basal insulin peglispro demonstrates preferentialhepatic
TRANSCRIPT

Basal Insulin PeglisproDemonstrates Preferential HepaticVersus Peripheral Action Relativeto Insulin Glargine in HealthySubjectsDiabetes Care 2014;37:2609–2615 | DOI: 10.2337/dc14-0210
OBJECTIVE
We evaluated the endogenous glucose production (EGP) and glucose disposal rate(GDR) over a range of doses of basal insulin peglispro (BIL) and insulin glargine inhealthy subjects.
RESEARCH DESIGN AND METHODS
This was a single-center, randomized, open-label, four-period, incomplete-block,crossover study conducted in eight healthy male subjects. Subjects had 8-h eugly-cemic clamps performed with primed, continuous infusions of BIL (5.1 to 74.1mU/min) in three dosing periods and insulin glargine (20 or 30 mU/m2/min) in afourth period, targeted to achieve 50–100% suppression of EGP. D-[3-3H] glucosewas infused to assess rates of glucose appearance and disappearance.
RESULTS
Mean BIL and insulin glargine concentrations (targeted to reflect the differences inintrinsic affinities of the two basal insulins) ranged from 824 to 11,400 and 212 to290 pmol/L, respectively, and increased accordingly with increases in dose. Sup-pression of EGP and stimulation of GDR were observed with increasing concen-trations of both insulins. At insulin concentrations where EGP was significantlysuppressed, insulin glargine resulted in increased GDR. In contrast, at comparablesuppression of EGP, BIL had minimal effect on GDR at lower doses and had sub-stantially less effect on GDR than insulin glargine at higher doses.
CONCLUSIONS
The novel basal insulin analog BIL has relative hepatopreferential action and de-creased peripheral action, compared with insulin glargine, in healthy subjects.
In vivo, insulin is secreted from pancreatic b-cells and enters the circulation via theportal vein, where on first pass the liver extracts ;40–80% (1–7). As a result,systemic circulating insulin levels are reduced compared with those in the portalvein, and subsequent insulin action in the peripheral target tissues is also reducedcompared with the liver. Consequently, the relative ratio of hepatic action to pe-ripheral action ranges between 2:1 and 4:1 (1,2,4,8–10). In contrast, when exoge-nous insulin is administered peripherally, insulin is distributed equally across theliver and peripheral tissues (11,12) and thus does not mimic normal physiology.
1Center for Metabolic Research, VA San DiegoHealthcare System, San Diego, CA2University of California, San Diego, La Jolla, CA3Eli Lilly and Company, Indianapolis, IN4Eli Lilly and Company, Singapore, Singapore
Corresponding author: Helle Linnebjerg,[email protected].
Received 22 January 2014 and accepted 19 May2014.
Clinical trial reg. no. NCT01654380, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc14-0210/-/DC1.
V.P.S. is currently affiliated with the Office ofClinical Pharmacology, Center for Drug Evalua-tion and Research, U.S. Food and Drug Adminis-tration, Silver Spring, MD.
© 2014 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
Robert R. Henry,1,2 Sunder Mudaliar,1,2
Theodore P. Ciaraldi,1,2
Debra A. Armstrong,1 Paivi Burke,1
Jeremy Pettus,2 Parag Garhyan,3
Siak Leng Choi,4 Scott J. Jacober,3
Mary Pat Knadler,3 Eric Chen Quin Lam,4
Melvin J. Prince,3 Namrata Bose,2
Niels Porksen,3 Vikram P. Sinha,3 and
Helle Linnebjerg3
Diabetes Care Volume 37, September 2014 2609
PATH
OPHYSIO
LOGY/COMPLIC
ATIO
NS
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022

Intraperitoneal administration of insulinvia implanted infusion pumps has beenpursued experimentally (13,14) to at-tempt to restore this physiologic balanceand provide the potential benefits com-pared with existing exogenous insulintherapy (15).Basal insulin peglispro (BIL; LY2605541),
a novel, polyethylene glycolylated insulinanalog currently in phase III, has a hepa-topreferential action and decreased pe-ripheral action in an insulinopenic dogmodel (16). The half-life of BIL is ;2 to3 days (17) and therefore requires;7 to10 days to reach steady state whenadministered subcutaneously. However,under experimental conditions for short-term studies, more rapid attainment ofsteady state can be achieved by intrave-nous infusion. BIL has reduced affinity forthe insulin receptor compared with insu-lin lispro (18) and a volume of distribu-tion that is only slightly larger than thecirculating blood volume (19), thus lowerthan that reported for insulin lispro andregular human insulin (20). The highersystemic circulating BIL levels (likeinsulin detemir [15]) reflect the differ-ences in in vitro insulin receptor–bindingaffinity (Ki) and volume of distribution. Inphase II trials in type 1 and type 2diabetes, in which BIL showed similarglycemic-lowering to insulin glargine(21,22), the steady-state BIL concentra-tions were estimated to be ;3,200 and4,300 pmol/L, respectively.Additionally, these phase II studies
(21,22) demonstrated that BIL com-pared with insulin glargine was associ-ated with lower rates of nocturnalhypoglycemia, weight loss, and a lackof suppression of serum triglycerides.In patients with type 1 diabetes (21),these findings were also associated witha modest increase in LDL cholesterol, amodest decrease in HDL cholesterol, anda higher rate of total hypoglycemia,which were noted with both a lowerhemoglobin A1c and lower dose of pran-dial insulin. All these findings led tothe speculation that BIL may havelower peripheral action, which may re-sult in a relative hepatopreferencecompared with insulin glargine. This hy-pothesis was first confirmed in an acutedog model of insulinopenic diabetes(somatostatin and portal glucagon-infused conscious, fasted dogs), whereintravenous infusions of BIL and humaninsulin were compared (16). The results
suggested that BIL may restore thephysiologic ratio of hepatic to periph-eral insulin action.
