
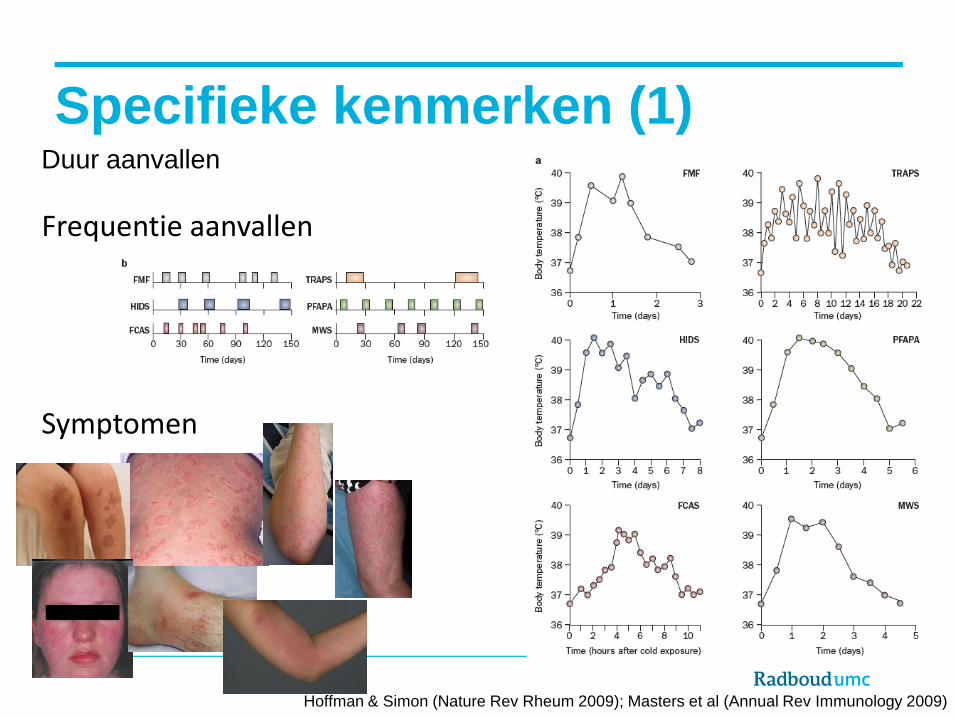
Specifieke kenmerken (1) Duur aanvallen
Hoffman & Simon (Nature Rev Rheum 2009); Masters et al (Annual Rev Immunology 2009)
Frequentie aanvallen
Symptomen

Specifieke kenmerken (2) Triggers: kou vaccinatie
Hoffman & Simon (Nature Rev Rheum 2009); Masters et al (Annual Rev Immunology 2009)
Afkomst familie
Colchicine

