beyond the patient: what support systems do our...
TRANSCRIPT

Beyond the patient: What support
systems do our pediatric trauma patients need?
Olivia Burrola Hernandez, M.S., CCC-SLP
Amanda Uribe, BSN, RN

Objectives…
Participants will have a better understanding of: The need for multi-disciplinary coordination of
services
Addressing age-appropriate responses to traumatic events

Long Term Consequences“She is a beautiful 4-year old. She was in
the hospital for several months and has a
severe brain injury. She can’t speak and has
difficulty maintaining balance for sitting. She
is more like a 2-year-old than a 4-year-old.
We know there are many challenges before
us in getting all the services she will need
throughout her life.”
--Jessica’s parents, who found their daughter comatose in
her crib at the age of 3 weeks, injured while in the care of
her nanny

“I have headaches and can’t concentrate in
school. I am a little impatient with my
friends, and they don’t call like they used to.
Maybe I am just over-stressed with sports
and schoolwork?”
--Kiesha, 17, a varsity volleyball player, one year after
sustaining a concussion when she hit her head on the gym
floor and was returned to play in that game against the
recommendation of the athletic trainer.
Long Term Consequences

“Our son is now 11 and has begun to do
poorly in school. We can’t figure out what is
bothering him. He was a great student until
third grade, but he just can’t keep up
anymore. His friends are a little on the wild
side and influence him to do bad things. He
is physically fine. Maybe he should play
sports and get rid of some of this energy.”--Matthew’s parents, discussing academic and behavioral
changes in their son, who was hit by a car when he was 8
years old. Matthew was unconscious for 24 hours,
hospitalized for three days, and discharged home with no
further recommendations.
Long Term Consequences

Core Team Members
Patient
Family
Medical Team
Nursing Team
Case Management
Respiratory Therapy
Laboratory
Radiology
Physical Therapy
Occupational Therapy
Speech-Language Pathology
Child Life Services
Family Support Services
Social Work
Clinical Nutritional Services
Pharmacy

Trauma Informed Care
Incorporating an understanding of posttraumatic stress in
each clinical encounter with ill or injured children and
their families.
SAMHSA promotes the approach of shifting away from
the view of “What’s wrong with this person?” to a more
holistic view of “What happened to this person?”
An organization that is trauma-informed follows the
four “Rs”: Realizes the widespread impact of trauma and understands potential paths
for recovery
Recognizes the signs and symptoms of trauma in clients, families, staff, and
others involved with the system
Responds by fully integrating knowledge about trauma into policies,
procedures, and practices
Actively seeks to resist re-traumatization

ACEs study
Adverse Childhood Experiences (ACEs).
ACEs have been linked to
risky health behaviors,
chronic health conditions,
low life potential, and
early death.
As the number of ACEs increases, so does the risk for these outcomes.
The original ACE Study was conducted at Kaiser
Permanente from 1995 to 1997 with two waves of data
collection.

The ACE Pyramid

12 Core Concepts- NCTSN1. Traumatic experiences are inherently complex.
2. Trauma occurs within a broad context that includes children’s
personal characteristics, life experiences, and current
circumstances.
3. Traumatic events often generate secondary adversities, life changes,
and distressing reminders in children’s daily lives.
4. Children can exhibit a wide range of reactions to trauma and loss.
5. Danger and safety are core concerns in the lives of traumatized children.
6. Traumatic experiences affect the family and broader caregiving
systems.
7. Protective and promotive factors can reduce the adverse impact of trauma.
8. Trauma and posttrauma adversities can strongly influence development.
9. Developmental neurobiology underlies children’s reactions to traumatic
experiences.
10. Culture is closely interwoven with traumatic experiences, response,
and recovery.
11. Challenges to the social contract, including legal and ethical issues, affect trauma
response and recovery.
12. Working with trauma-exposed children can evoke distress in
providers that makes it more difficult for them to provide good care.

Stages of Cognitive Development Sensorimotor Stage: Birth to 2 years
Infant knows and learns about their
environment through movements and
sensations.
Children learn about the world through basic
actions, such as, sucking, grasping, looking
and listening.
Infants develop object permanence.
Infants learn they are separate beings from
the people and objects around them.
Children realize that their actions can cause
things to happen in the world around them.

Stages of Cognitive Development Preoperational Stage: 2 years to 7 years
Children begin to think symbolically and learn
to use words and pictures to represent
objects.
Children are egocentric and struggle to see
things from the perspective of others.
Think about things in very concrete terms.