The aim of this present study was todetermine in humans a dose response ofintravenous infusions of BIL comparedwith an intravenous infusion of insulinglargine with regard to suppressionof endogenous glucose production(EGP), whole body glucose disposalrate (GDR), and glucose infusion rate(GIR).
RESEARCH DESIGN AND METHODS
Study SubjectsThis study was conducted in accordancewith the International Conferenceon Harmonisation Guideline for GoodClinical Practice and the Declaration ofHelsinki (23). All procedures were ap-proved by the Institutional Review Boardat the University of California, San Diego,Human Research Protections Program,and all subjects provided written, in-formed consent.
Healthy male subjects between theages of 23 and 27 years, inclusive,were screened and enrolled in thisrandomized, open-label, four-period,incomplete-block crossover study. Sub-jects were required to be overtly healthy(as determined by medical history andphysical examination), have a BMI of 20.0to 29.9 kg/m2, and have a fasting bloodglucose ,108 mg/dL (6.0 mmol/L).Subjects were excluded if their hemoglo-bin level was ,12.0 g/dL or if they hadused over-the-counter or prescriptionmedication within 7 and 14 days, re-spectively, prior to dosing.
Study ProtocolHealthy subjects who met the study en-rollment criteria were admitted to theclinical research unit in the afternoon/evening prior to dosing. Subjects fastedovernight for ;8 h and then received a
continuous infusion of D-[3-3H] glucosefor ;4 h to label the glucose pool priorto determination of the rate of EGP.Plasma glucose specific activity wasmeasured at 230, 220, and 210 minand immediately prior to BIL or insulinglargine dosing. Measurement of serumglucose, serum immunoreactive insulin,and C-peptide was also obtained duringthe basal period. Following basal mea-surements, the continuous infusion ofD-[3-3H] glucose was continued for theduration of the glucose clamp study.Subjects received an intravenous infu-sion of BIL or insulin glargine given in aprimed continuous fashion, as describedin Table 1. Euglycemia was maintainedat 90 mg/dL (5.0 mmol/L) using a simul-taneous variable intravenous infusion of20% dextrose containing D-[3-3H] glu-cose, as described previously (24). Bloodsamples were collected at selected timepoints to measure the plasma glucose,plasma glucose specific activity, andC-peptide levels. Blood samples werecollected for the determination of drugconcentrations at 20, 40, and 60min and2, 3, 4, 6, and 8 h postdose (BIL and in-sulin glargine) and also at 9 and 10 hpostdose (BIL only). There was a mini-mum of 6 days of washout betweendoses. Safety assessments includedmonitoring of adverse events (AEs),physical examinations, clinical labora-tory evaluations, vital signs, and electro-cardiogram parameters.
Study TreatmentsSubjects were randomized to either co-hort A or B and received intravenousBIL in the first three dosing periods andintravenous insulin glargine in the fourthperiod (Table 1). Based on BIL pharmaco-kinetics after intravenous administration(19), infusion rates were selected to at-tain steady-state BIL concentrations of2,000, 4,000, 6,000, 8,000, and 10,000
Table 1—Treatment sequences
Sequence/cohort Period 1 BIL Period 2 BIL Period 3 BILPeriod 4 insulin
glargine
Cohort A (n = 4)Priming dosea 660 mU 1,320 mU 2,000 mU 90 mU/m2
Constant infusionb 5.1 mU/min 10.2 mU/min 15.3 mU/min 30 mU/m2/min
Cohort B (n = 4)Priming dosea 2,000 mU 4,000 mU 8,000 mU 60 mU/m2
Constant infusionb 15.3 mU/min 37.0 mU/min 74.1 mU/min 20 mU/m2/min
aThe priming dose was given over ;10 min. bThe constant infusion for both BIL and insulinglargine was given over ;8 h.
