belgamwar 2011 aripiprazole vs placebo schizophrenia
TRANSCRIPT

Aripiprazole versus placebo for schizophrenia (Review)
Belgamwar RB, El-Sayeh HGG
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2011, Issue 8
http://www.thecochranelibrary.com
Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .
5BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
16DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
29CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
46DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 1 Global state: 1. Relapse. . . . . . 48
Analysis 1.2. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 2 Global state: 2. Poor compliance with study
protocol due to lack of efficacy, deterioration or psychosis. . . . . . . . . . . . . . . . . . . 49
Analysis 1.3. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 3 Global state: 3. Needing additional
antipsychotic medication. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Analysis 1.4. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 4 Global state: 4. Needing additional
benzodiazepines. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Analysis 1.5. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 5 Adverse effects: 1. Clinically important
specific adverse effects. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Analysis 1.6. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 6 Adverse effects: 2. Average change in QTc
interval (ms) from baseline. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Analysis 1.7. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 7 Adverse effects: 3. Physiological (serum)
measures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Analysis 1.8. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 8 Leaving the study early. . . . . . 60
Analysis 1.9. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 9 concomitant medication - anxiolytics. 61
61HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
63INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iAripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Aripiprazole versus placebo for schizophrenia
Ravindra B Belgamwar1, Hany George G El-Sayeh2
1Lymebrook Mental Health Centre, Newcastle Under Lyme, UK. 2Briary Wing, Harrogate District Hospital, Harrogate, UK
Contact address: Ravindra B Belgamwar, Lymebrook Mental Health Centre, Bradwell Hospital Site, Newcastle Under Lyme, Stafford-
shire, ST5 4LD, UK. [email protected]. [email protected].
Editorial group: Cochrane Schizophrenia Group.
Publication status and date: New, published in Issue 8, 2011.
Review content assessed as up-to-date: 19 September 2010.
Citation: Belgamwar RB, El-Sayeh HGG. Aripiprazole versus placebo for schizophrenia. Cochrane Database of Systematic Reviews
2011, Issue 8. Art. No.: CD006622. DOI: 10.1002/14651858.CD006622.pub2.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
First generation ’typical’ antipsychotics such as chlorpromazine and haloperidol have been the mainstay of treatment up until the
introduction of the second generation ’atypical’ antipsychotics such as risperidone and olanzapine. Typical and atypical antipsychotics
do provide a treatment response for most people with schizophrenia, whether a reduction in psychotic episodes or a lessening in the
severity of their illness. However, a proportion of people still do not respond adequately to antipsychotic medication. Additionally,
atypical and especially typical antipsychotics are associated with serious adverse effects, which can often compromise compliance with
medication and therefore increase the incidences of relapse. In this review we examine the effects of aripiprazole compared with placebo.
Objectives
To evaluate the effects of aripiprazole compared with placebo for people with schizophrenia and schizophrenia-like psychoses.
Search strategy
We searched the Cochrane Schizophrenia Group Trials Register (January 2008) which is based on regular searches of BIOSIS, CEN-
TRAL, CINAHL, EMBASE, MEDLINE and PsycINFO. For this update, we carried out an initial search in May 2007 and a second
search in August 2008.
Selection criteria
We included all randomised trials comparing aripiprazole with placebo in people with schizophrenia or schizophrenia-like psychosis.
Data collection and analysis
We extracted data independently. For dichotomous data we calculated risk ratios (RR) and their 95% confidence intervals (CI) on an
intention-to-treat basis based on a fixed-effect model. We calculated numbers needed to treat/harm (NNT/NNH) where appropriate.
For continuous data, we calculated mean differences (MD) again based on a fixed-effect model.
Main results
Despite the fact that 2585 people participated in nine randomised aripiprazole studies, we were unable to extract any usable data on
death, service outcomes, general functioning, behaviour, engagement with services, satisfaction with treatment; economic outcomes or
cognitive functioning. In general, study attrition was very large for all studies over four weeks’ duration. There was high attrition in
most of the included studies. Fewer people left the aripiprazole group compared with those in the placebo group (n = 2585, 9 RCTs,
RR 0.73 CI 0.60 to 0.87). Compared with placebo, aripiprazole significantly decreased relapse in both the short (n = 310, 1 RCT, RR
1Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

0.59 CI 0.45 to 0.77) and medium term (n = 310, 1 RCT, RR 0.66 CI 0.53 to 0.81). It also produced better compliance with study
protocol (n = 2275, 8 RCTs, RR 0.74 CI 0.59 to 0.93). Aripiprazole may decrease prolactin levels below those expected from placebo
(n = 305, 2 RCT, RR 0.21 CI 0.11 to 0.37). Insomnia (~23%) and headaches (~15%) were commonly reported in both groups, with
no significant difference.
Authors’ conclusions
Aripiprazole may be effective for the treatment of schizophrenia. Aripiprazole has a lower risk of raised prolactin and prolongation of
the QTc interval. Clearly reported pragmatic short-, medium- and long-term randomised controlled trials should be undertaken to
determine its position in everyday clinical practice.
P L A I N L A N G U A G E S U M M A R Y
Aripiprazole versus placebo for schizophrenia
Schizophrenia is one of the major psychiatric disorders; it affects individuals’ thinking, perception, affect and behaviour. It can occur in
around 1% of the population. Aripiprazole is one of the newer antipsychotic medications introduced for the treatment of schizophrenia.
When compared with placebo, people taking aripiprazole had fewer relapses, smaller numbers of participants left study early, and needed
less additional antipsychotic medications. Insomnia and headache were the most commonly reported side effects, but were not much
difference to placebo. Side effects such as akathisia, nausea and weight gain occurred more in the aripripazole group as compared to
placebo. There has been a worry with newer antipsychotic medications and their effect on conductance problems in the heart, impaired
glucose levels and excessive production of prolactin (which can cause unpleasant breast pain and secretion). On the limited evidence
available (due to participants leaving early and fewer studies) aripiprazole appears to have a similar effect to that of placebo. The overall
finding on its efficacy in treating schizophrenia is unchanged from those found in the original review.
2Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
Aripiprazole compared with placebo for schizophrenia
Patient or population: people with schizophrenia or like psychosis
Settings: outpatient, inpatient
Intervention: aripiprazole oral or IM
Comparison: placebo oral or IM
Outcomes Illustrative comparative risks* (95% CI) Relative effect
(95% CI)
No of Participants
(studies)
Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Placebo Aripiprazole
Poor compliance with
study protocol
16 per 100 11 per 100 RR 0.72 (0.53 to 0.97) 2275
(8 studies)
++OO
low
Relapse 61 per 100 40 per 100 RR 0.66 (0.57 to 0.75) 573 (2 studies) ++OO
low
Weight gain (equal or
greater then 7% of base-
line)
5.2 per 100 8.5 per 100 RR 2.33 (1.17 to 4.66) 615
(3 studies)
++OO
low
Concomitant medication
(Anxiolytic - Lorazepam)
84 per 100 85 per 100 OR 0.96 (0.61 TO 1.52) 787
(2 studies)
++OO
low
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: confidence interval; RR: risk ratio; OR: odds ratio; GRADE: GRADE Working Group grades of evidence (see explanations)
GRADE Working Group grades of evidence.
High quality (++++): further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality (+++O): further research is likely to have an important impact on our confidence in the estimate of effect and may
change the estimate.
3A
ripip
razo
leversu
sp
laceb
ofo
rsc
hiz
op
hre
nia
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Low quality (++OO): further research is very likely to have an important impact on our confidence in the estimate of effect and is likely
to change the estimate.
Very low quality (+OOO): we are very uncertain about the estimate.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
4A
ripip
razo
leversu
sp
laceb
ofo
rsc
hiz
op
hre
nia
(Revie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

B A C K G R O U N D
Description of the condition
Schizophrenia is one of the major psychiatric disorders; it affects in-
dividuals’ thinking, perception, affect and behaviour. The lifetime
prevalence of schizophrenia is reported to be between 0.4% and
1.4% across populations (Cannon 1996). Typically, schizophre-
nia is preceded by prodromal symptoms such as deterioration in
functioning, unusual behaviour, disturbed communications etc.;
these changes can be gradual. But a number of individuals may
not have any prodromal symptoms and present with an acute first
episode. The course of schizophrenia can be either continuous,
or episodic, with progressive or stable deficit, or there can be one
or more episodes with complete or incomplete remission (ICD
10). Between 14% and 20% of patients will recover fully; oth-
ers will show improvement, but will have recurrences. The early
stages of schizophrenia are characterised by repeated exaggeration
of symptoms, with a high proportion responding to the initial
treatment of antipsychotic medications. Around 80% will relapse
within five years (NICE 2009). The mortality amongst people
with schizophrenia is approximately 50% above the general pop-
ulation, partly related to high suicide rates, violent deaths and in-
creased risk of physical health problems (NICE 2009).
Description of the intervention
’Atypical’ or ’second generation’ antipsychotics include drugs such
as clozapine, olanzapine, risperidone, quetiapine, amisulpiride and
ziprasidone. Initially, these were said to differ from typical antipsy-
chotics in that they were found not to cause movement disorders
(catalepsy) in rats at clinically effective doses (Arnt 1998). These
atypical drugs, however, are far from ideal, and problematic adverse
effects do occur. With the exception of ziprasidone, most atypicals
are associated with weight gain (Anath 2003). Clozapine, which is
used for people whose illness is ’treatment-resistant’, may induce
life-threatening decreases in white blood cells (agranulocytosis) as
well as heart problems (acute myocarditis, cardiomyopathy) and
diabetes (Rivas-Vasquez 2003). Atypical antipsychotics are costly
but may be better tolerated than older anitpyschotics, with less
frequent extrapyramidal symptoms are reported. Aripiprazole is
reported to cause little or no elevation of prolactin concentration.
Aripiprazole is claimed to be at least as effective for positive symp-
toms of schizophrenia and negative symptoms of schizophrenia.
It has also been suggested that aripiprazole may be associated with
fewer movement disorders (parkinsonism, dystonias, tardive dysk-
inesia), less weight gain and reduced negative effects on the heart
(QTc interval abnormalities) and on glucose metabolism com-
pared with standard antipsychotics (Rivas-Vasquez 2003).
How the intervention might work
Technical background
Aripiprazole is said to be the prototype of a new third generation of
antipsychotics, the so-called dopamine-serotonin system stabilis-
ers (McQuade 2002). It is reported to exert its antipsychotic effects
by acting as a partial agonist at D2 dopamine- and 5-HT1a sero-
tonin receptors, and as an antagonist at 5-HT2 serotonin receptors
(Grunder 2006). It has been postulated that, through the above
receptor site actions, and hence dopamine and serotonin system
stabilisation, a partial D2 agonist would be able to act as an antag-
onist in pathways where an abundance of dopamine was produc-
ing psychosis. However, it would stimulate receptors as an agonist
at sites in which low dopaminergic tone would produce side ef-
fects (e.g. areas mediating motor movement and prolactin release)
(Rivas-Vasquez 2003). Aripiprazole, however, also has an affinity
to other receptors including D3, D4, 5-HT2c, 5-HT7, alpha-1
adrenergic and H1 histamine receptors (Burris 2002). When taken
orally, aripiprazole has bioavailability of 87% and peak plasma
concentration occurring at three to five hours; the recommended
target dose for aripiprazole is 10 mg to 15 mg per day (dose range
10 mg to 30 mg) (Abilify 2006). Phase III trials were initially
conducted in Japan in 1995, and the drug was granted approved
status for the treatment of schizophrenia by the Food and Drug
Adminstration (USA) on 15 November 2002 (FDA 2002a). Arip-
iprazole has since been licensed in most countries worldwide, and
is available as tablets, orally disintegrating tablets, oral solution
and intramuscular injection.
Why it is important to do this review
Aripiprazole is one of the newer antipsychotic medications; it is
marketed as having a different mechanism of action and a better
side effect profile compared to others, particularly with regard to
weight gain and prolactin levels. This review looks at, and updates
data from a single comparison of a previous systematic review,
Aripiprazole for schizophrenia (El-Sayeh 2006). A single compar-
ison has been split out of the old review and used to create a
new review, one that assesses aripiprazole’s efficacy and side effects
compared to placebo. This placebo review will then become part
of a family of aripiprazole reviews: Aripiprazole versus typical an-
tipyschotics (Bhattacharjee 2008) and Aripiprazole versus other
atypical antipsychotics (Komossa 2007).
O B J E C T I V E S
To review the effects of aripiprazole compared with placebo for
people with schizophrenia or other psychotic disorders or affective
psychotic disorders.
5Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

M E T H O D S
Criteria for considering studies for this review
Types of studies
We included all relevant randomised controlled trials. Where a trial
was described as ’double-blind’, but it was implied that the study
was randomised, we included the trial in a sensitivity analysis. If
there was no substantive difference within primary outcomes (see
’types of outcome measures’) when these ’implied randomisation’
studies were added, then we included these in the final analysis.
If there was a substantive difference, we only analysed clearly ran-
domised trials and described the results of the sensitivity analysis
in the text. We excluded quasi-randomised studies, such as those
allocating by using alternate days of the week. Randomised cross-
over studies were eligible, but only data up to the point of first
cross-over because of the instability of the problem behaviours and
the likely carryover effects of all treatments.
Types of participants
We included people with schizophrenia and other types of
schizophrenia-like psychosis (e.g. schizophreniform and schizoaf-
fective disorders), irrespective of the diagnostic criteria used. There
is no clear evidence that the schizophrenia-like psychoses are
caused by fundamentally different disease processes or require dif-
ferent treatment approaches (Carpenter 1994).
Types of interventions
1. Aripiprazole: any dose or form of application.
2. Placebo or no treatment.
Types of outcome measures
We grouped outcomes into the acute (up to one week), short term
(up to 12 weeks), medium term (13 to 26 weeks) and long term
(more than 26 weeks).
Primary outcomes
We chose relapse (as defined in the individual studies) as the pri-
mary outcome measure.
Secondary outcomes
1. Death - suicide and natural causes
2. Global state
2.1 Relapse as defined in the individual studies.
2.2 Poor compliance with study protocol due to lack of efficacy,
deterioration or psychosis.
2.3 Needing additional antipsychotic medication.
2.4 Needing additional benzodiazepines.
3. Service outcomes
3.1 Hospitalisation
3.2 Time to hospitalisation
4. Mental state (with particular reference to the positive and neg-
ative symptoms of schizophrenia)
4.1 No clinically important change in general mental state
4.2 Average endpoint general mental state score
4.3 Average change in general mental state scores
4.4 No clinically important change in specific symptoms (positive
symptoms of schizophrenia, negative symptoms of schizophrenia,
depression, mania)
4.5 Average endpoint specific symptom score
4.6 Average change in specific symptom scores
5. General functioning.
5.1 No clinically important change in general functioning
5.2 Average endpoint general functioning score
5.3 Average change in general functioning scores
5.4 No clinically important change in specific aspects of function-
ing, such as social or life skills
5.5 Average endpoint specific aspects of functioning, such as social
or life skills
5.6 Average change in specific aspects of functioning, such as social
or life skills
4. Behaviour
4.1 No clinically important change in general behaviour
4.2 Average endpoint general behaviour score
4.3 Average change in general behaviour scores
4.4 No clinically important change in specific aspects of behaviour
4.5 Average endpoint specific aspects of behaviour
4.6 Average change in specific aspects of behaviour
6. Adverse effects - general and specific (particularly movement
disorders, and those known to occur with newer antipsychotic
medications such as weight gain, glucose imbalance, hypotension,
QTc changes, tachycardia, raised prolactin, blood dyscrasias, sex-
ual side effects, anxiety, somnolence, disturbances of the gastroin-
testinal tract and headache)
6.1 Clinically important general adverse effects
6.2 Average endpoint general adverse effect score
6.3 Average change in general adverse effect scores
6.4 Clinically important specific adverse effects
6.5 Average endpoint specific adverse effects
6.6 Average change in specific adverse effects
7. Engagement with services
8. Satisfaction with treatment
8.1 Leaving the study early
8.2 Recipient of care not satisfied with treatment
8.3 Recipient of care average satisfaction score
8.4 Recipient of care average change in satisfaction scores
8.5 Carer not satisfied with treatment
8.6 Carer average satisfaction score
8.7 Carer average change in satisfaction scores
6Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