Uitbreiding van het autoinflammatoire spectrum • Deficiency of IL-1receptor antagonist (DIRA)
• Blau syndrome (NOD2): granulomatous disorder • Interferonopathies: SAVI, AGS, AGS-like • Proteasome-associated disorder (PRAAS)
• NLRC4-associated disorder • PAPA (PSTPIP1 gene): pyogenic inflammation • DITRA (IL-36ra): pustular psoriasis
• Ubiquitination regulation defects: HA20, LUBAC deficiency, otulipenia • Deficiency of ADA2: vasculitis • Phospholipase-associated autoinflammatory disorder (PLAID)
And more. (And this is just the monogenic ones) Some combination with autoimmunity, some with immunodeficiency
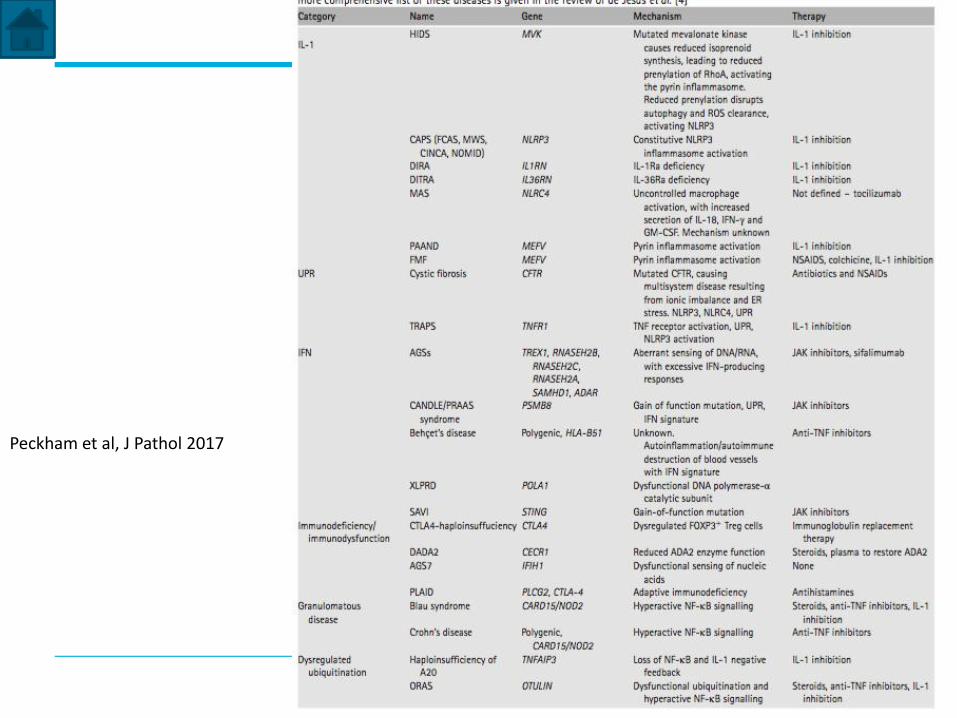
Peckham et al, J Pathol 2017