2610 Hepatic Action of Basal Insulin Peglispro Diabetes Care Volume 37, September 2014
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022

pmol/L. Insulin glargine infusion rateswere selected based on a previous pub-lication (24), the dose of 20 mU/m2/minglargine was selected to approximate theED50 to achieve half-maximal suppressionof EGP, and the dose of 30 mU/m2/minglargine was chosen to achieve near-maximal suppression of EGP.
AnalysisSerum concentrations of BIL were ana-lyzed at Charles River Laboratories in Sen-neville, Quebec (Canada) using a validatedELISA specific for BIL with no cross-reactivity with human insulin. The lowerlimit of quantification was 20 pmol/L,and the upper limit of quantificationwas 500 pmol/L. The interassay accuracy(percent relative error) during validationranged from 21.4 to 3.5%. The interas-say precision (percent relative SD) duringvalidation ranged from 5.2 to 8.5%.Glargine concentrations were ana-
lyzed at Covance Laboratories Inc.,Chantilly, VA, using a validated radioim-munoassay. The lower limit of quantifi-cation was 50 pmol/L, and the upperlimit of quantification was 2,000 pmol/L.The radioimmunoassay used to mea-sure insulin glargine was nonspecific,and concentrations represent insulinglargine, its two main metabolites(M1 and M2), and endogenous and ex-ogenous human insulin. The interassayaccuracy (percent relative error) duringvalidation ranged from 0.9 to 15.0%.The interassay precision (percent rela-tive SD) during validation ranged from7.1 to 16%. The insulin glargine con-centrations were corrected for en-dogenous insulin based on C-peptidemeasurements.C-peptide concentrations were ana-
lyzed by Covance Central LaboratoryServices, Indianapolis, IN, using ADVIACentaur C-Peptide assay. The assay is atwo-site sandwich immunoassay usingdirect chemiluminescent technology.The primary pharmacodynamic mea-
surement in this study was the evalua-tion of the glucodynamic response tothe study insulins during the euglycemicclamp, including the assessment of EGPand glucose turnover. Plasma glucosewas analyzed using a YSI 2300 STAT Plusglucose analyzer (YSI Inc., Yellow Springs,OH). Glucose turnover was calculated us-ing modified Steele equations for non–steady-state conditions (24–26), whereRa is EGP and Rd is the GDR. In the basal
state, Ra equals EGP. During the insulininfusion, the rate of EGP is calculated asthe difference between the Ra and theGIR. EGP values less than 0were imputedto 0 to indicate full suppression of EGP,as, conceptually, EGP less than 0 is im-plausible. Averages of preclamp mea-surements were used to establish basalrates. The average BIL concentration,C-peptide–corrected glargine concen-trations, EGP, and GDR were calculatedusing the last 2 h of the clamp whenserum concentrations of study insulins,EGP, and GDR had stabilized.
Safety parameters were listed andsummarized using standard descriptivestatistics.
RESULTS
Subject CharacteristicsA total of eight male subjects completedthe study. Subjects had a mean 6 SDage of 26.1 6 1.5 years, mean BMI of24.4 6 1.8 kg/m2, and mean fastingblood glucose 89.25 6 4.76 mg/dL(5.26 6 0.28 mmol/L) prior to dosing.