Stages of Cognitive Development Concrete- Operational: 7 years to 11 years
Children begin to think logically about
concrete events.
Children begin to understand the concept of
conservation (equal volume in various
containers).
Children begin to use inductive logic, or
reasoning, from specific information to a
general principle.

Stages of Cognitive Development Formal Operational: 12 years and older
Individuals begin to think abstractly and
reason about hypothetical problems.
Abstract thought emerges
Individuals begin to think more about moral,
philosophical, ethical, social, and political
issues that require theoretical and abstract
reasoning.
Individuals begin to use deductive logic from a
general principle to specific information.
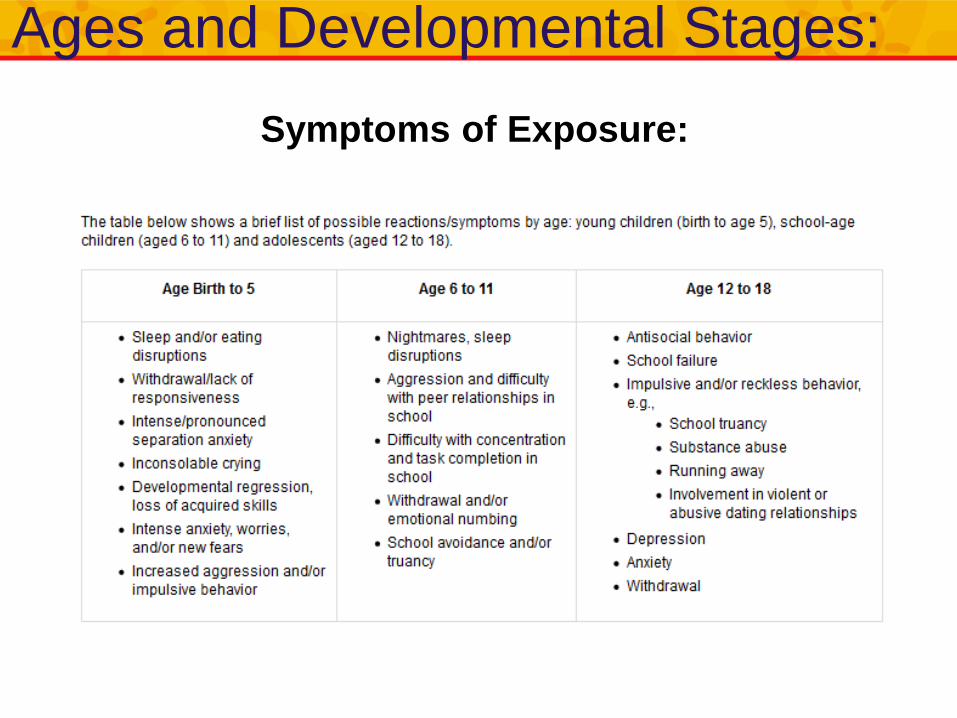
Ages and Developmental Stages:
Symptoms of Exposure:

ReferencesDePompei, R. (2010). Pediatric Traumatic Brain Injury Where Do We Go From Here?. The ASHA Leader. Vol. 15, 16-
20.
Kassam-Adams, N., Rzucidlo, S., Campbell, M., Good, G., Bonifacio, E., Slouf, K., . . . Grather, D. (2015). Nurses'
Views and Current Practice of Trauma-Informed Pediatric Nursing Care. Journal of Pediatric Nursing,
(30), 478-484. Retrieved October 10, 2017, from http://www.pediatricnursing.org/article/S0882-
5963(14)00328-5/fulltext?cc=y=
National Child Traumatic Stress Network - Child Trauma Home |. (n.d.). Retrieved November 25, 2017, from
http://www.nctsn.org Ages and Developmental Stages: Symptoms of Exposure and 12 Core Concepts
O’Connell, K., Fritzeen, J., Guzzetta, C., Clark, A., Lloyd, C., Scott, S., Aldridge, M., Kreling, B. (May 2017). Family
Presence During Pediatric Trauma Care Benefits Patients, Families and Medical Teams. American
Journal of Critical Care. Vol. 26, 229-239
Owens, R. (2015). Language Development An Introduction, 9th Ed., New York, Pearson.
C. (2016, September 01). SAMHSA's Efforts to Address Trauma and Violence. Retrieved November 25, 2017, from
https://www.samhsa.gov/topics/trauma-violence/samhsas-trauma-informed-approach Efforts to Address
Trauma and Violence
Violence Prevention. (2016, April 01). Retrieved November 25, 2017, from
https://www.cdc.gov/violenceprevention/acestudy/index.html
ACEs Study

Thank you!
If you have questions, contact us at:
Amanda 915.298.5444 extension 40653
Olivia 915.242.8360