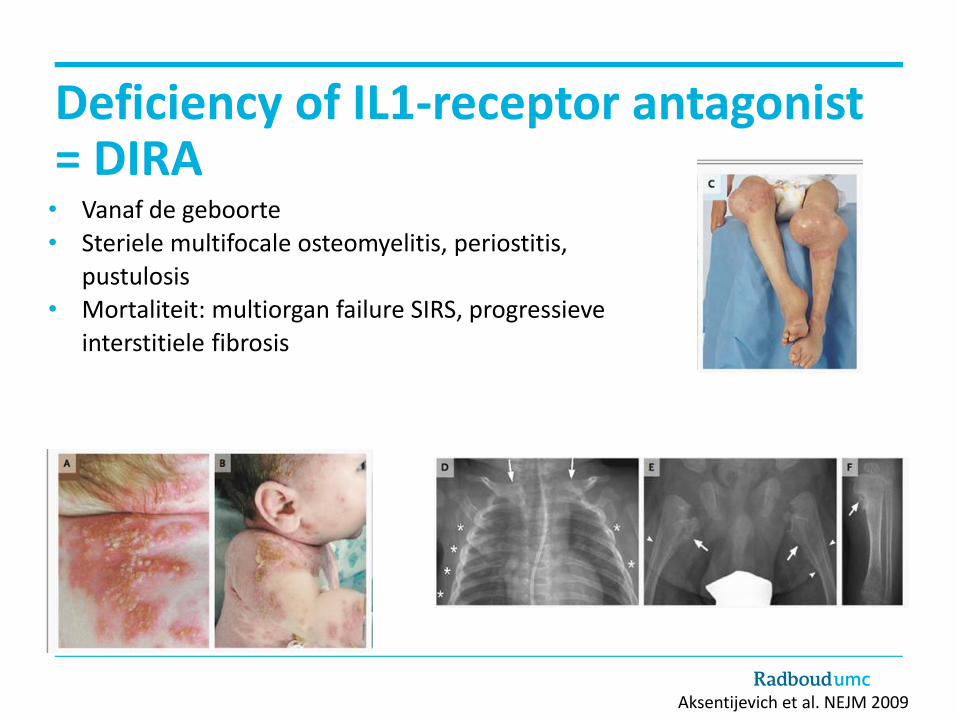
Deficiency of IL1-receptor antagonist = DIRA • Vanaf de geboorte
• Steriele multifocale osteomyelitis, periostitis, pustulosis
• Mortaliteit: multiorgan failure SIRS, progressieve
interstitiele fibrosis
Aksentijevich et al. NEJM 2009
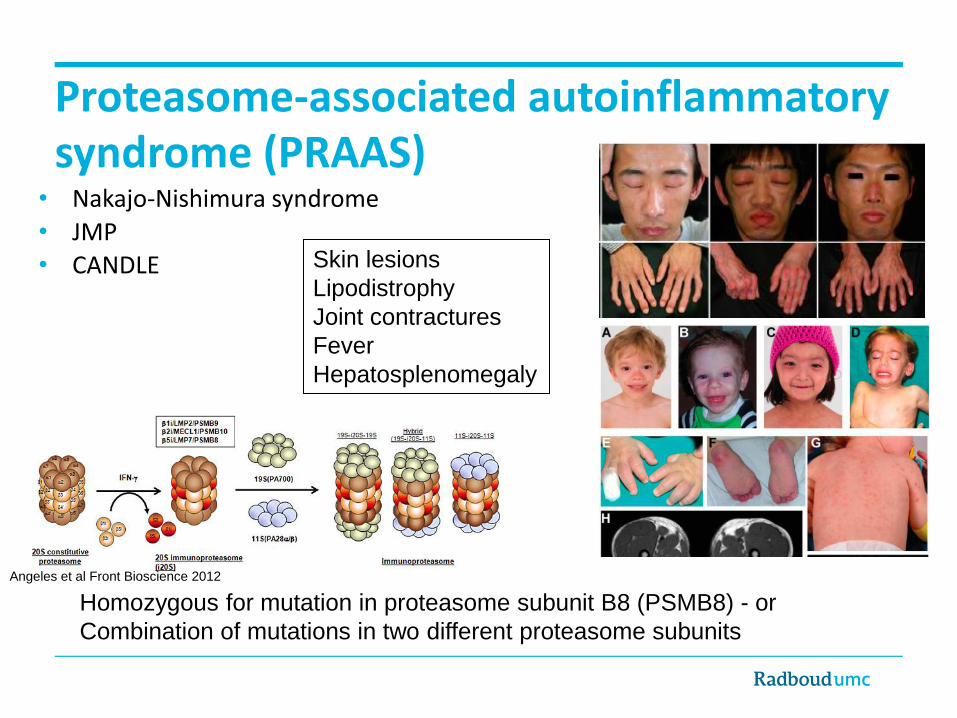
• Nakajo-Nishimura syndrome
• JMP • CANDLE Skin lesions
Lipodistrophy
Joint contractures
Fever
Hepatosplenomegaly
Homozygous for mutation in proteasome subunit B8 (PSMB8) - or
Combination of mutations in two different proteasome subunits
Angeles et al Front Bioscience 2012
Proteasome-associated autoinflammatory syndrome (PRAAS)
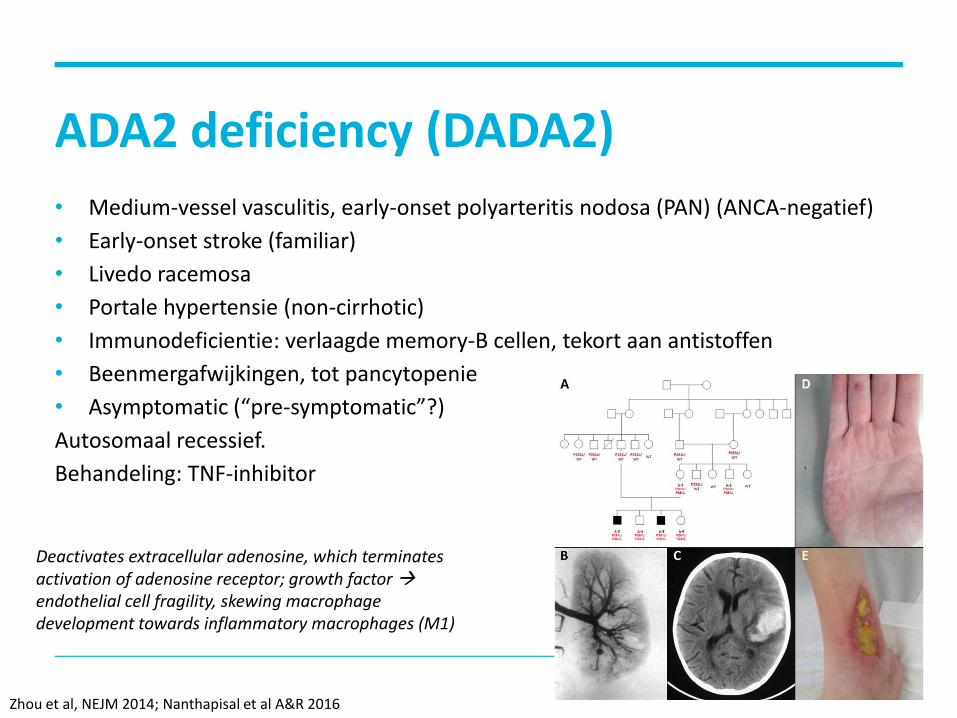
ADA2 deficiency (DADA2)
• Medium-vessel vasculitis, early-onset polyarteritis nodosa (PAN) (ANCA-negatief)
• Early-onset stroke (familiar)
• Livedo racemosa
• Portale hypertensie (non-cirrhotic)
• Immunodeficientie: verlaagde memory-B cellen, tekort aan antistoffen
• Beenmergafwijkingen, tot pancytopenie
• Asymptomatic (“pre-symptomatic”?)
Autosomaal recessief.
Behandeling: TNF-inhibitor
Zhou et al, NEJM 2014; Nanthapisal et al A&R 2016
Deactivates extracellular adenosine, which terminates activation of adenosine receptor; growth factor endothelial cell fragility, skewing macrophage development towards inflammatory macrophages (M1)
Heeft mijn patiënt een (klassiek erfelijk)
autoinflammatoir syndroom?
• Gedetailleerde anamnese
• Patient zien tijdens een ’episode’:
• Zien hoe ziek hij is
• Controleer CRP • Exclusie van andere diagnoses (infectie, maligniteit, autoimmuun), b.v.
Febris eci protocol
Age of onset Duur episoden Tijdsinterval Bijkomende verschijnselen Triggers / verlichtende factoren Ontwikkeling in de tijd Behandelingen eerder gegeven Familie geschiedenis, ethniciteit