9. Quality of life
9.1 No clinically important change in quality of life
9.2 Average endpoint quality of life score
9.3 Average change in quality of life scores
9.4 No clinically important change in specific aspects of quality
of life
9.5 Average endpoint specific aspects of quality of life
9.6 Average change in specific aspects of quality of life
10. Cognitive functioning
10.1 No clinically important change in cognitive functioning
10.2 Average endpoint cognitive functioning score
10.3 Average change in cognitive functioning scores
10.4 No clinically important change in specific aspects of cognitive
functioning
10.5 Average endpoint specific aspects of cognitive functioning
10.6 Average change in specific aspects of cognitive functioning
Search methods for identification of studies
Electronic searches
1. We searched The Cochrane Schizophrenia Groups Trials Reg-
ister (January 2007); An initial search was done in May 2007 and
second search was in August 2008, using the phrase:
[aripiprazole* or abilitat* or abilify* in title or *aripiprazole* or
*abilitat* or *abilify* in abstract, index terms of REFERENCE]
or [aripiprazole* in interventions of STUDY]
This register is compiled by systematic searches of major databases,
hand searches and conference proceedings (see Group Module).
2. The US Food and Drugs Administration (August 2003 and
January 2007). For this update HGE searched the whole site in
August 2008 site using the phrases ’aripiprazole’ and ’abilify’.
Searching other resources
1. Reference searching
We inspected the references of all identified studies for more trials.
2. Personal contact
Where necessary, we contacted authors of trials for missing data,
and additional unpublished studies.
Data collection and analysis
Selection of studies
RBB inspected all reports. HGE then re-inspected these in order
to ensure reliable selection. We resolved any disagreement by dis-
cussion, and where doubt remained, we acquired the full article
for further inspection. Once we obtained the full articles, we (RBB
and HGE) decided whether the studies met the review criteria. If
we could not resolve disagreement by discussion, we sought fur-
ther information and added these trials to the list of those awaiting
assessment.
Data extraction and management
1. Extraction
We electronically extracted initial data from the Aripripazole for
schizophrenia review (El-Sayeh 2006). RBB independently ex-
tracted additional data from selected trials, while HGE separately
re-examined the information. When disputes arose we attempted
to resolve these by discussion. When this was not possible and
further information was necessary to resolve the dilemma, we did
not enter data and added the trial to the list of those awaiting
assessment.
2. Management
2.1 Forms
We extracted data onto standard, simple forms.
2.2 Scale-derived data
We included continuous data from rating scales only if:
a. the psychometric properties of the measuring instrument have
been described in a peer-reviewed journal (Marshall 2000); and
b. the measuring instrument has not been written or modified by
one of the trialists for that particular trial.
Ideally the measuring instrument should either be i. a self-report
or ii. completed by an independent rater or relative (not the thera-
pist). We realise that this is not often reported clearly, in Descrip-
tion of studies noted if this is the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data. Change
data can remove a component of between-person variability from
the analysis. On the other hand calculation of change needs two
assessments (baseline and endpoint) which can be difficult in un-
stable and difficult to measure conditions such as schizophrenia.
We decided to primarily use endpoint data, and only use change
data if the former were not available. We combined endpoint and
change data in the analysis as we used mean differences (MD)
rather than standardised mean differences throughout (Higgins
2011).
7Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.4 Skewed data
Continuous data on clinical and social outcomes are often not
normally distributed. To avoid the pitfall of applying paramet-
ric tests to non-parametric data, we aimed to apply the following
standards to all data before inclusion: a) standard deviations and
means are reported in the paper or obtainable from the authors;
b) when a scale starts from the finite number zero, the standard
deviation, when multiplied by two, is less than the mean (as oth-
erwise the mean is unlikely to be an appropriate measure of the
centre of the distribution, (Altman 1996); c) if a scale started from
a positive value (such as PANSS which can have values from 30
to 210) the calculation described above was modified to take the
scale starting point into account. In these cases skew is present
if 2SD>(S-S min), where S is the mean score and S min is the
minimum score. Endpoint scores on scales often have a finite start
and end point and these rules can be applied. When continuous
data are presented on a scale that includes a possibility of negative
values (such as change data), it is difficult to tell whether data are
skewed or not. We entered skewed data from studies of less than
200 participants in additional tables rather than into an analysis.
Skewed data pose less of a problem when looking at mean if the
sample size is large, we entered such data into syntheses.
2.5 Common measure
To facilitate comparison between trials, we intended to convert
variables that can be reported in different metrics, such as days in
hospital (mean days per year, per week or per month) to a common
metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we made efforts to convert outcome measures
to dichotomous data. This can be done by identifying cut-off
points on rating scales and dividing participants accordingly into
’clinically improved’ or ’not clinically improved’. It is generally
assumed that if there is a 50% reduction in a scale-derived score
such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962)
or the Positive and Negative Syndrome Scale (PANSS, Kay 1986),
this could be considered as a clinically significant response (Leucht
2005; Leucht 2005a). If data based on these thresholds were not
available, we used the primary cut-off presented by the original
authors.
2.7 Direction of graphs
Where possible, we entered data in such a way that the area to
the left of the line of no effect indicated a favourable outcome for
aripiprazole. Where keeping to this made it impossible to avoid
outcome titles with clumsy double-negatives (e.g. ’Not improved’)
we reported data where the left of the line indicates an unfavourable
outcome. This was noted in the relevant graphs.
2.8 Summary of findings table
We used the GRADE approach to interpret findings (Schünemann
2008) and used GRADE profiler (GRADEPRO) to import data
from Review Manager 5 (RevMan) to create ’Summary of findings’
tables. These tables provide outcome-specific information con-
cerning the overall quality of evidence from each included study
in the comparison, the magnitude of effect of the interventions
examined, and the sum of available data on all outcomes we rated
as important to patient-care and decision making. We selected the
following main outcomes for inclusion in the summary of findings
table:
• Poor compliance with study protocol
• Relapse
• Weight gain (equal or greater then 7% of baseline)
• Concomitant medication (Anxiolytic - Lorazepam)
Assessment of risk of bias in included studies
RBB worked independently to assess risk of bias by using criteria
described in the Cochrane Handbook for Systematic Reviews of In-
terventions (Higgins 2011) to assess trial quality. This set of criteria
is based on evidence of associations between overestimate of effect
and high risk of bias of the article such as sequence generation,
allocation concealment, blinding, incomplete outcome data and
selective reporting.
If the raters disagreed, we made the final rating by consensus, with
the involvement of another member of the review group. Where
inadequate details of randomisation and other characteristics of
trials were provided, we contacted authors of the studies in order
to obtain further information. We reported non-concurrence in
quality assessment, but if disputes arose as to which category a
trial was to be allocated, again, we achieved resolution was by
discussion.
The level of risk of bias was noted in both the text of the review
and in the Summary of findings for the main comparison.
Measures of treatment effect
1. Binary data
For binary outcomes we calculated a standard estimation of the
risk ratio (RR) and its 95% confidence interval (CI). It has been
shown that RR is more intuitive (Boissel 1999) than odds ratios
and that odds ratios tend to be interpreted as RR by clinicians
(Deeks 2000). For statistically significant results we had planned
to calculate the number needed to treat to provide benefit /to
induce harm statistic (NNTB/H), and its 95% confidence interval
(CI) using Visual Rx (http://www.nntonline.net/) taking account
of the event rate in the control group. This, however, has been
superseded by Summary of findings for the main comparison and
calculations therein.
8Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2. Continuous data
For continuous outcomes we estimated mean difference (MD) be-
tween groups. We would prefer not to calculate effect size mea-
sures (standardised mean difference SMD). However, if scales of
very considerable similarity were used, we presumed there was a
small difference in measurement, and we would have calculated
effect size and transformed the effect back to the units of one or
more of the specific instruments.
Unit of analysis issues
1. Cluster trials
If cluster studies had been appropriately analysed taking into ac-
count ICCs and relevant data documented in the report, synthe-
sis with other studies would have been possible using the generic
inverse variance technique.
2. Cross-over trials
A major concern of cross-over trials is the carry-over effect. It oc-
curs if an effect (e.g. pharmacological, physiological or psycholog-
ical) of the treatment in the first phase is carried over to the second
phase. As a consequence, on entry to the second phase the par-
ticipants can differ systematically from their initial state despite a
wash-out phase. For the same reason, cross-over trials are not ap-
propriate if the condition of interest is unstable (Elbourne 2002).
As both effects are very likely in schizophrenia, we have only used
data of the first phase of cross-over studies.
3. Studies with multiple treatment groups
Where a study involved more than two treatment arms, if rele-
vant, the additional treatment arms were presented in compar-
isons. Where the additional treatment arms were not relevant,
these data were not reproduced.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss to follow-up data must lose credibility (Xia
2007). We were forced to make a judgment where this was likely
for the trials included in this review. Should more than 40% of
data be unaccounted for by eight weeks, we did not reproduce
these data or use them within analyses.
2. Binary
Where attrition for a binary outcome is between 0% and 40%,
and outcomes of these people are described, we included these data
as reported. Where the outcomes of such people were not clearly
described, we assumed the worst primary outcome, and rates of
adverse effects similar to those who did continue to have their data
recorded.
Assessment of heterogeneity
Clinical heterogeneity
First, we considered all the included studies within any compar-
ison to judge clinical heterogeneity. We then visually inspected
the graphs to investigate the possibility of statistical heterogene-
ity and supplemented this using, primarily, the I2. This provides
an estimate of the percentage of variability due to heterogeneity
rather than chance alone. Where the I2 estimate was greater than
or equal to 70%, we interpreted this as indicating the presence of
high levels of heterogeneity (Higgins 2003). If inconsistency had
been high, data would not have been summated, but we would
have presented them separately and investigated reasons for het-
erogeneity.
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings
is influenced by the nature and direction of results (Egger 1997).
We are aware that funnel plots may be useful in investigating
reporting biases but are of limited power to detect small-study
effects. We did not use funnel plots for outcomes where there were
10 or fewer studies, or where all studies were of similar sizes. In
other cases, where funnel plots were possible, we sought statistical
advice in their interpretation.
Data synthesis
1. Analysis
Where possible we employed a fixed-effect model for analyses. We
understand that there is no closed argument for preference for
use of fixed-effect or random-effects models. The random-effects
method incorporates an assumption that the different studies are
estimating different, yet related, intervention effects. While this
seem accurate to us, the random-effects method does put added
weight onto the smaller of the studies - those trials that are most
vulnerable to bias. For this reason we favour using fixed-effect
models, employing random-effects when we detected heterogene-
ity.
9Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2. General
Where possible, we entered data in such a way that the area to
the left of the line of no effect indicated a favourable outcome for
aripiprazole.
Subgroup analysis and investigation of heterogeneity
We did not carry out any subgroup analysis. We visually inspected
graphs to investigate the possibility of statistical heterogeneity. We
supplemented this by using primarily the I2 statistic. This provides
an estimate of the percentage of variability due to heterogeneity
rather than chance alone. Where the I2 estimate was greater than
or equal to 75%, we interpreted this as indicating the presence of
considerable levels of heterogeneity (Higgins 2003). Where het-
erogeneity was present, we investigated reasons for this. If it sub-
stantially altered the results, we did not summate data, but pre-
sented the data separately and investigated reasons for heterogene-
ity.
Sensitivity analysis
We compared results for high doses (however ’high’ was defined
in the study or, if such a definition was not presented, greater than
15 mg aripiprazole per day) to those for lower doses with regard
to the primary outcome of relapse.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies; Characteristics of studies awaiting classification.
1. Included studies
We identified nine studies that we could include. All were de-
scribed as randomised and as being double blind, although allo-
cation concealment was not adequately described in all studies.
Two main reasons for exclusion were non-randomised studies and
studies with active control without a placebo arm.
For substantive descriptions of the studies please see
Characteristics of included studies and Characteristics of excluded
studies .
2. Studies waiting assessment
Two studies currently await assessment. In both studies, partic-
ipants were adolescents. Nyilas 2007 is a six-week multi-centre
double blind randomised controlled trial; participants were 13 to
17 years old with a DSM-IV diagnosis of schizophrenia (N = 302).
Carson 2008 is a randomised placebo controlled trial on paediatric
participants (aged 10 to 17) with a DSM-IV diagnosis of bipolar
1 disorder (N = 296).
We have already contacted the lead authors for more information
on these trials; at the time of writing this report we have not
received study data.
Results of the search
For this placebo review we conducted an initial electronic search
on 15th May 2007; as there was a delay in writing report we car-
ried out another search on 13th of August 2008. RB inspected 359
electronic and 135 PDF reports from the first search, as well as 239
electronic reports and 237 PDF reports from the second search.
The original aripiprazole review had 15 studies; we included nine
studies from this review, excluding the other six as they were arip-
iprazole versus active control. J Xia inspected reports on the Chi-
nese-language studies.
Included studies
3. Included studies
3.1 Length of trials
Schizophrenia is a lifelong illness that affects young people. Out of
the nine included studies; six reported data on short-term follow-
up of up to six weeks ( Adson 2003; Carson 2000; Csernansky
2003; Daniel 2000; Marcus 2005; Potkin 2003), one on medium-
term follow-up of 26 weeks (Carson 2004) and two studies in-
volved the administration intramuscular preparation reported data
on 24 hours period (Daniel 2004, Oren 2005). There are no stud-
ies reporting on long term follow up i.e. above 26 weeks.
3.2 Participants
Three of the nine included studies involved participants without
clearly operationalised diagnoses (Carson 2002 b; Daniel 2004;
Marcus 2005). All nine trials included people with a diagnosis of
schizophrenia. Four studies included people with schizophrenia
and/or schizoaffective disorder (Carson 2000 a; Daniel 2004; Oren
2005; Potkin 2003). The majority of participants in most studies
were male, and had a mean age in their late thirties to early forties.
In four trials we could not elicit definitive exclusion criteria from
available reports (Carson 2002 b; Daniel 2004; Marcus 2005;
Oren 2005). Adson 2003 and Potkin 2003 required people taking
part in the trial to have had a history of response to other antipsy-
chotics excluding clozapine. Daniel 2000 excluded people with a
history of resistance to anti-psychotic medication. Most people in
these studies were moderately to severely ill and many were acutely
ill.
10Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

3.3 Setting
Eight of the nine studies were described as occurring in hospital
or inpatient settings (Adson 2003; Carson 2000 a; Csernansky
2003; Daniel 2000; Daniel 2004; Marcus 2005; Oren 2005;
Potkin 2003). One trial took place in out-patient or mixed settings
(Carson 2002 b).
3.4 Study size
All the studies included between 200 and 500 participants except
Csernansky 2003, which randomised only 103 participants.
3.5 Interventions
The trialists administered aripiprazole in a wide range of doses
from 1 mg to 30 mg per day, with placebo as a comparator. Most
drugs were given orally, except in two studies in which medication
was given intramuscularly (Daniel 2004; Oren 2005).
3.6 Outcomes
Carson 2002 b compared aripiprazole with placebo and reported
usable data on global state and mean change in CGI. No other
study explicitly reported usable data on this outcome. We have
used ’poor compliance with study protocol due to lack of efficacy,
deterioration or psychosis’ as a global outcome because, surpris-
ingly, there were no more data relevant to global outcomes to be
found in any of the reports.
Studies reported usable data on adverse effects spontaneously re-
ported in more than 5% to 10% of participants. This design pre-
cludes reporting of important less frequent effects. Two studies
reported usable weight gain data; in Carson 2002 b weight gain
of at least 7% was documented as being clinically significant and
Potkin 2003 reported the mean change in body weight.
All but one included study provide usable data on leaving the study
early.
3.6.1 Outcome scales
We have provided details of only the scales that provided usable
data. We have outlined reasons for exclusions of data under ’Out-
comes’ in the Characteristics of included studies
3.6.1.1 Global state - Clinical Global Impression Scale - CGI Scale
(Guy 1976)
This is used to assess both severity of illness and clinical improve-
ment, by comparing the conditions of the person standardised
against other people with the same diagnosis. A seven-point scor-
ing system is usually used, with low scores showing decreased sever-
ity and/or overall improvement. A CGI-I (CGI-Improvement)
score was also validated for used in this review. Carson 2002 b
reported usable data for this outcome.
3.6.1.2 Mental state - Positive and Negative Syndrome Scale -
PANSS (0)
This schizophrenia scale has 30 items, each of which can be de-
fined on a seven-point scoring system varying from 1 - absent to 7
- extreme. This scale can be divided into three sub-scales for mea-
suring the severity of general psychopathology, positive symptoms
(PANSS-P) and negative symptoms (PANSS-N). A low score in-
dicates lesser severity. Kane 2003 reported data from this scale.
3.6.1.3 Quality of life - Quality of Life Scale - QLS, (Carpenter
1994)
This is a semi-structured interview administered and rated by
trained clinicians. It contains 21 items rated on a seven-point scale
based on the interviewer’s judgement of patient functioning. A
total QLS and four sub-scale scores are calculated, with higher
scores indicating less impairment.
3.6.2 Redundant data
Enormous efforts are invested in studies rating and recording data
that are then reported in such a way as to render them useless
for reviews such as this. For example, in Carson 2000 the trial-
ists compare aripiprazole with both haloperidol and placebo. Out-
comes such as death, clearly of interest, were reported in an ob-
scure manner so we could not be sure of either the number of
deaths or the groups in which they took place. We are only sure
that they did take place. At a meeting held with workers from the
Outcomes Research department of Bristol-Myers Squibb Pharma-
ceuticals (UK) on the 27th October 2004 in Leeds, we requested
further clarification on numerous data that appeared on the FDA
web site. In particular, we were concerned by the high death rates
observed in the two studies we identified by FDA study number. It
was jointly agreed that this information (as well as other important
data) would be provided to us when located by company staff. We
did not hear from the company again until we published a short
version of this review at a conference (El-Sayeh 2006). Thereafter,
in May 2006, one author (H E-S) and editor (CEA) met with
representatives of Bristol-Myers Squibb Pharmaceuticals. These
representatives were most helpful in clarifying data on the FDA
web site, specifically on death which, on further evaluation, do
not suggest an increased risk of mortality as indicated in the con-
ference review (El-Sayeh 2006). They also encouraged the review
authors to ask for more data. We have amended this version and
hope to do so again in light of more data provided by industry,
especially on those studies that await assessment.
Carson 2000 a reported continuous measures of global state (CGI)
but no variances are reported. The same applies to their repeated
measures of mental state (BPRS, BPRS-PANNS), general func-
tioning (CGI) and adverse effects (Simpson-Angus scale, Barnes
Akathisia scale, Abnormal Involuntary Movement scale) and other
outcome measures including changes in body weight, serum pro-
lactin, and QTc interval changes. This poor reporting is by no
means unique to Carson 2000 a (see ’Outcomes’, Characteristics
of included studies). Participants in trials may be appalled to know
how much of their data has been rendered useless. It is possible
11Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

that there is a systematic bias in which data, such as the simple
binary outcome of death, are not reported well.
3.6.3 Missing outcomes
We found no usable outcomes for the following categories: death,
service outcomes, general functioning, behaviour, engagement
with services, satisfaction with treatment, economic outcomes or
cognitive functioning.
3.6.4 Primary outcomes
Our primary outcome of relapse was only reported in Carson 2002
b, which compares aripiprazole with placebo. All other outcomes
in this review were of secondary importance to the review authors
but we do recognise that they may be of primary interest to others.
Excluded studies
The original review had 15 included studies and six excluded stud-
ies (aripiprazole versus active control without placebo arm). Dur-
ing our search, we came across several new studies in the pipeline
where aripiprazole is compared to another antipsychotic medica-
tion.
We excluded nine other studies from the review. Three were re-
view articles (Carson 2002 a; Petrie 1997; Kujawa 2003). We
excluded one study because participants were healthy volunteers
(Mallikaarjun 2000). We excluded Auby 2002 because, although
randomised, it evaluated one dose of aripiprazole versus another
and also reported no data that we could include. We will contact
the authors for further information. We excluded Stroup 2003
from the study because participants who received aripiprazole in
this trial were not randomised at that stage. We excluded Marcus
2003 since the study described was a review of other short-term
studies, not an original research article. We excluded Casey 2003
and Saha 2004 from this version of the review, as different admin-
istration regimens of aripiprazole were randomised rather than the
new drug versus others or placebo.
Risk of bias in included studies
We have provided information on summary of risk of bias across
all included studies in Figure 1 and Figure 2
Figure 1. Methodological quality graph: review authors’ judgements about each methodological quality
item presented as percentages across all included studies.
12Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
13Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Allocation
All included studies were said to be randomised. None of the in-
cluded studies, however, explicitly detailed the method of ran-
domisation. No studies stated that those in charge of allocation
were blind to the participant list. This concealment of allocation
has repeatedly been shown to be of key importance in excluding
selection biases (Jüni P 2001). Therefore all trials were category B
(moderate risk of bias - some doubt about the results - see Meth-
ods). This was confirmed by poor ratings on the Jadad Scale (see
Characteristics of included studies) (Jadad 1996).
Blinding
Nine studies were described as being double-blind (Carson 2000
a; Carson 2002 b; Csernansky 2003; Daniel 2000; Daniel 2004;
Marcus 2005; McQuade 2003; Oren 2005; Potkin 2003). Adson
2003 was described as double-blind, but people who showed no
improvement or worsening of their symptoms by the third week
were offered the option of open-label treatment with aripiprazole
during the last three weeks of the study. In none of the studies was
testing of the blinding reported. Since blinding is recognised to be
important for minimising observation bias, it could be expected
that testing of this blinding be considered a priority.
Incomplete outcome data
Loss to follow-up
Several of the included studies reported data in terms of a last
observation carried forwards (LOCF) analysis and an OC analysis
(observed cases, defined as those completing the trial). Although
LOCF analyses are commonly used to account for missing ob-
servations, this technique could introduce bias as considerable as-
sumptions are made about people who did not stay in the study.
We saw no reporting of attempts to validate assumptions by fol-
lowing up people who did leave the study early. In some included
studies, rates of participants leaving early were more than 40%.
Using LOCF, 40% of the data on certain outcomes are assumed
and would lead to bias in the overall results.
The reasons for loss to follow-up are reasonably well reported and
we have documented these in the outcomes.
Selective reporting
Data reporting
Overall much of the data we found could not be used because of
poor reporting. Findings which are presented as graphs, in per-
centiles or just reported as P values are often of little use to a re-
viewer. Many studies failed to provide standard deviations when
reporting mean changes on a particular outcome measure
Other potential sources of bias
Aripiprazole being a relatively newer drug, it is not surprising that
all the trials were run by the drug company. Two studies with IM
preparation had 24-hour follow-up and a low rate of drop-out.
All other included studies have above four weeks follow-up and a
higher drop-out rate. The most common reason for drop-out in
both the arms of treatment was lack of efficacy.
The rates of attrition for individual studies are as follows: Adson
2003 0.66 (i.e. 34% of patients completed study); Carson 2000
a 0.40; Carson 2002 b 0.62; Csernansky 2003 0.48; Daniel 2000
0.40; Daniel 2004 0.05; Marcus 2005 0.47; Oren 2005 0.03; and
Potkin 2003 0.40.
Effects of interventions
See: Summary of findings for the main comparison
From the original review Aripripazole for schizophrenia, we iden-
tified 9 studies where aripripazole was compared with placebo; we
included all 9 studies. We carried out update searches in May 2007
and August 2008 to see if there are any new studies on Aripipra-
zole compared to placebo or any additional data on the existing
included studies. The two update searches did not find further
studies but provided additional study data, particularly on side
effects.
We also identified two new studies (Carson 2008; Nyilas 2007)
focusing on adolescent populations from conference posters. Since
the findings from these studies have been presented as graphs, in
percentiles or just reported as P values, we have not been able to
include them in the analysis at this stage. We contacted authors
for additional information but unable to get the data. This is
particularly unfortunate given that this age group is an important
subset of the general population, and research data and studies are
often lacking.
Comparison 1: ARIPIPRAZOLE versus PLACEBO
1. Global state
1.1 Relapse
14Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Relapse was the primary outcome for this review. Only one
aripiprazole versus placebo comparison contained relevant data.
Carson 2002 b provided usable data for short-term (up to 12
weeks) relapse. There were significantly fewer relapses for people
given aripiprazole compared with those in the placebo group (n =
310, 1 RCT, RR 0.59 CI 0.45 to 0.77, NNT 5 CI 3.2 to 10.7).
The same study provided usable data for medium-term (13 to 26
weeks) relapse. Again the aripiprazole group had significantly less
relapse compared with people given placebo (n = 310, 1 RCT, RR
0.66 CI 0.53 to 0.81, NNT 5 CI 3.0 to 8.5).
1.2 Poor compliance with study protocol due to lack of
efficacy, deterioration or psychosis
Two studies with IM preparation had follow-up at 24 hours and
a low rate of leaving the study early. All other studies (one-week
to 12-week duration) gave several reasons for the poor compli-
ance with study protocol, and several seemed to fall into a natu-
ral grouping reporting a poor global outcome. We have grouped
these throughout the review. Overall people allocated to aripipra-
zole encountered this outcome significantly less than those given
placebo (n = 2275, 8 RCTs, RR 0.74 CI 0.59 to 0.93, NNT 21
CI 12.7 to 60.5).
1.3 Needing additional antipsychotic medication
Four studies reported this outcome, one acute (up to one week)
and other three from short term (one week to 12 week). There was
significantly less need for additional antipsychotic medication in
those randomised to aripiprazole compared to those given placebo
(n = 1062, 4 RCTs, RR 0.73 CI 0.57 to 0.93, NNT 16 CI 8.9 to
73.2).
1.4 Needing additional benzodiazepines
Two studies, one from acute (up to one week) and one from short
term (one week to 12 week) reported this outcome. There was
significantly less need for additional benzodiazepine treatment in
those randomised to aripiprazole compared to those given placebo
(n = 683, 2 RCT, RR 0.53 CI 0.3 to 0.92, NNT 18).
Caution is advised in interpreting these results: in two studies
lorazepam was given as an anxiolytics and was received by 85% of
patients in both arms (section 4).
2. Adverse effects
2.1 Insomnia and headaches
Insomnia (~23%) (n = 1298, 4 RCTs, RR 1.09 CI 0.89 to 1.33,
NNH 46) and headaches (~15%) (n = 1962, 6 RCTs, RR 1.17 CI
0.94 to 1.47, NNH 33) were commonly reported in both groups
with no significant difference.
2.2 Akathisia, nausea, sedation, weight gain
People on aripiprazole were more likely to develop akathisia (n =
1595, 5 RCTs, RR 1.78 CI 1.16 to 2.74, NNH 34); nausea (n =
1962, 6 RCTs, RR 1.55 CI 1.07 to 2.24, NNH 27); sedation (n
= 1347, 4 RCTs, RR 1.82 CI 1.06 to 3.15, NNH 23); and weight
gain of equal to or greater than 7% of baseline weight (n = 615, 3
RCTs, RR 2.55 CI 1.35 to 4.82, NNH 20).
2.3 Constipation, dizziness, tachycardia, diarrhoea
Constipation was experienced by 7.3% of patients (n = 787, 2
RCTs, RR 1.42 CI 0.75 to 2.69, NNH 43); dizziness by 7.4%
of patients (n = 1347, 4 RCTs, RR 1.34 CI 0.83 to 2.14, NNH
33); tachycardia by 4.6% (n = 1084, 3 RCTs, RR 1.94 CI 0.89 to
4.25, NNH 41); and diarrhoea by 4% (n = 887, 2 RCTs, RR 0.79
CI 0.40 to 1.56, NNH 55). There was no significant difference
between the two groups.
2.4 General extrapyramidal symptoms, movement disorders,
vomiting, anxiety, dyspepsia
There appears to be no significant difference between the two
comparator groups in terms of reported general extrapyramidal
symptoms (n = 1298, 4 RCTs, RR 0.83 CI 0.47 to 1.45, NNH
118); needing anti-parkinsonian medication (n = 1043, 4 RCTs,
RR 0.83 CI 0.61 to 1.14, NNH 33); vomiting (n = 1699, 5 RCTs,
RR 1.46 CI 0.96 to 2.33, NNH 46); anxiety (n = 1035, 3 RCTs,
RR 0.83 CI 0.62 to 1.12, NNH 25); and dyspepsia (n = 887, 2
RCTs, RR 0.88 CI 0.50 to 1.40, NNH 36).
2.5 Agitation
Agitation was less in the aripiprazole group (n = 980, 3 RCTs,
RR 0.61 CI 0.40 to 0.92, NNH 22). Aripripazole appeared to
produce significantly less rise in serum prolactin (increase to >/
= 23ng/ml) than placebo (n = 725, 2 RCT, RR 0.21 CI 0.11 to
0.37, NNT 9).
2.6 Additional side effects
One study (Marcus 2005) reported detailed side effects informa-
tion; these included toothache (n = 367, 1 RCTs, RR 1.47 CI
0.43 to 5.00); upper abdominal pain (n = 367, 1 RCTs, RR 4.13
CI 0.24 to 72.63); Infections (n = 367, 1 RCT, RR 0.57 CI 0.20
to1.65); skin rash (n = 367, 1 RCT, RR 3.47 CI 0.45 to 26.5);
cough (n = 367, 1 RCT, RR 1.89 CI 0.43 to 8.29); pharyngola-
ryngeal pain (n = 367, 1 RCT, RR 8.58 CI 0.52 to 142.92); all
were statistically insignificant. One study (Adson 2003) reported
asthenia, with no significant difference amongst the groups (n =
420, 1 RCT, RR 0.94 CI 0.41 to 2.17).
15Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2.7 QTc interval
Two studies reported QTc interval of 450 or more or 10% above
baseline; 3 patients in the aripiprazole group showed these changes
whilst none from the placebo group. The difference was not sig-
nificant (n = 787, 2 RCTs, RR 2.44 CI 0.13 to 46.82, NNH 198).
For average change - QTc interval (ms) from baseline, there ap-
peared to be no significant difference between 20 mg/day aripipra-
zole and placebo on this continuous outcome measure (n = 204,
1 RCT, WMD 3.00 CI -3.19 to 9.19) and for the higher dose of
aripiprazole (30 mg/day) (n = 204, 1 RCT, WMD -1.00 CI -7.18
to 5.18), the standard deviations are very large and data could be
skewed.
2.8 Physiological (serum) measures
Physiological (serum) measures were reported by one study
(Carson 2002 b).
At 26 weeks there was no significant difference between groups on
total fasting cholesterol >/= 200 mg/dl (n = 310, 1 RCT, RR 1.21
CI 0.98 to1.50, NNH 10); total fasting cholesterol level >= 240
mg/dl (n = 310, 1 RCT, RR 1.22 CI 0.77 to 1.93, NNH 26); the
glucose levels of >/= 110mg/dl (n = 310, 1 RCT, RR 0.96 CI 0.7
to 1.33); haemoglobin 1AC (incidence >/= upper limit of normal)
(n = 310, 1 RCT, RR 0.74 CI 0.41 to 1.33); levels of low density
lipoprotein (>/= 130mg/dl) (n = 310, 1 RCT, RR 1.01 CI 0.80
to 1.28) and low density lipoprotein (>/= 160mg/dl) (n = 310, 1
RCT, RR 1.0 CI 0.62 to 1.61).
The same study measured triglycerides >= 200 mg/dl (n = 310,
1 RCT, RR 0.94 CI 0.67 to 1.31) and high density lipoprotein
(n = 310, 1 RCT, RR 0.86 CI 0.66 to 1.12) with no difference
amongst the groups.
3. Leaving the study early
We noted that data were heterogenous on visual inspection of
forest plot and had high I2. Significantly fewer people left (for any
reason) the aripiprazole group compared with those in the placebo
group (n = 2585, 9 RCTs, RR 0.73 CI 0.60 to 0.87, NNT 8,
95% CI 5.6 to 10.3). When the reason for leaving was recorded
as being due to adverse effects, there was no difference between
groups (n = 2585, 9 RCTS, RR 0.75 CI 0.42 to 1.35).
4. Concomitant medication
Two studies (Adson 2003; Marcus 2005) reported concomitant
use of anxiolytics and what appears to be lorazepam. This com-
bination was use in 85% of participants in both the groups (n =
787, OR 0.96 CI 0.61 to 1.52).
D I S C U S S I O N
Summary of main results
When compared with placebo, aripiprazole treated patients had
fewer relapses, fewer people left study early and needed less addi-
tional antipsychotic medications. Where reported, both the group
needed benzodiazepine/antianxiety medication (lorazepam) as an
adjunct treatment in most of the patients.
1. Applicability of findings
All the included studies occurred as multicentre trials in North
American and European settings. Clinicians should take this into
consideration when thinking of using aripiprazole in very different
settings of care.
The majority of trials involved inpatient participants with little in
the way of physical and psychiatric co-morbidity and with well-
defined schizophrenia or schizoaffective disorder. Such people are
a minority in everyday care, where people who are not in hospital
and suffer from less well defined illness, combined with problems
such as depression and substance abuse, are the norm. The reader
is subsequently left with the difficult decision as to whether the
findings of studies with such participants, interventions and out-
comes, gathered in standardised highly developed inpatient set-
tings, can still inform their daily practice.
2. Limited data, confusing data
The collection and quality of the data reported were very variable.
With the exception of one trial, no studies reported outcomes over
12 weeks. Aripiprazole is a relatively new antipsychotic medica-
tion, so it is not surprising that long-term studies are rare at this
point, but it is to be hoped that they are planned. Even if an in-
tervention works in the short term (by 12 weeks) there is no guar-
antee that this means that the compound has long-term benefits.
Data were often not used because of high drop-out rates. The
enormous degree of loss to follow-up is common in similar studies
of other compounds, but rare in everyday practice. This also casts
doubt on the applicability of findings to routine care. The design
of the studies is clearly encouraging loss to follow-up. People leave
for many reasons, often not specified, and their last observation is
carried forward to the end. These data, sometimes with an assump-
tion on over 50% of people are, nevertheless, acceptable to the
regulatory authorities. Until this ends, pharmaceutical companies
will see little reason to change their practices, as compounds such
as aripiprazole or any other new drug will gain licenses for clinical
use even if 40% to 60% of their data is unavailable. Often the tri-
alists do not have an obligation to follow people up for longer than
the period during which they took the medication. One possible
consequence of this might be that an extreme adverse reaction to
discontinuation of an intervention, such as death, would go un-
reported if it occurred a week after the treatment stopped. Data
beyond the discontinuation of the medications used within the
trial are collected but not reported. This data should be reported
16Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