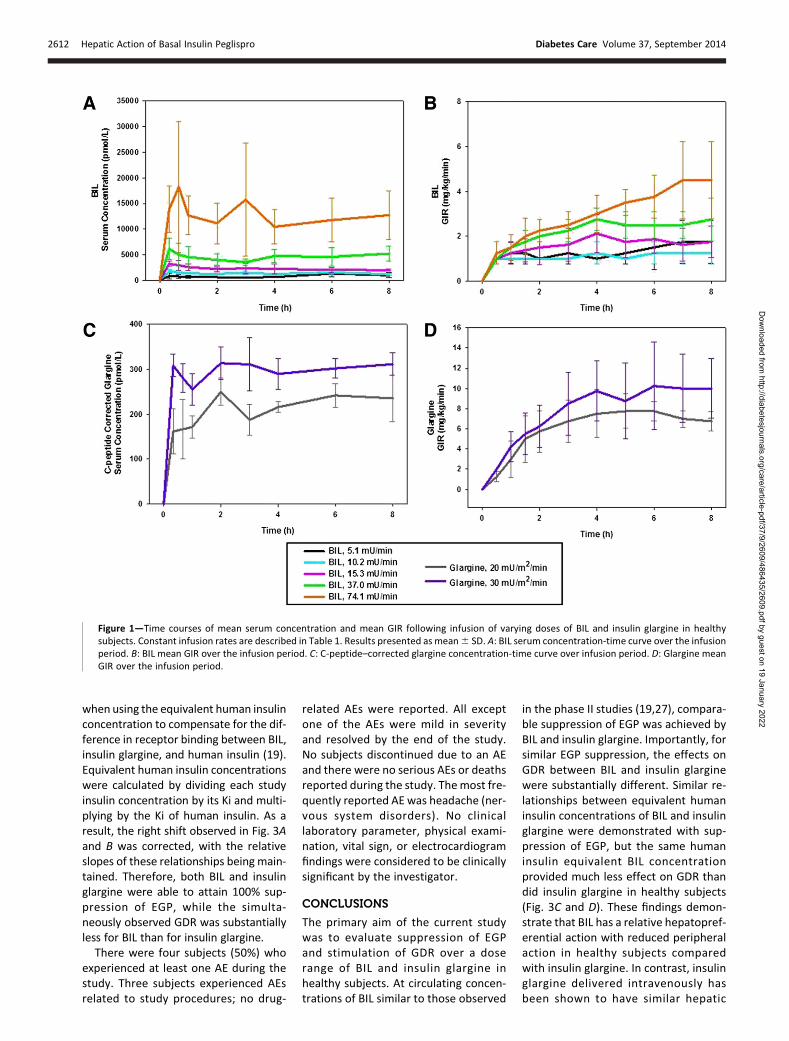
Pharmacokinetic and GlucodynamicResultsFigure 1 presents a panel of time-courseprofiles for the serum concentrations(pmol/L) and GIRs (mg/kg/min) in healthysubjects following the intravenous infu-sion of different doses of BIL or insulinglargine.
As shown in Fig. 1A and C, followingthe 10-min priming infusion, serum con-centrations of BIL and insulin glargineremained stable during the 8-h constantinfusion. Average concentrationstended to increase with increased dosesof BIL and insulin glargine. Average con-centrations ranged between 824 and11,400 pmol/L for BIL (Fig. 1A), and theaverage C-peptide–corrected insulinglargine concentrations were 212 and290 pmol/L, respectively (Fig. 1C).
GIR versus time profiles are shown inFig. 1B and D for BIL and insulin glargine,respectively. At the lowest dose of BIL,GIR rapidly (,1 h) stabilized; intermedi-ate doses required 3 to 4 h for the re-sponse to stabilize; while at the highestBIL dose, there was a tendency for GIRto increase for at least 6 to 7 h. For in-sulin glargine, GIR increased over timeuntil reaching stable values at ;3 h.
Figure 2 shows the time-course profilesfor EGP and GDR and relative responses(percent EGP suppression, fold change
from baseline in GDR stimulation) duringinfusion of BIL or insulin glargine. BILsuppressed EGP in a time- and dose-dependent manner. Except for the lowestdoses of BIL, essentially complete suppres-sion of EGP was reached within 1 to 2 h ofexposure to BIL or insulin glargine. Differ-ences between the effects of BIL and in-sulin glargine were observed with regardto stimulation of GDR. The lower BILdoses had essentially no effect on GDR,while the highest BIL dose showed a grad-ual increase in GDR that continued to riseup to 8 h of exposure. Both dose levels ofinsulin glargine resulted in substantial in-creases in GDR with values up to 15mg/kg/min, considerably higher thanthe largest BIL response (6 mg/kg/min)(Supplementary Fig. 1B).
These differences between BIL andinsulin glargine action are accentuatedby comparing concentration-responsecurves for percent EGP suppression(Fig. 3A) and fold GDR stimulation (Fig.3B). The x-axis of the figures present theconcentrations of BIL or insulin glarginemeasured in the circulation at steadystate for each separate infusion, whilethe y-axis is the activity measured inthe same procedure. With regard toEGP, both BIL and insulin glargine wereable to attain 100% suppression, thoughthe curve for BIL was right shifted by;15-fold compared with insulin glargine.The insulin glargine concentration-response curve for stimulation of GDR(Fig. 3B) was similar to that for suppres-sion of EGP (Fig. 3A), with maximal ef-fects of greater than sixfold increaseabove basal rate. Two differences areapparent for BIL action on GDR whencompared with insulin glargine. The firstis that the maximal effect observed, pre-dominately an approximately twofold in-crease, is much lower than that attainedwith insulin glargine, even at serumconcentrations where suppression ofEGP is similar. The second is that theBIL concentration-response curve forstimulation of GDR is shifted to theright of that for insulin glargine. TheBIL concentration-response relationshipfor GDR was observed to be nonlinearwhen analyzed using a linear regressionmodel (with random effects for subjects)fitted to the log-transformed GDR valuesand log-transformed BIL concentrations(slope of 0.372; P , 0.001).