Differentiaal diagnose
Hoffman & Simon (Nature Rev Rheum 2009)
+ ethnic origin
+ age of onset

Volgende stap in diagnose
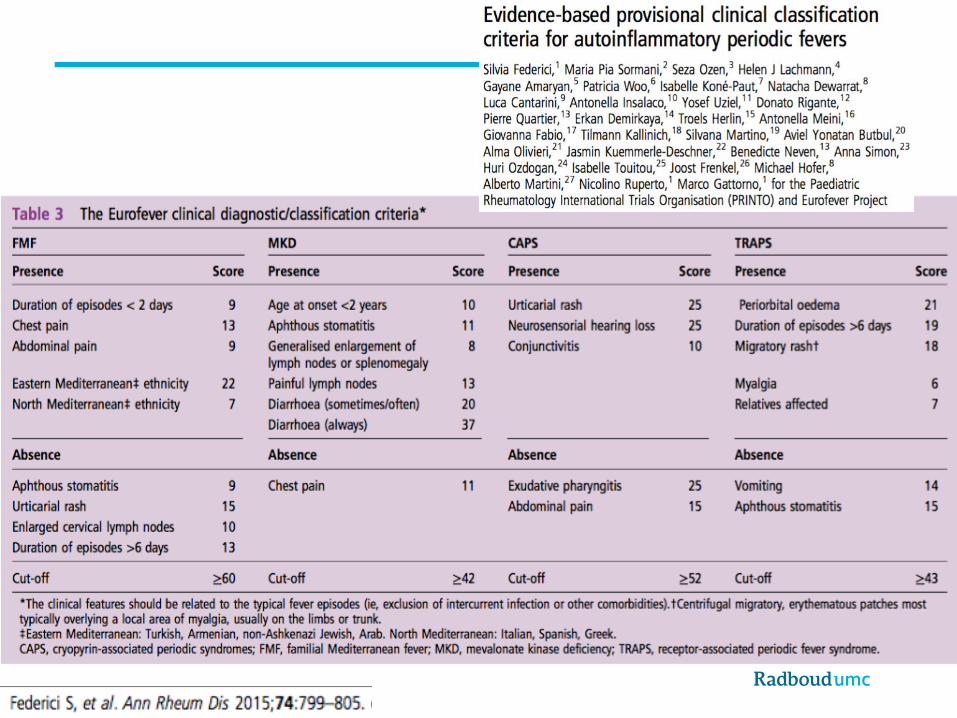
• Klinische criteria
• Genetica: specifiek gen of autoinflammatoir genen panel NGS • Specifieke andere testen, bv:
• IgD
• Mevalonzuur in urine • Respons op colchicine • M proteine
• ADA2 activiteit

Casus: Hyper-IgD syndroom?
• Verwijzing via huisarts: patient vraagt zelf om 2e mening na diagnose
hyper-IgD syndroom in ander ziekenhuis • Man, 34 jaar. Sinds 1 jaar episoden met koorts, 1x/mnd, duurt 7-8 dgn.
Verschijnselen: koorts, hoesten, hoofdpijn, vermoeidheid, lymfadenopathie
• CRP tijdens koorts 94 mg/L, IgD 420 mg/L (nl <140) • Voorgeschiedenis: op lft 24 jr: Hodgkin lymfoom st IIA
recidief Hodgkin lymfoom

CAPS – of toch niet? • Verwijzing via dermatoloog, 35 jaar oude man • Sinds lft 27 jaar, aanvallen met koorts: duur 2 dgn, 4-10x/ jaar • Bijkomende verschijnselen: erythemateuze uitslag, algehele malaise,
rugpijn, lymfadenopathie (liezen)
• Triggers: stress, drukte • Behandeling tot nu toe: NSAIDs, paracetamol. • Familie-anamnese: vader psoriasis, verder negatief

CAPS – of niet? (2)
• Tijdens aanval gezien:
• Hoge piekende koorts en huiduitsalg • CRP tot 200 mg/L.
NLRP3 gen: Leu677Pro mutatie
Masters et al. Annu Rev Immunol 2009