since it is not the individual compounds in a trial which are ran-
domised, but the intention to give those individual compounds.
Some trialists tended to report mean figures without giving stan-
dard deviations. This renders averages meaningless and of no use
to review authors.
We found it disappointing that, despite considerable investment
in clinical trials, no outcome data were available on death, ser-
vice outcomes, general functioning, behaviour, engagement with
services, economic outcomes and cognitive functioning. The pri-
mary outcome of this review was relapse and data were available
on this in the aripiprazole-placebo comparison. Other outcomes
were of secondary importance to the review authors, but we have
reported what we can in order to present the most complete data
set possible for the reader.
Several trials only reported adverse effects which occurred in at
least 5% to 10% of participants, which could exclude potentially
serious less frequent outcomes. Randomised trials are limited in
their ability to highlight important rare outcomes, so further re-
stricting what is reported seems odd. We note that the design of
the trials did not limit reporting of positive outcomes to only those
that occurred at least 5% to 10% of the time.
Some data were obtained from conference proceedings and posters.
This made extraction difficult as results were often summarised.
Several studies were reported multiple times. Without unique
study identifiers, this gives the impressions that there are more
data than actually exist and facilitates erroneous double counting.
3. Comparison 1: aripiprazole versus placebo
3.1 Global state
3.1.1 Relapse
Relapse, the primary outcome for this review, was only reported
by Carson 2002 b and was defined in one of three ways: i. a CGI
rating of minimally worse; ii. a PANSS rating of moderately severe
on hostility or uncooperativeness on two successive days; or iii. >/
= 20% increase in total PANSS score from randomisation. This
implies first, that these measures of severity of illness are indeed
markers of a relapse and second, that the measures agree on the
severity of illness needed to constitute a relapse. We are not sure
that these scores on these measures really would constitute what
clinicians or recipients of care would call relapse. We think that
the ratings listed above would be moderate deterioration rather
than an event that would be universally recognised as relapse. Nev-
ertheless, it is genuinely heartening that aripiprazole helps avoid
these degrees of deterioration and that the number needed to treat
of five is not very large in either the short or medium term.
3.1.2 Poor compliance with study protocol due to lack of
efficacy, deterioration or psychosis
This category constituted patients leaving the study due to poor
efficacy, those with deterioration in their mental state and those
who developed frank psychosis. There was a significant difference
in favour of aripiprazole with regard to this outcome, although the
number needed to treat is high (NNT 21 CI 12 to 60).
3.1.3 Needing additional antipsychotic medication
Few people needed ’rescue’ antipsychotics in the aripiprazole group
as compared to placebo. It has to be seen as encouraging that
aripiprazole does seem to have some antipsychotic activity within
the four studies.
3.1.4 Needing additional benzodiazepines
There appeared to be significantly less need for benzodiazepine
medication in the aripiprazole treated patients (NNT 16). Two
studies used intramuscular medication, however, and the out-
comes were only reported over the short term (up to 24 hours)
(Daniel 2004; Oren 2005).
This needs to be taken in context as in two studies (Adson 2003;
Marcus 2005), the majority (85%) of the patients in both arms
received lorazepam as an anti-anxiety drug. This may suggest that
in the short term, there is a need for an additional benzodiazepine
similar to placebo.
3.2 Adverse effects
3.2.1 Clinically important specific adverse effects
Overall results from the included studies suggest that the akathisia,
nausea and weight gain were more common in those treated with
aripiprazole; there were no significant differences in reported ad-
verse effects in people taking placebo compared to those taking
aripiprazole. No objective rating scales appeared to be used in mea-
suring these symptoms, even though for certain symptoms such as
anxiety and extrapyramidal side effects, these are commonly used
in research. Potkin 2003 did repeatedly find more adverse effects
than Carson 2002 b and, although there is nothing in the methods
of the papers to suggest this, it may be that the former study used
more sensitive measures of adverse effects. Potkin 2003 did seem
to suggest that aripiprazole may be associated with extrapyrami-
dal symptoms, vomiting and weight gain. Although no different
from placebo, about 17% of people given aripiprazole were also
medicated with antiparkinson medication. It was unclear from all
studies, both those in this comparison and those including an ac-
tive control group, how the level of significant weight gain (seven
percent) was decided upon. There was no mention of this figure
in the methodology section of the included study reports and if
17Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

it was decided on after the data were inspected, any results would
be prone to bias.
3.2.2 Average change in QT interval (ms) from baseline (high
= poor)
From these data it does not seem that 20 mg/day or 30 mg/day of
aripiprazole affects the heart in this way.
3.2.3 Physiological (serum) measures
All data, mostly from Carson 2002 b, suggest little effect on mea-
sures of glucose and lipids. Patients with schizophrenia do have
higher risk of cardiovascular and metabolic disorders, and some
newer antipsychotic medications increase this risk. Aripripazole,
however, seems to have a neutral effect.
There did appear to be a significant difference in favour of arip-
iprazole in terms of the numbers of people with a rise in serum
prolactin to at least 23 ng/ml (NNT 9 CI 6.2 to 15.7). This may
have clinical implications in terms of the problems caused by high
prolactin, such as galactorrhoea. Potkin 2003 suggested that nu-
merical decline in the prolactin levels in the aripiprazole group is
consistent with partial agonism at the D2 receptors and mirror
results from their pre-clinical trials. However data were missing for
baseline mean serum prolactin levels in 8/103 people allocated to
placebo and 21/202 people given aripiprazole. We have assumed
that these people did not have raised prolactin, but if they did
and we were incorrect in our assumption, there would be no clear
finding in favour of aripiprazole.
3.3 Leaving the study early
Significantly fewer people left the aripiprazole group compared
with placebo (NNT 8 CI 5.6 to 10.3) for any reason. These data
are heterogeneous and if the two studies with the most extreme
results are removed (Csernansky 2003; Potkin 2003), data become
more homogeneous and much less favourable for aripiprazole. We
do not see obvious reasons for heterogeneity. However, nearly half
of all trial participants chose to leave early. This reflects negatively
on study design and means that much of the remaining data are
uninformative. Adverse effects did not seem to be a reason for
study attrition, although again data were heterogeneous. There is
no evidence from these studies that aripiprazole is a major cause of
unacceptable short-term adverse effects. Results from the (Carson
2002 b) study provided more accurate data, but this did not sig-
nificantly affect the overall results.
Overall completeness and applicability ofevidence
There is a lack of evidence on the efficacy of aripiprazole in
schizophrenia (i.e. showing improvement of the schizophrenia
symptoms rating scales). The studies rely on other factors, such
as compliance and smaller numbers of relapses as a measure of
efficacy.
1. Limited data, confusing data
The collection and quality of the data reported were very variable.
With the exception of one trial, no studies reported outcomes over
12 weeks. Aripiprazole is a relatively new antipsychotic medica-
tion, so it is not surprising that long-term studies are rare at this
point. However, it is to be hoped that they are planned. Even if
an intervention works in the short term (by 12 weeks) there is
no guarantee that this means that the compound has long-term
benefits.
Data were often not usable because of high drop-out rates. The
enormous degree of loss to follow-up is common in similar studies
of other compounds, but rare in everyday practice. This also casts
doubt on the applicability of findings to routine care. The design
of the studies is clearly encouraging loss to follow-up. People leave
for many reasons, often not specified, and their last observation is
carried forward to the end. These data, sometimes with an assump-
tion on over 50% of people are, nevertheless, acceptable to the
regulatory authorities. Until this ends, pharmaceutical companies
will see little reason to change their practices, as compounds such
as aripiprazole or any other new drug will gain licenses for clinical
use even if 40% to 60% of their data are unavailable. Often the tri-
alists do not have an obligation to follow people up for longer than
the period during which they took the medication. One possible
consequence of this might be that an extreme adverse reaction to
discontinuation of an intervention, such as death, would go un-
reported if it occurred a week after the treatment stopped. Data
beyond the discontinuation of the medications used within the
trial are collected but not reported. This data should be reported
since it is not the individual compounds in a trial which are ran-
domised, but the intention to give those individual compounds.
Some trialists tended to report mean figures without giving stan-
dard deviations. This renders averages meaningless and of no use
to review authors.
We found it disappointing that, despite considerable investment
in clinical trials, no outcome data were available on death, ser-
vice outcomes, general functioning, behaviour, engagement with
services, economic outcomes and cognitive functioning. The pri-
mary outcome of this review was relapse and data were available
on this in the aripiprazole-placebo comparison. Other outcomes
were of secondary importance to the review authors, but we have
reported what we can in order to present the most complete data
set possible for the reader.
Several trials only reported adverse effects which occurred in at
least 5% to 10% of participants, which could exclude potentially
serious less frequent outcomes. Randomised trials are limited in
their ability to highlight important rare outcomes, so further re-
stricting what is reported seems odd. We note that the design of
18Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the trials did not limit reporting of positive outcomes to only those
that occurred at least 5% to 10% of the time.
We obtained some of the data from conference proceedings and
posters. This made extraction difficult, as results were often sum-
marised. Several studies were multiply reported. Without unique
study identifiers this gives the impression that there are more data
than actually exist and facilitates erroneous double counting.
2. Applicability of findings
All the included studies occurred as multicentre trials in North
American and European settings. Clinicians should take this into
consideration when thinking of using aripiprazole in very different
settings of care.
The majority of trials involved inpatient participants with little in
the way of physical and psychiatric co-morbidity and with well-
defined schizophrenia or schizoaffective disorder. Such people are
a minority in everyday care, where people who are not in hospital
and suffer from less well-defined illness, combined with problems
such as depression and substance abuse, are the norm. The reader
is subsequently left with the difficult decision as to whether the
findings of studies with such participants, interventions and out-
comes and standardised highly developed inpatient settings can
still inform their daily practice.
Quality of the evidence
1. All of the included studies were published in journals, although
we obtained some data from conference proceedings and hand-
searching.
2. All included studies were sponsored by the pharmaceutical in-
dustry.
3. Schizophrenia is a chronic condition and the long-term effect
of an antipsychotic medication is important. We noted that the
duration of follow-up was relatively short (i.e. less then 12 weeks
except for one study where the follow-up was for 26 weeks). Lack
of long-term studies limited the overall quality of evidence.
4. All studies reported being double blind in their methods sec-
tions, but did not give any further details.
5. High rates of participants leaving the studies early is another
important factor limiting the quality of evidence.
6. We noted variation in the data reporting amongst studies.
Potential biases in the review process
There were no disagreement between authors on the numbers
extracted.
Agreements and disagreements with otherstudies or reviews
1. No additional studies identified for this update of the original
aripiprazole for schizophrenia review.
2. Number needed to treat calculation showed variation to the
original review even with the same data. Following discussion with
the co-author we used the online calculation method for all results
(http://www.graphpad.com/quickcalcs/NNT1.cfm).
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
1. For people with schizophrenia
For this update, we found no new studies comparing aripiprazole
with placebo to add to those included in the original review and
update. However, we noted several new studies comparing arip-
iprazole with active control.
When compared with placebo, aripiprazole treated patients had
fewer relapses and fewer left study early, and needed less addi-
tional antipsychotic medications. Overall it appears that aripipra-
zole has a better side effect profile; those that were significantly
more prevalent than in the placebo group included akathisia, nau-
sea and weight gain.
There have been concerns in the medical community about the
effects of atypical antipsychotics on conductance problems in the
heart (QTc interval), increased prolactin levels (excessive produc-
tion of prolactin, which can cause unpleasant breast pain and se-
cretion) and glucose levels; on the limited evidence available (due
to subjects leaving study early and fewer studies), aripiprazole ap-
pears to have a similar effect to that of placebo. The overall finding
on its efficacy in treating schizophrenia is unchanged from what
we found in the original review.
2. For clinicians
Aripripazole efficacy on global state was superior to placebo in
one study. Aripripazole may offer significant advantages over other
atypicals in terms of outcomes, as it caused hyperprolactinaemia
and raised QTc interval; thus, aripiprazole’s effect appears to be
similar to that of placebo. More studies are needed to replicate
and validate these findings. In two studies, lorazepam was given to
85% of the patients in both arms, suggesting a need for additional
medication. Long-term studies are required to see how long this
is necessary.
19Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

3. For managers/policy makers
Aripiprazole is another new atypical antipsychotic drug and it does
seem to have an effect on some people with serious mental illnesses
such as schizophrenia. It appears to be tolerated well. Despite
the fact that thousands of people have been randomised in trials
of aripiprazole, there are no data on service outcomes and few
medium- or long-term data. In the context of finite resources, the
lack of good quality data leaves managers and policy makers with
difficult decisions to make.
Implications for research
1. General
As with all similar studies, public registration of a study before
anyone is randomised would ensure that participants could be
confident that people would know that the study had at least taken
place. Unique study numbers would help researchers to identify
single studies from multiple publications and reduce the risk of
duplicating the reporting of data. Compliance with CONSORT
(Moher 2001), both on the part of authors and editors, would help
to clarify methodology and many outcomes. Failure to comply
results in both loss of data and confusion in the results, neither of
which help clinicians, patients or managers.
Intention-to-treat analysis should be performed on all outcomes
and all trial data should be made easily accessible. A minimal re-
quirement should be that all data should, at least, be presented as
numbers. In addition, continuous data should be presented with
means, standard deviations (or standard errors) and the number of
participants. Data from graphs, P values of differences and state-
ments of significant or non-significant differences are of limited
value. Unfortunately, in spite of the large numbers of participants
randomised, we were unable to use most of the data in the trials
included in this review due to the high drop-out rates observed as
well as poor data reporting.
2. Specific
As an antipsychotic agent with a novel mechanism of action, arip-
iprazole is an interesting compound, but pragmatic, real world,
randomised controlled trials should be carried out to determine its
value in standard clinical practice. Studies of medium- and long-
term risks, including mortality, behaviour, satisfaction with treat-
ment and cost-effectiveness, in comparison to typical and atypical
antipsychotics, are a priority. Pragmatic entry criteria and non-
blinding with hard endpoints may be helpful in decreasing the
study attrition (Rowland 1998).
A C K N O W L E D G E M E N T S
The Cochrane Schizophrenia Group Editorial Base in Notting-
ham produces and maintains standard text for use in the methods
section of their reviews. We have used this text as the basis of what
appears here and adapted it as required.
We thank Mark Fenton, Judith Wright and Samantha Roberts for
their assistance in the literature searches, and Jun Xia for reviewing
Chinese studies. We would also like to thank Clive Adams, Claire
Irving, Bethany York and John Rathbone for their support during
this review.
R E F E R E N C E S
References to studies included in this review
Adson 2003 {unpublished data only}
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 4. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:176–232.∗ Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets; medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
McEvoy J, Daniel D, Carson WH Jr, McQuade R, Marcus
R. A randomized, double blind, placebo controlled, study
of the efficacy and safety of aripripazole 10, 15, 0r 20 mg/
day for the treatment of patients with acute exacerbations of
the schizophrenia. Journal of Psychiatric Research 2007;41:
895–905.
Carson 2000 a {published data only}
Anutosh S, Ali MW, Ingenito G, Carson WH. Controlled
study of aripiprazole and haloperidol in schizophrenia.
European Psychiatry 2002;Suppl 1:103s.
Carson WH, Ali M, Dunbar G, Ingenito G, Saha AR. A
double-blind, placebo-controlled trial of aripiprazole and
haloperidol. Schizophrenia Research 2001;1-2:221–2.
Carson WH, Ali M, Saha AR, Dunbar GC, Ingenito G. A
double-blind, placebo-controlled trial of aripiprazole and
haloperidol in patients with schizophrenia or schizoaffective
disorder. Proceedings of the 39th Annual Meeting of the
American College of Neuropsychopharmacology; 2000 Dec
10-14; San Juan; Puerto Rico. 2000.∗ Carson WH, Kane JM, Ali M, Dunbar GC, Ingenito G.
Efficacy of aripiprazole in psychotic disorders: comparison
with haloperidol and placebo. Journal of the European
20Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