Figure 3C and D show similar concen-tration-response curves to Fig. 3A and B
care.diabetesjournals.org Henry and Associates 2611
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022
when using the equivalent human insulinconcentration to compensate for the dif-ference in receptor binding between BIL,insulin glargine, and human insulin (19).Equivalent human insulin concentrationswere calculated by dividing each studyinsulin concentration by its Ki and multi-plying by the Ki of human insulin. As aresult, the right shift observed in Fig. 3Aand B was corrected, with the relativeslopes of these relationships being main-tained. Therefore, both BIL and insulinglargine were able to attain 100% sup-pression of EGP, while the simulta-neously observed GDR was substantiallyless for BIL than for insulin glargine.There were four subjects (50%) who
experienced at least one AE during thestudy. Three subjects experienced AEsrelated to study procedures; no drug-
related AEs were reported. All exceptone of the AEs were mild in severityand resolved by the end of the study.No subjects discontinued due to an AEand there were no serious AEs or deathsreported during the study. Themost fre-quently reported AE was headache (ner-vous system disorders). No clinicallaboratory parameter, physical exami-nation, vital sign, or electrocardiogramfindings were considered to be clinicallysignificant by the investigator.
CONCLUSIONS
The primary aim of the current studywas to evaluate suppression of EGPand stimulation of GDR over a doserange of BIL and insulin glargine inhealthy subjects. At circulating concen-trations of BIL similar to those observed
in the phase II studies (19,27), compara-ble suppression of EGP was achieved byBIL and insulin glargine. Importantly, forsimilar EGP suppression, the effects onGDR between BIL and insulin glarginewere substantially different. Similar re-lationships between equivalent humaninsulin concentrations of BIL and insulinglargine were demonstrated with sup-pression of EGP, but the same humaninsulin equivalent BIL concentrationprovided much less effect on GDR thandid insulin glargine in healthy subjects(Fig. 3C and D). These findings demon-strate that BIL has a relative hepatopref-erential action with reduced peripheralaction in healthy subjects comparedwith insulin glargine. In contrast, insulinglargine delivered intravenously hasbeen shown to have similar hepatic
Figure 1—Time courses of mean serum concentration and mean GIR following infusion of varying doses of BIL and insulin glargine in healthysubjects. Constant infusion rates are described in Table 1. Results presented as mean6 SD. A: BIL serum concentration-time curve over the infusionperiod. B: BIL mean GIR over the infusion period. C: C-peptide–corrected glargine concentration-time curve over infusion period. D: Glargine meanGIR over the infusion period.
2612 Hepatic Action of Basal Insulin Peglispro Diabetes Care Volume 37, September 2014
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022

and peripheral effects to intravenoushuman insulin (24).These observations in healthy human
subjects support those noted in an acutedog model of insulinopenic diabetes,where GIRs were matched between pe-ripheral intravenous infusions of BIL andhuman insulin (16). Under these condi-tions, BIL was found to produce a morerapid suppressive effect on hepatic glu-cose production accompaniedby a lesser,more delayed effect on peripheral action.These findings in the dog were corrobo-rated by two methodologies: the sameradioisotopic method used in this pres-ent study and direct organ balance (liverand hindlimb) obtained through invasivecatheterization. The results obtained inthis dog experiment suggested that BIL
may restore the physiologic ratio of he-patic to peripheral insulin action.
Some insulin analogs have been dem-onstrated to have a hepatopreferentialeffect based on the hypothesis thatmolecular size or binding to other pro-teins may inhibit permeability into theperiphery. For example, dimerizationof the insulin molecule and a thyroxyl-insulin analog, which binds to thyroidhormone–binding proteins, has shownrelative hepatopreferential activity,but these insulins apparently have notbeen further developed for use in hu-mans (28–30). The binding to albuminby insulin detemir has also been used toexplain a mild hepatopreferential actionof that insulin analog under hypoglycemicconditions (31). Additionally, the insulin
precursor,proinsulin, hasdemonstratedagreater effect on EGP than GDR (32,33).