CAPS of niet? (3) onder anakinra / prednison
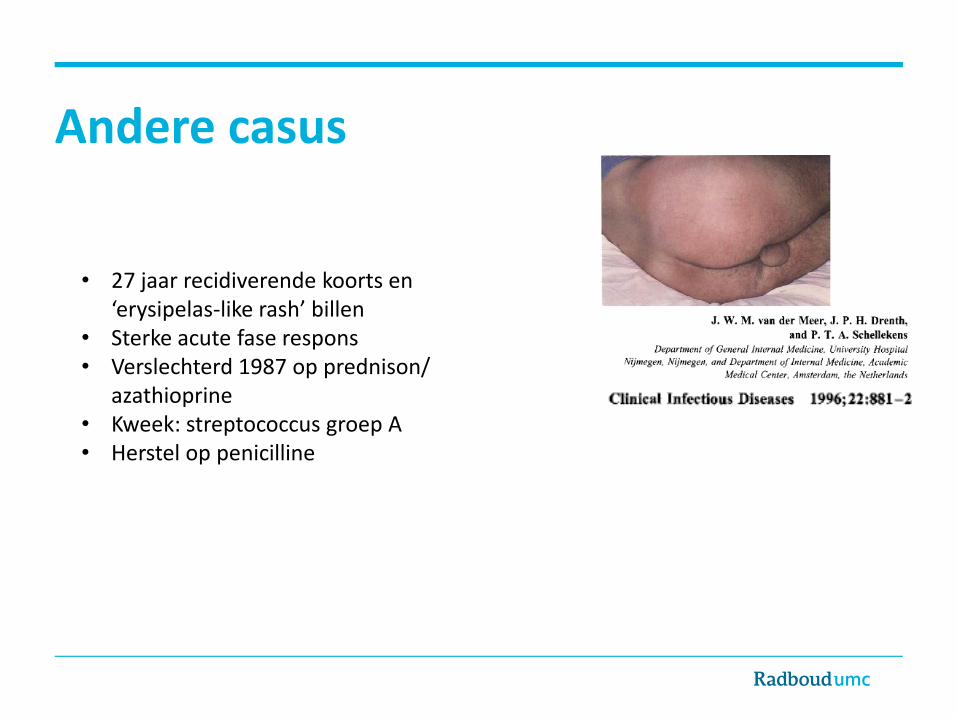
Andere casus
• 27 jaar recidiverende koorts en ‘erysipelas-like rash’ billen
• Sterke acute fase respons • Verslechterd 1987 op prednison/
azathioprine • Kweek: streptococcus groep A • Herstel op penicilline

CAPS of niet? (4) niet!
• Kweek perineum: hemolytische streptococcus gr C; AST: 800 IE/ml.
• Clindamycine 3 dd 600 mg voor 10 dgn (november 2012). • Geen klachten meer sinds die tijd
Diagnose: • Recidiverende erysipelas met streptococcus (spontaan herstel)
• Complicaties van onze immunosuppressiva
• NLRP3 variant waarschijnlijk toevalsbevinding(Leu677Pro)

Berucht: polymorfismen of laag-penetrante
mutaties
“Co-existent TRAPS” etc
Heightened inflammation trait
A Case of Tumor Necrosis Factor Receptor-Associated Periodic Fever Syndrome in a 58-Year-Old Man: Caution Not to Discount TRAPS as a Diagnosis in Older Patients.
Familial clustering of recurrent pericarditis may disclose tumour necrosis factor receptor-associated periodic syndrome.
TNF receptor-associated periodic syndrome (TRAPS): a new cause of joint destruction?
Overlap syndrome between FMF and TRAPS in a patient carrying MEFV and TNFRSF1A mutations.
Late-onset tumor necrosis factor receptor-associated periodic syndrome in multiple sclerosis patients carrying the TNFRSF1A R92Q mutation.
Severe TNF receptor-associated periodic syndrome due to 2 TNFRSF1A mutations including a new F60V substitution.
Gene Mutation
MEFV E148Q
TNFRSF1A R92Q (R121Q)
P46L (P75L)
NLRP3 V198M