College of Neuropsychopharmacology 2000;10(Suppl 3):S309.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 4. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm Vol. 2002:176–232.
Kane J, Ingenito G, Ali M. Efficacy of aripiprazole in
psychotic disorders: comparison with haloperidol and
placebo. Schizophrenia Research 2000;1:39.
Kane JM, Carson WH, Saha AR, McQuade RD, Ingenito
GG, Zimbroff DL, Ali MW. Efficacy and safety of
aripiprazole and haloperidol versus placebo in patients
with schizophrenia and schizoaffective disorder. Journal of
Clinical Psychiatry 2002;9:763–71.
Kane JM, Ingenito G, Ali M. Efficacy of aripiprazole in
psychotic disorders: comparison with haloperidol and
placebo. International Journal of Neuropsychopharmacology
2000;Suppl 1:S124.
Kane JM, Ingenito G, Ali M. Efficacy of aripiprazole in
psychotic disorders: comparison with haloperidol and
placebo. Proceedings of the 155th Annual Meeting of
the American Psychiatric Association; 2002 May 18-23;
Philadelphia, PA, USA. 2002.
Kane JM, Ingenito G, Ali M. Efficacy of aripiprazole in
psychotic disorders: comparison with haloperidol and
placebo. Proceedings of the 53rd Annual Meeting of
the American Psychiatric Association; 2000 May 13-18;
Chicago, USA. 2000.
Carson 2002 b {published data only}
Carson W, McQuade R, Saha A, Torbeyns A, Stock E.
Aripiprazole versus placebo for relapse prevention in patients
with chronic schizophrenia. Journal of the European College
of Neuropsychopharmacology 2002;12(Suppl 3):S288.
Carson W, Pigott T, Saha A, Ali M, McQuade RD, Torbeyns
AF, Stock E. Aripiprazole versus placebo in the treatment
of stable, chronic schizophrenia. Proceedings of the156th
Annual Meeting of the American Psychiatric Association;
2003 May 17-22; San Francisco, USA. 2003.∗ Carson WH, Pigott TA, Saha AR, Ali MW, McQuade
RD, Torbeyns AF, Stock EG. Aripiprazole vs placebo in the
treatment of chronic schizophrenia. International Journal of
Neuropsychopharmacology 2002;Suppl 1:S187.
Casey D, Saha A, Marcus R, Carson WH, McQuade RD,
Torbeyns AF, Stock E. Aripiprazole versus placebo for
relapse prevention in patients with chronic schizophrenia.
Schizophrenia Research 2003;60:276.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm 2002:111–75.
Marder SR, Jody D, Kaplita S, Saha A, Carson W, Torbeyns
A, Stock EG. Glycemic control and plasma lipids in long-
term treatment with aripiprazole. Proceedings of the 156th
Annual Meeting of the American Psychiatric Association;
2003 May 17-22; San Francisco, USA 2003.
Pigott TA, Carson WH, Saha AR, Torbeyns AF, Stock EG,
Ingenito GG. Aripiprazole for the prevention of relapse in
stabilized patients with chronic schizophrenia: a placebo-
controlled 26-week study. Journal of Clinical Psychiatry
2003;64(9):1048–56.
Pigott TA, Saha AR, Ali MW, McQuade RD, Torbeyns
AF, William HC, Stock EG. Aripiprazole versus placebo
in the treatment of chronic schizophrenia. Proceedings of
the 155th Annual Meeting of the American Psychiatric
Association; 2002 May 18-23; Philadelphia, PA, USA.
2002.
Stock E, Marder SR, Jody D, Kaplita S, Saha A, Carson
W, Torbeyns A. Plasma lipids levels and glycemic control
in long-term treatment with aripiprazole. Journal of the
European College of Neuropsychopharmacology 2003;13(4):
S327.
Torbeyns A, Marder SR, Carson W, Jody D, Kaplita S, Saba
A, Stock E. Glycemic control and plasma lipids in long-
term treatment with aripiprazole. Schizophrenia Research
2004;67(1):192–3.
Csernansky 2003 {unpublished data only}∗ Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 2. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:51–110.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.
Daniel 2000 {published data only}∗ Daniel DG, Saha AR, Ingenito G, Carson WH,
Dunbar G. Aripiprazole, a novel antipsychotic: overview
of a phase II study result. International Journal of
Neuropsychopharmacology 2000;Suppl 1:S157.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.
Saha AR, Petrie JL, Ali MW. Safety and efficacy profile of
aripiprazole, a novel antipsychotic. Schizophrenia Research
1999;1-3:295.
Daniel 2004 {published data only}
Daniel DG, Stock EG, Wilber CH, Marcus RN, Carson
Jr WH, Manos G, Iwamoto T. Intramuscular aripiprazole
in acutely agitated psychotic patients. Proceedings of
21Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the 157th Annual Meeting of the American Psychiatric
Association; 2004 May 1-6; New York, USA. 2004.
Kungel M, Daniel D, Stock E, Wilber R, Marcus R,
Carson W, Manos G, Iwamoto T. Efficacy and safety of
intramuscular aripiprazole in acutely agitated patients with
psychosis. Thematic Conference of the World Psychiatric
Association on “Treatments in Psychiatry: An Update”;
2004 Nov 10-13; Florence, Italy. 2004.
Marcus 2005 {published data only}
Cutler A, Marcus R, Sterling A, Hardy A, O’Donnell A,
Carson W, McQuade R. The efficacy and safety of lower
doses of Aripripazole for the treatment of patients with
acute exacerbation of schizophrenia. CNS Spectr 2006;11
(9):691–702.
Marcus RN. Efficacy and safety of lower doses of
aripiprazole. Proceedings of the 158th Annual Meeting of
the American Psychiatric Association; 2005 May 21-26;
Atlanta, USA. 2005.
Oren 2005 {published data only}
Andrezina R, Josiassen R, Marcus R, Oren D, Manos
G, Stcok E, Carson W, Iwamoto T. Intramuscular
aripripazole for the treatment of acute agitation in patients
with schizophrenia or schizoaffective disorder: a double
blind, placebo controlled comparison with intramuscular
haloperidol. Psychopharmacology 2006;188:281–92.
Oren D, Marcus R, Kostic D, McQuade R, Iwamoto
T, Archibald D. Efficacy and safety of intramuscular
aripiprazole, haloperidol or placebo in acutely agitated
patients with schizophrenia or schizoaffective disorder.
Schizophrenia Bulletin 2005;31:499.
Yocca F. Intramuscular aripiprazole in acute schizophrenia:
a pivotal phase-three study. Proceedings of the 158th annual
meeting of the American Psychiatric Association; 2005 May
21-26; Atlanta, USA. 2005.
Potkin 2003 {published data only}
Carson WH, Saha AR, Ali M, Dunbar GC, Ingenito G.
Aripiprazole and risperidone versus placebo in schizophrenia
and schizoaffective disorder. Proceedings of the Annual
Meeting of the American Psychiatric Association; 2001 May
5-10; LA, USA. Marathon Multimedia, 2001.
Carson WH, Saha AR, Mirza A, Dunbar GC, Ingenito G.
Aripiprazole and risperidone versus placebo in schizophrenia
and schizoaffective disorder. Proceedings of the 155th
Annual Meeting of the American Psychiatric Association;
2002 May 18-23; Philadelphia, USA. 2002.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 4. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:176–232.
Potkin SG, Kujawa M, Carson WH, Saha AR, Ali M,
Ingenito G. Aripiprazole and risperidone versus placebo in
schizophrenia and schizoaffective disorder. Schizophrenia
Research 2003;60:300.∗ Potkin SG, Saha AR, Kuwaja MJ, Carson WH, Ali
M, Stock E, Stringfellow J, Ingenito G, Marder SR.
Aripiprazole, an antipsychotic with a novel mechanism
of action, and risperidone vs placebo and schizoaffective
disorder. Archives of General Psychiatry 2003;60:681–90.
Saha A, Carson W, Ali M, Dunbar G, Ingenito G. Efficacy
and safety of aripiprazole and risperidone vs. placebo in
patients with schizophrenia and schizoaffective disorder.
Proceedings of the 7th World Congress of Biological
Psychiatry; 2001 Jul 1-6; Berlin, Germany. 2001.
Yeung P, Kujawa M, Carson WH, Saha A, Alid M,
Ingenito G. Aripiprazole and risperidone versus placebo in
schizophrenia and schizoaffective disorder. Schizophrenia
Research 2002;3(Suppl 1):185–6.
Yeung P, McQuade RD, Carson WH, Saha A, Ali MW,
Ingenito G. Aripiprazole and risperidone versus placebo in
schizophrenia. European Psychiatry 2002;Suppl 1:102s.
Yeung PP, Carson WH, Saha A, McQuade RD, Ali M,
Stringfellow JC, Ingenito G. Efficacy of aripiprazole, a novel
antipsychotic, in schizophrenia and schizoaffective disorder:
results of a placebo-controlled trial with risperidone.
European Neuropsychopharmacology 2001;11(3):259.
References to studies excluded from this review
Allain 2005 {published and unpublished data}∗ Allain H. A prospective, multicenter, open-label
study of aripiprazole in the management of patients
with schizophrenia in general psychiatric practices
(Broad Effectiveness Trial With Aripiprazole- BETA).
www.clinicaltrials.gov 2005.
Auby 2002 {published data only}∗ Auby P, Saha A, Ali M, Ingenito G, Wilber R,
Bramer S. Safety and tolerability of aripiprazole at doses
higher than 30 mg. Journal of the European College of
Neuropsychopharmacology 2002;Suppl 3:S288.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 111–75.
Saha AR, Ali MW, Ingenito GG, Wilber R, Luo X, Bramer
S. Safety and tolerability of aripiprazole at doses higher than
30 mg. International Journal of Neuropsychopharmacology
2002;Suppl 1:S185.
Saha AR, Ali MW, Ingenito GG, Wilber R, Luo X, Bramer
S. Safety and tolerability of aripiprazole at doses higher
than 30 mg. Proceedings of the 155th Annual Meeting of
the American Psychiatric Association; 2002 May 18-23;
Philadelphia, PA, USA. 2002.
Beuzen 2005 {published data only}
Beuzen J-N, Pans M, Modell S, Hagens P, McQuade R,
Iwamoto T, Carson W. Naturalistic study of aripiprazole
22Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

treatment. Proceedings of the XIII World Congress of
Psychiatry; 2005 10-15th Sept; Cairo, Egypt. 2005.
Blonde 2004 {published data only}
Blonde L, Ray S, Corey-Lisle PK, Cislo PR, L’Italien G.
The risk of new-onset type 2 diabetes and coronary heart
disease in chronic schizophrenic patients treated with
aripiprazole and olanzapine. Journal of the European College
of Neuropsychopharmacology 2004;14(Suppl 3):S275.
Carson 2002 a {published data only}∗ Carson WH, Ingenito GG, McQuade RD, Stock
EG, Iwamoto T. [Schizophrenia; safety/tolerability of
aripiprazole]. Proceedings of the XIIth World Congress of
Psychiatry; 2002 Aug 24-29; Yokohama, Japan. 2002.
Carson W, McQuade 2003 {published data only}
Carson W, McQuade R, Abou-Gharbia N, Iwamoto
T, Archibald D, Stock E. Long-term weight effects of
aripiprazole and olanzapine: results from a 26-week double-
blind comparison study. Journal of the European College of
Neuropsychopharmacology 2004;14(Suppl 3):S259.
Casey 2003 {published data only}∗ Casey D, Saha AR, Ali MW, Jody DN, Kujawa MJ, Stock
EG, Ingenito GG. Switching to aripiprazole monotherapy.
International Journal of Neuropsychopharmacology 2002;
Suppl 1:S187.
Casey DE, Carson WH, Saha AR, Liebeskind A, Ali MW,
Jody D, Ingenito GG. Switching patients to aripiprazole
from other antipsychotic agents: a multicenter randomised
study. Psychopharmacology 2003;166:391–9.
Casey DE, Saha AR, Ali MW, Jody D, Kujawa MJ, Stock
EG, Ingenito GG. Switching to aripiprazole monotherapy.
Proceedings of the 155th Annual Meeting of the American
Psychiatric Association; 2002 May 18-23; Philadelphia, PA,
USA. 2002.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.
Kujawa M, Saha AR, Ali MW, Jody DN, McQuade RD,
Ingenito GG. Switching to aripiprazole monotherapy.
Schizophrenia Research 2003;60:290.
Medori R, Gharbia N, Saha A, Ali M, Stock E, Ingenito
G. Switching to aripiprazole monotherapy. Journal of the
European College of Neuropsychopharmacology 2002;Suppl 3:
S292.
Chan 2007 {published data only}
Chan H-Y, Lin W-W, Lin S-K, Hwang T-J, Su T-P, Chiang
S-C, Hwu H-G. Efficacy and safety of aripiprazole in the
acute treatment of schizophrenia in Chinese patients with
risperidone as an active control: a randomized trial. Journal
of Clinical Psychiatry 2007;68(1):29–36.
Chen 2005 b {published data only}
Chen J-D, Zhao J-P, Li L-H, Guo X-F, Zhai J-G, Wang C-
Y, Xie S-P, Gao C-G, Ding Y, Chen Y-G. A multicenter,
randomized and double-blind controlled clinical trial of
aripiprazole in treatment of schizophrenia. Chinese Journal
of New Drugs and Clinical Remedies 2005;24(11):845–8.
Chrzanowski 2006 {published data only}
Chrzanowski WK, Marcus RN, Torbeyns A, Nyilas M,
McQuade RD. Effectiveness of long-term aripiprazole
therapy in patients with acutely relapsing or chronic, stable
schizophrenia: a 52-week, open-label comparison with
olanzapine. Psychopharmacology 2006;189(2):259–66.
Corey-Lisle 2006 {unpublished data only}
Corey-Lisle PK, Kolotkin RL, Crosby RD, L’Italien GJ.
Changes in weight and weight-related quality of life in
aripiprazole versus standard-of-care treatment. Proceedings
of the 159th Annual Meeting of the American Psychiatric
Association; 2006 May 20-25, Toronto, Canada. 2006.
Daniel 2006 {unpublished data only}
Daniel DG, Crandall D, Manos G, McQuade RD,
Gutierrez-Esteinou R, Pikalov AA, Oren D. Transitioning
from intramuscular (IM) to oral aripiprazole in patients
with schizophrenia. Proceedings of the 159th Annual
Meeting of the American Psychiatric Association; 2006 May
20-25, Toronto, Canada. 2006.
Fan 2005 a {published data only}
Fan W-L, Yu C-M, Wen J-S. Efficacy analysis of aripiprazole
and clozapine in the treatment of schizophrenia. Journal of
North Sichuan Medical College 2005;20(4):377–9.
Gismondi R, Mel2 {published data only}
Gismondi R, Meltzer H, Kujawa M, Carson W, Stringfellow
J, Iwamoto T, Marcus R, Stock E. Aripiprazole versus
perphenazine in treatment-resistant schizophrenia.
Proceedings of the XXIVth Collegium Internationale
Neuro-Psychopharmacologicum Congress; 2004 June 20-
24, Paris, France 2004.
Han 2005 a {published data only}
Han P, Zhang Y-H, Zhang Y-Q. A controlled study of
schizophrenia treated with aripiprazole and clozapine.
Chinese Journal of Rehabilitation Theory and Practice 2005;
11(10):853–4.
Hwang 2005 {published data only}
Hwang TJ, Chan HY, Lin WW, Lin SK, Hwu HG, Cheng
MY, Forbes R. Aripiprazole versus risperidone in the
treatment of acutely relapsed patients with schizophrenia
in Taiwan: a randomized controlled trial. Journal of the
European College of Neuropsychopharmacology 2005;15
(Suppl 3):S497.
Jody 2004 {published data only}
Jody D, Tandon R, Stock E, Riera L, Kujawa M, Lam
S, Pans M, Iwamoto T, Carson W. A naturalistic study
of aripiprazole treatment in a general psychiatric setting.
Proceedings of the XXIVth Collegium Internationale
Neuro-Psychopharmacologicum Congress; 2004 June 20-
24, Paris, France 2004.
Kane 2003 {unpublished data only}∗ Kane J, Carson W, Kujawa M, Stringfellow J, Marcus R,
Sanchez R, Meltzer HY. Aripiprazole vs. perphenazine in
treatment-resistant schizophrenia. Proceedings of the 156th
23Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Annual Meeting of the American Psychiatric Association;
2003 May 17-22; San Francisco, USA. 2003.
Kane J, Carson Wh, Kujawa M, Stringfellow J, Marcus
R, Sanchez R, Iwamoto T, Meltzer H. Aripiprazole in
treatment-resistant schizophrenia: a 6-week double- blind
comparison study versus perphenazine. Schizophrenia
Research 2004;67(1):155–6.
McQuade R, Jody D, Kane J, Carson W, Kujawa M,
Stringfellow J, Marcus R, Sanchez R, Meltzer HY. Efficacy
and safety of aripiprazole versus perphenazine in treatment-
resistant schizophrenia. Journal of the European College of
Neuropsychopharmacology 2003;13(4):S326.
McQuade R, Jody D, Kane J, Carson W, Kujawa M,
Stringfellow J, Marcus R, Sanchez R, Meltzer HY. Efficacy
and safety of aripiprazole versus perphenazine in treatment-
resistant schizophrenia. Journal of the European College of
Neuropsychopharmacology 2003;13(4):S326.
Meltzer HY, Kujawa MJ, Carson Jr WH, Stringfellow
J, Iwamoto T, Marcus RN, Stock EG. Aripiprazole and
perphenazine in severe treatment-resistant schizophrenia.
Proceedings of the 157th Annual Meeting of the American
Psychiatric Association; 2004 May 1-6; New York, USA.
2004.
Sanchez R, Meltzer HY, Marcus RN, Stringfellow J,
Carson WH, Kane JM. Aripiprazole versus perphenazine in
treatment - resistant schizophrenia. Schizophrenia Bulletin
2005;31:502.
Kane 2006 d {published and unpublished data}
Kane JM, Swyzen W, Wu X, McQuade R, Gutierrez-
Esteinou R, Van Tran Q, Marcus R. Long-term symptomatic
remission in schizophrenia patients treated with aripiprazole
or haloperidol. Proceedings of the 159th Annual Meeting
of the American Psychiatric Association; 2006 May 20-25,
Toronto, Canada. 2006.
Kane 2007 a {published data only}
Kane JM, Meltzer HY, Carson WH Jr, McQuade RD,
Marcus RN, Sanchez R, Aripiprazole Study Group.
Aripiprazole for treatment-resistant schizophrenia: results of
a multicenter, randomized, double-blind, comparison study
versus perphenazine. Journal of Clinical Psychiatry 2007;68
(2):213–23.
Kern 2001 {published data only}
Carson W, Cornblatt B, Saha A, Ali M, Kern R, Green M.
Neurocognitive benefits of aripiprazole versus olanzapine
in stable psychosis. Journal of the European College of
Neuropsychopharmacology 2002;Suppl 3:S291.
Cornblatt B, Kern RS, Carson WH, Ali MW, Luo X,
Green M. Neurocognitive effects of aripiprazole versus
olanzapine in stable psychosis. International Journal of
Neuropsychopharmacology 2002;Suppl 1:s185.
Cornblatt B, Kern RS, Carson WH, Stock E, Ali
M, Ingenito G, Green MF. Neurocognitive effects of
aripiprazole versus olanzapine in patients with stable
psychosis. Journal of Psychopharmacology 2002;16(3):A15.
Cornblatt B, Kern RS, Carson WH, Stock E, Ali
M, Ingenito G, Green MF. Neurocognitive effects of
aripiprazole versus olanzapine in patients with stable
psychosis. Schizophrenia Research 2002;3(Suppl 1):27.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–75.∗ Kern RS, Cornblatt B, Carson WH, Dunbar G, Ali M,
Ingenito G, Green MF. An open-label comparison of the
neurocognitive effects of aripiprazole versus olanzapine in
patients with stable psychosis. Schizophrenia Research 2001;
1-2:234.
Kern RS, Cornblatt B, Carson WH, Stock E, Saha AR,
Ali MW, Ingenito G, Green MF. Neurocognitive effects:
aripiprazole vs olanzapine in stable psychosis. European
Psychiatry 2002;Suppl 1:104s.
Kim 2006 d {published data only}
Kim JG, Cho DH, Lee SJ, Lee JK, Wang KS, Seo YI, Choi
SJ, Joo MJ, Kim HD, Lee KH, Kwon YJ, Han KR. The
comparison of efficacy between aripiprazole and haloperidol
in treatment of chronic schizophrenia and schizoaffective
disorder: results for 16-week clinical study. Journal of the
European College of Neuropsychopharmacology 2006;16
(Suppl 4):S417.
Kujawa 2002 {published data only}
Archibald DG, Manos G, Stock E, Jody D, Tourkodimitris
S, Marcus R, Iwamoto T, Yamamoto Y. Effects of long-
term aripiprazole therapy on the negative symptoms of
schizophrenia. Schizophrenia Research 2004;67(1):155.
Archibald DG, Manos G, Tourkodimitris S, Iwamoto T,
Carson WH, Stock E, Marcus R. Reduction in negative
symptoms of schizophrenia during long-term therapy with
aripiprazole. Schizophrenia Research 2003;60:271.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 1. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:1–50.
Kasper S, Lerman MN, McQuade RD, Saha A, Carson
WH, Ali M, Archibald D, Ingenito G, Marcus R, Pigott
T. Efficacy and safety of aripiprazole vs. haloperidol
for long-term maintenance treatment following acute
relapse of schizophrenia. International Journal of
Neuropsychopharmacology 2003;6(4):325–37.
Kostic D, Manos G, Stock E, Jody D, Archibald D,
Tourkodimitris S, Marcus R. Long-term effects of
aripiprazole on the negative symptoms of schizophrenia.
Journal of the European College of Neuropsychopharmacology
2003;13(4):S328.∗ Kujawa M, Saha AR, Ingenito GG, Ali MW, Luo X,
Archibald DG, Carson WH. Aripiprazole for long-term
maintenance treatment of schizophrenia. International
Journal of Neuropsychopharmacology 2002;Suppl 1:S186.
Kujawa MJ, Saha AR, Ingenito GG, Ali MW, Luo X,
Archibald DG, William Jr HC. Aripiprazole for long-term
maintenance treatment in schizophrenia. Proceedings of
the 155th Annual Meeting of the American Psychiatric
Association; 2002 May 18-23; Philadelphia, PA, USA.
24Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