Limitations of the current study in-clude the fact that equal molar dosesof insulin glargine and BIL could notbe administered because of differingreceptor-binding affinities, distributionvolumes, and pharmacokinetics. As aresult, estimation of the physiologiceffect on EGP was used to choosepredetermined doses of BIL to comparewith known EGP effects of insulin glarginedoses, and therefore a wider spectrumof BIL dosing was used. Because of therigors of the euglycemic clamp tech-nique in combination with radioisotopictracer infusions, subjects could not re-ceive all doses, and an incomplete-blockdesign was used in this study. Only male
Figure 2—Time courses of suppression of EGP and stimulation of GDR by varying infusions of BIL and insulin glargine. Results are presented asabsolute values (EGP and GDR), percent reduction in EGP from the baseline (percent EGP suppression), or increase over basal GDR (fold change inGDR), mean6 SD. A: EGP absolute values over the infusion period. B: GDR absolute values over the infusion period. C: Percent EGP suppression overthe infusion period. D: Fold increase in GDR over the infusion period.
care.diabetesjournals.org Henry and Associates 2613
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022

subjects were allowed to participate tolimit the impact of variations of insulinsensitivity over the menstrual cycle onthe compressed time course of thestudy. The radioisotopic techniquesalong with the Steele calculations usedin this study lack the precision of theorgan balance techniques used in thedog study (16), which are extremely in-vasive procedures and inappropriate forhuman studies. Lastly, these studieswere conducted in healthy subjects,thus these findings require confirma-tion in patients with both type 1 andtype 2 diabetes. At the highest dosesof BIL, stable values of GIR may not
have been achieved during the 8-hclamp.
In conclusion, this study in healthysubjects supports the findings of studiesperformed in an acute, insulinopenicdog model, which demonstrated thehepatopreferential action of BIL. Impor-tantly, the hepatopreferential action ofBIL results from a lesser peripheral ac-tion compared with human insulin andinsulin glargine and not an accentuatedor enhanced effect on the liver itself. Ahepatopreferential insulin analog couldoffer several advantages over other in-sulins (15), such as the weight benefit,lower rate of nocturnal hypoglycemia,
and decreased prandial insulin require-ments that were observed in the BILphase II trials (21,22).
Acknowledgments. The authors thank DebraHidayetoglu of Covance Inc. for help in thepreparation of the manuscript.Duality of Interest. This study was funded byEli Lilly and Company, Indianapolis, IN, whichalso supplied the investigational product BIL(LY2605541). R.R.H. serves on advisory panelsand as an author for Amgen Inc., AstraZenecaPharmaceuticals LP, Boehringer Ingelheim Phar-maceuticals Inc., Bristol-Myers Squibb Company,Daiichi Sankyo, Elcelyx Therapeutics Inc., GileadSciences Inc., Intarcia Therapeutics Inc., Johnson& Johnson, Janssen Pharmaceuticals, Eli Lilly and
Figure 3—Relationship between percent EGP suppression and fold GDR stimulation with drug concentration (pmol/L) and equivalent human insulinconcentration (pmol/L) for individual subjects. Each data point represents individual subject results for each infusion rate. The means of insulinconcentrations, percent EGP suppression, and fold GDR increase for each dose are connected by lines for each study insulin. Equivalent humaninsulin concentrations were calculated by dividing each study insulin concentration by its Ki and multiplying by the Ki of human insulin. A: PercentEGP suppression versus serum concentration. B: Fold increase in GDR versus serum concentration. C: Percent EGP suppression versus equivalenthuman insulin concentration. D: Fold increase in GDR versus equivalent human insulin concentration.