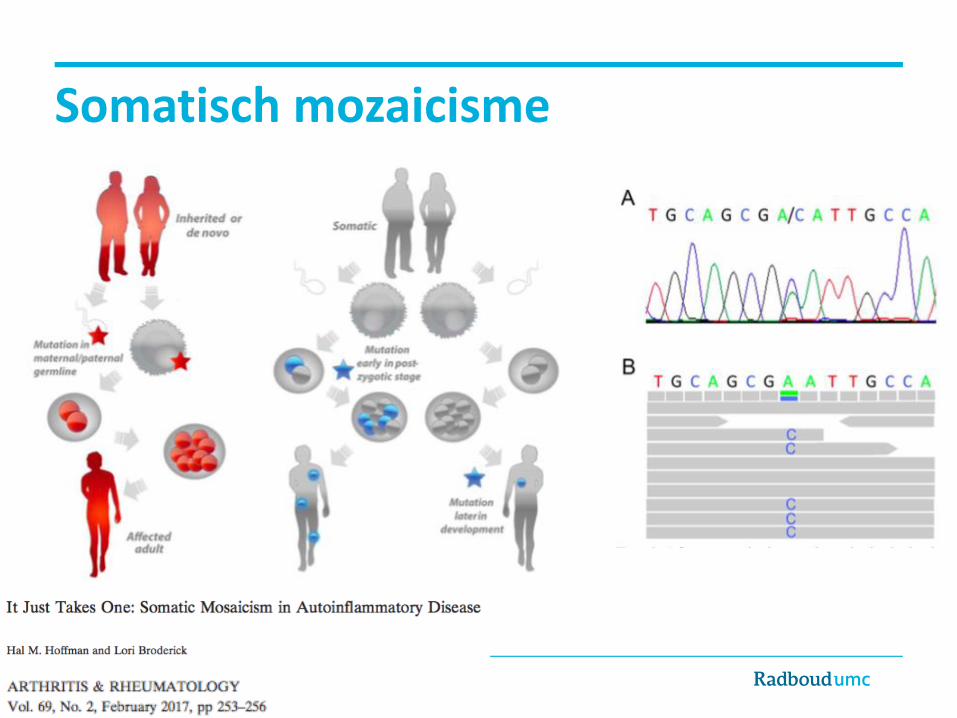
Somatisch mozaicisme
Adapted from http://www.proteus-syndrome.org.uk/
Tot nu toe beschreven in:
• CAPS (NLRP3)
• Schnitzler syndrome (NLRP3)
• TRAPS (TNFRSF1A)
• Blau syndrome (NOD2)
Somatisch mozaicisme

Diagnostic criteria Schnitzler syndrome • Obligatory criteria:
• Chronic urticarial rash • M-protein, IgM or IgG*
• Minor criteria:
• Recurrent fever • Abnormal bone remodelling +/- bone pain (bone scan, MRI) • Neutrophilic infiltrate in skin biopsy
• Leukocytosis and/or raised CRP
Definitive diagnosis: 2 obligatory criteria + 2 minor (IgM) or 3 minor (IgG)
Probable diagnosis: 2 obligatory criteria + 1 minor (IgM) or 2 minor (IgG)
Simon et al. Allergy 2013
* NB sometimes M-protein appears only after years follow-up – so criteria not perfect

NLRP3 mutations in 2 patients with Schnitzler syndrome
Mutation in NLRP3 gene Whole exome • Patient A: 17% of blood cells
Deep sequencing NLRP3 • Patient A: 8% (F523L) • Patient B: 27% (K435E)
De Koning et al, JACI 2015

In keratinocytes or fibroblasts: A: 0% A: 0% B: 0% B: 0%
Adapted from Wikipedia
Mutation in whole blood: Patient A: 8% Patient B: 27%
A: 7% B: 29% A: 13%
B: 32%
A: 0% B: 0%
A: 0% B: 0%
De Koning et al, JACI 2015

International resources
• ISSAID: international society
• Infevers: international genetics database & community • Registries: eg Eurofever • Orphanet
http://www.issaid2019.org/
Conclusies
• Autoinflammatie vs autoimmuniteit
• Zien tijdens klachten! • Overleg met ervaren collega/3e lijn • Niet in de luren laten leggen door uitslag genetica
• Niet bang zijn diagnose te heroverwegen