2002.
Manos G, Stock EG, Jody D, Archibald DG, Tourkodimitris
S, Marcus RN. Long-term effects of aripiprazole on the
negative symptoms of schizophrenia. Proceedings of
the 156th Annual Meeting of the American Psychiatric
Association; 2003 May 17-22; San Francisco, USA. 2003.
McQuade R, Carson W, Saha A, Ingenito G, Ali M,
Archibald D. Aripiprazole for long-term maintenance
treatment of schizophrenia. Journal of the European College
of Neuropsychopharmacology 2002;12(Suppl 3):S288.
McQuade RD, Kujawa M, Saha AR, Ingenito GG, Ali
MW, Luo X, Archibald DG, Carson WH. Aripiprazole
for long-term maintenance treatment of schizophrenia.
Schizophrenia Research 2003;60:295.
Saha AR, Carson WH, Mcquade RD, Stock EG, Inada I,
Ali MW. Long-term aripiprazole therapy in schizophrenia.
Proceedings of the XIIth World Congress of Psychiatry;
2002 Aug 24-29; Yokohama, Japan. 2002.
Stock E, Archibald DG, Tourkodimitris S, Kujawa M,
Marcus R, Carson W, Iwamoto T. Long-term effects of
aripiprazole and haloperidol on affective symptoms of
schizophrenia. Schizophrenia Research 2004;67(1):158–9.
Stock EG, Achibald DG, Tourkodimitris S, Kuwaja
MJ, Marcus RN, Carson Jr WH. Long-term effects of
aripiprazole on affective symptoms of schizophrenia.
Proceedings of the 156th Annual Meeting of the American
Psychiatric Association; 2003 May 17-22; San Francisco,
USA. 2003.
Kujawa 2003 {published data only}
Kujawa M, Stringfellow J, Hardy S, Ali M, Iwamoto T,
Lam S, Marcus R, Stock E. Efficacy, safety, and tolerability
of aripiprazole in patients with schizoaffective disorder.
Schizophrenia Research 2004;67(1):156.
Kujawa MJ, Stringfellow J, Hardy S, Ali M, Marcus RN,
Stock EG. The efficacy of aripiprazole in patients with
schizoaffective disorder. Proceedings of the 156th Annual
Meeting of the American Psychiatric Association; 2003 May
17-22; San Francisco, USA. 2003.
Kujawa 2004 {published data only}
Kujawa MJ, McQuade RD, Jody DN, Carson WH, Abou-
Gharbia N, Iwamoto T, Archibald DG, Stock EG. Long-
term weight effects of aripiprazole vs olanzapine in a 26-
week, double-blind study. Proceedings of the XXIVth
Collegium Internationale Neuro-Psychopharmacologicum
Congress; 2004 June 20-24, Paris, France 2004.
Liang 2005 {published data only}
Liang J, Chen D. Aripiprazole and haloperidol in the
treatment of schizophrenia. China Pharmaceuticals 2005;14
(6):82.
Mai 2005 {published data only}
Mai G-Y, Cai G-H, Huang J-M. Comparative study on
the effect of aripiprazole and risperidone on schizophrenia.
Chinese Journal of Rehabilitation 2005;20(3):184–5.
Mallikaarjun 2000 {published data only}∗ Mallikaarjun S, Salazar DE, Bramer SL. Pharmacokinetics,
tolerability, and safety of aripiprazole following single and
multiple oral dose administration. Journal of the European
College of Neuropsychopharmacology 2000;Suppl 3:S306.
Mallikaarjun S, Salazar DE, Bramer SL. The
pharmacokinetics, tolerability, and safety of aripiprazole
following single and multiple oral dose administration.
International Journal of Neuropsychopharmacology 2000;
Suppl 1:S123.
Marcus 2003 {published data only (unpublished sought but not used)}
Marcus RN, Kostic D, Stringfellow J, Hardy S, Carson
WH, Stock EG. Effects of aripiprazole on excitement
and hostility: Symptoms of schizophrenia. Proceedings
of the 156th Annual Meeting of the American Psychiatric
Association; 2003 17-22 May; San Francisco, USA. 2003.
Marder 2004 {published data only}
Marder SR, Archibald DG, Manos G, Stock EG, Jody DN,
Tourkodimitris S, Marcus RN, Iwamoto T, Yamomoto
Y, Carson WH. Long-term effects of aripiprazole therapy
on the negative symptoms of schizophrenia. Proceedings
of the XXIVth Collegium Internationale Neuro-
Psychopharmacologicum Congress; 2004 June 20-24; Paris,
France 2004.
McQuade 2002 {published data only}
McQuade R, Carson W, Saha A, Ingenito G, Ali M,
Archibald D. Aripiprazole for long-term maintenance
treatment of schizophrenia. Journal of the European College
of Neuropsychopharmacology 2002;12(S3):S288.
McQuade 2003 {unpublished data only}
Abou Gharbia N, McQuade R, Jody D, Kujawa M, Carson
W, Iwamoto T, Archibald D, Stock E. Comparative study
of the long-term effects of aripiprazole and olanzapine
treatment on body weight. Proceedings of the Thematic
Conference of the World Psychiatric Association on
“Treatments in Psychiatry: An Update”; 2004 Nov 10-13;
Florence, Italy. 2004.
Dubitsky GM, Harris R, Laughren T, Hardeman S. Abilify
(aripiprazole) tablets, medical review part 3. www.fda.gov/
cder/foi/nda/2002/21-436˙Abilify.htm. U.S. Food and
Drug Administration CDER, 2002:111–175.
Jody D, Mcquade Rd, Kujawa M, Carson W, Iwamoto
T, Archibald D, Stock E. Long-term weight effects of
aripiprazole versus olanzapine. Schizophrenia Research 2004;
67(1):187.∗ McQuade RD, Jody DN, Kujawa MJ, Carson WH,
Iwamoto T, Archibald DG, Stock EG. Long-term weight
effects of aripiprazole versus olanzapine. Proceedings of
the 156th Annual Meeting of the American Psychiatric
Association; 2003 May 17-22; San Francisco, USA. 2003.
McQuade RD, Stock E, Marcus R, Jody D, Gharbia NA,
Vanveggel SAD, Carson WH. A comparison of weight
change during treatment with olanzapine or aripiprazole:
results from a randomized, double-blind study. Journal of
Clinical Psychiatry 2004;65(Suppl 18):47–56.
Modell 2005 b {published data only}
Modell S, Jody D, Kujawa M, Carson W, Stringfellow J,
Iwamoto T, Marcus R, Stock E T. Efficacy of aripiprazole
and perphenazine in severe schizophrenia resistant to
25Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

treatment with atypical antipsychotics. Journal of the
European College of Neuropsychopharmacology 2004;14
(Suppl 3):S265.
N0025078569 {published data only}
N0025078569. A multi-centre, d-b, randomised
comparative study of aripiprazole and olanzapine in the
treatment of patients with acute schizophrenia. National
Research Register 2001; Vol. 1.
Newcomer 2006 {unpublished data only}
Newcomer JW, L’Italien G, Vester-Blokland, McQuade
RD, Carson WH, Marcus RN. Improvement of non-
HDL cholesterol levels among patients randomized to
aripiprazole versus olanzapine. Proceedings of the 159th
Annual Meeting of the American Psychiatric Association;
2006 May 20-25, Toronto, Canada. 2006.
Octavio 2004 {published data only}
Octavio I, Stock EG, Archibald DG, Tourkodimitris S,
Kujawa MJ, Marcus R, Carson WH, Iwamoto T. Long-
term effects of aripiprazole on affective symptoms of
schizophrenia. Proceedings of the XXIVth Collegium
Internationale Neuro-Psychopharmacologicum Congress;
2004 June 20-24 Paris, France 2004.
Octavio 2005 {published data only}
Octavio I, Stock E, Archibald D, Tourkodimitris S, Kujawa
M, Marcus R, Carson W, Iwamoto T. Long-term effects
of aripiprazole on affective symptoms of schizophrenia.
Journal of the European College of Neuropsychopharmacology
2004;14(Suppl 3):S261.
Petrie 1997 {published and unpublished data}∗ Petrie JL, Saha JR, McEvoy JP. Aripiprazole, a new typical
antipsychotic: phase 2 clinical trial result. Proceedings of
the 10th European College of Neuropsychopharmacology
Congress; Sep 13-17; Vienna, Austria. 1997.
Ray 2005 {published data only}
Ray S, Corey-Lisle PK, Cislo PR, L’Italien G, Weiden
P. An economic evaluation of aripiprazole compared to
olanzapine based on metabolic side-effect profile. Journal of
the European College of Neuropsychopharmacology 2004;14
(Suppl 3):S279.
Riera 2004 {published data only}
L’Italien GJ, Tandon R, Han J, Li H, Ray S, Carson W.
Schizophrenic patients treated with aripiprazole exhibit
improved overall effectiveness compared to patients treated
with atypical antipsychotics. Proceedings of the Thematic
Conference of the World Psychiatric Association on
“Treatments in Psychiatry: An Update”; 2004 Nov 10-13;
Florence, Italy. 2004.
McQuade RD. Investigator assessment of clinical
parameters after initiating aripiprazole therapy. Proceedings
of the 158th Anual Meeting of the American Psychiatric
Association; 2005 May 21-26; Atlanta, USA. 2005.
Octavio I, Tandon R, Stock E, Riera L, Kujawa M, Lam
S, Pans M, Iwamoto T, Carson W. A naturalistic study
of aripiprazole treatment in a general psychiatric setting.
Proceedings of the Thematic Conference of the World
Psychiatric Association on “Treatments in Psychiatry: An
Update”; 2004 Nov 10-13; Florence, Italy. 2004.
Riera L, Hu R, Stock E, Nyilas M, Torbeyns A, Borian F,
Gentile K, Carson W, Iwamoto T. Broad effectivness trial
with aripiprazole. Proceedings of the 157th Annual Meeting
of the American Psychiatric Association; 2004 May 1-6;
New York, USA. 2004.
Tandon R, Han J, Litalien G, Ray S, Carson Jr WH.
Investigator’s assessment questionnaire of antipsychotics’
effectiveness. Proceedings of the 157th Annual Meeting of
the American Psychiatric Association; 2004 May 1-6; New
York, USA. 2004.
Tandon R, Stock EG, Kujawa MJ, Torbeyns AF, Borian
FE, Riera L, McQuade RD. Broad effectiveness trial
with aripiprazole. Proceedings of the 55th Institute on
Psychiatric Services of the American Psychiatric Association;
2003 October/November; Boston, USA. 2003.
Tandon R, Stock EG, Riera L, Kujawa MJ, Lam S, Pans
M, Iwamoto T. A naturalistic trial with aripiprazole in a
general psychiatric setting. Proceedings of the 157th Annual
Meeting of the American Psychiatric Association; 2004 May
1-6; New York, USA. 2004.
Saha 2004 {published data only}
Saha AR, Brown D, McEvoy J, Ali M, Abou-Gharbia N,
Stock S, Iwamoto T. Tolerability and efficacy of aripiprazole
in patients with first episode schizophrenia: An open label
pilot study. Proceedings of the 12th Biennial Winter
Workshop on Schizophrenia; 2004 Feb 7-13; Davos,
Switzwerland. 2004.
Sanchez 2006 {published data only}
Sanchez R, Kostic D, Stock E, Torbeyns AF, Kerselaers
W, Nyilas M, McQuade R, Carson WH, Marcus RN.
Aripiprazole vs olanzapine in patients with acutely relapsing
or chronic, stable schizophrenia: a 52-week open-label
extension study. Proceedings of the 13th Biennial Winter
Workshop on Schizophrenia Research; 2006 Feb 4-10,
Davos, Switzerland. 2006.
STAR 2006 {published and unpublished data}
Corey-Lisle P, Kolotkin RL, Crosby RD, L’Italien G.
Changes in weight and weight-related quality of life in
aripiprazole versus standard-of-care treatment. Proceedings
of the 14th Congress of the Association of European
Psychiatrists; 2006 March 4-8; Nice, France. 2006.
Hanssens L, Biro E, Dillenschneider A, Spitzerova H,
McQuade R, Iwamoto T. Reasons for participation and
preference of medicine in community-treated schizophrenic
patients in a naturalistic setting (schizophrenia trial of
aripiprazole: star study). Proceedings of the 14th Congress
of the Association of European Psychiatrists; 2006 March 4-
8; Nice, France. 2006.
Hanssens L, L’Italien G, Marcus RN, McQuade R, Carson
WH, Beuzen JN. Effectiveness of aripiprazole versus
olanzapine, quetiapine, or risperidone: sub-analysis of a
large, randomized, naturalistic study (STAR). Journal of the
European College of Neuropsychopharmacology 2006;16(4):
S421.
Hanssens L, L’Italien G, Marcus RN, McQuade RD,
26Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Carson WH, Beuzen J-N. Evaluation of quality of life in
community-treated schizophrenic patients: a naturalistic
open-label study comparing aripiprazole to standard-of-care.
Proceedings of the 159th Annual Meeting of the American
Psychiatric Association; 2006 May 20-25, Toronto, Canada.
2006.
Hanssens L, L’Italien G, Marcus RN, McQuade RD,
Carson WH, Beuzen J-N. Reasons for switching among
community-treated schizophrenic patients in a naturalistic
setting : schizophrenia trial of aripiprazole: STAR study.
Proceedings of the 159th Annual Meeting of the American
Psychiatric Association; 2006 May 20-25, Toronto, Canada.
2006.
Hanssens L, L’Italien G, Marcus RN, McQuade RD, Carson
WH, Beuzen J-N. Sexual dysfunction in a naturalistic
open label study of aripiprazole and standard of care in the
management of community-treated schizophrenic patients.
Proceedings of the 159th Annual Meeting of the American
Psychiatric Association; 2006 May 20-25, Toronto, Canada.
2006.
Hanssens L, L’Italien G, McQuade R, Iwamoto T, Pans
M. Evaluation of quality of life in community-treated
schizophrenic patients: a naturalistic open-label study
comparing aripiprazole to standard care (schizophrenia
trial of aripiprazole: star study). Proceedings of the 14th
Congress of the Association of European Psychiatrists; 2006
March 4-8; Nice, France. 2006.
Kerwin R, L’Italien G, Hanssens L, Marcus RN,
McQuade R, Carson WH, Beuzen JN. Effectiveness
of aripiprazole versus standard of care treatment in
patients with schizophrenia: the Schizophrenia Trial of
Aripiprazole (STAR) study. Journal of the European College
of Neuropsychopharmacology 2006;16(4):S411.
Kerwin R, L’Italien G, Hanssens L, Marcus RN, McQuade
RD, Beuzen J-N. Effectiveness of aripiprazole versus
standard of care: schizophrenia trial of aripiprazole (STAR
trial). Proceedings of the 159th Annual Meeting of the
American Psychiatric Association; 2006 May 20-25,
Toronto, Canada. 2006.
L’Italien G, Hanssens L, Marcus RN, McQuade RD, Carson
WH, Beuzen J-N. Metabolic effects of aripiprazole versus
standard of care (the STAR trial). Proceedings of the 159th
Annual Meeting of the American Psychiatric Association;
2006 May 20-25, Toronto, Canada. 2006.
Stock 2005 {published data only}
McQuade R, Kostic D, Marcus R, Carson W, Torbeyns A,
Kerselaers W, Yocca F. Aripiprazole versus olanzapine in a
52-week open label extension study. Schizophrenia Bulletin
2005;31:496–7.
Stock EG. Aripiprazole versus olanzapine in schizophrenia:
A 52-week, open-label study. Proceedings of the 158th
Annual Meeting of the American Psychiatric Association;
2005 May 21-26; Atlanta, USA. 2005.
Stroup 2003 {published data only}
Stroup TS, McEvoy JP, Swartz MS, Byerly MJ, Glick
ID, Canive JM, McGee MF, Simpson GM, Stevens MC,
Lieberman JA. The National Institute of Mental Health
Clinical Antipsychotic Trials of Intervention Effectiveness
(CATIE) project: schizophrenia trial design and protocol
development. Schizophrenia Bulletin 2003;29(1):15–31.
Tandon 2006 {published data only}
Tandon R, Marcus RN, Stock EG, Riera LC, Kostic D,
Pans M, McQuade RD, Nyilas M, Iwamoto T, Crandall
DT. A prospective, multicenter, randomized, parallel-group,
open-label study of aripiprazole in the management of
patients with schizophrenia or schizoaffective disorder in
general psychiatric practice: Broad Effectiveness Trial With
Aripiprazole (BETA). Schizophrenia Research 2006;84(1):
77–89.
Wang 2005 {published data only}
Wang G-P, Xie R, Pei G-X. A comparative study between
aripiprazole and chlorpromazine in the treatment of
schizophrenia. Shandong Archives of Psychiatry 2005;18(4):
250–1.
Wang 2005 j {published data only}
Wang R, Liu Y, Ning Z. A controlled study of aripiprazole
vs clozapine in the treatment of first-episode schizophrenia.
Journal of Clinical Psychosomatic Diseases 2005;11(4):301–2.
Wu 2005 d {published data only}
Wu J-D, Li Y-D, Song Z-W. Effect of aripiprazole or haldol
on intelligence and memory in the first-onset schizophrenia.
Chinese Journal of Rehabilitation Theory and Practice 2006;
12(1):64–5.
Xia 2005 {published data only}
Xia S-Y, Hua P, Nie Y-B. A treatment study of schizophrenia
with aripiprazole and chlorpromazine. Practical Clinical
Medicine 2005;6(10):33–4.
Ye 2005 {published data only}
Ye X-R, Xia X-L. A comparative study between aripiprazole
and risperidone in treatment of first-onset schizophrenia.
Medical Journal of National Defending Forces in Southwest
China 2005;15(6):616–8.
Zhang 2005 {published data only}
Zhang Y, Gu Z, Sun A. Aripiprazole on the quality of life
of patients with schizophrenia. Journal of Jining Medical
College 2005;28(4):50–1.
Zhang 2005 a {published data only}
Zhang Y, Liu X, Li X-Y, Wang W. Aripiprazole and
risperidone in the treatment of schizophrenia. Chinese
Journal of Behavioural Medical Sciences 2005;14(10):923–5.
Zhao 2005 {published data only}
Zhao Z-Z, Li X-L, Zou Z-M. A comparative study on
aripiprazole and sulpiride in treating schizophrenia whose
predominant clinical features were negative symptoms.
Medical Journal of Chinese People Health 2005;17(12):
728–30.
Zhi 2005 {published data only}
Zhi S-L. Comparison study of aripiprazole and risperidone
on schizophrenia. Modern Journal of Integrated Traditional
Chinese and Western Medicine 2005;14(21):2787–8.
27Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Zhu 2005 {published data only}
Zhu L, Wu H, Huang S, Liu X-X. Aripiprazole and
risperidone in the treatment of schizophrenia-control study.
Nervous Diseases and Mental Hygiene 2005;5(4):282.
Zhu 2005 a {published data only}
Zhu P-J, Cheng Z-E, Zhang J, Zhu P-L, Zhan X-M.
Clinical study of therapeutic effects of aripiprazole in
treatment of patients with schizophrenia. Chinese Journal
of Clinical Pharmacology and Therapeutics 2005;10(10):
1194–7.
Zhu 2005 b {published data only}
Zhu L, Wu H, Huang S, Liu X-X. Aripiprazole and
risperidone in the treatment of schizophrenia. Shanghai
Medical and Pharmaceutical Journal 2005;26(9):425–6.
References to studies awaiting assessment
Carson 2008 {published and unpublished data}
Carson WH, Nyilas M, Forbes RA, Pikalov A, McQuade
RD, Ivanova S, Owen R, Ginsberg L, Wagner KD. Acute
efficacy of aripripazole for the treatment of bipolar 1
disorder in paediatric patients. Schizophrenia Research 2008;
98:42.
Nyilas 2007 {unpublished data only}
Nyilas M, Findling RL, Johnson B, Forbes RA, Pikalov
A, Marcus R, Carson WH, Robb A. Proceedings of
the 46th Annual Meeting of the American College of
Neuropsychopharmacology; 2007 Dec 9-13; Florida, USA.
2007.
Additional references
Abilify 2006
Otsuka America Pharmaceutical Inc. Abilify (aripiprazole).
www.abilify.com (accessed 10 April 2010).
Altman 1996
Altman DG, Bland JM. Detecing skewness from summary
information. BMJ 1996;313:1200.
Anath 2003
Anath J, Venkatesh R, Burgoyne K, Augustines D, Corpuz
V, Gunatilake S. Weight gain associated with atypical
antipsychotic drugs: mechanisms and management. Expert
Review of Neurotherapeutics 2003;3(1):59–68.
Arnt 1998
Arnt J, Skarsfeldt T. Do novel antipsychotics have similar
pharmacological characteristics? A review of the evidence.
Neuropsychopharmacology 1988;18:63–101.
Bhattacharjee 2008
Bhattacharjee J, El-Sayeh HGG. Aripiprazole versus typical
antipsychotic drugs for schizophrenia. Cochrane Database
of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/
14651858.CD006617.pub2]
Boissel 1999
Boissel JP, Cucherat M, Li W, Chatellier G, Gueyffier F,
Buyse M, Boutitie F, Nony P, Haugh M, Mignot G. The
problem of therapeutic efficacy indices. 3. Comparison of
the indices and their use. Therapie 1999;54(4):405–11.
Burris 2002
Burris KD, Molski TF, Xu C, Ryan E, Tottori K, Kikuchi T,
Yocca FD, Molinoff PB. Aripiprazole, a novel antipsychotic,
is a high-affinity partial agonist at human dopamine
D2 receptors. Journal of Pharmacology and Experimental
Therapeutics 2002;302(1):381–9.
Cannon 1996
Cannon M, Jones P. Schizophrenia. Journal of Neurology,
Neurosurgery and Psychiatry 1996;60:604–13.
Carpenter 1994
Carpenter WT Jr, Buchanan RW. Schizophrenia. New
England Journal of Medicine 1994;330:681–90.
Carson 2000
Carson WH, Kane JM, Ali M, Dunbar GC, Ingenito
G. Efficacy of aripiprazole in psychotic disorders:
comparison with haloperidol and placebo. European
Neuropsychopharmacology 2000;10(Suppl 3):S309.
Deeks 2000
Deeks J. Issues in the selection for meta-analyses of binary
data. Proceedings of the 8th International Cochrane
Colloquium; 2000 Oct 25-28th; Cape Town, South Africa.
2000.
Egger 1997
Egger M, Davey-Smith G, Schneider M, Minder C. Bias
in meta-analysis detected by a simple, graphical test. BMJ
1997;315:629–34.
El-Sayeh 2006
El-Sayeh HG, Morganti C. Aripiprazole for schizophrenia.
Cochrane Database of Systematic Reviews 2006, Issue 2.
[DOI: 10.1002/14651858.CD004578.pub3]
Elbourne 2002
Elbourne DR, Altman DG, Higgins JP, Curtin F,
Worthington HV, Vail A. Meta-analyses involving cross-
over trials: methodological issues. International Journal of
Epidemiology 2002;31(1):140–9.
FDA 2002a
U.S. Federal Drug Administration CDER. Abilify
(aripiprazole) tablets, medical review. www.fda.gov/cder/
foi/nda/2002/21-436˙Abilify.htm 2002.
Grunder 2006
Grunder G, Kungel M, Ebrecht M, Göröcs T, Modell
S. Aripiprazole: pharmacodynamics of a dopamine
partial agonist for the treatment of schizophrenia.
Pharmacopsychiatry 2006;39(Suppl 1):S21–5.
Guy 1976
Guy W. Clinical Global Impressions. ECDEU Assessment
Manual for Psychopharmacology. revised. Rockville, MD:
National Institute of Mental Health, 1976:218–22.
Higgins 2003
Higgins JPT, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. BMJ 2003;327:
557–60.
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.2 [updated
28Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