2614 Hepatic Action of Basal Insulin Peglispro Diabetes Care Volume 37, September 2014
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022

Company, Merck, Novo Nordisk Inc., Roche Phar-maceuticals, Genentech, and Vivus Inc.; servesas a consultant and an author for Alere, Boeh-ringer Ingelheim Pharmaceuticals Inc., Eisai Inc.,Gilead Sciences Inc., Intarcia Therapeutics Inc., IsisPharmaceuticals, Johnson & Johnson, JanssenPharmaceuticals, Eli Lilly and Company, NovoNordisk Inc., and Roche Pharmaceuticals; andprovides research support and serves as an au-thor for AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb Company, Hitachi ChemicalResearch Center Inc., Eli Lilly and Company,and Sanofi. S.M. serves on advisory panels forAstraZeneca Pharmaceuticals and Bristol-MyersSquibb Company and provides research supportfor Intarcia Therapeutics Inc. and Elcelyx Thera-peutics Inc. P.G. is an employee of, stock/share-holder of, and author for Eli Lilly and Company.S.L.C. is an employee of and author for Eli Lillyand Company. S.J.J. is an employee of and authorfor Eli Lilly and Company. M.P.K. is an employeeof, stock/shareholder of, and author for Eli Lillyand Company. E.C.Q.L. is an employee of andauthor for Eli Lilly and Company. M.J.P. is anemployee of, stock/shareholder of, and authorfor Eli Lilly and Company. N.P. is an employee of,stock/shareholder of, and author for Eli Lilly andCompany. H.L. is an employee of, stock/share-holder of, and author for Eli Lilly and Company.No other potential conflicts of interest relevantto this article were reported.Author Contributions. R.R.H., S.M., T.P.C.,D.A.A., P.B., J.P., and N.B. contributed to theresearch and reviewed and edited the manu-script. P.G. contributed to the research, dataanalysis and interpretation, discussion, and writ-ing of the manuscript. S.L.C. contributed re-search, data analysis and interpretation,discussion, and writing of the manuscript. S.J.J.contributed to the research; data analysis andinterpretation; and discussion, writing, and edit-ing of the manuscript. M.P.K. contributed to theprotocol, data generation, discussion, andwritingof the manuscript. E.C.Q.L. contributed to dataanalysis and interpretation and reviewed andedited the manuscript. M.J.P. contributed to theprotocol development and data analysis andinterpretation and reviewed and edited themanuscript. N.P. contributed to data analysis,data interpretation, discussion, andwriting of themanuscript. V.P.S. contributed to the research;data analysis and interpretation; and discussion,writing, and editing of the manuscript. H.L.contributed to the research, data analysis andinterpretation, discussion, and editing of themanuscript. All authors approved the version tobe published. M.J.P. is the guarantor of this workand, as such, had full access to all the data in thestudy and takes responsibility for the integrity ofthe data and the accuracy of the data analysis.
References1. Henriksen JH, Tronier B, Bulow JB. Kinetics ofcirculating endogenous insulin, C-peptide, andproinsulin in fasting nondiabetic man. Metabo-lism 1987;36:463–4682. Samols E, Ryder JA. Studies on tissue uptakeof insulin in man using a differential immunoas-say for endogenous and exogenous insulin.J Clin Invest 1961;40:2092–21023. Campioni M, Toffolo G, Basu R, Rizza RA,Cobelli C. Minimal model assessment of hepatic
insulin extraction during an oral test from stan-dard insulin kinetic parameters. Am J PhysiolEndocrinol Metab 2009;297:E941–E9484. Meier JJ, Veldhuis JD, Butler PC. Pulsatile in-sulin secretion dictates systemic insulin deliveryby regulating hepatic insulin extraction in hu-mans. Diabetes 2005;54:1649–16565. Dimitriadis G, Mitrou P, Lambadiari V,Maratou E, Raptis SA. Insulin effects in muscleand adipose tissue. Diabetes Res Clin Pract2011;93(Suppl. 1):S52–S596. Ferrannini E, Wahren J, Faber OK, Felig P,Binder C, DeFronzo RA. Splanchnic and renalmetabolism of insulin in human subjects:a dose-response study. Am J Physiol 1983;244:E517–E5277. Rabkin R, Simon NM, Steiner S, Colwell JA. Ef-fect of renal disease on renal uptake and excretionof insulin in man. N Engl J Med 1970;282:182–1878. Cherrington AD, Neal DW, Edgerton DS, et al.Inhalation of insulin in dogs: assessment of in-sulin levels and comparison to subcutaneous in-jection. Diabetes 2004;53:877–8819. Eaton RP, Allen RC, Schade DS. Hepatic re-moval of insulin in normal man: dose responseto endogenous insulin secretion. J Clin Endocri-nol Metab 1983;56:1294–130010. Eaton RP, Allen RC, Schade DS, Standefer JC.“Normal” insulin secretion: the goal of artificialinsulin delivery systems? Diabetes Care 1980;3:270–27311. Iglesias P, Dıez JJ. Insulin therapy in renaldisease. Diabetes Obes Metab 2008;10:811–82312. Owens DR. Insulin preparations with pro-longed effect. Diabetes Technol Ther 2011;13(Suppl. 