September 2011]. The Cochrane Collaboration, 2011.
Available from www.cochrane-handbook.org..
ICD 10
World Health Organization. ICD 10. http://apps.who.int/
classifications/apps/icd/icd10online/ (accessed 10 April
2010).
Jadad 1996
Jadad A, Moore A, Carroll D, Jenkinson C, Reynolds
DJM, Gavaghan DJ, McQuay HJ. Assessing the quality of
reports of randomized clinical trials: is blinding necessary?.
Controlled Clinical Trials 1996;17:1–12.
Jüni P 2001
Jüni P, Altman DG, Egger M. Systematic reviews in health
care: Assessing the quality of controlled clinical trials. BMJ
2001;323(7303):42–6.
Kay 1986
Kay SR, Opler LA, Fiszbein A. Positive and Negative
Syndrome Scale (PANSS) Manual. North Tonawanda, NY:
Multi-Health Systems, 1986.
Komossa 2007
Komossa K, Rummel-Kluge C, Schmid F, Hunger
H, Schwarz S, El-Sayeh HGG, Kissling W, Leucht S.
Aripiprazole versus other atypical antipsychotics for
schizophrenia. Cochrane Database of Systematic Reviews
2007, Issue 3. [DOI: 10.1002/14651858.CD006569.pub2]
Leucht 2005
Leucht S, Kane JM, Kissling W, Hamann J, Etschel E,
Engel RR. What does the PANSS mean?. Schizophrenia
Research 2005;79(2-3):231–8. [PUBMED: 15982856]
Leucht 2005a
Leucht S, Kane JM, Kissling W, Hamann J, Etschel E,
Engel R. Clinical implications of Brief Psychiatric Rating
Scale Scores. British Journal of Psychiatry 2005;187:366–71.
Marshall 2000
Marshall M, Lockwood A, Adams C, Bradley C, Joy C,
Fenton M. Unpublished rating scales - a major source
of bias in randomised controlled trials of treatments for
schizophrenia?. British Journal of Psychiatry 2000;176:
249–52.
NICE 2009
National Institute of Clinical Excellence. Core interventions
in the treatment and management of schizophrenia
in primary and secondary care (update). http://
www.nice.org.uk/guidance/CG82 2009.
Overall 1962
Overall JE, Gorham DR. The Brief Psychiatric Rating Scale.
Psychological Reports 1962;10:799–812.
Rivas-Vasquez 2003
Rivas-Vasquez RA. Aripiprazole: a novel antipsychotic with
dopamine stabilising properties. Professional Psychology:
Research and Practice 2003;34(1):108–11.
Rowland 1998
Roland M, Torgerson DJ. What are pragmatic trials?. BMJ
1998;316:285.
Schünemann 2008
Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks
JJ, Glasziou P, et al.Chapter 12: Interpreting results and
drawing conclusions. In: Higgins JPT, Green S editor(s).
Cochrane Handbook for Systematic Reviews of Interventions.
The Cochrane Collaboration, 2008:359–83.
Xia 2007
Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P,
El-Sayeh H, Pinfold V, Takriti Y. The Leeds Outcomes
Stakeholders Survey (LOSS) Study. Proceedings of the 15th
Cochrane Colloquium; 2007 Oct 23-27; Sao Paulo. 2007.∗ Indicates the major publication for the study
29Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Adson 2003
Methods Allocation: randomised.
Blindness: double (in treatment responders).
Duration: 6 weeks, preceded by > 2 day wash-out period.
Design: parallel, multicentre.
Setting: hospital, North America.
Consent: not described.
Loss: described.
Participants Diagnosis: schizophrenia (DSM-IV).
N = 420.
Age: over 18, average ~ 41 years.
Sex: M 327, F 93.
History: acute relapse, response to previous neuroleptics other than clozapine, outpatient
> 3 months in past year, PANSS total > 60, and > 4 on 2 defined PANSS criteria.
Exclusions: pregnancy, lactation, schizoaffective disorder, organic, bipolar disorders, hos-
pitalisation for 14 days prior to screening, substance dependence within 3 months, sui-
cide risk, unstable thyroid pathology, history of neuroleptic malignant syndrome, history
of unstable medical condition
Interventions 1. Aripiprazole: dose 10 mg/day. N = 106.
2. Aripiprazole: dose 15 mg/day. N = 106.
3. Aripiprazole: dose 20 mg/day. N = 100.
4. Placebo. N = 108.
Outcomes Leaving the study early.
Unable to use -
Death: suicide and natural causes (incomplete data).
Mental state: PANSS total , PANSS-derived BPRS core score, PANSS negative score (no
SDs)
Notes Greater than 60% discontinuation rate.
Patients not responding by week 3 were offered open-label aripiprazole for weeks 4-6.
Original protocol amended to provide two secondary outcome criteria.
Data reported in both OC and LOCF analyses.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
30Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Adson 2003 (Continued)
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double blind, no further details
Incomplete outcome data (attrition bias)
All outcomes
High risk Very high drop-out rate with limited de-
tails.
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Unclear
Carson 2000 a
Methods Allocation: randomised, method not described.
Blindness: double, no further details.
Duration: 4 weeks, preceded by > 5 day washout period.
Design: parallel, multicentre.
Setting: hospital, USA.
Consent: obtained.
Loss: described.
Participants Diagnosis: schizophrenia or schizoaffective disorder (DSM-IV).
N = 414.
Age: mean ~ 39 years.
Sex: M 288, F 126.
History: acute relapse, mean age at first episode ~ 22 years, mean number of previous
hospitalisations ~ 10.
Exclusions: other psychiatric disorders, history of violence or suicidal ideation/self-harm,
significant neurological abnormality, psychoactive drug or alcohol abuse/dependence,
recent treatment with an investigational drug
Interventions 1. Aripiprazole: dose 15 mg/day. N = 102.
2. Aripiprazole: dose 30 mg/day. N = 102.
3. Haloperidol: dose 10 mg/day. N = 104.
4. Placebo. N = 106.
Outcomes Leaving the study early
Unable to use -
Death: suicide and natural causes (incomplete data).
Global state: CGI (no SDs).
Mental state: BPRS, BPRS-PANSS derived (no SDs).
General functioning: CGI (no SDs).
Adverse effects: SAS, Barnes Akathisia scale, Abnormal Involuntary Movement scale,
other outcome measures including changes in body weight, serum prolactin, and QTc
interval changes (no usable/standard deviation data)
Notes Overall 40% discontinuation rate.
No information given on standard deviations.
Data reported in both OC and LOCF analyses.
31Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Carson 2000 a (Continued)
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double blind, method of blinding not de-
scribed
Incomplete outcome data (attrition bias)
All outcomes
High risk High attrition rate
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Unclear
Carson 2002 b
Methods Allocation: randomised, method not described.
Blindness: double, no further details.
Duration: 26 weeks, preceded by 3-14 day washout period.
Design: parallel, multicentre.
Setting: mixed in and out patients, multi-national.
Consent: not described.
Loss: High attrition rate.
Participants Diagnosis: schizophrenia.
N = 310.
Age: mean ~ 42 years.
Sex: M 174, F 136.
History: chronic stable, no significant worsening of symptoms in past 3 months, diagnosis
for > 2 years, baseline PANSS score mean ~ 82.
Exclusions: not described.
Interventions 1. Aripiprazole: dose 15 mg/day. N = 155.
2. Placebo: N = 155.
Outcomes Global state: relapse.
Adverse effects: adverse events above 10%, weight gain > 7%, fasting plasma glucose
>/= 110 mg/dl, Hb 1AC >/= upper limit of normal, clinically significant laboratory
measurements.
Leaving the study early.
Unable to use -
32Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Carson 2002 b (Continued)
Global state: CGI (no SDs).
Mental state: PANSS, PANSS-derived BPRS (no SDs).
Adverse effects: change in weight, change in serum prolactin, SAS, AIMS, Barnes
Akathisia rating scale, change in QTc interval, change in fasting plasma glucose, change
in Hb 1AC from baseline (no usable/SDs)
Notes Limited data given on standard deviations.
Different numbers of patients were analysed for efficacy and safety characteristics.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
High risk High attrition rate, reasons for discontinu-
ation given
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Unclear
Csernansky 2003
Methods Allocation: randomised, method not described.
Blindness: double.
Duration: 4 weeks, preceded by 3-7 day placebo washout period.
Design: parallel, multicentre.
Setting: inpatient, USA.
Consent: not described.
Loss: described.
Participants Diagnosis: schizophrenia (DSM-III-R).
N = 103.
Age: 18-65 years, average ~ 36.
Sex: M 91, F 12.
History: acute relapse, BPRS score > 30 & score of > 4 on 2 of 4 positive symptoms,
evidence of previous response to antipsychotic medication.
Exclusions: > moderate motor symptoms as measured by SAS, AIMS and Barnes
Akathisia scale, other primary diagnoses, substance dependence within 2 months, cardiac
33Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Csernansky 2003 (Continued)
patients, acute/unstable medical conditions
Interventions 1. Aripiprazole (OPC-14597): dose 5 mg/day 1+2, 10 mg/day 3+4, 15 mg/day 5+6, 20
mg/day 7-12, 30 mg/day 13-28. N = 34.
2. Haloperidol: dose 5 mg/day 1+2, 10 mg/day 3+4, 15 mg/day 5+6, 20 mg/day 7-12,
20 mg/day 13-28. N = 34.
3. Placebo. N = 35.
Outcomes Leaving the study early.
Unable to use -
Mental state: BPRS (no SDs).
Global state: CGI (no usable data).
Notes Overall 48.5% discontinuation rate.
Limited information on standard deviations.
Considered a ’negative’ study by the FDA.
Data reported in OC and LOCF analyses.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
High risk High attrition rate
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Unclear
34Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Daniel 2000
Methods Allocation: randomised, method not described.
Blindness: double.
Duration: 4 weeks, preceded by 3-7 day washout period.
Design: parallel, multicentre.
Setting: inpatient.
Consent: not described.
Loss: described.
Participants Diagnosis: schizophrenia (DSM-IV).
N = 307.
Age: 18-65 years, average ~ 38.
Sex: M 247, F 60.
History: acute relapse, BPRS score > 36 & score of > 2 on 4 criteria, antipsychotic
medication taken for > 72 hours prior to randomisation.
Exclusions: first episode of schizophrenia, refractory to antipsychotics, moderate to severe
EPS, dyskinesia or akathisia, substance abuse, cardiac disease, acute or unstable medical
condition, pregnancy, lactation, women not using adequate contraception
Interventions 1. Aripiprazole: dose 2 mg/day. N = 59.
2. Aripiprazole: dose 10 mg/day. N = 60.
3. Aripiprazole: dose 30 mg/day. N = 61.
4. Haloperidol: dose 10 mg/day after 5 mg/day 1+2). N = 63.
5. Placebo. N = 64.
Outcomes Leaving the study early.
Unable to use -
Global state: CGI (no SDs).
Mental state: BPRS, PANSS (no SDs).
Adverse effects: reported adverse effects, extra-pyramidal side effects, mean weight gain,
mean prolactin levels (no usable data)
Notes Over 40% overall discontinuation rate.
No data given on standard deviations.
Marked sex differential in participants.
Data reported in both LOCF and OC analyses.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Unclear
35Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Daniel 2000 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Unclear
Selective reporting (reporting bias) Unclear risk Unclear
Other bias Unclear risk Unclear
Daniel 2004
Methods Allocation: randomised, method not described.
Blindness: double.
Duration: 24hrs.
Design: parallel, multicentre.
Setting: inpatient.
Consent: not described.
Loss: described.
Participants Diagnosis: schizophrenia, schizoaffective disorder, schizophreniform disorder.
N = 357*.
Age: not described.
Sex: not described.
History: acute agitation.
Exclusions: not described.
Interventions 1. Aripiprazole IM: dose 1 mg/day. N = 57.
2. Aripiprazole IM: dose 5 mg/day. N = 62.
3. Aripiprazole IM: dose 10 mg/day. N = 56.
4. Aripiprazole IM: dose 15 mg/day. N = 58.
5. Haloperidol IM: dose 7.5 mg/day. N = 60.
6. Placebo IM. N = 62.
Outcomes Global state: poor compliance with study protocol due to lack of efficacy, deterioration,
or psychosis.
Leaving the study early.
Adverse effects: reported in > 5% participants, extrapyramidal symptoms
Unable to use -
Behaviour: PEC score - mean change (no SD), CAB score- mean change (no SD), ACES
- (no SD), response - > 40% reduction in PEC score (unvalidated sub-scale), requiring
additional dose of antipsychotic medication, benzodiazepines (incomplete data)
Notes *Two participants not accounted for.
Limited data reported on standard deviations.
Data reported in LOCF analyses.
Jadad = 2.
Only adverse effects occurring in over 5% participants recorded.
Not all outcomes reported at 24 hrs.
Risk of bias
36Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Daniel 2004 (Continued)
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
Low risk 95% completed study, details of loss of fol-
low-up given
Selective reporting (reporting bias) Low risk appears to be
Other bias Unclear risk Unclear
Marcus 2005
Methods Allocation: randomised, method not described.
Blindness: double.
Duration: 6 weeks.
Design: parallel, multicentre.
Setting: hospital, USA.
Consent: not described.
Loss: not described.
Participants Diagnosis: schizophrenia.
N = 367.
Age: unknown.
Sex: unknown.
History: acute relapse.
Exclusions: not described.
Interventions 1. Aripiprazole: dose 2 mg/day. N = 93.
2. Aripiprazole: dose 5 mg/day. N = 92.
3. Aripiprazole: dose 10 mg/day. N = 94.
4. Placebo. N = 88.
Outcomes Leaving the study early.
Unable to use -
Global state: CGI (no SD).
Mental state: PANSS (no SD), time to response (defined by CGI and PANSS) (no usable
data).
Adverse effects: self-reported > 5% participants (no usable data)
37Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Marcus 2005 (Continued)
Notes Greater than 40% discontinuation rate.
Limited data on standard deviations given.
Data reported in LOCF analyses.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
High risk High attrition rate
Selective reporting (reporting bias) Low risk Appears to be
Other bias Unclear risk Unclear
Oren 2005
Methods Allocation: randomised, block randomisation.
Blindness: double.
Duration: 24 hours.
Design: parallel, multicentre.
Setting: hospital.
Consent: not described.
Loss: described.
Participants Diagnosis: schizophrenia or schizoaffective disorder (DSM-IV).
N = 448.
Age: >/= 18 years.
Sex: unknown.
History: acute agitation, voluntarily hospitalised, able to comply and comprehend pro-
tocol, PEC score of >/= 15 and </= 32, and at least 2 components >/= 4 (moderate).
Exclusions: not described.
Interventions 1. Aripiprazole IM: dose 10 mg/day. N = 175.
2. Placebo IM. N = 88.
3. Haloperidol IM: dose 6.5 mg/day. N = 185.
Allowed concomitant medication of up to 4 mg lorazepam or equivalent
38Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Oren 2005 (Continued)
Outcomes Global state: poor compliance with study protocol due to lack of efficacy, deterioration,
or psychosis, requiring additional dose of antipsychotic medication, benzodiazepines.
Leaving the study early.
Adverse effects: reported in > 5% participants, extrapyramidal symptoms
Unable to use -
Global state: CGI (no SD)
Behaviour: PEC score - mean change (no SD), CAB score - mean change (no SD), ACES
- (no data), response - > 40% reduction in PEC score (unvalidated sub-scale)
Notes Limited information given on standard deviations.
Data was analysed in LOCF.
Jadad = 2.
Adverse effects reported occurring in >/= 5% participants.
Not all outcomes recorded over 24 hrs.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Via a central call-in system
Allocation concealment (selection bias) Low risk Randomised, permuted block randomisa-
tion
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
Low risk 96.6% competed study
Selective reporting (reporting bias) Unclear risk Secondary efficacy measures were not re-
ported in details
Other bias Unclear risk Unclear
Potkin 2003
Methods Allocation: randomised, method not described.
Blindness: double.
Duration: 4 weeks, preceded by 5-day placebo washout period.
Design: parallel, multicentre.
Setting: hospital, USA.
Consent: described.
Loss: described.
39Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Potkin 2003 (Continued)
Participants Diagnosis: schizophrenia or schizoaffective disorder (DSM-IV).
N = 404.
Age: 18-65 years, average ~ 39.
Sex: M 283, F 121.
History: acute relapse, responsive to antipsychotic medication other than clozapine,
outpatient for > 3 months in past year, PANSS > 60 & score > 2 on psychotic symptom
sub-scale, adequate time interval since receiving previous anti-psychotic.
Exclusions: other psychiatric disorders requiring medication, history of violence, suici-
dal attempts or ideation, significant neurological abnormality, alcohol/psychoactive sub-
stance misuse within 1 month of study start, treatment with investigational drug within
4 weeks of washout phase, unstable/acute medical conditions, pregnancy, lactation
Interventions 1. Aripiprazole: dose 20 mg/day. N = 101.
2. Aripiprazole: dose 30 mg/day. N = 101.
3. Risperidone: dose 2 mg day 1, 4 mg day 2, 6 mg/day thereafter. N = 99.
4. Placebo. N = 103.
Outcomes Leaving the study early
Adverse effects: self-reported > 5% participants, mean change in body weight, mean
change in serum prolactin, mean change in QTc interval
Unable to use -
Global state: CGI - much, or very much improved (no SD).
Mental state: PANSS - 30% decrease in baseline score, PANSS-derived BPRS (no SD).
Adverse effects: SAS, Barnes Akathisia Rating scale, AIMS, vital signs (no usable data/
SD)
Notes Overall 40% discontinuation rate.
No information given on standard deviations.
Data was analysed in terms of OC and LOCF.
Jadad = 2.
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Unclear
Allocation concealment (selection bias) High risk Randomised, method not described
Blinding (performance bias and detection
bias)
All outcomes
Unclear risk Double, no further details
Incomplete outcome data (attrition bias)
All outcomes
High risk High attrition rate
Selective reporting (reporting bias) Unclear risk Unclear
40Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Potkin 2003 (Continued)
Other bias Unclear risk Unclear
BAS: Barnes Akathesia Rating Scale
SAS: Simpson Angus Scale
CGI-I: CGI Improvement Scale
CGI-S: CGI Severity Scale
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Allain 2005 Allocation: not randomised, an open label study
Auby 2002 Allocation: randomised.
Participants: people with stable schizophrenia or schizoaffective disorder.
Intervention: aripiprazole at multiple doses - no other comparator drug.
Outcomes: no usable data.
Beuzen 2005 Allocation: not randomised, an open label study.
Intervention: aripiprazole versus other antipsychotics, no placebo group
Blonde 2004 Allocation: states it is randomised.
Participants: states people with schizophrenia etc.
Intervention: aripripazole versus olanzapine, no placebo group
Carson 2002 a Allocation: not randomised, a review.
Carson W, McQuade 2003 Allocation: randomised.
Blindness: double.
Participants: people with schizophrenia.
Intervention: aripiprazole: dose 15-30 mg/day. N = 156. Olanzapine: dose 10-20 mg/day. N = 161.
No placebo group
Casey 2003 Allocation: randomised.
Participants: people with schizophrenia or schizoaffective disorder.
Intervention: aripiprazole at different regimens - no other comparator or placebo
Chan 2007 Intervention: aripripazole versus risperidol, no placebo control group
Chen 2005 b Intervention: aripripazole versus risperidone, no placebo control group
Chrzanowski 2006 Allocation: not randomised, an open label study.
Intervention: aripiprazole versus olanzapine, no placebo control group
41Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Corey-Lisle 2006 Allocation: not randomised, a naturalistic trial.
Daniel 2006 Intervention: IM aripripazole versus IM haloperidol, no placebo control group
Fan 2005 a Intervention: aripripazole versus clozapine, no placebo control group
Gismondi R, Mel2 Intervention: aripripazole versus perphenazine, no placebo control group
Han 2005 a Intervention: aripripazole versus clozapine, no placebo control group
Hwang 2005 Intervention: aripripazole versus risperidone, no placebo control group
Jody 2004 Allocation: not randomised, an open label study.
Kane 2003 Allocation: randomised, method not described
Blindness: double (during treatment phase).
Duration: 6 weeks, preceded by 14-day patient screening, 2-day neuroleptic washout, 4-6 weeks’
confirmation of treatment resistance, 2-10 day neuroleptic washout.
Design: multicentre, parallel.
Intervention: aripiprazole versus perphenazine, no placebo control group
Kane 2006 d Intervention: aripripazole versus haloperidol, no placebo control group
Kane 2007 a Intervention: aripripazole versus perphenazine, no placebo control group
Kern 2001 Allocation: randomised, method not described.
Blindness: open label.
Duration: 26 weeks.
Design: multicentre, parallel.
Setting: outpatient.
Participants: N = 256*. Age: 18-65 years, average ~ 40 years. Sex: M 164, F 92.
Diagnosis: schizophrenia or schizoaffective disorder.
History: chronic stable, not hospitalised for > 2 months prior to randomisation, previously on stable
dose of antipsychotic for > 2 months
Intervention: aripiprazole versus olanzapine, no placebo control group
Kim 2006 d Intervention: aripiprazole versus haloperidol, no placebo control group
Kujawa 2002 Intervention: aripiprazole versus haloperidol, no placebo control group
Kujawa 2003 Intervention: a review article.
Kujawa 2004 Allocation: randomised, method not described.
Blindness: double.
Duration: 26 weeks.
Design: parallel, multi-centre.
Participants: N = 317. Age: average ~ 38 years. Sex: M 229, F 88.
42Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Diagnosis: schizophrenia.
Intervention: aripripazole versus olanzapine, no placebo control group
Liang 2005 Intervention: aripiprazole versus haloperidol, no placebo control group
Mai 2005 Intervention: aripripazole versus risperidone, no placebo control group
Mallikaarjun 2000 Allocation: randomised.
Participants: healthy volunteers.
Marcus 2003 Allocation: not randomised, review.
Marder 2004 Intervention: aripripazole versus haloperidol, no placebo control group
McQuade 2002 Intervention: aripiprazole versus haloperidol, no placebo control group
McQuade 2003 Intervention aripiprazole versus olanzapine, no placebo control group
Modell 2005 b Intervention: aripripazole versus perphenazine, no placebo control group
N0025078569 Intervention: aripiprazole versus olanzapine, no placebo control group
Newcomer 2006 Intervention: aripripazole versus olanzapine, no placebo group
Octavio 2004 Intervention: aripiprazole versus haloperidol, no placebo control group
Octavio 2005 Intervention: aripiprazole versus haloperidol, no placebo control
Petrie 1997 Allocation: not randomised, review.
Ray 2005 Intervention: aripiprazole versus olanzapine, no placebo control group
Riera 2004 Intervention: aripiprazole versus standard care, no placebo control group
Saha 2004 Allocation: randomised.
Participants: first episode of schizophrenia or schizoaffective disorder occurring within 1 year of study.
Intervention: aripiprazole at multiple doses - no other comparator drug or placebo
Sanchez 2006 Allocation: not randomised, an open-label study.
Intervention: aripiprazole versus olanzapine, no placebo control group
STAR 2006 Allocation: not randomised, naturalistic trial.
Stock 2005 Intervention: aripiprazole versus olanzapine, no placebo control group
Stroup 2003 Allocation: not randomised.
43Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Tandon 2006 Intervention: aripiprazole versus other antipsychotics, no placebo control group
Wang 2005 Intervention: aripiprazole versus chlorpromazine, no placebo control group
Wang 2005 j Intervention: aripiprazole versus clozapine, no placebo control group
Wu 2005 d Intervention: aripripazole versus haloperidol, no placebo control group
Xia 2005 Intervention: aripiprazole versus chlorpromazine, no placebo control group
Ye 2005 Intervention: aripripazole versus risperidone, no placebo control group
Zhang 2005 Intervention: aripiprazole versus sulpiride, no placebo control group
Zhang 2005 a Intervention: aripripazole versus risperidone, no placebo control group
Zhao 2005 Intervention: aripripazole versus sulpiride, no placebo control group
Zhi 2005 Intervention: aripripazole versus risperidone, no placebo control group
Zhu 2005 Intervention: aripripazole versus risperidone, no placebo control group
Zhu 2005 a Intervention: aripripazole versus clozapine, no placebo control group
Zhu 2005 b Intervention: aripripazole versus risperidone, no placebo control group
Characteristics of studies awaiting assessment [ordered by study ID]
Carson 2008
Methods 4 weeks randomised double blind controlled trial
Participants Paediatric age 10-17 years, with DSM-IV diagnosis of bipolar 1 disorder, manic or mixed episode with/with out
psychotic symptoms (n = 296)
Interventions Placebo versus aripiprazole 10 or 30 mg
Outcomes >= 50% change on Young mania rating scale
Notes
44Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nyilas 2007
Methods 6 weeks multicentre, randomised double blind controlled trial
Participants Age 13-17 years, DSM-IV diagnosis of schizophrenia (n = 302)
Interventions Placebo versus aripiprazole 10 or 30 mg
Outcomes Mean change on PANSS
Notes
45Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. ARIPIPRAZOLE versus PLACEBO
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Global state: 1. Relapse 2 883 Risk Ratio (M-H, Fixed, 95% CI) 0.65 [0.57, 0.74]
1.1 short term 1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.59 [0.45, 0.77]
1.2 medium term 1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.66 [0.53, 0.81]
1.3 Acute (2 hr after IM) 1 263 Risk Ratio (M-H, Fixed, 95% CI) 0.71 [0.57, 0.89]
2 Global state: 2. Poor compliance
with study protocol due to lack
of efficacy, deterioration or
psychosis
8 2275 Risk Ratio (M-H, Fixed, 95% CI) 0.74 [0.59, 0.93]
3 Global state: 3. Needing
additional antipsychotic
medication
4 1062 Risk Ratio (M-H, Fixed, 95% CI) 0.73 [0.57, 0.93]
4 Global state: 4. Needing
additional benzodiazepines
2 683 Risk Ratio (M-H, Fixed, 95% CI) 0.53 [0.30, 0.92]
5 Adverse effects: 1. Clinically
important specific adverse
effects
9 23455 Risk Ratio (M-H, Fixed, 95% CI) 1.17 [1.07, 1.28]
5.1 anxiety 3 1035 Risk Ratio (M-H, Fixed, 95% CI) 0.83 [0.62, 1.12]
5.2 extrapyramidal symptoms
- akathisia
5 1595 Risk Ratio (M-H, Fixed, 95% CI) 1.78 [1.16, 2.74]
5.3 extrapyramidal symptoms
- general
4 1298 Risk Ratio (M-H, Fixed, 95% CI) 0.83 [0.47, 1.45]
5.4 extrapyramidal symptoms
- needing antiparkinson
medication at least once
4 1043 Risk Ratio (M-H, Fixed, 95% CI) 0.83 [0.61, 1.14]
5.5 headache 6 1962 Risk Ratio (M-H, Fixed, 95% CI) 1.17 [0.94, 1.47]
5.6 insomnia 4 1298 Risk Ratio (M-H, Fixed, 95% CI) 1.09 [0.89, 1.33]
5.7 nausea 6 1962 Risk Ratio (M-H, Fixed, 95% CI) 1.55 [1.07, 2.24]
5.8 vomiting 5 1699 Risk Ratio (M-H, Fixed, 95% CI) 1.46 [0.96, 2.23]
5.9 weight gain - > 7% over
baseline
3 1035 Risk Ratio (M-H, Fixed, 95% CI) 2.55 [1.35, 4.82]
5.10 constipation 2 787 Risk Ratio (M-H, Fixed, 95% CI) 1.42 [0.75, 2.69]
5.11 diarrhoea 2 787 Risk Ratio (M-H, Fixed, 95% CI) 0.79 [0.40, 1.56]
5.12 dyspepsia 2 787 Risk Ratio (M-H, Fixed, 95% CI) 0.89 [0.56, 1.41]
5.13 toothache 1 367 Risk Ratio (M-H, Fixed, 95% CI) 1.47 [0.43, 5.00]
5.14 upper abdominal pain 1 367 Risk Ratio (M-H, Fixed, 95% CI) 4.13 [0.24, 72.63]
5.15 infections 1 367 Risk Ratio (M-H, Fixed, 95% CI) 0.57 [0.20, 1.65]
5.16 dizziness 4 1347 Risk Ratio (M-H, Fixed, 95% CI) 1.34 [0.83, 2.14]
5.17 sedation 4 1347 Risk Ratio (M-H, Fixed, 95% CI) 1.82 [1.06, 3.15]
5.18 skin rash 1 367 Risk Ratio (M-H, Fixed, 95% CI) 3.47 [0.45, 26.50]
5.19 cough 1 367 Risk Ratio (M-H, Fixed, 95% CI) 1.89 [0.43, 8.29]
5.20 pharyngolaryngeal pain 1 367 Risk Ratio (M-H, Fixed, 95% CI) 8.58 [0.52, 142.92]
5.21 tachycardia 3 1084 Risk Ratio (M-H, Fixed, 95% CI) 1.94 [0.89, 4.25]
5.22 agitation 3 980 Risk Ratio (M-H, Fixed, 95% CI) 0.61 [0.40, 0.92]
46Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

5.23 asthenia 1 420 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.41, 2.17]
5.24 QTc interval >= 450 or
10% above baseline
2 787 Risk Ratio (M-H, Fixed, 95% CI) 2.44 [0.13, 46.82]
6 Adverse effects: 2. Average
change in QTc interval (ms)
from baseline
1 408 Mean Difference (IV, Fixed, 95% CI) 0.99 [-3.38, 5.37]
6.1 Aripiprazole 20 mg/day 1 204 Mean Difference (IV, Fixed, 95% CI) 3.00 [-3.19, 9.19]
6.2 Aripiprazole 30 mg/day 1 204 Mean Difference (IV, Fixed, 95% CI) -1.0 [-7.18, 5.18]
7 Adverse effects: 3. Physiological
(serum) measures
3 3515 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.86, 1.04]
7.1 cholesterol - total fasting
>/= 200 mg/dl
1 310 Risk Ratio (M-H, Fixed, 95% CI) 1.04 [0.83, 1.30]
7.2 cholesterol - total fasting
>/= 200 mg/dl - long-term
effect
1 310 Risk Ratio (M-H, Fixed, 95% CI) 1.21 [0.98, 1.50]
7.3 cholesterol - total fasting
>/= 240mg/dl long-term effect
1 310 Risk Ratio (M-H, Fixed, 95% CI) 1.22 [0.77, 1.93]
7.4 glucose - plasma levels >/=
110mg/dl
1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.96 [0.70, 1.33]
7.5 haemoglobin 1AC -
incidence >/= upper limit of
normal
1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.74 [0.41, 1.33]
7.6 low density lipoprotein
cholesterol (LDL) - >/= 130
mg/dl
1 310 Risk Ratio (M-H, Fixed, 95% CI) 1.01 [0.80, 1.28]
7.7 low density lipoprotein
cholesterol (LDL) >/= 160
mg/dl - long-term effect
1 310 Risk Ratio (M-H, Fixed, 95% CI) 1.0 [0.62, 1.61]
7.8 triglycerides >/= 200
mg/dl long-term effect
1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.67, 1.31]
7.9 high density lipoprotein <
40 mg/dl long-term effect
1 310 Risk Ratio (M-H, Fixed, 95% CI) 0.86 [0.66, 1.12]
7.10 prolactin - increase to
>/= 23 ng/ml or level above
upper limit of normal
2 725 Risk Ratio (M-H, Fixed, 95% CI) 0.21 [0.11, 0.37]
8 Leaving the study early 9 5170 Risk Ratio (M-H, Random, 95% CI) 0.73 [0.61, 0.87]
8.1 due to any reason 9 2585 Risk Ratio (M-H, Random, 95% CI) 0.73 [0.60, 0.87]
8.2 due to adverse effects 9 2585 Risk Ratio (M-H, Random, 95% CI) 0.75 [0.42, 1.35]
9 concomitant medication -
anxiolytics
2 787 Odds Ratio (M-H, Fixed, 95% CI) 0.96 [0.61, 1.52]
47Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
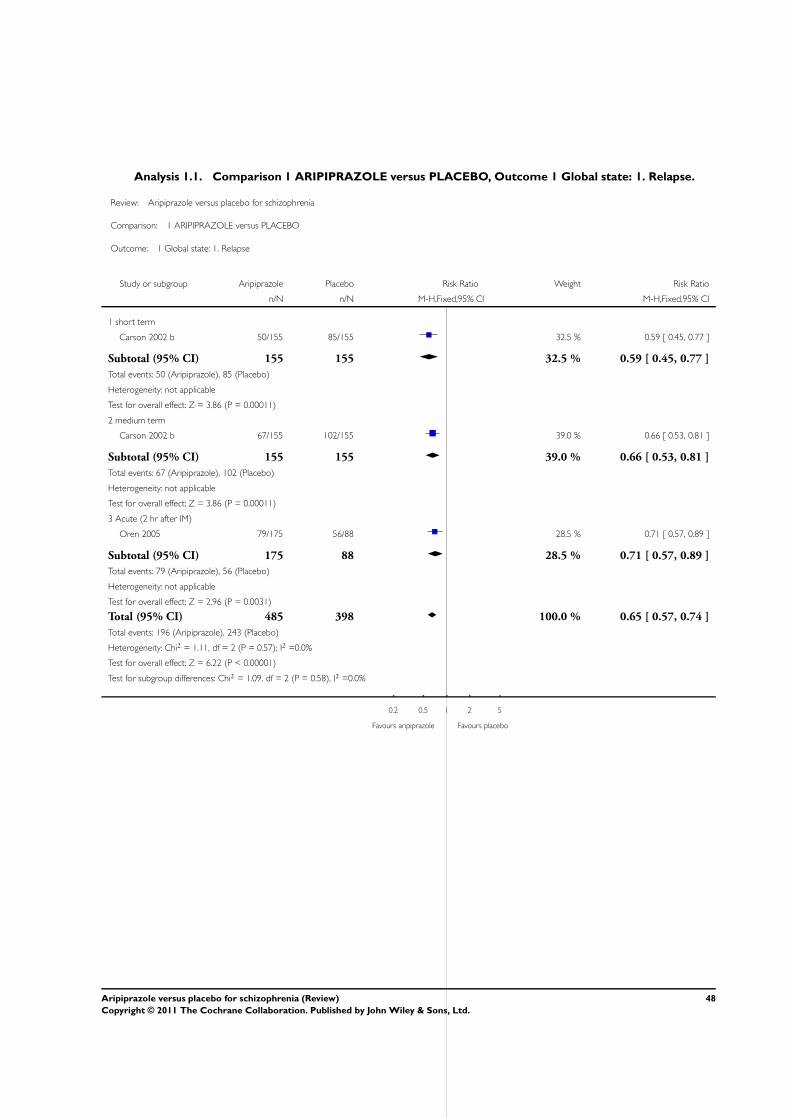
Analysis 1.1. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 1 Global state: 1. Relapse.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 1 Global state: 1. Relapse
Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 short term
Carson 2002 b 50/155 85/155 32.5 % 0.59 [ 0.45, 0.77 ]
Subtotal (95% CI) 155 155 32.5 % 0.59 [ 0.45, 0.77 ]
Total events: 50 (Aripiprazole), 85 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 3.86 (P = 0.00011)
2 medium term
Carson 2002 b 67/155 102/155 39.0 % 0.66 [ 0.53, 0.81 ]
Subtotal (95% CI) 155 155 39.0 % 0.66 [ 0.53, 0.81 ]
Total events: 67 (Aripiprazole), 102 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 3.86 (P = 0.00011)
3 Acute (2 hr after IM)
Oren 2005 79/175 56/88 28.5 % 0.71 [ 0.57, 0.89 ]
Subtotal (95% CI) 175 88 28.5 % 0.71 [ 0.57, 0.89 ]
Total events: 79 (Aripiprazole), 56 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 2.96 (P = 0.0031)
Total (95% CI) 485 398 100.0 % 0.65 [ 0.57, 0.74 ]
Total events: 196 (Aripiprazole), 243 (Placebo)
Heterogeneity: Chi2 = 1.11, df = 2 (P = 0.57); I2 =0.0%
Test for overall effect: Z = 6.22 (P < 0.00001)
Test for subgroup differences: Chi2 = 1.09, df = 2 (P = 0.58), I2 =0.0%
0.2 0.5 1 2 5
Favours aripiprazole Favours placebo
48Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 2 Global state: 2. Poor
compliance with study protocol due to lack of efficacy, deterioration or psychosis.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 2 Global state: 2. Poor compliance with study protocol due to lack of efficacy, deterioration or psychosis
Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Adson 2003 24/312 11/108 12.2 % 0.76 [ 0.38, 1.49 ]
Carson 2000 a 30/204 16/106 15.7 % 0.97 [ 0.56, 1.70 ]
Csernansky 2003 8/34 15/35 11.0 % 0.55 [ 0.27, 1.12 ]
Daniel 2000 24/180 20/64 22.0 % 0.43 [ 0.25, 0.72 ]
Daniel 2004 1/235 1/62 1.2 % 0.26 [ 0.02, 4.16 ]
Marcus 2005 49/279 12/88 13.6 % 1.29 [ 0.72, 2.31 ]
Oren 2005 0/175 1/88 1.5 % 0.17 [ 0.01, 4.10 ]
Potkin 2003 32/202 23/103 22.7 % 0.71 [ 0.44, 1.15 ]
Total (95% CI) 1621 654 100.0 % 0.74 [ 0.59, 0.93 ]
Total events: 168 (Aripiprazole), 99 (Placebo)
Heterogeneity: Chi2 = 10.76, df = 7 (P = 0.15); I2 =35%
Test for overall effect: Z = 2.55 (P = 0.011)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours aripiprazole Favours placebo
49Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.3. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 3 Global state: 3. Needing
additional antipsychotic medication.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 3 Global state: 3. Needing additional antipsychotic medication
Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Adson 2003 12/312 6/108 10.1 % 0.69 [ 0.27, 1.80 ]
Carson 2000 a 9/204 9/106 13.4 % 0.52 [ 0.21, 1.27 ]
Csernansky 2003 4/35 1/34 1.1 % 3.89 [ 0.46, 33.02 ]
Oren 2005 72/175 50/88 75.3 % 0.72 [ 0.56, 0.93 ]
Total (95% CI) 726 336 100.0 % 0.73 [ 0.57, 0.93 ]
Total events: 97 (Aripiprazole), 66 (Placebo)
Heterogeneity: Chi2 = 2.92, df = 3 (P = 0.40); I2 =0.0%
Test for overall effect: Z = 2.55 (P = 0.011)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours aripiprazole Favours placebo
Analysis 1.4. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 4 Global state: 4. Needing
additional benzodiazepines.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 4 Global state: 4. Needing additional benzodiazepines
Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Adson 2003 11/312 4/108 20.8 % 0.95 [ 0.31, 2.93 ]
Oren 2005 14/175 17/88 79.2 % 0.41 [ 0.21, 0.80 ]
Total (95% CI) 487 196 100.0 % 0.53 [ 0.30, 0.92 ]
Total events: 25 (Aripiprazole), 21 (Placebo)
Heterogeneity: Chi2 = 1.58, df = 1 (P = 0.21); I2 =37%
Test for overall effect: Z = 2.25 (P = 0.025)
Test for subgroup differences: Not applicable
0.2 0.5 1 2 5
Favours aripiprazole Favours placebo
50Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 5 Adverse effects: 1. Clinically
important specific adverse effects.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 5 Adverse effects: 1. Clinically important specific adverse effects
Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 anxiety
Carson 2002 b 23/155 34/155 0.68 [ 0.42, 1.09 ]
Potkin 2003 41/202 19/103 1.10 [ 0.67, 1.80 ]
Adson 2003 31/312 14/108 0.77 [ 0.42, 1.39 ]
Subtotal (95% CI) 669 366 0.83 [ 0.62, 1.12 ]
Total events: 95 (Aripiprazole), 67 (Placebo)
Heterogeneity: Chi2 = 2.04, df = 2 (P = 0.36); I2 =2%
Test for overall effect: Z = 1.21 (P = 0.23)
2 extrapyramidal symptoms - akathisia
Carson 2002 b 14/155 12/155 1.17 [ 0.56, 2.44 ]
Daniel 2004 9/235 1/62 2.37 [ 0.31, 18.39 ]
Oren 2005 1/175 1/88 0.50 [ 0.03, 7.94 ]
Potkin 2003 40/202 9/103 2.27 [ 1.14, 4.49 ]
Adson 2003 25/312 4/108 2.16 [ 0.77, 6.08 ]
Subtotal (95% CI) 1079 516 1.78 [ 1.16, 2.74 ]
Total events: 89 (Aripiprazole), 27 (Placebo)
Heterogeneity: Chi2 = 2.76, df = 4 (P = 0.60); I2 =0.0%
Test for overall effect: Z = 2.62 (P = 0.0088)
3 extrapyramidal symptoms - general
Carson 2002 b 7/155 10/155 0.70 [ 0.27, 1.79 ]
Oren 2005 3/175 3/88 0.50 [ 0.10, 2.44 ]
Potkin 2003 7/202 0/103 7.68 [ 0.44, 133.24 ]
Adson 2003 13/312 7/108 0.64 [ 0.26, 1.57 ]
Subtotal (95% CI) 844 454 0.83 [ 0.47, 1.45 ]
Total events: 30 (Aripiprazole), 20 (Placebo)
Heterogeneity: Chi2 = 3.16, df = 3 (P = 0.37); I2 =5%
Test for overall effect: Z = 0.65 (P = 0.51)
4 extrapyramidal symptoms - needing antiparkinson medication at least once
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
51Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Carson 2000 a 23/204 13/106 0.92 [ 0.49, 1.74 ]
Csernansky 2003 6/34 10/35 0.62 [ 0.25, 1.51 ]
Daniel 2000 41/180 19/64 0.77 [ 0.48, 1.22 ]
Adson 2003 24/312 8/108 1.04 [ 0.48, 2.24 ]
Subtotal (95% CI) 730 313 0.83 [ 0.61, 1.14 ]
Total events: 94 (Aripiprazole), 50 (Placebo)
Heterogeneity: Chi2 = 0.96, df = 3 (P = 0.81); I2 =0.0%
Test for overall effect: Z = 1.14 (P = 0.26)
5 headache
Carson 2002 b 17/155 21/155 0.81 [ 0.44, 1.47 ]
Daniel 2004 32/235 2/62 4.22 [ 1.04, 17.13 ]
Oren 2005 13/175 7/88 0.93 [ 0.39, 2.26 ]
Potkin 2003 63/202 28/103 1.15 [ 0.79, 1.67 ]
Marcus 2005 48/279 18/88 0.84 [ 0.52, 1.37 ]
Adson 2003 78/312 17/108 1.59 [ 0.99, 2.56 ]
Subtotal (95% CI) 1358 604 1.17 [ 0.94, 1.47 ]
Total events: 251 (Aripiprazole), 93 (Placebo)
Heterogeneity: Chi2 = 8.31, df = 5 (P = 0.14); I2 =40%
Test for overall effect: Z = 1.42 (P = 0.15)
6 insomnia
Carson 2002 b 67/155 63/155 1.06 [ 0.82, 1.38 ]
Oren 2005 10/175 9/88 0.56 [ 0.24, 1.32 ]
Potkin 2003 53/202 23/103 1.17 [ 0.77, 1.80 ]
Adson 2003 54/312 14/108 1.34 [ 0.77, 2.30 ]
Subtotal (95% CI) 844 454 1.09 [ 0.89, 1.33 ]
Total events: 184 (Aripiprazole), 109 (Placebo)
Heterogeneity: Chi2 = 2.98, df = 3 (P = 0.39); I2 =0.0%
Test for overall effect: Z = 0.80 (P = 0.42)
7 nausea
Carson 2002 b 10/155 7/155 1.43 [ 0.56, 3.66 ]
Daniel 2004 17/235 3/62 1.50 [ 0.45, 4.94 ]
Oren 2005 10/175 2/88 2.51 [ 0.56, 11.23 ]
Potkin 2003 17/202 10/103 0.87 [ 0.41, 1.82 ]
Marcus 2005 21/279 3/88 2.21 [ 0.67, 7.23 ]
Adson 2003 54/312 10/108 1.87 [ 0.99, 3.54 ]
Subtotal (95% CI) 1358 604 1.55 [ 1.07, 2.24 ]
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
52Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Total events: 129 (Aripiprazole), 35 (Placebo)
Heterogeneity: Chi2 = 3.45, df = 5 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 2.34 (P = 0.019)
8 vomiting
Carson 2002 b 11/155 7/155 1.57 [ 0.63, 3.95 ]
Daniel 2004 9/235 2/62 1.19 [ 0.26, 5.35 ]
Potkin 2003 23/202 6/103 1.95 [ 0.82, 4.65 ]
Marcus 2005 13/279 7/88 0.59 [ 0.24, 1.42 ]
Adson 2003 32/312 5/108 2.22 [ 0.89, 5.54 ]
Subtotal (95% CI) 1183 516 1.46 [ 0.96, 2.23 ]
Total events: 88 (Aripiprazole), 27 (Placebo)
Heterogeneity: Chi2 = 5.41, df = 4 (P = 0.25); I2 =26%
Test for overall effect: Z = 1.77 (P = 0.076)
9 weight gain - > 7% over baseline
Carson 2002 b 9/155 6/155 1.50 [ 0.55, 4.11 ]
Potkin 2003 22/202 2/103 5.61 [ 1.35, 23.39 ]
Adson 2003 26/312 4/108 2.25 [ 0.80, 6.30 ]
Subtotal (95% CI) 669 366 2.55 [ 1.35, 4.82 ]
Total events: 57 (Aripiprazole), 12 (Placebo)
Heterogeneity: Chi2 = 2.29, df = 2 (P = 0.32); I2 =13%
Test for overall effect: Z = 2.89 (P = 0.0039)
10 constipation
Marcus 2005 22/279 4/88 1.73 [ 0.61, 4.90 ]
Adson 2003 25/312 7/108 1.24 [ 0.55, 2.78 ]
Subtotal (95% CI) 591 196 1.42 [ 0.75, 2.69 ]
Total events: 47 (Aripiprazole), 11 (Placebo)
Heterogeneity: Chi2 = 0.26, df = 1 (P = 0.61); I2 =0.0%
Test for overall effect: Z = 1.08 (P = 0.28)
11 diarrhoea
Marcus 2005 9/279 6/88 0.47 [ 0.17, 1.29 ]
Adson 2003 17/312 5/108 1.18 [ 0.44, 3.11 ]
Subtotal (95% CI) 591 196 0.79 [ 0.40, 1.56 ]
Total events: 26 (Aripiprazole), 11 (Placebo)
Heterogeneity: Chi2 = 1.64, df = 1 (P = 0.20); I2 =39%
Test for overall effect: Z = 0.68 (P = 0.50)
12 dyspepsia
Marcus 2005 17/279 8/88 0.67 [ 0.30, 1.50 ]
Adson 2003 41/312 14/108 1.01 [ 0.58, 1.79 ]
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
53Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Subtotal (95% CI) 591 196 0.89 [ 0.56, 1.41 ]
Total events: 58 (Aripiprazole), 22 (Placebo)
Heterogeneity: Chi2 = 0.68, df = 1 (P = 0.41); I2 =0.0%
Test for overall effect: Z = 0.51 (P = 0.61)
13 toothache
Marcus 2005 14/279 3/88 1.47 [ 0.43, 5.00 ]
Subtotal (95% CI) 279 88 1.47 [ 0.43, 5.00 ]
Total events: 14 (Aripiprazole), 3 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.62 (P = 0.54)
14 upper abdominal pain
Marcus 2005 6/279 0/88 4.13 [ 0.24, 72.63 ]
Subtotal (95% CI) 279 88 4.13 [ 0.24, 72.63 ]
Total events: 6 (Aripiprazole), 0 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.97 (P = 0.33)
15 infections
Marcus 2005 9/279 5/88 0.57 [ 0.20, 1.65 ]
Subtotal (95% CI) 279 88 0.57 [ 0.20, 1.65 ]
Total events: 9 (Aripiprazole), 5 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.04 (P = 0.30)
16 dizziness
Marcus 2005 13/279 6/88 0.68 [ 0.27, 1.74 ]
Daniel 2004 25/235 5/62 1.32 [ 0.53, 3.31 ]
Oren 2005 11/175 3/88 1.84 [ 0.53, 6.44 ]
Adson 2003 31/312 6/108 1.79 [ 0.77, 4.17 ]
Subtotal (95% CI) 1001 346 1.34 [ 0.83, 2.14 ]
Total events: 80 (Aripiprazole), 20 (Placebo)
Heterogeneity: Chi2 = 2.68, df = 3 (P = 0.44); I2 =0.0%
Test for overall effect: Z = 1.20 (P = 0.23)
17 sedation
Marcus 2005 13/279 0/88 8.58 [ 0.52, 142.92 ]
Daniel 2004 20/235 4/62 1.32 [ 0.47, 3.72 ]
Oren 2005 11/175 3/88 1.84 [ 0.53, 6.44 ]
Adson 2003 33/312 7/108 1.63 [ 0.74, 3.58 ]
Subtotal (95% CI) 1001 346 1.82 [ 1.06, 3.15 ]
Total events: 77 (Aripiprazole), 14 (Placebo)
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
54Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
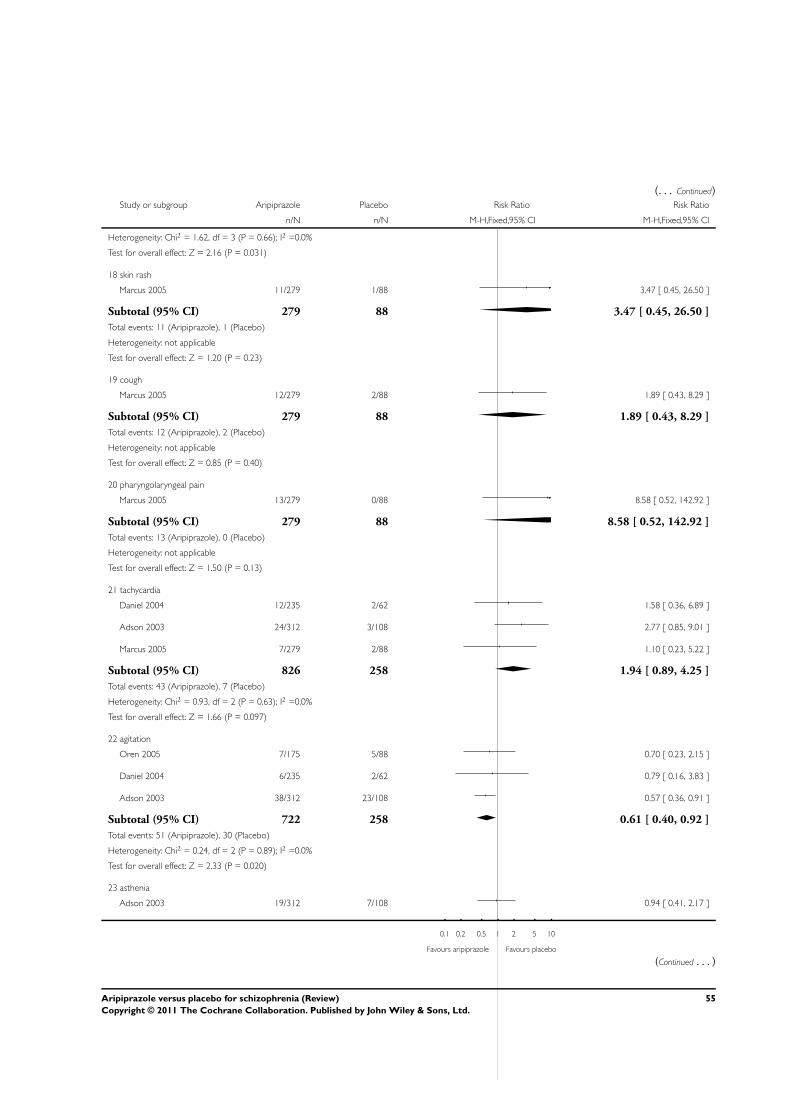
(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Heterogeneity: Chi2 = 1.62, df = 3 (P = 0.66); I2 =0.0%
Test for overall effect: Z = 2.16 (P = 0.031)
18 skin rash
Marcus 2005 11/279 1/88 3.47 [ 0.45, 26.50 ]
Subtotal (95% CI) 279 88 3.47 [ 0.45, 26.50 ]
Total events: 11 (Aripiprazole), 1 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.20 (P = 0.23)
19 cough
Marcus 2005 12/279 2/88 1.89 [ 0.43, 8.29 ]
Subtotal (95% CI) 279 88 1.89 [ 0.43, 8.29 ]
Total events: 12 (Aripiprazole), 2 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.85 (P = 0.40)
20 pharyngolaryngeal pain
Marcus 2005 13/279 0/88 8.58 [ 0.52, 142.92 ]
Subtotal (95% CI) 279 88 8.58 [ 0.52, 142.92 ]
Total events: 13 (Aripiprazole), 0 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.50 (P = 0.13)
21 tachycardia
Daniel 2004 12/235 2/62 1.58 [ 0.36, 6.89 ]
Adson 2003 24/312 3/108 2.77 [ 0.85, 9.01 ]
Marcus 2005 7/279 2/88 1.10 [ 0.23, 5.22 ]
Subtotal (95% CI) 826 258 1.94 [ 0.89, 4.25 ]
Total events: 43 (Aripiprazole), 7 (Placebo)
Heterogeneity: Chi2 = 0.93, df = 2 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 1.66 (P = 0.097)
22 agitation
Oren 2005 7/175 5/88 0.70 [ 0.23, 2.15 ]
Daniel 2004 6/235 2/62 0.79 [ 0.16, 3.83 ]
Adson 2003 38/312 23/108 0.57 [ 0.36, 0.91 ]
Subtotal (95% CI) 722 258 0.61 [ 0.40, 0.92 ]
Total events: 51 (Aripiprazole), 30 (Placebo)
Heterogeneity: Chi2 = 0.24, df = 2 (P = 0.89); I2 =0.0%
Test for overall effect: Z = 2.33 (P = 0.020)
23 asthenia
Adson 2003 19/312 7/108 0.94 [ 0.41, 2.17 ]
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
55Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Subtotal (95% CI) 312 108 0.94 [ 0.41, 2.17 ]
Total events: 19 (Aripiprazole), 7 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.15 (P = 0.88)
24 QTc interval >= 450 or 10% above baseline
Adson 2003 3/312 0/108 2.44 [ 0.13, 46.82 ]
Marcus 2005 0/279 0/88 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 591 196 2.44 [ 0.13, 46.82 ]
Total events: 3 (Aripiprazole), 0 (Placebo)
Heterogeneity: Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.59 (P = 0.55)
Total (95% CI) 16634 6821 1.17 [ 1.07, 1.28 ]
Total events: 1486 (Aripiprazole), 573 (Placebo)
Heterogeneity: Chi2 = 84.13, df = 67 (P = 0.08); I2 =20%
Test for overall effect: Z = 3.37 (P = 0.00075)
Test for subgroup differences: Chi2 = 46.94, df = 23 (P = 0.00), I2 =51%
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
56Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.6. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 6 Adverse effects: 2. Average
change in QTc interval (ms) from baseline.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 6 Adverse effects: 2. Average change in QTc interval (ms) from baseline
Study or subgroup Aripiprazole Placebo Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
1 Aripiprazole 20 mg/day
Potkin 2003 101 1 (24) 103 -2 (21) 49.9 % 3.00 [ -3.19, 9.19 ]
Subtotal (95% CI) 101 103 49.9 % 3.00 [ -3.19, 9.19 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
2 Aripiprazole 30 mg/day
Potkin 2003 101 -3 (22) 103 -2 (23) 50.1 % -1.00 [ -7.18, 5.18 ]
Subtotal (95% CI) 101 103 50.1 % -1.00 [ -7.18, 5.18 ]
Heterogeneity: not applicable
Test for overall effect: Z = 0.32 (P = 0.75)
Total (95% CI) 202 206 100.0 % 0.99 [ -3.38, 5.37 ]
Heterogeneity: Chi2 = 0.80, df = 1 (P = 0.37); I2 =0.0%
Test for overall effect: Z = 0.45 (P = 0.66)
Test for subgroup differences: Chi2 = 0.80, df = 1 (P = 0.37), I2 =0.0%
-10 -5 0 5 10
Favours aripiprazole Favours placebo
57Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.7. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 7 Adverse effects: 3. Physiological
(serum) measures.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 7 Adverse effects: 3. Physiological (serum) measures
Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
1 cholesterol - total fasting >/= 200 mg/dl
Carson 2002 b 78/155 75/155 14.6 % 1.04 [ 0.83, 1.30 ]
Subtotal (95% CI) 155 155 14.6 % 1.04 [ 0.83, 1.30 ]
Total events: 78 (Aripiprazole), 75 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.34 (P = 0.73)
2 cholesterol - total fasting >/= 200 mg/dl - long-term effect
Carson 2002 b 91/155 75/155 14.6 % 1.21 [ 0.98, 1.50 ]
Subtotal (95% CI) 155 155 14.6 % 1.21 [ 0.98, 1.50 ]
Total events: 91 (Aripiprazole), 75 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.81 (P = 0.070)
3 cholesterol - total fasting >/= 240mg/dl long-term effect
Carson 2002 b 33/155 27/155 5.3 % 1.22 [ 0.77, 1.93 ]
Subtotal (95% CI) 155 155 5.3 % 1.22 [ 0.77, 1.93 ]
Total events: 33 (Aripiprazole), 27 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.86 (P = 0.39)
4 glucose - plasma levels >/= 110mg/dl
Carson 2002 b 49/155 51/155 9.9 % 0.96 [ 0.70, 1.33 ]
Subtotal (95% CI) 155 155 9.9 % 0.96 [ 0.70, 1.33 ]
Total events: 49 (Aripiprazole), 51 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.24 (P = 0.81)
5 haemoglobin 1AC - incidence >/= upper limit of normal
Carson 2002 b 17/155 23/155 4.5 % 0.74 [ 0.41, 1.33 ]
Subtotal (95% CI) 155 155 4.5 % 0.74 [ 0.41, 1.33 ]
Total events: 17 (Aripiprazole), 23 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.01 (P = 0.31)
6 low density lipoprotein cholesterol (LDL) - >/= 130 mg/dl
Carson 2002 b 74/155 73/155 14.2 % 1.01 [ 0.80, 1.28 ]
Subtotal (95% CI) 155 155 14.2 % 1.01 [ 0.80, 1.28 ]
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
(Continued . . . )
58Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Weight Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Total events: 74 (Aripiprazole), 73 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.11 (P = 0.91)
7 low density lipoprotein cholesterol (LDL) >/= 160 mg/dl - long-term effect
Carson 2002 b 28/155 28/155 5.4 % 1.00 [ 0.62, 1.61 ]
Subtotal (95% CI) 155 155 5.4 % 1.00 [ 0.62, 1.61 ]
Total events: 28 (Aripiprazole), 28 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.0 (P = 1.0)
8 triglycerides >/= 200 mg/dl long-term effect
Carson 2002 b 46/155 49/155 9.5 % 0.94 [ 0.67, 1.31 ]
Subtotal (95% CI) 155 155 9.5 % 0.94 [ 0.67, 1.31 ]
Total events: 46 (Aripiprazole), 49 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 0.37 (P = 0.71)
9 high density lipoprotein < 40 mg/dl long-term effect
Carson 2002 b 60/155 70/155 13.6 % 0.86 [ 0.66, 1.12 ]
Subtotal (95% CI) 155 155 13.6 % 0.86 [ 0.66, 1.12 ]
Total events: 60 (Aripiprazole), 70 (Placebo)
Heterogeneity: not applicable
Test for overall effect: Z = 1.15 (P = 0.25)
10 prolactin - increase to >/= 23 ng/ml or level above upper limit of normal
Adson 2003 8/312 19/108 5.5 % 0.15 [ 0.07, 0.32 ]
Potkin 2003 7/202 11/103 2.8 % 0.32 [ 0.13, 0.81 ]
Subtotal (95% CI) 514 211 8.3 % 0.21 [ 0.11, 0.37 ]
Total events: 15 (Aripiprazole), 30 (Placebo)
Heterogeneity: Chi2 = 1.67, df = 1 (P = 0.20); I2 =40%
Test for overall effect: Z = 5.24 (P < 0.00001)
Total (95% CI) 1909 1606 100.0 % 0.94 [ 0.86, 1.04 ]
Total events: 491 (Aripiprazole), 501 (Placebo)
Heterogeneity: Chi2 = 35.41, df = 10 (P = 0.00011); I2 =72%
Test for overall effect: Z = 1.18 (P = 0.24)
Test for subgroup differences: Chi2 = 33.96, df = 9 (P = 0.00), I2 =74%
0.1 0.2 0.5 1 2 5 10
Favours aripiprazole Favours placebo
59Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.8. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 8 Leaving the study early.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 8 Leaving the study early
Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
1 due to any reason
Adson 2003 200/312 78/108 0.89 [ 0.77, 1.02 ]
Carson 2000 a 76/204 48/106 0.82 [ 0.63, 1.08 ]
Carson 2002 b 84/155 110/155 0.76 [ 0.64, 0.91 ]
Csernansky 2003 13/34 23/35 0.58 [ 0.36, 0.95 ]
Daniel 2000 67/180 35/64 0.68 [ 0.51, 0.91 ]
Daniel 2004 8/235 3/62 0.70 [ 0.19, 2.57 ]
Marcus 2005 128/279 44/88 0.92 [ 0.72, 1.17 ]
Oren 2005 5/175 1/88 2.51 [ 0.30, 21.19 ]
Potkin 2003 37/202 51/103 0.37 [ 0.26, 0.53 ]
Subtotal (95% CI) 1776 809 0.73 [ 0.60, 0.87 ]
Total events: 618 (Aripiprazole), 393 (Placebo)
Heterogeneity: Tau2 = 0.05; Chi2 = 26.46, df = 8 (P = 0.00088); I2 =70%
Test for overall effect: Z = 3.37 (P = 0.00076)
2 due to adverse effects
Adson 2003 19/312 6/108 1.10 [ 0.45, 2.67 ]
Carson 2000 a 17/204 11/106 0.80 [ 0.39, 1.65 ]
Carson 2002 b 16/155 13/155 1.23 [ 0.61, 2.47 ]
Csernansky 2003 0/34 0/35 0.0 [ 0.0, 0.0 ]
Daniel 2000 10/180 1/64 3.56 [ 0.46, 27.23 ]
Daniel 2004 2/235 0/62 1.33 [ 0.06, 27.45 ]
Marcus 2005 7/279 6/88 0.37 [ 0.13, 1.07 ]
Oren 2005 1/175 0/88 1.52 [ 0.06, 36.86 ]
Potkin 2003 4/202 12/103 0.17 [ 0.06, 0.51 ]
Subtotal (95% CI) 1776 809 0.75 [ 0.42, 1.35 ]
Total events: 76 (Aripiprazole), 49 (Placebo)
Heterogeneity: Tau2 = 0.30; Chi2 = 13.84, df = 7 (P = 0.05); I2 =49%
Test for overall effect: Z = 0.95 (P = 0.34)
0.5 0.7 1 1.5 2
Favours aripiprazole Favours placebo
(Continued . . . )
60Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(. . . Continued)Study or subgroup Aripiprazole Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Total (95% CI) 3552 1618 0.73 [ 0.61, 0.87 ]
Total events: 694 (Aripiprazole), 442 (Placebo)
Heterogeneity: Tau2 = 0.05; Chi2 = 40.14, df = 16 (P = 0.00074); I2 =60%
Test for overall effect: Z = 3.41 (P = 0.00065)
Test for subgroup differences: Chi2 = 0.02, df = 1 (P = 0.90), I2 =0.0%
0.5 0.7 1 1.5 2
Favours aripiprazole Favours placebo
Analysis 1.9. Comparison 1 ARIPIPRAZOLE versus PLACEBO, Outcome 9 concomitant medication -
anxiolytics.
Review: Aripiprazole versus placebo for schizophrenia
Comparison: 1 ARIPIPRAZOLE versus PLACEBO
Outcome: 9 concomitant medication - anxiolytics
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Adson 2003 262/312 91/108 56.7 % 0.98 [ 0.54, 1.78 ]
Marcus 2005 239/279 76/88 43.3 % 0.94 [ 0.47, 1.89 ]
Total (95% CI) 591 196 100.0 % 0.96 [ 0.61, 1.52 ]
Total events: 501 (Treatment), 167 (Control)
Heterogeneity: Chi2 = 0.01, df = 1 (P = 0.94); I2 =0.0%
Test for overall effect: Z = 0.16 (P = 0.87)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
61Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