1):S5–S1413. Selam JL, Raccah D, Jean-Didier N, LozanoJL, Waxman K, Charles MA. Randomized com-parison of metabolic control achieved by intra-peritoneal insulin infusion with implantablepumps versus intensive subcutaneous insulintherapy in type I diabetic patients. DiabetesCare 1992;15:53–5814. Saudek CD, DuckworthWC, Giobbie-HurderA, et al.; Department of Veterans Affairs Im-plantable Insulin Pump StudyGroup. Implantableinsulin pump vs multiple-dose insulin for non-insulin-dependent diabetes mellitus: a random-ized clinical trial. JAMA 1996;276:1322–132715. Herring R, Jones RH, Russell-Jones DL. He-patoselectivity and the evolution of insulin.Diabetes Obes Metab 2014;16:1–816. Moore MC, SmithMS, Sinha VP, et al. NovelPEGylated basal insulin LY2605541 has a prefer-ential hepatic effect on glucose metabolism.Diabetes 2014;63:494–50417. Sinha VP, Howey DC, Choi SL, Mace KF,Heise T. Steady-state pharmacokinetics and glu-codynamics of the novel, long-acting basal in-sulin LY2605541 dosed once-daily in patientswith type 2 diabetes mellitus. Diabetes ObesMetab 2014;16:344–35018. Owens RA, Lockwood JF, Dunbar JD, et al. Invitro characterization of novel basal insulinLY2605541: reduced mitogenicity and IGF-IRbinding. Abstract presented at the 72ndScientific Sessions of the American DiabetesAssociation, 8–12 June 2012, Philadelphia,Pennsylvania19. Sinha VP, Howey DC, Kwang Wei Soon D,et al. Single-dose pharmacokinetics (PK) andglucodynamics (GD) of the novel, long-acting
basal insulin LY2605541 in healthy subjects. Ab-stract presented at the 72nd Scientific Sessionsof the American Diabetes Association, 8–12June 2012, Philadelphia, Pennsylvania20. Humalog [package insert]. Indianapolis, IN,Eli Lilly & Co, 201321. Rosenstock J, Bergenstal RM, Blevins TC,et al. Better glycemic control and weight losswith the novel long-acting basal insulinLY2605541 compared with insulin glargine intype 1 diabetes: a randomized, crossover study.Diabetes Care 2013;36:522–52822. Bergenstal RM, Rosenstock J, Arakaki RF,et al. A randomized, controlled study of once-daily LY2605541, a novel long-acting basal insu-lin, versus insulin glargine in basal insulin-treatedpatients with type 2 diabetes. Diabetes Care2012;35:2140–214723. World Medical Association Declaration ofHelsinki. WorldMedical Association Declarationof Helsinki: ethical principles for medical re-search involving human subjects. JAMA 2000;284:3043–304524. Mudaliar S, Mohideen P, Deutsch R, et al.Intravenous glargine and regular insulin havesimilar effects on endogenous glucose outputand peripheral activation/deactivation kineticprofiles. Diabetes Care 2002;25:1597–160225. Steele R. Influences of glucose loading andof injected insulin on hepatic glucose output.Ann N Y Acad Sci 1959;82:420–43026. Finegood DT, Bergman RN, Vranic M. Esti-mation of endogenous glucose production dur-ing hyperinsulinemic-euglycemic glucoseclamps. Comparison of unlabeled and labeledexogenous glucose infusates. Diabetes 1987;36:914–92427. Morrow LA, Hompesch M, Jacober SJ, ChoiSL, Qu Y, Sinha VP. LY2605541 (LY) exhibits aflatter glucodynamic profile than insulin glargine(GL) at steady state in subjects with type 1 di-abetes (T1D). Abstract presented at the 73rdScientific Sessions of the American Diabetes As-sociation, 21–25 June 2013, Chicago, Illinois28. Shojaee-Moradie F, Jackson NC, BoroujerdiM, Brandenburg D, Sonksen PH, Jones RH. Dem-onstration of a relatively hepatoselective effectof covalent insulin dimers on glucose metabo-lism in dogs. Diabetologia 1995;38:1007–101329. Shojaee-Moradie F, Eckey H, Jackson NC,et al. Novel hepatoselective insulin analogues:studies with covalently linked thyroxyl-insulincomplexes. Diabet Med 1998;15:928–93630. Shojaee-Moradie F, Powrie JK, SundermannE,et al. Novel hepatoselective insulin analog: studieswith a covalently linked thyroxyl-insulin complexin humans. Diabetes Care 2000;23:1124–112931. Smeeton F, Shojaee Moradie F, Jones RH,et al. Differential effects of insulin detemir andneutral protamine Hagedorn (NPH) insulin onhepatic glucose production and peripheral glu-cose uptake during hypoglycaemia in type 1 di-abetes. Diabetologia 2009;52:2317–232332. Sonksen PH, Tompkins CV, Srivastava MC,Nabarro JDW. A comparative study on the me-tabolism of human insulin and porcine proinsulinin man. Clin Sci Mol Med 1973;45:633–65433. Glauber HS, Henry RR, Wallace P, et al. Theeffects of biosynthetic human proinsulin on car-bohydrate metabolism in non-insulin-dependentdiabetes mellitus. N Engl J Med 1987;316:443–449
care.diabetesjournals.org Henry and Associates 2615
Dow
nloaded from http://diabetesjournals.org/care/article-pdf/37/9/2609/486435/2609.pdf by guest on 19 January 2022