H I S T O R Y
Protocol first published: Issue 3, 2007
Review first published: Issue 8, 2011
C O N T R I B U T I O N S O F A U T H O R S
El-Sayeh HGG - initial protocol development, data extraction, analysis, writing review.
Belgamwar RB - update review protocol development, data extraction, writing review.
D E C L A R A T I O N S O F I N T E R E S T
Dr Ravindra Belgamwar - none.
Dr Hany George El-Sayeh - none.
S O U R C E S O F S U P P O R T
Internal sources
• North Staffordshire Combined Health Care NHS Trust, UK.
External sources
• none, Not specified.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Apart from two studies (Daniel 2004; Oren 2005), all other studies had high attrition rates. We have included these studies in the
analysis and reported attrition rates. Adson 2003 had a very high attrition rate (higher than 40%); this study had been included in the
original review and is one of the initial aripripazole studies used for gaining its licence. As its inclusion necessitates a deviation from the
protocol, we performed sensitivity analysis to see whether its exclusion makes a significant difference in overall outcome of the results.
The sensitivity analysis is reported by producing a summary table as below.
Outcome Authors’ view after comparing test for overall results with and
without Adson 2003
1.2 Global state: 2. Poor compliance with study protocol due to
lack of efficacy, deterioration or psychosis
No changes to overall outcome
1.3 Global state: 3. Needing additional antipsychotic medication No changes to overall outcome
1.4 Global state: 4. Needing additional benzodiazepines No changes to overall outcome
62Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
1.5 Adverse effects on: anxiety, akathisia, extrapyramidal symp-
toms, headache, insomnia, weight gain, constipation, diar-
rhoea, dyspepsia, dizziness, sedation, asthenia and tachycar-
dia
No changes to overall outcome
1.5 Adverse effects on: nausea, vomiting and agitation Result favours placebo
1.7.10 Prolactin - increase to >/= 23 ng/ml or level above upper limit
of normal
No changes to overall outcome
1.8.1 Leaving the study early: due to any reason No changes to overall outcome
1.8.2 Leaving the study early: due to adverse effects No changes to overall outcome
1.9 Concomitant medication - anxiolytics No changes to overall outcome
We included data on use of concomitant medication for antipsychotics and benzodiazepines.
We have also updated the format and content of the methods section to reflect changes in Cochrane methodology since our protocol
was published, for example the inclsuion of a ’Summary of Findings’ table.
I N D E X T E R M SMedical Subject Headings (MeSH)
Antipsychotic Agents [adverse effects; ∗therapeutic use]; Patient Dropouts [statistics & numerical data]; Piperazines [adverse effects;∗therapeutic use]; Placebos [therapeutic use]; Quinolones [adverse effects; ∗therapeutic use]; Randomized Controlled Trials as Topic;
Schizophrenia [∗drug therapy]
MeSH check words
Humans
63Aripiprazole versus placebo for schizophrenia (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.